Embed Size (px)
Citation preview
Teaching Communication Skills at the Bedside
September 19, 2014
Michael D. Barnett, MD, MS
Laurel B. Kilpatrick, MD
Objectives
1. To appreciate the importance of
communication in the medical encounter &
barriers to effective bedside teaching.
2. To explain the framework approach to
communication skills training.
3. To describe the coaching model and its
applicability to bedside teaching.
4. To demonstrate the use of coaching in
bedside communication teaching.

Good Communication
Numerous studies have shown that good patient-
doctor communication leads to good outcomes:
Patient satisfaction
Family satisfaction
Provider satisfaction
Symptom control
Efficiency
Medico-legal issues
Utilization & costs
Non-adherence
Provider burnout
Mandate
Communication skills training is required in
graduate medical education:
IV.A.5.d) Residents must demonstrate
interpersonal and communication skills that result
in the effective exchange of information and
collaboration with patients, their families, and
health professionals.
ACGME Common Program Requirements
Needs Assessment
Learners actually want more training in
communication skills:
• Discussing bad news
• Discussing prognosis
• Discussing code status
Kolarik R. Pediatrics. 2006; 117(6):1949-54
Michelson KN, et al. J Palliat Med. 2009; 12(5):451-7.
Various Curricula
• 5-hour workshop during 2-day retreat for Medicine
residents @ Duke Alexander SC, et al. Acad Med. 2006; 81(11):1008-12.
• 2-year series of 3-hour workshops for General
Surgery residents @ UMass Larkin AC, et al. J Am Coll Surg. 2010; 211:285-92.
• 12 one-hour sessions with Oncology fellows @ MD
Anderson Epner DE & Baile WF. Acad Med. 2014; 89:578-84.
• 3-day retreat for Neonatology fellows @ UPMC Boss RD, et al. J Perinatol. 2013; 33(8):642-6.
What are barriers to communication
teaching at the bedside?
Potential Barriers
• Lack of faculty training
• Faculty discomfort
• Learners overwhelmed by biomedical
aspects of care
• Learners lack motivation
• Competing demands
• Lack of time
Perron NJ, et al. Med Teacher. 2009; 31:e316-22.
Learning Theory
I hear and I forget
I see and I remember
I do and I understand.
~ Confucius (551-479 BC)
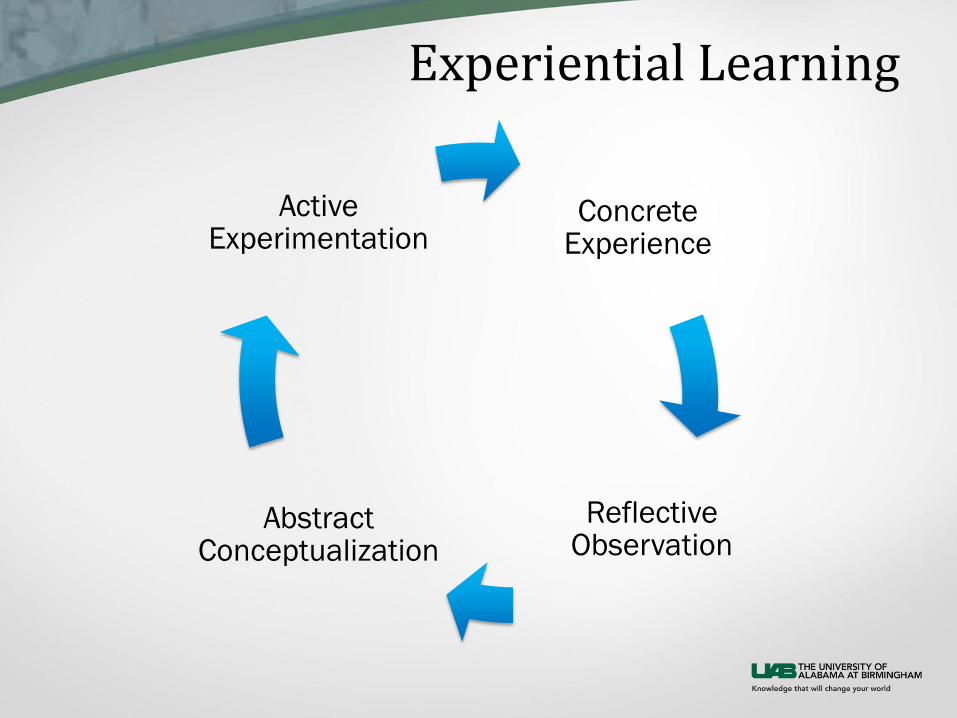
Experiential Learning
Concrete Experience
Reflective Observation
Abstract Conceptualization
Active Experimentation
Premises
1. Communication is essential to the patient-
doctor relationship.
