Embed Size (px)
Citation preview

9/14/2015
1
Target Specific Oral Anti-Coagulants: Management in the Peri-Endoscopic PeriodC. Andrew Kistler, MD, PharmDDaniel M. Quirk, MD, MPH, MBADivision of Gastroenterology and HepatologyThomas Jefferson University Hospital
Disclosures
• I have no financial relationships to disclose

9/14/2015
2
Objectives
• Review the Target Specific Oral Anticoagulants (TSOACs)• Dosing and monitoring• Pharmacodynamics/Pharmacokinetics, Drug-Drug Interactions
(DDIs)• GI adverse events
• Discuss the impact of TSOACs on endoscopic procedures• Pre- and post-procedure management• Acute management of gastrointestinal bleeding• Ongoing and future studies evaluating TSOACs and GI procedures
• Retrospective reviews• Reversal agents
Anticoagulation in Atrial Fibrillation
• Atrial fibrillation is associated with a 5 fold increase in ischemic stroke
• Warfarin reduces the risk of stroke in patients with atrial fibrillation by 2/3
• Warfarin Limitations• Unpredictable pharmacodynamics and pharmacokinetics
• Genetic polymorphisms• Variations in dietary vitamin K intake
• Numerous drug-drug interactions (DDIs)• Need for monitoring (INR)

9/14/2015
3
Thromboembolic and bleeding risk
• Thrombotic risk• CHA2DS2-Vasc Score (atrial fibrillation)• Caprini score (VTE)
• Bleeding risk• HAS-BLED score (atrial fibrillation)• RIETE score (VTE)
CHA2DS2-Vasc Score
CHA2DS2 Vasc Factor Points
C CHF 1
H HTN 1
A2 Age >75 2
D DM 1
S2 Stroke, TIA, TE 2
V Vascular disease 1
A Age 65-74 1
Sc Sex category: F 1
January CT, et al. 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation: J Am Coll Cardiol 2014.
CHA2DS2Vasc
Ischemic Stroke Rate/year
0 0.2%
1 0.6%
2 2.2%
3 3.2%
4 4.8%
5 7.2%
6 9.7%
7 11.2%
8 10.8%
9 12.2%
MAX SCORE = 9

9/14/2015
4
HAS-BLED
HAS-BLED Risk Factor Points
H HTN (SBP >160mmHg) 1
A Abnl renal or liver fx 1 or 2 (each 1)
S Stroke 1
B Bleeding(hx, anemia, predisposition)
1
L Labile INR 1
E Elderly (>65 yrs.) 1
D Drug (antiplatelet,NSAIDs) or ETOH
1 or 2 (each 1)
Total Points Major bleeding risk, %
2 3.3
3 3.9
4 6.1Apolstolakis S. J Am Coll Cardiol. 2013 Jan 22;61(3):386-7.
TSOACs: Target Specific Oral Anticoagulants• Specifically target either factor Xa or IIa (thrombin)• AKA novel oral anticoagulants (NOACs) & direct oral anticoagulants
(DOACs)• Four TSOACs currently FDA approved
• Indications:• DVT/PE post-op prophylaxis and treatment• Prevention of stroke in non-valvular atrial fibrillation
• At least as effective as warfarin for stroke prevention• ½ the rate of intracranial hemorrhage• Fixed dosing without monitoring
• ? Impact on compliance• Higher cost
• No generic formulations available
Factor Xa Inhibitors Direct Thrombin Inhibitors
Rivaroxaban (Xarelto ®)Apixiban (Eliquis ®)Edoxaban (Savaysa ®)
Dabigatran etexilate(Pradaxa ®)

9/14/2015
5
Desai J et al. Gastrointestinal Endoscopy 2013;78:227-239.
TSOACs: Pharmacologic ComparisonTSOAC Dabigatran Rivaroxaban Apixaban Edoxaban
Brand Name Pradaxa ® Xarelto ® Eliquis ® Savaysa ®
MOA DTI FXa Inhibitor FXa Inhibitor FXa Inhibitor
Dosing 150 mg BID75 mg BID
10/15/20 mg QD-BID 2.5/5/10 mg bid 15-60 mg QD*dose dec if <60 kg
Renal Dosing GFR: 15-30 = 75 mg bid (*watch DDIs)
GFR>50 = 20 mg qpmGFR 15-50: 15 mg qpm
N/A* unless:SCr > 1.5 mg/dL and > 80 yo OR wt < 60 kg
GFR>95 = don’t use (inc risk of stroke)15-50: 30 mg qd<15: don’t useDose Dec if <60 kg
Hepatic Dosing Avoid in severe Avoid in mod-severe Avoid in severe Avoid in mod-severe
Half Life 12-17 hrs 5-9 hrs 8-15 hrs 10-14 hrs
Protein Binding 35% (HD ~50-60%)
92-95% ~87% 55%
Monitoring Prolonged aPTTECT, TT**
PT, anti-FXa activity PT, INR, PTT, anti-FXa acitivity
PT, PTT
GI Side Effects 25-35% (dyspepsia, gastritis)
<3% (N, AP,dyspepsia)
Nausea: 3%Elev LFTs: < 1%
Elev LFTs: 5-8%
Misc Open capsules = incF by 75%
*not studied in SCr>2.5 or CrCl <25
Not dialyzable

