Embed Size (px)
Citation preview

Technical quality and standards session:
What is my agency doing?
Global Health Cluster Partner Meeting 17-19 June 2015
Geneva, Switzerland
GHC Partners: CDC (Richard Garfield) ERA/AMU (Ossama Rasslan) [by email] IMC (Jill John Kall) IOM (Teresa Zakaria) Malteser (Marie-Therese Benner) Medair (Trina Helderman) SC (Francesco Checchi) UNHCR (Allen Maina) Unicef (Heather Papowitz) WVI (Ando Raobelison)

Ground rules
• About 5 min per agency
• About 2 min questions per agency
• Some space at the end for any other contributions
• Main idea is to map initiatives, not discuss in depth their merit / details

CDC Related Methods and Measurement
Global Health Cluster Partner Meeting 17-19 June 2015
Geneva, Switzerland
Richard Garfield

SMART



EWARN

Special Surveys
• Mortality
• Injury
• Disability
• WASH
• Vaccine campaign coverage
• MISP

Quality Improvement in ERA/AMU Performance
Global Health Cluster Partner Meeting 17-19 June 2015
Geneva, Switzerland
Prof. Ossama Raslsan, Secretary General, AMU
Supervisor, ERA

Who we are
• Arab Medical Union (AMU) is the union of medical syndicates, professional societies and organizations in the Arab World.
• It was established in Egypt 1962, for the purpose of fortifying the efforts to enhance medical practice and health status in the Arab world, as well as coordinating efforts in humanitarian work world wide.
Objectives To become a leading organization in the whole region AMU
aimed at: - Promoting medical profession, building capacity of medical personnel and improving health status in the Arab world. - Taking care of Emergency and Relief wherever the need calls - Supporting Vulnerable, Migrants and Refugees . - Achieving professional integration between Arab Countries
in medical fields - Building and exchanging Medical expertise among AMU countries. .

Main Functioning Bodies of AMU

I- The Arab Institute for Continuing Professional Development (AICPD)
AICPD is a non for profit institute affiliated to AMU.
It aims at raising the standards of healthcare practice through the provision of vocational training programs in various medical, surgical and health-related specialties.
These programs equip physicians and other healthcare professionals with core competencies needed to practice as specialists in their respective field.

II- Emergency And Relief Agency ERA

• ERA is the biggest AMU committee , established in early nineties.
• Whatever the nature of a crisis affecting a population - natural disaster, political crisis, armed conflict, etc. - ERA intervenes.
• Our emergency response aims to satisfy emergency needs especially medical ones.
• Taking into account the material needs that are essential for survival, is at the heart of our emergency response programs.

Improving Performance How did we do that with our
very limited resources?

1- Capacity Building • To facilitate adoption and implementation of
accountability and transparency measures to respond to donors, clients, governmental agencies and the community.
• To support and promote the implementation and/or improvement of ERA performance measures.

• To promote research that contributes with new knowledge, best practices, and innovative strategies to strengthen ERA, their operations, image and public trust.
• To promote the integration of evaluation as part of the institutional control system.
Capacity building comprised two main functions:
Medical Staff capacity building
Admin staff capacity building

Medical Staff capacity building
How did we use AICPD in Capacity Building?

We created a Professional Diploma in Disaster Management
Curriculum Contents Disaster cycle phases and the appropriate management Specific Multiple Casualty Treatment Research in Disaster Medicine Disaster Mental Health Education and Training in Disaster Medicine Leadership During Disasters Humanitarian Emergencies Media Management during disasters Communications during disasters Transport during disasters Trauma Management

AICPD Partners


Admin Staff Capacity Building • Proposal writing training
• Many training courses and workshops have been conducted to build the capacity of our staff;
• The proposal does not stand alone. It must be part of a process of planning and of research on, outreach to, and cultivation of potential foundation and corporate donors.
• Raising funds is an investment in the future. It takes time and persistence to succeed.