2. Communication is comprised of a series of
specific skills.
3. Communication skills can be taught.
4. Communication experience may be a poor
teacher.
Imperfect Practice
Learners often revert to collecting and/or
exchanging medical information:
• Faculty rarely observe learners
• Learners rarely observe faculty
• “OSCE mentality”
• Communication not seen as “real” medicine
Kurtz, S, et al. Teaching and Learning Communication Skills in Medicine. San
Francisco, CA: Radcliffe Publishing, 2009.
Adult Learning
• Scaffolding
• Contiguity/Anchored learning
• Segmentation
• Desirable difficulties/Goldilocks principle
• Manageable cognitive load
• Self-generation/Discovery
• Feedback
National Research Council Commission on Behavioral & Social Sciences &
Education. How People Learn: Brain, Mind, Experience, and School. Washington,
DC: National Academy Press, 2000.
Ambrose SA, et al. How Learning Works: Seven Research-Based Principles for
Smart Teaching. San Francisco, CA: Jossey-Bass, 2010.

Communication Skills

What are good communication skills?
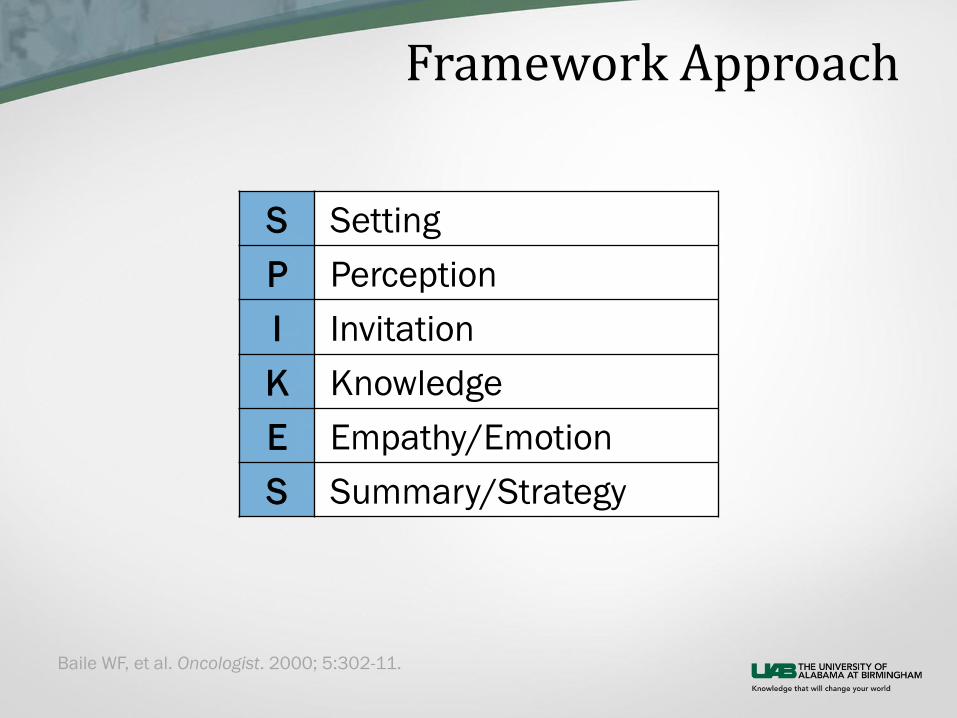
Framework Approach
S Setting
P Perception
I Invitation
K Knowledge
E Empathy/Emotion
S Summary/Strategy
Baile WF, et al. Oncologist. 2000; 5:302-11.