9/14/2015
6
TSOACs vs Warfarin
Desai J et al. Gastrointestinal Endoscopy 2013;78:227-239
Drug-Drug Interactions
Dabigatran/Edoxaban Rivaroxaban/Apixaban/Edoxaban
Increase plasma levels of TSOACs(increase bleeding risk)
P-glycoprotein inhibitors: Fluconazole, verapamil, systemic azole antifungals, cyclosporin, dronedarone, tacrolimus, clarithromycin, erythromycin, HIV protease inhibitors
CYP3A4 and/or P-glycoprotein inhibitors: systemic azole antifungals, protease inhibitors, diltiazem,erythromycin, grapefruit juice, quinidine, tacrolimus, verapamil
Reduce plasma levels of TSOACs(increase VTE risk)
CYP3A4 and/or P-glycoprotein inducers: carbamazepine, phenobarbital, phenytoin, rifampin, St John’s wort
Pharmacodynamic(increased bleeding risk)
Aspirin, NSAIDs, selective COX-2 inhibitors, clopidogrel, prasugrel and ticagrelor, fish oils,Thrombolytics, SSRIs, SNRIs

9/14/2015
7
Pharmacodynamics
Desai J et al. Gastrointestinal Endoscopy 2013;78:227-239
Major Clinical Trials
RE-LY ROCKET-AF ARISTOTLE ENGAGE
NOAC Dabigatran Rivaroxaban Apixaban Edoxaban
Comparator Warfarin Warfarin Warfarin Warfarin
Design Multicenter/Ran Multicenter/Ran Multicenter/Ran Multicenter/Ran
Blinding Open Blinded Blinded Blinded
Endpoint Stroke/SEE Stroke/SEE Stroke/SEE Stroke/SEE
Safety end. Bleeding Bleeding Bleeding Bleeding
Dose 110mg/150mg BID 20mg daily 5mg BID 30mg/60mg
No. pts 18,113 14,264 18,201 21,105
No. countries 44 45 39 46
No. sites 951 1178 1034 1393
Pub date Sept 17, 2009 Sept 8, 2011 Sept 15, 2011 Nov 28, 2013
Trial duration 2 years 2 years 2 years 2 years

9/14/2015
8
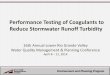
TSOAC & Warfarin Comparison: Major Safety and Efficacy Rates
Risk Dabigatran Rivaroxaban Apixaban Edoxaban
Stroke & SE
Major Bleed*
Maj GI Bleed
Intracranial B
Isch. stroke
All mort.
Desai J et al. Gastrointestinal Endoscopy 2013;78:227-239Giugliano RP et al. N Engl J Med 2013;369:2093-2104
*major bleeding definition: dec in Hgb > 2 gr/dL or transfusion of > 2 U PRBC or bleeding into critical site (ICH, intraspinal, intraocular, pericardial, intra-articular, IM w/ compartment syndrome, RP) or fatal bleeding
TSOAC Risk of Bleeding Per Year vs WarfarinRisk Dabigatran Rivaroxaban Apixaban Edoxaban
Major Bleed 3.32% vs 3.57% (P=0.32)
3.6% vs 3.4%(P=0.58)
2.13% vs 3.09%(P<0.001)
2.75% vs 3.43% (P<0.001)
Major GI Bleed 1.85% vs 1.36%(P=0.002)*esp initialmonths,morelife-threatening (0.76% vs 0.48%)
2.0% vs 1.24% 0.76% vs 0.86% (P=0.37)
Hi dose: 1.51% vs 1.23% (P=0.03)Low dose: 0.82 % vs 1.23% (P<0.001)
Type of GIB UGIB > LGIB N/A UGIB >LGIB UGIB > LGIB
Desai J et al. Gastrointestinal Endoscopy 2013;78:227-239Giugliano RP et al. N Engl J Med 2013;369:2093-2104