2- Strategic Planning • Strategic planning guided by experts was approved as
a corner stone in improving ERA performance.
• A clear strategic plan strengthens the idea behind the organization and how it can move forward.
• Establishing an organization with a mission and objectives is just one part of the work; running it in the right direction is equally important.
• A strategic plan really did that; it has guided the organization to move towards the same mission and objectives for which it was developed.

3- Initiatives • Ibsar ( Fighting Blindness Centre )
• It’s a committee for fighting blindness all over the Globe
• Managed to do over 25.000 operations to date bring back the hope to those who have lost it
• Succeeded in cutting down the cost to almost 20%
• All its work is based on donations and all the operations were completely for free

• Maak ( Disability limitation Centres )
• With over 7 centres across Egypt, Maak is helping daily hundreds of mentally disabled and neglected children
• Providing support for both the children and the families, Maak has issued a manual to be used as a guide for how to deal with cases, creating a success story for others to be inspired.

Motadaminon ( Psycho-social support Centre )
• A committee specialized in providing psycho-social support for those who need it
• A lot of sessions were conducted in refugee camps where families, especially children, were severely traumatized after they have lost everything because of war (e.g. Syrian Refugees )


Future initiatives
• There are increasing calls from crisis-affected communities, governments of disaster-prone countries, donor foundations, as well as the general public, for a fair global system, which will help objectively verify the impact and quality of humanitarian aid agencies; regardless of their origin or size.

• Better understanding of the impact of these interconnected trends and approaches
• Share best practices and find innovative ways to make humanitarian action more effective
• Transformation through innovation
• Serving the needs of people in conflict.

Thank You

Presentation Title ©2012 International Medical Corps
Improving Quality of Emergency Health Programs
From Relief to Self-Reliance
Dr. Jill John-Kall Health Advisor
All content in this document is the property of International Medical Corps and should not be reproduced without prior written consent. This material is protected by copyright. ©2015 International Medical Corps. Materials may not be reproduced without International Medical Corps’ prior written consent.

Presentation Title ©2012 International Medical Corps
Approaches
Country teams and HQ staff work together to improve assessments and program design: • Regional outlook • Adaptability in remote management programs • Sector advisors (Health, SRH, WASH, MH, GBV, PSCM, DRR, M&E) provide
assistance and help integrate various programs • Technical learning sessions • Sharing of lessons learned from similar contexts (emergency response,
early recovery and HSS) • Continue to work with Ministries of Health, donors and other partners to
address needs across emergency, early recovery and development phases • Continue to provide capacity building to local staff and partners

Presentation Title ©2012 International Medical Corps
Assessments
• M&E technical workshop on needs assessments for 17
countries which will be replicated in country • Focused on overcoming realities on the ground, sector
specific issues and standardized tool kits but to maintain flexibility to adapt tools on the ground in real time as needed
• Explore mHealth options for more efficient data collection and analysis
• Continue to work with all stakeholders and input to assessment processes

Presentation Title ©2012 International Medical Corps
Technical Capacity Building
• Training of health care workers in all contexts; training needs are met with in country training sessions, eLearning modules, overseas training, etc.
• Provide support to Ministries to develop training curricula for health workforce, support national level hospitals in clinical care and management; support verification of suspected communicable diseases especially in conflict areas with limited access
• Sector specific training (M&E, SRH, GBV)
• Non technical training (English, computer skills, leadership/managerial skills)
Presentation Title ©2012 International Medical Corps
Health Information Management
• Emergency Response Information System (ERIS)
• DHIS 2
• Data quality audits
• Exploring mHealth modalities for common issues: digitizing data at the point of service delivery to improve patient information and reduce errors; using available apps for reporting purposes, especially for inaccessible areas

