Embed Size (px)
Citation preview

RESEARCH ARTICLE Open Access
Teaching history taking to medicalstudents: a systematic reviewKatharina E. Keifenheim1*, Martin Teufel1, Julianne Ip2, Natalie Speiser1, Elisabeth J. Leehr1, Stephan Zipfel1,3
and Anne Herrmann-Werner1
Abstract
Background: This paper is an up-to-date systematic review on educational interventions addressing historytaking. The authors noted that despite the plethora of specialized training programs designed to enhancestudents‘ interviewing skills there had not been a review of the literature to assess the quality of each publishedmethod of teaching history taking in undergraduate medical education based on the evidence of the program’sefficacy.
Methods: The databases PubMed, PsycINFO, Google Scholar, opengrey, opendoar and SSRN were searched using keywords related to medical education and history taking. Articles that described an educational intervention to improvemedical students’ history-taking skills were selected and reviewed. Included studies had to evaluate learning progress.Study quality was assessed using the Medical Education Research Study Quality Instrument (MERSQI).
Results: Seventy-eight full-text articles were identified and reviewed; of these, 23 studies met the final inclusion criteria.Three studies applied an instructional approach using scripts, lectures, demonstrations and an online course. Seventeenstudies applied a more experiential approach by implementing small group workshops including role-play,interviews with patients and feedback. Three studies applied a creative approach. Two of these studies made useof improvisational theatre and one introduced a simulation using Lego® building blocks. Twenty-two studiesreported an improvement in students’ history taking skills. Mean MERSQI score was 10.4 (range 6.5 to 14; SD = 2.65).
Conclusions: These findings suggest that several different educational interventions are effective in teaching historytaking skills to medical students. Small group workshops including role-play and interviews with real patients, followedby feedback and discussion, are widespread and best investigated. Feedback using videotape review was also reportedas particularly instructive. Students in the early preclinical state might profit from approaches helping them to focus oninterview skills and not being distracted by thinking about differential diagnoses or clinical management. Theheterogeneity of outcome data and the varied ways of assessment strongly suggest the need for further researchas many studies did not meet basic methodological criteria. Randomized controlled trials using externalassessment methods, standardized measurement tools and reporting long-term data are recommended toevaluate the efficacy of courses on history taking.
Keywords: Undergraduate medical education, Medical students, History taking, Medical history, Medical interview,Interview skills
* Correspondence: [email protected] for Psychosomatic Medicine and Psychotherapy, UniversityHospital of Tuebingen, Osianderstr. 5, 72076 Tübingen, GermanyFull list of author information is available at the end of the article
© 2015 Keifenheim et al. Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, andreproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link tothe Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver(http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Keifenheim et al. BMC Medical Education (2015) 15:159 DOI 10.1186/s12909-015-0443-x

BackgroundIn the course of his or her professional life, a clinicianwill conduct between 100,000 and 200,000 patient inter-views [1, 2]. The medical interview is the most commontask performed by physicians. Thus, for good reason,Engel and Morgan called it “the most powerful and sen-sitive and most versatile instrument available to thephysician” [3]. Scientific discoveries and technologicalinnovations of the last decades fundamentally changeddiagnostics and treatment of diseases. Imaging studiesand laboratory tests seem crucial for an accurate diagno-sis, all the more in times of multidisciplinary treatmentsand overall availability of instrument-based examinations.But neither scientific nor technological advances in medi-cine have changed the fact that a physician’s core clinicalskills are interpersonal [4–6]. Interview skills contributesignificantly to problem detection, diagnostic accuracy,patient and physician satisfaction, patient adjustment tostress and illness, patient recall of information, patient ad-herence to therapy and patient health outcomes [7–11].Accuracy of diagnoses and the establishment of a goodphysician-patient relationship depend on effective com-munication within the medical interview [12, 13]. By themedical history, physicians garner 60–80 % of the infor-mation that is relevant for a diagnosis [13–17] and the his-tory alone can lead to the final diagnosis in 76 % [13].There are different definitions and models of history
taking in the international literature, suggesting a limitedshared understanding of the medical interview. Severalstatements and checklists try to define what qualifies amedical interview as “good” and come to divergent re-sults. One reason might be that history taking is highlycontextual, depending on situation, patient and phys-ician attributes, cultural characteristics and other factors.For example, a “good” medical interview in an emer-gency ward would differ distinctly from a “good” firstinterview in a psychiatric medical practice. Severalauthors refer to the “three-function model” [18] thathighlights gathering data (1), responding to patients’emotions (2) and educating patients and influencingtheir behaviour (3) as main functions of the medicalinterview. Each function is served by a separate set ofskills. Other models focus on risk assessment, collectionof data to make a diagnosis and assessment of patients’available support system [19] as main tasks within themedical interview. The “five step model” [20] links phy-sicians’ patient-centred skills with a more focused pro-ceeding within the interview. Other models emphasisepatient-centeredness even more, describing an equal ex-change of information and shared decision-making [21,22]. Despite this heterogeneity, there seems to be anagreement that in a “good” medical interview, patient-centered techniques must at least complement the trad-itional clinician-centred focused questioning style.
Being a successful communicator has long been seenas part of the “art” of medicine, implying that communi-cation skills were a natural gift with which one was orwas not born [23]. However, some researchers describedthat basic communication skills deteriorate during med-ical education if they are not particularly activated andpractised [24, 25]. Students’ psychosocial interviewingskills especially seem to decline without targeted inter-ventions [7, 19, 25]. This has often been associated withstudents’ growing medical knowledge and concentrationon clinical reasoning and diagnostic skills. On the otherhand, many studies have shown that students, havingpassed specialized history taking skills training, ask rele-vant questions and structure their interviews well. Theyare better at responding appropriately to patients’ verbaland non-verbal cues [26] as well as being able to elicitgreater quantity and quality of information [27, 28].History taking and communication skills programmes
have become cornerstones in medical education overthe past 30 years and are implemented in most US[6],Canadian [8], German [29] and UK [30] medicalschools. National accreditations and expert panel con-sensus guidelines have stressed the importance of edu-cational interventions addressing history taking [31,32]. Today, it is a proven fact that interview skills canbe taught if effective methods are used. Even 25 yearsago, articles and consensus statements outlined the as-sumed essential elements of effective interview skillscourses [33, 34], despite not having much experientialevidence for their recommendations. Since then, manystudies investigated the effectiveness of a multitude ofdifferent educational methods for teaching history tak-ing. But there is still an uncertainty about: which ofthese methods are particularly effective; when in the cur-riculum they should be implemented; or which method isespecially helpful for certain subgroups, for example, maleor female students or not being a native speaker. In viewof this uncertainty, the present systematic review of the lit-erature has been undertaken to collect the currently re-ported knowledge in the field of teaching history taking inorder to make recommendations for curriculum planners,medical teachers and future investigators.
