Embed Size (px)
Citation preview

TEACHING SELF-TREATMENT OF COLD SYMPTOMS TO AN ANOXIC BRAIN INJURED ADULT
MARK F. O’REILLY ANTHONY J. CUVO
Southern Illinois University at Carbondale, Carbondale, Illinois 62901
Traumatic brain injury can result in behavioral and physical deficits that require intensive post-acute residential rehabilitation. Behaviors targeted by such programs include basic self-care and living skills. We examined the efficacy of a behavioral training strategy to teach appropriate medical treatment of four different groups of simulated cold symptoms to an anoxic brain injured adult. The strategy included instructor prompting and feedback in the use of written task analyses and picture cues as self- administered prompts. Subsequent to baseline, the participant used written generic task analyses combined with picture cues and then, if necessary, written specific task analyses combined with picture cues to prompt appropriate self-treatment of the four types of colds. Written individualized task analyses, tailored to participant errors, were used to fade specific task analysis prompts and transfer stimulus control to the discriminative stimuli present in the picture cues. A multiple baseline design across responses showed that skill acquisition did not occur after generic task analysis training, but did so after specific task analysis train- ing. The participant responded to all four types of colds for three con- secutive trials at 100% correct under baseline conditions. Follow-up results indicated that transfer of stimulus control to the cold symptoms simulated by the picture cues alone did not maintain over time. Correct responding was retrained using generic and, if necessary, individualized task analysis training conditions .
Behavioral Residential Treatment, Vol. 4, No. 4 (1989) 0 1989 John Wiley & Sons, Inc. 0884-5581/89/040359-17$04.00
360/0’REILLY AND CUVO
Traumatic brain injury is defined as damage to the brain caused by external force (Vogenthaler, 1987). Every year approxi- mately 50,000 people suffer brain injuries as a result of car acci- dents, drowning accidents, cardiac arrest, and other injuries. Anoxic encephalopathy , a particular form of traumatic brain injury, is caused by the restriction of oxygenated blood to the brain. Some of the major cognitive deficits that people suffering from anoxic encephalopathy exhibit are reduced ability to plan, organize, and learn new information because of severe impair- ments of both short-term verbal and nonverbal memory.
Since anoxic brain injured individuals display behavioral defi- cits that have been successfully treated in other clinical popula- tions, a behavioral approach to rehabilitation may be promising with this population (Goldstein & Ruthven, 1983; Zahara & Cuvo, 1984). Little empirical evidence exists, however, to support this proposal, especially for teaching adaptive living skills.
Over the past decade, behavior analysts have developed train- ing strategies to promote the learning of functional living skills by persons who are mentally retarded or who have related develop- mental disorders (Cuvo & Davis, 1983). The majority of these teaching strategies have relied on external change agents to pro- mote the acquisition and maintenance of skills. More recently, researchers have begun to focus on techniques in which persons with mental retardation can promote their own instruction (Agran & Martin, 1987; Browder & Shapiro, 1985). Self-management procedures may provide learners a means to perform target be- haviors in environments in which prompts and consequences are not consistently delivered by others (e.g., when staff are not presenkb
Antecedent cue self-management procedures in the form of picture prompts and written task analyses have been used to teach living skills to persons with mental retardation (Lingnugaris/ Kraft, McCuller, Exum, & Salzberg, 1988; Mooney, 1988). Self- management procedures have been used to teach: (a) meal prepa- ration (Johnson & Cuvo, 1981), (b) vocational tasks (Fisher, 1984; Wacker & Berg, 1983, 1984; Wacker, Berg, Berrie & Swatta, 1985), (c) domestic cleaning skills (Mooney, 1988), and (d) health care skills (Brickey, 1978; Cuvo et al., 1986; Matson, 1980). In these studies, participants were taught by some combination of prompting, feedback, correction, and re- peated practice to imitate the responses depicted by the pictorial or written cues. Teacher delivered prompts typically have been
SELF-TREATMENT OF COLD SYMPTOMS/361
faded until participants perform under the control of the natural discriminative stimuli.
In the few published studies involving head trauma individuals, mnemonic techniques (e.g., rehearsal and visual imagery) served as effective discriminative stimuli to remediate memory problems (Glasgow, Zeiss, Barrera, & Lewinsohn, 1977). Self-recording of conversational behavior using mechanical counters combined with instructor feedback has effectively increased socially appropriate conversational skills with this population (Gajar, Schloss, Schloss, & Thompson, 1984).
