Embed Size (px)
Citation preview

Review
Targeting the mTOR/4E-BP Pathway in Endometrial Cancer
Sharmilee Bansal Korets1, Sarah Czok1, Stephanie V. Blank1,3, John P. Curtin1,3, and Robert J. Schneider2,3
AbstractEndometrial cancer is the most common gynecologic malignancy. Although it is highly treatable in the
early stages of disease, therapies for advanced and recurrent disease are rarely curative. A molecular and
genetic understanding of endometrial cancer involves the mTOR signaling pathway, an emerging target for
treatment of type I disease (the most common presentation). Endometrial cancers show a significant
reliance on themTORpathway for survival, and studies todatehave revealed a clinical advantage in targeting
this pathway. Lesswell developed in the study of endometrial cancer is an understanding ofmTOR signaling
to its major downstream effector, translational control. Given the poor rate of success for treatment of late-
stage endometrial cancer, increasing attention is being directed to the development of new therapeutic
approaches, including targeting the mTOR pathway. Here, we discuss the potential benefit of targeting
mTOR combined with existing chemotherapies by monitoring its impact on translational regulatory
pathways and key translation targets in endometrial cancer. We also highlight laboratory and clinical
research findings that will provide new avenues for future research and clinical development. Clin Cancer
Res; 17(24); 7518–28. �2011 AACR.
Introduction
Endometrial cancer is the most common gynecologicmalignancy and the fourth most common malignancy inAmerican women, with 43,470 new diagnoses and 7,950deaths for the year 2010 (1). Although themajority of endo-metrial cancers are diagnosed at an early stage of disease,conferring a favorable prognosis, women who are diag-nosed with advanced or recurrent disease have far worsesurvival rates and limited adjuvant treatment options. Inthe United States, �15% of endometrial cancers are diag-nosed at stage III or IV, with a 5-year survival rate of 20% to50% depending on grade and histologic subtype (2). Overthe past 30 years, little significant improvement has beenseen in the survival of patients with advanced disease (3).
Endometrial cancers are commonly classified into 2 his-tologic subtypes (4): endometrioid (type I) and nonendo-metrioid (type II). Each has distinct risk factors, clinicalbehaviors, and natural histories. Type I tumors are themostcommon (85%), primarily early stage at diagnosis in post-menopausal, obesewomenover the age of 50, and estrogen-dependent in a background of atypical hyperplasia. Type IIlesions (15%) are primarily comprised of serous and clear-cell histologies. Type II tumors are more aggressive and
associated with extrauterine spread, later-stage disease, andpoorer prognosis.
Type I and type II malignancies also have distinct molec-ular and genetic characteristics (5). Type I endometrialcancers exhibit a high frequency of microsatellite instabilityand loss-of-function mutations in the phosphatase andtensin homolog PTEN tumor-suppressor gene. Type II can-cers more frequently show p53 mutations.
Patients with advanced disease typically receive adjuvantchemotherapy [cisplatin–doxorubicin–paclitaxel (6)] withorwithout radiation after surgical staging. As a result of poortoxicity profiles, the molecular targets and signal transduc-tion pathways involved in endometrial cancer are nowunder investigation in multiple phase I and II trials (7).
Here, we focus on the role of mTOR inhibition in futuretreatment strategies and downstream effects on proteinsynthesis, with the goal of increasing new combinationtherapeutic approaches and the use of novel biomarkers toachieve better treatment response. Indirect (allosteric)mTOR inhibitors, known collectively as rapalogs, showactivity in the treatment of type I disease. Therefore, rapa-logs represent attractive investigational drugs for the man-agement of endometrial cancer due to their relationshipwith the PTEN signaling pathway, which is frequentlymutated in type I endometrial cancers. However, a newclass of catalyticmTOR inhibitors that act directly onmTORhave been introduced in phase I dose-escalation trials.These drugs more effectively inhibit mTOR in both of itssignaling complexes, mTORC1 and mTORC2. Taking intoaccount the emergence of direct mTOR inhibitors and thedeveloping knowledge about the effects of mTOR inhibi-tion on protein synthesis, we review the present under-standing of the role of the mTOR–translational control
Authors' Affiliations: Departments of 1Obstetrics and Gynecology and2Microbiology, and 3NYU Cancer Institute, New York University School ofMedicine, New York, New York
Corresponding Author: Robert Schneider, Department of Microbiology,NYU School of Medicine, 550 First Avenue, New York, NY 10016. Phone:212-263-6006; Fax: 212-263-8276; E-mail: [email protected]
doi: 10.1158/1078-0432.CCR-11-1664
�2011 American Association for Cancer Research.
ClinicalCancer
Research
Clin Cancer Res; 17(24) December 15, 20117518
on October 19, 2020. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 5, 2011; DOI: 10.1158/1078-0432.CCR-11-1664

pathway in the etiology, progression, and treatment ofendometrial cancer.
Major Molecular Alterations in Type IEndometrial Cancer: A Brief Overview
The genes that are commonly mutated in type I endo-metrial cancers are largely responsible for the regulationof signal transduction, which is involved in normal cellreplication and cell–cell adhesion. Thus, disruption ofthese pathways and functions leads to abnormalities incell proliferation and to the ability to invade or metasta-size. The most frequent alterations in type I endometrialcancers are summarized in Table 1. Because this area hasbeen extensively reviewed in the past (8, 9), we provideonly a summary of key features that also affect mTORand translational regulation in this disease.
PTENThe most common genetic mutation in type I endo-
metrial cancers (83%) occur in the phosphatase genePTEN, with loss or mutation (8, 9). PTEN is a tumor-suppressor gene, the loss of which plays a major role instimulating the phosphoinositide 3-kinase (PI3K)–AKT–mTOR pathway (10). PI3K–AKT–mTOR upregulationmodestly upregulates protein synthesis and more stronglyupregulates translation of survival, angiogenesis, and so-called oncogenic mRNAs (ref. 11; Fig. 1).
PTEN has lipid and protein phosphatase activity(10, 12, 13). The lipid phosphatase domain maintainscell-cycle arrest at the G1–S checkpoint, upregulatesAKT-dependent proapoptotic pathways, and downregu-lates Bcl-2–dependent antiapoptotic pathways (14).PTEN controls the levels of phosphorylated AKT byopposing PIK3CA activity. The protein phosphatasedomain inhibits focal adhesion formation, cell spread-ing, and migration (15). Increased mTOR activation andprotein synthesis are necessary to sustain these activities(11). Studies of PTEN knockout mice have helped elu-cidate its role in endometrial cancer. In one study (16),100% of the mice examined developed hyperplasticlesions in the endometrium and 20% developed endo-metrial carcinoma as a result of heterozygous mutationsin PTEN.
PIK3CAThe PIK3CA gene encodes the a catalytic subunit of
PI3K. This lipid kinase catalyzes production of PIP3, result-ing in the activation of multiple downstream targets, mostnotably AKT, leading to mTOR activation, and thus pro-moting cell proliferation and survival (17). As noted above,this pathway is upregulated in a majority of endometrialcancers. Thirty-six percent of patients with endometrialcancer have PIK3CA mutations, and 26% have concurrentPTEN and PIK3CA mutations (18). PIK3CA mutations arestrongly associated with endometrioid histology and ahigher stage, and show a trend toward increased incidenceof lymphovascular invasion (19).
