Embed Size (px)
Citation preview

31
THE FLANK INCISION AND
EXPOSURE OF THE KIDNEY 2Good flank exposure of the kid-
ney can be achieved by many sur-gical approaches. In general, thekidney lies higher than expectedfrom the radiologic studies, withthe left kidney slightly higherthan the right kidney. Except forlower pole renal biopsy, most op-erations require good exposure ofthe renal pelvis and the renalpedicle and thus call for either asupra–twelfth-rib incision or atwelfth-rib rib resection. In the fol-lowing discussion of these twoapproaches, important anatomicconsiderations for all flank expo-sures are highlighted.
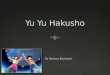
FIG. 2-1. The flexion of the oper-ating table should be in line withthe anterior superior iliac spine ofthe pelvis. This spine is a constantlandmark that the surgeon canpalpate in both thin and obesepatients.
After the patient is positionedon the side, the kidney rest can beelevated and the operating tableflexed. It is important to monitorthe patient’s vital signs becausethe vena cava can be compressedduring this maneuver. We preferthat the patient is in a straight lat-eral position 90 degrees to thetable as opposed to an angled po-sition; the straight lateral positioncan be angled by simple rotationof the operating table from side toside. The surgeon should apply 5-inch–wide adhesive tape horizon-tally across at the level of the iliacspine and around the operatingtable to secure and maintain thepatient in this flank position. Thetaping stabilizes patient position
perpendicular to the operatingtable and thus allows the operat-ing table to be rolled from side toside for improved exposure of theanterior or posterior kidney.
Although the anterior superioriliac spine is positioned at the flex-ion of the table, when the table isfully flexed, the final position ofthe body will cause the entirepelvis to be slightly below theapex of the flexion and the ribs tobe slightly above, which createstension in the area of the lower
2-1
Flank Position
Tension placed on ribs and skin
Anterior Superior iliac spinein line with flexion of table
Flexion of lower Leg
Anterior Superior iliac spine
Axillary Pad

32 Critical Operative Maneuvers in Urologic Surgery
ribs and flank. The surgeonshould palpate the region be-tween the eleventh and twelfthribs and between the ribs and theiliac spine when the operatingtable is adequately flexed to en-sure that this tension has beenmaintained.
The lower leg is flexed to 90 de-grees at the knee to prevent thebody from rolling from side toside, but the upper leg is keptstraight to maintain the tension ofthe incision site; pillows are placedbetween the legs as support.
An axillary pad is placed underthe lower dependent arm to pre-vent any neural compression. Theupper arm should be placed on anairplane rest for stabilization.
EXPOSURE
For any flank exposure of thekidney, the surgeon must releasethree components holding the ribstogether:
1 Intercostal muscles2 Diaphragmatic attachments
to the ribs and retroperito-neum
3 Internal intercostal mem-brane holding the proximalribs together
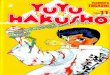
Supra–Twelfth-Rib IncisionFIG. 2-2. The surgeon makes the
incision extending from the lateral
border of the rectus abdominismuscle to beyond the posterioraxillary line. This incision is es-sentially slightly superior to thetwelfth rib.1 Anterior and medialto the rib, the external oblique (1),internal oblique (2), and transver-sus abdominis (3) muscles are se-quentially divided.
Although it is not always pos-sible, the surgeon should attemptto preserve the intercostal nerve toprevent the “frog belly” protru-sion of the abdomen after surgery.The intercostal nerve can be freedfrom the muscles and can bepushed medially and laterally tothe incision during the operation.
Once the internal oblique mus-cle is divided, the dense lumbardorsal fascia, which lies anteriorand medial to the tips of theeleventh and twelfth ribs, can beidentified.
FIG. 2-3. By opening this fasciallandmark, the surgeon can enterthe retroperitoneal space and mo-bilize the peritoneum anteriorly.
FIG. 2-4. The surgeon inserts theleft index and middle fingers andbluntly spreads the fingers be-neath the transversus abdominismuscle to establish a dissectionplane between the anterior peri-toneum and the muscle. Thetransversus abdominis muscle isthen divided to the lateral marginof the rectus fascia.
3
2
1Eleventh
rib
Twelfthrib
Lumbardorsalfascia
Transversusabdominis
muscle
Internalobliquemuscle
External oblique muscle
Rectus abdominis muscle
Flankincision
2-2
2-3
Lumbar dorsal fascia opened
11
12
Divided transversusabdominis muscle
Peritoneumreflected medially2-4