Given that: (a) limited empirical evidence exists that some head injured individuals are capable of promoting their own instruction using mnemonic and self-recording techniques, and (b) no published research has evaluated behavioral techniques to teach living skills to head injured individuals, the present study examined whether an anoxic brain injured adult could use written prompts and picture cues to perform basic health care skills.
In a previous study, Mooney (1988) examined the efficacy of written generic and specific task analyses as self-adminis- tered prompts for instruction of domestic cleaning tasks by persons with mild mental retardation. Specific task analyses provide a detailed specification of responses to achieve the links in a behavioral chain. Generic task analyses, in contrast, incorporate only those mandatory steps to achieve task outcomes. Subsequent to baseline, Mooney (1 988) introduced generic task analyses and then, if necessary, specific task analyses to prompt clean- ing skills. Individualized task analyses, tailored to participant errors, were used to fade specific task analysis prompts and transfer stimulus control to discriminative stimuli in the natural environment. The rationale for the Mooney (1 988) study was not only to introduce the task analyses using a least prompt necessary strategy, but also to use textual cue fading as a means of trans- ferring stimulus control.
The present study systematically replicated the Mooney (1988) training strategy by examining the efficacy of self-man- agement of textual cues to teach basic health care skills to an anoxic brain injured adult. The study also replicated health care tasks used in research with mildly retarded persons (Cuvo e t al., 1986). Teaching such residents to identify, monitor, and report symptoms of illness and to self-administer medications increases their ability to participate in their own rehabilitation.
362/O’REILLY AND CUVO
METHOD
Participant
Kay, a 44-year-old female, had suffered a cardiac arrest at the age of 33 which resulted in anoxic encephalopathy. Cognitive evaluation revealed WAIS-R scores of 96, 86, and 91 for Verbal, Performance, and Full Scale, respectively. Clinical reports cited impairments of short-term verbal and nonverbal memory. She had been a resident of various post-acute residential rehabilitation facilities for 8 years. At the time of this study, Kay resided at a post-acute residential rehabilitation facility that taught living skills (including how to self-treat minor illnesses) to rehabilitation clients. Kay had little difficulty relearning complex physical operant chains such as basic cooking, home maintenance, and laundry skills. Kay exhibited poor performance, however, making discriminations when discriminative stimuli were not visual (e.g., identifying and treating cold symptoms appropriately).
Settings and Sessions
Training and testing occurred in a rehabilitation facility class- room (20 X 30 m) containing a table (3 X 4 m) and 6 chairs. Training sessions, 50 minutes in duration, were conducted 5 days per week.
Materials
A plastic basin containing first aid materials, various types and brands of medication, a telephone (disconnected), and phone- book were present on the table during each trial. A complete list of medical materials is shown in Table I.
Scenarios
The instructional tasks consisted of treating four different classes of simulated cold symptoms (i.e. , nonworsening colds, worsening colds, worsening colds with no end, and worsening colds that become more serious). These four symptom groups
SELF-TREATMENT OF COLD SYMPTOMS/363
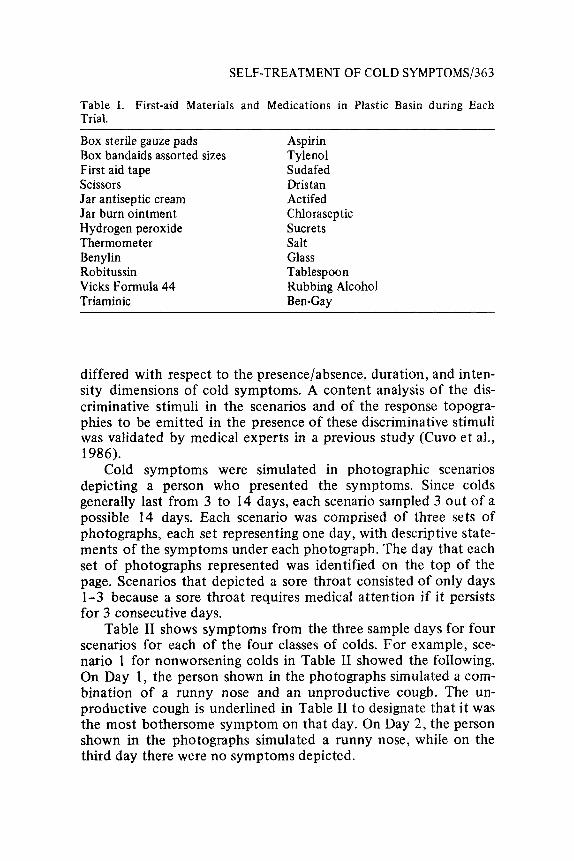
Table I. First-aid Materials and Medications in Plastic Basin during Each Trial.
