Embed Size (px)
Citation preview
BRTO complications
Saher Sabri ,MD
University of Virginia

Saher Sabri, M.D.
• Speakers Bureau: W.L.Gore & Associates, Abbott
BRTO complications
• Short term– Shunt extravasation– Varix Rupture– Balloon rupture– PE– PVT– Stroke– Sepsis
• Long term– Worsening ascites and hydrotorax– Worsening esophageal varices
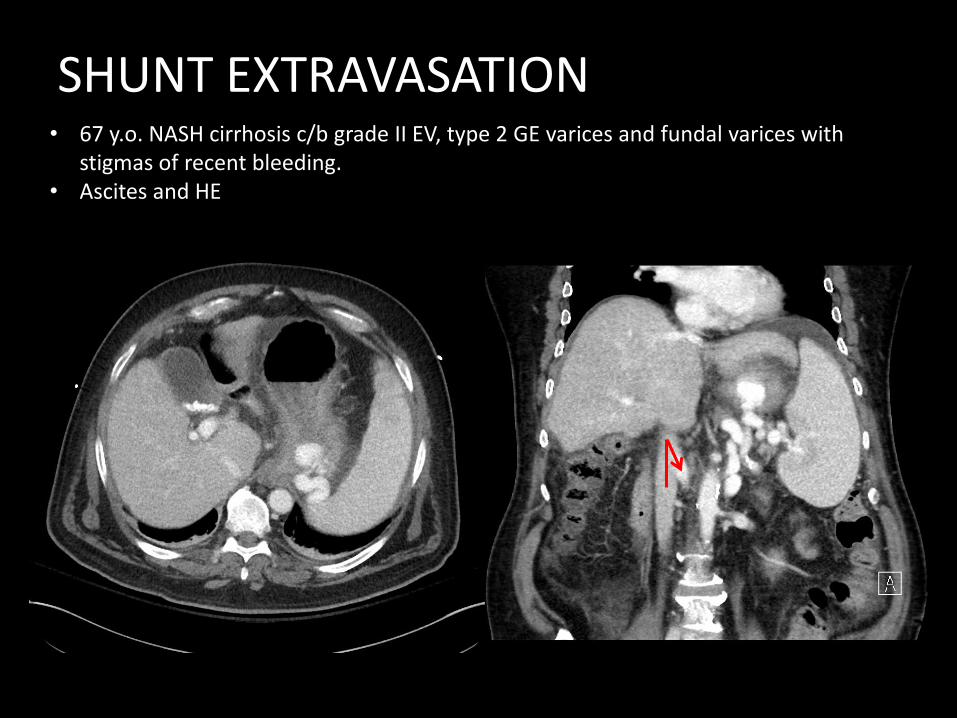
SHUNT EXTRAVASATION • 67 y.o. NASH cirrhosis c/b grade II EV, type 2 GE varices and fundal varices with
stigmas of recent bleeding. • Ascites and HE
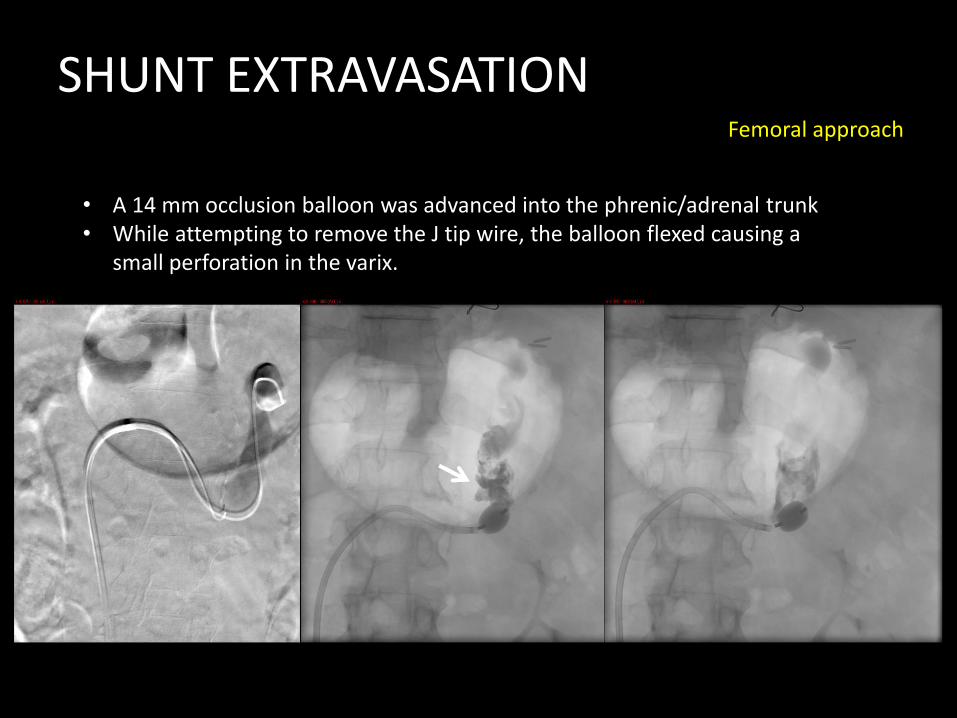
Femoral approach
• A 14 mm occlusion balloon was advanced into the phrenic/adrenal trunk• While attempting to remove the J tip wire, the balloon flexed causing a
small perforation in the varix.
SHUNT EXTRAVASATION
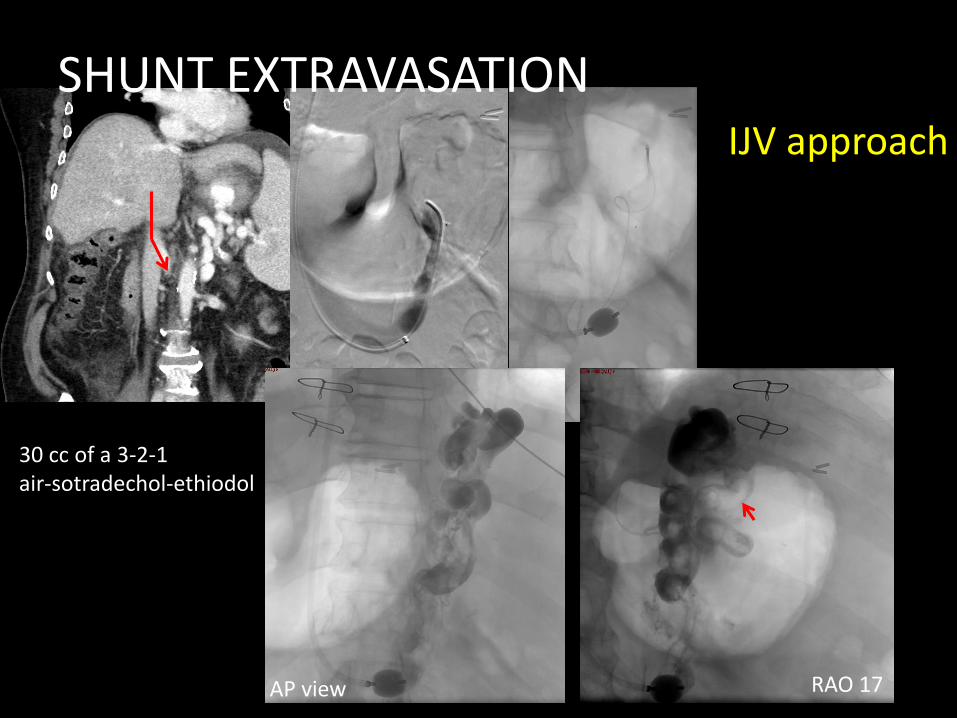
AP view RAO 17
IJV approach
30 cc of a 3-2-1 air-sotradechol-ethiodol
SHUNT EXTRAVASATION
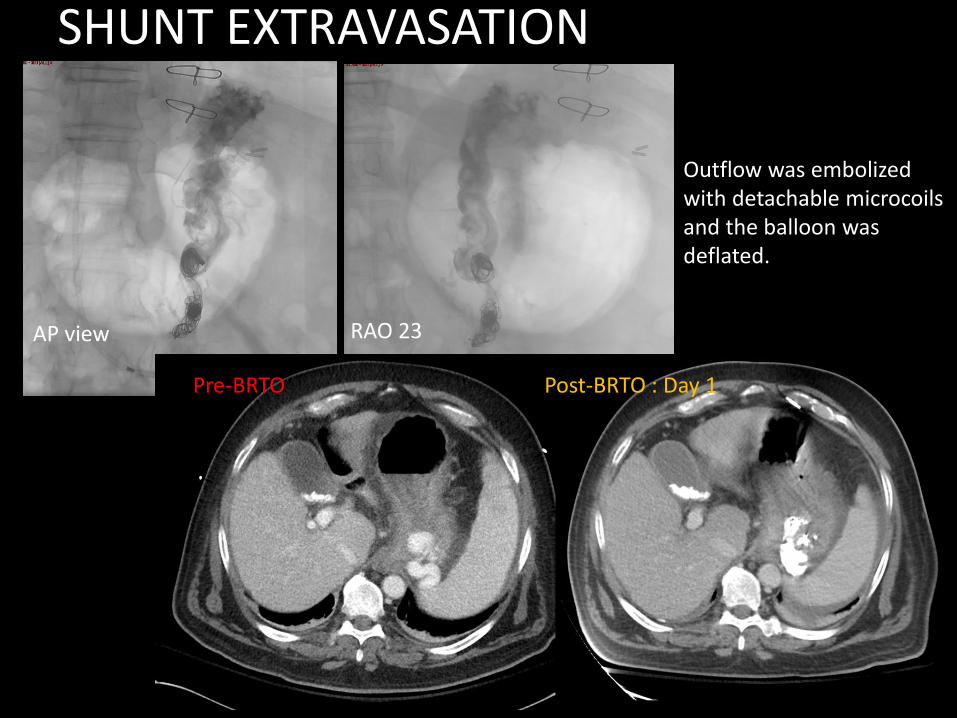
AP view RAO 23
Post-BRTO : Day 1
Outflow was embolizedwith detachable microcoilsand the balloon was deflated.
