Embed Size (px)
Citation preview

H a n n a h W u n s c h , M D M S cH e r b e r t I r v i n g A s s i s t a n t P r o f e s s o r o f A n e s t h e s i o l o g y &
E p i d e m i o l o g y
D e p a r t m e n t o f A n e s t h e s i o l o g y , C o l l e g e o f P h y s i c i a n s & S u r g e o n sD e p a r t m e n t o f E p i d e m i o l o g y , M a i l m a n S c h o o l o f P u b l i c H e a l t h
C o l u m b i a U n i v e r s i t y
Targeting patients for use of dexmedetomidine

Conflicts
• None
• Talking about off-label uses of dexmedetomidine
Dexmedetomidine
Alpha-2 agonist
7 times more selective than clonidine for the receptor
Infusion only
0.2 to 1.5 μg/kg/hr PER HOUR
Loading dose of 1 mcg/kg over 10 min
Distribution half-life of 6 minutes
Terminal elimination half-life of 2 hours
Hepatic clearance, renal excretion of metabolites

US FDA approval
1999/2000
Mechanically ventilated patients in the intensive care setting up to 24 hrs
0.2 to 0.7 μg/kg/hr
2008
Non-intubated patients requiring sedation prior to and/or during surgical and other procedures
Canada
Sedation of initially intubated and mechanically ventilated postsurgical patients during treatment in an intensive care setting by continuous intravenous infusion (must not exceed 24 hours).
Sedation of non-intubated patients prior to and/or during surgical and other procedures: Monitored Anesthesia Care (MAC)
Awake Fiberoptic Intubation (AFI)
Clinical profile
Anxiolysis
Some analgesia
No respiratory depression Can keep it going during extubation
No amnesia
Bradycardia
hypotension

Does it help with delirium?
Delirium
• 4 large RCTs recently in JAMA• MENDS
• (vs lorazepam)
• SEDCOM
• (vs midazolam)
• MIDEX/PRODEX
• (vs midazolam and vs propofol)
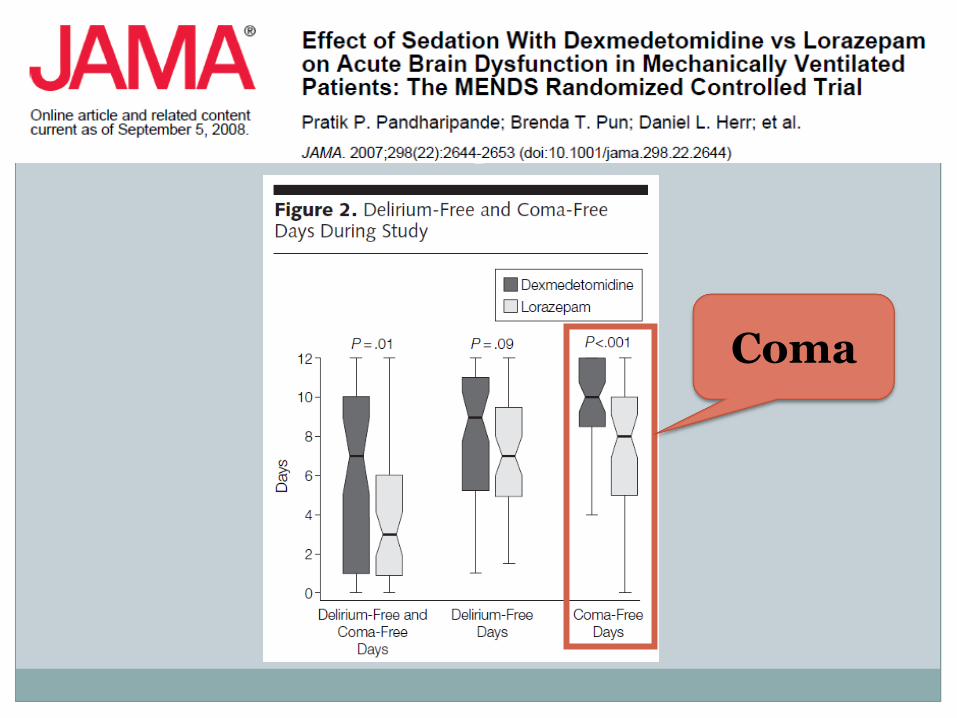
Coma