Box sterile gauze pads Aspirin Box bandaids assorted sizes T yle no 1 First aid tape Sudafed Scissors Dristan Jar antiseptic cream Actifed Jar burn ointment Chloraseptic Hydrogen peroxide Sucrets Thermometer Salt Benylin Glass Robitussin Tablespoon Vicks Formula 44 Rubbing Alcohol Triaminic Ben-Gay
differed with respect to the presence/absence, duration, and inten- sity dimensions of cold symptoms. A content analysis of the dis- criminative stimuli in the scenarios and of the response topogra- phies to be emitted in the presence of these discriminative stimuli was validated by medical experts in a previous study (Cuvo et al., 1986).
Cold symptoms were simulated in photographic scenarios depicting a person who presented the symptoms. Since colds generally last from 3 to 14 days, each scenario sampled 3 out of a possible 14 days. Each scenario was comprised of three sets of photographs, each set representing one day, with descriptive state- ments of the symptoms under each photograph. The day that each set of photographs represented was identified on the top of the page. Scenarios that depicted a sore throat consisted of only days 1-3 because a sore throat requires medical attention if it persists for 3 consecutive days.
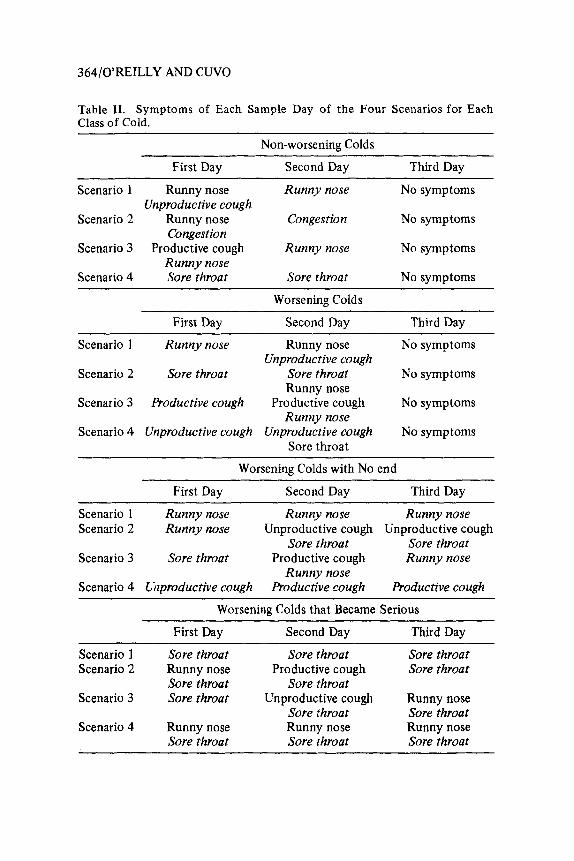
Table I1 shows symptoms from the three sample days for four scenarios for each of the four classes of colds. For example, sce- nario 1 for nonworsening colds in Table I1 showed the following. On Day 1, the person shown in the photographs simulated a com- bination of a runny nose and an unproductive cough. The un- productive cough is underlined in Table I1 to designate that it was the most bothersome symptom on that day. On Day 2, the person shown in the photographs simulated a runny nose, while on the third day there were no symptoms depicted.
364/O’REILLY AND CUVO
Table 11. Symptoms of Each Sample Day of the Four Scenarios for Each Class of Cold.