Pre-BRTO
SHUNT EXTRAVASATION
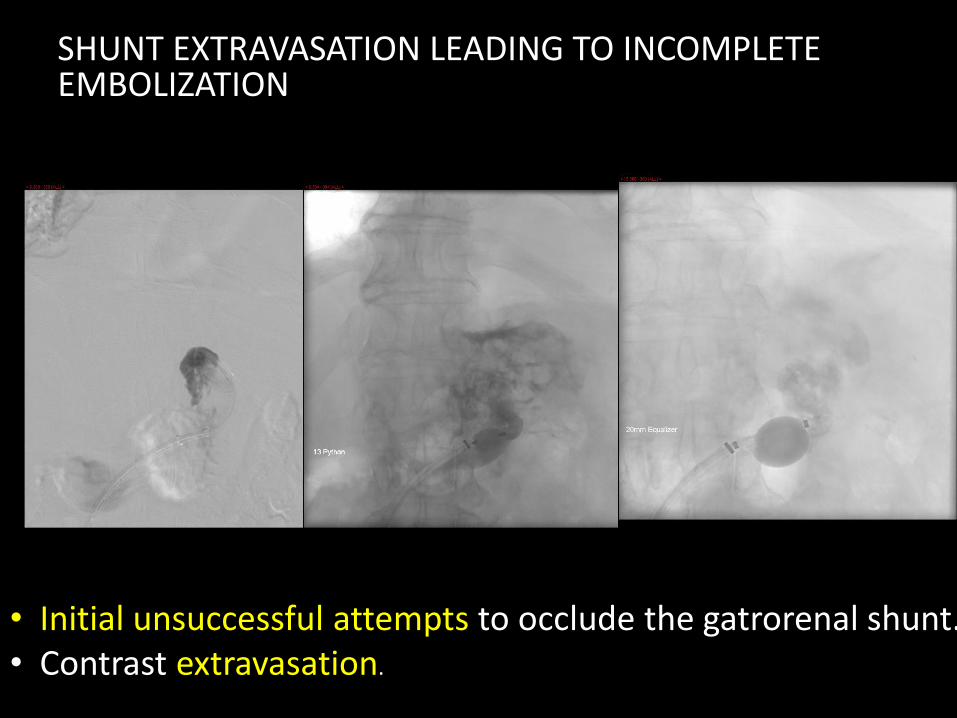
SHUNT EXTRAVASATION LEADING TO INCOMPLETE EMBOLIZATION
• Initial unsuccessful attempts to occlude the gatrorenal shunt.• Contrast extravasation.
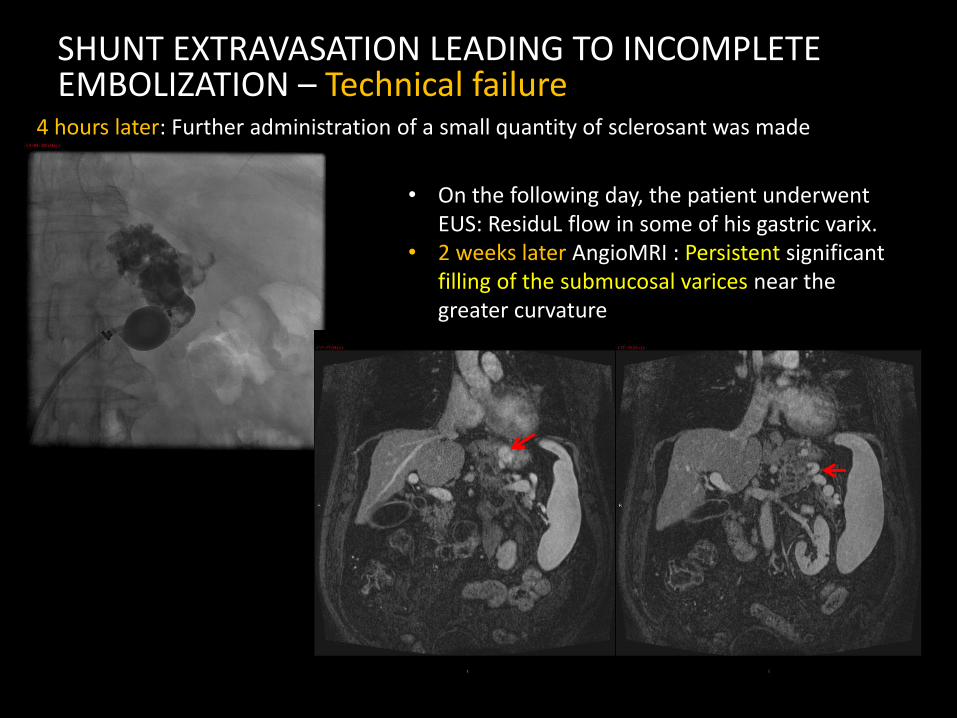
SHUNT EXTRAVASATION LEADING TO INCOMPLETE EMBOLIZATION – Technical failure
• On the following day, the patient underwent EUS: ResiduL flow in some of his gastric varix.