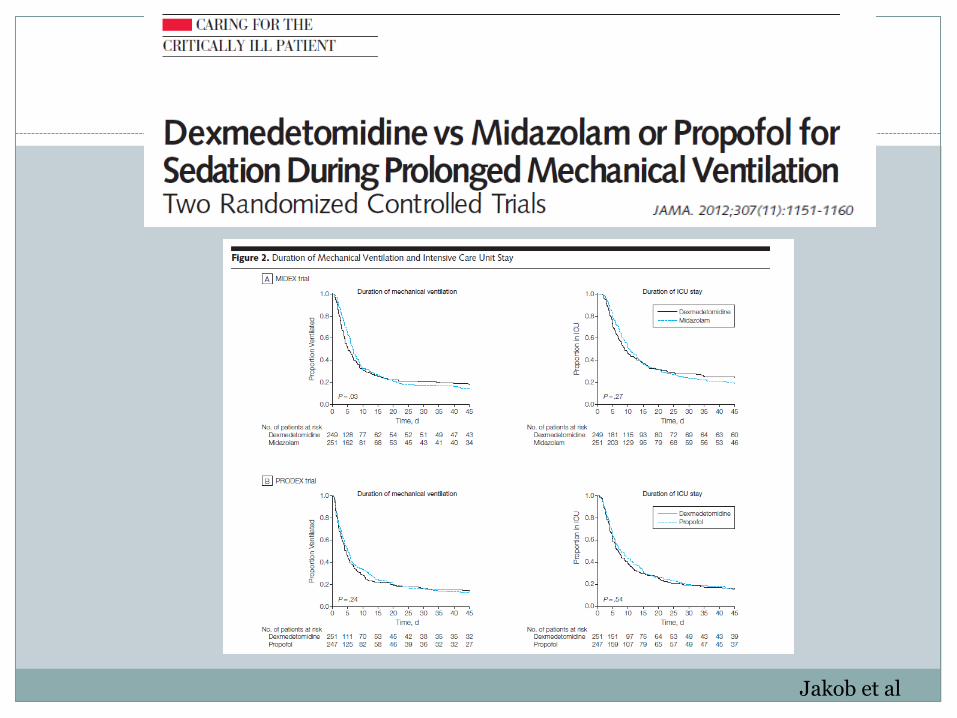
PRODEX/MIDEX
Jakob et al
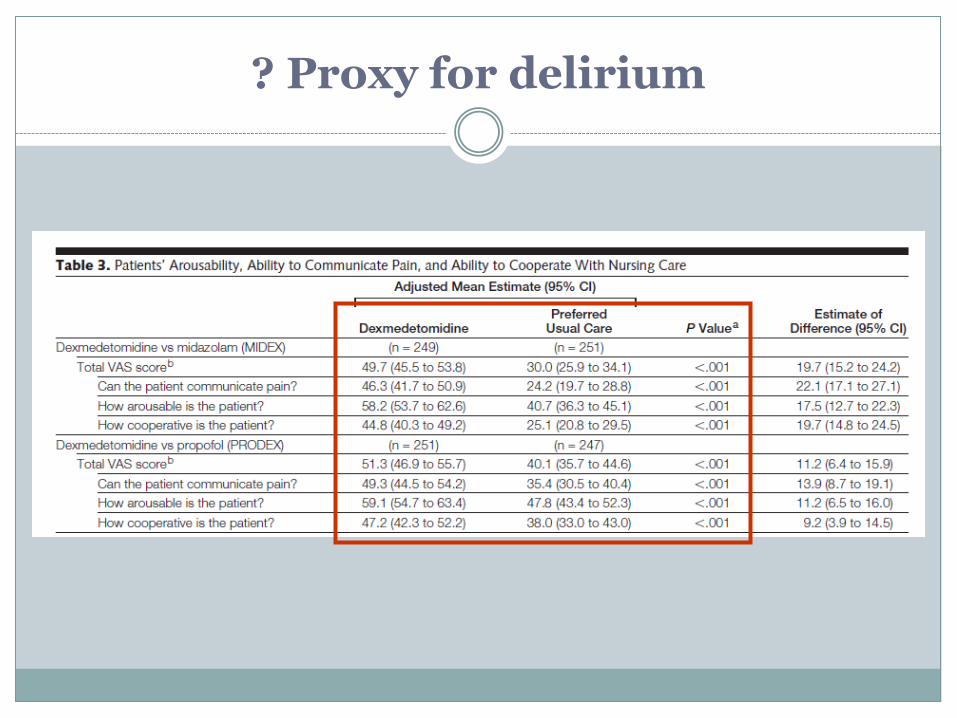
? Proxy for delirium