Non-worsening Colds
First Day Second Day Third Day
Scenario 1 Runny nose Runny nose No symptoms
Scenario 2 Runny nose Congestion No symptoms
Scenario 3 Productive cough Runny nose No symptoms
Scenario 4 Sore throat Sore throat N o symptoms
Unproductive cough
Congestion
Runny nose
~
Worsening Colds
First Day Second Day Third Day
Scenario 1 Runny nose Runny nose No symptoms
Scenario 2 Sore throat Sore throat No symptoms
Scenario 3 Productive cough Productive cough No symptoms
Scenario 4 Unproductive cough Unproductive cough No symptoms
Unproductive cough
Runny nose
Runny nose
Sore throat
Worsening Colds with No end ~ ~~ ~~
First Day Second Day Third Day
Scenario 1 Runny nose Runny nose Runny nose Scenario 2 Runny nose Unproductive cough Unproductive cough
Sore throat Sore throat Scenario 3 Sore throat Productive cough Runny nose
Runny nose Scenario 4 Cizproductive cough Productive cough Productive cough
Worsening Colds that Became ISerious
First Day Second Day Third Day
Scenario 1 Sore throat Sore throat Sore throat Scenario 2 Runny nose Productive cough Sore throat
Scenario 3 Sore throat Unproductive cough Runny nose Sore throat Sore throat
Scenario 4 Runny nose Runny nose Runny nose Sore throat Sore throat Sore throat
Sore throat Sore throat
SELF-TREATMENT OF COLD SYMPTOMS/365
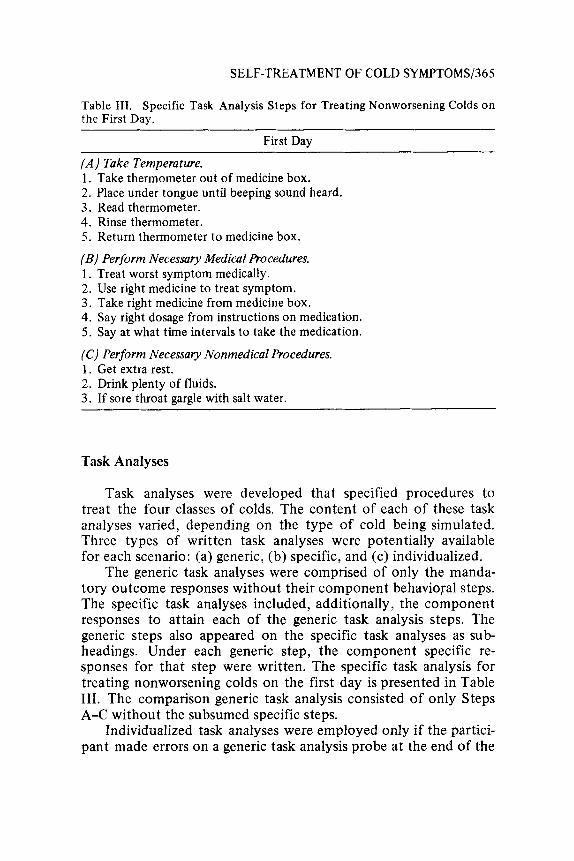
Table 111. Specific Task Analysis Steps for Treating Nonworsening Colds on the First Day.
First Day
( A ) Take Temperature. 1. Take thermometer out of medicine box. 2. Place under tongue until beeping sound heard. 3. Read thermometer. 4. Rinse thermometer. 5 . Return thermometer to medicine box.
(B) Perform Necessary Medical Procedures. 1. Treat worst symptom medically. 2. Use right medicine to treat symptom. 3. Take right medicine from medicine box. 4. Say right dosage from instructions on medication. 5 . Say at what time intervals to take the medication.
(C) Perform Necessary Nonmedical Procedures. 1. Get extra rest. 2 . Drink plenty of fluids. 3. If sore throat gargle with salt water.
Task Analyses
Task analyses were developed that specified procedures to treat the four classes of colds. The content of each of these task analyses varied, depending on the type of cold being simulated. Three types of written task analyses were potentially available for each scenario: (a) generic, (b) specific, and (c) individualized.
The generic task analyses were comprised of only the manda- tory outcome responses without their component behavioral steps. The specific task analyses included, additionally, the component responses to attain each of the generic task analysis steps. The generic steps also appeared on the specific task analyses as sub- headings. Under each generic step, the component specific re- sponses for that step were written. The specific task analysis for treating nonworsening colds on the first day is presented in Table 111. The comparison generic task analysis consisted of only Steps A-C without the subsumed specific steps.
Individualized task analyses were employed only if the partici- pant made errors on a generic task analysis probe at the end of the
366/O’REILLY AND CUVO
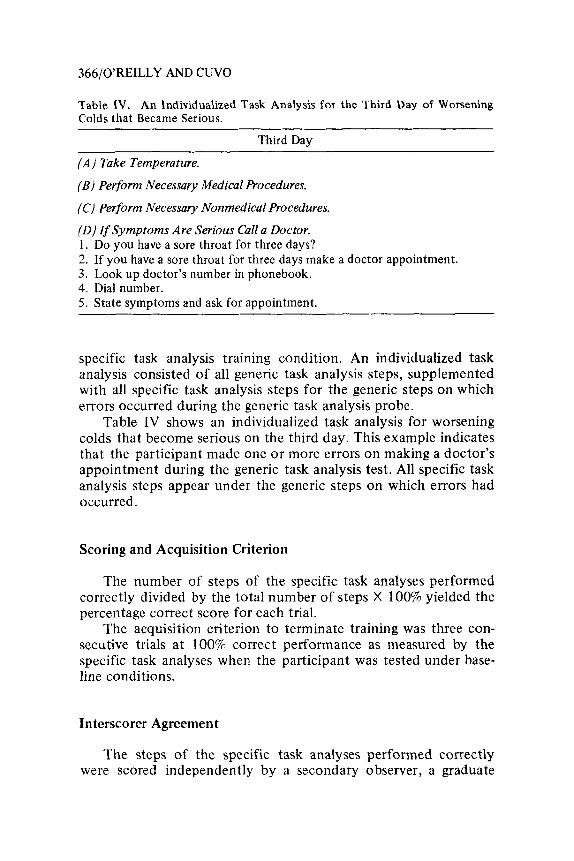
Table IV. An Individualized Task Analysis for the Third Day of Worsening Colds that Became Serious.