Review objectivesThis review aims to answer the following questions: (1)What interventions to teach history taking to medicalstudents exist? (2) How has the effectiveness of these in-terventions been measured? (3) What is the quality ofevidence for these interventions?
MethodInformation sources and searchThis review process was conducted according to thePRISMA statement [35, 36]. The databases PubMed,
Keifenheim et al. BMC Medical Education (2015) 15:159 Page 2 of 12

PsycINFO and GoogleScholar were searched for articlespublished between January 1990 and June 2014. Handsearches were performed in the reference lists of thesearch results. Additionally, the “grey literature” data-bases opengrey, opendoar and SSRN were searched.Search terms were related to history taking and med-
ical education, using combinations of the following:medical history taking, history-taking, medical communi-cation, medical interview, anamnesis, medical students,medical education and teaching. Search was narrowedto titles and abstracts and terms were searched asMeSH-Terms in PubMed. It was ensured that the searchterms captured the previously published reviews [37, 38]and all relevant studies included in these reviews.
Underlying definition of “history-taking”The authors of this review understand “history-taking”as a way of eliciting relevant personal, psychosocial andsymptom information from a patient with the aim ofobtaining information useful in formulating a diagnosisand providing medical care to the patient. The medicalinterview is seen as an encounter between physician andpatient, both contributing to the results.
Inclusion criteriaArticles were included if the following criteria were met:
– Description of an educational interventionconcerning history taking: This review investigates(introductory) workshops teaching history-taking ingeneral, considering content, completeness, verbaland non-verbal interviewing techniques and rapport.
– Evaluation of learning progress (at least a self-evaluation of students)
– Reporting on undergraduate medical education (i.e.“medical students”)
– Publication dates between January 1, 1990 and June30, 2014
– English- or German-language articles
We also included articles that described teaching unitsaddressing other clinical skills (e.g. physical examinationor clinical reasoning) in addition to history taking ifintervention and outcomes concerning history takingwere reported in detail and separately from the resultsregarding the other objectives.
Exclusion criteriaThe following results were excluded in this review:
– Teaching units concerning only specific aspects ofthe medical history (e.g. taking a sexual history oran occupational history). Specific aspects of themedical interview are usually taught later in medical
education and after an introductory course inmedical interviewing has taken place, which is whyinterventions with regard to these specific aspectswere excluded in this review.
– Teaching units addressing communication skills ingeneral, patient-centred behaviour or empathywithout regard to history taking
– Articles describing only the assessment of interviewskills without describing a teaching unit
– Articles with no measured outcome at all, e.g.project descriptions with course evaluation only andwithout any assessment of learning progress
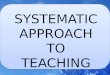
Article selection and data collectionThe literature search yielded 1254 potential publicationson teaching units addressing history taking for medicalstudents (see flowchart in Fig. 1 for complete search andstudy selection strategy). Following an initial review forrelevancy by title and abstract (KEK and NS) and re-moval of duplicate results, 78 studies were left for full-text review, of these, 23 studies finally met the inclusioncriteria. Interrater reliability was excellent with к = 0.84.In case of differing judgement, EJL was consulted as in-dependent evaluator.Relevant data was extracted from the included articles
using an a priori developed data extraction form com-posed for this review (KEK, NS). Data extraction fieldsincluded (1) authors and year of publication, (2) descrip-tion of study design and (3) participants, (4) descriptionof the educational intervention, (5) assessment tech-niques and measurement tools, (6) reported change inhistory taking ability and (7) MERSQI score. Discussionwith EJL resolved differences in data extraction.
Quality assessmentStudy quality was considered using the Medical Educa-tion Research Study Quality Instrument (MERSQI), atool developed especially to assess educational studies[39]. The 10-item scale (possible range 5 to 18) surveysthe following domains: study design, sampling, type ofdata, validity of the evaluation instrument, data analysisand outcomes. Patient or health care outcomes areassessed higher than students’ satisfaction, attitudes oropinions. The MERSQI domains are very similar to therequired methodical standards that Sanson-Fisher sug-gested for educational studies [40]. Neither the authorsof the MERSQI scale nor Sanson-Fisher and colleaguesdefined a cut-off value to differ methodically “good”studies from “less good studies”.
ResultsThis systematic review includes 23 studies. Table 1 de-scribes these studies in detail, reporting basic data con-cerning study design and participants, teaching methods
Keifenheim et al. BMC Medical Education (2015) 15:159 Page 3 of 12

and training procedures, assessment of learning pro-gress, use of measurement tools and the calculatedMERSQI score of the study (see Table 1).
Study characteristicsThe study design of the 23 finally selected articles washeterogeneous. There were randomized, two-group, pre-post comparisons (n = 4) as well as randomized andnon-randomized two-group post-tests (n = 6). Five stud-ies were single-group pre-post comparisons and fivewere single-group post-test evaluations only. Two weremodified cohort controlled studies and one a non-randomized, three-group post-test. Of those studiesreporting the duration of their educational interventions,the shortest intervention took two hours and the longesttook seven 4-hour sessions (28 h).
