Upload
hugo-azzolina
View
218
Download
0
Embed Size (px)
Citation preview
8/11/2019 Tass Et Al_RNN 2012_Counteracting Tinnitus by Acoustic CR Neuromodulation
1/23
Restorative Neurology and Neuroscience 30 (2012) 137159DOI 10.3233/RNN-2012-110218IOS Press
137
Counteracting tinnitus by acousticcoordinated reset neuromodulation
Peter A. Tass a,b,, Ilya Adamchic a , Hans-Joachim Freund a , Tatjana von Stackelberg c
and Christian Hauptmann aa Research Center J ulich, Institute for Neuroscience and Medicine Neuromodulation INM-7, J ulich, Germanyb Department of Stereotaxic and Functional Neurosurgery, University Hospital, Cologne, Germanyc Ear, Nose and Throat (ENT) Center, Meerbusch, Germany
Abstract . Purpose : Subjective tinnitus is associated with pathologic enhanced neuronal synchronization. We used a modelbased desynchronization technique, acoustic coordinated reset (CR) neuromodulation, to specically counteract tinnitus-relatedneuronal synchrony thereby inducing an unlearning of pathological synaptic connectivity and neuronal synchrony. Methods : In a prospective, randomized, single blind, placebo-controlled trial in 63 patients with chronic tonal tinnitus and upto 50 dB hearing loss we studied safety and efcacy of different doses of acoustic CR neuromodulation. We measured visualanalogue scale and tinnitus questionnaire (TQ) scores and spontaneous EEG. Results : CR treatment was safe, well-tolerated and caused a signicant decrease of tinnitus loudness and symptoms. Placebo
treatment did not lead to any signicant changes. Effects gained in 12 weeks of treatment persisted through a preplanned 4-week therapy pause and showed sustained long-term effects after 10 months of therapy: Response, i.e. a reduction of at least 6 TQpoints, was obtained in 75% of patients with a mean TQ reduction of 50% among responders. CR therapy signicantly loweredtinnitus frequency and reversed the tinnitus related EEG alterations.Conclusion : TheCR-induced reductionof tinnitus andunderlyingneuronalcharacteristics indicatesa newnon-invasive therapywhich might also be applicable to other conditions with neuronal hypersynchrony.
Keywords: Tinnitus treatment, desynchronization, plasticity, non-invasive neuromodulation
1. Introduction
Subjective tinnitus is an acoustic phantom phe-nomenon, a perception of sound in the absence of physical sound sources (Eggermont, 2003; Lockwoodet al., 2002; Moller, 2003; Weisz et al., 2005a).This type of tinnitus is typically initiated by dam-age to the peripheral hearing system (Irvine et al.,2001; Lockwood et al., 2002; Norena et al., 2002;
Corresponding author: Prof. Dr. Peter A. Tass, Research CenterJulich, Institute for Neuroscience and Medicine NeuromodulationINM-7, 52425 J ulich, Germany. Tel.: +49 2461 61 2087; Fax: +492461 61 1880; E-mail: [email protected] .
Weisz et al., 2006) leading to a sequence of structuraland functional changes in the central hearing system(Eggermont, 2003; Lockwood et al., 2002; Moller,2003; Eggermont and Roberts, 2004; Saunders, 2007).Both human and animal data show that deafferenta-tion alters receptive elds (Rajan and Irvine, 1998;Rauschecker, 1999; Irvine et al., 2001; Dietrich et al.,2001) and spontaneous activity (Eggermont, 2003;Norena and Eggermont, 2003; Elbert et al., 1997) of neurons in the auditory cortex. There are two majorphenomenaassociated with tinnitus: cortical map reor-ganization (Robertson and Irvine, 1989; M uhlnickelet al., 1998; Lockwood et al., 2002; Moller, 2003)and the emergence of pathological neural synchrony
0922-6028/12/$27.50 2012 IOS Press and the authors. All rights reserved
mailto:[email protected]:[email protected]8/11/2019 Tass Et Al_RNN 2012_Counteracting Tinnitus by Acoustic CR Neuromodulation
2/23
138 P.A. Tass et al. / Counteracting tinnitus by acoustic coordinated reset neuromodulation
(Ochi and Eggermont, 1997; Norena and Eggermont,2003; Seki and Eggermont, 2003; Weisz et al., 2005a;Weisz et al., 2007).
Cortical map reorganization was demonstrated inanimals with restricted cochlear lesions (RobertsonandIrvine, 1989; RajanandIrvine, 1998;Rauschecker,1999; Irvine et al., 2001) and in tinnitus patients(Muhlnickel et al., 1998; Dietrich et al., 2001; Weiszet al., 2005b). In a magnetoencephalography (MEG)study Muhlnickel et al. (1998) found that the corticalrepresentation of the tinnitus frequency was clearlyshifted into an area adjacent to the expected tono-topic location. However, patients with audiometricallyimpairedhearing were excludedfrom that study, so thatsubjects were not representative of typical tinnitus suf-ferers. In contrast, recent results obtained with MEGrecordingsin tinnituspatients suggest thatmechanismsof map reorganization cannot explain the emergenceof tinnitus in a satisfactory manner (Weisz et al.,2005a).
Pathologically increased activity emerges in corti-cal regions deprived of afferent input (Steriade, 2006).Correspondingly, MEGstudies in patientswithchronicsubjective tinnitus revealed an increase of power inparticular frequency bands (Llin as et al., 1999; Weisz
et al., 2005a; Weisz et al., 2007). An increase of bandpower in MEG,electroencephalogram(EEG) and localeld potential (LFP) signals is typically interpretedas an increase in neuronal synchronization in termsof coincident ring within a neuronal population (seeKlaas and Daly, 1979; Nunez, 1981; H amalainen etal., 1993; Niedermeyer and Lopes da Silva, 1999 andDiscussion). In an MEG study Weisz et al. (2005a)showed that in tinnitus patients band power wassignicantly reduced, whereas band power was sig-nicantly increased, particularly in temporal regions.Furthermore, tinnitus related distress was correlatedwith this abnormal pattern of spontaneous activityin particular in right temporal and left frontal brainareas. In a further MEG study Weisz et al. (2007)analyzed band activity during brief epochs of pro-nounced enhancement of wave activity. In bothgroups, controls and tinnitus patients, band activ-ity was signicantly increased after onset of waves.However, was more pronounced in tinnitus sub- jects compared to controls. activity at 55 Hz wasrelated to the laterality of the tinnitus perception.Pathological neural synchronization has consistentlybeen conrmed in further studies as the electrophys-iological correlate of the tinnitus percept. Tinnitus
could be reduced by an EEG neurofeedback mediatedsuppression of band activity and enhancement of band (Dohrmann et al., 2007a). In an MEG study a sig-nicant reduction of band activity in temporal areaswas found during residual inhibition (Kahlbrock andWeisz, 2008). Epidural recordings from the secondaryauditory cortex in a tinnitus patient revealed abnormal
bandactivity highly correlatedwith tinnitus loudness(De Ridder et al., 2011). Also in patients with acutetinnitus afternoisetrauma abnormal neuronal synchro-nization, namely increased band activity in the rightauditory cortex, was found in an MEG study (Ort-mann et al., 2011). Not only auditory cortical areas areinvolved in the generation of tinnitus. Rather there isgrowing evidence that non-auditory areas, e.g., amyg-dala, cingulate cortex and parahippocampus, play acrucial rule, in particular, in patients with relevanttinnitus distress (Rauschecker et al., 2010; Vannesteet al., 2010). In fact, the functional interaction betweennon-auditory and auditory areas displaying abnormalsynchrony appears to be a central feature underlyingtinnitus distress (Schlee et al., 2009a).
As yet, typically used tinnitus treatment strate-gies, such as tinnitus retraining therapy (Jastreboff and Hazell, 1993), are basically approaches to facil-
itate habituation. In fact, there is a great demand formore causally oriented treatments specically target-ing the neuronal correlates of the tinnitus percept.Different approaches have been tested so far (Molleret al. 2011). Depending on the parameters chosen,transcranial magnetic stimulation (TMS) may lead toa decrease (Chen et al., 1997) or increase (Pascual-Leone et al., 1994) of cortical excitability along withlong-term potentiation or long-term depression (Wanget al., 1996). TMS has been applied to tinnitus patients(Plewniaet al., 2003; De Ridderet al., 2005).Althoughin a subgroup of patients repetitive TMS resultedin tinnitus relief, the effects were only moderate,whereas interindividual variability is high, so thatfurther improvement is required until TMS can be rec-ommended for clinical use (Kleinjung et al., 2011).Another intervention with quite complex and still notsufciently understood mechanism of action is audi-tory cortex stimulation (De Ridder et al., 2005; DeRidder et al., 2006). One mechanism of action may bethat cortical stimulation directly provides deafferentedcortexwith missing input (DeRidderet al., 2007).Onein three patients responds best to tonic auditory cortexstimulation, and one in three to burst stimulation (DeRidder et al., 2011; De Ridder and Vanneste, 2011).
8/11/2019 Tass Et Al_RNN 2012_Counteracting Tinnitus by Acoustic CR Neuromodulation
3/23
8/11/2019 Tass Et Al_RNN 2012_Counteracting Tinnitus by Acoustic CR Neuromodulation
4/23
140 P.A. Tass et al. / Counteracting tinnitus by acoustic coordinated reset neuromodulation
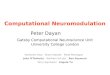
Fig.1. Acoustic coordinated reset(CR) neuromodulation:(a) The conceptof CR neuromodulationcomprises a spatial andtemporalcoordinationof the applied stimuli to induce desynchronization leading to anti-kindling (Tass, 2003): utilizing the tonotopic organization of the primaryauditory cortex (left, brain adapted from Chittka and Brockmann PLoS Biology, 2005 with kind permission of the authors) short sinusoidaltones of different frequencies (f 1 to f 4) induce a soft reset in different target areas grouped around the tinnitus focus (Tass, 2002). Three CRcycles, each comprising a randomized sequence of four tones (right), are followed by two silent cycles. That pattern is repeated periodically. Therandom variation of the tone sequences (Tass and Majtanik, 2006) and the 3 : 2 ON-OFF pattern (Tass, 2003, Lysyansky et al., 2011) optimizethe desynchronizing CR effect. (b) Four stimulation groups and one placebo group were investigated. For G1, G3 and G4 four tones (top, f 1 to
f 4) are grouped around the tinnitus frequency (f t). G3 differs only in repetition rate F being adapted to the individual EEG -band peak. For G2each CR cycle is formed by a varying composition of four tones (dark green: active) chosen out of twelve tones (middle, f 1 to f 12 ) surrounding f t.Placebo stimulation (bottom, G5) is formed similar to G1 using a down-shifted stimulation-frequency f p (f p = 0.7071 f t / (2n), f p within [300 Hz,600 Hz]) outside the synchronized tinnitus focus.
band of the stimulation tones measured by an audio-gram from 0.125 to 12 kHz) were randomly allocatedto receive CR neuromodulation (group G1 to G4) orplacebo stimulation (G5): G1 ( n = 22), G2 (n = 12), G3(n =12), G4 (n =12), G5 (n = 5), see Table 1. Cen-tral randomization was provided by a clinical researchorganization (CRO). The randomization scheme wascomputer generated utilizing a block randomization.The assignment of treatments occurred in accordancewith thenumericalsequenceof patient enrolmentusingsealed envelopes.A higher number of patientswasallo-cated toG1 tocorroborate thedatabasefor itssuspectedmost efcacious stimulation algorithm.