KRASThe KRAS gene is a proto-oncogene encoding a small
inner plasma membrane GTPase that is involved in cellsignaling related to growth and differentiation. KRASmutations resulting in constitutive activity are present in10% to 30% of type I endometrial cancers and 16% ofhyperplastic lesions. Similar to the PTEN mutation, thefrequency of the KRAS mutation is increased in endo-metrial cancers that show genomic instability (8, 9, 20).Additionally, KRAS mutations stimulate downstreammTOR kinase activity, leading to increased selective trans-lation of mRNAs involved in tumor cell survival, angio-genesis, and proliferation (11).
Mutation of the LKB1 geneLKB1 (also known as STK11) is a serine–threonine
kinase that phosphorylates and activates AMPK-dependent
Table 1. Molecular alterations in type Iendometrial cancer
Molecular alteration Frequency Reference
PTEN 50–83% Hecht and Mutter (8)PIK3CA 36% Liu et al. (80)b-catenin 20–40% Bansal et al. (9)K-ras 10–30% Hecht and Mutter (8)Microsatellite instability 20% Basil et al. (81)LKB1 20% Lu et al. (25)E-cadherin 10–20% Bansal et al. (9)p53 10–20% Bansal et al. (9)
Translational Relevance
Endometrial cancer remains the most common gyne-cologic malignancy. Although it is highly curable bysurgery when diagnosed at an early stage and grade, theburden of advanced stage and recurrent disease is sub-stantial. Current combination therapies are highly toxicand of limited efficacy for the treatment of patients whorequire systemic therapy. Advances in the moleculargenotyping of endometrial cancers have led to an intensefocus on molecularly targeted agents that act on themTOR pathway, and this approach has shown some ofthe best responses in the treatment of advanced andrecurrent disease. In this short review, we explore therelationship between endometrial cancer and themTORpathway and its downstream regulation of protein syn-thesis. We suggest that there is a critical need to matchexperimental mTOR therapeutics with existing chemo-therapies by optimizing the impact on translationalregulatory pathways in the treatment of endometrialcancer.
mTOR and Translational Regulation in Endometrial Cancer
www.aacrjournals.org Clin Cancer Res; 17(24) December 15, 2011 7519
on October 19, 2020. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 5, 2011; DOI: 10.1158/1078-0432.CCR-11-1664

kinase [AMPK (21)]. AMPK senses ATP–AMP levels, there-by regulating cellular metabolism (22). mTOR is inhibitedby active AMPK through phosphorylation and activationof the tuberous-sclerosis complex-2 (TSC2) protein, anupstream inhibitor of mTORC1 (ref. 23; Fig. 1). Thus,
mutation of LKB1, similar to mutation of PTEN or KRAS,and elevated levels of insulin-like growth factor I (IGF-I)results in strong mTOR activation and upregulation ofprotein synthesis. Animal models of LKB1 deficiency showa high level of aggressive features in endometrial cancers,
© 2011 American Association for Cancer Researchsociation for Cancer Research
AMPK
4E-BP
mLST8
4E-BP
PDCD4
eIF4E
eIF4A
eIF4F
eIF4G
eIF4E eIF4A
eIF4B
S6K
S6K
S6
P P
P
P
P
MEK
Raf
IRS
1Ras
PTEN
GβLRictor
PRAS40
GDPGTP
RHEB RHEB
mTOR
mTORC2
Receptortyrosine kinases
Plasmamembrane
mTORC1inhibition
Cap-dependenttranslation off
Cap-dependenttranslation on
Hyper-P 4E-BPHypo-P 4E-BP
mTORC1
PDK1
Akt
TSC1
TSC2
PI3K
ERK
RSK
mTORRaptor
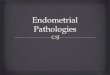
Figure 1. Signal transduction pathways for translational control. PI3K–AKT–mTORC1 and Ras–MAPK pathways, as well as their targets involved intranslation initiation, are shown. Mitogenic signals (growth factors, cytokines, and hormones) act on receptor tyrosine kinases to stimulate Ras andPI3K. The activation of PI3K stimulates AKT, which inhibits TSC1–TSC2 GAP activity, allowing Rheb-GTP–mediated stimulation of mTORC1. Inaddition, AKT negatively regulates PRAS40, an inhibitor of mTORC1. The activation of mTORC1 may also be mediated by inhibitory phosphorylationof TSC1/2 complex by extracellular signal-regulated kinase (ERK) and p90RSK. PTEN, a phosphatase, opposes activation of mTORC1 by PI3K.Under hypoxia and low-ATP conditions, the activation of AMP kinase leads to mTORC1 inhibition. mTORC1 activity is, therefore, stimulated bymitogenic and growth-promoting signals and suppressed by growth-inhibiting signals. Activated mTORC1 phosphorylates the 4E-BPs, resulting ineIF4E dissociation from 4E-BPs and eIF4E interaction with eIF4G. In addition, mTORC1 stimulates eIF4B-enhanced eIF4A helicase activity through theS6K-mediated phosphorylation of eIF4B and PDCD4, an inhibitor of eIF4A. All of these events promote the assembly of the cap-binding complex eIF4F(composed of eIF4E, eIF4G, and eIF4A), stimulating cap-dependent translation. In contrast, downregulation of mTORC1 leads to decreasedphosphorylation of 4E-BPs and eIF4E sequestration, and inactivation of eIF4A, eIF4B, and eEF2, which results in reduced cap-dependent mRNAtranslation. MAPK, MAP kinase; MEK, MAP–ERK kinase; 4E-BP, eIF4E binding/inhibiting protein.
Korets et al.
Clin Cancer Res; 17(24) December 15, 2011 Clinical Cancer Research7520
on October 19, 2020. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 5, 2011; DOI: 10.1158/1078-0432.CCR-11-1664

consistent with elevated mTOR activity (24). Studies ofhuman endometrial tumors have shown that �20% areLKB1-negative, and as many as 65% have a functionaldeficit in the protein (25).
Elevated IGF-I levelsEndometrial cancers are associated with elevated IGF-I
expression and activation of the IGF-I signal transductionpathway (26). Whereas estrogen increases IGFI gene tran-scription (26), PTEN downregulates IGF-I receptor levels(27), which are typically increased in endometrial cancers(28). The IGF-I pathway thus links loss of PTEN,increased AKT–mTOR activation (29), and estrogensignaling in endometrial cancer. Recently, a direct linkwas established for the regulation of IGF-I and insulin bythe PTEN–AKT–mTOR axis through mTOR target proteinGrb10, which when phosphorylated is a negative regula-tor of insulin signaling and IGF-I (30, 31).
The Role of Hormones in EndometrialCarcinogenesis
Hormones act on the endometrium to modify the genet-ically predetermined risk of cancer. Estrogen and proges-terone have divergent and often opposing effects on theendometrium (8). Estrogen can promote cell proliferationand inhibit apoptosis, whereas progesterone can inhibitproliferation and promote apoptosis and involution (32).Increased proliferative activity can increase the rate ofrandom mutation, possibly accounting for some of thepotential carcinogenic effects of estrogen on the endome-trium. Further, by promoting cell proliferation, estrogencreates a selective advantage for PTEN mutant clones thathave escaped the usual proapoptotic, antiproliferativecheckpoints (32). In addition to opposing endometrial cellproliferation, progesterone further counteracts the effect ofestrogen by downregulating expression of the estrogenreceptor itself. Progestins therefore reduce the proliferativeadvantage of PTEN mutant cells, leading these clones toinvolute (8).