9/14/2015
9
Prevention of TSOAC-related bleeding
• Adhere to administration guidelines and indications• Minimize risk factors• Concomitant ASA only for those with clear indication
• Bleeding risk for dabigatran is 30% - 50% higher with anti-platelet agents
• Consider PPI therapy for those on chronic NSAIDS• Intermittent monitoring of patient’s age, weight, and renal
function
• Utilize bleeding scores to risk-stratify patients• Consultation with cardiology and neurology
ASGE Standards of Practice Committee, Anderson MA, et al. Gastrointest Endosc. 2009 Dec;70(6):1060-70.

9/14/2015
10
Peri-endoscopic TSOAC management
• Balance the risk of thrombosis and the risk of bleeding• Thrombotic risk of interruption (<1 week) is <0.5%/day in non-
valvular atrial fibrillation• TSOACs are easier to titrate than warfarin
• Rapid return of ability to coagulate: 12-24 hrs.• Near complete coagulation recovery in 5 drug half-lives• Anticoagulation restored within hours of next dose
• Low risk procedures: diagnostic endoscopy or bx• Continue treatment and ideally schedule procedure at trough (~10
hrs) if can be safely done• High risk procedures: polypectomy, PEG, Sphincterotomy, FNA
• Normal renal function: hold 2-3 half-lives (24 -48 hrs.)• Renal insufficiency (GFR 30-50 mL/min): hold 3-5 days• Consider consultation with cardiology +/- neurology in patients at
higher risk that may require bridging therapy
Pre-procedure TSOAC management
Dabigatran Rivaroxaban Apixaban
Procedure risk Hold daysLow risk 2 days 1 day 1 day
High risk 4 days 2 days 2 days
Renal Dysfunction Hold daysLess Severe 1 or 2 days (> 50 mL/min) > 1 day (> 90 mL/min) 1 or 2 days (> 60 mL/min)
3 – 5 days (< 50 mL/min) 2 days (60-90 mL/min) 3 days (50-59 mL/min)
3 days (30-59 mL/min) 4 days (30-49 mL/min)
More Severe 4 days (15-29 mL/min)
Baron et al. NEJM.2013May;368:(22):2113-24.Kozek-Langenecker SA. Seminars in Hematology.2014;51:112-120.Dincq et al. BioMed Research International.2014;1-16.
2

9/14/2015
11
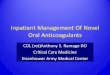
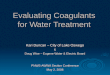
Peri-procedural TSOAC management
Dincq et al. BioMed Research International.2014;1-16.
Peri-procedural TSOAC management
Baron et al. NEJM.2013May;368:(22):2113-24.

9/14/2015
12
Peri-endoscopic TSOAC management
• Resumption of TSOAC• Peak plasma concentrations in 2-3 hrs.• Options
• Immediately• Diagnostic• Cold snare < 5 mm
• > 2-3 days• Large flat polyp >1-2.5 cm with injection and cold snare• ? Benefit of prophylactic clipping
• Reasonable protocol• Resume 24-48 hrs. after hemostasis has been achieved• Warn patient of risk of delayed bleeding particularly for post-cautery (up
to two weeks)• Resume in > 72 hours in patients undergoing sphincterotomy
TSOACs: Management of acute GI bleeding
• ASGE 2009 guidelines: the decision to reverse should be individualized based on the potential risk of thrombosis and continued bleeding
• There are no FDA approved antidotes for TSOACs• Supportive Care
• IVF• PRBCs• Consider platelets for those on anti-platelet therapy
• Early endoscopy vs. supportive care and stabilization for 12 hrs.• Rapid loss of anticoagulation effect in patients with normal renal and liver
function• Laboratory monitoring
• Dabigatran: Prolonged aPTT, ECT, TT (most sensitive)• Rivaroxaban: PT, anti-FXa activity• Apixiban: PT, INR, PTT, anti-FXa acitivity• Edoxaban: PT, PTT• Results of TT and Anti-Factor Xa assay are typically not rapidly available