Chapter 2 The Flank Incision and Exposure of the Kidney 33
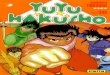
FIG. 2-5. The two large muscles,the latissimus dorsi and the serra-tus posterior, are partially dividedto expose the posterior part of theribs and the intercostal muscles.One common error is to fail tocomplete the posterior dissectiondespite an excellent anterior dis-section.
FIGS. 2-6 AND 2-7. The surgeon usesa sponge stick bluntly and gentlyto sweep the posterior Gerota’sfascia medially off the psoas andquadratus lumborum muscles (1in Fig. 2-6). The kidney and peri-toneum are rolled medially bythis maneuver, exposing the pos-terior surface of the kidney andits pedicle in Gerota’s fascialcompartment.
Latissimusdorsi muscle
Pleural cavity
Eleventh rib
Twelfth rib
Lumbar dorsal fascia
Serratus posterior muscle
Cut edge of latissimusdorsi muscle
Iliac crest2-5
12
11
Latissimus dorsi muscle
Serratus posterior muscle
Psoasmuscle
Kidney
Peritoneumreflected medially2-7
External oblique muscleInternal oblique muscle
Transversus abdominismuscle
Latissimus dorsi muscle
Quadratus lumborummuscle
Serratus posterior musclePsoas muscle
Sacrospinalis muscle
Proper entry for vascular isolation
Peritoneum
Rectus abdominismuscle
Peritoneum
1
Entry into Retroperitoneum
Kidney withGerota's fascia
2-6

34 Critical Operative Maneuvers in Urologic Surgery
Diaphragmatic Attachments
FIGS. 2-8 AND 2-9. With outwardtraction of the free end of thetwelfth rib, the surgeon uses theright index finger and gentlypushes proximally against theinner aspect of the twelfth rib,thereby separating strands of thediaphragmatic muscles from therib. This maneuver exposes the in-ner aspect of the rib completelyand gives the surgeon a clear viewof the diaphragmatic muscles’ at-tachments to the rib and retroper-itoneum. These diaphragmatic at-tachments are then divided.
Using the index finger, the sur-geon must apply pressure againstthe rib rather than on diaphrag-matic muscles or the adjacentpleura. This maneuver, in essence,separates the pleura from the rib.
Intercostal Attachments
FIG. 2-10. With the same tractionapplied outward and downwardon the distal tip of the twelfth rib,the intercostal muscles are nowgently divided from the superiormargin of the rib, beginning at thedistal tip of the rib and extendingto the proximal region, avoidinginjury to the pleura.
The surgeon can divide themuscle directly above the ribwithout injury to the vasculatureand nerves, which are located im-mediately below the rib.
FIG. 2-11. The surgeon’s right in-dex finger pushes gently againstthe most proximal inner aspectof the twelfth rib until the junctionof the vertebral body is felt. Thesurgeon can now palpate the in-ternal intercostal membrane andeleventh rib above. The intercostalmembrane is a thin, dense band oftissue holding the two ribs to-gether. Only this dense membraneis divided; the tissue deeper tothis membrane is left intact. Whendividing this membrane, the sur-geon can feel the release of ten-sion. The Finochetto retractor withtwo dry laparotomy pads can beplaced on either side of the ribsand opened slowly for full expo-sure of the kidney.
This same exposure can be ap-plied to the eleventh rib if neces-sary.
Twelfth-Rib Rib ResectionFIG. 2-12. Using periosteal eleva-
tors such as Doyen periosteal ele-vators, the surgeon first cleans andfrees the rib from its intercostal at-tachments with periosteal eleva-tors in opposing directions as illus-trated. The Doyen elevators curlaround the bony rib and essen-tially release the periosteum andits diaphragmatic attachments.
Diaphragmaticattachments to ribs
Crus ofdiaphragm
2-8
Pleura
Diaphragmatic attachments
Rib
Plane of dissection
Lung
Diaphragmaticattachments
2-9
Latissimusdorsi muscle
Serratusposterior muscle
Vessels and nerves
Intercostal muscles
11
12
2-10