Outcome measuresAssessment methods and measurement tools, much likethe study designs, also were very heterogeneous. In eightstudies [9, 10, 24, 26, 28, 41–43] out of 22, trained ob-servers assessed an interaction between a student and asimulated patient (SP) using a standardized history tak-ing measurement tool. Seven of the applied scales werespecific to history taking, but only one had a proven reli-ability and validity and all of them had been developed
especially to assess the published intervention. Theremaining 15 studies used either non-validated, self-report questionnaires developed by the respective studyinvestigators, course evaluation questionnaires or qualita-tive analyses of students’ comments. One of the studiesused a written examination; one used focus groups.Twenty-two studies out of 23 found positive effects oftheir educational interventions on students’ history-takingskills. For a full overview of the results see Table 1.
Study qualityThe mean MERSQI score for the 23 included studieswas 10.36 (SD 2.65) [39]. The range was from 6.5 to 14(possible range 5 to 18). Scores were limited especiallyby: deficiencies in the field of study design (ex: no con-trol group, missing baseline measurements or lack ofrandomization); by missing validity of the outcomemeasurement tools; and by measurement of students’ at-titudes or skills rather than by patient or health careoutcomes.
InterventionsInstructional (traditional) approachesFocus scripts Students in the multi-institutional RCT ofPeltier [44] received “focused history and physical examscripts” (Focus Scripts). The authors developed one
Fig. 1 Flow chart of the literature search and study selection process
Keifenheim et al. BMC Medical Education (2015) 15:159 Page 4 of 12

Table 1 Characteristics of 23 studies of educational interventions concerning history-taking skills
Source Study design Participants Educational intervention Assessment technique andmeasurement tool
Improvement in history-taking ability reported?
MERSQIScore
Instructional (traditional) approaches
Focus scripts
Peltier et al. 2007 [44] Randomized, two-grouppost-test
n = 60 clinical medical students Focus Scripts Students’ write-ups werescored by a blinded rater
Yes 12,5
Videotape review: Communication benchmarks
Losh et al. 2005 [45] Single-group post-test n = 180 preclinical medical students One 2-hour teaching session includingan introduction of communicationbenchmarks and a video demonstrationof short scenarios contrasting “ok” with“better” communication skills
Course evaluationquestionnaire
Yes 6,5
Online course
Wiecha et al. 2003 [46] Single-group, pre-postcomparison
n = 10 preclinical medical students Four weeks online elective courseincluding video demonstrations, textmodules, a moderated, asynchronousdiscussion board and written personalfeedback
Questionnaire on self-reportedknowledge; qualitative analysisof interviews, focus groupsand student course postings.
Yes 11
Experiental approaches
Small group workshops including role-play and feedback
Mukohara et al. 2004[41]
Non-randomized, two-group post-test
n = 105 clinical medical students Two-day, small group seminar,including role-play, videotape review,feedback and discussion
OSCE station; communicationskills rated by two trainedobservers
Yes in one skill,tendency notable in 15other skills
11,5
Evans et al. 1993 [27] Non-randomized, two-group post-test
n = 106 preclinical medical students Programme of lectures and skillsworkshops
Assessment of videotapedinterviews with real patientsby two independent, trainedraters using the HTRS
Yes 11,5
Small group workshops including simulated patients
von Lengerke et al. 2011[51]
Single-group, pre-postcomparison
n = 267 preclinical medical students Seven 4-hour sessions in small groups,training program with lecture, self-study,(videotaped) role-play and SP interviews
Self-evaluation questionnaireon communication skills,course evaluation
Yes 8,5
Ozcakar et al. 2009 [42] Randomized, two-group,pre-post comparison
n = 52 preclinical medical students Two videotaped SP interviews and(visual/verbal) feedback by trainer
Self-assessment, assessmentby trained observers using achecklist
Yes 13,5
Hulsman et al. 2009 [49] Single-group post-test n = 331 preclinical medical students Seven small group sessions includingSP interviews, videotape review, writtenself-evaluations, peer-feedback anddiscussion
Rating of students’ reflectionsby trained observers; evaluationquestionnaire
Yes 9
Nestel& Kidd 2003 [50] Randomized, two-grouppost-test
n = 40 preclinical medical students One 3-hour session, including SPinterviews, feedback and videotapereview. Small groups facilitated eitherby peer tutors or by medical teachers
Written course evaluationquestionnaire; self-assessment;rating by SPs and trainedassessors
Yes 13
Keifenheimet
al.BMCMedicalEducation
(2015) 15:159 Page
5of
12

Table 1 Characteristics of 23 studies of educational interventions concerning history-taking skills (Continued)
Yedidia et al. 2003 [52] Randomized, two-group,pre-post comparison
n = 293 clinical medical students Demonstration of interviewing skills, SPinterviews, feedback and self-reflection
OSCE station, communicationskills rated by SPs
Yes 13,5
Fortin et al. 2002 [7] Single-group post-test n = 127 preclinical medical students Two half-day workshops including amini lecture, demonstration by faculty,role-play, SP interviews and discussion
Course evaluation questionnaire;free-text on what studentslearned from the workshop
Yes 7
Utting et al. 2000 [43] Randomized, single-blinded, three-group post-test comparison
n = 111 clinical medical students Two 4-week basic skills coursesincluding small group activities,discussion, role-play and SP interviewscompared with a 10-week courseincluding mainly lectures and instructions
Evaluation of videotaped SPinterviews by two independentobservers using IGS and CSS
No 12,5
Eoaskoon et al. 1996 [48] Non-randomized, three-group post-test
n = 115 clinical medical students Theoretical sessions, then division intothree groups: (1) SP interview andfeedback, (2) role-play in front of thegroup and feedback, (3) role playwithin the group and feedback
Course evaluation, assessmentof students’ interviews by tutors
Yes 8
Battles et al. 1992 [47] Two-group post-test n = 358 preclinical medical students Small group sessions one-half day every2 weeks using lectures, SP interviews,feedback and discussion
OSCE using brief SP encountersand writing stations
Yes 8
Kraan et al. 1990 [24] Modified cross-sectionalstudy
n = 563 preclinical and clinicalmedical students from fivedifferent academic years
Six-year undergraduate curriculumteaching communication skills usingsmall group sessions including SPinterviews, videotape review, feedbackand discussion
Assessment of live SP interviewsby trained observers using theMAAS
Yes 10,5
Using virtual patients
Vash et al. 2007 [53] Randomized, two-grouppost-test
n = 48 clinical medical students Fourteen 1-hour sessions in a computerlab working through virtual patients insmall groups
Written examination Yes 11
Small group workshops including real patients
Fischer et al. 2005 [54] Single-group, pre-postcomparison
n = 154 clinical medical students 9 weekly 2-hour small group sessionsincluding role-plays, SP interviews andvideotaped interviews with real patients,each followed by feedback
Pre and post self-assessment bystudents using a 1–6 point scale;OSCE stations where skills wererated by SP and trained observer
Yes 10,5
Windish et al. 2005 [10] Randomized, two-grouppre-post comparison
n = 121 preclinical medical students Six weekly 3-hour small group sessionsincluding brief lecture, short videohighlighting certain skills and role-playwith feedback
Assessment of studentperformance by trained SPsusing a checklist; courseevaluation
Yes 13,5
Evans et al. 1996 [26] Randomized, two-group,pre-post comparison
n = 60 clinical medical students Training programme including lectures,comprehensive notes and workshopswith role-plays, videotaping of realpatients and SPs and discussions insmall groups
Rating of videotaped SPinterviews by trained, blindedobservers using the MIRS
Yes 12,5
Novack et al. 1992 [9] Single-group, pre-postcomparison
n = 60 preclinical medical students Two initial lecture demonstrations, then12 weekly 2-hour sessions in smallgroups including role-plays, interviewswith patients and discussions.