• 2 weeks later AngioMRI : Persistent significant filling of the submucosal varices near the greater curvature
4 hours later: Further administration of a small quantity of sclerosant was made
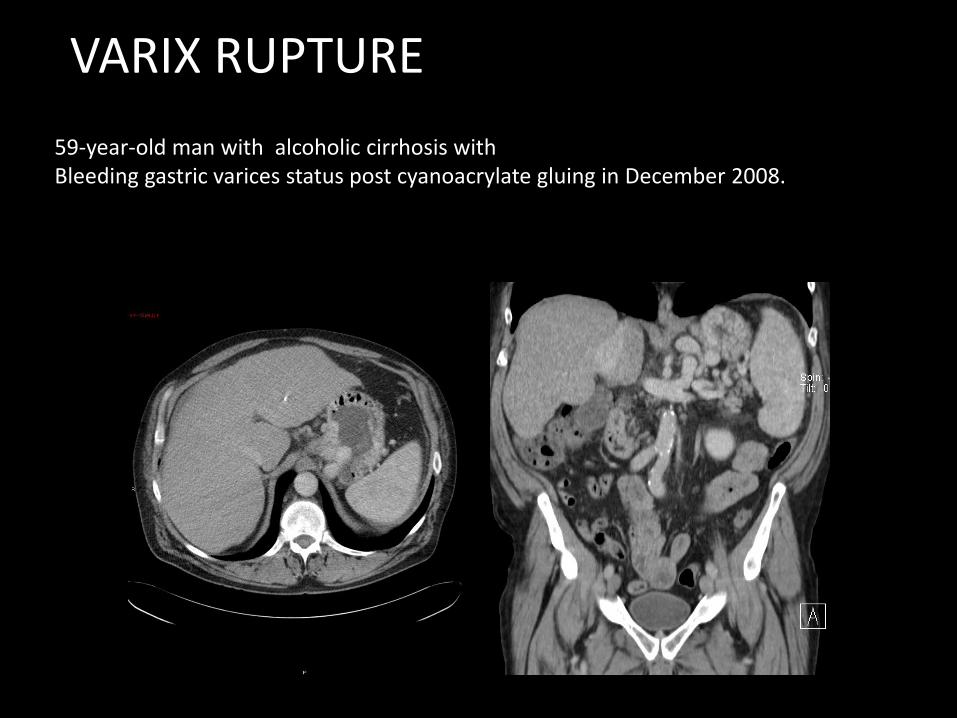
VARIX RUPTURE
59-year-old man with alcoholic cirrhosis with Bleeding gastric varices status post cyanoacrylate gluing in December 2008.
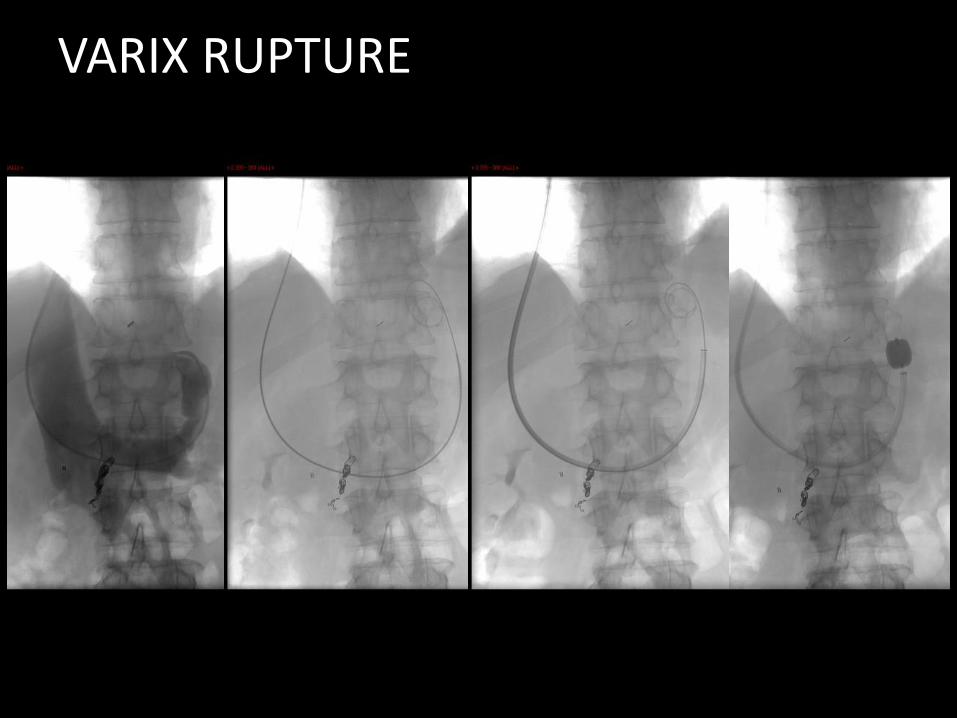
VARIX RUPTURE

VARIX RUPTURE
Varix rupture
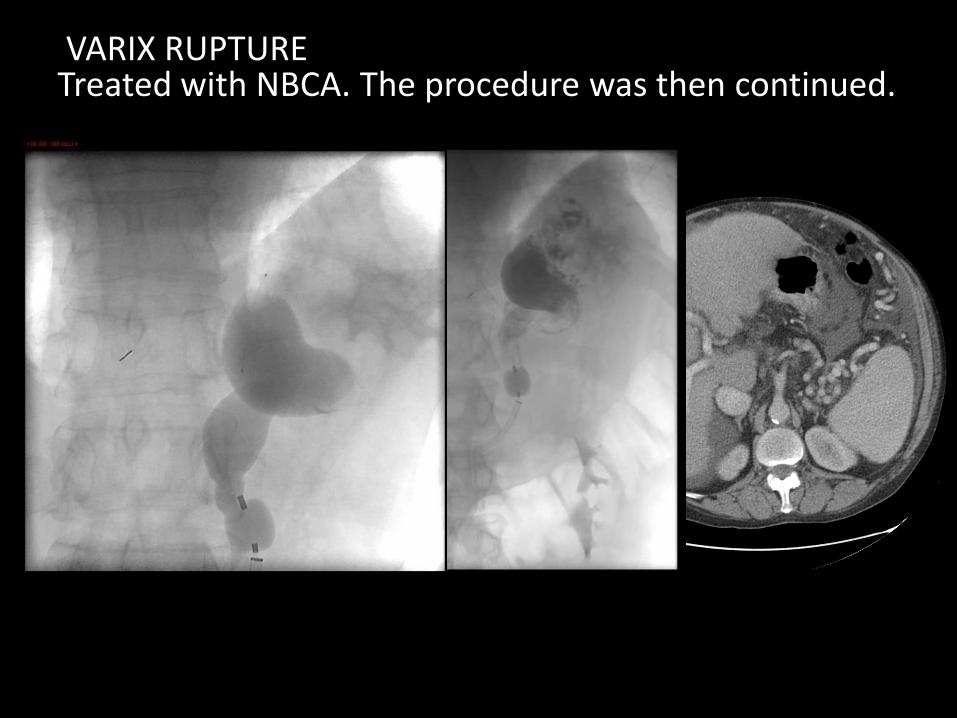
VARIX RUPTURETreated with NBCA. The procedure was then continued.

• 68 years old male with NASH /alcohol cirrhosis,• Encephalopathy and • Gastric varices with recent history of GI bleed• Transplant candidate
BALLOON RUPTURE
BALLOON RUPTURE
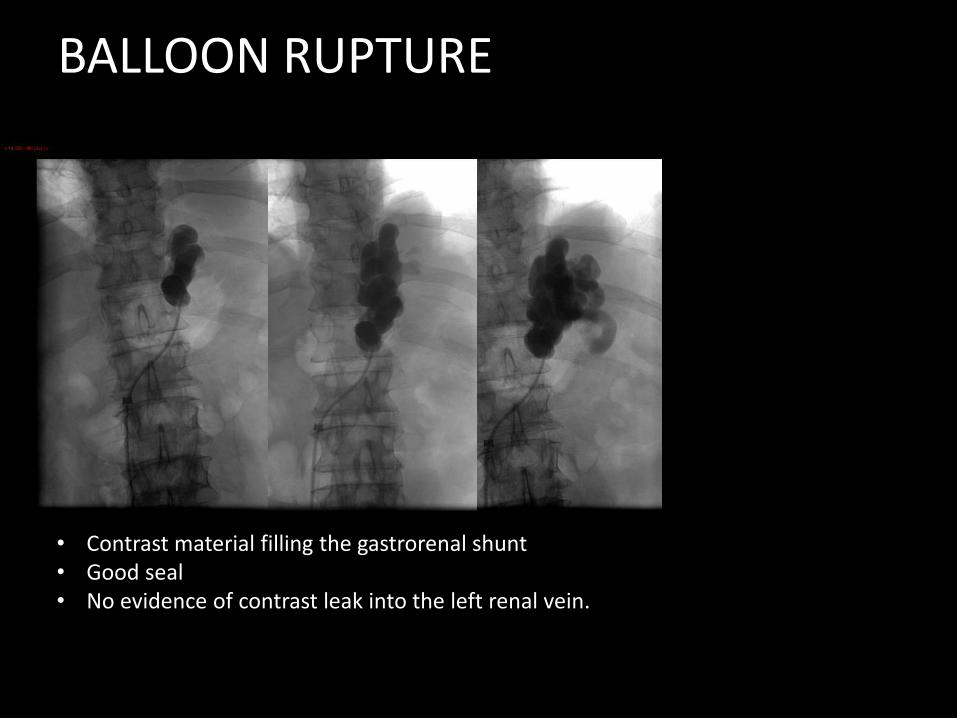
• Contrast material filling the gastrorenal shunt • Good seal • No evidence of contrast leak into the left renal vein.