Internal intercostal membraneand costotransverse ligament
Eleventhrib
Chapter 2 The Flank Incision and Exposure of the Kidney 35
AIntercostal nerve (ventralramus of thoracic nerve)
Internal intercostal membraneover external intercostal muscle
Externaloblique muscle
Innermostintercostal muscle
Internal intercostal muscle
External intercostal muscle
Rectus abdominis muscle
ScapulaInfraspinatus muscle
Subscapularismuscle
Serratusanteriormuscle
Internal intercostal membrane
2-11
B © Copyright 1995. CIBA-GEIGYCorporation. Reprinted withpermission from Atlas of HumanAnatomy illustrated by FrankNetter, M.D. All rights reserved.
B
2-12
Rib
Nerve andvasculature
Doyen periostealelevators

36 Critical Operative Maneuvers in Urologic Surgery
Since the rib is resected at itsproximal end with rongeurs, thereis no need to divide the intercostalmembrane as is performed in thesupra–twelfth-rib incision.
After the rib is resected, thesurgeon uses blunt dissection toreestablish the plane between thequadratus lumborum and psoasmuscles on one side and the pos-terior Gerota’s fascia and kidneyon the other side as described pre-viously.
SIMPLE NEPHRECTOMY ANDRECONSTRUCTIVE RENAL SURGERY
FIG. 2-13. The surgeon divides themost lateral posterior aspect of theGerota’s fascia to expose the lat-eral surface of the kidney.
Dissection between the Ge-rota’s fascia and the kidney medi-ally on both sides provides excel-lent exposure of the kidney, renalpelvis, and renal pedicle.
RADICAL NEPHRECTOMY IN FLANKPOSITION FOR SMALL RENALCANCERS IN LOWER HALF OFKIDNEY
FIG. 2-14. The dissection pre-serves the integrity of the Gerota’sfascia and includes the adrenalgland (1).
The surgeon separates the pos-terior Gerota’s fascia from thepsoas muscle (2).
The surgeon then identifies theupper ureter and places a vesselloop for traction. Often the go-nadal vein is next to the ureterand can be divided on the rightside.
The most difficult maneuver ofthe operation is to separate theposterior peritoneum from the an-terior Gerota’s fascia (3). The as-sistant holds the peritoneum upwhile the surgeon uses the fingersto gently tease a dissection planebetween the two. The reflection ofthe posterior peritoneum can of-ten be seen and used as a guide.As the surgeon gently uses the
fingers to separate the two layers,first the renal vein and then therenal pelvis can be identifiedmedially.
With the patient in the fullflank position for right-side dis-section to expose the kidney, thesurgeon will not see the duode-num as clearly as when the pa-tient is in the supine position(Kocher maneuver, see p. 12). Asthe separation of the peritoneumand the Gerota’s fascia is com-pleted, the duodenum will be justanterior to the vena cava.
FIG. 2-15. From the anterior as-pect of the kidney, the surgeoncan usually identify all venousstructures, renal vein, adrenalvein, gonadal vein, and lumbarvein.
At times it may be necessary tofree the entire posterior Gerota’sfascia from the posterior musclesto isolate the renal artery locatedslightly inferior to and behind therenal vein.
The renal artery is always li-gated and/or divided before therenal vein is. Two ties (0 silk) areplaced proximally and one distally.
Superiorly, the surgeon followsthe Gerota’s fascia and proceedsbeyond the adrenal gland. Whilecautiously using gentle down-ward traction with the left indexand middle fingers on either sideof the adrenal gland, the surgeoncan clip and divide the attach-ments superiorly with the righthand. If the adrenal vein has notbeen identified yet, it will usuallylie on the medial aspect of theadrenal gland (for right-sidednephrectomy).
RENAL AND ADRENALVASCULATURE
On the right side, the adrenal, re-nal, and gonadal veins branch di-rectly from the vena cava, whereason the left side, the adrenal, acces-sory lumbar, and gonadal vesselsjoin the renal vein.
On the right side, the adrenal
2-13
2-14
Division ofGerota's
fascia foraccess to
kidney
Kidney
Adrenal gland
3
2
1

