Embed Size (px)
Citation preview

TM
Taeosviotpaeo
ULTla
A
A
0d
echnical Tips for EVAR for Ruptured AAAanish Mehta, MD, MPH
Endovascular treatment of ruptured abdominal aortic aneurysms is associated with de-creased morbidity and mortality when compared to the open surgical approach, yet, thereare several fundamental obstacles to our ability to offer these endovascular techniques tomany patients with ruptured aneurysms. This article will focus on the technical aspects ofendovascular aneurysm repair for rupture aneurysms, with particular attention on devel-oping a standardized multidisciplinary approach that will address some practical issues,such as the need for preoperative computed tomography, choice of anesthesia, percuta-neous access versus surgical exposure of the femoral arteries, use of aortic occlusionballoons, bifurcated versus aorto-uniiliac stent grafts, adjunctive procedures, diagnosis andtreatment of abdominal compartment syndrome, and conversion to open surgical repair.Semin Vasc Surg 22:181-186 © 2009 Elsevier Inc. All rights reserved.
GAmvdmrn
decdsmdas
EATppo
HE EVOLUTION OF endovascular aneurysm repair(EVAR) has led to improvements in our ability to treat
bdominal aortic aneurysms (AAA) under elective as well asmergent circumstances.1-3 The implications of our ability toffer EVAR for patients presenting with aneurysm rupture areignificant because no other therapy has offered such a sur-ival advantage to these high-risk patients. When consider-ng these endovascular techniques for treating ruptured AAA,ne has to streamline patient care from the emergency roomo the operating room, which often requires a multidisci-linary approach. The focus of this article will be to establishcomprehensive and standardized technical approach for
ndovascular treatment of ruptured AAA that can maximizeur ability to offer this treatment to patients.
nderstanding theimitations of EVAR for Rupture
here are several reasons for our failure to adopt endovascu-ar technology as the “first-line therapy” for patients withneurysm rupture:
1. Availability of preoperative computed tomography(CT) in all patients with ruptured AAA.
2. Availability of dedicated operating room staff equippedto perform emergent EVAR at all times.
3. Availability of “off-the-shelf” stent grafts.
lbany Medical College, The Institute for Vascular Health and Disease, Al-bany, NY.
ddress reprint requests to Manish Mehta, The Vascular Group, PLLC, 43New Scotland Avenue MC157, Albany, NY 12208. E-mail: mehtam@
ualbanyvascular.com
895-7967/09/$-see front matter © 2009 Elsevier Inc. All rights reserved.oi:10.1053/j.semvascsurg.2009.07.010
4. Inadequate experience in managing unexpected endo-vascular issues during emergent repair.
etting Startedlthough one or more of the aforementioned limitationsight have some impact on the ability to incorporate endo-
ascular techniques for patients with ruptured AAA, the fun-amentals of success begin from establishing a standardizedultidisciplinary approach that is inclusive of emergency
oom physicians, anesthesiologists, operating room (OR)urses, technologists, and vascular surgeons.The operator should be comfortable performing EVAR un-
er elective circumstances; have an inventory of standardquipment (ie, wires, catheters, sheaths, angioplasty and oc-lusion balloons, and fluoroscopic equipment) and en-ografts to match the largest aortic neck diameter and thehortest aneurysm length with a variety of iliac extensions forost AAA anatomies; and be familiar with adjunctive proce-ures, such as iliac interventions to facilitate access, use of anortic occlusion balloon, and placement of large Palmaztents.
VAR for Ruptured AAA:Standardized Approach
reatment of ruptured AAA patients involves a multidisci-linary approach that facilitates a seamless transition of theatient from the emergency room to the OR. Success dependsn early diagnosis, obtaining an expeditious CT scan to eval-
ate the aortoiliac anatomy, and rapid transport from the181

el
AatsTetstOta
OBessflvtoftisp
FTrhadgeladodlpfloaa
afmvbpmtt
comp
182 M. Mehta
mergency room to the OR equipped to perform endovascu-ar as well as open surgical repairs.
In 2002, at the Vascular Institute for Health and Disease inlbany, we developed a standardized approach4 that has en-bled us to use and endovascular approach as the first line ofherapy for all patients who present with ruptured AAA, re-ulting in a significant improvements in patient survival (Fig 1).he protocol includes a heightened awareness among themergency room staff of diagnosis of a ruptured AAA andimely notification of the on-call vascular surgeon and the ORtaff. In the emergency room, hemodynamically stable pa-ients undergo expeditious CT scan and are transferred to theR. Hemodynamically unstable patients are moved directly
o the OR without a CT scan for endovascular-first approachnd conversion to open surgical repair, as needed.