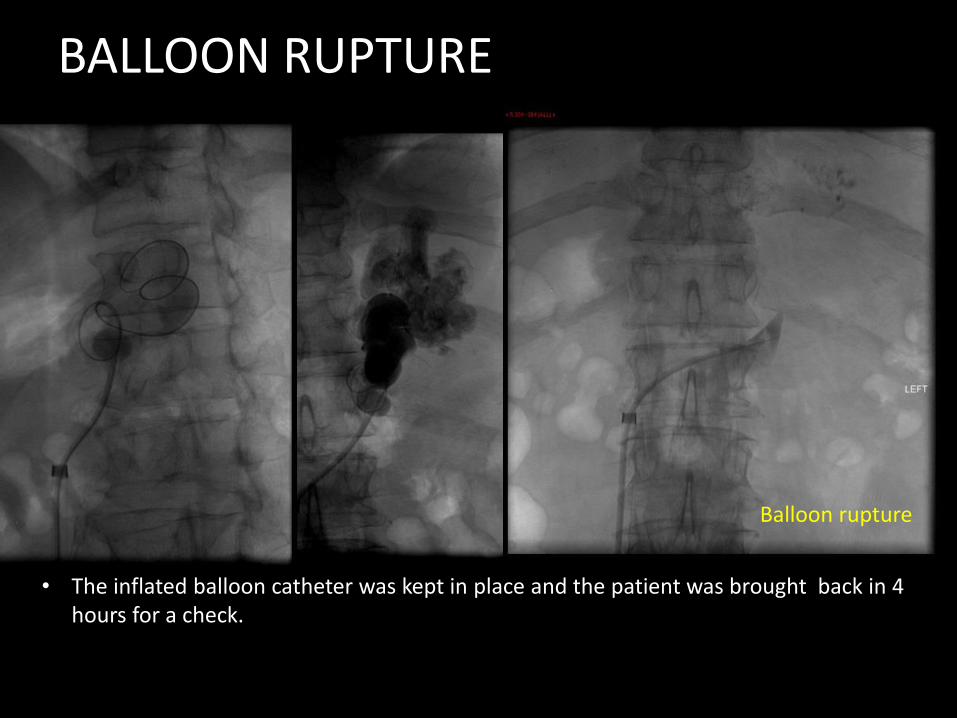
Balloon rupture
BALLOON RUPTURE
• The inflated balloon catheter was kept in place and the patient was brought back in 4 hours for a check.
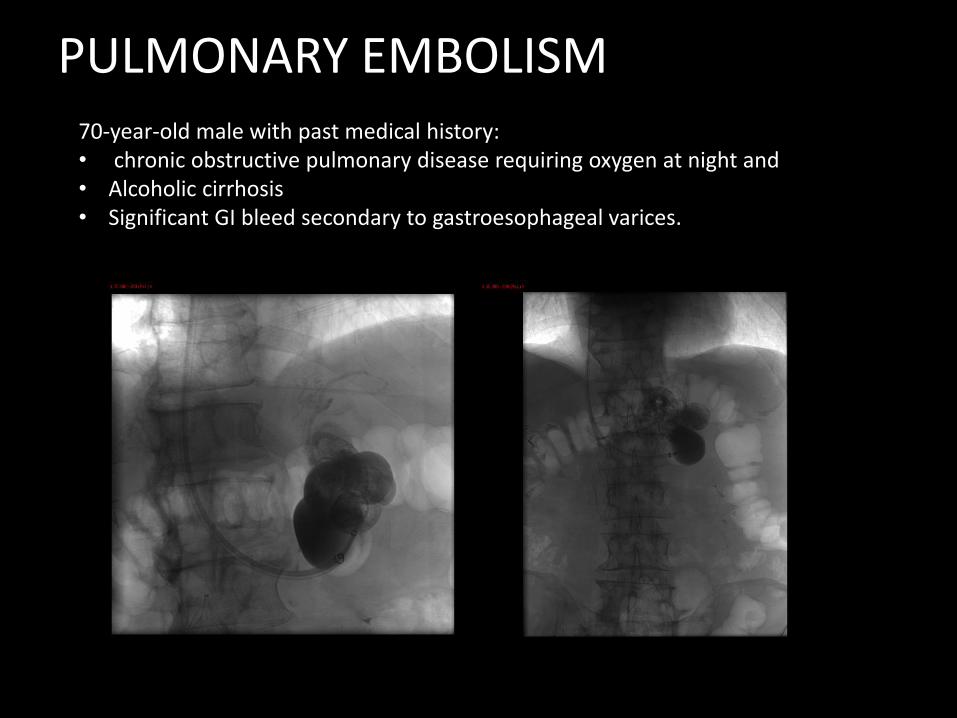
PULMONARY EMBOLISM70-year-old male with past medical history:• chronic obstructive pulmonary disease requiring oxygen at night and • Alcoholic cirrhosis • Significant GI bleed secondary to gastroesophageal varices.
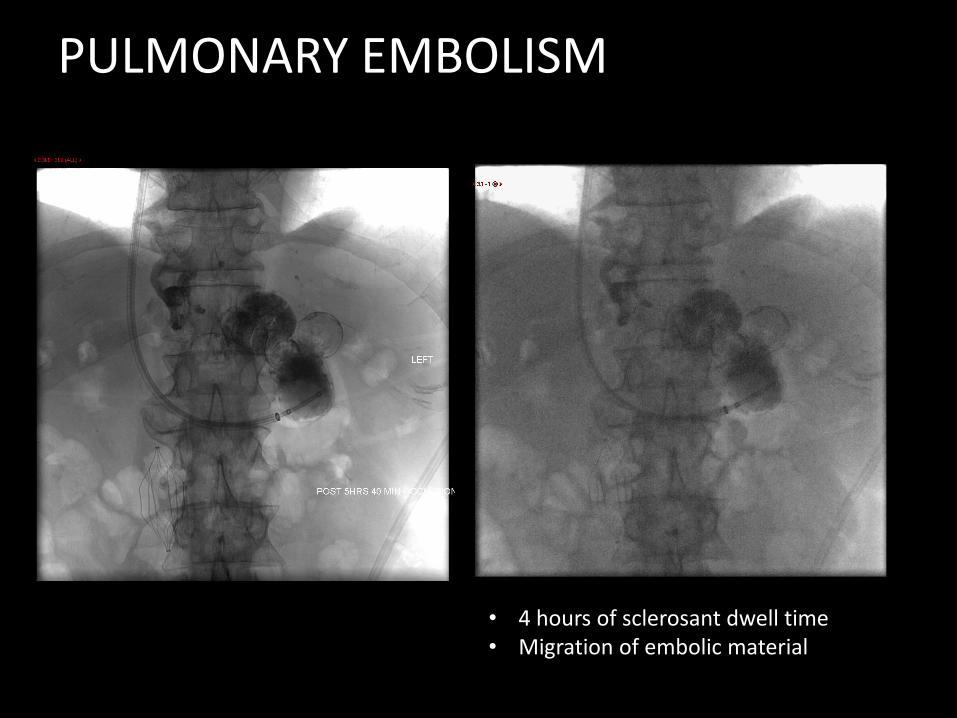
PULMONARY EMBOLISM
• 4 hours of sclerosant dwell time• Migration of embolic material

PULMONARY EMBOLISM
• 12 hours later• Additional sotradecol + coils
Incomplete embolization. Likely secondary to multiple affferentveins

• 56-year-old female with NASH cirrhosis and a history of recurring upper GI bleed secondary to a gastric varices.
