Embed Size (px)
Citation preview

Children and Youth Services Review 34 (2012) 973–982
Contents lists available at SciVerse ScienceDirect
Children and Youth Services Review
j ourna l homepage: www.e lsev ie r .com/ locate /ch i ldyouth
Teacher involvement in school mental health interventions: A systematic review
Cynthia G.S. Franklin a, Johnny S. Kim b, Tiffany N. Ryan a, Michael S. Kelly c, Katherine L. Montgomery a,⁎a The University of Texas at Austin, United Statesb University of Kansas, United Statesc Loyola University, United States
⁎ Corresponding author at: The University of Texas at1 University Station, D3500, Austin, TX 78712, United S
E-mail addresses: [email protected] (C.G.S.(J.S. Kim), [email protected] (T.N. Ryan), mkell17@[email protected] (K.L. Montgomery).
0190-7409/$ – see front matter © 2012 Elsevier Ltd. Alldoi:10.1016/j.childyouth.2012.01.027
a b s t r a c t
a r t i c l e i n f oArticle history:Received 3 November 2011Received in revised form 27 January 2012Accepted 29 January 2012Available online 3 February 2012
Keywords:TeacherMental healthSchool-based servicesResponse to interventionEffective
Schools are large providers of mental health services for children and adolescents. Recent educational policyinitiatives at the federal level have ushered in Response to Intervention and school-wide behavior supportsthat have potential to involve teachers in school mental health interventions. Little research exists investigat-ing the involvement of teachers in school mental health services or the level of efficacy associated withteachers providing these services. This paper conducts a systematic review to investigate the extent towhich teachers a) are the primary school-based service providers, b) collaboratively work with other profes-sionals to provide services, and c) what levels of interventions within the Response to Intervention (RTI)framework apply to these interventions. This paper further evaluates how efficacious teachers and schoolmental health professionals are in impacting outcomes in previous studies. Results indicated that out ofthe 49 school mental health studies analyzed, teachers were actively involved in 40.8% of mental health in-terventions evaluated, and were the sole providers of interventions in 18.4% of the studies. It was alsofound that many of these school mental health interventions were universal (Tier 1) and took place in theclassrooms. Further examination of findings suggested that different personnel, such as school mental healthprofessionals and teachers, achieved similar outcomes across the studies.
© 2012 Elsevier Ltd. All rights reserved.
1. Introduction
The 2005–2006 national survey by the Substance Abuse and Men-tal Health Services Administration (SAMHSA, 2007) revealed that ap-proximately three million youths received school-based services forbehavioral or emotional problems during the 2005–2006 academicyear. As this national survey indicates, schools often serve as a deliv-ery point for mental health services for children and adolescents(Adelman & Taylor, 2010; Hoagwood et al., 2007; Stormont, Reinke,& Herman, 2011). Adelman and Taylor (2010) suggest, for example,that over 50% of students from urban districts may have serious learn-ing, emotional, and behavioral problems that schools must address.These authors also point out that students' behavioral problemsmay be more psychosocial in nature and highlight that all problemsmay not warrant a mental health diagnosis. However, the resolutionof emotional and behavior problems has become a necessity for theimprovement of educational outcomes and falls under the auspicesof school-based mental health professionals. School based mentalhealth professionals (sbmhp), sometimes called Related Services(i.e. school social workers, psychologists, and counselors), are mainly
Austin, School of Social Work,tates. Tel.: +1 512 565 5750.Franklin), [email protected] (M.S. Kelly),
rights reserved.
responsible for the delivery of school mental health services.Teachers, however, have also become involved in classroom interven-tions and various learning supports.
1.1. Definitions of school mental health
School mental health is a broad category that describes many dif-ferent psychosocial interventions and services that are designed spe-cifically to be learning supports for students with social, emotional,and learning challenges. School-based mental health services havebeen defined very broadly to reflect a diversity of services that maybe used in schools to meet the learning needs of students. Schoolmental health, for example, has been defined by The National Assem-bly of School-based Health Care as being an overarching concept thatencompasses many programs and frameworks including, but not lim-ited to, student assistant teams, Response to Intervention (RTI), posi-tive behavioral interventions and supports, special education, socialand emotional learning services, Safe Schools and Healthy Students,school climate and many other initiatives that are meant to addressthe social and emotional learning, and behavioral responses of stu-dents. Weist and Paternite (2006) suggest that school mental healthmay focus on all students, general and special education, and includea full range of programs, strategies, and services ranging from mentalhealth promotion to mental health intervention.
Adelman and Taylor (2010) also describe the roles of school men-tal health professionals as including the delivery of mental health

974 C.G.S. Franklin et al. / Children and Youth Services Review 34 (2012) 973–982
promotion, prevention programs aimed at resolving psychosocialproblems, enhancing resiliency in students and early interventions,building the capacity of school staff towardmental health and system-ic changes in school programs, as well as supporting schools with em-pirically supported treatments for students thatmay have one ormorediagnosable mental disorders. Through the lens of an RTI framework,this manuscript investigates the effectiveness of school mental healthservices, with a specific focus on understanding the extent to whichteachers are involved in intervention service delivery.
2. Background
2.1. Response to intervention and school mental health
Recent reauthorizations of IDEA (1997, 2004) have encouragedthe use of RTI, a public health framework that promotes the use ofthree tiers of intervention corresponding to primary, secondary, andtertiary prevention (Fuchs & Fuchs, 2006; Hoover, Baca, Wexler-Love, & Saenz, 2008). Though RTI began as an initiative rooted in spe-cial education, goals of the policy have become focused on: 1) an in-creased direct involvement of regular education teachers in theassessment of at-risk students and 2) enabling school districts touse the RTI framework as a tool to develop school-wide strategiesthat coalesce around helping all children achieve positive academicand behavioral outcomes (Vaughn & Fuchs, 2003).
Over the past decade, RTI has been expanded to include two relat-ed, but distinct, strands of school-based interventions for bothteachers and school-based mental health professionals. RTI has beenoffered as a framework to design and implement evidence-basedearly intervention strategies for students with specific behavioral inter-ventions for specific students (Gresham, 2005), though there is littleevidence yet on the efficacy of this approach. Additionally, school-wide positive behavioral supports aimed at improving the schoolclimate, and evidence-based mental health practices within schoolsare often characterized as RTI (though they are also sometimes de-scribed by the related term Positive Behavior Supports or PBS). In par-ticular, many of these interventions have focused on the classroommanagement strategies employed by teachers and their abilities to de-liver social–emotional learning curriculum in their classrooms(Lindsey, White, & Korr, 2006).
Related service personnel, specifically school-based mental healthprofessionals (SBMHP) such as school social workers, school coun-selors, and school psychologists, have begun to adapt their practiceroles to work explicitly within the various facets of the RTI frame-work. Though this process is far from uniform, recent survey data col-lected on SBMHP practice indicate that SBMHP participate in RTI inthe following ways:
1) Attending RTI team meetings2) Identifying students for more intensive tier-based interventions
based on data collected by the SBMHP and the RTI team,3) Measuring the impact of interventions delivered by the SBMHP to
address student behavioral issues at all three tiers4) Delivering universal (Tier 1) and more targeted interventions
(Tier 2 and Tier 3)5) Working collaboratively with classroom teachers to implement
behavior plans6) Consulting with the administrative team by helping them select
appropriate universal interventions to address behavioral andsocio-emotional problems in the school building (Kelly, Raines,Stone, & Frey, 2010; Sabatino, 2009).
2.2. Roles of teachers and school mental health professionals within RTI
RTI has changed the way special education and general educationteachers function. For example, it has caused their roles to more
frequently overlap and has also increased the workload of general ed-ucation teachers through helping children with serious behavioralchallenges and/or mental health disorders (Fairbanks, Simonsen, &Sugai, 2008; Horner et al., 2009; Simonsen, Shaw, Faggella-lubymSugai, Coyne, & Alfano, 2010). In a typical RTI framework, the schoolfirst implements “Tier 1,” universal strategies in every classroom. Itis presumed that general education teachers will learn the best class-room management strategies, which are based on the principles ofapplied behavioral analysis (e.g. setting clear rules and consequences,contingent praise, and the use of positive reinforcement). Then sec-ondly, the school offers “Tier 2,” selective interventions that consistof small group instruction or intervention for children. Progress ofTier 2 interventions is revealed through continuous progress moni-toring in data-based assessments to extend help beyond the universallevel. While all students in a school that implements the RTI approachreceive Tier 1 interventions, only approximately 20% may be referredto a Tier 2 intervention (Frey, Lingo, & Nelson, 2011).
Students that need help beyond the Tier 2 interventions may re-ceive “Tier 3” (indicated) interventions that involvemore intensive in-dividualized instruction and/or therapeutic approaches (Kelly, 2008).At the point of needing Tier 3 interventions, many students may be re-ferred for special education services. RTI approaches that involve spe-cial education and intensive, individualized therapeutic interventionsare considered to be the last and greatest effort to help a child. Whilethismay become the exclusive domain of schoolmental health profes-sionals, it is conceptualized to only involve approximately 5% of chil-dren in schools (Kelly, 2008). This means that special educators andschool mental health teams, such as school social workers and psy-chologists, have an important role to play in providing support to gen-eral education teachers that are on the front-lines of the Tier 1interventions andmay further work closely with teachers in the deliv-ery of Tier 2 interventions (Fairbanks et al., 2008).