R Setupecause not all patients with ruptured AAA can undergondovascular repair, all OR/hybrid endovascular OR suiteshould be set up to facilitate endovascular as well as openurgical repair. Depending on the size of the room and theuoroscopic equipment, which can be fixed or portable withiewing screens and power injectors, one has to customizehe layout of the suite so it is conducive for endovascular andpen surgical repair. We have found it best to set up the roomor endovascular repair with standard needles, wires, cathe-ers, and sheaths open on a sterile table, have the surgicalnstruments in the room if needed, situate the patient on aurgical table and, as the anesthesiology team prepares the
Figure 1 Albany Vascular Group standardized protocol final aortic aneurysm (r-AAA). BP, blood pressure; CTA,
atient, set up the fluoroscopic equipment and supplies. b
undamental Techniqueshe technique of “hypotensive hemostasis” by limiting theesuscitation to maintain a detectable blood pressure canelp minimize ongoing hemorrhage. The patient is preppednd draped in supine position and via a femoral artery cut-own ipsilateral access is obtained using a needle, floppyuide wire, and a guiding catheter. The floppy guide wire isxchanged for a super-stiff wire that can be used to place aarge sheath (12-14Fr � 45 cm) in the ipsilateral femoralrtery and the sheath is advanced to the juxtarenal aorta toeliver the aortic occlusion balloon, if needed. A compliantcclusion balloon should always be available in these proce-ures and, in hemodynamically unstable patients, the bal-
oon is advanced through the ipsilateral sheath over the su-er-stiff wire into the supraceliac abdominal aorta underuoroscopic guidance, and inflated. Access is subsequentlybtained from contralateral femoral artery in similar fashion,nd a marker flush-catheter is advanced to the juxtarenalorta for an aortogram.
The placement of the stent-graft main body is based on theortoiliac morphology. In hemodynamically stable patients,ollowing the initial aortogram, the occlusion balloon is re-oved from the ipsilateral side and the main body is ad-
anced under fluoroscopic guidance, which limits the num-er of catheter exchanges. In hemodynamically unstableatients, the flush-catheter is exchanged for the stent-graftain body, which is delivered to the renal arteries. An aor-
ogram is done via the occlusion balloon sheath, the top ofhe main body is aligned with the lowermost renal artery, the
ovascular aneurysm repair (EVAR) of ruptured abdom-uted tomographic angiography; ER, emergency room.
or end
alloon is deflated and withdrawn back with the delivery

sTTc
PTatCcepT�Ttagt
sefUc“a�Ocwt
CDrtcctta2aapchafipbama
dcsjcastmti
ATntpp
lblOasfq
vetpJssatcssn
(m
Technical tips for EVAR for ruptured AAA 183
heath into the aneurysm sac, and the main body is deployed.he remainder of the procedure is performed routinely.here are several important technical aspects that merit dis-ussion.
reoperative CT Scanhe hemodynamic status of the ruptured AAA patient gener-lly dictates the need for a preoperative CT scan and, al-hough for an emergent open surgical repair a preoperativeT may not be necessary, for an emergent EVAR a CT scanan be vital for evaluating the feasibility of EVAR as well as forndograft sizing. Lloyd et al examined the time to death inatients with ruptured AAA who did not undergo treatment.5
heir findings indicated that 88% (49 of 56) of patients died2 hours after admission with diagnosis of ruptured AAA.he median time from the onset of symptoms to admission to
he hospital was 2.5 hours, and the interval between hospitaldmission and death was 10.5 hours. This data would sug-est that the majority of patients with ruptured AAA haveime to undergo a CT scan.
We evaluated CT scans of 50 consecutive patients that pre-ented with ruptured AAA and had a preoperative CT scan. Thendovascular anatomical inclusion criteria was slightly modifiedrom the standard “Indications for Use” defined by each of theS Food and Drug Administration�approved devices and fo-used on the feasibility of EVAR for ruptured AAA. Theserevised” criteria included aortic neck length �10 mm,ortic neck diameter �32 mm, aortic neck angulation75 degrees, and bilateral iliac artery diameter �5 mm.ur findings indicated that 80% of ruptured AAA patients
ould be considered anatomically suitable for EVAR. Thisas comparable to our experience to date of endovascular
reatment of over 100 ruptured AAA patients.