Question of doses…
MIDEX
0.2 μg/kg/hr dex = 2.1 mg/hr midaz (0.03 mg/kg)
My version
0.2 μg/kg/hr dex = 0.5 mg/hr midazolam

Goal RASS -3 to 0
Dexmed Midazolam Dexmed Propofol
RASS Score during study period
-0.9
(-1.9 to -0.1)
-1.5
(-2.5 to -0.5)
-1.0
(-1.9 to -0.2)
-1.7
(-2.5 to -0.7)
Sedation stop performed
89.7% 93.3% 89.0% 90.1%
Jakob et al JAMA 2012
Which patients get dexmedetomidine?

Medical/Surgical Patients – use over time
Wunsch et al Anesthesiology 2010
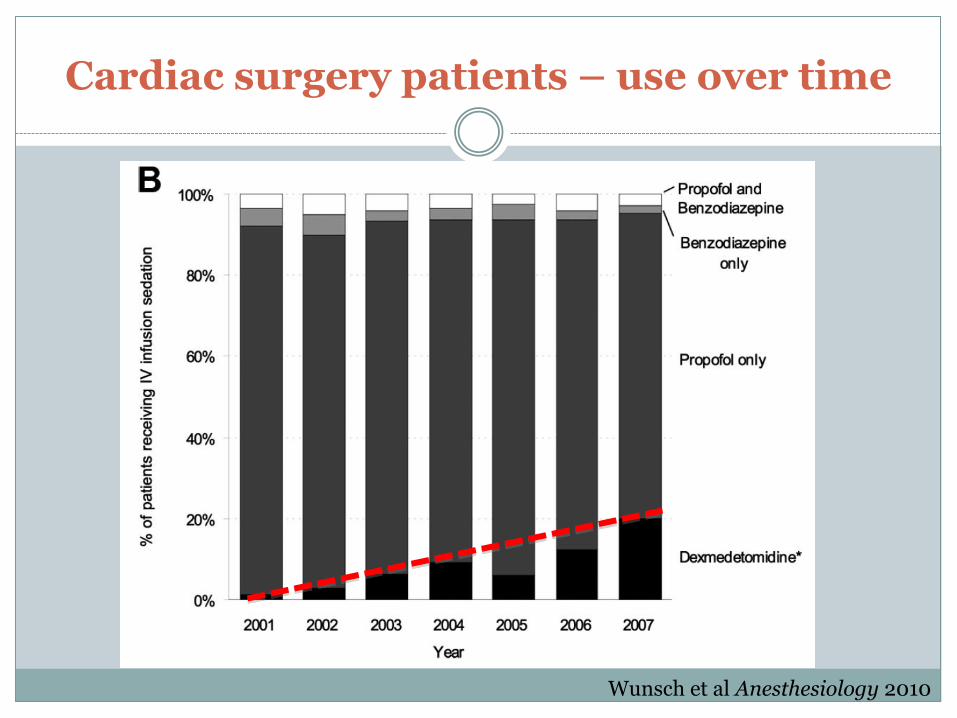
Cardiac surgery patients – use over time
Wunsch et al Anesthesiology 2010

Why cardiac surgery patients?
Prelim studies in cardiac surgery patients
Generally <24 hrs on ventilator
Low analgesia requirements (for surgical patients)
?More likely to be cared for by anesthesiologists