As Richards, Pavri, Golez, Canges, and Murphy (2007) point out inactual school settings, the interventions that are delivered across tiersmay become blurred, and general education teachers may also be in-volved in delivery of the Tier 2 interventions. Frey et al. (2011) alsosuggest that Tiers 2 and 3 interventions may be hard to differentiatefrom one another. The result being that Tiers 1 and 2 may overlapand may scaffold on one another, and Tiers 2 and 3 may increase inten-sity of interventions, but use the same types of interventions in differ-ent ways. For example, a student assessed by the 3-tier framework andfound to needmore intensive social skills instructionmay participate in30 min of small group social skills instruction (Tier 2) delivered by aclassroom teacher or fill out a daily report card while continuing theircurrent Tier 1 classroom instruction by a teacher. When moving toTier 3, social skills interventions may focus more intensively on stu-dents who continue to receive the same social skills instruction and in-tensive monitoring interventions as other students (such as a dailyreport card) along with other individual, family, and community inter-ventions that may be delivered by a school mental health team, butmay also involve the student's general education teacher.
2.3. Teamwork between school based mental health professionalsand teachers
Literature suggests that teachers are valuable partners with schoolmental health professionals and may take on significant roles in thedelivery of mental health interventions in school settings (Feinstein,Fielding, Udvari-Solner, & Joshi, 2009; Ringwalt et al., 2010; Smolak,Harris, Levine, & Shisslak, 2001; Stormont, Lewis, Beckner, & Johnson,2008; Wolmer, Hamiel, & Laor, 2011). Several authors have also sug-gested advantages to including teachers on mental health teams. Adiand colleagues suggested that teachers may be better at sustaininglonger-term effects because interventions may be reinforced in class-rooms (Adi, Killoran, Janmohamed, & Stewart-Brown, 2007). Similar-ly, Diekstra (2008) also pointed out that teachers are better at

975C.G.S. Franklin et al. / Children and Youth Services Review 34 (2012) 973–982
integrating social and emotional interventions in ways that may im-pact academic performance because they are more involved with stu-dents for prolonged periods of time and across different schoolprograms and, therefore, may have the largest impact on studentfunctioning. This is a point that is also echoed by Feinstein et al.(2009), who suggested that effective delivery of mental health inter-ventions in schools might not be possible without the collaboration ofteachers, because mental health professionals have substantially lessaccess to students.
Implementation of an RTI framework within a school suggests thatschool-based mental health professionals may work together as ateam with teachers in the delivery of school mental health interven-tions. When researchers examine the roles of teachers and schoolmental health professionals in school mental health services the re-sults are not as clear concerning how often the two work togetheras a team. A national survey of school-based mental health programsfound, for example, that most mental health programs that were onceprovided have withdrawn their screening and counseling servicesand, further, that there was little time for collaboration betweenteachers and mental health professionals (Foster et al., 2005). In an-other more recent national survey of school social work professionals,however, Berzin et al. (2011) found that school social workers oftencollaborated with teachers to assist with the following: 1) helpedteachers with behavior intervention plans and classroom manage-ment techniques, 2) conducted joint sessions with teachers and stu-dents, and 3) improved teacher professional development. Othercollaborative roles with teachers also included those that involvedcase management and school-wide reform (Berzin et al., 2011). Thissurvey suggests that teamwork is occurring between school mentalhealth professionals and teachers, but more research is needed toclarify how often teachers may work as a team with mental healthprofessionals in the delivery of mental health interventions.
2.4. Effective school mental health interventions
Baskin, Slaten, Sorenson, Glover-Russell, and Merson (2010) com-pleted a meta-analysis of 107 counseling and psychotherapy youthstudies in schools and found an overall medium effect size (0.45)for youth interventions. This review allowed for studies that weredesigned by psychologists and other mental health professionals,but were delivered by teachers. The study further examined interven-tion moderators grouping teachers into a paraprofessional categoryalong with parents. Twenty-three of the 107 studies analyzed wereimplemented by the paraprofessionals including both teachers andparents. Results indicated that licensed mental health professionalsout performed (0.67) the paraprofessionals (0.45) and, further, para-professionals had better results than graduate students (0.17). It isworth noting, however, that the teachers and parent deliverers of in-terventions achieved a medium effect size, which is the same as theoverall study results.
In separate narrative reviews, Rones and Hoagwood (2000) iden-tified 47 effective mental health interventions, and Hoagwood et al.(2007) identified 24 effective school-based mental health interven-tions. Although these empirical reviews did not specifically focuson the role that teachers might play in the delivery of these inter-ventions, the results do provide some insights into effective pro-gram components. For example, Hoagwood et al. (2007)discovered that the more efficacious interventions included class-room, family, and school-wide interventions that suggested ecologi-cal and collaborative approaches are the most effective ways toimpact both mental health and academic outcomes. Other re-searchers reviewing the school-based intervention literature havesuggested that school mental health professionals work withteachers who are intricately involved in carrying out many of theevidence-based, behavioral interventions in schools, especially
those delivered at the Tiers 1 and 2 levels (Anderson-Butcher &Ashton, 2004; Berzin et al., 2011; Frey et al., 2011).
2.5. Teacher effectiveness in school mental health
Teachers may play a central role in the implementation of strat-egies and interventions rooted in the RTI framework, but their effec-tive role in the implementation of RTI and mental healthinterventions is a point of controversy within the educational litera-ture (e.g., Chitiyo & Wheeler, 2009; Hawkins & Heflin, 2011;Ringwalt et al., 2010; Tillery, Varjas, Meyers, & Collins, 2010). Forexample, researchers suggest that many teachers lack knowledgeabout RTI and others do not understand the core concepts of RTIwell enough to carry them out effectively over time. Reviews ofthe research have also indicated that teachers lack knowledge andtraining in mental health and are not well equipped to carry out be-havioral interventions (Frey et al., 2011). On the other hand, re-search suggests that teacher–student relationships are key to socialand emotional development and the academic achievement of stu-dents (Helker, Schottelkorb, & Ray, 2007). Teachers may also bevery effective in the implementation of both RTI and evidence-based mental health practices if teacher efficacy is increased, theyare thoroughly trained, and are provided the appropriate supportsand supervision by administration and mental health professionalsto carry-out and sustain the interventions (Durlak, Weissberg,Dymnicki, Taylor, & Schellinger, 2011; Easton & Erchul, 2011; Lane,Weisenbach, Little, Phillips, & Wehby, 2006; Murray, Rabiner,Schulte, & Newitt, 2008; Pierce, Reid, & Epstein, 2004).
The classroom management practices of teachers are highlightedthe most as an effective behavioral intervention. Effective classroommanagement has been shown to decrease children's behavior prob-lems, as well as offer promising implications regarding the preventionand development of more serious emotional and behavioral disorders(Hester et al., 2004; Leflot, van Lier, Onghena, & Colpin, 2010; Myers,Simonsen, & Sugai, 2011; Pierce et al., 2004).
Although, teachers may obviously have important roles in class-room management strategies, researchers have not specifically stud-ied teacher implementation and effectiveness in the delivery ofevidence-based, mental health interventions. In a meta-analysis onschool-based programs for aggressive and disruptive behavior, how-ever, Wilson, Lipsey, and Derzon (2003) found that “interventionswere generally more effective when implemented well and relativelyintense, used one on one formats and were administered by teachers”(p. 148). Interventions studied included social competence training,behavioral interventions, therapy and counseling, multimodal pro-grams and peer mediation. In a separate but related study Wilsonand Lipsey (2007) also concluded that the interventions deliveredby teachers to prevent violence and aggression were more sustain-able and cost effective when compared to other interventionists.
3. Purpose of current review
The purpose of this article is to conduct a retrospective systematicreview of the literature on school mental health interventions tomore closely examine the extent to which teachers may be involvedin the delivery of school-based mental health services. The mainfocus of this article is twofold: 1) to assess how often teachers are in-volved in delivering school mental health interventions and 2) to as-sess at what level of intervention teachers may be involved using theframework of Response to Intervention. As a supplementary aim, thisarticle will also examine the efficacy of school mental health inter-ventions implemented by teachers in conjunction with and compari-son to other professionals, and in relationship to diverse outcomesthrough calculating corresponding effect sizes.

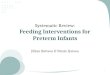
Records identified through database searching from January 1999 to
September 2010(n = 1443)
Additional records identified through references from systematic reviews published
from January 1999 to September 2010 (n = 72)
Potentially relevant studies examined for inclusion(n = 1515)
Potentially relevant studies re - examined for inclusion(n = 81)
Studies excluded (n= 1436)Reasons include: Duplicate studies, study lacking test of mental health or behavioral intervention, study not an experimental design, study not conducted in school setting or in US, not published between Jan. 1999-Sept. 2010
Studies excluded (n = 30)Reasons include: Insufficient data or information to calculate effect sizes
Studies included insystematic review
(n = 49)
Fig. 1. Study selection flowchart.