ThemTOR/4E-BP Translational Control Pathway
Growth factor stimulation and hormone receptor acti-vation, as well as cellular responses to nutrient status,hypoxia, and other physiologic and metabolic altera-tions, ultimately signal to the protein kinase mTOR(Fig. 1; ref. 33). mTOR is a member of the PI3K–AKTfamily, which promotes cell proliferation, survival, andangiogenesis (34). mTOR is a serine–threonine kinasethat acts on factors in the protein synthesis machinery,integrating signals from a variety of growth factors andnutrients to regulate key metabolic and macromolecularprocesses, including mRNA translation, cell motility, andribosome biogenesis. mTOR forms 2 different proteincomplexes, mTORC1 and mTORC2, that mediate verydifferent functions, in part through mRNA translationalcontrol.
mTORC1 is a protein complex that contains mTOR,regulatory-associated protein of mTOR (Raptor), G-pro-tein b-subunit-like protein/LST8 [GbL (33)], and proline-rich AKT substrate 40 kDa (PRAS40). Raptor recruitssubstrates to mTORC1 for phosphorylation, includingthe eIF4E binding/inhibiting protein (4E-BP, inhibitedby mTORC1 phosphorylation) and ribosomal proteinS6 kinases-1,2 (S6K-1,2). S6K-1,2 phosphorylates ribo-somal protein S6, initiation factor eIF4B (stimulating itsRNA binding activity and translation), tumor suppressorprotein PDCD4 (increasing initiation factor eIF4A acti-vity), and translation elongation factor eEF2 kinase,thereby inactivating the kinase, and in turn promotingeEF2 activity and elongation (Fig. 1).
The second mTOR complex, mTORC2, contains GbL,the protein rapamycin-insensitive companion of mTOR(Rictor), and mammalian stress-activated protein kinase(SAPK)–interacting protein [mSIN1 (35)]. Activation ofmTORC2 regulates cytoskeleton organization in responseto growth factors and leads to increased phosphorylation(activation) of AKT, which in turn is an upstream activatorof mTORC1 and protein synthesis (36). mTORC2 is gen-erally insensitive to inhibition by allosteric mTOR rapaloginhibitors such as sirolimus, but not to small-moleculecatalytic mTOR inhibitors. Of importance, rapalog treat-ment can actually stimulate AKT–mTOR through mTORC2activation (37–40), which has fueled interest in the clinicaldevelopment of small-molecule, catalytic-site mTORC1/2inhibitors.
Rapalog inhibition of mTORAmplification of PI3K–AKT, increased transcription, or
loss of regulatory control by mutation or deletion of regu-lators such as PTEN can result in mTOR activation. Loss ofPTEN is the primary means for maintenance of increasedmTOR activity in endometrial cancer (41), as supported byanimal studies (42). Analyses of human type I and type IIendometrial cancers have shown a compelling associationamong PTEN loss, increased mTOR activity, hyperpho-sphorylation (inactivation) of the translation inhibitor4E-BP1, increased cancer progression, and reduced survivalin type I disease (43). That said, overexpression of mTORitself in endometrial cancer as a means for increased mTORactivity is actually quite rare (�7% incidence) and may notcorrelate with disease progression, survival, or even sensi-tivity to mTOR inhibition (44). In principle, however, theoveractive PI3K–AKT–mTOR pathway in endometrial can-cer should provide an excellent target for treatment due toan increased requirement for mTOR activity and increasedsensitivity when inhibited.
Rapamycin was initially used as an antifungal agent andsubsequently was applied as an immunosuppressant fortissue transplant patients. First-generationmTOR inhibitors(also known as rapalogs) include sirolimus (rapamycin),temsirolimus, everolimus, and ridaforolimus. All of theseinhibitors are sirolimus analogues that were developed fororal or i.v. administration by derivatization of the C40hydroxyl group. They inhibit mTORC1 by acting on FK506
mTOR and Translational Regulation in Endometrial Cancer
www.aacrjournals.org Clin Cancer Res; 17(24) December 15, 2011 7521
on October 19, 2020. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 5, 2011; DOI: 10.1158/1078-0432.CCR-11-1664

binding protein 12 (FKBP12), an intracellular receptor thatactivates mTORC1 through a mechanism that remainspoorly understood (35). Rapalogs insufficiently inhibitmTOR, with loss of S6K-negative regulation ofIRS-1, poor activation of the 4E-BPs, and little inhibitionof protein synthesis. Rapalogs used as single-agent inhibi-tors have also been linked to increased AKT activity dueto positive feedback regulation of AKT by mTORC2(37, 39, 40).
mTOR-mediated translational control and itsimplications in endometrial cancer
The initiation of mRNA translation is generally the rate-limiting step of protein synthesis. A number of featurescontribute to widely different rates of initiation on differentmRNAs, creating a scenario of scalable and remarkablyselective translation of different mRNAs in response tophysiologic signals (11). Cellular mRNAs contain a 50
inverted 7-methylguanosine cap that serves as the recogni-tion site for the translation initiation machinery. The cap isrecognized by initiation factor eIF4E, which in turn recruitsthe scaffolding protein eIF4G and the ATP-dependent RNAhelicase, eIF4A, that collectively comprise the factor eIF4F(45). eIF4F interacts with the multisubunit factor eIF3,which in turn recruits the 40S small ribosome subunit andthe complex containing the initiating methionyl-tRNA,eIF2, and GTP (Fig. 1).
mTOR plays a pivotal role in regulating translationinitiation through control of eIF4F. The majority ofmRNAs require cap recognition by eIF4E and assemblyof the cap-initiation complex to recruit ribosomes andinitiate translation. mTOR phosphorylation of the 4E-BPs(4E-BP1 is the major epithelial cell form) promotescap-dependent mRNA translation by inactivating theireIF4E-sequestering activity (46). mTOR also phosphory-lates the major form of eIF4G (eIF4GI). The function ofeIF4G phosphorylation is unclear, but it may stimulate astructural alteration that promotes greater translationof a subset of mRNAs (47). mTOR phosphorylationactivates S6K-1 and S6K-2, which promotes cancer pro-gression (11). In particular, S6K1 phosphorylation ofeIF4B stimulates eIF4A activity and translation (48).Although increased mTOR activity (34) and levels ofprotein synthesis are a hallmark of many human cancers,as are increased levels of eIF4E, eIF4GI, and several othertranslation factors (11), the selectively increased transla-tion of a specific group of mRNAs that encode proteinsinvolved in angiogenesis, survival, and oncogenic func-tions is thought to provide the rationale for targeting theincreased mTOR activity found in endometrial and othercancers.