Presentation Title ©2012 International Medical Corps
Pharmaceutical Supply Chain Management
• Train field staff on tools for quality assurance and quality to manage the flow, storage and distribution of medical commodities (PSCM manual)
• Use National, WHO and/or donor specific essential drug lists to support the rational selection of medicines and treatment guidelines to support RUD
• Utilize a transparent procurement system- only WHO/donor prequalified suppliers are openly bidding on our tenders
• Member of QUAMED consortium and participate in trainings and supplier assessment surveys

Presentation Title ©2012 International Medical Corps
END

Health Management at Borders Lessons Learnt and Opportunities
International Organization for Migration
GHC Meeting, 19 June 2015

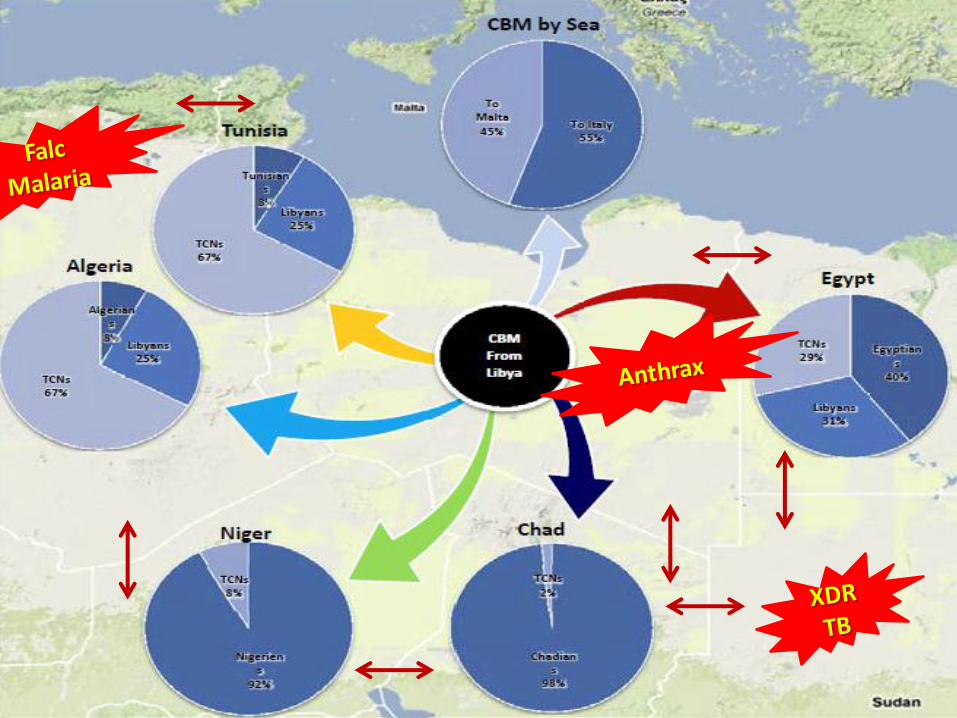
West Africa EVD Outbreak How Human Mobility Exacerbates Infection
Transmission
“Even if you have a contact tracing system, what do you do when your contact picks up
and moves 60 km away one morning without telling you? If Ebola moves from location A to
location B, suddenly you need to duplicate everything…This explains a large part of why the control systems were overrun so quickly” – A. Petherick (2015), Ebola in West Africa: learning
the lessons. The Lancet, 385 (9968), 591-592.

Understanding mobility for better prevention, detection and response
to health threats
• The importance of mobility
– A known social determinant of health
– Direct contribution of spread of diseases
– A special skills set not possessed by many…
• Displacement vs mobility tracking
• The added value of integrating mobility pattern mapping with other sectors

The
Mo
bility C
on
tinu
um
And everything outside
the border

Understanding mobility for better prevention against health threats
• Better targeting of preventive measures
• Better targeting of resource allocation
• Working with otherwise unidentified vulnerable communities
• The role of transit points and destinations in prevention actions
Understanding mobility for better detection of health threats
• The border buffer zone and the importance to identify mobility hotspots – 20 km radius?
• Screening at the market places and the mines?
• Alert to important spots along the mobility continuum

Understanding mobility for better response to health threats
• Strategic stock-piling
• Proper referrals from hotspots
• Contact tracing
• PHC strengthening along the vulnerable corridor

Arising Opportunities & Challenges
• The tripartite cooperation (IOM-WHO-CDC)
• “A new science in the making”
• How to document knowledge rapidly?
• Validity of the approach, tools, SOPs?