976 C.G.S. Franklin et al. / Children and Youth Services Review 34 (2012) 973–982
4. Method
For this review, we have concentrated our literature search andstudy inclusion on specific criteria and recent school mental healthstudies for two specific reasons. First, we wish to review school men-tal health literature that reflects a more recent shift in the ways ser-vices are being conceptualized and delivered, specifically related tothe framework of Response to Intervention (RTI) and its relatedframework SWPBS, because these studies may better reflect the cur-rent roles of teachers in the delivery of school mental health services.The RTI framework has become a major emphasis of state and localschool policy initiatives, and many studies conducted in the 1980sand early 1990s were not conducting school mental health practiceswithin this framework and, therefore, may not adequately reflectthe programs that are currently being implemented in many schools.Second, other scholars have examined school-based interventionsfrom 1980 and beyond (Baskin et al., 2010; Franklin, Kim, & Tripodi,2009; Rones & Hoagwood, 2000) and we wish to add to this literatureby more carefully examining the changing roles of teachers in the de-livery of school mental health services. Thus, the following inclusioncriteria were created to most adequately address the aims associatedwith this article.
4.1. Study selection
School mental health interventions may be best identified by thepurposes for which they are designed and delivered, and that is toassist the mental health functioning of students and to supporttheir social and emotional learning within schools. School mentalhealth services are not determined by or limited to any specificmental health diagnosis or intervention but instead are servicesthat are self-defined as being a school-related, mental health servicewith a specific focus on improving the social, emotional and behav-ioral functioning of students. Since the school mental health litera-ture is vast and interventions grounded in research evidence aremost critical, we will narrow our examination of the literature toschool-based mental health interventions that have been studiedusing experimental and quasi-experimental designs. Fig. 1 depictsthe review process and decisions made that led the final study se-lection. A computerized search on several databases (ERIC, Psy-cINFO, MEDLINE, CINHAL, & Social Science Abstracts) wasconducted to locate studies that tested any school-based mentalhealth services for children. Studies were identified using the key-words: school*, children or adolescent* or youth, mental health ormental health service*, and outcome study or effective or efficacy,with an * on some words to include multiple variations of thatterm. Furthermore, other published systematic reviews weresearched to locate additional studies that might be included in thismeta-analysis. In order to meet study inclusion for this systematicreview, primary studies needed to meet the following eligibility cri-teria: (a) study research design is either a randomized controlledtrials or quasi-experimental involving a comparison between andintervention and control group; (b) study published between Janu-ary 1999 and September 2010; (c) study conducted in a school set-ting; (d) involved a mental health and behavioral service such asprevention, risk reduction, and intervention/treatment; (e) studyconducted in the United States; and (f) study contained enough sta-tistical information to calculate effect sizes. Qualitative studies, de-scriptive case studies, and single-case design were excluded due tothe lack of statistical information to calculate effect sizes.
4.2. Effect size calculation
For each study, one effect size was calculated and entered usingComprehensive Meta-Analysis software 2.0 (Borenstein, Hedges,Higgins, & Rothstein, 2005). Hedges's g effect sizes (with small
sample size bias adjustment) were calculated for studies reportingstandardized mean differences between treatment and control condi-tions while odds ratio effect sizes were calculated for dichotomousoutcomes and then converted to Hedges's g effect sizes (Cooper &Hedges, 1994). One study (Hallfors et al., 2006) reported non-significant results without providing any detailed statistical informa-tion; therefore, an effect size of zero was substituted for non-significant outcomes as recommended by Perry (1997). This providesa more conservative pooled point estimate of the effect size. All effectsizes were recorded such that a positive value indicated a better out-come for the experimental condition regardless of the direction of thescale used in the original study.
When studies reported multiple follow-up points, the firstfollow-up point was selected to help calculate effect sizes(Corcoran & Pillai, 2007). Several studies contained two different in-terventions in addition to a control group with results comparingboth interventions to the control as well as between the two inter-ventions. In these instances, an effect size was calculated for eachcomparison between the experimental and control group and thenthose effect sizes were averaged together to come up with one ef-fect size estimate for the study. Effect sizes were interpreted basedon classification by Cohen (1988), with 0.20 indicating a small effectsize, 0.50 indicating medium, and 0.80 and above considered large.A 95% confidence interval (CI) level was also calculated for eachstudy effect size measure to indicate the precision of the estimatedeffect size (Lipsey & Wilson, 2001), as well as used to indicate statis-tical significance for a study's outcome measure. If the 95% confi-dence interval level does not contain zero, then we can reject thenull hypothesis and conclude that the effect size estimate is signifi-cantly different from zero (Littell, Corcoran, & Pillai, 2008; Shadish &Haddock, 1994). When a primary study used multiple measures fora single outcome construct, we followed Lipsey's (1994) suggestionto calculate individual effect sizes for each of the different measuresin a single study and then average them to come up with one effectsize for that measure.

Table 1Study characteristics.
Characteristic N (%)
Publication date1999–2004 37 (75.5)2005–2010 12 (24.5)
Research designExperimental 33 (67.3)Quasi-experimental 16 (32.7)
Type of controlNo treatment 57.1Waitlist control 18.4Alternative treatment 14.3Treatment as usual 10.2
Outcomes examinedInternalizing problems 17 (34.7)Externalizing problems 1 (2.0)Internalizing and externalizing problems 5 (10.2)Substance abuse 6 (12.2)Social skills or psycho-education 7 (14.3)Academic performance 2 (4.1)Multiple outcomes 11 (22.4)
School levelElementary school 19 (38.8)Middle school 12 (24.5)High school 14 (28.6)Multiple levels 4 (8.2)
Ethnicity of studentsAsian, Black, Hispanic, and White 20 (40.8)Black, Hispanic, and White 13 (26.5)Black only 3 (6.1)Hispanic only 5 (10.2)Minority only 3 (6.1)Did not specify 5 (10.2)
Classroom settingGeneral education 46 (93.9)Special education 3 (6.1)
977C.G.S. Franklin et al. / Children and Youth Services Review 34 (2012) 973–982
4.3. RTI coding
After the final selection of studies to be included in this review,two of the authors independently went through all the studies andcoded the RTI levels and then compared their results for agreement.Those studies that were coded differently were double checked andresolved through a consensus agreement between the authors ofthis study. When coding the RTI levels in this study, we delineatedthe tiers as follows:
• Universal (Tier 1): An intervention delivered to either at an entireschool-level or across specific grade-levels within an entire schoolto all students (e.g., all 3rd–5th grade classrooms get interventionor all students in a school learn from a bullying preventioncurriculum).
• Selective (Tier 2): An intervention delivered at either a classroom orsmall-group level that identifies a specific group of students who ei-ther are at-risk for certain problems, but have not developed specif-ic diagnostic and behavioral severity within the school (i.e., aspecific IEP label for special education or a high number of behav-ioral or discipline referrals).
• Indicated (Tier 3): An intervention that is conducted in individualor small group (or self-contained Special education classroom) set-tings for students who are already “identified” for specific serviceswithin the school or community setting (i.e., an IEP, a DSM diagno-sis, severe behavioral/discipline issues, involvement with juvenilejustice, etc.)
5. Results
This study reviewed published articles from January 1999 to Sep-tember 2010 and found 1443 studies that met the initial inclusion cri-teria and 49 studies that met the final inclusion criteria. The finalstudies included contained 3 published studies by the Conduct Prob-lems Prevention Research Group (CPPRG) group and a decision wasmade to treat them as one study since the same sample was used aspart of a larger longitudinal study. The studies that were excludedfrom the final review sample either did not meet criteria for the re-search inclusion design or did not have necessary information in thearticle to calculate an effect size. As seen in Table 1, results showthree-fourths of the studies were published during 1999–2004,while a quarter of the studies were published during 2005–2010.The majority of the studies (67.3%) used an experimental design.More than half the final studies (57.1%) used a control group that re-ceived no treatment, followed by waitlist control group (18.4%), alter-native treatment (14.3%), and business as usual (10.2%). Regardingoutcomes examined, 34.7% looked at internalizing problems, 2%looked at externalizing problems, and 10.2% looked at both internal-izing and externalizing problems. Studies in this review also exam-ined substance abuse (12.2%), social skills or psycho-education(14.3%), academic performance (4.1%), and multiple outcomes(22.4%).