• Upper endoscopy: gastric varix without esophageal varices or significant gastropathy
• Chronic mild encephalopathy .
Partial PVT
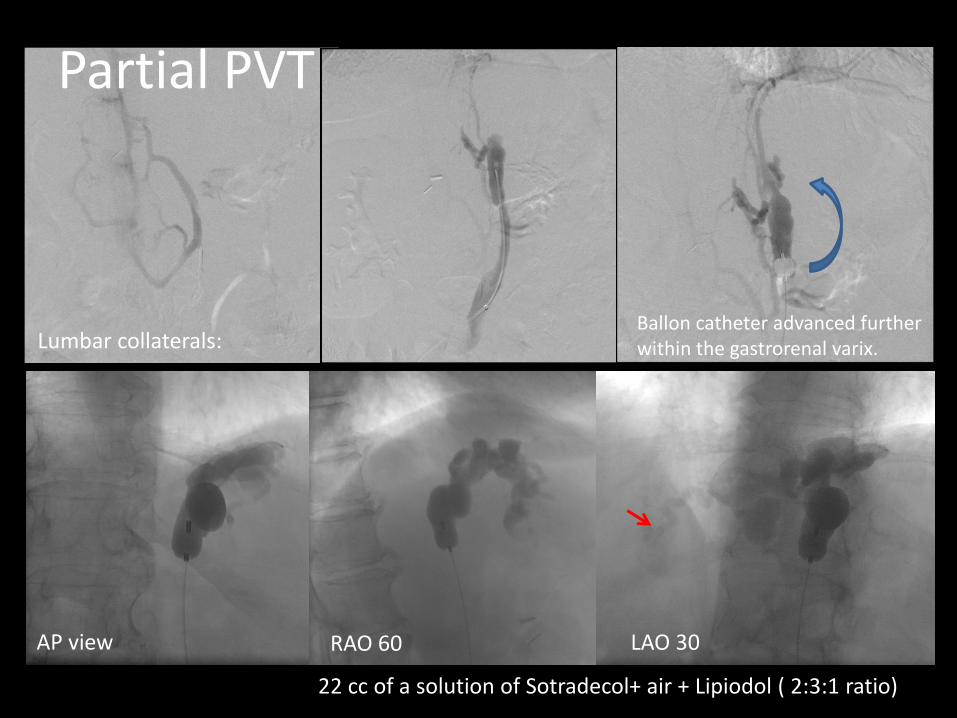
AP view RAO 60 LAO 30
Lumbar collaterals:
22 cc of a solution of Sotradecol+ air + Lipiodol ( 2:3:1 ratio)
Ballon catheter advanced further within the gastrorenal varix.
Partial PVT
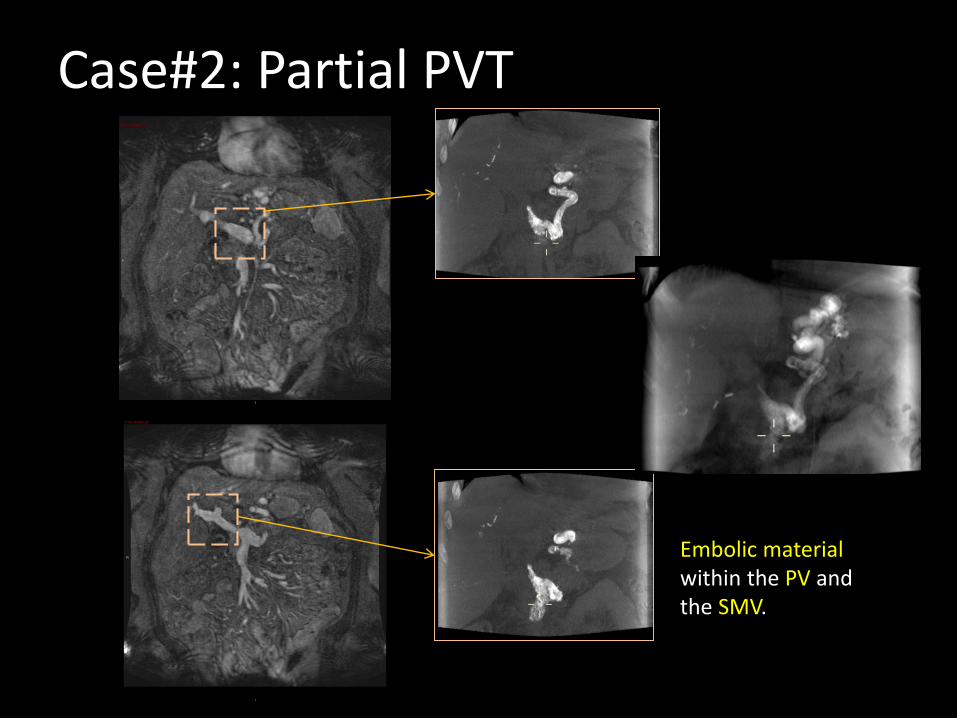
Case#2: Partial PVT
Embolic material within the PV and the SMV.
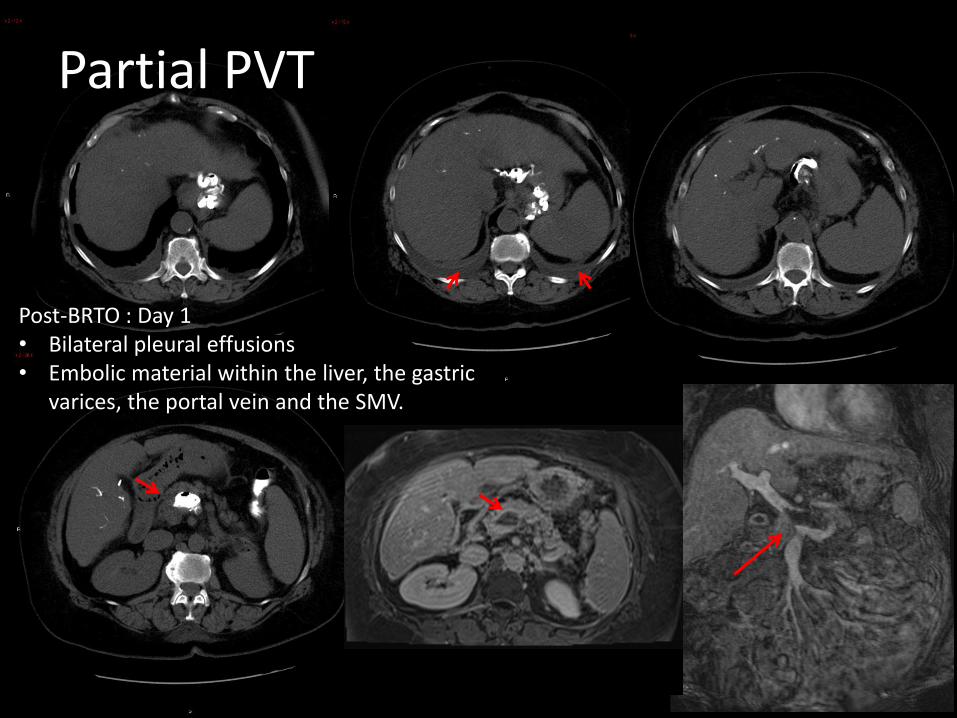
Partial PVT
Post-BRTO : Day 1• Bilateral pleural effusions• Embolic material within the liver, the gastric
varices, the portal vein and the SMV.