Thank you!

Quality Initiatives
Global Health Cluster Partner Meeting 17-19 June 2015
Geneva, Switzerland
Marie T Benner, Malteser International

Warehouse in a Box
Pilot Test in refugee setting in Thailand to control medicine stock outs and expiry:
• Increase awareness for the role of inventory management
• Reduce time spent on administrative tasks
• Increase visibility in consumption patterns and inventory status resulting into better forecasting
• Ensure better decision making through availability of information at various levels of the organization
• Equipment: tablet, solar charger and wirless barcode

COMBI=Communication for behaviour change impact
The COMBI method is a strategic and targeted communication approach based on concepts from marketing and includes different Behaviour Change Communication (BCC) theories/models.
•“The way how we make decisions buying a bottle of water, the same way people make decisions regarding
i.e. health issues”

COMBI Process
Connectdness and listening to the community is most important; think of the ‚competitor‘.
State the behavior to be changed (behavior change objective) – using 4W‘s and SMART
4 W’s: Who, What, Where, When, ….and, by the way, Why?
MANTRA 1: do nothing….(no pamphlets, no shirts or caps, no videos…until one has set up a precise specific behavioral Objective.

NYU/WHO IMC/COMBI - Doc #4 –Page 3 of 4
HICDARM : Needs and Goals Priority Market Segmentation
H I
C
D
A R
M
Have yet to Hear about family
planning
Have heard but now need to
be Informed
Now need to be
Convinced
Need to be encouraged to
Maintain their
family
planning behaviour
Need to be prompted to Act
Need to be triggered or
encouraged to
Decide to do
something about
family planning
Have acted and now
need to have action
Re-
confirmed

54

Afghanistan © Medair/Paul Hageman
Quality Initiatives GHC
June 2015

Country Program Sphere Audits
• Measures individual program and country level compliance against relevant, measurable Sphere indicators
• Quarterly
• Able to demonstrate improvement and areas where additional work is required over time


Country and Global QPI

Exit Criteria/Thresholds
services
services

Ebola Dashboard
• Utilized partnership with private sector to develop dashboard to follow the ebola outbreak
• Data currently limited to public data and Medair facility and quarantine data
• Final product soon to be completed

Technical quality and standards session:
What is my agency doing?
Global Health Cluster Partner Meeting 17-19 June 2015
Geneva, Switzerland
Francesco Checchi, Save the Children

What is Save the Children doing?
Assessment Macro (population-level) Micro (facility-level)
Decision-making Which beneficiaries? Which package of services? What delivery modalities?
Implementation Staff and job descriptions Work planning Training and supervision Audit Pharma. management
Project design Logframe MEAL + indicators/targets Programmatic budget
Tech
nic
al s
taff
re
cru
itm
ent a
nd
re
ten
tio
n
Staf
f ca
pac
ity
bu
ild
ing
MEAL Health information system Specific MEAL activities
Mainstreaming vulnerabilities (HIV, gender, disability,
age)
Health system support practices
Integration with other sectors
Early recovery provisions

What is Save the Children doing?
Assessment Macro (population-level) Micro (facility-level)
Decision-making Which beneficiaries? Which package of services? What delivery modalities?
Implementation Staff and job descriptions Work planning Training and supervision Audit Pharma. management
Project design Logframe MEAL + indicators/targets Programmatic budget
Tech
nic
al s
taff
re
cru
itm
ent a
nd
re
ten
tio
n
Staf
f ca
pac
ity
bu
ild
ing
MEAL Health information system Specific MEAL activities
Mainstreaming vulnerabilities (HIV, gender, disability,
age)
Health system support practices
Integration with other sectors
Early recovery provisions