The grade levels of student participants in the studies were divid-ed somewhat equally, with 38.8% only including elementary schoolaged participants, 24.5% middle school, 28.6% high school, and 8.2%studying multiple grade levels. The majority of the studies (40.8%) ex-amined all students with coded diverse ethnic and racial back-grounds. Twenty-six percent of the studies examined a combinationof Caucasian, Black, and Hispanic students, and 10.2% did not specifyracial composition of their sample. Noteworthy, we chose to codeunder the term “Black” rather than “African American,” because notall Black students identify their ancestors as being from Africa (for ex-ample, some are from Jamaica or Haiti). The remainder of the articlesidentified either one specific group to study or a combination of mi-nority groups with 6.1% using a sample of only minority students,6.1% only including Black students, and 10.2% only Hispanic students.
Most of the articles (93.9%) conducted studies on general educationclassrooms and only 6.1% looked at both general education and spe-cial education classrooms.
Results compiled in Table 2 reveal that more than half of the studyinterventions (59.2%) were conducted by a combination of experi-enced clinicians, graduate interns, or other non-teaching profes-sionals, such as nurses. Studies using only professional clinicians,such as school social workers and psychologists, accounted for28.6% of the studies, and 18.4% of the studies had only teachers pro-vide the interventions to the students. As most of the studies wereconducted in the classroom, 40.8% of the interventions involvedteachers at some level in the delivery of the interventions. The mostcommon RTI level targeted was the Tier 1, universal preventative in-terventions (40.8%). Only one study (Eron et al., 2002) targeted allthree RTI levels, leaving two studies (Conduct Problems PreventionResearch Group, 1999, 2002, 2004; Fast, Fanelli, & Salen, 2003) thattargeted some combination involving 2 of the 3 RTI levels.
Effect size results across all 49 studies ranged from zero (Hallforset al., 2006) to a very large effect size of 1.898 (Larkin & Thyer,1999). When teachers were the sole providers of interventions(n=8), study effect sizes ranged from a zero (Hallfors et al., 2006),which indicates no treatment effect, to a large effect size of 1.214(Duncan, Duncan, Beauchamp, Wells, & Ary, 2000). More specifically,three studies (Cho, Hallfors, & Sánchez, 2005; Hallfors et al., 2006;Melnyk et al., 2009) had small effect sizes, three studies (Botvin,Griffin, Diaz, & Ifill-Williams, 2001; Hennessey, 2007; Robinson,Smith, & Miller, 2002) had medium effect sizes, and one study(Duncan et al., 2000) that offered a large effect size. For those studieswhere teachers were involved in the delivery of the interventionalong with others (n=12), effect sizes ranged from a small effectsize of 0.100 (McWhirter & Page, 1999) to a large effect size of0.706 (Franklin, Moore, & Hopson, 2008). A majority of these studiesreported small treatment effects, with only two studies (Flay, Allred,

Table 2RTI intervention results.
Study Intervention RTI level Intervention deliverers Effect size (95% CI)
Armbruster and Lichtman (1999) School-based mental health service program Indicated Clinical therapists 0.093 (0.27, −0.09)Asarnow, Scott, and Mintz (2002) Cognitive behaviors family education intervention Indicated Graduate interns 0.298 (−0.51, 1.11)Bauer, Lozano, and Rivara (2007) Olweus Bullying Prevention Program Universal Whole school — teacher,
staff, administration0.136 (0.06, 0.22)
Bohman, Barker, Bell, Lewis, Holleran,and Pomeroy (2004)
Protecting Me, Protecting You Curriculum Universal Teachers and students 0.278 (0.06, 0.50)
Botvin, Griffin, Diaz,and Ifill-Williams (2001)
Life skills training to prevent drug and alcohol use Universal Teachers 0.494 (0.25, 0.74)
Bruning, Brown, Winzelberg, Abascal,and Taylor (2004)
Student bodies program — internet-based eatingdisorder prevention program
Universal Clinical therapists 0.354 (−0.06, 0.76)
Carbonell and Partelemo-Barehmi(1999)
Psychodrama group program Indicated Clinical therapists 0.672 (−0.10, 1.45)
Cho, Hallfors, and Sánchez (2005) Reconnecting Youth class Universal Teachers 0.101 (−0.05, 0.25)Cardemil, Reivich, and Seligman (2002) Penn Resiliency Program (Depression
Prevention Program)Selective Graduate interns and
clinical therapists0.170 (−0.17, 0.51)
Chemtob, Nakashima, andCarlson (2002)
EMDR Indicated Graduate interns 0.172 (−0.51, 0.85)
Conduct Problems Prevention ResearchGroup (1999, 2002, 2004)
Fast Track and PATH's curriculum Universal andindicated
Teachers andClinical Therapists
0.113 (0.03, 0.19)
DeRosier, 2004 Social skills group intervention Selective Graduate interns andclinical therapists
0.118 (−0.08, 0.32)
Donaldson, Thomas, Graham, Au,and Hansen (2000)
Adolescent Alcohol Prevention Trial Universal Clinical therapists 0.269 (0.06, 0.48)
Duncan, Beauchamp, Wells,and Ary (2000)
CD-ROM refuse to use Selective Teachers 1.214 (0.72, 1.71)
Eron, Huesmann, Spindler, Guerra,Henry, and Tolan (2002)
Yes I Can curriculum — for social skills and conduct Universal, selective,and indicated
Teachers, interns, andclinical therapists
0.229 (0.01, 0.45)
Fast, Fanelli, and Salen (2003) Mediation curriculum by Yale Child Studies Center Universal andselective
Administrator andgraduate interns
0.589 (−0.07, 1.25)
Flay, Allred, and Ordway (2001) Positive action Universal Whole school- teacher,staff, administration
0.580 (0.50, 0.66)
Franklin, Moore, and Hopson (2008) Solution Focused Brief Therapy Selective Teachers andclinical therapists
0.706 (−0.01, 1.42)
Frey (2002) Social skills classroom meeting program Universal Clinical therapists 0.440 (0.08, 0.80)Gillham et al. (2007). Penn Resiliency Program Universal Teachers, interns,
and clinical therapists0.172 (−0.02, 0.36)
Ginsburg and Drake, (2002) Cognitive behavioral small groups Indicated Graduate interns 0.610 (−0.48, 1.70)Gottfredson and Gore (2002) Cognitive behavioral instruction — Social Problem
Solving CurriculumUniversal Graduate interns 0.143 (−0.12, 0.40)
Hallfors, Cho, Sanchez, Khatapoush,Kim, Bauer (2006)
Reconnecting Youth class Selective Teachers 0a
Hardin, Weinrich, Weinrich, Garrison,Addy, Hardin (2002)
Catastrophic stress intervention Selective Nurses 0.267 (0.15, 0.39)
Harris and Franklin, 2003 Cognitive behavioral small groups Indicated Clinical therapistsand students
0.748 (0.28, 1.22)
Hawkins, Catalano, Kosterman,Abbott, and Hill (1999)
Classroom instruction and management,child skill development, parent intervention
Universal Teachers andClinical Therapists
0.161 (−0.05, 0.37)
Hennessey (2007). Open Circle Program Universal Teachers 0.461 (0.13, 0.79)Herrmann and McWhirter (2003) Student created aggression replacement
education programSelective Graduate Interns 0.326 (−0.23, 0.88)
Ialongo, Poduska, Werthamer,and Kellam (2001)
Classroom centered intervention and familycentered partnership intervention
Universal Teachers andClinical Therapists
0.369 (0.15, 0.59)
Jaycox et al. (2006) Break the cycle's ending violence curriculum Universal Attorneys 0.191 (0.10, 0.28)Jenson and Dieterich, (2007) Youth matters Universal Clinical Therapists 0.092 (−0.06, 0.24)Kataoka et al. (2003) Group based on the cognitive behavioral
intervention for trauma in schoolsIndicated Clinical therapists 0.350 (0.02, 0.68)
Ko, S., and Cosden (2001). Child abuse listening and mediation Universal Clinical therapists 0.237 (−0.36, 0.84)Kumpfer, Alvarado, Tait
and Turner (2002)Project SAFE — I can problem solve andstrengthening families
Universal Teachers andclinical therapists
0.649 (0.35, 0.95)
Larkin and Thyer, 1999 Cognitive behavioral small groups Indicated Clinical therapists 1.898 (1.23, 2.57)McWhirter and Page (1999) Skills for living anger management curriculum Selective Teachers and
clinical therapists0.100 (−0.37, 0.57)
Melnyk Jacobson, Kelly, O'Haver,Small, Mays and (2009)
Creating opportunities for personal empowerment,healthy lifestyle and thinking, emotions, exerciseand nutrition
Universal Teachers 0.189 (−0.76, 1.14)
Mufson et al. (2004) Interpersonal therapy amended Indicated Clinical therapists 0.543 (0.05, 1.04)Murray and Malmgren (2005) teacher student relationship program Selective Teachers 0.271 (−0.29, 0.83)Pedro-Carroll et al. (1999) Children of divorce intervention program Selective Clinical Therapists
and Graduate interns0.945 (0.31, 1.58)
Post, P. (1999). Child centered play therapy Selective Graduate interns 0.252 (−0.05, 0.56)Robinson, Smith, and Miller (2002) Anger control curriculum — cognitive behavioral Indicated Teachers 0.526 (−0.10, 1.15)Stein et al. (2003) CBT for trauma in schools Indicated Clinical therapists 0.356 (−0.01, 0.72)Viggiani et al. (2002) Social worker–teacher classroom collaboration Universal Teachers and
graduate interns0.378 (−0.07, 0.83)
Walkeret al. (2006) Motivational enhancement therapy Indicated Clinical therapists 0.208 (−0.19, 0.60)
978 C.G.S. Franklin et al. / Children and Youth Services Review 34 (2012) 973–982

Table 2 (continued)
Study Intervention RTI level Intervention deliverers Effect size (95% CI)
Weiss, Harris, Catron,and Han (2003)
RECAP — a psychosocial intervention Selective Clinical therapists 0.220 (−0.21, 0.65)
Werch et al. (2010) Planned success brief intervention Selective Nurses and certifiedhealth educators
0.132 (−0.08, 0.34)
Yampolskaya, Brown,and Vargo (2004)
Youth asset development program and postponingsexual involvement program
Universal Clinical therapists 0.361 (0.10, 0.62)
Zubernis et al. (1999) Depression prevention program for children Selective Graduate interns 0.594 (−0.27, 1.46)
a This study did not report enough information to calculate effect sizes but did report non-significant results.