Exclusion criteria were: Morbus Meniere, audi-tory hallucinations, symptomatic hearing disorders,tinnitus due to temporomandibular joint disorders,brainstem diseases, psychiatric disorders and objec-tive tinnitus. The ethical committee approved the trialdesign and all changes. The safety of the study was
monitored by an independent Data and Safety Mon-itoring Board (DSMB). The study was performed inaccordance with the Declaration of Helsinki and GoodClinical Practice guidelines. All participating patientsgave their written informed consent.
2.2. Tinnitus characteristic analysis
The tinnitus frequency f t (from 10010.000 Hz)wasassessed with a pure tone matching, where intensityand frequency of the matching tone were controlledby the patient.
2.3. Study design
Patients were stimulated for 12 weeks using aportable acoustic device and comfortable earphones(loudness controlled by patient) followed by an addi-tional off-stimulation 4-week period to assess lasting
8/11/2019 Tass Et Al_RNN 2012_Counteracting Tinnitus by Acoustic CR Neuromodulation
5/23
P.A. Tass et al. / Counteracting tinnitus by acoustic coordinated reset neuromodulation 141
Table 1Baseline data
Gl (n = 22) G2 (n = 12) G3 (n = 12) G4 (n = 12) G5 ( n = 5)Age [mean (SD)] 45 .7(10 .8) 47.7 (5 .6) 50 .0 (14 .7) 50.3(11 .8) 57 .6 (6 .3)Sex (male %) 72.7 83.3 50.0 75.0 60.0BMI (kg/m 2) [mean (SD)] 26 .1 (5.2) 27.7 (4 .2) 26.8 (4.3) 25.7 (3 .6) 25 .3 (4 .0)Smoke (yes %) 27.3 25.0 16.7 0.0 40.0Social drinking (yes %) 77.3 66.7 66.7 75.0 100.0Tinnitus duration (in years) [mean (SD)] 5 .7 (5.1) 6.6 (6 .0) 5.4 (3.5) 7.9 (9 .8) 11 .3 (5 .6)Tinnitus side (unilateral %) 45.5 33.3 50.0 16.7 40.0VAS Loudness [mean (SD)] 70 .9(14 .9) 52.1(21 .5) 66.3(20 .4) 72.1(16 .7) 43.0(19 .2)VAS Annoyance [mean (SD)] 66 .4(17 .3) 54.2(21 .6) 64 .2 (22 .0) 70.8(17 .0) 38.0(14 .8)TQ [mean (SD)] 43 .1(16 .7) 38.6(15 .9) 36.5(16 .4) 50.8(15 .9) 29.2 (7 .7)Tinnitus frequeny (kHz) [mean (SD)] 7 .7 (2 .9) 5.0 (2 .5) 4.7 (3.5) 5.4 (3 .3) 5.8 (3 .4)EEG power (a.u.) [mean (SD)] 0.23 (0.11) 0.27 (0.13) 0 .26(0 .09) 0 .22(0 .10) 0.24(0 .1)EEG power (a.u.) [mean (SD)] 0.37 (0.2) 0.32 (0.19) 0 .34(0 .21) 0.36(0 .17) 0.35(0 .17)EEG analysis: n = 21 (11) were evaluable in Gl (G2).
effects of acoustic CR neuromodulation; an optionalopen-label long-term extension (LTE) period (24weeks) was offered. Visits took place 1, 4, 8, 12 and 16weeks after beginning of treatment and every 4 weeksduring LTE.
Tinnitus loudness and annoyance were rst mea-sured off-stimulation (at least 2.5 hours after
cessation of CR neuromodulation) and consecutivelyon-stimulation (15minafter turning on CR neuromod-ulation) by a visual analog scale (VAS). VAS scalesranged from 0 (corresponding to absence of tinnitus)to 100 (corresponding to maximal imaginable loud-ness or annoyance). The tinnitus distress level wascaptured by the German version of the Tinnitus Ques-tionnaire (TQ, measured off-stimulation) (Goebel andHiller, 1994). The TQ is a patient reported measureof 52 items assessing emotional and cognitive dis-tress, intrusiveness, auditory perceptual difculties,sleep disturbances and associated somatic complaints.The TQ is a highly reliable (test-retest reliability 0.94)and valid instrument with scores ranging from 0 to84 (Goebel and Hiller, 1998). Like the VAS loud-ness and VAS annoyance, higher scores on the TQreect greater severity. Mean values and standarddeviations are given. Auditory thresholds were mea-sured by an audiogram (performed at 0.125, 0.25, 0.5,0.75, 1, 1.5, 2, 3, 4, 6, 8, 12 kHz) in a sound-proof chamber.
2.4. Euclidean distance of normalized clinicalscores
The Euclidean distance was calculated based on thenormalizedclinical scores (VAS Loudness , VAS Annoyanceand TQ). The Euclidean distance d between two sub-groups of n patients was dened as
1n2
n
l= 1
n
k= 1
2
VAS lLoudness VAS
kLoudness
2
+ VAS lAnnoyance VAS
kAnnoyance
2
+ TQl
TQk 2
= : d
where VASlLoudness (VAS
k Loudness ) denote the normal-
ized valueof theVAS Loudness scoreforpatientl(k)fromthe rst (second) subgroup, respectively (similarly forVAS Annoyance and TQ). Normalization, i.e. division bythe maximal value, was performed in order to achievea uniform weighting of all three clinical scores.
2.5. Stimulation protocol
G1toG3allreceived stimulationfor46hourseveryday (Fig. 1b) applied either continuously or split intoseveral sessions not shorter than 1 hour each to uti-lize cumulative effects (Jacobson and Truax, 1991);G4 and G5 all received stimulation for 1 hour max.every day. Stimulation signals weregeneratedbasedona specic formula reecting the logarithmic tonotopicorganization of the auditory cortex and on the matchedtinnitus (frequency f t) with an equal number of tonesplaced below and above tinnitus frequency (except forplacebo, Fig. 1b). Stimulation tones were equally loudand just super-threshold. 4 tones per cycle were playedin random order with 3 stimulation cycles followed by
8/11/2019 Tass Et Al_RNN 2012_Counteracting Tinnitus by Acoustic CR Neuromodulation
6/23
142 P.A. Tass et al. / Counteracting tinnitus by acoustic coordinated reset neuromodulation
2 silent cycles (Fig. 1a). The silent cycles were intro-duced in order to optimize the duration of the transientdesynchronization and, hence, the anti-kindling effect(see Tass, 2003;Lysyanskyet al., 2011).The 4 tonesarebasedona patient specic list of frequencies,seeFig. 1:G1, G3, G4(f 1 to f 4); G2(prior toeachcycle 4 frequen-cies are chosen from f 1 to f 12); G5 based on a modiedtinnitus frequency (f p =0.7071f t /(2n), f p within 300 to600 Hz).Thestimulation tonesare equidistantlyplacedon a logarithmic scale within the interval [0.5 f t, 2f t]for G1 to G4 and within [0.5 f p , 2f p] for G5. Cyclerepetition rate was 1.5Hz, i.e. in the lower frequencyrange, for G1, G2, G4, G5, because the primary tar-get for desynchronization was the pathological bandactivity. We have chosen the repetition rate within thelower frequency range because according to theoret-ical studies it is more favorable to use a stimulationrate that is slightly to low instead of being slightlytoo high (see Tass, 2003; Lysyansky et al., 2011).Also, psychophysically greater repetition rates wereperceived as less relaxing and, hence, less convenient.In contrast, in G3 the repetition rate was set equal tothe peak frequency in the patients frequency rangeaccording to the EEG data (Tass, 2003; Tass et al.,2009).
A readjustment of stimulation parameters could bedone at each visit if matched tinnitus frequency hadchanged.
2.6. EEG data
Every patient underwent two EEG recording ses-sions:on therst treatmentdaybefore treatmentbeganand atthe 12weeks visit,at least two hours after the endof the last stimulation session. EEG recordings wereobtained in a Faraday cage with a 128 EEG surfaceelectrodes system (128 channel HydroCel GeodesicSensor Net) in a quiet and dimly lighted room witheach participant sitting upright on a comfortable chair.All electrodes were referenced to Cz.Recordings wereperformed twice in awake patients with eyes closedand eyes open for 2 min each. We have selected eyesclosed data for further analysis since they were lessaffected by artifacts. Impedances were kept below 100k as required by the EEG recording system. EEGsignals were digitized at 1 kHz and digitally lteredwith a 0.8130 Hz digital lter. Each EEG recordingwas corrected for blink and eye movements in BESAusing a surrogate model approach from BESA (Scherg
et al., 2002) (BrainElectrical SourceAnalysis,MEGISSoftware, version 5.2). Recordings were further ana-lyzed in MATLAB (The Mathworks, Natick, MA)using EEGLAB ( http://sccn.ucsd.edu/eeglab ) wheremuscle artifacts and artifacts from heart activity (elec-trocardiogram) were removed. The total eyes closedrecording after artifact correction lasted on average3min 36sec 24 sec. Two types of inverse calcula-tion of the surface EEG signals were performed: (i)Surface EEG was transformed into brain source activ-ity of the primary auditory cortex (ACI, Brodmannarea 41) using the source montage approach in BESAfor G1 (n = 21 evaluable) and G5 ( n = 5). According toprevious studies (M uhlnickel et al., 1998; Lockwoodet al., 1998; Lockwood et al., 1999; Melcher et al.,2000; Kovacs et al., 2006; Smits et al., 2007; Weiszet al., 2007; van der Loo et al., 2009) in patients withunilateral tinnitus we used the contralateral ACI, inpatients with bilateral tinnitus we used both ACI. (ii) Inpatients with bilateral tinnitus surface EEG was trans-formed into current source density with sLORETA(Pascual-Marqui, 2002), where the three-dimensionalsolution space was restricted to the cortical gray mat-ter. Unilateral and bilateral tinnitus patients can havedifferent EEG abnormalities (Vanneste et al., 2011).
Accordingly, to avoid an inuence of such differ-ences, we selected only patients with bilateral tinnitus(n = 28) from G1 to G4. To increase the signal-to-noise ratio from this population of 28 patients withbilateral tinnitus 12 patients were selected for thesLORETA analysis following the TQ based reliable-change-index (RCI) method (Jacobson and Truax,1991). This subgroup of n = 12 patients had the fol-lowing demographic and clinical characteristics (mean(SD)): age 46.5 (7.9), tinnitus duration 7.6 (7.4), TQat baseline 52.3 (17.5), VAS Loudness at baseline 72.1(20.7), VAS Annoyance at baseline 71.7 (23.1) and tinni-tus frequency 5.9 kHz (3.5). The sLORETA subgroupshowed the following improvements at 12 weeks:TQ 19.5 (9.1), VAS Loudness on/off stimulation 37.9(35.4)/26.7 (26.2), VAS Annoyance on/off stimulation41.3 (35.2)/21.3 (26.6). Images were transformedto the stereotactic Talairach space and overlaid witha standard, structural MRI scan (MNI152 template).Statistical signicance of sLORETA changes wasnon-parametrically assessedon a voxel-by-voxel basiswitha randomization test (Nichols and Holmes, 2002)which corrects for multiple comparisons. Finally,power spectra were calculated for both types of inversesolutions and averaged across patients. Power spec-
http://sccn.ucsd.edu/eeglabhttp://sccn.ucsd.edu/eeglab8/11/2019 Tass Et Al_RNN 2012_Counteracting Tinnitus by Acoustic CR Neuromodulation
7/23
P.A. Tass et al. / Counteracting tinnitus by acoustic coordinated reset neuromodulation 143
tra, calculated using fast Fourier transform, weredivided into normalized EEG frequency bands: (14 Hz), (48 Hz), (812Hz), (1230 Hz), low(3048 Hz) and high (5290 Hz). Power spectra wereaveraged across patients, and frequency bands groupdifferences between the untreated and treated con-ditions were tested with the Wilcoxon signed-rank test.