Third Day
( A ) Take Temperature.
(B) Perform Necessary Medical Procedures.
(C) Perform Necessary Nonmedical Procedures.
(0) If Symptoms Are Serious Call a Doctor. 1. Do you have a sore throat for three days? 2. If you have a sore throat for three days make a doctor appointment. 3. Look up doctor’s number in phonebook. 4. Dial number. 5 . State symptoms and ask for appointment.
specific task analysis training condition. An individualized task analysis consisted of all generic task analysis steps, supplemented with all specific task analysis steps for the generic steps on which errors occurred during the generic task analysis probe.
Table IV shows an individualized task analysis for worsening colds that become serious on the third day. This example indicates that the participant made one o r more errors on making a doctor’s appointment during the generic task analysis test. All specific task analysis steps appear under the generic steps on which errors had occurred.
Scoring and Acquisition Criterion
The number of steps of the specific task analyses performed correctly divided by the total number of steps X 100% yielded the percentage correct score for each trial.
The acquisition criterion to terminate training was three con- secutive trials at 100% correct performance as measured by the specific task analyses when the participant was tested under base- line conditions.
In terscorer Agreement
The steps of the specific task analyses performed correctly were scored independently by a secondary observer, a graduate
SELF-TREATMENT OF COLD SYMPTOMS/367
student in behavior analysis. The secondary observer was trained by the experimenter preceding the experiment. Observer training consisted of the experimenter modeling the treatment of symp- toms from one scenario from each class of cold. At the end of each trial, both scorers compared data sheets and discussed dis- crepancies. Training trials continued until the secondary observer scored responses on the four types of colds at 100% agreement with the experimenter on two consecutive trials.
Interscorer agreement was taken on 28% of all experimental sessions including all tasks. Interscorer agreement was computed for number of steps performed correctly by dividing the number of agreements by the number of agreements plus disagreements X 100%. Mean interscorer agreement was 97.6% with a range from 86 to lOOa/o.
Experimental Design
Experimental control was demonstrated by a multiple baseline design across the four classes of colds with baseline, generic task analysis, specific task analysis, and individualized task analysis phases embedded. Phase changes within each class of cold oc- curred when the data stabilized. Phase changes between the differ- ent classes of colds occurred when there was noticeable improve- ment in performance in the class of cold under treatment.
Training Procedures
Four different scenarios for each of the classes of colds (See Table 11) were presented in an interspersed manner during training and testing. Interspersal presentation helped ensure that the participant would make discriminations based on the relevant stimulus dimensions presented in the scenarios (i.e., presence/ab- sence and intensity of certain types of symptoms).
The participant responded to one scenario from each type of cold during each trial. For all training conditions subsequent to baseline, the participant received the following instructions: “Read a step, Do what it says, and then check off the step you did with the pencil.” Checking off not only ensured that the partici- pant attended to the textual prompts, but also served a self-moni- toring function. If the participant failed to check off steps, cor- rective feedback was provided at the end of that trial (i.e., “It
368/OREILLY AND C W O
seems like you did not check off each step. Please check off the steps as you go along.”)
Baseline
Prior to the performance of the first baseline trial, the partici- pant was told that her skill at treating various classes of colds would be assessed. The participant was told, “Here is a set of photographs that shows the symptoms a person has for 3 days of a cold. Look at the photographs and read the captions for the first day. Then tell me how you would treat the symptoms. The medi- cine box in front of you contains any medicines you may wish to use. When you are finished treating the symptoms of Day 1, go on to the second day and do the same thing, then go on to the third day.” The experimenter sat in the background, scored responses, and did not provide any contingent prompting, feedback, or other consequences.