979C.G.S. Franklin et al. / Children and Youth Services Review 34 (2012) 973–982
& Ordway, 2001; Kumpfer, Alvarado, Tait, & Turner, 2002) offeringmedium effect sizes, and one study (Franklin et al., 2008) reportinga large effect size.
When examining effect size results for those studies where onlyprofessional clinicians provided the intervention (n=14), effectsizes were mostly small, with three studies (Carbonell & Partelemo-Barehmi, 1999; Frey, 2002; Mufson et al., 2004) offering medium ef-fect sizes and one study (Larkin & Thyer, 1999) having a very large ef-fect size. For those studies that only used graduate interns (n=7) toprovide the intervention, effect sizes were also mostly small, withonly two studies (Ginsburg & Drake, 2002; Zubernis, Cassidy,Gillham, Reivich, & Jaycox, 1999) reporting a medium effect size. Forthose studies that had interventions delivered by non-teaching pro-fessionals only or by professional clinicians along with graduate in-terns or other non-teaching professionals (n=8), most of the effectsizes ranged in the small category. Only one study had a medium ef-fect size (Fast et al., 2003), and two studies (Harris & Franklin, 2003;Pedro-Carroll, Sutton, & Wyman, 1999) had large effect sizes.
Effect size results based on targeted RTI levels primarily revealedsmall treatment effects across all three levels. Universal preventativeinterventions included in this review revealed that 75% of the studieshad small effect size estimates, five studies (Botvin et al., 2001; Flay etal., 2001; Frey, 2002; Hennessey, 2007; Kumpfer et al., 2002) offeredmedium effect size estimates, and no studies that fell into the large ef-fect size category. About 71% of the selective preventative interven-tions also had small effect sizes. Only one selective interventionstudy (Zubernis et al., 1999) had a medium effect size estimate, andthree studies (Pedro-Carroll et al.,1999; Duncan et al., 2000;Franklin et al., 2008) had large effect sizes. Regarding the indicatedpreventative intervention studies, 50% included in this review hadsmall effect sizes. Four studies (Carbonell & Partelemo-Barehmi,1999; Ginsburg & Drake, 2002; Mufson et al., 2004; Robinson et al.,2002) at this level had medium effect size estimates, and two studies(Harris & Franklin, 2003; Larkin & Thyer, 1999) had large effect sizes.With the three studies that looked at multiple RTI levels, two of themhad small treatment effects (Eron et al., 2002; CPPRG, 1999, 2002,2004) and one had a medium effect size (Fast et al., 2003).
6. Discussion
The purpose of this article was to assess the frequency with whichteachers are involved in delivering school mental health interven-tions and to assess at what level of intervention school mental healthinterventions are being delivered using an RTI framework. In addi-tion, the efficacy of school mental health interventions implementedwas also evaluated by comparing different personnel involved inthe delivery of school mental health interventions. This review sys-tematically identified mental health interventions that were exam-ined in research studies and that also met the aforementionedinclusion criteria as a school mental health intervention. Only themost recent studies were included because scholars have suggestedthat school policy changes, and more specifically the RTI movement,may be increasing the teamwork between teachers andmental healthprofessionals and increasing teacher involvement in behavioral inter-ventions (Frey et al., 2011). Even though several authors have
suggested that teachers are actively involved in the delivery of schoolmental health interventions (e.g., Anderson-Butcher & Ashton, 2004;Berzin et al., 2011; Frey et al., 2011), the active participation ofteachers in school mental health interventions has not been widelyinvestigated in empirical studies. This current study hopes to addressa gap in this knowledge base, specifically aimed at understandingwho is delivering school mental health interventions and how effec-tive these services may prove to be.
This current review found that out of 49 school mental healthstudies analyzed, teachers were actively involved in 40.8% of mentalhealth interventions evaluated and were the sole providers of inter-ventions in 18.4% of the studies. It was also found that many ofthese school mental health interventions were universal (Tier 1)and took place in the classrooms. This Tier 1 focus may also partly ex-plain the active involvement of teachers in a relatively high percent-age of these interventions. These findings suggest that teachers havebeen actively involved in school mental health interventions andthat they are more likely to work as a team with other professionalsthan as sole providers of these interventions. However, they may bethe primary deliverer of a smaller percentage of school mental healthinterventions. The school-based service literature has suggested thatteachers are increasingly involved in school mental health servicesdue to the implementation of the RTI framework and school wide be-havioral supports that support their involvement (Berzin et al., 2011;Frey et al., 2011; Kelly et al., 2010). While these findings cannot con-firm or disconfirm how wide spread teacher involvement may be inschool mental health services, the data indicates that out of the stud-ies examined over the past ten years, that teachers served as collabo-rators in a respectable percentage of school mental healthinterventions (40.8%)
6.1. School mental health outcomes
The overall results of this study suggest that there is no wide var-iation in outcomes between different school mental health studies,regardless of which personnel may be implementing the interven-tions. In this regard, studies involving teachers as sole providers ofmental health services and those studies that involved teachers ascollaborators on mental health teams had fairly equivocal resultswith most studies having small effect sizes, and only a few studies of-fered medium and large effect sizes. The results from studies whereteachers were involved in the implementation of school mentalhealth interventions were also fairly equivocal with those that weredelivered by mental health professionals, and there did not seem tobe a clear advantage of one type of personnel over another. Eventhough this study found no differences between different personnelthat delivered the mental health interventions, the overall findingsfor this outcome remain mixed across different studies. Similar tothis study, for example, some researchers have found that teachersmay effectively administer school-based, mental health services (i.e.Wilson et al., 2003 & Wilson & Lipsey, 2007). In another systematicreview (Baskin et al., 2010), however, researchers found that para-professionals such as teachers and parents did not achieve as largeof effect sizes as licensed mental health professionals. Furthermore,results from the Baskin review indicated that studies using graduate

980 C.G.S. Franklin et al. / Children and Youth Services Review 34 (2012) 973–982
interns, whether alone or in combination with professional clinicians,had fairly equivocally small effect size results. This current study dif-fers further from Baskin and colleagues' (2010) study in that the out-comes from students and interns were weaker than those found forprofessionals (whether they were teachers or clinicians).
One possibility for why licensed professionals appeared to do bet-ter in Baskin and colleagues' (2010) study may have been the focuson psychotherapy verses broader types of psychosocial interventionsand also the grouping of teachers with parents. In this current study,for example, there was a higher percentage (18.4%) of articles includ-ed where teachers were the sole providers of the mental health inter-ventions, and also worked together in teams with other mental healthprofessionals instead of paraprofessionals or lay people. This differ-ence may have served to elevate the outcomes of teachers withinthe studies. Since different studies offer contradictory results regard-ing the outcomes of different personnel delivering school mentalhealth interventions, future studies will have to clarify the effective-ness of different professionals.
6.2. Professional roles and levels of intervention
This study suggests that the levels of intervention delivered maydiffer between professionals, with teachers (alone), delivering almostexclusively Tiers 1 and 2 interventions (7 studies) and mental healthprofessionals (alone) delivering more of the Tier 3 selective interven-tions (7 studies). The greatest crossover between teachers andmentalhealth professionals is in the universal and indicated categories, withmental health professionals being most distinguished from teachersby delivering slightly more indicated interventions, yet usually work-ing on the first two levels as partners with teachers. This suggests thatwhen empirically evaluating school mental health studies, it might beimportant to assess who is most involved at what level of interven-tion and also to look more closely at the roles of different profes-sionals involved in the delivery of school mental health services. Inorder to better understand professional roles in school mental healthservices and the levels of intervention, future studies will need toevaluate in more depth the roles of teachers and other professionalsin relationship to the RTI framework.