Technical staff recruitment and retention
• Expanded global humanitarian health advisory team – 10 generalist health advisers
– 11 specialists (1 HIV, 5 RH, 1 neonatal, 1 epidemics / vaccination, 1 health policy, 3 HMIS-MEAL)
– 10 roving advisers
– 8 pharmacists
– 3 cluster support staff
• Five times larger than 2012
– Delay between investment and effect

What is Save the Children doing?
Assessment Macro (population-level) Micro (facility-level)
Decision-making Which beneficiaries? Which package of services? What delivery modalities?
Implementation Staff and job descriptions Work planning Training and supervision Audit Pharma. management
Project design Logframe MEAL + indicators/targets Programmatic budget
Tech
nic
al s
taff
re
cru
itm
ent a
nd
re
ten
tio
n
Staf
f ca
pac
ity
bu
ild
ing
MEAL Health information system Specific MEAL activities
Mainstreaming vulnerabilities (HIV, gender, disability,
age)
Health system support practices
Integration with other sectors
Early recovery provisions

Staff capacity building
• Distance-learning modules for HIV in emergencies – HIV in emergency preparedness
– PMTCT in emergencies
– Mainstreaming HIV vulnerabilities
• DL and face to face modules for family planning and post-abortion care in emergencies
• Extensive CMAM and IYCF toolkits – Inspiration for health & HIV
• 6-month Humanitarian Health & Nutrition Diploma

About the Diplomas
2-week Residential
5-month Distance Learning + Mentoring
Closed book exam +
Critical Report
3-week Residential
5-month Distance Learning + Mentoring
Field placements
Closed book exam +
Critical Report
OVERALL AIM: Equip national humanitarian health and nutrition staff in key regions with
the required skills, knowledge and experience to a) organise and deliver, and b) design and lead field health and nutrition interventions in emergencies
a) Professional Diploma
in ‘Humanitarian Health
& Nutrition for
Practitioners’
b) Professional Diploma
in ‘Humanitarian Health &
Nutrition for
Managers’

Modules * Humanitarian Context
* (Rapid) Assessment & Surveillance
* Key Health & Nutrition Interventions
* Programme Cycle Management
* Emergency Health/Nutrition Operations
accreditation
Both Diplomas are accredited as Professional Diplomas by Liverpool School
of Tropical Medicine.
This partnership with LSTM means:
Quality Assurance
Professionalisation
Certification
“It motivated me to work harder in order to excel”
“It is an internationally recognised Diploma attesting to the high level
of the training” [Participant from 3rd cohort]

Gender
Female
Male
Specialisms Health
Nutrition
Health &Nutrition
HIV
68 participants
based in 14 countries in East Africa and West
and Central Africa.
Outputs

57% said they had been
engaged in a
humanitarian response
since starting the Diplomas
15% have been promoted 6 months later...
68% said their
responsibilities
had increased
after receiving the
Diploma
“Before the training I was
a Nutrition Officer, I am
now Health & Nutrition
Coordinator. Colleagues
and managers
acknowledge this new
integrated dimension of
my work. I now feel
entirely legitimate.” Graduate from Mali
“I am now
regularly consulted
for advice on
humanitarian
issues”
“I really developed my capacity and
confidence to lead an emergency
response. I gained important hands-on
skills that I was able to utilise (…) in
the Puntland Cyclone” Graduate from Somalia

What is Save the Children doing?
Assessment Macro (population-level) Micro (facility-level)
Decision-making Which beneficiaries? Which package of services? What delivery modalities?
Implementation Staff and job descriptions Work planning Training and supervision Audit Pharma. management
Project design Logframe MEAL + indicators/targets Programmatic budget
Tech
nic
al s
taff
re
cru
itm
ent a
nd
re
ten
tio
n
Staf
f ca
pac
ity
bu
ild
ing
MEAL Health information system Specific MEAL activities
Mainstreaming vulnerabilities (HIV, gender, disability,
age)
Health system support practices
Integration with other sectors
Early recovery provisions

Assessment and decision-making
• Reviewing emergency health assessment tools
• Developing consolidated assessment tool to be used at macro and micro levels
• Guidance for decision-making (late 2015?)