Our own experience

Patients who have received dexmedetomidine
Post cardiac surgery
Post general surgery
Transplants (heart, lung, liver, kidney)
ARDS
Septic shock
Etoh withdrawal
Pancreatitis
Etc…
We do not have IV clonidine
Potential problems
Barriers
Dosing error (mcg/kg/HR)
Staff anxiety regarding its sedative effects
‘Wrong’ patients
Bradycardia
Need for deeper sedation
Need for long period of sedation Rebound (a la clonidine) after many days
Planning to transfer a patient out of the ICU
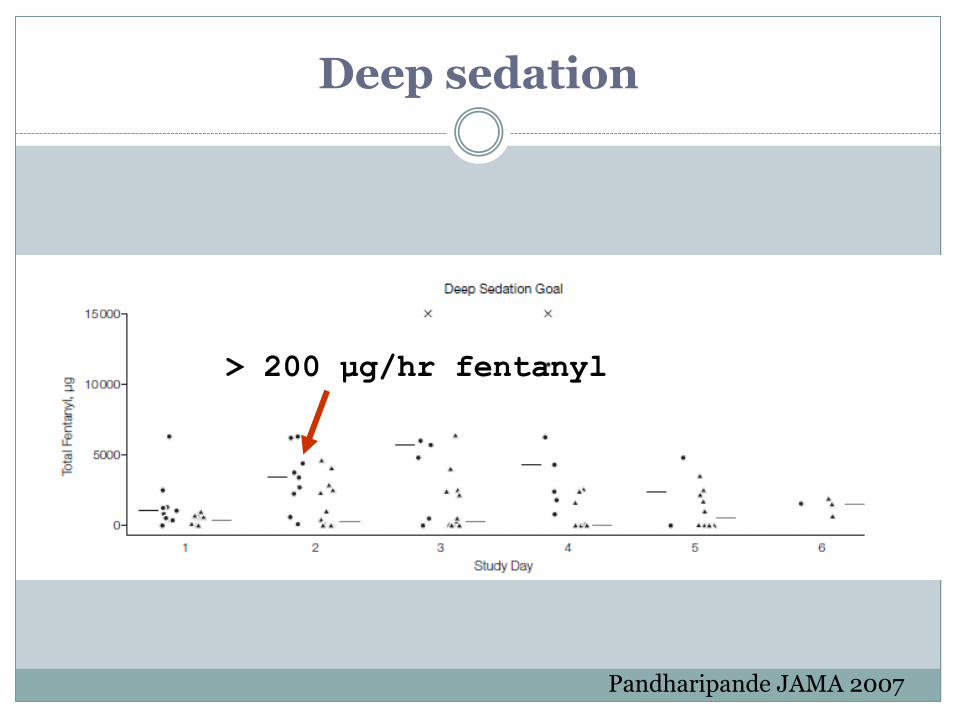
Deep sedation
> 200 μg/hr fentanyl
Pandharipande JAMA 2007
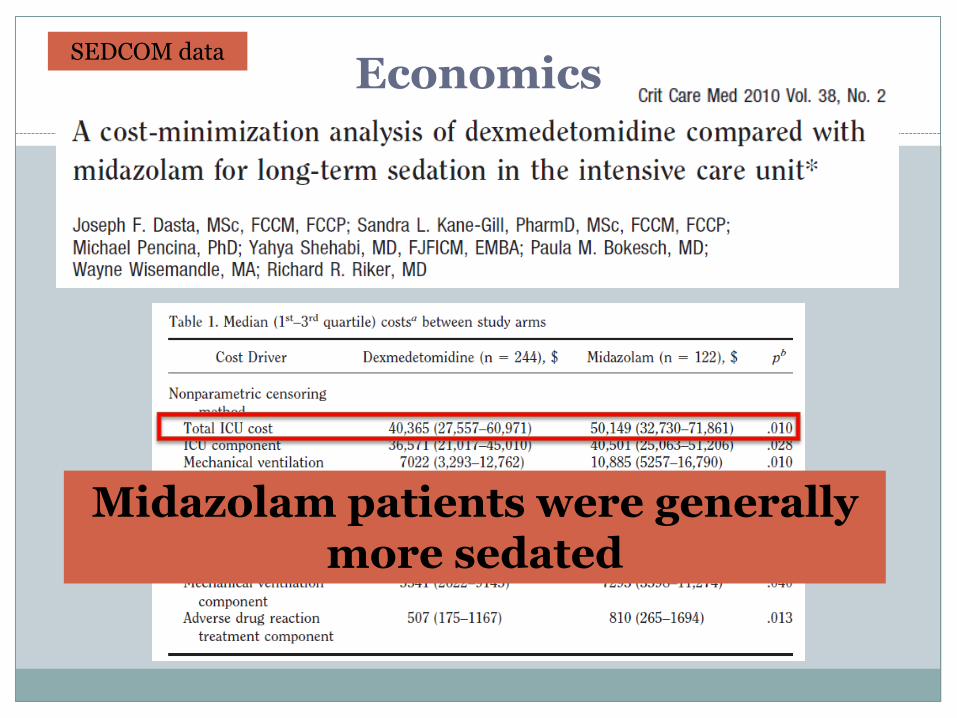
Economics
Midazolam patients were generally more sedated
SEDCOM data