Increased mTOR activation favors selective mRNAtranslation
Studies have shown that increasedmTOR activity and theincreased expression of eIF4E and eIF4GI primarily favorstrong, selectively increased translation of a subset ofmRNAs with extensively structured 50 untranslated regions
(50UTR) and/or low abundance or multiple upstream openreading frames (49, 50). In general,whenmRNAswith thesecharacteristics are increased in translation, they become keyplayers in cancer development, angiogenesis, survival, hyp-oxia responses, and disease progression (11). Examplesinclude mRNAs that encode proteins for survival (MCl1,survivin, XIAP, and Bcl2), cell-cycle progression (c-myc,ODC1, and cyclin D1), angiogenesis (VEGF-A and FGF2),and response to hypoxia (HIF1a), among others (11).Increased expression of eIF4E/eIF4GI and/or increasedavailability of eIF4E or eIF4A (through reduced antagonisticPDCD4 levels) are thought to promote greater unwindingby eIF4A of 50UTR structures and, therefore, to dispropor-tionately promote greater translation of these mRNAs. Thisin turn is associated with increased malignancy anddecreased survival in a variety of human cancers, includingendometrioid endometrial cancers (43). Increased expres-sion of eIF4E and/or eIF4GI or hyperphosphorylation of4E-BP1 by activated mTOR is similarly associated withhigher tumor grade and stage, cancer progression, andreduced survival in a number of human cancers (43). Ina recent study, elevated expression of eIF4E was observedin more than half of the type I endometrial cancers exam-ined,with the greatest expression found at stages III/IV (51),suggesting that these tumors have a greater sensitivitytomTOR inhibition. The underlyingmechanism is thoughtto be strongly increased translation of select mRNAs. Inthis regard, understanding the dependence of selectivelyincreased mRNA translation on increased mTOR/eIF4Eactivity in endometrial cancer provides a new paradigmfor the design of therapeutic clinical trials. As describedbelow, single-agent and MTD strategies for mTOR inhibi-tors fail to take advantage of a low-toxicity therapeuticwindow in which we might be able to achieve selectivetranslation inhibition of oncogenic mRNAs while largelysparing overall protein synthesis.
Preclinical studies of mTOR inhibition in endometrialcancers
Rapalog studies in endometrial cancer have focusedprimarily on expression of mTOR pathway proteins(44, 52–58) and cellular responses to mTOR inhibitors(25, 52, 59–62). Several groups have also investigated therole of small-molecule mTOR kinase inhibitors in endo-metrial cancer cell lines (59, 63) and the effects of mTORinhibitors on mouse models of endometrial cancer(3, 64–66).
In multiple studies, investigators have tested the correla-tion between themTOR pathway and the control of proteinsynthesis and the clinical behavior of endometrioid tumors.Activation of mTOR and phosphorylation of 4E-BP1 occurmore frequently in advanced-stage and high-grade endo-metrial tumors, respectively (52), associated with cancerprogression and reduced survival (43). Similarly, a trendtoward increased activation of the AKT–mTORpathwaywasfound in patients with progesterone-refractory endometrialhyperplasia (55). Increased signaling in breast cancersthrough hormone receptors has been linked to increased
Korets et al.
Clin Cancer Res; 17(24) December 15, 2011 Clinical Cancer Research7522
on October 19, 2020. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 5, 2011; DOI: 10.1158/1078-0432.CCR-11-1664

activation of mTOR and, by extension, protein synthesis(67). Surprisingly, however, 2 studies in endometrial cancerrevealed no statistically significant correlation betweenexpression or activity of the AKT–mTOR pathway andsurvival or clinical-pathologic characteristics, includingstage, grade, and lymph node involvement (44, 56).In tissue-cell culture studies, researchers have further
investigated the impact of mTOR inhibition by rapalogtreatment on biologic activities and tumor developmentusing endometrial cancer cell lines. Overall, the resultsindicate that rapalogs are more effective as cytostatic agentsthan as cytotoxic ones and that they have the ability topotentiate the effects of other cytotoxic chemotherapeuticdrugs, including cisplatin and paclitaxel (58–60). In addi-tion, cell culture studies have shown dose-dependentantiproliferative properties of rapalogs as single agents(52, 58, 59, 61, 62).Mirroring human studies, tissue culturestudies have shown contradictory results with regard tothe impact of PTEN status on rapamycin sensitivity(32, 40, 41, 43). Investigators have also examined rapalogtreatment in mouse models of endometrial hyperplasia,and they found that treatment with rapalogs reduced tumorburden, slowed progression of disease, and decreased theincidence of hyperplastic lesions in mice predisposed tohyperplasia (3, 64–66).
Current clinical trials of mTOR inhibitors inendometrial cancerIn a number of completed and ongoing phase I and II
trials, researchers have investigated the role of oral andparenteral rapalogmTOR inhibitors in advanced and recur-rent endometrial cancers (7, 68). All rapalogs, whetheradministered by oral or i.v. routes, provide similar lowbiologic exposure and have been shown to inhibit thephosphorylation of 4E-BP1 or S6K1 as surrogate markersof activity in tumor specimens or circulating peripheralbloodmononuclear cells (69). Plasma concentrations showa prolonged half-life for sirolimus (�50 hours) comparedwith temsirolimus (�15 hours), which is converted tosirolimus (70). Using preclinical studies and demonstratedactivity in other malignancies as a reference, investigatorsare developing new regimens with the goal of achievingmore tolerable, efficacious treatments for advanced orrecurrent endometrial cancer.Studies have shown a variable response to mTOR
inhibition in the treatment of advanced and recurrentendometrial cancer. Treatment-na€�ve endometrial cancersshowed some of the highest objective response rates tosingle-agent mTOR inhibitors, second only to lympho-mas (71). Response rates in previously treated endome-trial cancers were also encouraging (72). Most of thesestudies, however, included varied patient populationswith endometrial cancers of different histologies anddiverse numbers of prior cytotoxic or hormonal treatmentregimens. Collectively, these studies showed responserates from 7% to 25%, with up to 57% of patientsachieving stable disease, i.e., potential clinical benefit(71, 73). One study with a 20-week follow-up, limited
to patients with endometrioid histology, showed a 21%stable disease rate at 20 weeks (74). A recent single-agentphase II study of temsirolimus showed a strong response(>80% stable disease) with long duration in chemother-apy-na€�ve women with recurrent or metastatic endome-trial cancer, compared with 50% in women with priorchemotherapy treatment (75). There was no correlationwith PTEN status. These data suggest that we have a realopportunity to inhibit mTOR as a first-line treatmentfor endometrial cancer by using judicious combinationsthat capitalize on biologic synergies other than PTENstatus and by exploiting combinations with other che-motherapeutics to maximize tumor cell killing andantiangiogenesis.
A significant untapped opportunity exists in the devel-opment of activity markers in the mTOR translationalcontrol pathway (76), focusing on highly mTOR-depen-dent oncogenic and survival mRNAs as biologic surrogatemarkers for treatment sensitivity and response. Clinicaltrials have produced conflicting results regarding whethermTOR or S6K phosphorylation (activity) correlates withtreatment response, mirroring preclinical studies (71, 74).Clearly, there is a need to develop better biomarkers ofmTOR sensitivity and endometrial cancer response, as wellas treatment strategies that build on the molecular bio-logic understanding of selective translation inhibitionby mTOR interference. Investigators need to reexaminethe important issue of rapalog toxicity as currently con-figured in clinical use. It is unknown whether present levelsof treatment efficacywill bemaintained at lower dose levels.The fact that biologic exposure (i.e., plasma concentrationover time) does not proportionally increase with dosemay indicate that higher or more frequent dosing near theMTD merely increases toxicity, with little if any gain inantitumor activity and survival. A more fruitful approachmight be to focus on achieving better synergy based onbiologic activities with conventional chemotherapeutics,rather than on the MTD. In this regard, temsirolimus andeverolimus are used at slightly lower levels than the MTD,whereas sirolimus is used at the MTD. Toxicities in clinicaltrials have included dyslipidemia, mucositis, myelo-suppression, fatigue, infections, and pneumonitis. In aphase I trial of temsirolimus in combination with topo-tecan for advanced or recurrent gynecologic malignancies,the dose-limiting toxicity was myelosuppression, and theregimen was intolerable in women who had previouslyreceived radiation (77). Researchers have now completedor are conducting more than 10 early-phase clinical trialsof rapalogs in patients with endometrial cancer to furtherinvestigate response, active combinations, and toxicities.The outcomes and biomarkers of these trials are beingevaluated, and available results are summarized in Table 2.Overall, it is likely that intermittent rather than daily dosingwill provide lower toxicity while preserving antitumoractivity (34). These trials give investigators the ability toevaluate both retrospectively and prospectively treatmentresponse with potential biomarkers based on translationalcontrol and translation targets of mTOR activity.