Chapter 2 The Flank Incision and Exposure of the Kidney 37
vein can be injured during a radi-cal nephrectomy for large upperpole cancer as previously dis-cussed (see p. 12).
FIG. 2-16. On the left side, the loca-tion and vasculature of the adrenalgland is more accessible and eas-ier to expose. The most commonvenous injury involves the acces-sory lumbar vein draining into therenal vein from a posterior posi-tion. Because this vein is locateddirectly behind the renal vein, thesurgeon may miss it before divid-ing the renal pedicle vein (seep. 20).
PLEUROTOMY
Inadvertent pleurotomy is com-mon with flank incisions. The sim-plest method to correct this prob-lem is to insert a chest tube (seep. 23).
For a small opening, a red rub-ber catheter can be placed withinthe pleural cavity, and the open-ing can be closed with a stitch (2-0chromic).
After the surgery is completedand the wound is reapproximatedaround this catheter, the proximalend of the red rubber catheter isplaced to an underwater seal suchas a medicine cup filled with water.
The anesthesiologist can ex-pand the lung by inflation and canpush the air within the cavity outthrough the red rubber catheter.
The surgeon gradually movesthe catheter out while watchingfor air bubbles to be expelled.
When no further air bubblescome out through the catheter, thesurgeon pulls the catheter out.
In most cases, the postoperativechest radiograph shows a smallresidual defect of 10% pneumo-thorax. This small defect does notrequire treatment but needs onlymonitoring with serial radio-graphs.
Rightadrenal
vein
Rightrenal
artery
Rightrenal vein
Rightgonadal
vein
Left adrenalvein
Left renalartery
Left renal veinLumbar vein
Left gonadalvein
2-15
A
Rightrenalvein
Rightgonadal
vein
Leftadrenalvein
Leftrenalvein
Leftgonadal
vein
Rightadrenal
vein
B
Leftrenalvein
Leftgonadal
vein
Leftadrenalvein
Accessorylumbarvein
2-16

38 Critical Operative Maneuvers in Urologic Surgery
K E YP O I N T S
� The patient is positioned withthe anterior iliac crest in line withthe flexion of the table.
� The retroperitoneum space is es-tablished first.
� The intercostal muscles, di-aphragmatic attachments, andintercostal membrane (for supra–twelfth-rib incision) are released.
� Note that above the twelfth ribthe pleura can be easily sweptoff, whereas the pleura is moreadherent to the ribs above theeleventh rib.
� The Gerota’s fascia is divided toexpose the kidney and renalpedicle for reconstructive renalsurgery.
� The posterior peritoneum andanterior Gerota’s fascia are sepa-rated to expose the renal pediclefor a cancer operation.
� The right adrenal vein is care-fully dissected out for right-sidedtumors. For left-sided tumors, thesurgeon must watch for the lum-bar vein draining into the renalvein from a posterior position.
P O T E N T I A LP R O B L E M S
� Pleurotomy: Perform postopera-tive closure with the tip of a redrubber catheter in the pleuralcavity and the open end to an un-derwater seal to blow out the airin the pleural cavity or placechest tube
� Intercostal vasculature and nerve in-jury: Achieve hemostasis by elec-trocoagulation → perform stitchligation of vasculature not in-cluding the nerve
� Inadvertent opening of the posteriorperitoneum: Perform immediateclosure because this defect maybe forgotten subsequently
� Torn adrenal vein on right side: Ap-ply hand compression on thevena cava → apply curved Satin-sky vascular clamp on a cuff ofthe vena cava before repairs ifnecessary (see p. 59)
� Excessive manipulation of left-sideddissection leading to splenic injurywith hemorrhage suspected based onsudden drop in blood pressure: Per-form peritoneotomy → explorespleen to see if preservation ispossible → if not, perform splen-ectomy (see p. 28)
REFERENCE1 Turner-Warwick RT: The supracostal
approach to the renal area, Br J Urol37:671, 1965.