Generic Task Analysis Training
The participant was given the written generic task analysis for each type of cold and asked to read it aloud to ensure that she could read the text sufficiently well. The participant read the written generic task analysis for each class of cold without experi- menter prompting. She was then asked to respond to each scenario using the appropriate generic task analysis as a textual prompt. The experimenter sat in the background, engaged in observational recording, and did not provide instruction during the trial.
At the end of each trial, the experimenter provided perform- ance feedback on each step of the generic task analysis sequen- tially. Praise was provided for correct responses, and nonspecific generic feedback for incorrect responses. For example, if the participant did not take her temperature appropriately (e.g., did not place the thermometer under her tongue until a beeping sound was heard), nonspecific feedback took the form: “You did not take your temperature properly. You left out certain things re- lated to taking your temperature.” The experimenter pointed to the written generic task analysis step(s) on which the error(s) occurred (i.e., heading A on Day 1 in Table 111). If scores on any
SELF-TREATMENT OF COLD SYMPTOMS/369
of the four types of colds stabilized at less than 100% correct, specific task analysis training was required.
Specific Task Analysis Training
Prior to training, the participant was given the written specific task analysis for each type of cold and asked to read it aloud to ensure that she could read the text sufficiently well. The partici- pant read the written specific task analysis for each class of cold without experimenter prompting. She was then asked to respond to each scenario using the appropriate specific task analysis as a textual prompt. Again, the trainer did not participate in any direct instruction while the participant was responding to the scenarios. At the end of each trial, step-by-step feedback was given with praise for correct responses. Specific corrective feedback was provided on task analysis steps on which errors occurred. For example, if the participant did not perform the necessary medical procedures (e.g., did not take the right medicine from the medi- cine box on Day l), specific corrective feedback took the form: (e.g., “You did not perform the necessary medical procedures on Day 1. You did not take the right medicine from the medicine box.”) The experimenter pointed to the specific task analysis step(s) on which the error(s) occurred (i.e., Step 3 under heading B on Day 1 in Table 111).
When scores stabilized at 100% correct on three consecutive trials for a particular class of cold, the generic task analysis probe was administered. The participant was tested using only the written generic task analysis as a prompt. If the participant scored 100% correct on this generic task analysis probe, she proceeded to the baseline condition. If she did not score 100% correct on the probe, she then proceeded to individualized task analysis training for that type of cold.
Individualized Task Analysis Training
Individual task analyses were developed based on an error analysis on the generic task analysis probe. Use of the individual- ized task analysis was explained verbally and with gestures. For example, the participant was told, “You performed these steps
370/0’REILLY AND CUVO
correctly (experimenter pointed to the generic task analysis steps without their specific steps printed underneath). The steps with the numbered steps underneath are the steps on which you made errors, (experimenter pointed to the generic task analysis steps with printed specific task analysis steps printed underneath). You can use these guidelines to perform the task with no errors.”
If a score of 100% correct was not achieved on the first trial using the individualized task analysis as a textual prompt without response contingent feedback, then individualized task analysis training was begun for that class of cold. The individualized task analysis was used as a prompt, and step-by-step feedback was given as described for the specific task analysis condition. If the participant made a novel error on a generic step that was not supplemented with individualized specific task analysis steps, then the experimenter provided specific feedback on the error(s). The individualized task analysis was revised for the next trial to include written specific task analysis steps on which errors occurred during the previous training trial. When 100% correct was scored, the generic task analysis probe was readministered as described previ- ously. If 100% was scored on the generic task analysis probe, the participant proceeded to the baseline condition for that class of cold.
Follow-up
Follow-up testing under baseline conditions was conducted on all tasks 1 week and 1 month after training to assess response maintenance.
Maintenance Training
Generic task analysis probes, and if necessary, individualized task analysis training conditions were reintroduced for all four classes of colds following maintenance assessment to retrain cor- rect responding to 100%.