6.3. Limitations
This study has several limitations including its descriptive natureand the large number of studies that did not meet the final inclusioncriteria to be included in the review. As the results on Fig. 1 show,around 1500 studies met our initial criteria for inclusion but only 49studies met all the necessary requirements for inclusion in our re-view. While this type of big exclusion of studies is quite common insystematic reviews, it's clear that there are still potentially importantstudies that were not included because of research design issues orinsufficient data to calculate effect sizes. Also, many of the studies inschool settings are using advanced multilevel modeling and structur-al equation modeling analysis which makes calculating effect sizesvery complicated, if not impossible, depending on the data provided.Authors of future studies should report effect sizes for between andwithin group contrasts. Caution should also be warranted when gen-eralizing these results because many of the effect size results from thestudies were based on combining multiple outcome measures whichcan lead to oversimplified interpretations andmask subtle differencesfound between various outcomes. Furthermore, the comparisons ofeffect sizes across the various professionals who provided the inter-ventions were limited statistically, as we were unable to examinethese results through a mixed-effects model using teacher as a pre-dictor variable. Despite these limitations, the current study looks sys-tematically at a large number of school mental health studies andevaluated the participation of teachers in the implementation of men-tal health interventions and shows important results. Future studies
may wish to conduct a more comprehensive meta-analysis on the ef-fects of teacher mental health interventions and their specific roles asthe providers of these services.
7. Conclusion
Schools are large providers of mental health services for childrenand adolescents Adelman & Taylor, 2010; Hoagwood et al., 2007;Stormont, Reinke, & Herman, 2011). Recent educational policy initia-tives at the Federal level have ushered in RTI and school-wide behav-ior supports that have potential to involve teachers in school mentalhealth interventions. The results of this ten-year review suggest thatteachers are not only involved in the delivery of school mental healthinterventions mostly as team members with other school mentalhealth professionals, but also less frequently may serve as the soleproviders of these interventions. Consistent with what has been sug-gested in other literature (Berzin et al., 2011; Frey et al., 2011;O'Connor, 2003; Tilly, Reschly, & Grimes, 1999) this study indicatesthat mental health professionals, such as school social workers andpsychologists, may take on more of a clinical practitioner role in thedelivery of Tier 3 interventions. They may also support teachers orwork as a team with them when delivering school mental health in-terventions at Tiers 1 and 2 levels. Although this current review con-tributes empirical knowledge documenting the involvement ofteachers with school mental health services, it also indicates that fur-ther research is needed to understand and clarify the efficacy associ-ated with the roles that both mental health professionals andteachers play in offering the most effective mental health services tostudents in school settings.
References
Adelman, H. S., & Taylor, L. (2010). Mental health in schools: Engaging learners, prevent-ing problems, and improving schools. Thousand Oaks, CA: Corwin.
Adi, Y., Killoran, A., Janmohamed, K., & Stewart-Brown, S. (2007). Systematic review ofthe effectiveness of interventions to promote mental wellbeing in primary schools:Universal approaches which do not focus on violence or bullying. London: NationalInstitute for Clinical Excellence.
Anderson-Butcher, D., & Ashton, D. (2004). Innovative models of collaboration to servechildren, youth, families, and communities. Children and Schools, 1, 39–53.
*Armbruster, P., & Lichtman, J. (1999). Are school based mental health services effec-tive? Evidence from 36 inner city schools. Community Mental Health Journal, 35,493–504, doi:10.1023/a:1018755100381.
*Asarnow, J. R., Scott, C. V., & Mintz, J. (2002). A combined cognitive–behavioral familyeducation intervention for depression in children: A treatment development Study.Cognitive Therapy and Research, 26, 221–229, doi:10.1023/a:1014573803928.
Baskin, T. W., Slaten, C. D., Sorenson, C., Glover-Russell, J., & Merson, D. N. (2010). Doesyouth psychotherapy improve academically related outcomes? A meta-analysis.Journal of Counseling Psychology, 57, 290–296.
*Bauer, N. S., Lozano, P., & Rivara, F. P. (2007). The effectiveness of the olweus bullyingprevention program in public middle schools: A controlled trial. The Journal of Ad-olescent Health, 40, 266–274, doi:10.1016/j.jadohealth.2006.10.005.
Berzin, S. C., O'brien, Khm, Frey, A., Kelly, Ms, Alvarez, M. E., & Shaffer, G. L. (2011).Meeting the social and behavioral health needs of students: Rethinking the rela-tionship between teachers and school social workers. The Journal of School Health,81, 493–501.
*Bohman, T. M., Barker, E. D., Bell, M. L., Lewis, C. M., Holleran, L., & Pomeroy, E. (2004).Early intervention for alcohol use prevention and vehicle safety skills: Evaluatingthe “Protecting You/Protecting Me” Curriculum. Journal of Child & Adolescent Sub-stance Abuse, 14, 17–40.
Borenstein, M., Hedges, L., Higgins, J., & Rothstein, H. R. (2005). Comprehensive metaanalysis, version 2. Englewood, NJ: Biostat, Inc..
*Botvin, G., Griffin, K., Diaz, T., & Ifill-Williams, M. (2001). Preventing binge drinkingduring early adolescence: One- and two- year follow-up of a school-based pre-ventive intervention. Psychology of Addictive Behaviors, 15, 360–365, doi:10.1037/0893-16.
*Bruning Brown, J., Winzelberg, A. J., Abascal, L. B., & Taylor, C. B. (2004). An evalua-tion of an internet-delivered eating disorder prevention program for adolescentsand their parents. The Journal of Adolescent Health, 35, 290–296, doi:10.1016/j.jadohealth.2003.10.010.
*Carbonell, D. M., & Partelemo-Barehmi, C. (1999). Psychodrama groups for girls cop-ing with trauma. International Journal of Group Psychotherapy, 49, 285–306.
*Cardemil, E. V., Reivich, K. J., & Seligman, M. (2002). The prevention of depressivesymptoms in low-incomeminority middle school students. Prevention & Treatment,5, 8.

981C.G.S. Franklin et al. / Children and Youth Services Review 34 (2012) 973–982
*Chemtob, C. M., Nakashima, J., & Carlson, J. G. (2002). Brief treatment for elementaryschool children with disaster-related post traumatic stress disorder: A fieldstudy. Journal of Clinical Psychology, 58, 99–112.
Chitiyo, M., & Wheeler, J. (2009). Challenges faced by school teachers in implementingpositive behavior support in their school systems. Remedial and Special Education,30(1), 58–63, doi:10.1177/0741932508315049.
*Cho, H., Hallfors, D. D., & Sánchez, V. (2005). Evaluation of a high school peer groupintervention for at-risk youth. Journal of Abnormal Child Psychology, 33, 363–374,doi:10.1007/s10802-005-3574-4.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.). Hills-dale NJ: Lawrence Erlbaum.
*Conduct Problems Prevention Research Group. (1999; 2002; 2004). Initial impact ofthe fast track prevention trial for conduct problems: The high risk sample. Journalof Consulting and Clinical Psychology, 67, 631–647.
Cooper, H., & Hedges, L. (1994). The handbook of research synthesis. New York, NY: Rus-sel Sage Foundation.
Corcoran, J., & Pillai, V. K. (2007). Effectiveness of secondary pregnancy prevention pro-grams: A meta-analysis. Research on Social Work Practice, 17, 5–20.
*DeRosier, M. E. (2004). Building relationships and combating bullying: Effectivenessof a school-based social skills group intervention. Journal of Clinical Child and Ado-lescent Psychology, 33, 196–201.
Diekstra, R. (2008). Effectiveness of school-based social and emotional education pro-grammes worldwide—Part one, a review of meta-analytic literature. Social andemotional education: An international analysis (pp. 255–284). Santander: FundacionMarcelino Botin.
*Donaldson, S. I., Thomas, C. W., Graham, J. W., Au, J. G., & Hansen, W. B. (2000). Veri-fying drug abuse prevention program effects using reciprocal best friend reports.Journal of Behavioral Medicine, 23, 585–601, doi:10.1023/a:1005559620739.
*Duncan, T. E., Duncan, S. C., Beauchamp, N., Wells, J., & Ary, D. V. (2000). Developmentand evaluation of an interactive CD-ROM refusal skills program to prevent youthsubstance use: “Refuse to use”. Journal of Behavioral Medicine, 23, 59–72, doi:10.1023/a:1005420304147.
Durlak, J. A., Weissberg, R. P., Dymnicki, A. B., Taylor, R. D., & Schellinger, K. (2011). Theimpact of enhancing students' social and emotional learning: A meta-analysis ofschool-based universal interventions. Child Development, 82, 474–501.
Easton, J. E., & Erchul, W. P. (2011). An exploration of teacher acceptability of treatmentplan implementation: Monitoring and feedback methods. Journal of Educationaland Psychological Consultation, 21(1), 56–77.
*Eron, L., Huesmann, R., Spindler, A., Guerra, N., Henry, D., & Tolan, P. (2002). Acognitive-ecological approach to preventing aggression in urban settings: Initialoutcomes for high-risk children. Journal of Consulting and Clinical Psychology, 70,179–194, doi:10.1037/0022-006X.70.1.179.