mTOR and Translational Regulation in Endometrial Cancer
www.aacrjournals.org Clin Cancer Res; 17(24) December 15, 2011 7523
on October 19, 2020. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 5, 2011; DOI: 10.1158/1078-0432.CCR-11-1664

Table 2. Completed and ongoing phase I and II studies of mTOR inhibitors in endometrial cancer
Study name Summary Status Findings Reference
Carboplatin–paclitaxel–ridaforolimus in endometrial,ovarian, and solids
Phase: IB Approved,not yetactive
N/A N/AAssessment: MTD of ridaforolimus
(rapalog) in combination withcarboplatin–paclitaxel
Population: metastatic/recurrentendometrial cancer, up to 1 priorchemotherapy regimen
BEZ235 trial in patientswith advanced endometrialcarcinoma
Phase: II Approved,not yetactive
N/A N/A
Assessment: safety and activityof BEZ235 (dual P13K–mTORinhibitor)
Population: recurrent or progressiveendometrial carcinoma after first-line treatment
Study of the combination oftemsirolimus and pegylatedliposomal doxorubicin inadvanced or recurrent breast,endometrial, and ovarian cancer
Phase: I Active N/A N/AAssessment: combination of
temsirolimus (rapalog) and PLDPopulation: advanced/recurrent
breast, endometrial and ovariancancer
Phase II study of Akt inhibitorMK2206 in patients with PIK3CAmutation recurrent or advancedendometrial carcinoma
Phase: II Active N/A N/AAssessment: activity of MK2206
(Akt inhibitor)Population: recurrent/persistent
endometrial cancerBiomarkers: PIK3CA mutation
Study of weekly oral RAD001in combination with oraltopotecan in patients withadvanced or recurrentendometrial cancer
Phase: I Active N/A N/AAssessment: activity of topotecan
and RAD001 (rapalog)Population: advanced/recurrent
endometrial cancerBKM120 as second-line therapyfor advanced endometrial cancer
Phase: I Active N/A N/AAssessment: activity of BKM120
(PI3K inhibitor)Population: recurrent endometrial
cancer,Biomarkers: PI3K activation status
Safety study of XL147 incombination with paclitaxel andcarboplatin in adults with solidtumors
Phase: I Active N/A N/AAssessment: safety and tolerability
of XL147 (PI3K inhibitor)Population: solid tumors, including
advanced/recurrent endometrialcancer
Letrozole and RAD001 in advancedor recurrent endometrial cancer
Phase: II Active N/A N/AAssessment: activity and safety
of RAD001 and Femara (letrozole)Population: recurrent/progressive
endometrial cancer.
(Continued on the following page)
Korets et al.
Clin Cancer Res; 17(24) December 15, 2011 Clinical Cancer Research7524
on October 19, 2020. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 5, 2011; DOI: 10.1158/1078-0432.CCR-11-1664

Table 2.Completed and ongoing phase I and II studies of mTOR inhibitors in endometrial cancer (Cont'd )
Study name Summary Status Findings Reference
Phase II study of temsirolimusand bevacizumab in patients withlocally advanced, recurrent,metastatic, or progressiveendometrial, ovarian epithelial,hepatocellular, islet cell, orcarcinoid cancers
Phase: IIAssessment: tolerability and activity
of temsirolimus and bevacizumab(anti-VEGF antibody)Population: multiple solid tumors
Active N/A N/A
Molecular correlates associatedwith a phase II study oftemsirolimus (CCI-779) in patientswith metastatic or recurrentendometrial cancer (NCIC IND160)
Phase: IIAssessment: activity of temsirolimus
Population: chemotherapy-naïve,recurrent/metastatic endometrialcancer
In progress 26% partial response,63%stable disease;responsesirrespective ofPTEN status
Oza et al. (71)
Biomarkers: PTEN statusPhase II trial of the mTORinhibitor AP23573 as a singleagent in advanced endometrialcancer (NCIC IND 148)
Phase: IIAssessment: response to
AP23573 (ridaforolimus)Population: progressiveendometrial cancer, up to 2 priorchemotherapy regimens
In progress 33% stable disease,partial or completeresponse; 52%discontinuedtreatment before4 cycles due toprogression
Columboet al. (73)
Phase II study of the oralmammaliantarget of rapamycin inhibitor,everolimus, in patients withrecurrent endometrial cancer
Phase: IIAssessment: response and toxicities
of everolimusPopulation: pretreated, recurrent,endometrioid endometrial cancer
Completed No partial or completeresponses; 21%stable disease at 20weeks;49%requireddose reduction tohalfstartingdosedueto toxicity
Slomovitzet al. (74)
Phase I studyofweekly temsirolimusand topotecan in the treatment ofadvanced and/or recurrentgynecologic malignancies
Phase: IAssessment: tolerability of weekly
topotecanwithweekly temsirolimusPopulation: recurrent gynecologicmalignancies not responsive tostandard therapy
Completed DLT for thecombination wasmyelosuppression;patients with historyof pelvic RT couldnot receive fulldoses of each agentin combination;82% had stabledisease at firstevaluation
Temkin et al.(77)
Phase II study of temsirolimus inwomen with recurrent ormetastatic endometrial cancer; atrial of the NCIC group
Phase: IIAssessment: response and toxicityof single-agent temsirolimusPopulation: chemotherapy-naïve orpreviously treated recurrent ormetastatic endometrial cancerBiomarkers: PTEN status
Completed Naïve patients: 14%partial response,69% stable diseaseat 5 months and 9months,respectively.Previously treatedpatients: 4% partialresponse, 48%stable disease at�4months. Nocorrelation withPTEN status.