RESULTS
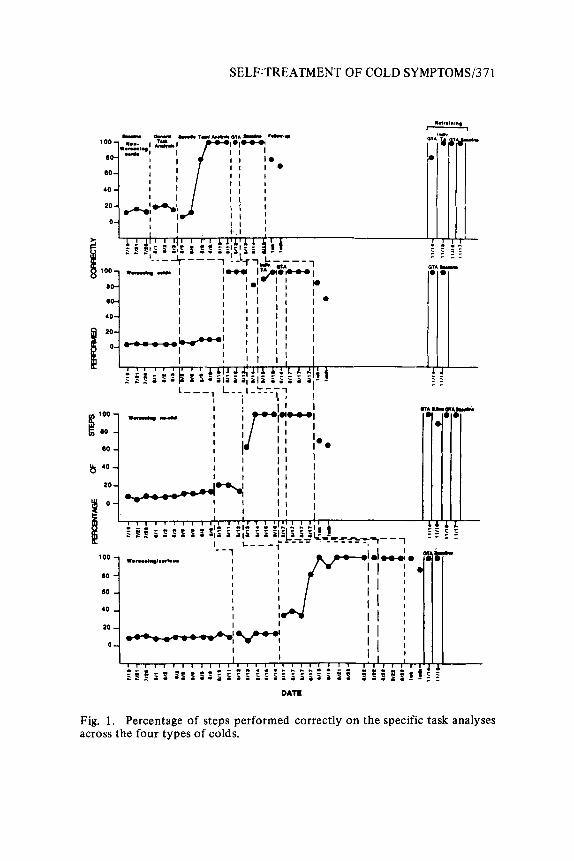
Figure 1 shows data across the four classes of cold symptoms (i.e., nonworsening, worsening, worsening with no end, worsening
SELF:TREATMENT OF COLD SYMPTOMS/371
DATE
k
Fig. 1 . Percentage of steps performed correctly on the specific task analyses across the four types of colds.
372/OREILLY AND CUVO
that became serious). Low stable initial baselines are evident across all four classes of colds. Little improvement over baseline scores occurred when the written generic task analyses were used as prompts and nonspecific feedback was provided. The generic task analysis training condition was inadequate to promote effec- tive stimulus control over the target behaviors.
When the specific task analysis condition was employed, re- sponding rapidly improved to the criterion level (Le., three consec- utive trials at 100% correct). Following specific task analysis training, correct performance was maintained for nonworsening, worsening with no end, and worsening that became serious colds during the generic task analysis probe. The participant did not achieve 100% correct on the generic task analysis probe for worsening colds; therefore, she received two individualized task analysis trials. All classes of colds met the terminal objective of 100% correct performance on three consecutive baseline trials.
The participant remained at 100% correct responding for only one class of cold (worsening that became serious) at a 1 week follow-up, but failed to maintain 100% correct responding on any class of cold at a 1 month follow-up. Dramatic decreases in correct responding are evident during follow-up probes with 62% correct responding for worsening no-end colds a t 1 week and 64% correct responding for worsening colds at 1 month.
Correct responding rapidly improved again to the 100% cri- terion under baseline conditions for worsening, worsening no end, and worsening/serious colds when the generic task analysis re- training condition was introduced. Nonworsening colds required individualized task analysis re training in addition to generic task analysis training to return to 100% criterion responding under baseline conditions.
DISCUSSION
Results showed that using self-administered specific task analy- ses as prompts, self-monitoring, and specific performance feedback only at the end of training trials, an anoxic brain injured adult learned appropriate treatment of different types of colds. No direct trainer instruction was provided while the participant re- sponded during training trials. Previous research has demonstrated
SELF-TREATMENT OF COLD SYMPTOMS/373
that persons with mental retardation have learned similar health care skills (Brickey, 1978; Cuvo et al., 1986; Matson, 1980). The present study extends that literature to a head injured person.
As in the Mooney (1988) study, generic task analyses com- bined with nonspecific generic feedback did not exert stimulus control. Specific task analyses combined with specific feed- back resulted in criterion performance across all tasks in both the present and the Mooney (1988) study. Follow-up results indicate that transfer of stimulus control to picture cues did not maintain over time for this head injured individual. These results contrast with those of Mooney (1988) for whom mildly retarded participants maintained accurate responding during follow-up probes.
In the present study, correct responding returned to criterion levels under baseline conditions for three classes of colds when the generic task analysis training condition was re-introduced. Non- worsening colds required one individualized task analysis training probe in addition to generic task analysis training to return to criterion responding under baseline conditions. Re training results indicate that the less intrusive training strategy (i.e., written generic task analyses combined with generic feedback at the end of trials) was an effective means of promoting continued respond- ing at criterion levels for this head injured participant.
Future research with individuals who have been labeled as having severe short-term memory deficits should further investi- gate stimulus control procedures. Written cues could provide age- appropriate, nonstigmatizing, permanent prompts in situations where fading of cues may not result in long-term transfer of stimulus control. In addition, other skill maintenance training techniques (e.g., self-reinforcement) also should be assessed. Furthermore, additional independent living and vocational tasks should be targeted across different types of head injuries to isolate relevant variables involved in acquisition, maintenance, and gen- eralization of skills across subgroups of this population.