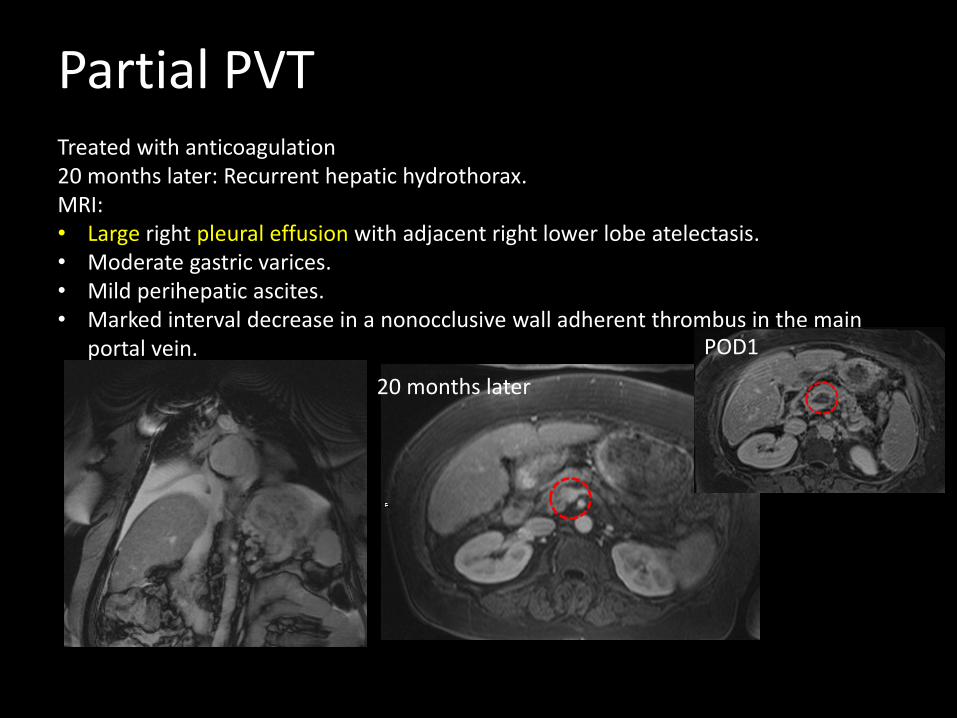
Partial PVTTreated with anticoagulation20 months later: Recurrent hepatic hydrothorax.MRI: • Large right pleural effusion with adjacent right lower lobe atelectasis.• Moderate gastric varices.• Mild perihepatic ascites.• Marked interval decrease in a nonocclusive wall adherent thrombus in the main
portal vein. POD1
20 months later
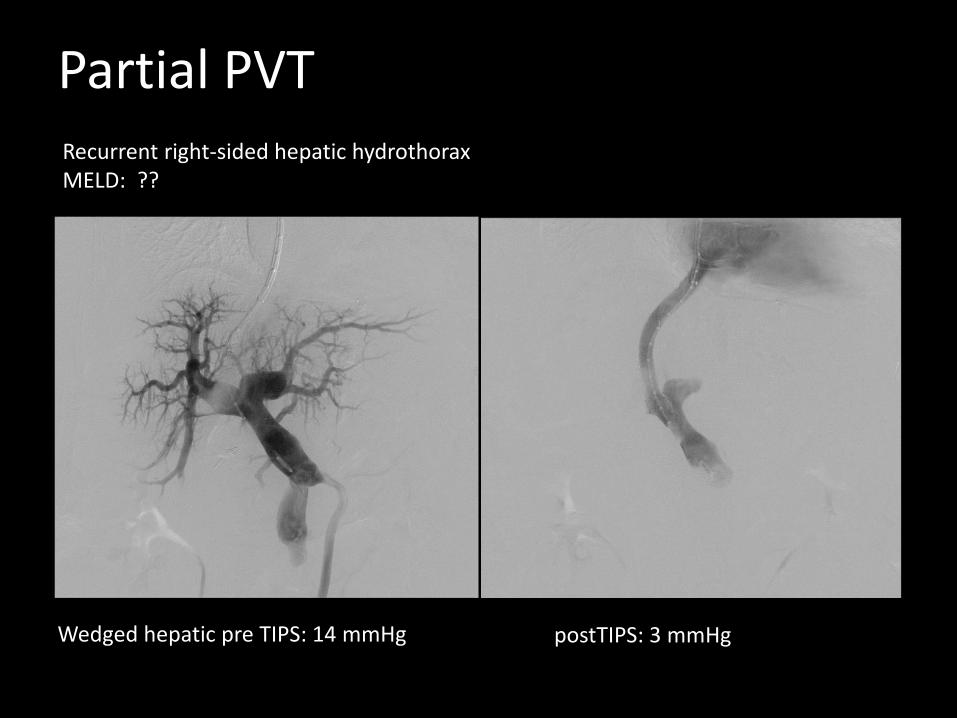
Wedged hepatic pre TIPS: 14 mmHg postTIPS: 3 mmHg
Partial PVTRecurrent right-sided hepatic hydrothoraxMELD: ??
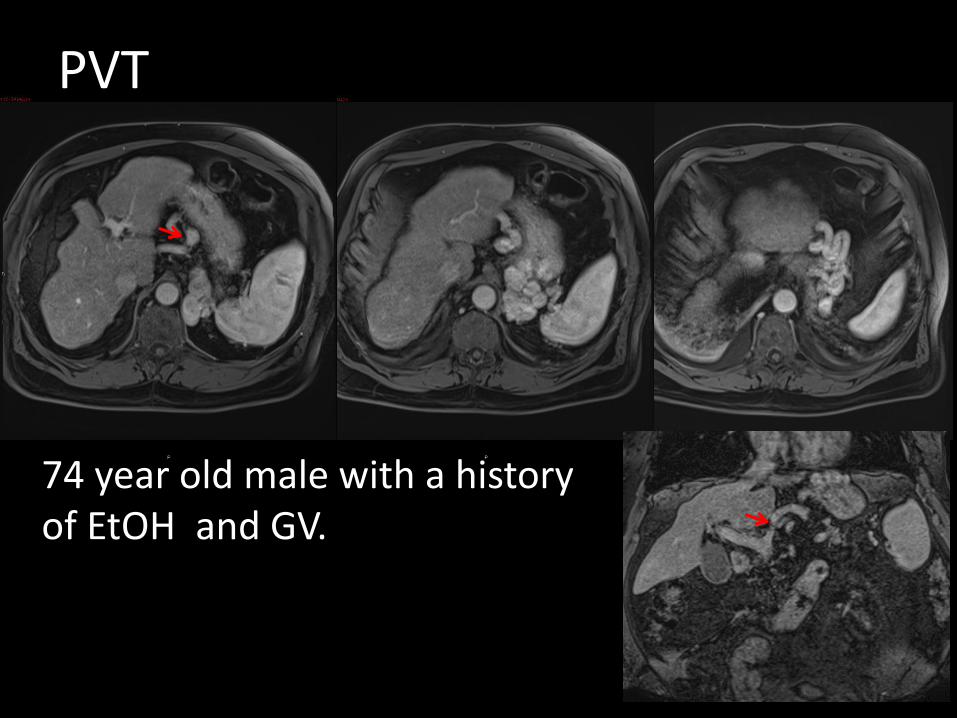
74 year old male with a history of EtOH and GV.