2.7. Statistical methods
The statistical analysis was based on an intention-
to-treat analysis including all randomized subjects.The sample size estimation was based on pre-clinicalobservations and empirical considerations. For miss-ing values the LOCF method was used (rst 16weeks).
Descriptive statistics were used to compare baselineto end-of-treatment values (Wilcoxon matched pairsperformed on non-log-transformed data and Signtest). Comparison to placebo was done applying theMannWhitney U test. Due to the exploratory naturewe tested two-sided without adjustment for multiplecomparisons at the 5% signicance level. Correlationwas calculated using the Pearson product-momentcorrelation.
For sLORETA we assessed statistical signicance,correctedfor multiple comparisons,by meansof a non-parametric randomization test (Nichols and Holmes,2002).
3. Results
Clinical examination after 12 weeks of therapyrevealed a strong (29.6 to 37.3 points) and signi-cant reduction of VAS loudness/annoyance in G1 andG3 in the on-stimulation condition ( p 0.01 com-pared to baseline, Fig. 2a, Table 2). The effects inG1 are signicant also compared to placebo ( p < 0.05,Fig. 2b). In the off-stimulation condition signicanteffects persisted for G1/G3 VAS loudness/annoyance(18.0 to 28.8 points, p < 0.004 Fig. 2a, Table 2) inaccordance with theoretically predicted lasting anti-kindling effects. In G2, the noisy CR group, onlyon-stimulation effects showed signicant reductions( p < 0.05, Fig. 2a, Table 2) and the difference betweenon- and off-stimulation effect was strongest (Fig. 2c, p < 0.01). In G4 (reduced stimulation time of 1 h/day)we observed a signicant decrease for both VAS loud-
ness/annoyance scores in the on-stimulation condition( p < 0.05) andmarkedly less inoff-stimulation (Fig. 2a,Table 2). In contrast, theplacebo group G5showednei-ther on-noroff-stimulation signicant changes in VASloudness/annoyance scores after 12 weeks, (Fig. 2a,Table 2).
After a subsequent 4-week therapy pause G1 andG3 preserved signicant reductions in tinnitus loud-ness and annoyance (Fig. 2a, Table 2). In general,we found a high correlation between the CR inducedchanges in VAS loudness ( VAS Loudness ) and annoy-ance ( VAS Annoyance ) i.e. r = 0.92 (baseline to 12weeks, p < 0.001, Fig. 2f).
TQ severity levels signicantly improved after 12and 16 weeks in G1 ( p < 0.01 compared to baseline)and G3 ( p < 0.05, Fig. 2d, Table 2). In G4, a small butsignicant decrease of the TQ severity levels was seenafter12weeks( p < 0.05,Fig. 2d,Table2). G5(placebo)did not show any signicant change.
TQ scores (mean values) were signicantly reducedcompared to baseline in G1 to G4 with the strongestimprovements in G1 and G3 (12/16 weeks, Table 2).In contrast, there were no signicant changes in TQscore in the placebo group G5 (Table 2).
Tinnitus frequency (pure tone matching) was signif-
icantly reduced in G1 after 12 and 16 weeks ( p < 0.01,Table 2), while placebo did not show signicantchanges of tinnitus frequency.
In all patients with a hearing impairment it was of asensorineural type. Auditory threshold averaged fromthe three frequencies of our audiogram procedure (seemethods) closest to the tinnitus frequencywas 29.8 dB.No signicant changes in auditory thresholds weredetected pre/post treatment.
3.1.1. Impact of tinnitus duration, tinnitusseverity and age on treatment outcome
Analyzingfor tinnitus duration, tinnitus severityandage revealed no confounding factor for treatment suc-cess of 46 h/day treated CR neuromodulation (CRgroups G1 + G3 after 12 weeks tinnitus duration inyears versus relative TQ change r = 0.14, p = 0.43,tinnitus severity in TQ versus relative TQ changer = 0.16, p = 0.35 and age versus relative TQ changer = 0.09, p = 0.62; after40weeksforall patients tinnitusduration in years versus relative TQ change r = 0.05, p = 0.74, tinnitus severity in TQ versus relative TQchange r = 0.18, p = 0.19 and age versus relative TQchange r = 0.01, p = 0.94).
8/11/2019 Tass Et Al_RNN 2012_Counteracting Tinnitus by Acoustic CR Neuromodulation
8/23
144 P.A. Tass et al. / Counteracting tinnitus by acoustic coordinated reset neuromodulation
Fig. 2. (Continued )
8/11/2019 Tass Et Al_RNN 2012_Counteracting Tinnitus by Acoustic CR Neuromodulation
9/23
P.A. Tass et al. / Counteracting tinnitus by acoustic coordinated reset neuromodulation 145
3.1.2. Comparison between placebo group and equally sized, matched subgroups of G1
To better control for the baseline characteristics of the placebo group we matched G5 ( n =5) with anequally sized subgroup of G1 with comparable base-line characteristics (mean TQ exactly 29.2 pts in bothgroups at baseline and VAS scales for loudness andannoyance also not signicantly different). We founda signicant improvement compared to baseline (off-stimulation) after the rst 12 weeks of treatment forthe G1 subgroup only (VAS loudness G1 sub 24 pts.mean, p = 0.07, vs. G5 9y pts. mean, not signicant;VAS annoyance G1 sub 23 pts. mean, p = 0.04 vs. G52 pts. mean, not signicant; TQ G1 sub 11.8 pts.mean, p = 0.04, vs. G5 8.4 pts. mean, not signicant).
Furthermore we matched G5 ( n = 5) with 100equally sized subgroups of G1 with comparable base-line characteristics (mean TQ exactly 32.4 pts. atbaseline ( p = 0.67 as compared to G5) and VAS scalesfor loudness and annoyance also not signicantly dif-ferent). These G1 subgroups were selected from the26334 possible combinations of 5 patients in the G1subgroup derived from 22 patients in G1 based on theshortestEuclideandistancebetweeneachG1 subgroup
and G5. Euclidean distances were calculated based onthe VAS loudness/annoyance and TQ for each G1 subgroupseparately (seeMethods).Wefounda substantialimprovementascomparedto baseline(off-stimulation)after therst12weeksof treatmentfor theG1 subgroup(VAS loudness G1 sub 22 pts. mean, p = 0.08, vs. G5
9y pts. mean, p = 0.50; VAS annoyance G1 sub 19pts. mean, p = 0.08 vs. G52 pts. mean, p = 1.00; TQG1 sub 9.5 pts. mean, p = 0.06, vs. G5 8.4 pts. mean, p = 0.12).
3.1.3. Pooled comparison between effectiveand ineffective stimulation groups
For a robust statistical comparison of all 46 h/dayCR treated patients with the rest of the patients wepooled two big groups with comparable sizes: theeffective stimulation group G1 + G3 ( n =34) wascompared with the ineffective stimulation groupcomprising all data of G2 (noisy stimulation with amasker effect but without lasting off-effect), G4 (only1 h of CR neuromodulation per day leading to smallerimprovements) andG5 (the placebo group) with n = 29patients, see Table 4.
As a result, after 12 weeks of stimulation VASloudness ( p = 0.0009, p = 0.0186), VAS annoyance( p = 0.0021, p = 0.0488) and TQ ( p = 0.0076) allshowed markedly higher improvements in the effec-tive stimulation group compared to the ineffectivestimulation group (for on-, off-stimulation if appli-cable). Notably, the improvements in tinnitus severityand loudness were accompanied by a signicant and
pronounced shift in tinnitus frequency in thepooled CRneuromodulation group (between 16.5% and 22.2%average Tinnitus frequency shift in % of baseline)but not for the pooled ineffective stimulation group(between+2.4%and2.6 % average tinnitus frequencyshift in % of baseline), see Table 4.
Fig. 2. Clinical effects of acoustic CR neuromodulation assessed in the framework of the RESET study. (a) Visual analogue scale (VAS) scoresfor loudness(left)and annoyance (right) forgroup1 to 5. TheVAS scoresare displayedat baseline (0)and at 4, 12 and16 weeks.The black (red)lines indicate the VAS scores obtained during off-stimulation (on-stimulation). The gray shaded area indicates the 12 weeks treatment phase,followedby a treatmentpause of 4 weeks.The stars indicate signicant results as compared to baseline.AcousticCR neuromodulationinducedasignicant long-lastingreduction of VAS scores(off-stimulation, black)for therapy groups1 and3 while groups 2, 4 and5 (placebo stimulation)
showed no signicant long-lasting treatment effects. Additionally, therapy groups 1 to 4 showed strong benecial effects during stimulation(on-stimulation, red). (b) Changes of the VAS scores for loudness (left) and annoyance (right) with respect to baseline for the 12-week visit (leftside of each plot) and the 16-week visit (right side of each plot) are given. The scores are plotted for off-stimulation (top) and on-stimulation(bottom) for G1 to G5 (from left to right). The stars indicate signicant results as compared to placebo. Since at 16-week visit placebo (G5)started to receive G1 treatment, no data for on-stimulation was available. (c) On/Off-treatment effects ( VASon VASoff ) at 12 weeks aregiven. The stars indicate signicant results as compared to placebo. (d) Tinnitus related distress level based on the tinnitus questionnaire (TQ,ranging from 0 to 84 points) is given (Goebel and Hiller 1998). Subjects are grouped into four severity levels: very severe (6084, black),severe (4759, dark gray), moderate (3146, light gray) or mild (030, white). TQ severity level distribution is displayed at baseline, 12 and16 weeks. Improvement in tinnitus severity level distribution was signicant for G1 ( p < 0.01), G3 and G4 ( p < 0.05), but not for placebo (G5)(stars indicate signicant results as compared to baseline, Sign-nonparametric test, p-values (12/16 weeks): G1 0.0002/0.0003, G2: 0.48/-,G3 : 0.023/0.041, G4 : 0.041/0.08, G5 : 0.48/-; -: test not applicable due to no level variation). (e) Treatment induced changes in oscillatoryEEG activity (off-stimulation). EEG activity for G1 (top) and placebo (bottom) was assessed at baseline (white) and at 12 weeks (gray). Thenormalized EEG power in the and band is shown for G1 ( n = 21 evaluable) and G3 ( n = 5). Stars indicate signicant results as comparedto baseline. (f) Correlation between VASLoudness and VASAnnoyance . VAS-values are calculated for the 12-week visit (off-stimulation)compared to baseline. Changes of tinnitus loudness and annoyance are strongly and signicantly correlated ( r = 0.92, p < 0.001). Dashed linesindicate 95% condence levels. For all plots: mean values (ac, e) and TQ grouping (d) is shown, * p < 0.05, ** p < 0.01.