Fairbanks, S., Simonsen, B., & Sugai, G. (2008). Classwide secondary and tertiary tierpractices and systems. Teaching Exceptional Children, 40, 44–52.
*Fast, J., Fanelli, F., & Salen, L. (2003). How becoming mediators affects aggressive stu-dents. Children and Schools, 25, 161–171.
Feinstein, N. R., Fielding, K., Udvari-Solner, A., & Joshi, S. V. (2009). The supporting al-liance in child and adolescent treatment: Enhancing collaboration among thera-pists, parents, and teachers. American Journal of Psychotherapy, 63, 319–344.
*Flay, B. R., Allred, C. G., & Ordway, N. (2001). Effects of the positive action program onachievement and discipline: Two matched-control comparisons. Prevention Sci-ence, 2, 71–89.
Foster, S., Rollefson, M., Doksum, T., Noonan, D., Robinson, G., & Teich, J. (2005). Schoolmental health services in the United States, 2002–2003. DHHS Pub. No. (SMA) 05-4068. Rockville, MD: Center for Mental Health Services, Substance Abuse and Men-tal Health Services Administration.
Franklin, C., Kim, J., & Tripodi, S. J. (2009). A meta-analysis of published school socialwork practice studies: 1980–2007. Research on Social Work Practice, 19, 667–677.
*Franklin, C., Moore, K., & Hopson, L. M. (2008). Effectiveness of solution-focused brieftherapy in a school setting. Children and Schools, 30, 15–26.
*Frey, A. (2002). Enhancing children's social skills through classroom meetings. SchoolSocial Work Journal, 26, 46–57.
Frey, A., Lingo, A., & Nelson, C. M. (2011). Positive behavior support and response to in-tervention in elementary schools. In H. Walker, & M. K. Shinn (Eds.), Interventionsfor achievement and behavior problems: Preventive and remedial approaches(pp. 397–433). : National Association for School Psychologists.
Fuchs, D., & Fuchs, L. F. (2006). Introduction to response to intervention: What, why,and how valid is it? Reading Research Quarterly, 41, 93–100.
*Gillham, J., Reivich, K., Freres, D., Chaplin, T., Shatté, A., Samuels, B., et al. (2007).School-based prevention of depressive symptoms: A randomized controlledstudy of the effectiveness and specificity of the penn resiliency program. Journalof Consulting and Clinical Psychology, 75, 9–19, doi:10.1037/0022-006X.75.1.9.
*Ginsburg, G. S., & Drake, K. L. (2002). School-based treatment for anxious Africa Amer-ican adolescents: A controlled pilot study. Journal of the American Academy of Childand Adolescent Psychiatry, 41, 68–75.
*Gottfredson, Jones, & Gore (2002). Implementation and evaluation of a cognitive–be-havioral intervention to prevent problem behavior in a disorganized school. Pre-vention Science, 3, 43–56.
Gresham, F. M. (2005). Response to intervention: An alternative means of identifying stu-dents as emotionally disturbed. Education and Treatment of Children, 28, 328–344.
*Hallfors, D., Cho, H., Sanchez, V., Khatapoush, S., Kim, H., & Bauer, D. (2006). Efficacy vseffectiveness trial results of an indicated ‘model’ substance abuse program: Impli-cations for public health. American Journal of Public Health, 96, 2254–2259, doi:10.2105/AJPH.2005.067462.
*Hardin, S. B., Weinrich, Sally, Weinrich, Martin, Garrison, Carol, Addy, Cheryl, &Hardin, Thomas L. (2002). Effects of a long-term psychosocial nursing intervention
on adolescents exposed to catastrophic stress. Issues in Mental Health Nursing, 2,537–551, doi:10.1080/0161284029005271 2.
*Harris, M. B., & Franklin, C. (2003). Effects of a cognitive–behavioral, school-based,group intervention with Mexican American pregnant and parenting adolescents.Social Work Research, 27, 71–83.
*Hawkins, D. J., Catalano, R. F., Kosterman, R., Abbott, R., & Hill, K. G. (1999). Preventingadolescent health risk behaviors by strengthing protection during childhood. Ar-chives of Pediatrics & Adolescent Medicine, 153, 226–234.
Hawkins, S. M., & Heflin, L. (2011). Increasing secondary teachers' behavior-specificpraise using a video self-modeling and visual performance feedback intervention.Journal of Positive Behavior Interventions, 13, 97–108.
Helker, W. P., Schottelkorb, A. A., & Ray, D. (2007). Helping students and teachers CON-NECT: An intervention model for school counselors. Journal of Professional Counsel-ing: Practice, Theory, & Research, 35, 31–45.
*Hennessey, B. A. (2007). Promoting social competence in school-aged children: Theeffects of the Open Circle Program. Journal of School Psychology, 45, 349–360.
*Herrmann, D. S., & McWhirter, J. J. (2003). Anger & aggression management in youngadolescents: An experimental validation of the SCARE program. Education andTreatment of Children, 26, 273–302.
Hester, P. P., Baltodano, H. M., Hendrickson, J. M., Tonelson, S. W., Conroy, M. A., &Gable, R. A. (2004). Lessons learned from research on early intervention: Whatteachers can do to prevent children's behavior problems. Preventing School Failure,49, 5–10.
Hoagwood, K. E., Olin, S. S., Kerker, B. D., Kratochwill, T. R., Crowe, M., & Saka, N. (2007).Empirically based school interventions targeted at academic and mental healthfunctioning. Journal of Emotional and Behavioral Disorders, 15, 66–92.
Hoover, J. J., Baca, L., Wexler-Love, E., & Saenz, L. (2008). National implementation of Re-sponse to Intervention (RTI): Research summary. Retrieved on August 28, 2011from. http://www.spannj.org/pti/NationalImplementationofRTI-ResearchSummary.pdf
Horner, R. H., Sugai, G., Smolkowski, K., Eber, L., Nakasato, J., Todd, A. W., et al. (2009). Arandomized, wait-list controlled effectiveness trial assessing school-wide positivebehavior supporting elementary schools. Journal of Positive Behavior Interventions,11, 133–144.
*Ialongo, N., Poduska, J., Werthamer, L., & Kellam, S. (2001). The distal impact of twofirst-grade preventive interventions on conduct problems and disorder in early ad-olescence. Journal of Emotional and Behavioral Disorders, 9, 146–160.
*Jaycox, L. H., McCaffrey, D., Eiseman, B., Aronoff, J., Shelley, G. A., Collins, R. L., et al.(2006). Impact of a school-based dating violence prevention program among Lati-no teens: Randomized controlled effectiveness trial. The Journal of AdolescentHealth, 39, 694–704, doi:10.1016/j.jadohealth.2006.05.002.
*Jenson, J., & Dieterich, W. (2007). Effects of a skills-based prevention program on bul-lying and bully victimization among elementary school children. Prevention Sci-ence, 8, 285–296, doi:10.1007/s11121-007-0076-3.
*Kataoka, S. H., Stein, B. D., Jaycox, L. H., Wong, M., Escudero, P. I. A., Tu, W., et al.(2003). A school-based mental health program for traumatized Latino immigrantchildren. Journal of the American Academy of Child and Adolescent Psychiatry, 42,311–318, doi:10.1097/00004583-200303000-00011.
Kelly, M. S. (2008). The demands and domains of school social work. New York, NY: Ox-ford University Press.
Kelly, M. S., Raines, J. C., Stone, S., & Frey, A. (2010). School social work: An evidence-informed framework for practice. New York: Oxford University Press.
*Ko, S., & Cosden, M. (2001). Do elementary school-based child abuse prevention pro-grams work: A high school follow-up. Psychology in the Schools, 38, 57.
*Kumpfer, K., Alvarado, R., Tait, C., & Turner, C. (2002). Effectiveness of school-basedfamily and children's skills training for substance prevention among 6–8 year-oldrural children. Psychology of Addictive Behaviors, 16, S65–S71, doi:10.1037/0893-164X.16.4S.S65.
Lane, K. L., Weisenbach, J. L., Little, M., Phillips, A., & Wehby, J. (2006). Illustrations offunction-based interventions implemented by general education teachers: Build-ing capacity at the school site. Education and Treatment of Children, 29, 549–571.
*Larkin, R., & Thyer, B. A. (1999). Evaluating cognitive-behavioral group counseling toimprove elementary school students' self-esteem, self-control and classroom be-havior. Behavioral Interventions, 14, 147–161.
Leflot, G., van Lier, P. C., Onghena, P., & Colpin, H. (2010). The role of teacher behaviormanagement in the development of disruptive behaviors: An intervention studywith the good behavior game. Journal of Abnormal Child Psychology: An official pub-lication of the International Society for Research in Child and Adolescent Psychopathol-ogy, 38, 869–882.
Lindsey, B. C., White, M., & Korr, W. S. (2006). Conducting in-service training and con-tinuing education for staff and teachers. In C. Franklin, M. B. Harris, & P. Allen-Meares (Eds.), School services sourcebook. New York: Oxford University Press.