PVT
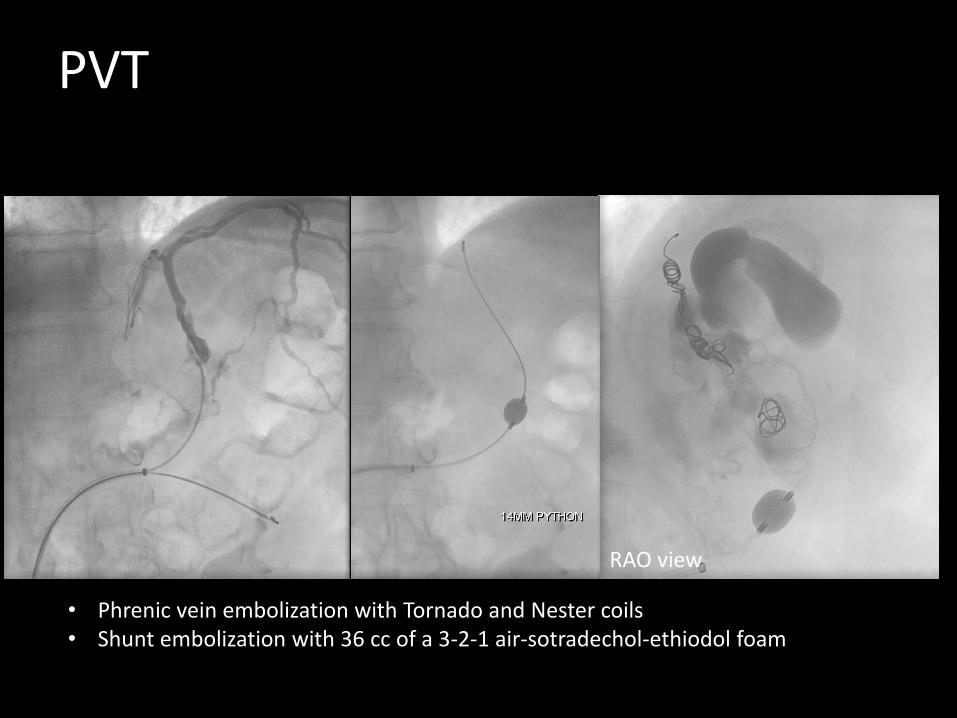
RAO view
• Phrenic vein embolization with Tornado and Nester coils • Shunt embolization with 36 cc of a 3-2-1 air-sotradechol-ethiodol foam
PVT
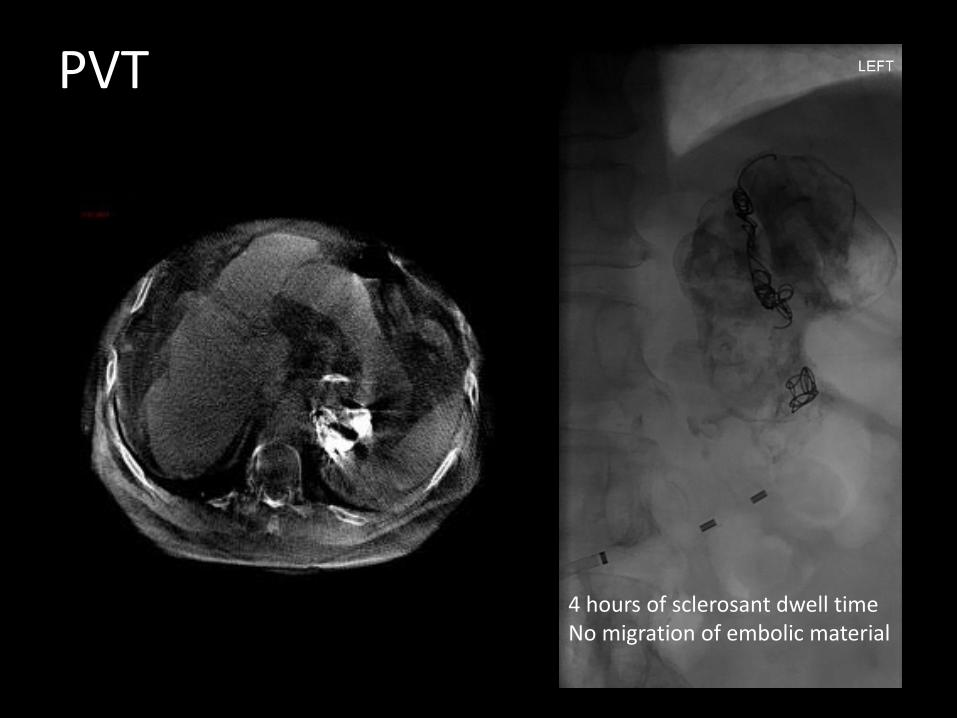
4 hours of sclerosant dwell timeNo migration of embolic material
PVT
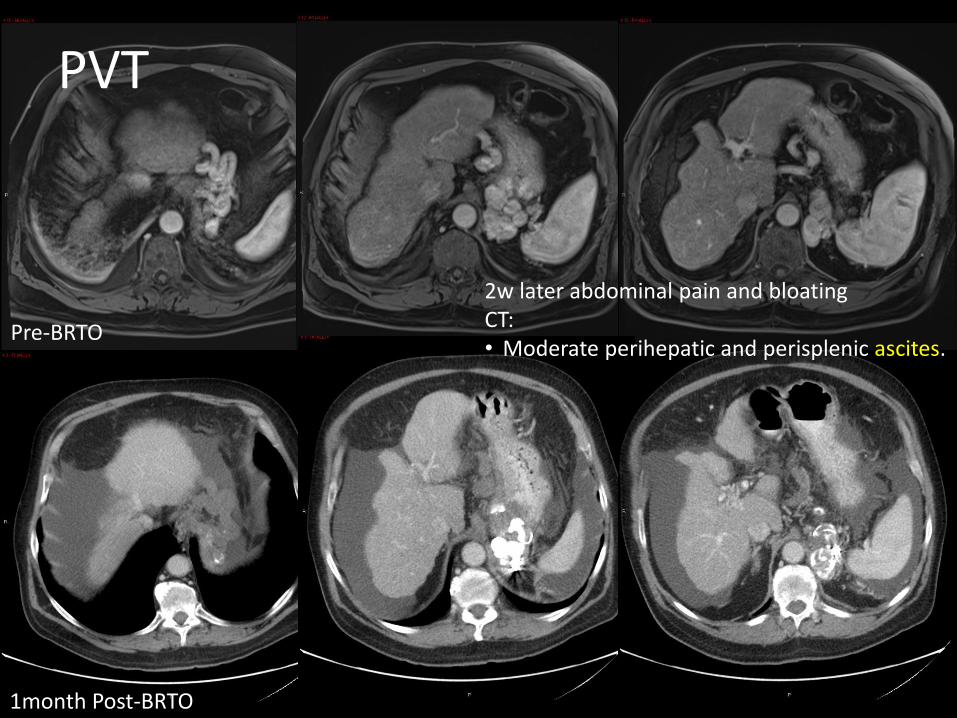
1month Post-BRTO
Pre-BRTO
2w later abdominal pain and bloatingCT:• Moderate perihepatic and perisplenic ascites.
PVT
PVT
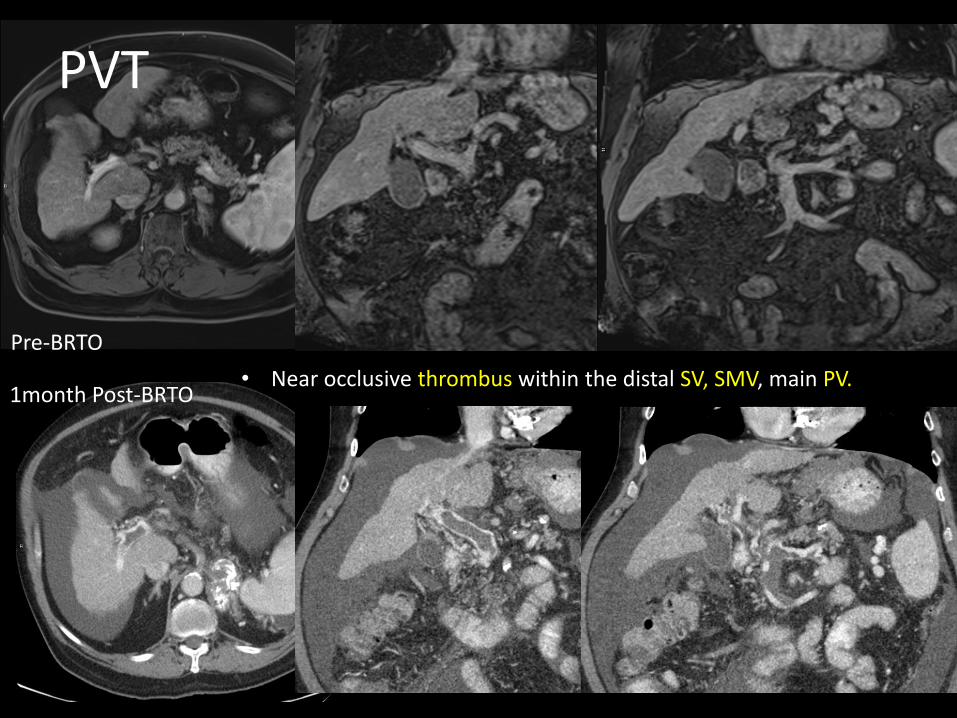
1month Post-BRTO
Pre-BRTO
• Near occlusive thrombus within the distal SV, SMV, main PV.