8/11/2019 Tass Et Al_RNN 2012_Counteracting Tinnitus by Acoustic CR Neuromodulation
10/23
Table 2Change from baseline to end of treatment phase (12 week follow up) and after the 4 weeks treatment pause (16 week follow up) in primary efcacy
Treatment-group G1 ( n = 22) G2 (n = 12) G3 (n = 12) G4 (n = 12) Follow-up (week) 12 16 12 16 12 16 12 1VAS Loudness
Change from baseline(off-stimulation) [mean (SD)]
21.8 (19.2) 17.0 (22.8) 2.1 (21.7) 2.1 (22.4) 25.8 (25.3) 18.3 (26.8) 6.7 (15.3) 6.7 (11
p value (change from baseline )
8/11/2019 Tass Et Al_RNN 2012_Counteracting Tinnitus by Acoustic CR Neuromodulation
11/23
P.A. Tass et al. / Counteracting tinnitus by acoustic coordinated reset neuromodulation 147
3.1.4. Comparison to masker type of stimulation(noisy CR, G2)
All groups were compared with the noisy maskerlike stimulation (G2) that showed a good on-effect likeG1 and G3 but no lasting off-effect. After 12 weeks of treatment signicant differences occurred for TQ infavor of G1 ( p = 0.0171) and G3 ( p = 0.0347), for VASloudness off-stimulation in favor of G1 ( p = 0.0166)and G3 ( p = 0.0330) and for VAS annoyance off-stimulation in favor of G3 ( p = 0.0233).
3.1.5. EEG analysis
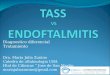
Source montage analysis of whole-head EEG mea-surements revealed a signicant decrease of bandpower and increase of band power in the primaryauditory cortex of G1 ( p < 0.01) while no signicantchanges in G5 (placebo) were observed ( p = 0.89,Fig. 2e, Table 2). Additionally, we determined 3Dmaps of signicant changes of oscillatory brain activ-ity, usingthe sLORETA technique,in typical frequencybands in 12 patients with bilateral tinnitus takenfrom the stimulation groups G1G4 (see Methods).Reduced levels of band power were signicantlyincreased after 12 weeks of treatment (red voxels, p < 0.05, Fig. 3): the widespread bilateral increasewas strongest in temporal regions and the entire pre-frontal cortex (Fig. 3 and Table 3). Tinnitus-associatedenhanced and activity was signicantly reducedin a widespread network comprising auditory andnon-auditory areas (blue voxels, p < 0.05, Fig. 3): activity was decreased mainly in temporal and pre-frontal regions including the primary and secondaryauditorycortices. activitywassignicantly decreasedin frontal regions and the anterior cingulate area(Brodmann Area (BA) 32). A signicant decrease in
activity was observed in temporal areas, thereinmaximal in the superior temporal gyrus (bilateral,BA 41, 42). low activity, i.e. activity of low fre-quency (see Methods), was signicantly decreased inthe temporal and frontal cortex covering wider areasin the right prefrontal cortex, while high showeda left-centered signicant decrease in the temporalcortex (maximal in the superior temporal gyrus, BA41). All results are displayed in Fig. 3 (red voxels, p < 0.05), corresponding Brodmann areas are listed inTable 3.
3.1.6. Long-term extension
In LTE (all subjects receiving CR neuromodulationlike in G1; 58 subjects started, 52 subjects completedLTE) already gained treatment effects were sustainedor even improved further. The overall improvementin TQ was 36% ( p < 0.0001 t -test, compared to base-line). Using the responder analysis by Goebel et al.(2006) we found at the end of 40 weeks 40% win-ners (TQ improvement 15 points), 35% responders(TQ improvement 614 points), 23% non-responders(TQ unchanged 5 points) and 2% losers (TQ wors-ening 6 points).
3.1.7. Safety
15 AEs occurred in total: 13 AEs during blindedphase, 2 AEs in LTE. Two SAEs (an abdominal preg-nancy and avascular necrosis of the femoral head, notassociated with treatment) were reported. All otherAEs were of mild to moderate intensity and nonewas permanent. 8 AEs were judged to be treatmentrelated of which 3 AEs were associated with a tran-sient increase of tinnitus loudness; all three patientscontinued treatment into the LTE.
4. Discussion
4.1. Clinical effects
We showed that acoustic CR neuromodulation wassafe and well-tolerated. We found a signicant andclinically relevant concordant strong decrease of VASscores (loudness and annoyance), TQ scores and TQseverity levels. Improvements persisted a preplanned4-week therapy pause on a slightly reduced, but sig-
nicant level, regaining the reduction in VAS aftercontinuation of the CR therapy and showing sustainedlong-termeffects during theLTE.At theendof LTE(at40 weeks) we observed 75% winners and responderswith a mean TQ reduction of 50%. A similar reductionof tinnitus distress, i.e. 70% of winners/responders inTQ after 6 months of acoustic CR neuromodulation,was shown in a cohort of seventy real life patientssuffering from chronic tonal tinnitus in an outpatientsetting (TRI Tinnitus Conference 2011, Buffalo, USA,Abstract H. Wurzer). In contrast, when treated with
8/11/2019 Tass Et Al_RNN 2012_Counteracting Tinnitus by Acoustic CR Neuromodulation
12/23
148 P.A. Tass et al. / Counteracting tinnitus by acoustic coordinated reset neuromodulation
Fig. 3. Electrophysiological effects of acoustic CR neuromodulation assessed in the framework of the RESET study. 3D mapping of treatmentinduced changes in oscillatory EEG activity (baseline compared to 12 weeks, off-stimulation). To increase signal-to-noise ratio 12 patientswith bilateral tinnitus (from G1 to G4) were selected using reliable-change-index (RCI) applied to improvements of TQ scores. Statisticalnon-parametric maps from sLORETA (Pascual-Marqui, 2002) for the localization of changes of , , , , low and high current source densityare given. Results are superimposed onto a three-dimensional brain (rst three columns) and onto a horizontal brain section (right column)of a standard anatomical template. Signicantly decreased activity after acoustic CR neuromodulation compared to baseline is labeled blue,increased activity is labeled red (corrected, p < 0.05).
noisers and maskers only a minority of patients experi-ences tinnitus-suppressing after-effects, and these lastonly seconds to minutes (Surr et al., 1985; Roberts etal., 2010). Comparing the active arms, CR therapy was
more efcaciouswhenused 46 h/d compared to 1 h/d,and the results of noisy CR neuromodulation (G2)were less efcacious and importantly lacked a last-ing offstimulation effect resembling the typical short
8/11/2019 Tass Et Al_RNN 2012_Counteracting Tinnitus by Acoustic CR Neuromodulation
13/23
P.A. Tass et al. / Counteracting tinnitus by acoustic coordinated reset neuromodulation 149
Table 3Signicant effects of acoustic CR neuromodulation on the EEG activity (baseline compared to 12 week follow up). The Brodmann areas wheresignicant changes were observed are listed. Arrows indicate the effect of the treatment ( : decrease, : increase, corrected, p < 0.05). Changes
were localized using statistical non-parametric maps from sLORETA (Pascual-Marqui, 2002)
Band Frequency Effect Positionrange Left Bilateral Right
14Hz Prefrontal 46, 47 Postcentral 1, 2; Precentral 4 Parietal 40Orbilo frontal 11 Prefrontal 6, 8, 9, 10; Insula 13Frontal 44 Occipital 18, 19; Fusiform 20
Temporal 21, 22, 28, 37, 38, 39, 41, 42Cingulate cortex 23, 31, 29Parahippocampus 30, 36Subcentral 43; Frontal 45
48Hz Prefrontal 47 Prefrontal 9, 10; Orbitofrontal 11
Temporal 38 Anterior cingulate 32 812 Hz Postcentral 1, 2, 3; Precentral 4
Prefrontal 6, 8, 9, 10, 46; Parietal 7;Orbitofrontal 11, 47; Insula 13Occipital 17, 18, 19; Fusiform 20Temporal 21, 22, 28, 34, 35, 37, 38, 39, 41, 42Posterior cingulate 23, 31Anterior cingulate 24, 32, 33Frontal 25, 44, 45; Piriform 27Cingulate cortex 29; Parahippocampus 30, 36Parietal 40; Subcentral 43
1230 Hz Parietal 39 Postcentral 2; Parietal 40 Prefrontal 10Temporal 37 Frontal 47; Fusiform 20 Orbitofrontal 11Occipital 18, 19 Temporal 21, 22, 41, 42
low 3048 Hz Piriform 27 Postcentral 1, 2; Precentral 4 Occipital 17, 18
Parahimpocampus Prefrontal 6, 8, 9, 10, 46, 47; Orbitofrontal 11 Temporal 2830 Insula 13; Fusiform 20 Parietal 40
Temporal 21, 22, 35, 37, 41Parahimpocampus 36; Frontal 44, 45, 47
high 5290 Hz Precentral 4 Insula 1 3 Postcentral 1,2Prefrontal 9 Temporal 21, 22, 41, 42 Temporal 20Frontal 45, 47 Subcentral 43, 44 Parietal 40Occipital 19
term effects of noisers or maskers (Terry et al., 1983).In contrast,placebo treatmentshowedlimited andnon-signicantchangesfor VASscores andTQ,whichwerein the range of previously reported effects of inpa-tient treatment including cognitive behavioral therapy(CBT, Goebelet al., 2006).Thiscouldbe indicativeofatrueplacebo effect in ourstudy; oftentimes instead of placebo groups waiting list control groups are usedthat sometimes improve slightly on tinnitus specicmeasurements (Hesser et al., 2011) but studies havealso shown no changeor even worseningof thewaitinglist control group over time (Cafer et al., 2006).
The placebo group tended to be older and had alonger lasting tinnitus with lower VAS and TQ scoresat baseline. However, tinnitus patients with a longertinnitus duration (>4 years)beneted in the same order
of magnitude as patients with shorter tinnitus duration(
8/11/2019 Tass Et Al_RNN 2012_Counteracting Tinnitus by Acoustic CR Neuromodulation
14/23
150 P.A. Tass et al. / Counteracting tinnitus by acoustic coordinated reset neuromodulation
Table 4Comparison of the pooled groups Gl & G3 ( n = 34, with 46hours/day acoustic CR Neuromodulation, effective treatment groups) and G2, G4& G5 (n = 29, ineffective treatment groups). The change from baseline to end of treatment phase (12 week follow up) and after the 4 weeks
treatment pause (16 week follow up) in primary efcacy outcomes
Pooled-groups G1 & G3 ( n = 34) G2, G4 & G5 ( n = 29)Follow-up (week) 12 16 12 16VAS Loudness
Change from baseline (off-stimulation) [mean (SD)] 23.2 (21.2) 17.5 (23.9) 5.2 (18.3) 2.1 (19.6) p value (change from baseline ## )
8/11/2019 Tass Et Al_RNN 2012_Counteracting Tinnitus by Acoustic CR Neuromodulation
15/23
P.A. Tass et al. / Counteracting tinnitus by acoustic coordinated reset neuromodulation 151
ness (Dohrmann et al., 2007b). The other strategy of reducing the intensity of the tinnitus and to observewhether concomitant changesoccurin theelectrophys-iological activity was carried out in this study withacoustic CR neuromodulation.
The EEG pattern of our patients prior to treatmentresembles previous ndings by Weisz et al. (2005a)who showed a marked reduction of along with anenhancement of frequency power in tinnitus patientsparticularly in temporal regions. In our study we addi-tionally found reduction and enhancement inassociative and limbic areas (prefrontal and cingu-late). Functional connectivity of these areas has beendescribedas basis for impairment andmany secondarytinnitus symptoms (Llin as et al., 1999; Tyler, 2006;Schlee et al., 2009b; Moazami-Goudarzi et al., 2010;Rauschecker et al., 2010). These ndings are in linewith the notion of Llin as et al. (1999) and Jeanmonodet al. (1996), that clinical symptoms, e.g., neurogenicpain, tinnitus, abnormal movements, epilepsy and cer-tain neuropsychiatric disorders, are associated withlow frequency rhythmic bursting activity.