hoice of Anesthesia and Approachepending on operator experience and logistics, EVAR for
upture can be performed under local anesthesia via percu-aneous approach or general anesthesia and femoral arteryut-down. The potential benefits of local anesthesia and per-utaneous approach is that it might avoid the loss of sympa-hetic tone in the hypotensive patients.6 The percutaneousechniques have several limitations because currently avail-ble stent grafts are delivered through large sheaths (18-4Fr), and one has to be familiar with gaining percutaneousccess and using closure devices in patients with weak orbsent femoral pulses. In hemodynamically stable patients,articularly in the hands of experienced operators, these per-utaneous procedures are quite feasible. In our practice, weave routinely performed EVAR for rupture under generalnesthesia with femoral artery cut-down. We have found thatemoral cut-down can be accomplished within minutes andn most instances this approach was easier than obtaining aercutaneous access. However, in hemodynamically unsta-le patients, when the induction of general anesthetic can bessociated with further hemodynamic collapse, we recom-end and have routinely used the percutaneous approach to
ccess the initial femoral artery. In these instances our stan- l
ard approach is to access the initial femoral artery via per-utaneous approach, exchange the floppy guide wire for auper-stiff wire, advance a 12-14Fr (45 cm) sheath into theuxtarenal aorta, and advance the aortic occlusion balloonatheter through the sheath to the level of the supraceliacorta. The aortic occlusion balloon is inflated as needed. Sub-equently, the patient undergoes general anesthesia and con-ralateral femoral artery cutdown is performed, and the re-ainder of the procedure initiated. Following completion of
he procedure, the site of percutaneous femoral artery accesss primarily repaired via femoral cutdown.
ortic Occlusion Balloonhe appropriate use of aortic occlusion balloons in hemody-amically unstable patients is vital to the success of EVAR inhese emergent circumstances. Our preferred method forlacing aortic occlusion balloons is to use the femoral ap-roach, and we have found this to have several advantages:
1. It allows anesthesia to have access to both upper ex-tremities for arterial and venous access;
2. Patients who require an occlusion balloon are hypoten-sive and percutaneous brachial access can be difficultand more time-consuming than femoral cut-down;
3. Currently available occlusion balloons require at least a12Fr sheath, which require a brachial artery cut-down;and
4. Stiff wires and catheters across the aortic arch withoutprior imaging might lead to arterial injuries and/or in-creased risk of embolic stroke.
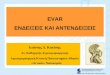
To stabilize the inflated balloon catheter at the suprarenalevel, the sheath should be advanced into the aortic neckecause this will prevent downward displacement and pro-
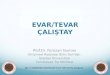
apse of the occlusion balloon into the aneurysm sac (Fig 2).ccasionally, the sheath may not be able to fully engage the
ortic neck because of the presence of significant aortoiliactenosis, calcifications, or tortuosity. This requires a forwardorce to be applied on the balloon catheter to maintain ade-uate position in the suprarenal aorta (Fig 3).If inflation of the aortic balloon is required to maintain a
iable blood pressure, the procedure should be conductedxpeditiously to limit the time of aortic occlusion and reducehe risk hemorrhagic complications, such as abdominal com-artment syndrome (ACS) and multisystem organ failure.ust prior to deployment of the main body, the aortic occlu-ion balloon should be deflated and withdrawn from theuprarenal level to avoid trapping the balloon between theortic neck and the stent graft. This temporary deflation ofhe aortic occlusion balloon rarely results in hemodynamicollapse. In hemodynamically unstable patients, the occlu-ion balloon can be redirected into the aortic neck from theide ipsilateral to the main body and reinflated at the infrare-al aortic neck within the main body.Currently, there are three compliant occlusion balloons
Table 1). Occlusion balloons are constructed of compliantaterials, such as polyurethane, latex, or silicone, and have
ow burst pressures of �5 atmospheres. Their primary func-

tgro
BAAstuttapfictaRcastf
pses
Fbda
Ftt
184 M. Mehta
ion is to mold the stent graft to the surrounding aorta withentle inflation and provide aortic occlusion during EVAR foruptured AAA, and should be in the armamentarium of allperators treating AAA.
ifurcated versusorto-Uniiliac Stents Graftslthough the decision to use a particular stent-graft type andize is determined by the anatomy, there are several factorshat influence our decision to use a bifurcated versus aorto-niiliac device, and they include inability to access the con-ralateral gate expeditiously and inability to access the con-ralateral iliac artery due to significant occlusive diseasend/or tortuosity. When using bifurcated stent grafts, even inatients who are hemodynamically stable, there is potentialor ongoing bleeding until adequate proximal and distal sealsn the aortic neck and iliac arteries are obtained. If the gateannot be cannulated rapidly, particularly in unstable pa-ients, the bifurcated stent graft should be converted to anorto-uniiliac configuration by using devices such as theenu device (Cook, Inc., Bloomington, IN) or placing aorticuffs or a second main body across the flow divider to divertll blood flow to the ipsilateral iliac limb. This does requireubsequent interruption of retrograde flow from the con-ralateral iliac artery into the AAA using an occluder and aemoral�femoral bypass.