Videotaped SP interviews ratedby blind reviewers using ISIE;Brief questionnaire for students’self-evaluation of progress
Yes 14
Keifenheimet
al.BMCMedicalEducation
(2015) 15:159 Page
6of
12

Table 1 Characteristics of 23 studies of educational interventions concerning history-taking skills (Continued)
Creative approaches
Improvisational theatre
Shochet et al. 2013 [56] Single-group post-test n = 38 preclinical medical students Four weekly 2-hour sessions,improvisational theatre
Online course evaluation,qualitative analysis ofstudents’ comments
Yes 6,5
Watson 2011 [55] Single-group post-test n = 116 preclinical medical students Five weekly 2-hour sessions in smallgroups, improvisational theatre
Qualitative analysis of courseevaluations, self-reportquestionnaire on acquired skills
Yes 7
Lego® simulation
Harding& D’Eon 2001 [57] Single-group, pre-postcomparison
n = 57 preclinical medical students Two-hour session including interactivelecture and a Lego simulation
Survey, information recall,qualitative analysis of focusgroups
Yes 7
SP simulated patient, OSCE Objective Structured Clinical Examination, IGS Information Gathering Scale, CSS Communication Skills Scale, MIRS Medical Interview Rating Scale, HTRS History-Taking Rating Scale, ISIE Inter-national Analysis System for Interview Evaluation, MAAS Maastricht History-Taking and Advice Checklist
Keifenheimet
al.BMCMedicalEducation
(2015) 15:159 Page
7of
12

generic acute patient script template and one templatefor a focused chronic illness history. The organizationalstructure of the scripts was aimed to support students’collection of data on any symptom. Students’ writtenprogress notes were scored by a blind rater using a stan-dardized scale. Five of 11 variables were statisticallyhigher in the group that learned with the focused scripts.These included history taking, clarity of diagnosis andoverall score. This intervention focuses on content andcompleteness of the medical interview and does not takeverbal or non-verbal interview skills into account.
Videotape review: Communication benchmarksLosh [45] held a lecture introducing communicationbenchmarks for inpatient history and then showed shortvideotaped scenarios that illustrated segments of a stu-dent history, contrasting an acceptable version of com-munication with a better version. The better versiondemonstrated the appropriate benchmarked skills. Thescenarios were used in teaching sessions to help studentsidentify effective communication techniques within themedical interview. Participants were medical studentsdoing their first medical interview. After the sessions,76 % of the students felt that this design helped them tounderstand the introduced communication benchmarksand 92 % felt that the videotape helped to point out sub-tle communication issues that might otherwise havebeen missed. The intervention imparted both knowledgeabout content and structure of the medical interviewand particular communication skills.
Online courseWiecha [46] reported on an online course developed toteach the cognitive basis for interviewing skills. The au-thors provided video demonstrations of patient inter-views, text modules presenting communication concepts(not further clarified by the authors) and a moderated,asynchronous discussion board asking students to posttheir observations. The authors addressed questioningtechniques, affect and nonverbal cues, eliciting the car-dinal features of a symptom, and stages and transitions.Students received individual feedback on their participa-tion and performance by personal e-mail. They reportedimprovement in self-awareness, increased understandingof interviewing concepts and benefits of online learning.Self-reported knowledge scores also increased significantly.
Experiential (“learning by doing”) approachesSmall group workshops including role-play andfeedback In two studies [28, 41], students participatedin small group workshops practising history taking byrole-play. Feedback was provided by facilitator andgroup members. Evans [28] implemented a specializedhistory-taking training programme consisting of lectures
and skills workshops. Trained students were significantlymore efficient on all areas covered by the applied scale(commencement of the interview, problem processing,communication, summary and overall effectiveness). In anon-randomized, controlled study, Mukohara [41] im-plemented a 2-day seminar on communication processskills and content aspects of the medical interview.Learning activities were a trigger videotape critiquefollowed by role-play with videotape review and feed-back by facilitator and group. The authors found an im-provement for students’ ability to assess “how the illnessaffects the patient’s life”. No differences were observedbetween intervention group and waiting control groupin the other 15 core communication skills.