Neuromagnetic changes caused by maskers inchronic tinnitus sufferers (Kahlbrock and Weisz,2008) showed a decrease of slow-wave spontaneous
brain activity from pre- to post-stimulation caused byresidual inhibition(RI), i.e.a suppression of pathologicneuronal activity. The corresponding suppression of tinnitus extends only seconds or minutes beyond theduration of the direct stimulation. In contrast, acousticCR neuromodulation decreases the slow-wave ( )activity by desynchronization leading to long-lastingtherapy induced changes of spontaneous EEG activityafter 12 weeks of therapy measured in the off-state,namely a reduction and enhancement, indicativeof neuroplastic changes by acoustic neuromodulation,modifying the neuronal correlates of tinnitus in theseareas in our patients (Weisz et al., 2005a; Dohrmannet al., 2007a). So we here focus the outcome measureson assessing the impact of the treatment based on theneurophysiological pathway of tinnitus as suggestedby the Cochrane collaboration (Martinez-Devesa etal., 2010).
4.3. Long-lasting therapy induced changes
In our study thedecrease of tinnitus frequency, EEGchanges and persistence of clinical improvement dur-ing the 4-week therapy pause (instead of completewash-out) mightbe indicative of neuroplastic changes.
In computational studies it was shown that CR neuro-modulation induces a long-lasting desynchronizationmediated by an unlearning of synaptic connectiv-ity (Tass and Majtanik, 2006; Hauptmann and Tass,2007; Tassand Hauptmann, 2009; Tassand Popovych,2012). The EEG changes and the persistence of clin-ical improvement during the 4-week therapy pauseobserved in our study are in accordance to the predic-tions of these computational studies. However, giventhe results presented here, we cannot prove that in thetinnitus patients CR works as shown computationally,i.e. by means of a sequential phase reset of neuronalsub-populations (Tass, 2003). Accordingly, in a forth-coming EEG study we shall investigate whether and, if so, in which cortical areas single tones induce a phasereset of pathological rhythms, whereas CR stimuli (i.e.time-shifted sequences of phase resetting tones) causea desynchronization (i.e. a decrease of the power inpathological frequency bands).
This forthcoming study might be helpful to furtherreveal the mechanism underlying our therapy.
Based on the data presented here, we cannot rule outthat a qualitatively different mode of action might leadto the observed long-lasting clinical and electrophysi-ological changes.
In fact, the acoustic stimulation delivered to ourpatients might have primarily changed the synap-tic connectivity which, in turn, might have caused adecrease of neuronal synchronization. Also, the mech-anism underlying residual inhibition (RI, Feldmann,1971; Hazell and Wood, 1981; Terry et al., 1983) is notyetunderstood. Long-lastingRI,observede.g. after15-minmasking periods,occursonly in a small percentageof patients (Hazell and Wood, 1981). Accordingly, thesignicant off-stimulation effects outlasting the treat-ment pause of four weeks which were observed in G1can hardly be explained by a RI-related mechanism.Mechanisms primarily employing lateral inhibitionand, hence, a suppression of the tinnitus-related neu-ronal synchronization cannot be ruled out based onthe results presented here. However, such a mech-anism would be in contradiction to computationalresults showing that blocking/inhibitory stimulationcannot induce an unlearning of synaptic connectiv-ity, since the latter requires neurons to be active (Tassand Majtanik, 2006; Hauptmann and Tass, 2007; Tassand Hauptmann, 2009; Tass and Popovych, 2012).A phenomenon that might be related to this issue iswell-known from electrical deep brain stimulation inParkinsons disease (PD). High-frequency electrical
8/11/2019 Tass Et Al_RNN 2012_Counteracting Tinnitus by Acoustic CR Neuromodulation
16/23
152 P.A. Tass et al. / Counteracting tinnitus by acoustic coordinated reset neuromodulation
deep brain stimulation (Benabid et al., 1991) has nolong-lasting clinical effects: PD symptoms reappearafter cessation of stimulation (Temperli et al., 2003).Analogously, PD-related oscillatory band activity,suppressed during stimulation, reemerges after cessa-tion of stimulation within seconds (K uhn et al., 2008).
Another remarkable phenomenon is the tinnituspitch change. This phenomenon hasnotbeen predictedby our computational studies. In fact, the underlyingphysiological mechanism of the CR-induced tinnituspitch change still remains open. Taking into accountthe tonotopic organization of the primary auditory cor-tex, a CR-induced tinnitus pitch change may likelycorrespond to a spatial shift of the tinnitus-relatedfocus of synchronized neuronal activity within the pri-mary auditory cortex. Based on the dynamical modeof action of CR neuromodulation (Tass, 2003; Tassand Majtanik, 2006; Hauptmann et al., 2007; Tass andHauptmann, 2009; Tass and Popovych, 2012) such aneffect might be caused by asymmetries of both thestimulation and the network subjected to stimulation:(i) In a modeling study (Franosch et al., 2003) on theemergence of the Zwicker tone (Zwicker, 1964), i.e.an auditory after effect, the impact of a spatial gradientof the lateral inhibition in the auditory cortex on the
neuronal dynamics in the central auditory cortex hasbeen analyzed. It turned out that a gradient of the lat-eral inhibition has signicant impact on the neuronaldynamics. In particular, a noise reduction mechanismcombined with a dominantly unilateral inhibition isable to explain the emergence of the Zwicker tone(Franosch et al., 2003). Such a gradient of the lat-eral inhibition combined with a spatially equidistantdeliveryof acoustic stimuli might bea candidatemech-anism causing a spatial shift of the synchronous focusin the primary auditory cortex. (ii) In case of a spatiallywell-balanced lateral inhibition asymmetries of thealignmentof theCR tones (with respect to thepatientsindividual tonotopic organization of the primary audi-tory cortex) might also spatially shift the synchronousfocus in the primary auditory cortex. Possible mech-anisms underlying the shift of the tinnitus frequencywill be in the focus of forthcoming theoretical andexperimental studies.
4.4. Comparison with other therapeuticapproaches
Vagusnervestimulation (VNS)combined with mul-tiple tone pairing an invasive therapy tested so far in
animals aims at counteracting tinnitus by controllingmap plasticity (Engineer et al., 2011).Another invasiveapproach to suppresssynchronized
hyperactivity associated with tinnitus has been carriedout by De Ridder and his group (De Ridder et al.,2007):aftera complex diagnostic procedurewith fMRIand neuronavigation-guided trans-magnetic stimula-tion (TMS) patients responding to TMS received viacraniotomy the insertion of an epidurally xed octopo-lar electrode and consequent bipolar stimulation bymeans of a pulse generator. A reduction of tinnitusloudness measured by a VAS scale occurred in tonaltinnitus whereas in atonal tinnitus the technique failedto show signicant results. After a while, tinnitus reoc-curred inall patientsandreorganizationof theelectrodearray was necessary (De Ridder et al., 2006).
Based on initial animal studies tinnitus is proposedto be an auditory phantom phenomenon associatedwith a synchronized hyperactivity and reorganizationof the two auditory pathways (lemniscal and extralem-niscal) all the way up to the auditory cortex (Moller,2007).
The correlation between tinnitus strength and theamount of reorganization of the primary cortex foundin earlier study (M uhlnickel et al., 1998) was not repli-
cated or weakened in subsequent studies (Weisz et al.,2005a; Yang et al., 2011).
In a previous study tailor-made notched music (i.e.music with a frequency band of one octave width cen-teredat the individual tinnitus frequencyremovedfromthe music energy spectrum via digital notch lter)was used to counteract tinnitus-related auditory cortexreorganization. The presumed mechanism here is inhi-bition of tinnitus-related activity mediated by lateralinhibition (Okamoto et al., 2010). For the placebogroup a moving notch lter of one octave around thetinnitus frequency was applied. A third group didntreceive any music treatment at all and served as acontrol group.
In this study patients with very mild to mild tinnitusdistress were enrolled (TQ 18.4 10.8; scale 084).Both, the active group ( n = 8) listening to tailor-madenotched music and the control group ( n = 7) withoutany music treatment showed after 6 months improve-ments in loudness (measured by a VAS scale, 0100).On the other hand, the placebo group ( n = 8) usinga moving notch lter showed worsening of the per-ception of tinnitus loudness which might be explainedby a tinnitus worsening effect of the moving notch l-ter technique itself. This observed deterioration of the
8/11/2019 Tass Et Al_RNN 2012_Counteracting Tinnitus by Acoustic CR Neuromodulation
17/23
P.A. Tass et al. / Counteracting tinnitus by acoustic coordinated reset neuromodulation 153
placebo group contrasts with the improvements of theplacebo group described here in RESET and contra-dicts also latest pharmacological studies in the eldof tinnitus like the Neramexane trial (Suckf ull et al.,2011) where also a pronounced placebo effect wasnotable.
In contrast, the CR approach strictly avoids inhi-bition of pathologically synchronized activity (Tassand Majtanik, 2006; Hauptmann and Tass, 2007; Tassand Hauptmann, 2009). As shown computationally, ingeneral, inhibitory stimulation is unfavorable for anti-kindling, since inactive neurons are unable to unlearn(Tass and Majtanik, 2006; Hauptmann and Tass, 2007;Tass and Hauptmann, 2009). However, CR robustlyworks even if only inhibitory synapses are stimulated(Hauptmann and Tass, 2007; Tass and Hauptmann,2009), because a phase reset can be achieved byboth excitatory and inhibitory stimuli (Winfree, 1977;Guttman et al., 1980).
Optimal desynchronizing CR effects require mutu-ally sufciently distant stimulation sites (herefrequencies) (Tass, 2003; Lysyansky et al., 2011).As yet, there is no neuroimaging or electrophysio-logical technique available which enables to assessthe spatial extent of the synchronized focus in tinni-
tus patients. Psychoacoustic measurements of tinnitusspectra revealed that broad frequency ranges, largelycorresponding to ranges with abnormally elevatedhearing thresholds, contribute to the patients tinnitussensations (Norena et al., 2002). The correspondingcentral auditory neurons, deprived of afferent input,were supposed to be engaged in the pathological,tinnitus-related neuronal activity (Norena et al., 2002).Accordingly, based on results from theoretical studies(Tass, 2003; Tass and Hauptmann, 2009; Lysyanskyet al., 2011) we derived rules for choosing pitch andamplitude of the desynchronizing CR tones: Ideallythe CR stimuli should be conned to the synchronizedfocus. However, CR is still (but less) effective if oneor two stimulation sites are misplaced, e.g. becausethey are located outside the synchronized focus. Mostimportantly, a dense spacing of the stimulation sitesplaces the desynchronizing effect in jeopardy. In fact,for sufciently dense spacing of the stimulation sitesthe effect of CR stimulation nally approaches thesynchronizing effect of a spatially homogenous stimu-lation that is periodic in time (Tass and Hauptmann,2009). Accordingly, given the spatial prole of thetuning curves, especially in patients with impairedhearing, a spatially selective stimulation requires the
CR tones to be sufciently spaced, equally loud and just super-threshold (see Methods). Accordingly, themasking effect in G2 suggests that due to a relevantportion of stimulation cycles with neighboring tonesthe noisy CR in G2 suppresses the tinnitus-relatedneuronal activity via lateral inhibition. The signicantdifference of the long-lasting, cumulative and long-term effects in G1/G3 vs. the masking effects in G2indicate that the therapeutic outcome might be opti-mized by further adapting the arrangement of the CRfrequencies to the individual tonotopy and the dimen-sions of the pathological synchronized activity in theprimary auditory cortex. Also, a closermeshedadapta-tion of therepetition rate F to the intrinsically varyingpeakfrequencymightpossibly improve the therapeuticoutcome.