What is Save the Children doing?
Assessment Macro (population-level) Micro (facility-level)
Decision-making Which beneficiaries? Which package of services? What delivery modalities?
Implementation Staff and job descriptions Work planning Training and supervision Audit Pharma. management
Project design Logframe MEAL + indicators/targets Programmatic budget
Tech
nic
al s
taff
re
cru
itm
ent a
nd
re
ten
tio
n
Staf
f ca
pac
ity
bu
ild
ing
MEAL Health information system Specific MEAL activities
Mainstreaming vulnerabilities (HIV, gender, disability,
age)
Health system support practices
Integration with other sectors
Early recovery provisions

Project design and implementation
• Establishing various pharmaceutical management systems – Quality procurement
– Gifts in kind
– Supply chain and ordering
– Field-level forecasting and drug management
• Specific guidance on thematic priorities – Newborn health in emergencies guide
– FP/PAC guidance and toolkits
– PMTCT in emergencies
• Medical risk management project
• COMPASS project

Project design and implementation
COMPASS
• Complete Operational Modules of Public health Activities and Standardised Systems
• Software application pre-loaded with evidence / best practices / tools
• Designed to streamline work of field health managers
• Conduit for evidence and best practices

Project design and implementation
COMPASS
COMPASS Tips for implementation
Tips for inter-sector integration, vulnerability mainstreaming
Menu of indicators, how to interpret them
Training and supervision materials and schedule
Audit tools, protocols and schedule
HR lists and job descriptions
Programmatic budget
Drug lists and quantification
Operational library
Specify which services ~15-25 other input parameters

What is Save the Children doing?
Assessment Macro (population-level) Micro (facility-level)
Decision-making Which beneficiaries? Which package of services? What delivery modalities?
Implementation Staff and job descriptions Work planning Training and supervision Audit Pharma. management
Project design Logframe MEAL + indicators/targets Programmatic budget
Tech
nic
al s
taff
re
cru
itm
ent a
nd
re
ten
tio
n
Staf
f ca
pac
ity
bu
ild
ing
MEAL Health information system Specific MEAL activities
Mainstreaming vulnerabilities (HIV, gender, disability,
age)
Health system support practices
Integration with other sectors
Early recovery provisions

MEAL
• Health Management Information System roll-out
• Defined indicators by module (service)
• DHIS-2
• 2 pilot countries this year
• Expanding to 60 countries by 2018

What is Save the Children doing?
Assessment Macro (population-level) Micro (facility-level)
Decision-making Which beneficiaries? Which package of services? What delivery modalities?
Implementation Staff and job descriptions Work planning Training and supervision Audit Pharma. management
Project design Logframe MEAL + indicators/targets Programmatic budget
Tech
nic
al s
taff
re
cru
itm
ent a
nd
re
ten
tio
n
Staf
f ca
pac
ity
bu
ild
ing
MEAL Health information system Specific MEAL activities
Mainstreaming vulnerabilities (HIV, gender, disability,
age)
Health system support practices
Integration with other sectors
Early recovery provisions

Cross-cutting issues
• Mainstreaming and integration tip sheets
• Reviewing evidence to write practical “how to” guidance on best practice for health system support in emergencies
– Health financing / user fee removal
– Human resources for health
– District health team support package
THANK YOU!
Francesco Checchi

PUBLIC HEALTH IN REFUGEE
EMERGENCIES
GHC Partner Meeting
19th June 2015

On June 20, the world commemorates the strength, courage, and resilience of millions of refugees.
English student. Brother. Footballer. “I am alive thanks to my sister.”