9/14/2015
13
TSOAC Acute Bleeding Management OptionsTSOAC Dabigatran Rivaroxaban Apixaban Edoxaban
Brand Name Pradaxa ® Xarelto ® Eliquis ® Savaysa ®
MOA DTI FXa Inhibitor FXa Inhibitor FXa Inhibitor
Renal Excretion 80-85% 35% 25% 35%
Half Life 12-17 hrs 5-9 hrs 8-15 hrs 10-14 hrs
Five Half Lives (normal renal fxn)
60-85 hrs 25-45 hrs 40-75 hrs 50-70 hrs
Reversal Management aPCC (FEIBA) >PCCAminocaproic AcidTranexamic AcidCharcoal (<2 hrs)HD (~50% removal)PRBC/PltmAb (Phase III)
Unactivated PCCAminocaproic acidTranexamic AcidCharcoal <2-8 hrsPRBC/Plt***NO DIALYSIS 2/2 high protein binding
Unactivated PCCAminocaproic acidTranexamic AcidCharcoal <2-8 hrsPRBC/Plt***NO DIALYSIS 2/2 high protein binding
Unactivated PCCAminocaproic acidTranexamic AcidCharcoal <2-8 hrsPRBC/Plt***NO DIALYSIS 2/2 high protein binding
**Activated PCC (FEIBA): factors II, VII, IX, X (and Protein C/S)4 Factor unactivated PCC: II, VII, IX, X (Kcentra ®) (and Protein C/S)3 factor unactivated PCC: II, IX, X (and Protein C/S)
*DISCLAIMER: There are no FDA approved antidotes for any TSOAC
Endoscopic management
• Consider emergent upper or lower endoscopy: • Acute hemorrhage• Persistent or recurrent hypotension• Signs of end-organ hypoperfusion• Failure to respond to supportive measures
• Delayed endoscopy (12-24 hrs.)• Stable hemodynamics or respond to resuscitation• Theoretical advantages:
• Increased effectiveness of endoscopic therapy• Increased safety in semi-elective setting• Increased time for colon cleansing if needed• Enhanced endoscopic visualization

9/14/2015
14
TSOAC Antidotes: Future Research
• PER977• Intravenous Cation that binds all TSOACs through hydrogen
bonds (Edoxaban > other TSOACs)• Currently in Phase II clinical trials
• Idarucizumab• Intravenous monoclonal antibody that binds dabigatran• Entering Phase III clinical trials
• Andexanet Alfa• Intravenous Factor Xa decoy that binds FXa inhibitors• Phase III
Conclusions
• TSOACs have their own distinct pharmacokinetic properties that vary considerably from warfarin
• TSOACs are associated with a higher risk of major GI bleeding when compared to warfarin• Apixaban is at least equivalent to warfarin
• There are no formal guidelines on the acute GIB management or peri-procedural endoscopic management of TSOACs• Important factors to consider include renal function, drug-drug
interactions, age and the risk of both procedure and condition
• There are no FDA approved antidotes for TSOACs, however several agents are currently being studied

9/14/2015
15
Acknowledgements
• Pennsylvania Society of Gastroenterology Board Members• Dr. Manish Thapar• Dr. David Sass• Dr. Dan Quirk• Dr. AJ DiMarino• Dr. Sri Nagalla
References
• Ansell JE , et al. NEJM. 2014 Nov 27;371(22): 2141-2.• Apolstolakis S, et al. J Am Coll Cardiol. 2013 Jan 22;61(3):386-7.• ASGE Standards of Practice Committee, Anderson MA, et al. Gastrointest Endosc. 2009 Dec;70(6):1060-
70.• Baron et al. NEJM.2013 May;368:(22):2113-24.• Desai J et al. Gastrointestinal Endoscopy 2013;78:227-239.• Desai J, et al. Thromb Haemost. 2013 Aug;110(2):205-12.• Dincq et al. BioMed Research International.2014;1-16.• Eliquis ® (Apixiban) [package insert]. Princeton, NJ: Bristol-Myers Squibb Company; December 2012. • Giugliano RP et al. N Engl J Med 2013;369:2093-2104• January CT, et al. J Am Coll Cardiol 2014.• Kozek-Langenecker SA, et al. Seminars in Hematology.2014;51:112-120.• Pollack CV, et al. NEJM. 2015 Aug 6;373(6):511-20.• Pradaxa ® (Dabigatran Etexilate Mesylate) [package insert]. Ridgefield, CT: Boehringer Ingelheim
Pharmaceuticals, Inc.;December 2012.• Savaysa ® (Edoxaban) [package insert]. Parsippany, NJ: Daiichi Sankyo, Inc.;January 2015. • Xarelto ® (Rivaroxaban) [package insert]. Titusville, NJ: Janssen Pharmaceuticals, Inc.; November
2012.