Oza et al. (75)
Abbreviations: DLT, dose-limiting toxicity; N/A, not applicable; NCIC, National Cancer Institute of Canada; PLD, phospholipase D; RT,radiotherapy.
mTOR and Translational Regulation in Endometrial Cancer
www.aacrjournals.org Clin Cancer Res; 17(24) December 15, 2011 7525
on October 19, 2020. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 5, 2011; DOI: 10.1158/1078-0432.CCR-11-1664

Future Directions: The Difficulty of TargetingmTOR and Translational Control
A significant problem in targeting mTOR withrapalogs is that these agents show partial inhibitoryactivity. They only moderately block mTORC1 andhave little (if any) effect on mTORC2, thereby increas-ing AKT activity (37, 39, 40). It is unlikely that wecan overcome this obstacle therapeutically by conti-nuous rapalog exposure, which is reported to inhibitmTORC2 (78), because such an approach would re-quire a dose that is not clinically sustainable. This issuemay be obviated by the development of mTORC1/2active-site catalytic kinase inhibitors that more stronglyblock S6K and 4E-BP phosphorylation and mTORC2activity and consequent upregulation of AKT activity,and thus would likely provide greater therapeutic ben-efit. Preclinical studies in a murine B-cell lymphomamodel suggest a particular synergy for tumor cell kill-ing with mTORC1/2 inhibition in the setting of hyper-activated eIF4E (79). This may be particularly relevantfor the majority of endometrial cancers in which eIF4Eis overexpressed. On the other hand, preclinical and
clinical trials to date have only begun to capitalize onthe ability to synergize additional chemotherapies withpartial mTORC1 inhibition, such as addition of ERKinhibitors. Further study of the rapalogs in combina-tion with traditional cytotoxic agents, as well as themore-specific small-molecule mTOR kinase inhibitors,is therefore warranted.
Disclosure of Potential Conflicts of Interest
R.J. Schneider is a consultant to PTC Therapeutics, Inc., CelgeneCorporation, and Eli Lilly/ImClone companies. S.V. Blank, J.P.Curin, S.B. Korets, and S. Czok disclosed no potential conflicts ofinterest.
Grant Support
Department of Defense Breast Cancer Research Program, Breast CancerResearch Foundation, and Avon Breast Cancer Foundation (R.J. Schneider);Ortho Biotech Gynecologic Oncology Fellowship Program Grant (S.V.Blank, J.P. Curin, and S. Czok).
Received June 28, 2011; revised October 4, 2011; accepted October 10,2011; published OnlineFirst December 5, 2011.
References1. American Cancer Society [homepage on the Internet]. Cancer Facts
and Figures 2010. Available from: http://www.cancer.org/Research/CancerFactsFigures/CancerFactsFigures/cancer-facts-and-figures-2010.
2. Sorosky JI. Endometrial cancer. Obstet Gynecol 2008;111:436–47.3. ContrerasCM,AkbayEA,GallardoTD,Haynie JM,SharmaS, TagaoO,
et al. Lkb1 inactivation is sufficient to drive endometrial cancers thatare aggressive yet highly responsive to mTOR inhibitor monotherapy.Dis Model Mech 2010;3:181–93.
4. Bokhman JV. Two pathogenetic types of endometrial carcinoma.Gynecol Oncol 1983;15:10–7.
5. Gadducci A, Tana R, Cosio S, Fanucchi A, Genazzani AR. Moleculartarget therapies in endometrial cancer: from the basic research to theclinic. Gynecol Endocrinol 2008;24:239–49.
6. Fleming GF, Brunetto VL, Cella D, Look KY, Reid GC, Munkarah AR,et al. Phase III trial of doxorubicin plus cisplatin with or withoutpaclitaxel plus filgrastim in advanced endometrial carcinoma:a Gynecologic Oncology Group Study. J Clin Oncol 2004;22:2159–66.
7. Barrena Medel NI, Bansal S, Miller DS, Wright JD, Herzog TJ. Phar-macotherapy of endometrial cancer. Expert Opin Pharmacother2009;10:1939–51.
8. Hecht JL,Mutter GL.Molecular and pathologic aspects of endometrialcarcinogenesis. J Clin Oncol 2006;24:4783–91.
9. Bansal N, Yendluri V, Wenham RM. The molecular biology of endo-metrial cancers and the implications for pathogenesis, classification,and targeted therapies. Cancer Contr 2009;16:8–13.
10. HollanderMC,BlumenthalGM,DennisPA.PTEN loss in thecontinuumof common cancers, rare syndromes and mouse models. Nat RevCancer 2011;11:289–301.
11. Silvera D, Formenti SC, Schneider RJ. Translational control in cancer.Nat Rev Cancer 2010;10:254–66.
12. Stambolic V, Suzuki A, de laPompaJL,BrothersGM,MirtsosC,SasakiT, et al. Negative regulation of PKB/Akt-dependent cell survival by thetumor suppressor PTEN. Cell 1998;95:29–39.
13. Maehama T, Dixon JE. PTEN: a tumour suppressor that functions as aphospholipid phosphatase. Trends Cell Biol 1999;9:125–8.
14. Zhu X, Kwon CH, Schlosshauer PW, Ellenson LH, Baker SJ. PTENinduces G(1) cell cycle arrest and decreases cyclin D3 levels inendometrial carcinoma cells. Cancer Res 2001;61:4569–75.
15. Raftopoulou M, Etienne-Manneville S, Self A, Nicholls S, Hall A.Regulation of cell migration by the C2 domain of the tumor suppressorPTEN. Science 2004;303:1179–81.
16. Stambolic V, Tsao MS, Macpherson D, Suzuki A, Chapman WB, MakTW. High incidence of breast and endometrial neoplasia resemblinghuman Cowden syndrome in ptenþ/� mice. Cancer Res 2000;60:3605–11.
17. CullyM, YouH, Levine AJ,Mak TW.Beyond PTENmutations: the PI3Kpathway as an integrator of multiple inputs during tumorigenesis. NatRev Cancer 2006;6:184–92.
18. Oda K, Stokoe D, Taketani Y, McCormick F. High frequency ofcoexistent mutations of PIK3CA and PTEN genes in endometrialcarcinoma. Cancer Res 2005;65:10669–73.
19. Catasus L,GallardoA, CuatrecasasM, Prat J. PIK3CAmutations in thekinase domain (exon 20) of uterine endometrial adenocarcinomas areassociated with adverse prognostic parameters. Mod Pathol 2008;21:131–9.
20. Liu FS. Molecular carcinogenesis of endometrial cancer. Taiwan JObstet Gynecol 2007;46:26–32.
21. Woods A, Johnstone SR, Dickerson K, Leiper FC, Fryer LG, NeumannD, et al. LKB1 is the upstream kinase in the AMP-activated proteinkinase cascade. Curr Biol 2003;13:2004–8.
22. Kahn BB, Alquier T, Carling D, Hardie DG. AMP-activated proteinkinase: ancient energy gauge provides clues tomodern understandingof metabolism. Cell Metab 2005;1:15–25.
23. Inoki K, Zhu T, Guan KL. TSC2 mediates cellular energy response tocontrol cell growth and survival. Cell 2003;115:577–90.
24. Contreras CM,Gurumurthy S, Haynie JM, Shirley LJ, Akbay EA,WingoSN, et al. Loss of Lkb1 provokes highly invasive endometrial adeno-carcinomas. Cancer Res 2008;68:759–66.
25. Lu KH, Wu W, Dave B, Slomovitz BM, Burke TW, Munsell MF, et al.Loss of tuberous sclerosis complex-2 function and activation ofmammalian target of rapamycin signaling in endometrial carcinoma.Clin Cancer Res 2008;14:2543–50.
Korets et al.
Clin Cancer Res; 17(24) December 15, 2011 Clinical Cancer Research7526
on October 19, 2020. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 5, 2011; DOI: 10.1158/1078-0432.CCR-11-1664

26. Rutanen EM. Insulin-like growth factors in endometrial function. Gyne-col Endocrinol 1998;12:399–406.
27. Tanno S, Tanno S, Mitsuuchi Y, Altomare DA, Xiao GH, Testa JR. AKTactivation up-regulates insulin-like growth factor I receptor expressionand promotes invasiveness of human pancreatic cancer cells. CancerRes 2001;61:589–93.