Small group workshops including simulated patientsTen studies [7, 24, 28, 42, 43, 47–52] reported on inter-ventions using simulated patients (SP). SP interviewswere conducted by one of the participating students andwere usually combined with a feedback session and dis-cussion. Feedback was given by the group and/or the fa-cilitator. SP interviews in these workshops were oftensupplemented by lectures, demonstrations, small groupexercises including role-play and self-reflection. Battles[47] used SPs with abnormal medical histories to dem-onstrate pathology. Utting [43] compared two skillscourses using an active “learning by doing” approachwith one course and applying instructional methods inthe other. The authors found no differences in students’interview skills, which were assessed using standardizedscales. Eoaskoon [48] conducted a three-group post-test.SP interview and feedback (1) were compared with role-play and feedback in front of the group (2) and role-playand feedback within the group (3). The group thattrained with SP interviews gained the highest scores withregard to interview skills. Five studies [24, 42, 49–51]used videotape review for feedback. Kraan [24] investi-gated a graded teaching program of medical interviewingskills. Each year a different set of skills was highlighted.In the first years, basic interviewing skills, medicalhistory-taking skills and psychosocial issues were em-phasized. Effective exchange of information and difficultsituations such as dealing with aggressive patients orsexual problems were topics for advanced learners. Eachsmall group had both a physician and a behavioural sci-entist as facilitators. Ozcakar [42] found that studentshaving both verbal and visual (videotape review) feed-back were more successful than those having verbalfeedback alone. Although self-assessment of the studentsdid not improve significantly, feedback based on video-taped interviews was superior to the feedback givensolely based on the observation of assessors. Hulsman[49] showed that students valued SP interviews, videoobservation and feedback as instructive and helpful to
Keifenheim et al. BMC Medical Education (2015) 15:159 Page 8 of 12

develop their own strengths and to identify certain kindsof behaviour to improve. Nestel and Kidd [50] used peertutors and reported no differences regarding patient-centred interview skills between groups taught by peersand those taught by faculty. Von Lengerke [51] and For-tin [7] found that SP interviews were evaluated as one ofthe most effective teaching methods. Von Lengerke per-formed a pre-post comparison of students’ self-assessedcompetencies and had participants evaluate key teachingmethods. In addition to history taking, disclosure ofdiagnosis was taught in this course. Fortin [7] focusedon integrating patient-centred skills (listening, negotiat-ing, responding to emotion empathetically, focusing thepatient’s story) into a medical interview skills course.Mini-lectures, demonstrations by faculty and role-playpreceded the SP interviews.
Using virtual patientsOne RCT by Vash [53] reported on small groups work-ing on virtual surgical patients in a computer lab. Thepatient was initially introduced to them, and then thestudents worked through eight sections including inter-view (chief complaint), medical history and review ofsystems. Students had to ask relevant questions by typ-ing them. Students in the lab performed better thantheir colleagues in the control group, which had seen pa-tients in the surgery clinic instead. Significant differenceswere only found in the history taking area.
Small group workshops including real patientsFour interventions [9, 10, 26, 54] provided real patients.Fischer [54] included real patient interviews at the endof a course including role-play and simulated patients aswell. Students interviewed real patients and videotapedthe interviews. One aspect of the intervention was thatthe students visited the real patients in their homes. Theinterviews were watched back in the classroom and thestudents received feedback from facilitators and groupmembers. The authors reported a significant learningprogress and improvement in taking a case history. Re-sults of self-reported questionnaires corresponded wellwith the results of the Objective Structured ClinicalExamination (OSCE). Windish [10] compared a commu-nication skills course applying SPs to a control groupinterviewing inpatients. Students in the interventiongroup were better at establishing rapport and were ableto list more psychosocial history items. Evans [26] usedreal patients in the context of a communication skillscourse. The authors applied lectures, role-play, SP inter-views and discussion as well. All three studies made useof videotape review. Novack [9] included interviews withreal patients in a course using lectures, role-play anddiscussion as well as textbooks with additional informa-tion. Students were supposed to follow a chronically ill
patient for 1 year and after regular interviews, write upprogress notes.
Creative approachesImprovisational theatre Watson [55], as well as Shochet[56], implemented elective courses including improvisa-tional theatre techniques to improve specific communi-cation skills. In Shochet’s study, students practisedspecific skills including listening, affirmation, non-verbalcommunication and other skills. Students discussed therelevance of these skills in communication with their pa-tients. The authors showed that students felt moreconfident in their role as future physicians after thecourse and that they improved their ability to be flexiblein communication styles and “respond in the moment”.Most students thought that the concepts that were ad-dressed in the course were highly relevant to the care ofpatients. Students in Watson’s classes felt they becamebetter listeners and observers.
Lego® simulationHarding and D’Eon [57] implemented a Lego® simulationin their interactive lecture to improve patient-centredinterviewing skills. Student volunteers took on the rolesof doctor and patient. The doctor had to query the pa-tient and through his responses replicate the patient’sLego® construction without looking at it. The authorsfound this intervention helped preclinical students toconcentrate on interviewing skills without being pre-occupied with medical knowledge.
DiscussionHeterogeneity of interventionsOne clear finding of the literature review is that the in-cluded studies applied very heterogeneous teachingmethods and determined different core areas to teach.While some interventions focused on content or struc-ture of the medical interview and imparted techniqueson “how to ask the right questions”, others highlightednon-verbal communication skills, patient-centerednessand establishing rapport. There is no accordance onwhen in medical education certain skills should betaught, leading to interventions that were taught for stu-dents at very different levels of training. While somestudies evaluated long existing training programmes ex-tending over several semesters, others investigated in-novative approaches sometimes lasting only a few hours.Fourteen studies included medical students in the pre-
clinical years, eight studies included students in the clin-ical years and one study included both. Authors of thestudies investigating improvisational theatre and Lego®simulation presumed that preclinical students might es-pecially benefit from creative approaches where no sig-nificant medical knowledge was required. Not being
Keifenheim et al. BMC Medical Education (2015) 15:159 Page 9 of 12

preoccupied with complicated clinical reasoning may fa-cilitate history-taking exercises for this subgroup and en-hance patient-centred approaches.Heterogeneity might also be due to the context de-
pendence of the medical interview itself. Goals of the in-cluded studies were to enable students to attain a set ofbasic knowledge and skills in the medical interview. Butencounters with patients are highly complex events andno simple approach can do justice to all possible pro-cesses and challenges in such interactions. No singlecourse can comprehensively address all the communica-tion problems that a physician will encounter, nor willskills be effective in every imaginable clinical situation.Most articles in the field of history taking don’t differ-
entiate between interview skills, interpersonal skills andcommunication skills – this conceptual mixture alsocontributed to the heterogeneity of interventions. Veryoften, specific interpersonal and communication skills(e.g. nonverbal behaviour, communication of empathy)are taught within the context of medical interviewcourses. Maybe an exact separation of these terms anddefinitions is neither even possible nor desirable as thereis a continuum from communication skills to interviewskills to history taking.