UNHCR Global Public Health Strategy
83
Public Health
HIV & Reproductive Health
Food Security
Nutrition
WASH
2014 - 2018

How to reach results:
• Integrate services into national systems whenever feasible
• Robust contingency planning and emergency response that focuses on integration and sustainability of services
• Reinforce partnerships specifically with government line ministries
• Create synergies with other sectors from onset
• Develop and implement standard operating procedures for public health areas

How to reach results:
• Use data from TWINE, SENS and WMS systems to make evidence-based decision
• Promote and use innovative and appropriate technologies for diagnosis, treatment and monitoring
• Capitalise on health financing opportunities to address needs
• Increase HCR and partner expertise

Refugee camps
• Primary health care programs
• Aim for integration/synergies with national programs
• Referral for 2̊ and 3̊ care
• Capacity building
• Health information systems easier
Urban & Out of Camp
• Alternative to camps, including PHC and Referral care
• Legal / protection access to services
• HI schemes where feasible
• Challenges to monitor health status and health access

Monitoring tools refugee camps
Refugee camps
• HIS
• Disease outbreaks
• WMS
• Nutrition Survey
• Balanced score card
• Laboratory evaluation
• Referral care
• Maternal death review
• Neonatal death review

Monitoring tools out of camp
• HIS ONLY where there are vertical clinics outside MOH,
(some countries disaggregation by nationality)
• HAUS
• Nutrition survey (either included in national or separate)
• Balanced score card
• Referral care

Regular order

What to improve
• Integration with MOH – legal status/dilemma
• Too often establishment of vertical systems in
refugee camps, rather than working towards integration from emergency phase onwards.
• UNHCR limited accepted role in supporting MoH on quality improvement and health systems strengthening.
• Media hype emergencies versus no media emergencies
• Donor and funding fatigue (protracted nature of refugee operations)
• Challenges to find quality partners in protracted situations
• Beneficiaries not fully involved
• Empowering communities


Technical Quality and Standards UNICEF 2015

Content
1
2
3
UNICEF Core Commitments for Children in Humanitarian Emergencies (CCC)
Humanitarian Performance Monitoring
Capacity Building

UNICEF
UNICEF’s core humanitarian
policy to uphold the rights of
children affected by humanitarian
crisis
Promote predictable, effective
and timely collective
humanitarian action
A framework based on norms and
standards, around which UNICEF
seeks to engage with partners
What are the CCCs?

UNICEF 95
CCCs: Core Commitments for Children
Strategic Result
Commitments – the first
commitment in each sector
refers to coordination or
cluster lead (when relevant)
aligning UNICEF’s
commitments in humanitarian
reform with the CCCs.
Benchmarks – aligned with
globally accepted standards
including SPHERE and INEE
Content: Hierarchy of Results

UNICEF 96
CCCs: Core Commitments for Children
Content: Technical Justification and
Programme Actions
Technical Justification
Programme Actions: UNICEF has identified key
preparedness,
response and early recovery
actions to contribute to each sectoral
commitment, based on evidence
available and best practice,
recognizing that partners will employ
diverse strategies to work towards
global benchmarks for children in
humanitarian action.

UNICEF 97
CCCs: Core Commitments for Children
Content: Operational Commitments
Operational commitments now also
include defined
preparedness and
response actions
Some operational commitments also
include early recovery actions

Humanitarian Performance Monitoring
1. Does response have adequate resources? e.g. tracking % funding by sector, % staffing filled, % supplies from allocation to delivery
Informs management of HQ-RO support to CO
2. Are we making progress/ enough progress? e.g. tracking children <5 with SAM enrolled in TFPs
• # and estimated coverage as % of target
• by UNICEF / by Cluster
Decisions to allocate more resources -- advocacy, $, human
Humanitarian Performance Monitoring
3. Is the quality of the response as expected? e.g. % sites visited where issues identified related to – use of supplies; services functioning; equity of access….
Feedback to specific site/partners; changes to strategy
4. Are we meeting Cluster Lead Agency accountabilities?
e.g. tracking key milestones--TORs, IM systems, strategy, technical standards
Increase in management resources, advocacy