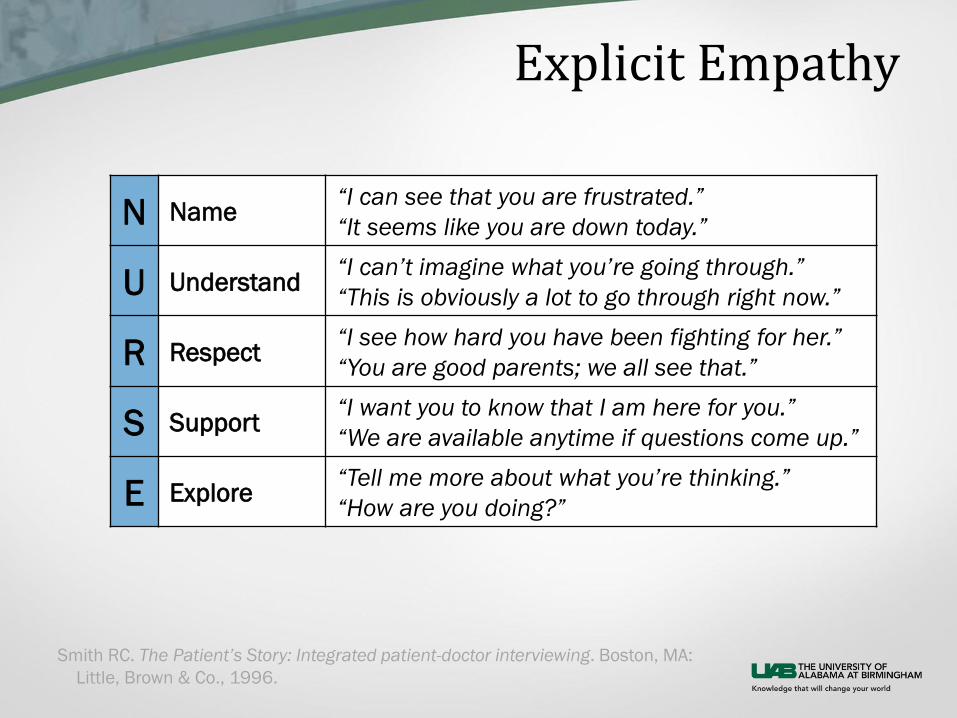
Explicit Empathy
N Name “I can see that you are frustrated.”
“It seems like you are down today.”
U Understand “I can’t imagine what you’re going through.”
“This is obviously a lot to go through right now.”
R Respect “I see how hard you have been fighting for her.”
“You are good parents; we all see that.”
S Support “I want you to know that I am here for you.”
“We are available anytime if questions come up.”
E Explore “Tell me more about what you’re thinking.”
“How are you doing?”
Smith RC. The Patient’s Story: Integrated patient-doctor interviewing. Boston, MA:
Little, Brown & Co., 1996.
Coaching
Tenets
• Learner-centered relationship
• Safe learning environment
• Honest feedback
• Accountability (results-focused)
West L & Staub FC. Content-Focused Coaching: Transforming Mathematics
Lessons. Portsmouth, ME: Heinemann, 2003.