28. McCampbell AS, Broaddus RR, Loose DS, Davies PJ. Overexpressionof the insulin-like growth factor I receptor and activation of theAKT pathway in hyperplastic endometrium. Clin Cancer Res 2006;12:6373–8.
29. Brader S, EcclesSA. Phosphoinositide 3-kinase signalling pathways intumor progression, invasion and angiogenesis. Tumori 2004;90:2–8.
30. Hsu PP, Kang SA, Rameseder J, Zhang Y, Ottina KA, Lim D, et al. ThemTOR-regulated phosphoproteome reveals a mechanism ofmTORC1-mediated inhibition of growth factor signaling. Science2011;332:1317–22.
31. Yu Y, Yoon SO, Poulogiannis G, Yang Q, Ma XM, Vill�en J, et al.Phosphoproteomic analysis identifiesGrb10 as anmTORC1substratethat negatively regulates insulin signaling. Science 2011;332:1322–6.
32. Zheng W, Baker HE, Mutter GL. Involution of PTEN-null endometrialglands with progestin therapy. Gynecol Oncol 2004;92:1008–13.
33. Guertin DA, Sabatini DM. Defining the role of mTOR in cancer. CancerCell 2007;12:9–22.
34. Dancey J. mTOR signaling and drug development in cancer. Nat RevClin Oncol 2010;7:209–19.
35. Sabatini DM. mTOR and cancer: insights into a complex relationship.Nat Rev Cancer 2006;6:729–34.
36. Cybulski N, Hall MN. TOR complex 2: a signaling pathway of its own.Trends Biochem Sci 2009;34:620–7.
37. Sarbassov DD, Guertin DA, Ali SM, Sabatini DM. Phosphorylation andregulation of Akt/PKB by the rictor-mTOR complex. Science2005;307:1098–101.
38. She QB, Halilovic E, Ye Q, ZhenW, Shirasawa S, Sasazuki T, et al. 4E-BP1 is a key effector of the oncogenic activation of the AKT and ERKsignaling pathways that integrates their function in tumors.Cancer Cell2010;18:39–51.
39. O'Reilly KE, Rojo F, She QB, Solit D, Mills GB, Smith D, et al. mTORinhibition induces upstream receptor tyrosine kinase signaling andactivates Akt. Cancer Res 2006;66:1500–8.
40. Carracedo A, Ma L, Teruya-Feldstein J, Rojo F, Salmena L, Alimonti A,et al. Inhibition of mTORC1 leads toMAPK pathway activation througha PI3K-dependent feedback loop in human cancer. J Clin Invest2008;118:3065–74.
41. Kanamori Y, Kigawa J, Itamochi H, Shimada M, Takahashi M, Kama-zawa S, et al. Correlation between loss of PTEN expression and Aktphosphorylation in endometrial carcinoma. Clin Cancer Res 2001;7:892–5.
42. Podsypanina K, Ellenson LH, Nemes A, Gu J, Tamura M, Yamada KM,et al. Mutation of Pten/Mmac1 in mice causes neoplasia in multipleorgan systems. Proc Natl Acad Sci U S A 1999;96:1563–8.
43. Castellvi J, Garcia A, Ruiz-Marcellan C, Hern�andez-Losa J, Peg V,Salcedo M, et al. Cell signaling in endometrial carcinoma: phosphor-ylated 4E-binding protein-1 expression in endometrial cancer corre-lates with aggressive tumors and prognosis. Hum Pathol 2009;40:1418–26.
44. No JH, Jeon YT, Park IA, KangD, Kim JW, ParkNH, et al. Expression ofmTOR protein and its clinical significance in endometrial cancer. MedSci Monit 2009;15:BR301–5.
45. GingrasAC,RaughtB,SonenbergN. eIF4 initiation factors: effectors ofmRNA recruitment to ribosomes and regulators of translation. AnnuRev Biochem 1999;68:913–63.
46. Pause A, Belsham GJ, Gingras AC, Donz�e O, Lin TA, Lawrence JC Jr,et al. Insulin-dependent stimulation of protein synthesis by phosphor-ylation of a regulator of 5¢-cap function. Nature 1994;371:762–7.
47. Raught B, Gingras AC, Gygi SP, Imataka H, Morino S, Gradi A, et al.Serum-stimulated, rapamycin-sensitive phosphorylation sites in theeukaryotic translation initiation factor 4GI. EMBO J 2000;19:434–44.
48. Shahbazian D, Roux PP, Mieulet V, Cohen MS, Raught B, Taunton J,et al. The mTOR/PI3K and MAPK pathways converge on eIF4B tocontrol its phosphorylation and activity. EMBO J 2006;25:2781–91.
49. Mamane Y, Petroulakis E, Martineau Y, Sato TA, Larsson O, Rajase-khar VK, et al. Epigenetic activation of a subset of mRNAs by eIF4Eexplains its effects on cell proliferation. PLoS ONE 2007;2:e242.
50. Mamane Y, Petroulakis E, Rong L, Yoshida K, Ler LW, Sonenberg N.eIF4E—from translation to transformation. Oncogene 2004;23:3172–9.
51. Choi CH, Lee JS, Kim SR, Lee YY, Kim CJ, Lee JW, et al. Directinhibition of eIF4E reduced cell growth in endometrial adenocarcino-ma. J Cancer Res Clin Oncol 2011;137:463–9.
52. Darb-Esfahani S, Faggad A, Noske A, Weichert W, Buckendahl AC,M€uller B, et al. Phospho-mTOR and phospho-4EBP1 in endometrialadenocarcinoma: associationwith stage andgrade in vivo and linkwithresponse to rapamycin treatment in vitro. J Cancer Res Clin Oncol2009;135:933–41.
53. Hayes MP, Douglas W, Ellenson LH. Molecular alterations of EGFRand PIK3CA in uterine serous carcinoma. Gynecol Oncol 2009;113:370–3.
54. Li X, Xiao L, Yang Y, Shen H, Zeng H, Wang Z. The expression ofmammalian target of rapamycin in Ishikawa and HEC-1A cells. JHuazhong Univ Sci Technolog Med Sci 2008;28:340–2.
55. Milam MR, Soliman PT, Chung LH, Schmeler KM, Bassett RL Jr,Broaddus RR, et al. Loss of phosphatase and tensin homologuedeleted on chromosome 10 and phosphorylation of mammalian targetof rapamycin are associated with progesterone refractory endometrialhyperplasia. Int J Gynecol Cancer 2008;18:146–51.
56. Mori N, Kyo S, Sakaguchi J, Mizumoto Y, Ohno S, Maida Y, et al.Concomitant activation of AKT with extracellular-regulated kinase 1/2occurs independently of PTEN or PIK3CA mutations in endometrialcancer and may be associated with favorable prognosiss. Cancer Sci2007;98:1881–8.
57. Mutter GL, Lin MC, Fitzgerald JT, Kum JB, Baak JP, Lees JA, et al.Altered PTEN expression as a diagnostic marker for the earliestendometrial precancers. J Natl Cancer Inst 2000;92:924–30.
58. Wahl H, Daudi S, Kshirsagar M, Griffith K, Tan L, Rhode J, et al.Expression of metabolically targeted biomarkers in endometrial car-cinoma. Gynecol Oncol 2010;116:21–7.