Lipsey, R. E. (1994). Quality change and other influences on measures of export prices ofmanufactured goods. Policy Research Working Paper Series, 1438, : The WorldBank.
Lipsey, M. W., & Wilson, D. B. (2001). Practical meta-analysis, Vol. 49, Thousand Oaks,CA: Sage Publications.
Littell, J. H., Corcoran, J., & Pillai, V. (2008). Systematic reviews and meta-analysis. NewYork: Oxford University Press.
*McWhirter, B. T., & Page, G. L. (1999). Effects of anger management and goal settinggroup interventions on state-trait anger and self-efficacy beliefs among high riskadolescents. Current Psychology, 18, 223–237.
*Melnyk, B., Jacobson, D., Kelly, S., O'Haver, J., Small, L., & Mays, M. (2009). Improvingthe mental health, healthy lifestyle choices, and physical health of Hispanic adoles-cents: A randomized controlled pilot study. The Journal of School Health, 79,575–584.

982 C.G.S. Franklin et al. / Children and Youth Services Review 34 (2012) 973–982
*Mufson, L., Pollack, K., Wickramaratne, P., Nomura, Y., Olfson, Y., & Weissman, M. M.(2004). A randomized effectiveness trial of interpersonal psychotherapy for de-pressed adolescents. Archives of General Psychiatry, 61, 577–584.
*Murray, C., & Malmgren, K. (2005). Implementing a teacher–student relationship pro-gram in a high-poverty urban school: Effects on social, emotional, and academicadjustment and lessons learned. Journal of School Psychology, 43, 137–152.
Murray, D. W., Rabiner, D., Schulte, A., & Newitt, K. (2008). Feasibility and integrity of aparent–teacher consultation intervention for ADHD students. Child & Youth CareForum, 37(3), 111–126.
Myers, D. M., Simonsen, B., & Sugai, G. (2011). Increasing teachers' use of praise witha response-to-intervention approach. Education and Treatment of Children, 34,35–59.
O'Connor, R. (2003, December). Tiers of intervention in kindergarten through thirdgrade. Presented at the National Research Center on Learning DisabilitiesResponsiveness-to-Intervention Symposium, Kansas City, MO.
*Pedro-Carroll, J. L., Sutton, S. E., & Wyman, P. A. (1999). A two year follow up evalua-tion of a preventative intervention for young children of divorce. School PsychologyReview, 28, 467–476.
Perry, P. D. (1997). Realities of the effect size calculation process: Considerations forbeginning meta-analysts. In W. J. Bukoski (Ed.),Meta-analysis of drug abuse preven-tion programs. NIDA Report, 170. (pp. .165–.182) Rockville, MD: National Instituteon Drug Abuse.
Pierce, C. D., Reid, R., & Epstein, M. H. (2004). Teacher-mediated interventions for chil-dren with EBD and their academic outcomes: A review. Remedial and Special Edu-cation, 25, 175–188.
*Post, P. (1999). Impact of child-centered play therapy on the self-esteem, locus of con-trol, and anxiety of at-risk 4th, 5th, and 6th grade students. International Journal ofPlay Therapy, 8, 1–18.
Richards, C., Pavri, S., Golez, F., Canges, R., & Murphy, J. (2007). Response to interven-tion: building the capacity of teachers to serve students with learning difficulties.Issues in Teacher Education, 16, 55–64.
Ringwalt, C. L., Pankratz, M. M., Jackson-Newsom, J., Gottfredson, N. C., Hansen, W. B.,Giles, S. M., et al. (2010). Three-year trajectory of teachers' fidelity to a drug pre-vention curriculum. Prevention Science, 11, 67–76.
*Robinson, T. R., Smith, S. W., & Miller, M. D. (2002). Effect of a cognitive–behavioral in-tervention on responses to anger by middle school students with chronic behaviorproblems. Behavioral Disorders, 27, 256–271.
Rones, M., & Hoagwood, K. (2000). School-based mental health services: A research re-view. Clinical Child and Family Psychological Review, 3, 223–241.
Sabatino, C. A. (2009). School social work consultation models and response to inter-vention: A perfect match. Children & Schools, 31, 197–206.
Shadish, W. R., & Haddock, C. K. (1994). Combining estimates of effect size. In C. Harris,& H. Larry (Eds.), The handbook of research synthesis (pp. 97–109). New York: Rus-sell Sage Foundation.
Simonsen, B., Shaw, S. F., Faggella-lubym Sugai, G., Coyne, M. D., & Alfano, M. (2010). Aschool-wide model for service delivery: Redefining special educators as Interven-tionist. Remedial and Special Education, 31, 17–23.
Smolak, L., Harris, B., Levine, M. P., & Shisslak, C. M. (2001). Teachers: The forgotten in-fluence on the success of prevention programs. Eating Disorders: The Journal ofTreatment & Prevention, 9, 261–265.
*Stein, B., Jaycox, L., Kataoka, S., Wong, M., Tu, W., Elliott, M., et al. (2003). A mentalhealth intervention for schoolchildren exposed to violence: A randomized con-trolled trial. Journal of the American Medical Association, 290, 603–611, doi:10.1001/jama.290.5.603.
Stormont, M., Lewis, T. J., Beckner, R., & Johnson, N. W. (2008). Implementing systems ofpositive behavior support systems in early childhood and elementary settings. Thou-sand Oaks, CA: Corwin Press.
Stormont, M., Reinke, W., & Herman, K. (2011). Teachers' knowledge of evidence-basedinterventions and available school resources for children with emotional and be-havioral problems. Journal of Behavioral Education, 20, 138–147.
Substance Abuse and Mental Health Services Administration (2007). Results from the2006 National Survey on Drug Use and Health: National Findings (Office of AppliedStudies, NSDUH Series H-32, DHHS Publication No. SMA 07-4293). Rockville, MD.
Tillery, A., Varjas, K., Meyers, J., & Collins, A. (2010). General education teachers' per-ceptions of behavior management and intervention strategies. Journal of PositiveBehavior Interventions, 12, 86–102.
Tilly, W. D., Reschly, D. J., & Grimes, J. (1999). Disability determination in problem-solving systems: Conceptual foundations and critical components. In D. Reschly,W. D. Tilly, & J. Grimes (Eds.), Special education in transition: Functional assessmentand noncategorical programming. Longmont, CO: Sporis West.
Vaughn, S., & Fuchs, L. (2003). Redefining learning disabilities as inadequate responseto instruction: The promise and potential problems. Learning Disabilities Researchand Practice, 18, 137–146.
*Viggiani, P. A., Reid, W. J., & Bailey-Dempsey, C. (2002). Social worker-teacher collab-oration in the classroom: Help for elementary students at risk of failure. Researchon Social Work Practice, 12, 604–620.
*Walker, D., Roffman, R., Stephens, R., Wakana, K., & Berghuis, J. (2006). Motivationalenhancement therapy for adolescent marijuana users: A preliminary randomizedcontrolled trial. Journal of Consulting and Clinical Psychology, 74, 628–632, doi:10.1037/0022-006X.74.3.628.
*Weiss, B., Harris, V., Catron, T., & Han, S. (2003). Efficacy of the RECAP interventionprogram for children with concurrent internalizing and externalizing problems.Journal of Consulting and Clinical Psychology, 71, 364–374, doi:10.1037/0022-006X.71.2.364.
Weist, M. D., & Paternite, C. E. (2006). Building an interconnected policy-training-practice-research agenda to advance school mental health. Education and Treat-ment of Children, 29, 173–196.
*Werch, C., Bian, H., DiClemente, C., Moore, M., Thombs, D., Ames, S., et al. (2010). Abrief image-based prevention intervention for adolescents. Psychology of AddictiveBehaviors, 24, 170–175, doi:10.1037/a0017997.
Wilson, S. J., & Lipsey, M. W. (2007). School-based interventions for aggressive and dis-ruptive behavior: Update of a meta-analysis. American Journal of Preventive Medi-cine, 33, 130–143.
Wilson, S. J., Lipsey, M. W., & Derzon, J. H. (2003). The effects of school-based programson aggressive behavior: A meta-analysis. Journal of Consulting and Clinical Psychol-ogy, 71, 136–149.
Wolmer, L., Hamiel, D., & Laor, N. (2011). Preventing children's prosttaumatic stressafter disaster with teacher-based intervention: A controlled study. Journal of theAmerican Academy of Child and Adolescent Psychiatry, 50, 340–348.
*Yampolskaya, S., Brown, E., & Vargo, A. (2004). Assessment of teen pregnancy preven-tion interventions among middle school youth. Child and Adolescent Social WorkJournal, 21, 69–83, doi:10.1023/B:CASW.0000012349.79750.b6.
*Zubernis, L. S., Cassidy, K. W., Gillham, J. E., Reivich, K. J., & Jaycox, L. H. (1999). Pre-vention of depressive symptoms in preadolescent children of divorce. Journal ofDivorce & Remarriage, 30, 11–36.