4.5. Neuronal synchronization
Tinnitus animal research mainly focuses on neu-ral correlates of short-term tinnitus. In several studiesit was shown that noise trauma causes an immediateincreaseof neuronal cross-correlation, whichmay evenprecede theincreaseof theringrates (Ochi andEgger-mont, 1997; Norena and Eggermont, 2003; Seki andEggermont, 2003). For several reasons comparison toresults obtained in humans with MEG, EEG or LFPmeasurements has to be drawn carefully:
(i) Human EEG, MEG and LFP studies have typ-ically been performed in patients with chronictinnitus (see Weisz et al., 2005a; Weisz et al.,2007). In analogy to animal studies, in onehuman study a rapid increase of neuronal syn-chronization, in terms of a rapid increase of power in the auditory cortex, following noisetrauma was observed (Ortmann et al., 2011).
(ii) In tinnitus animal experiments and in humanstudies neuronal dynamics is studied on dif-ferent scales. While in tinnitus animal studiestypically neuronal spikes or bursts are ana-lyzed (Eggermont, 1992; Ochi and Eggermont,1997), in human studies LFP, scalp EEG andMEG oscillations are investigated, which areconsidered to be generated by oscillations of neocortical postsynaptic potentials (Klaas andDaly, 1979; Nunez, 1981; H amalainen et al.,1993; Niedermeyer and Lopes da Silva, 1999).
(iii) In this paper the term neuronal synchroniza-tion stands for coincident ring in a large
8/11/2019 Tass Et Al_RNN 2012_Counteracting Tinnitus by Acoustic CR Neuromodulation
18/23
154 P.A. Tass et al. / Counteracting tinnitus by acoustic coordinated reset neuromodulation
population of neurons. This type of synchro-nization leadsto large-amplitudeoscillationsasdetected by LFP, EEG, and MEG signals, typi-cally in particular frequency ranges (see Klaasand Daly, 1979; Nunez, 1981; H amalainenet al., 1993; Niedermeyer and Lopes da Silva,1999). In contrast, cross correlation analysis istypically performed for singleunit and/or multiunit data (Eggermont, 1992; Ochi and Egger-mont, 1997). Qualitatively different types of collective synchronization patterns may leadto large-amplitude LFP, EEG and MEG oscil-lations, see e.g. (Popovych and Tass, 2011).However, fundamental dynamical phenomena,such as collective coincident ring, can bedetected with different synchronization andcross correlation measures, for review see(Quiroga et al., 2002).
4.6. Mechanisms of CR neuromodulation at thecortical level
The auditory pathway has a complex, hierarchi-cal tonotopic organization (Ehret and Romand, 1997).Based on the results presented here, we can hypothe-size about how acoustic CR neuromodulation actuallyworks at the cortical level. Based on previous, inparticular computational studies, CR might cause adesynchronization of cortical neuronal populations inqualitatively different ways:
(i) Stimuli can effectively induce a phase reset nomatter whether they act on neurons directly(as e.g., electrical pulses delivered to the neu-ronal membrane) or indirectly (i.e. transmittedvia synapses) (Popovych and Tass, 2012; Tassand Popovych, 2012). Due to the tonotopicorganization of the central auditory system,these phase resets may, hence, occur at dif-ferent sites. The spatial spread of the differentstimuli crucially depends on the characteristicsof the tuning curves of auditory nerve bers,which may, e.g., be pathologically broadenedin patients with cochlear hearing loss (Wight-man et al., 1977; Ryan et al., 1979; Libermanand Dodds 1984; Pickles, 1984). However,it has computationally been shown that CRneuromodulation is quite robust with respectto variations of the spatial spread (Lysyanskyet al., 2011). So, in principle, acoustic CR
neuromodulation might induce a desynchro-nization of the rhythm at the cortical levelby inducing phase resets of the rhythm in dif-ferent cortical subpopulationsat different times.Fora discussion of phase resetsof ongoing brainrhythms we refer to (Klimesch et al., 2006).
(ii) However,desynchronization at the cortical levelmight also be induced by CR in a qualita-tivelydifferentway. Thetypical CRmechanism,desynchronization via time-shifted phase resetsof neuronal subpopulations (Tass, 2003), mighttake place at an upstream nucleus in the centralauditory system. From computational stud-ies it is known, that desynchronizing effectspropagate between neuronal populations: Thishas been shown for qualitatively different(single-site vs. multi-site) stimulation tech-niques and, in particular, for different topologiesof the connectivity (Hauptmann et al., 2005;Popovych et al., 2006; Popovych and Tass,2010). Remarkably, desynchronizing effects donot only propagate between neuronal popula-tions in case of a connectivity pattern with aGaussian connection probability (Hauptmannetal.,2005),butevenwithameaneldcoupling,
i.e. a connectivity pattern where each neuron of one of the populations is coupled to all neuronsof the other population with equal strength in a uni-directional or even bi-directional set-up (Popovych et al., 2006; Popovych and Tass,2010). These results indicate that the propa-gation of desynchronizing effects might be arobust mechanism which does not depend onthe type of thestimulation techniquecausing thedesynchronization in an upstream population.Mechanism (ii) might be particularly relevantfor the propagation of desynchronizing effectsfrom auditory to non-auditory areas, since itdoes not require a tonotopic organization of theconnections.
In other words, the desynchronization at the level of the primary auditory cortex might be induced by thegenuine CR mechanism, time-shifted phase resets of neuronal subpopulations (Tass, 2003), or by a prop-agation of desynchronizing effects from an upstreamnucleus of thecentral auditory system. In the lattercasethegenuine CR mechanismtakes place in theupstreamnucleus. From a theoretical standpoint, combinationsof mechanisms (i) and (ii) might also be conceivable.
8/11/2019 Tass Et Al_RNN 2012_Counteracting Tinnitus by Acoustic CR Neuromodulation
19/23
P.A. Tass et al. / Counteracting tinnitus by acoustic coordinated reset neuromodulation 155
To study the dynamical mechanism of acoustic CRneuromodulation in tinnitus patients in more detail, ina forthcoming EEG study we shall analyze in whichauditory and non-auditory brain areas single tonescause a phase reset of pathological rhythms (e.g. )and CR stimuli (i.e. time-shifted sequences of phaseresetting tones) cause a desynchronization.
4.7. Pathophysiology of tinnitus
One limitation of the pioneering MEG study byWeisz and coworkers (2005a), revealing pathologi-cally enhanced and decreased in tinnitus patients,was that contrary to the normal hearing control groupthe tinnitus group had a high-frequency hearing loss.Since the brain regions with increased power werealso the regions of decreased power, the results byWeisz et al. (2005a) are similar to ndings obtainedduring slow-wave sleep (Benoit et al., 2000). Accord-ingly, Weisz et al. (2005a) could not rule out that thechanges in spontaneous brain activity might simplybe due to sensory deprivation, in terms of the high-frequency hearing loss, rather than being specic fortinnitus. In contrast, our EEG results were obtained inone group of patients with tinnitus and after signi-
cant CR induced tinnitus relief and having the samehearing levels before and after therapy. Accordingly,our study does not feature the limitation of a non-matched hearing loss between comparison groups and,hence, substantially conrms the ndings by Weisz etal. (2005a), in accordance, e.g., with the neurofeed-back (Dohrmann et al., 2007a) and residual inhibition(Kahlbrockand Weisz,2008) studies. Hyperacusis anddepression were not assessed in our RESET study.
4.8. Limitation of the RESET trial
The RESET trial is an exploratory rst in man trialand not a fully powered trial. It serves the purposeto collect safety information as well as efcacy datafor different doses of acoustic CR. Therefore severalshortcomings of the trial have to be taken into account:no conrmatory statistical approach was used but sev-eral efcacy endpoints common in tinnitus researchwere investigated with statistics of exploratory nature.EEG recordings were used as biomarkers to explorethe effects of acoustic CR on different brain regions.Randomization was done using computer randomcodes. By chance and small group effect the allo-cation of patients to the placebo group (G5) showed
signicant differences in baseline scores concerningseveral importantparameters. Thesmall groupsizeandthebaseline difference of theplacebo group is clearly aweakpointofthetrial.Themainpurposeofourplacebogroup was to have stimulation tones, that where suf-ciently remote from the tinnitus frequency. This wasmotivated by few case studies of acoustic CR treat-ment performed prior to the start of the RESET trial.In these cases we observed that shifting all CR tonesby around 50% to either side of the tinnitus frequencyandapplied for severalhours perdaymayhave adverseeffects (e.g. transient headache, transient increase of tinnitus loudness and annoyance). For this reason, toavoid side effects but nevertheless perform acousticstimulation resembling therapeutic stimulation, in theplacebo group we delivered CR tones far away fromthe range of tinnitus frequency for one hour per dayonly. Dosage based un-blinding of the placebo groupwas prevented byanactive stimulation group (G4) withsimilar dosage (one hour per day).
Another important aspect in the context of un-blinding is the on-stimulation effect. Remarkably,in accordance with our theoretical predictions (Tassand Hauptmann, 2009) the stimulation in G2 hason-stimulation effects, but no off-stimulation effects
(pseudo placebo).However, additional analyses provide further evi-
dence for the effectiveness of the CR treatment.Concerning the differentbaseline characteristicsof theplacebo group, on the one hand we showed that treat-ment success did not correlate with tinnitus duration,tinnitus severity or age. On the other hand, subgroupsof G1 matched to the placebo group with respect tosize andtinnitus severitywere compared to theplacebogroup. We found a substantially greater improvementin G1 subgroups as compared to G5. Furthermore, toperform a statistical comparison between two groupswith comparable sizes, we pooled two big groups:The effective stimulation group G1 + G3 ( n =34,46 h/day CR neuromodulation) was compared withthe ineffective stimulation group comprising all dataof G2 (noisy stimulation with a masking effect butwithout lasting off-effect), G4 (only 1 h of CR neu-romodulation per day leading to small improvementsonly) and G5 (the placebo group) with n = 29 patients.Although the ineffective stimulation group showedsignicant results compared to baseline concerningVAS loudness and annoyance in the ON conditionas well as TQ, the effective stimulation group wassignicantly better than the ineffective stimulation
8/11/2019 Tass Et Al_RNN 2012_Counteracting Tinnitus by Acoustic CR Neuromodulation
20/23
156 P.A. Tass et al. / Counteracting tinnitus by acoustic coordinated reset neuromodulation
group with respect to VAS loudness on/off after 12and 16 weeks, VAS annoyance on/off after 12 weeks,and TQ after 12 weeks. These results are accompa-nied by a pronounced shift in tinnitus frequency in thepooled CR neuromodulation group (G1+ G3). Finally,we performed a comparison between all groups andthe active control group G2, the masker-like noisy CRgroup, which showed a good on-effect without last-ing off-effect. G1 and G3, both groups with 46h/dayof CR neuromodulation turned out to reveal signi-cantly better results than the masker like group G2.Still the exploratory data from the RESET trial servenow for the start of a fully powered prospective mul-ticenter double blind placebo controlled randomizedtrial (RESET 2) that will randomize 100 patientswith chronic tonal tinnitus either to pseudo placeboor acoustic CR.
Patients proted differently from the CR neuro-modulation. In future studies, we aim to elucidate theinuence of clinical or/andEEG variables prior to ther-apy on the therapy success.
Overall, our study strongly supports the pivotalrole of pathological synchrony in tinnitus generation(Llin as et al., 1999; Weisz et al., 2005a; Dohrmannet al., 2007a; Kahlbrock and Weisz, 2008; van der
Loo et al., 2009; Moazami-Goudarzi et al., 2010), assuggested, e.g., in the context of thalamocortical dys-rhythmia (Llin as et al., 1999). Along with the resultsof the experimental studies of our group this approachmay therefore open novel therapeutic and neuroscien-tic avenues.