59. Bae-Jump VL, Zhou C, Boggess JF, Gehrig PA. Synergistic effect ofrapamycin and cisplatin in endometrial cancer cells. Cancer 2009;115:3887–96.
60. Shafer A, Zhou C, Gehrig PA, Boggess JF, Bae-Jump VL. Rapamycinpotentiates the effects of paclitaxel in endometrial cancer cells throughinhibition of cell proliferation and induction of apoptosis. Int J Cancer2010;126:1144–54.
61. Treeck O, Wackwitz B, Haus U, Ortmann O. Effects of a combinedtreatment with mTOR inhibitor RAD001 and tamoxifen in vitro ongrowth and apoptosis of human cancer cells. Gynecol Oncol 2006;102:292–9.
62. Zhou C, Gehrig PA, Whang YE, Boggess JF. Rapamycin inhibitstelomerase activity by decreasing the hTERT mRNA level in endome-trial cancer cells. Mol Cancer Ther 2003;2:789–95.
63. An HJ, Cho NH, Yang HS, Kwak KB, Kim NK, Oh DY, et al. TargetedRNA interference of phosphatidylinositol 3-kinase p110-beta inducesapoptosis and proliferation arrest in endometrial carcinoma cells.J Pathol 2007;212:161–9.
64. Erdemoglu E, G€uney M, Giray SG, Take G, Mungan T. Effects ofmetformin on mammalian target of rapamycin in a mouse model ofendometrial hyperplasia. Eur J Obstet Gynecol Reprod Biol 2009;145:195–9.
65. McCampbell AS, Walker CL, Broaddus RR, Cook JD, Davies PJ.Developmental reprogramming of IGF signaling and susceptibility toendometrial hyperplasia in the rat. Lab Invest 2008;88:615–26.
66. MilamMR, Celestino J,WuW, Broaddus RR, Schmeler KM, SlomovitzBM, et al. Reduced progression of endometrial hyperplasia with oralmTOR inhibition in the Pten heterozygote murine model. Am J ObstetGynecol 2007;196:247, e1–5.
67. Massarweh S, Schiff R. Resistance to endocrine therapy in breastcancer: exploiting estrogen receptor/growth factor signaling crosstalk.Endocr Relat Cancer 2006;13[Suppl 1]:S15–24.
68. Gadducci A, Cosio S, Genazzani AR. Old and new perspectives in thepharmacological treatment of advanced or recurrent endometrial
mTOR and Translational Regulation in Endometrial Cancer
www.aacrjournals.org Clin Cancer Res; 17(24) December 15, 2011 7527
on October 19, 2020. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 5, 2011; DOI: 10.1158/1078-0432.CCR-11-1664

cancer: Hormonal therapy, chemotherapy and molecularly targetedtherapies. Crit Rev Oncol Hematol 2006;58:242–56.
69. O'Donnell A, Faivre S, Burris HA 3rd, Rea D, PapadimitrakopoulouV, Shand N, et al. Phase I pharmacokinetic and pharmacodynamicstudy of the oral mammalian target of rapamycin inhibitor ever-olimus in patients with advanced solid tumors. J Clin Oncol2008;26:1588–95.
70. Raymond E, Alexandre J, Faivre S, Vera K, Materman E, Boni J, et al.Safety and pharmacokinetics of escalated doses of weekly intrave-nous infusion of CCI-779, a novel mTOR inhibitor, in patients withcancer. J Clin Oncol 2004;22:2336–47.
71. Oza AM, Elit L, Biagi J, ChapmanW, TsaoM, Hedley D, et al. Molecularcorrelates associatedwith aphase II study of temsirolimus (CCI-779) inpatients with metastatic or recurrent endometrial cancer—NCIC IND160. J Clin Oncol 2006;24:3003.
72. Oza AM, Eisenhauer EA, Elit L, Cutz JC, Sakurada A, Tsao MS, et al.Phase II study of erlotinib in recurrent or metastatic endometrialcancer: NCIC IND-148. J Clin Oncol 2008;26:4319–25.
73. Colombo N, McMeekin S, Schwartz P, Kostka J, Sessa C, Gehrig P,et al. A phase II trial of themTOR inhibitor AP23573 as a single agent inadvanced endometrial cancer. J Clin Oncol 2007;25:5516.
74. Slomovitz BM, Lu KH, Johnston T, Coleman RL, Munsell M, BroaddusRR, et al. A phase 2 study of the oral mammalian target of rapamycininhibitor, everolimus, in patientswith recurrent endometrial carcinoma.Cancer 2010;116:5415–9.
75. Oza AM, Elit L, Tsao MS, Kamel-Reid S, Biagi J, Provencher DM, et al.Phase II study of temsirolimus in women with recurrent or metastaticendometrial cancer: a trial of the NCIC Clinical Trials Group. J ClinOncol 2011;29:3278–85.
76. Bae-Jump VL, Zhou C, Boggess JF, Whang YE, Barroilhet L, GehrigPA. Rapamycin inhibits cell proliferation in type I and type II endome-trial carcinomas: a search for biomarkers of sensitivity to treatment.Gynecol Oncol 2010;119:579–85.
77. Temkin SM, Yamada SD, Fleming GF. A phase I study of weeklytemsirolimus and topotecan in the treatment of advanced and/orrecurrent gynecologic malignancies. Gynecol Oncol 2010;117:473–6.
78. Sarbassov DD, Ali SM, Sabatini DM. Growing roles for the mTORpathway. Curr Opin Cell Biol 2005;17:596–603.
79. Hsieh AC, Costa M, Zollo O, Davis C, Feldman ME, Testa JR, et al.Genetic dissection of the oncogenicmTORpathway reveals druggableaddiction to translational control via 4EBP-eIF4E. Cancer Cell2010;17:249–61.
80. Liu Q, Wang J, Kang SA, Thoreen CC, Hur W, Ahmed T, et al.Discovery of 9-(6-aminopyridin-3-yl)-1-(3-(trifluoromethyl)phenyl)-benzo[h][1,6]naphthyridin-2(1H)-one (Torin2) as a potent, selective,and orally available mammalian target of rapamycin (mTOR) inhibitorfor treatment of cancer. J Med Chem 2011;54:1473–80.
81. Basil JB, Goodfellow PJ, Rader JS, Mutch DG, Herzog TJ. Clinicalsignificance of microsatellite instability in endometrial carcinoma.Cancer 2000;89:1758–64.
Korets et al.
Clin Cancer Res; 17(24) December 15, 2011 Clinical Cancer Research7528
on October 19, 2020. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 5, 2011; DOI: 10.1158/1078-0432.CCR-11-1664

2011;17:7518-7528. Published OnlineFirst December 5, 2011.Clin Cancer Res Sharmilee Bansal Korets, Sarah Czok, Stephanie V. Blank, et al. Targeting the mTOR/4E-BP Pathway in Endometrial Cancer
Updated version
10.1158/1078-0432.CCR-11-1664doi:
Access the most recent version of this article at:
Cited articles
http://clincancerres.aacrjournals.org/content/17/24/7518.full#ref-list-1
This article cites 80 articles, 24 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/17/24/7518.full#related-urls
This article has been cited by 3 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/17/24/7518To request permission to re-use all or part of this article, use this link
on October 19, 2020. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 5, 2011; DOI: 10.1158/1078-0432.CCR-11-1664