Assessment of history taking skillsSix different methods of assessing learning progress wereapplied in the included studies. Many studies used morethan one of the following:
1. Self-evaluation questionnaires2. Free-text response on what students learned from
the workshop3. Written examinations4. Qualitative analysis of students’ reflections and
write-ups5. Assessment of (videotaped) interviews by either
trained observers, SPs or student tutors, either usinga checklist/validated measurement tool or just givinga global impression
6. OSCE-stations and assessment of the interviews bytrained observers or SPs, using a checklist/validatedmeasurement tool.
Studies with a higher MERSQI score (>11.5) mostlyused the latter methods (numbers 4, 5, 6) of assessinglearners’ progress. Very often, they combined differentmethods and had self-report course evaluation formsas well as formal assessments of students’ interviewswith SPs.
Findings from the MERSQI scoreIf articles are sub-divided by methodological quality, itbecomes apparent that studies with a higher MERSQI
score (>11,5) often report on small-group skills work-shops using role-play, simulated patients, virtual patientsand/or real patients. In these courses, teachers andgroup, sometimes also SPs or peer tutors, give feedback.Mostly, interviews are videotaped to facilitate and en-hance feedback. Studies with a lower MERSQI score(<9) frequently apply a more traditional approach usingdemonstrations, theoretical sessions and self-study. Ascreative approaches also tend to achieve a lower MERSQIscore, innovative approaches don’t seem to be associatedwith a better study quality. Experiential approaches(“learning by doing”, see Table 1) achieved the highestMERSQI scores. Differences in MERSQI scores are pri-marily explicable by implementation of control groups,objective assessment of (videotaped) interviews and use ofassessment tools. Limitations of the MERSQI score couldbe that the scale is based on a quantitative experimentalstudy design paradigm that might underestimate qualita-tive or observational studies. Reliance on the MERSQIscore only might therefore be biased towards particularforms of research.
Implications for future researchWith regard to content, the included interventions wereoften innovative, mostly well-thought-out and substanti-ated. Many of them were descriptive studies that reliedon students’ self-evaluation and didn’t provide evidencethat the intervention was effective in improving history-taking skills. Though there is a well-established method-ology for adequate evaluative research that should beused if the effectiveness of history-taking courses is tobe properly determined, studies mostly lack baselinemeasurement, randomization, adequate control groups,external measurement, blinded raters or standardizedmeasurement scales. Often self-developed assessmentscales were used although proven scales for external as-sessment do exist (for example the History-Taking Rat-ing Scale (HTRS) [28], the Maastricht History-takingand Advice Checklist (MAAS) [24] or the Brown Inter-viewing Checklist (BIC) [6]). And although essential ele-ments of effective history taking courses were defined inthe 80s and 90s [33, 34], there is still no evidence-basedgold standard that could serve as control group for aninnovative new approach. Of course innovative ideasshould be described in articles to provoke and stimulatediscussion with colleagues but there is still a need forsubstantiated not just experiential studies. Innovativenew concepts must be welcomed, but they should becoupled with acceptable methodology to examine anddemonstrate their effectiveness [40].An effort should always be made to question if certain
interventions provide a more significant improvementfor certain groups of students. There may be circum-stances that predispose students to require more specific
Keifenheim et al. BMC Medical Education (2015) 15:159 Page 10 of 12

interventions, for example a non-native speaker of a lan-guage may need training in appropriate phrasing ofquestions as well as non-verbal cues to be most effectiveat history taking.
Implications for curriculum planners and medical teachersSmall group workshops including interview simulations(role-play, SP interviews, virtual patients) and interviewswith real patients, followed by feedback and discussion,are widespread and have been most thoroughly investi-gated and reported on. Feedback using videotape reviewseems to be particularly successful in providing studentswith instructive techniques in history taking. Students inthe early preclinical state might profit from creative ap-proaches helping them to focus on the interview skillsand not being preoccupied by attempts to make diagno-ses beyond their abilities. There is no evidence on whenhistory-taking workshops should take place in the cur-riculum. Some authors recommend implementing themin the clinical clerkships, others favour implementationin preclinical years. Curriculum planners should con-sider addressing the reported decline in history-takingskills over time when medical interviewing is taughtearly in the curriculum, especially concerning psycho-social issues. This might be achieved by implementing along-term “communication skills” course or by offeringbooster sessions later in the clinical years.
Limitations of this reviewIt is possible that our search strategy may have missedsome papers, especially those published in different lan-guages as we only included articles written in English orGerman. However, it is unlikely that we missed a sub-stantial number of relevant publications, especially asthis review covers such a long period. But more import-ant than that, this review only included published stud-ies while it is recognized that many training programsdo teach history taking in a variety of ways world widethat may not be mentioned in this review as they havenot been published.
ConclusionsHistory taking is an essential skill of every physician andhas to be taught in the course of their medical educa-tion. Today, there are many studies demonstrating thatstudents can acquire interview skills by specific work-shops. There seems to be little evidence noting the su-periority of one specific method however, there is abroad scope of interventions that all seem to provide his-tory taking skills. It is not known if the acquired skills canbe generalized across situations or maintained over time.Important formal goals for this research area are to
meet acceptable methodological standards for evaluativeresearch. External measurement of students’ skills –
either by a clinician, a SP or student/peer tutor utilizingestablished proven scales – is an important objective forthe evaluation of future methods of teaching history tak-ing. Practical examinations involving SPs, especiallyOSCE stations, should be gold standard in assessing his-tory taking skills.
Competing interestsThe authors declare that they have no competing interests.