• Few key progamme indicators
• Few key operations indicators
• Cluster milestones
VISION – Supply, Human Resources & Funding Data
SitRep
High frequency coverage estimates -- partner reporting
• 2-3 key programme indicators per sector
Cluster coordination milestone
monitoring
• UNICEF CLA accountabilities
Field monitoring to check quality
• Implementation
bottlenecks • Equity
• Do no harm • Engagement local
capacities
Key Components of Humanitarian Performance Monitoring
SitRep feeds into CO management
team review
Monitoring of Results for Equity System (MoRES) adapted in Emergencies
Level 1 Needs assessment draws on prior Situation Analysis, and re-assesses same key determinants: • enabling environment; services and support; access and use
of services
Level 2 High frequency internal SitReps cover monitoring of availability and use of key UNICEF resources (narrative report and VISION management reports on resources for selected IRs)
Level 3 In major emergencies (e.g. Appeals > $15 million), country offices prioritize/redirect resources to scale up monitoring • Monitoring aligns to new priority results in line with CCCs • Indicators and methods systematically include:
― Key output indicators for coverage estimates (supply) through partners
― Quality issues (access, use) through field monitoring ― Cluster process milestones (coordination) through self-
reporting • Monitoring feeds higher frequency management review

Monitoring of Results for Equity System (MoRES) adapted in High Emergency-Risk Contexts
Level 1 Emergency-risk informed analysis entails:
• Examining impact of emergency threats and likely humanitarian consequences on equity gaps;
• Which can lead to identification/prioritization of different key result areas; geographic focus; or bottlenecks;
• And to equity-focused programming with specific risk prevention/reduction/mitigation focus.
Level 2
Level 3 Choice of indicators and data collection methods influenced by potential use in monitoring humanitarian response
Level 4


CAPACITY BUILDING

Humanitarian Learning Strategy
• Three tiers: Junior, Mid – level and Senior Management;
• Four phases: Induction, Pre-deployment, During Employment and End of Deployment
• Seven topic areas: Security, Well-Being, Humanitarian Action, UNICEF in Humanitarian Action, Leadership and Management, Technical and Simulations/ Team Building;


Health in Emergencies training
• Train all health staff globally (development staff): move capacity to the country level – Basics of IASC systems and Health Cluster
– Operational/technical issues
– UNICEF procedures
• Resources: compilation of resources and tools
• Process – Review of existing training: start now
– Mixed methods, modules, hands on, mentoring

eLearning and Resources
• http://www.unicefinemergencies.com/
• Health Resources for Emergencies: http://www.unicefinemergencies.com/downloads/eresource/Health.html


Humanitarian Performance Monitoring


Assuring Quality in WVI Emergency Health Response
Operations
Global Health Cluster Partner Meeting 17-19 June 2015
Geneva, Switzerland
Dr Ando Tiana Raobelison

International Standards: Emergency and Humanitarian Accountability Framework
– Do No Harm
– Code of Conduct
– Sphere Standards in Health Action
– HAP
– Convention on the rights of children

Own Quality Standards : LEAP approach (Learning, Evaluation, Accountability and
Planning)
Joint Assessment/ Health
Cluster/Community Participation PRIORITY INTERVENTIONS
Health HIV Nutrition DADDs
(Do Don’t Assure) DELIVERY MECHANISMS
HEA Disaster Management Standards OPERATIONAL ROLES

Own Quality Standards (ctd)
Pharmaceutical Management Policy Drug procurement
Orientation/Mentoring/Coaching Staff Capacity Building
Feedback from the
beneficiaries/Updates to the
community
Inform decision-making, Ensure Mutual
Accountability

Real-time Learning Evaluation process Improve current programming
Post –response Learning Event Inform future response
Operational Audit Measure quality of the Response
Own Quality Standards (ctd)