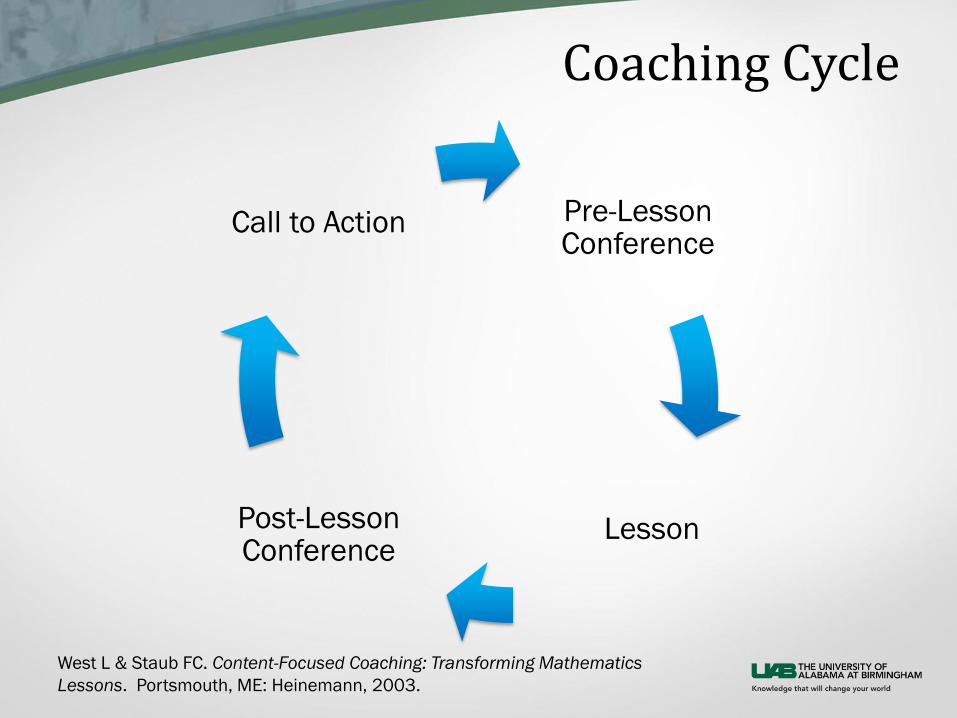
Coaching Cycle
Pre-Lesson Conference
Lesson Post-Lesson Conference
Call to Action
West L & Staub FC. Content-Focused Coaching: Transforming Mathematics
Lessons. Portsmouth, ME: Heinemann, 2003.
Demonstration

Coaching at the Bedside
1. Ask learner for specific skill to practice (plan) – Guide learner to doable skill based on prior experience
2. Observe learner in action (practice) – Take notes of phrases used & reactions from patients/families
3. Debrief the encounter (reflect) – Guide towards a learning point (clarify “stuck” point)
– Highlight specific skills that learner did well
– Brainstorm skills/phrases to use in the future
4. Ask learner for “take home point” (call to action)
Adapted from “Steps in Primary Teaching Method of the Introduction to Medical
Interviewing Course” by William Cohen, MD of the University of Pittsburgh School of
Medicine.
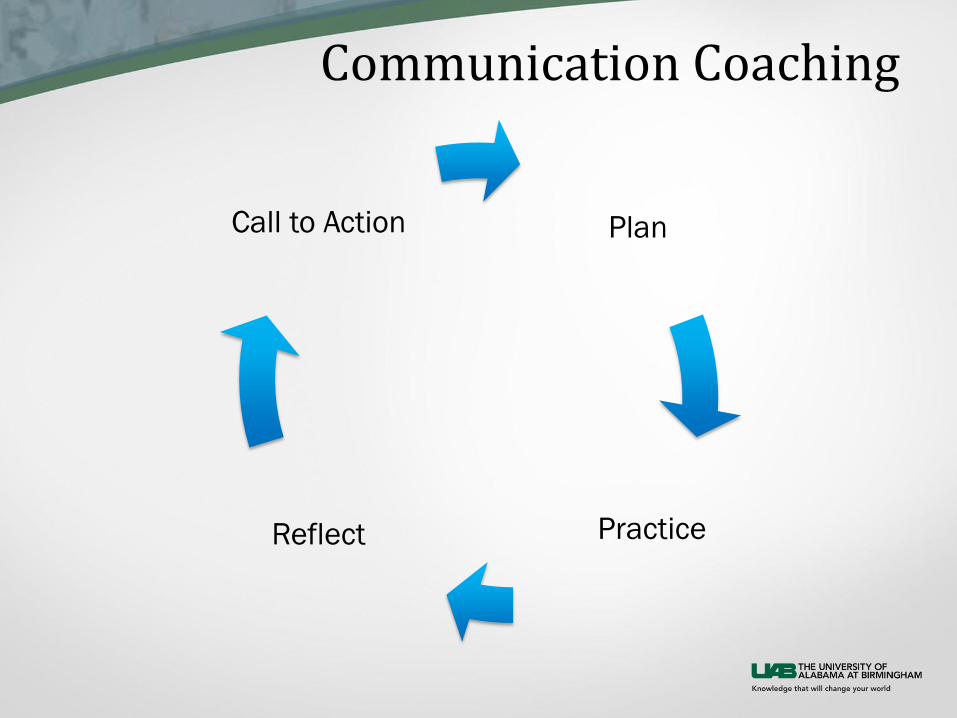
Communication Coaching
Plan
Practice Reflect
Call to Action
Practice
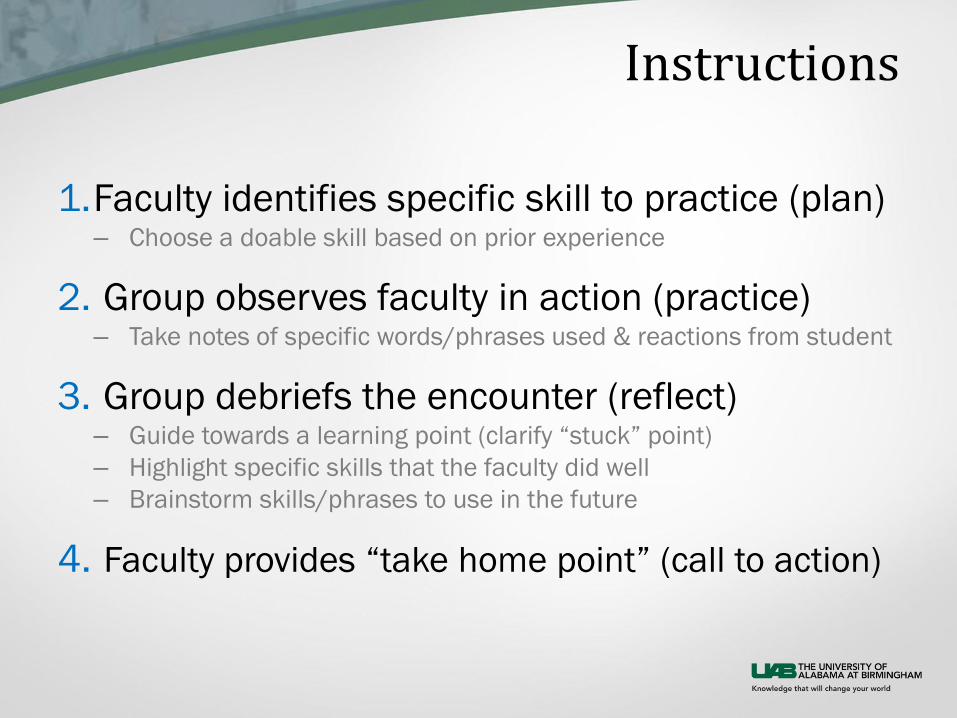
Instructions
1.Faculty identifies specific skill to practice (plan) – Choose a doable skill based on prior experience
2. Group observes faculty in action (practice) – Take notes of specific words/phrases used & reactions from student
3. Group debriefs the encounter (reflect) – Guide towards a learning point (clarify “stuck” point)
– Highlight specific skills that the faculty did well
– Brainstorm skills/phrases to use in the future
4. Faculty provides “take home point” (call to action)
Pearls
• Keep it learner-centered.
• Be specific.
• Pay attention to emotion of learner.
• Highlight the positives.
• Be careful giving your opinion.
• Remember to get a take home point.
Summary
• Communication is essential to the patient-
doctor relationship & should be a regular
part of our teaching.
• A framework approach helps to guide
learners & teachers.
• Communication teaching can be done
quickly & effectively at the bedside.
• A coaching model can help all of us teach
communication in a learner-centered,
experiential manner.
Questions?

![[PPT]Slide 1d2j7fjepcxuj0a.cloudfront.net/meetings/ttt2014/... · Web viewBedside Teaching the most important methods of teaching the most neglected and most deficient Bedside teaching](https://img.pdfslide.net/doc/110x75/5af9c6ef7f8b9ad2208e516a/pptslide-viewbedside-teaching-the-most-important-methods-of-teaching-the-most.jpg)



