The authors’ thanks go to the staff and clients of the Evaluation and Developmental Center at Southern Illinois University at Carbondale where the research was conducted. We also would like to acknowledge with thanks Ruth Crowley who served as secondary observer. Requests for reprints may be addressed to the second author at: Rehabilitation Institute, Southern Illinois University at Carbondale, Carbondale, IL 62901.
374/O’REILLY AND CUVO
References
Agran, M., & Martin, J. E. (1987). Applying a technology of self-control in community environments for individuals who are mentally retarded. In M. Hersen, R. M. Eisler, & P. M. Miller (Eds.), Progress in behavior modification (Vol. 21). New York: Academic.
Brickey, M. (1 978). A behavioral procedure for teaching self-medication. Mental Retardation, 16, 29-32.
Browder, D. M., & Shapiro, E. S . (1985). Applications of self-management to individuals with severe handicaps: A review. Journal of the Associatic-; for Persons with Severe Handicaps, 10, 200-208.
Cuvo, A. J., & Davis, P. K. (1983). Behavior therapy and community living skills. In M. Hersen, R. M. Eisler, & P. M. Miller (Eds.),Progress in be- havior modification (Vol. 14). New York: Academic.
Cuvo, A. J., Davis, P. K., Faw, G. D., Wilson, P., Boitos, T., Kyle, M., & Kessler, M. L. (1986). A behavioral strategy for teaching health care to rehabilitation clients: Self-treatment and emergency recognition. In A. J. Cuvo and M. L. Jones (Chairs), Innovative topics and topics for skills training. Symposium presented at the meeting of the Association for Behavior Analysis, Milwaukee, WI.
Fisher, M. K. (1984). Vocational assembly skills using isometric projection exploded view drawings for mentally handicapped students. Education and naining of the Mentally Retarded, 19, 285-290.
Gajar, A., Schloss, P. J., Schloss, C. N., & Thompson, C. K. (1984). Relative effects of feedback and self-monitoring on small group conversational behavior of head trauma youth. Journal of Applied Behavior Analysis,
Glasgow, R. E., Zeiss, R. A., Barrera, M. Jr., & Lewinsohn, P. M. (1977). Case studies on remediating memory deficits in brain damaged individuals. Journal of Clinical Psychology, 33, 1049-1 054.
Goldstein, G., & Ruthven, L. (1983). Rehabilitation of the brain damaged adult. New York: Plenum,
Johnson, B., & Cuvo, A. J. (1981). Teaching mentally retarded adults to cook. Behavior Modification, 5 , 187-202.
Koegel, R. L., & Koegel, L. K. (1988). Generalized responsivity and pivotal behaviors. In R. H. Horner, G. Dunlap, & R. L. Koegel (Eds.), Cenerali- zation and maintenance: Life-style changes in applied settings. Balti- more, MD: Brookes Publishing Co.
Lingnugaris/Kraft, B., McCuller, G. L., Exum, M., & Salzberg, C. L. (1988). A review of research on picture reading skills of developmentally dis- abled individuals. The Journal of Special Education, 22(3), 197-229.
17, 353-358.
SELF-TREATMENT OF COLD SYMPTOMS/375
Matson, J . L. (1980). Preventing home accidents: A training program for the retarded. Behavior Modificatbn, 4, 379-41 0.
Mooney, B. M. (1988). The use of general and specific task analyses in the self-management o f instruction by persons with mild handicaps. Unpub- lished master’s thesis, Southern Illinois University at Carbondale, Carbondale, IL.
Vogenthaler, D. R. (1987). An overview of head injury: Its consequences and rehabilitation. Brain Injury, 1 , 1 13-1 17.
Wacker, D. P., & Berg, W. K. (1983). Effects of picture prompts on the acqui- sition of complex vocational tasks by mentally retarded adolescents. Journal ofApplied BehaviorAnalysis, 16, 417-433.
Wacker, D. P., & Berg, W. K. (1984). Training adolescents with severe handi- caps to set up job tasks independently using picture prompts. Analysis and Intervention in Developmental Disabilities, 4, 353-365.
Wacker, D. P., Berg, W. K., Berrie, P., & Swatta, P. (1985). Generalization and maintenance of complex skills by severely handicapped adolescents following picture prompt training, Journal of Applied Behavior Analy- sis, 1 8, 3 2 9-3 36.
Zahara, D. J. , & Cuvo, A. J. (1984). Behavioral applications to the rehabilita- tion of traumatically head injured persons. Clinical Psychology Review, 4,477-491.