PVT
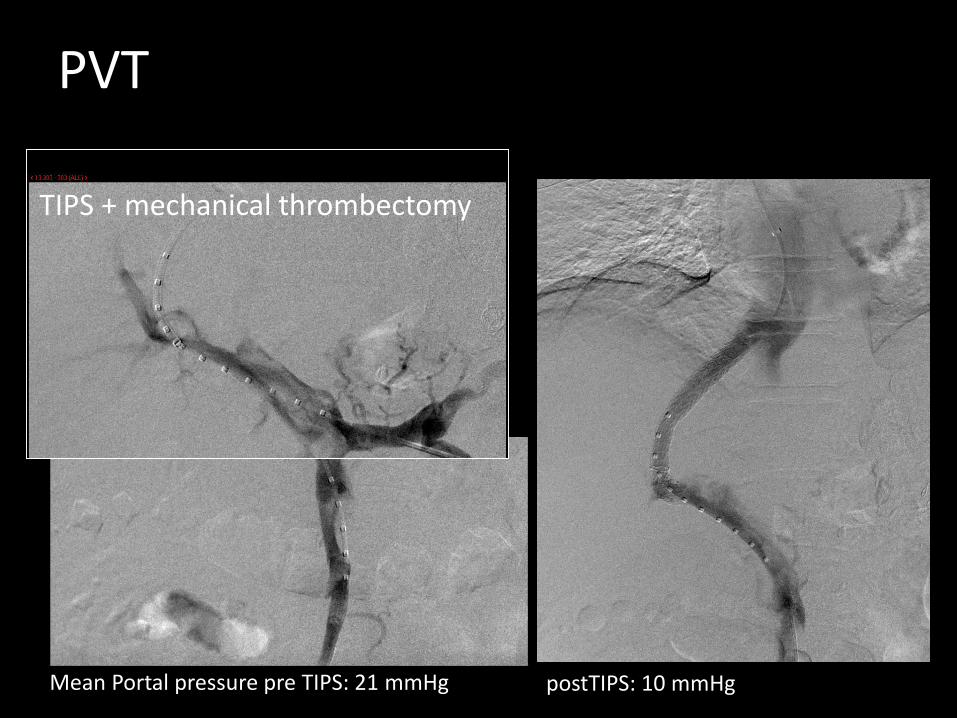
Mean Portal pressure pre TIPS: 21 mmHg postTIPS: 10 mmHg
TIPS + mechanical thrombectomy
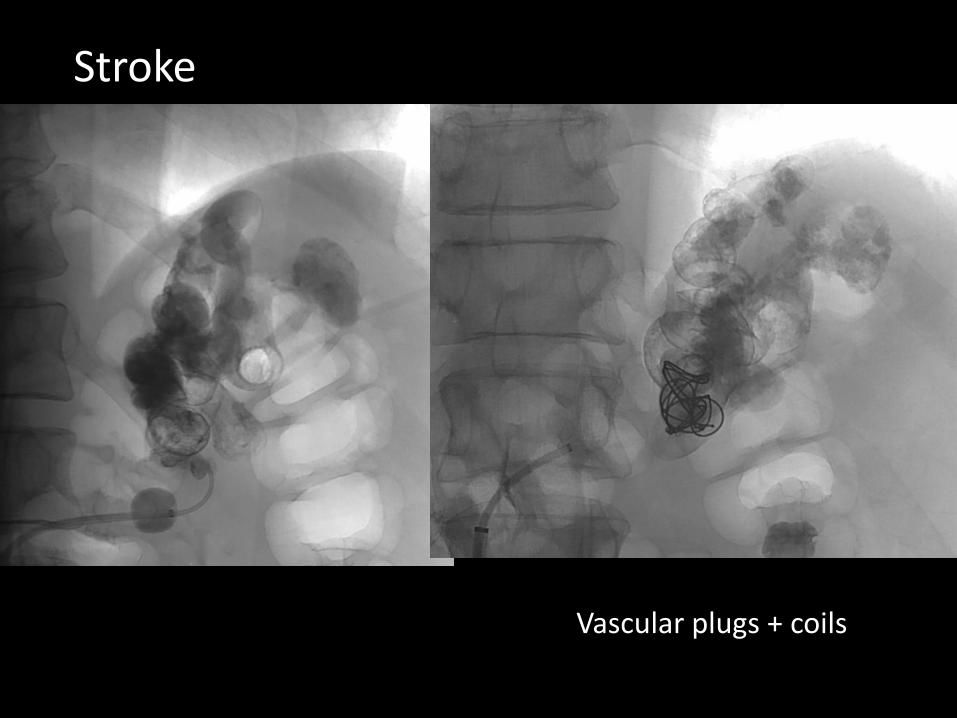
Vascular plugs + coils
Stroke
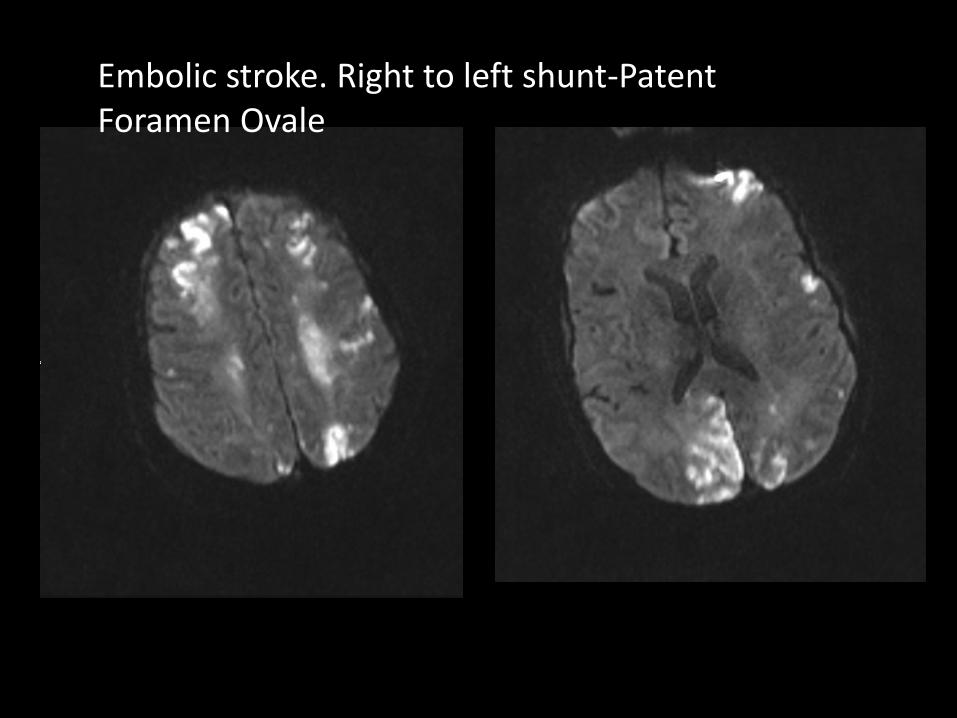
Embolic stroke. Right to left shunt-Patent Foramen Ovale
BRTO complications
• Short term– Shunt extravasation– Varix Rupture– Balloon rupture– PE– PVT– Stroke– Sepsis
• Long term– Worsening ascites and hydrothorax– Worsening esophageal varices