Costs of drugs
$58.31 per 200-microgm vial, and the midazolam cost was $1.56 per 5-mg vial
0.7 mcg/kg/hr = 49 mcg/hr = 1,176 mcg/day
6 vials (at 200 mcgs) = $350.00
Dosing of 1.5 mcg/kg/hr = $700.00

Areas for potential use
That patient who is agitated and/or delirious every time you try to wake them up
Anxious patient not receiving mechanical ventilation
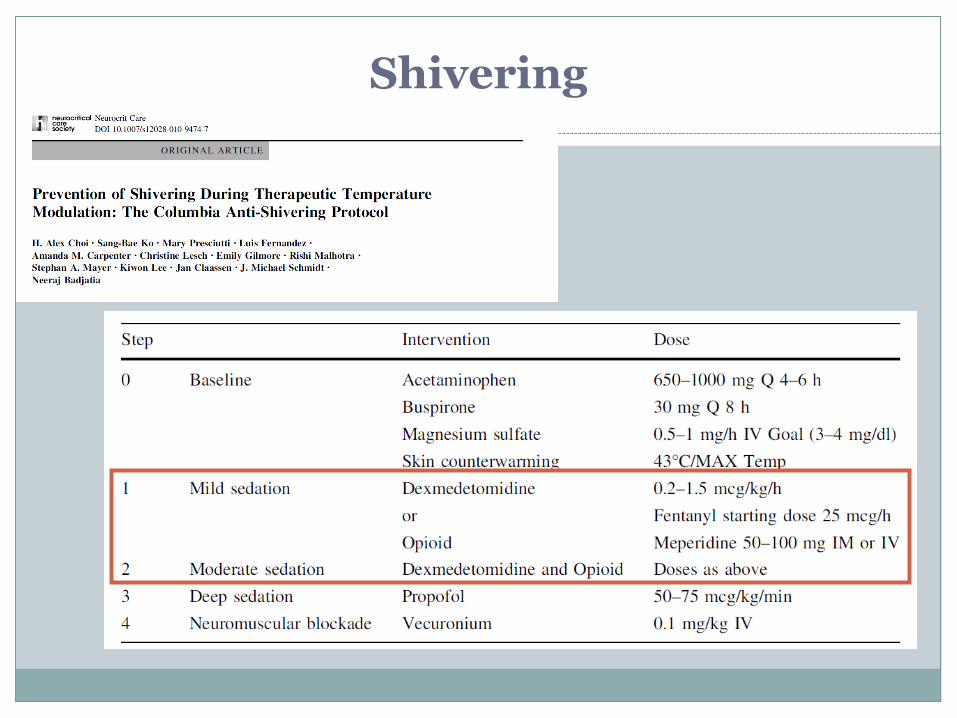
Neurological ICU: shivering
?Alcohol withdrawal
?Sleep deprived

So who are those ‘ideal’patients?
Example #1
Slightly hemodynamically unstable (but not so much that they can’t be awake)
Trying to wean
Emerging agitated from other sedation
Oversedated when given antipsychotics

Example #2
Elderly/fragile – (you know they are a setup for delirium)
Mild respiratory distress but not needing intubation Trying to tolerate BIPAP
Moderately anxious, starting to get sleep deprived
Shivering

Etoh withdrawal
• Adjunct to benzodiazepines• Case reports only

“In mechanically ventilated patients, nighttime infusions of dexmedetomidine preserved the day-night cycle of sleep but induced severely disturbed sleep
architecture without evidence of [slow wave sleep] or REM sleep”

Other options…
No sedation
Opiate-based sedation
Antipsychotic medications Haloperidol
Atypicals
Ketamine infusion
(Inhaled anesthetic)
(New formulation of etomidate)
Summary
Dexmedetomidine is another tool
Greatest benefits
Lack of respiratory depression
Hard(er) to over-sedate
May help with delirium
Downsides
Cost
Bradycardia
Lack of deep sedation