Authors’ contributionsKEK: literature review concept design, analysis and interpretation of data,drafting of manuscript. JI: critique for revision of manuscript and editing. MT:literature review concept design, critical revision of manuscript. NS: analysisand interpretation of data. EJL: literature review concept design, analysis andinterpretation of data. SZ: literature review concept design and coordinationAHW: literature review concept design, critical revision of manuscript. Allauthors read and approved the final manuscript.
FundingWe acknowledge support by Deutsche Forschungsgemeinschaft and OpenAccess Publishing Fund of University of Tübingen.
Author details1Department for Psychosomatic Medicine and Psychotherapy, UniversityHospital of Tuebingen, Osianderstr. 5, 72076 Tübingen, Germany. 2ClinicalAssociate Professor of Family Medicine, Associate Dean of Medicine, BrownUniversity, Providence, RI, USA. 3Dean of Medical Education, Medical Faculty,University of Tuebingen, Tuebingen, Germany.
Received: 20 April 2015 Accepted: 14 September 2015
References1. Nichols LO, Mirvis DM. Physician-patient communication: does it matter?
Tenn Med. 1998;91(3):94–6.2. Davidoff F, Deutsch S, Egan KL, Ende J. Who Has Seen A Blood Sugar? -
Reflections on Medical Education. Edited by the American College ofPhysicians. Philadelphia: American College of Physicians; 1996.
3. Engel GE, Morgan WL. Interviewing and patient care. Philadelphia: Saunders;1973.
4. Lipkin Jr M. The medical interview and related skills. In: Branch W, editor. OfficePractice of Medicine. Philadelphia: WB Saunders Co; 1987. p. 1287–306.
5. Engel GL. Enduring attributes of medicine relevant for the education of thephysician. Ann Intern Med. 1973;78:587–93.
6. Novack DH, Volk G, Drossman DA, Lipkin Jr M. Medical interviewing andinterpersonal skills teaching in US medical schools. Progress, problems, andpromise. JAMA. 1993;269(16):2101–5.
7. Fortin AH, Haeseler FD, Angoff N, Cariaga-Lo L, Ellman MS, Vasquez L, et al.Teaching pre-clinical medical students an integrated approach to medicalinterviewing: half-day workshops using actors. J Gen Intern Med.2002;17(9):704–8.
8. Hatem DS, Barrett SV, Hewson M, Steele D, Purwono U, Smith R. Teachingthe medical interview: methods and key learning issues in a facultydevelopment course. J Gen Intern Med. 2007;22(12):1718–24.
9. Novack DH, Dube C, Goldstein MG. Teaching medical interviewing. A basiccourse on interviewing and the physician-patient relationship. Arch InternMed. 1992;152(9):1814–20.
10. Windish DM, Price EG, Clever SL, Magaziner JL, Thomas PA. Teachingmedical students the important connection between communication andclinical reasoning. J Gen Intern Med. 2005;20(12):1108–13.
11. Sanson-Fisher R, Maguire P. Should skills in communicating with patients betaught in medical schools? Lancet. 1980;2(8193):523–6.
12. Novack DH. Therapeutic aspects of the clinical encounter. J Gen Intern Med.1987;2(5):346–55.
13. Peterson MC, Holbrook JH, Von Hales D, Smith NL, Staker LV. Contributionsof the history, physical examination, and laboratory investigation in makingmedical diagnoses. West J Med. 1992;156(2):163–5.
14. Hampton JR, Harrison MJ, Mitchell JR, Prichard JS, Seymour C. Relativecontributions of history-taking, physical examination, and laboratory
Keifenheim et al. BMC Medical Education (2015) 15:159 Page 11 of 12

investigation to diagnosis and management of medical outpatients. Br MedJ. 1975;2(5969):486–9.
15. Kassirer JP. Teaching clinical medicine by iterative hypothesis testing. Let’spreach what we practice. N Engl J Med. 1983;309(15):921–3.
16. Roshan M, Rao AP. A study on relative contributions of the history, physicalexamination and investigations in making medical diagnosis. J AssocPhysicians India. 2000;48(8):771–5.
17. Sandler G. The importance of the history in the medical clinic and the costof unnecessary tests. Am Heart J. 1980;100(6 Pt 1):928–31.
18. Bird J, Cohen-Cole SA. The three-function model of the medical interview.An educational device. Adv Psychosom Med. 1990;20:65–88.
19. Rezler AG, Woolliscroft JA, Kalishman SG. What is missing from patienthistories? Med Teach. 1991;13(3):245–52.
20. Smith RC. Patient-centered interviewing: an evidence-based method. 2nded. Philadelphia: Lippincott Williams&Wilkins; 2002.
21. Rosenberg EE, Lussier MT, Beaudoin C. Lessons for clinicians from physician-patient communication literature. Arch Fam Med. 1997;6(3):279–83.
22. Lazare A, Putnam S, Lipkin M. Three functions of the medical interview. In:The Medical Interview. New York: Springer; 1995. p. 3–19.
23. Engel GL. What if music students were taught to play their instruments asmedical students are taught to interview? Pharos Alpha Omega AlphaHonor Med Soc. 1982;45(4):12–3.
24. Kraan HF, Crijnen AA, de Vries MW, Zuidweg J, Imbos T, Van der Vleuten CP.To what extent are medical interviewing skills teachable? Med Teach.1990;12(3–4):315–28.
25. Pfeiffer C, Madray H, Ardolino A, Willms J. The rise and fall of students’ skillin obtaining a medical history. Med Educ. 1998;32(3):283–8.
26. Evans BJ, Coman GJ, Goss B. Consulting skills training and medical students’interviewing efficiency. Med Educ. 1996;30(2):121–8.
27. Evans BJ, Sweet B. Consulting-skills training to improve medical students’diagnostic efficiency. AcadA Med. 1993;68(2):170–1.
28. Evans BJ, Sweet B, Coman GJ. Behavioural assessment of the effectivenessof a communication programme for medical students. Med Educ.1993;27(4):344–50.
29. Schildmann J, Kampmann M, Schwantes U. Teaching courses on aspects ofmedical history taking and communication skills in Germany: a surveyamong students of 12 medical faculties. Z Arztl Fortbild Qualitatssich.2004;98(4):287–92.