Acknowledgments
We are grateful to Drs. N. Pasch, H. Hermes, D.Jurgens, J. Alberty, G. Kr uckels, W. Sch utz, and S.Schutz for contributions to patient selection. We grate-fully acknowledge discussions with Dr. OleksandrPopovych and Dr. Timea T oth. The RESET study wasfunded by Research Center J ulich and ANM AdaptiveNeuromodulation GmbH.
Conict of interest
Dr. Peter Tass and Dr. Christian Hauptmann have acontractual relationship with ANM Adaptive Neuro-modulation GmbH, the sponsor of the clinical trial.Dr. Peter Tass and Dr. Hans-Joachim Freund are
holding shares of ANM Adaptive NeuromodulationGmbH.
References
Benabid, A.L., Pollak, P., Gervason, C., Hoffmann, D., Gao,D.M., Hommel, M., Perret, J.E. & de Rougemount, J. (1991).Longterm suppression of tremor by chronic stimulation of ven-tral intermediate thalamic nucleus. The Lancet , 337 , 403-406.
Benoit, O., Daurat, A. & Prado, J. (2000). Slow (0.72 Hz) and fast(24 Hz) delta components are differently correlated to theta,alpha and beta frequency bands during NREM sleep. Clin Neu-rophysiol , 111 , 2103-2106.
Cafer, P., Haupt, H., Scherer, H. & Mazurek, B. (2006). Outcomesof long-term outpatient tinnitus-coping therapy: psychometricchanges and value of tinnitus-control instruments. Ear Hear ,27 , 619-627.
Chen, R., Classen, J., Gerloff, C., Celnik, P., Wassermann, E.M.,Hallett, M. & Cohen, L.G. (1997). Depression of motor cortexexcitability by low-frequency transcranial magnetic stimula-tion. Neurology , 48 , 1398-1403.
De Ridder, D., Verstraeten, E., Van der Kelen, K., De Mulder, G.,Sunaert, S., Verlooy, J., Van de Heyning, P. & Moller, A.R.(2005). Transcranial magnetic stimulation for tinnitus: Inu-ence of tinnitus duration on stimulation parameter choice andmaximal tinnitus suppression. Otol Neurootol , 26 , 616-619.
De Ridder, D., De Mulder, G., Verstraeten, E., Van der Kelen, K.,Sunaert, S., Smits, M., Kovacs, S., Verlooy, J., Van de Heyning,P. & Moller, A.R. (2006). Primary and secondary auditory cor-texstimulationfor intractable tinnitus. ORL J Otorhinolaryngol Relat Spec , 68 , 48-55.
De Ridder, D., De Mulder, G., Menovsky, T., Sunaert, S. & Kovacs,S. (2007). Electrical stimulation of auditoryandsomatosensorycortices for treatment of tinnitus and pain. Prog Brain Res ,166 (36), 377-388.
De Ridder, D., Van der Loo, E., Vanneste, S., Gais, S., Plazier,M., Kovacs, S., Menovsky, T. & Van de Heyning, P. (2011).Theta-gamma dysrhythmia and auditory phantom perception. J Neurosurg , 114 (4), 912-921.
De Ridder, D. & Vanneste, S. (2011). Auditory Cortex Stimulationfor Tinnitus. In: Moller, A.R., Langguth, B., De Ridder, D. &
Kleinjung, T.(Eds.),Textbook of Tinnitus, Springer, NewYork,717-726.
Dietrich,V., Nieschalk, M.,Stoll, W., Rajan,R. & Pantev, C. (2001).Cortical reorganizationin patientswith highfrequencycochlearhearing loss. Hear Res , 158 , 95-101.
Dohrmann, K., Elbert, T., Schlee, W. & Weisz, N. (2007a). Tun-ing the tinnitus percept by modication of synchronous brainactivity. Restor Neurol Neurosci , 25, 371-378.
Dohrmann, K., Weisz, N., Schlee, W., Hartmann, T. & Elbert, T.(2007b). Neurofeedback for treating tinnitus. Prog Brain Res ,166 , 473-485.
Eggermont, J.J. (1992). Neural interaction in cat primary auditorycortex. Dependence on recording depth, electrode separation,and age. J Neurophysiol , 68, 1216-1228.
8/11/2019 Tass Et Al_RNN 2012_Counteracting Tinnitus by Acoustic CR Neuromodulation
21/23
P.A. Tass et al. / Counteracting tinnitus by acoustic coordinated reset neuromodulation 157
Eggermont, J.J. (2003). Central tinnitus. Auris Nasus Larynx , 30 ,7-12.
Eggermont, J.J.& Robert, L.E. (2004). Theneuroscience of tinnitus.Trends Neurosci , 27 , 676-682.
Ehret, G. & Romand, R. (1997). (Eds.), Thecentral auditory system,Oxford University Press, Oxford.
Elbert, T., Rockstroh, B., Kowalik, Z.J. & Hoke, M. (1997). Clinicalapplications of EEG analyses using tools derived from non-linear system theory. In: Angelieri, F., Butler, S.R., Giaquinto,S. & Majkowski, J. (Eds.), Analysis of the electrical activity of the brain, Wiley and Sons, London.
Engineer, N.D., Riley, J.R., Seale, J.D., Vrana, W.A., Shetake, J.A.,Sudanagunta, S.P., Borland, M.S. & Kilgard, M.P. (2011).Reversing pathological neural activity using targeted plasticity.
Nature , 470 , 101-104.Feldmann, H. (1971). Homolateral and contralateral masking of
tinnitus by noise-bands and pure tones. Audiol (Basel) , 10,138-144.
Frank, G., Kleinjung, T., Landgrebe, M., Vielsmeier, V., Steffen-hagen, C., Burger, J., Frank, E., Vollberg, G., Hajak, G. &Langguth, B. (2010).Left temporallow-frequencyrTMS for thetreatment of tinnitus: Clinical predictors of treatment outcome a retrospective study. Eur J Neurol , 17 , 951-956.
Franosch, J.M., Kempter, R., Fastl, H. & Van Hemmen, J.L. (2003).Zwicker tone illusion and noise reduction in the auditory sys-tem. Phys Rev Lett , 90 , 178103.
Gerstner, W., Kempter, R., Van Hemmen, L. & Wagner, H. (1996).A neuronal learning rule for sub-millisecond temporal coding.
Nature , 383 , 76-81.Goebel, G. & Hiller, W. (1994). The tinnitus questionnaire. A stan-
dard instrument for grading the degree of tinnitus. Results of a multicenter study with the tinnitus questionnaire. HNO , 42 ,166-172.
Goebel, G. & Hiller, W. (1998). Tinnitus-Fragebogen (TF). EinInstrument zur Erfassung von Belastung und Schweregrad beiTinnitus. Handanweisung, G ottingen, Hogrefe.
Goebel, G., Kahl, M., Arnold, W. & Fichter, M. (2006). 15-yearprospective follow-up study of behavioral therapy in a largesample of in patients with chronic tinnitus. Acta OtolaryngolSuppl , 556 , 70-79.
Guttman, R., Lewis, S. & Rinzel, J. (1980). Control of repetitive r-ingin squid axon membrane as a modelfor a neuroneoscillator.
J Physiol , 305 , 377-395.Hamalainen, M., Hari, R., Ilmoniemi, R.J., Knuutila, J. &
Lounasmaa, O.V. (1993). Magnetoencephalographytheory,instrumentation, and applications to noninvasive studies of theworking human brain. Rev Mod Phys , 65, 413-497.
Hartmann, T., Lorenz, I. & Weisz, N. (2011). Neurobiofeedback.In: Moller, A.R., Langguth, B., De Ridder, D. & Kleinjung, T.(Eds.), Textbook of Tinnitus, Springer, New York, 691-696.
Hauptmann, C., Popovych, O. & Tass, P.A. (2005). Effectivelydesynchronizing deepbrainstimulation basedon a coordinateddelayedfeedbackstimulationviaseveralsites:A computationalstudy. Biol Cybern , 93, 463-470.
Hauptmann, C. & Tass, P.A. (2007). Therapeutic rewiring by meansof desynchronizing brainstimulation. Biosystems , 89 , 173-181.
Hauptmann, C. & Tass, P.A. (2009). Cumulative and after-effectsof short and weak coordinated reset stimulation: A modelingstudy. J Neural Eng , 6 , 016004.
Hauptmann, C. & Tass, P.A. (2010). Restoration of segregated,physiological neuronal connectivity by desynchronizing stim-ulation. J Neural Eng , 7 , 056008.
Hazell, J.W.P. & Wood, S. (1981). Tinnitus masking a signicantcontribution to tinnitusmanagement. Brit J Audiol , 15 , 223-230.
Hesser, H., Weise, C., Rief, W. & Andersson, G. (2011). The effectof waiting: A meta-analysis of wait-list control groups in trialsfor tinnitus distress. J Psychosom Res , 70(4), 378-384.
Irvine, D.R., Rajan, R. & Brown, M. (2001). Injury- and use-relatedplasticityin adult auditorycortex. AudiolNeurootol , 6 , 192-195.
Jacobson, N.S. & Truax, P. (1991). Clinical signicance: A statisti-cal approach to dening meaningful change in psychotherapyresearch. J Consult Clin Psychol , 59, 12-19.
Jastreboff, P.J. & Hazell, J.W. (1993). A neurophysiologicalapproach to tinnitus: Clinical implications. Br J Audiol , 27 (1),7-17.
Jeanmonod, D., Magnin, M. & Morel, A. (1996). Low-thresholdcalcium spike bursts in the human thalamus. Common phys-iopathology for sensory, motor and limbic positive symptoms. Brain , 119 , 363-375.
Kahlbrock, N. & Weisz, N. (2008). Transient reduction of tinnitusintensity is marked by concomitant reductions of delta bandpower. BMC Biol , 16 (6), 4.
Klass,D.W. & Daly, D.D. (1979). (Eds.), Current practice of clinicalelectroencephalography, Raven Press, New York.
Kleinjung, T., Langguth, B. & Khedr, E. (2011). Transcranial mag-netic stimulation. In: Moller, A.R., Langguth, B., De Ridder,D. & Kleinjung, T. (Eds.), Textbook of Tinnitus, Springer, NewYork, 697-710.
Klimesch, W., Hanslmayr, S., Sauseng, P. & Gruber, W.R. (2006).Distinguishing the evoked response from a phase reset: A com-ment to M akinen et al. Neuroimage , 26 , 808-811.
Kovacs, S., Peeters, R., Smits, M., De Ridder, D., Van Hecke, P.& Sunaert, S. (2006). Activation of cortical and subcorticalauditory structures at 3 T by means of a functional magneticresonance imaging paradigm suitable for clinical use. Invest Radiol , 41, 87-96.
Kuhn, A.A., Kempf, F., Br ucke, C., Doyle, L.G., Martinez-Torres,I., Pogosyan, A., Trottenberg, T., Kupsch, A., Schneider, G.H.,Hariz, M.I., Vandenberghe, W., Nuttin, B. & Brown, P. (2008).High-frequency stimulation of the subthalamic nucleus sup-presses oscillatory beta activity in patients with Parkinsonsdisease in parallel with improvement in motor performance. J Neurosci , 28, 6165-6173.
Langguth, B.,Eichhammer,P., Wiegand, R., Marienhagen,J., Maen-ner, P., Jacob, P. & Hajak, G. (2003). Neuronavigated rTMS ina patient with chronic tinnitus. Effects of 4 weeks treatment. Neuroreport , 14, 977-980.
Liberman, M.C. & Dodds, L.W. (1984). Single-neuron labeling andchronic cochlear pathology. III Stereocilia damage and alter-ations of threshold tuning curves. Hear Res , 16 , 55-74.
Llinas, R.R., Ribary, U., Jeanmonod, D., Kronberg, E.& Mitra, P.P. (1999). Thalamocortical dysrhythmia:
8/11/2019 Tass Et Al_RNN 2012_Counteracting Tinnitus by Acoustic CR Neuromodulation
22/23
158 P.A. Tass et al. / Counteracting tinnitus by acoustic coordinated reset neuromodulation
A neurological and neuropsychiatric syndrome characterizedby magnetoencephalography. Proc Natl Acad Sci U S A , 96 ,15222-15227.
Lockwood, A.H., Salvi, R.J., Coad, M.L., Towsley, M.L., Wack,D.S. & Murphy, B.W. (1998). The functional neuroanatomy of tinnitus: Evidence for limbic system links and neural plasticity. Neurology , 50, 114-120.
Lockwood, A.H.,Salvi, R.J.,Burkard,R.F.,Galantowicz,P.J., Coad,M.L. & Wack, D.S. (1999). Neuroanatomy of tinnitus. Scand Audiol Suppl , 51, 47-52.
Lockwood, A.H., Salvi, R.J. & Burkard, R.F. (2002). Tinnitus. N Engl J Med , 347 , 904-910.
Lysyansky, B., Popovych, O.V. & Tass, P.A. (2011). Desynchroniz-ing anti-resonance effect of the m:n ON-OFF coordinated reset
stimulation. J Neural Eng , 8, 036019.Markram, H., L ubke, J., Frotscher, M. & Sakmann, B. (1997). Reg-
ulation of synapticefcacy by coincidence of postsynaptic APsand EPSPs. Science , 275 , 213-215.
Martinez-Devesa, P., Perera, R., Theodoulou, M. & Waddell, A.(2010). Cognitive behavioural therapy for tinnitus. Cochrane Database Syst Rev , 8(9), 1-33.
Melcher, J.R., Sigalovsky, I.S., Guinan, J.J. Jr. & Levine, R.A.(2000). Lateralized tinnitus studied with functional magneticresonance imaging: Abnormal inferior colliculus activation. J Neurophysiol , 83, 1058-1072.
Moazami-Goudarzi, M., Michels, L., Weisz, N. & Jeanmonod, D.(2010). Temporo-insular enhancement of EEG low and highfrequencies in patients with chronic tinnitus. QEEG study of
chronic tinnitus patients. BMC Neurosci , 11 , 40.Moller, A.R. (2003). Pathophysiology of tinnitus. Otolaryngol Clin
North Am , 36 , 249-266.
Moller, A.R. (2007). The role of neural plasticity in tinnitus. Prog Brain Res , 166 , 37-45.
Moller, A.R., Langguth, B., De Ridder, D. & Kleinjung, T. (2011),(Eds.), Textbook of tinnitus, Springer, New York.
Muhlnickel, W., Elbert, T., Taub, E. & Flor, H. (1998). Reorganiza-tion of auditory cortex in tinnitus. Proc Natl Acad Sci U S A ,95 , 10340-10343.
Neiman, A.B., Russell, D.F., Yakusheva, T.A., DiLullo, A. &Tass, P.A. (2007). Response clustering in transient stochas-tic synchronization and desynchronization of coupled neuronalbursters. Phys Rev E Stat Nonlin Soft Matter Phys,E76 , 021908.
Nichols, T.E. & Holmes, A.P. (2002). Nonparametric permutationtests for functional neuroimaging: A primer with examples. Hum Brain Mapp , 15 , 1-25.
Niedermeyer, E. & Lopes da Silva, F.H. (1999), (Eds.), Elec-troencephalography. Basic principals, clinical applications,andrelated elds. 4th ed., Williams & Wilkins, London.
Norena, A., Micheyl, C., Chery-Croze, S. & Collet, L. (2002).Psychoacoustic characterization of the tinnitus spectrum:Implications for the underlying mechanisms of tinnitus. Audiol Neurootol , 7 , 358-369.
Norena, A.J.& Eggermont, J.J.(2003).Changesin spontaneousneu-ral activity immediately after an acoustic trauma: Implicationsfor neural correlates of tinnitus. Hear Res , 183 , 137-153.
Nunez, P.L. (1981). Electric elds of the brain: The neurophysics of EEG, Oxford University Press, New York.
Ochi, K. & Eggermont, J.J. (1997). Effects of quinine on neu-ral activity in cat primary auditory cortex. Hear Res , 105 ,105-118.
Okamoto, H., Stracke, H., Stoll, W. & Pantev, C. (2010). Listeningto tailor-made music reversesmaladaptive auditorycortex reor-ganization and alleviates tinnitus. Proc Natl Acad Sci U S A ,107 (3), 1207-1210.
Ortmann, M., M uller, N., Schlee, W. & Weisz, N. (2011). Rapidincreases of gamma power in the auditory cortex followingnoise trauma in humans. Eur J Neurosci , 33 , 568-575.
Pascual-Leone, A., Valls-Sol e, J., Wassermann, E.M. & Hallett, M.(1994). Responses to rapid-rate transcranial magnetic stimula-
tion of the human cortex. Brain , 117 (4), 847-858.Pascual-Marqui, R.D. (2002). Standardized low resolution brain
electromagnetic tomography (sLORETA): Technical details. Methods Find Exp Clin Pharmacol , 24, 5-12.
Pickles, J.O. (1984). Frequency threshold curves and simultaneousmasking functions in high-threshold, broadly-tuned, bres of the guinea pig auditory nerve. Hear Res , 16 , 91-99.
Plewnia,C., Bartels, M. & Gerloff, C. (2003). Transient suppressionof tinnitus by transcranial magnetic stimulation. Ann Neurol ,53 , 263-266.
Popovych, O.V., Hauptmann, C. & Tass, P.A. (2006). Desynchro-nization and decoupling of interacting oscillators by nonlineardelayed feedback. Int J Bif Chaos , 16 , 1977-1987.
Popovych, O.V. & Tass, P.A. (2010). Synchronization control of interacting oscillatory ensembles by mixed nonlinear delayedfeedback. Phys Rev E , 82, 026204.
Popovych, O.P. & Tass, P.A. (2011). Macroscopic entrainment of periodically forced oscillatory ensembles. Prog Biophys Mol Biol, 105 , 98-108.
Popovych, O.V. & Tass, P.A. (2012). Desynchronizing electricaland sensory coordinated reset neuromodulation. Front Hum Neurosci , 6 , 58. doi:10.3389/fnhum.2012.00058
Quiroga, R.Q., Kraskov, A., Kreuz, T. & Grassberger, P. (2002).Performance of differentsynchronizationmeasuresin realdata:A case study on electroencephalographic signals. Phys Rev E ,65 , 041903.
Rajan, R. & Irvine, D.R. (1998). Neuronal responses across corti-cal eld A1 in plasticity induced by peripheral auditory organdamage. Audiol Neurootol , 3, 123-144.
Rauschecker, J.P. (1999). Auditorycortical plasticity: A comparisonwith other sensory systems. Trends Neurosci , 22 , 74-80.
Rauschecker, J.P., Leaver, A.M. & M uhlau, M. (2010). Tuning outthe noise: Limbic-auditory interactions in tinnitus. Neuron , 66 ,819-826.
Roberts, L.E., Eggermont, J.J., Caspary, D.M., Shore, S.E.,Melcher, J.R. & Kaltenbach, J.A. (2010). Ringing Ears:The Neuroscience of Tinnitus. J Neurosci , 30(45), 14972-14979.
Robertson, D. & Irvine, D.R. (1989). Plasticity of frequency organi-zation in auditory cortex of guinea pigs with partial unilateraldeafness. J Comp Neurol , 282 , 456-471.
8/11/2019 Tass Et Al_RNN 2012_Counteracting Tinnitus by Acoustic CR Neuromodulation
23/23
P.A. Tass et al. / Counteracting tinnitus by acoustic coordinated reset neuromodulation 159
Ryan, A., Dallos, P. & McGee, T. (1979). Psychophysical tuningcurves and auditory thresholds after hair cell damage in thechinchilla. J Acoust Soc Am , 66 , 1096-1098.
Saunders, J.C. (2007). The role of central nervous system plasticityin tinnitus. J Commun Disord , 40 , 313-334.
Scherg, M., Ille, N., Borneth, H. & Berg, P. (2002). Advanced toolsfor digital EEG review: Virtual source montages, whole-headmapping, correlation, and phase analysis. J Clin Neurophysiol ,19(2), 91-112.
Schlee, W., Mueller, N., Hartmann, T., Keil, J., Lorenz, I. & Weisz,N. (2009a). Mapping cortical hubs in tinnitus. BMC Biol , 7 , 80.
Schlee, W., Hartmann,T.,Langguth, B. & Weisz,N. (2009b).Abnor-mal resting-state cortical coupling in chronic tinnitus. BMC Neuroscience , 10 , 11.
Seki, S. & Eggermont, J.J. (2003). Changes in spontaneous ringrate and neural synchrony in cat primary auditory cortex afterlocalizedtone-induced hearing loss. Hear Res , 180 (1-2), 28-38.
Smits, M., Kovacs, S., De Ridder, D., Peeters, R.R., Van Hecke,P. & Sunaert, S. (2007). Lateralization of functional magneticresonanceimaging (fMRI) activationin theauditorypathway of patients with lateralized tinnitus. Neuroradiology , 49 , 669-679.
Steriade, M. (2006). Grouping of brain rhythms in corticothalamicsystems. Neuroscience , 137 , 1087-1106.
Suckf ull, M., Althaus, M., Ellers-Lenz, B., Gebauer, A.,Gortelmeyer, R., Jastreboff, P.J., Moebius, H.J., Rosenberg,T., Russ, H., Wirth, Y. & Krueger, H. (2011). A randomized,double-blind, placebo-controlled clinical trial to evaluate theefcacy and safety of neramexane in patients with moderate
to severe subjective tinnitus. BMC Ear Nose Throat Disord ,11 (11), 1.
Surr, R.K., Montgomery, A.A. & Mueller, H.G. (1985). Effect of amplication on Tinnitus among new hearing aid users. Ear Hear , 6 (2), 71-75.
Tass, P.A. (2002). Desynchronization of brain rhythms with softphase-resetting techniques. Biol Cybern , 87 , 102-115.
Tass, P.A. (2003). A model of desynchronizing deep brain stim-ulation with a demand-controlled coordinated reset of neuralsubpopulations. Biol Cybern , 89, 81-88.
Tass, P.A. & Majtanik, M. (2006). Long-term anti-kindling effectsof desynchronizing brain stimulation: A theoretical study. BiolCybern , 94, 58-66.
Tass,P.A. & Hauptmann, C. (2009). Anti-kindling achieved by stim-ulationtargeting slowsynaptic dynamics. Rest Neurol Neurosci ,27 , 589-609.
Tass, P.A., Silchenko, A., Hauptmann, C., Barnikol, U.B. & Speck-mann, E.-J. (2009). Long-lasting desynchronization in rathippocampal slice induced by coordinated reset stimulation.Phys Rev E Stat Nonlin Soft Matter Phys , 80 , 011902.
Tass, P.A. & Popovych, O.P. (2012). Unlearning tinnitus-relatedcerebral synchrony with acoustic coordinated reset stimulation theoretical concept and modelling. Biol Cybern , 106 , 27-36.doi:10.1007/s00422-012-0479-5
Temperli, P., Ghika, J., Villemure, J.-G., Bur