30. Hargie O, Dickson D, Boohan M, Hughes K. A survey of communication skillstraining in UK schools of medicine: present practices and prospectiveproposals. Med Educ. 1998;32(1):25–34.
31. Assiciation of American Colleges. Learning Objectives for Medical StudentEducation: Guidelines for Medical Schools (MSOP Report). Washington DC:Association of American Medical Colleges; 1998.
32. General Medical Council. Tomorrow’s Doctors: Recommendations onUndergraduate Medical Education. London: General Medical Council; 1991.
33. Maguire P. Can communication skills be taught? Br J Hosp Med.1990;43(3):215–6.
34. Simpson M, Buckman R, Stewart M, Maguire P, Lipkin M, Novack D, et al.Doctor-patient communication: the Toronto consensus statement. BMJ.1991;303(6814):1385–7.
35. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, Ioannidis JP, et al.The PRISMA statement for reporting systematic reviews and meta-analysesof studies that evaluate health care interventions: explanation andelaboration. PLoS Med. 2009;6(7):e1000100.
36. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reportingitems for systematic reviews and meta-analyses: the PRISMA statement.PLoS Med. 2009;6(7):e1000097.
37. Henwood PG, Altmaier EM. Evaluating the effectiveness of communication skillstraining: a review of research. Clin Perform Qual Health Care. 1996;4(3):154–8.
38. Aspegren K. BEME Guide No. 2: Teaching and learning communication skillsin medicine-a review with quality grading of articles. Med Teach.1999;21(6):563–70.
39. Reed DA, Cook DA, Beckman TJ, Levine RB, Kern DE, Wright SM. Associationbetween funding and quality of published medical education research.JAMA. 2007;298(9):1002–9.
40. Sanson-Fisher R, Fairbairn S, Maguire P. Teaching skills in communication tomedical students–a critical review of the methodology. Med Educ.1981;15(1):33–7.
41. Mukohara K, Kitamura K, Wakabayashi H, Abe K, Sato J, Ban N. Evaluation ofa communication skills seminar for students in a Japanese medical school: anon-randomized controlled study. BMC Med Educ. 2004;4:24.
42. Ozcakar N, Mevsim V, Guldal D, Gunvar T, Yildirim E, Sisli Z, et al. Is the useof videotape recording superior to verbal feedback alone in the teaching ofclinical skills? BMC Public Health. 2009;9:474.
43. Utting MR, Campbell F, Rayner C, Whitehouse CR, Dornan TL. Consultationskills of medical students before and after changes in curriculum. J R SocMed. 2000;93(5):247–53.
44. Peltier D, Regan-Smith M, Wofford J, Whelton S, Kennebecks G, Carney PA.Teaching focused histories and physical exams in ambulatory care: a multi-institutional randomized trial. Teach Learn Med. 2007;19(3):244–50.
45. Losh DP, Mauksch LB, Arnold RW, Maresca TM, Storck MG, Maestas RR, et al.Teaching inpatient communication skills to medical students: an innovativestrategy. Acad Med. 2005;80(2):118–24.
46. Wiecha JM, Gramling R, Joachim P, Vanderschmidt H. Collaborativee-learning using streaming video and asynchronous discussion boards toteach the cognitive foundation of medical interviewing: a case study. J MedInternet Res. 2003;5(2):e13.
47. Battles JB, Sprankell SJ, Carpenter JL, Bedford JA, Kirk LM. Developing asupport system for teaching and assessing clinical competence. J Biocommun.1992;19(4):19–25.
48. Eoaskoon W, Sumawong V, Silpakit C. Evaluation of training medicalstudents in patient-interviewing skills by three modes of learning. J MedAssoc Thai. 1996;79(8):526–30.
49. Hulsman RL, Harmsen AB, Fabriek M. Reflective teaching of medicalcommunication skills with DiViDU: assessing the level of student reflectionon recorded consultations with simulated patients. Patient Educ Couns.2009;74(2):142–9.
50. Nestel D, Kidd J. Peer tutoring in patient-centred interviewing skills:experience of a project for first-year students. Med Teach. 2003;25(4):398–403.
51. von Lengerke T, Kursch A, Lange K. The communication skills course forsecond year medical students at Hannover Medical School: An evaluationstudy based on students’ self-assessments. GMS Z Med Ausbild.2011;28(4):Doc54.
52. Yedidia MJ, Gillespie CC, Kachur E, Schwartz MD, Ockene J, Chepaitis AE,et al. Effect of communications training on medical student performance.JAMA. 2003;290(9):1157–65.
53. Vash JH, Yunesian M, Shariati M, Keshvari A, Harirchi I. Virtual patients inundergraduate surgery education: a randomized controlled study. ANZ JSurg. 2007;77(1–2):54–9.
54. Fischer T, Chenot J-F, Kleiber C, Kochen MM, Simmenroth-Nayda A, Staats H,et al. Kurs “ärztliche Basisfertigkeiten” - Evaluation eines primärärztlichorientierten Unterrichtskonzepts im Rahmen der neuenApprobationsordnung. GMS Z Med Ausbild. 2005;22:Doc59.
55. Watson K. Perspective: Serious play: teaching medical skills withimprovisational theater techniques. Acad Med. 2011;86(10):1260–5.
56. Shochet R, King J, Levine R, Clever S, Wright S. ‘Thinking on my feet’: animprovisation course to enhance students’ confidence and responsivenessin the medical interview. Educ Prim Care. 2013;24(2):119–24.
57. Harding SR, D’Eon MF. Using a Lego-based communications simulation tointroduce medical students to patient-centered interviewing. Teach LearnMed. 2001;13(2):130–5.
Submit your next manuscript to BioMed Centraland take full advantage of:
• Convenient online submission
• Thorough peer review
• No space constraints or color figure charges
• Immediate publication on acceptance
• Inclusion in PubMed, CAS, Scopus and Google Scholar
• Research which is freely available for redistribution
Submit your manuscript at www.biomedcentral.com/submit
Keifenheim et al. BMC Medical Education (2015) 15:159 Page 12 of 12