In our experience of �100 EVARs for ruptured AAA, ap-roximately 15% require emergent conversion of bifurcatedtent grafts into aorto-uniiliac devices. To facilitate contralat-ral gate cannulation during EVAR, we routinely cross the
igure 2 The sheath supporting the aortic occlusion balloon shoulde advanced and supported fully into the aortic neck to preventownward displacement and prolapse into the abdominal aorticneurysm.
tent-graft limbs to align them with the contralateral sheath.b
igure 3 Inability to fully engage the sheath into the aortic neck dueo the presence of significant aortoiliac stenosis, calcifications, orortuosity might result in downward displacement of the inflated
alloon (A-C).
Wp
ABptotatpcLwdtncaapm
ATmahmcwa
AddacovtcAtSprb
switimlmt
CRncttcnoswnptn
CEtEioatphtspslap
R1
T
RCE
Technical tips for EVAR for ruptured AAA 185
ith this approach, gate cannulation can be usually accom-lished within 1 to 2 minutes.
djunctive Proceduresecause of the obvious emergent nature of ruptured AAA,reoperative planning can be less than ideal, and can lead tohe need for unexpected adjunctive procedures. Discussionf all adjunctive procedures that might be needed is beyondhe scope of this article; however, use of Palmaz stents at theortic neck for treatment of type I endoleaks is a techniquehat one should be familiar with.7 Briefly, our standard ap-roach includes a Palmaz P4910 stent hand-crimped andentered onto a 20- to 25-mm angioplasty balloon (eg, Maxi-D, Cordis Endovascular, Miami, FL); the ends of the balloonith the stent are slightly inflated to avoid “watermelon seed”isplacement of the Palmaz stent during deployment. A 16-o 18Fr introducer sheath is advanced into the straight andontortuous main body of the stent graft and the balloonatheter with the Palmaz stent is delivered to the juxtarenalorta and deployed partially in the stent graft and the nativeortic neck. The angioplasty balloon is exchanged for a com-liant aortic occlusion balloon and the Palmaz stent isolded to anchor the stent graft to the aortic wall.
ssessing for ACShe pathophysiology of ACS8 after EVAR for ruptured AAA isultifactorial, ie, the retroperitoneal hematoma, which acts
s a space-occupying lesion contributing to intraabdominalypertension; ongoing bleeding from lumbar and inferioresenteric arteries from the disrupted aneurysm sac due to
oagulopathy; and the shock associated with ruptured AAA,hich can induce alterations in microvascular permeability
nd lead to visceral and soft-tissue edema.Most published data would suggest that the incidence of
CS for ruptured AAA varies and is dependent on the hemo-ynamic status of the patient. In our own series, the inci-ence of ACS was 18%, and several variables were identifieds contributing factors. These included use of an aortic oc-lusion balloon, need for massive blood transfusions (meanf 8 U packed red blood cells), and coagulopathy with ele-ated activated partial thromboplastin time at completion ofhe case. Patients that developed ACS had a significantly in-reased mortality (67%) when compared to those withoutCS (10%). As a result of these observations, our protocol for
he endovascular treatment of ruptured AAA has evolved.ystemic anticoagulation, which was used earlier in our ex-erience, is avoided and coagulopathy is aggressively cor-ected during the perioperative period to limit any ongoing
able 1 Properties of Compliant Aortic Occlusion Balloons
Occlusion Balloon Sheath Siz
eliant (Medtronic, Santa Rosa, CA) 12oda (Cook, Bloomington, IN) 14qualizer (Boston Scientific, Natick, MA) 14-16
leeding from collateral vessels. Furthermore, bladder pres-
ures are recorded on an hourly basis during the procedure asell as in the postoperative period. If bladder pressures are
ncreased, regardless of the presence of other associated fac-ors, we proceed to a decompressive laparotomy. However,n practice, regardless of bladder pressures, if a patient has
ore than one risk factor for developing ACS, immediateaparotomy is performed. It is our opinion that taking these
easures might decrease the associated morbidity and mor-ality of ACS.
onversion to Open Surgical Repairegardless of all the improvements in endovascular tech-iques there are times when open surgical repair is needed. Aomprehensive discussion of open surgical repair is beyondhe scope of this article, but a few key points deserve men-ion. When surgical conversion is needed, use of aortic oc-lusion balloon can be valuable in maintaining hemody-amic stability. It is crucial to maintain the position of thecclusion balloon and its introducer sheath, and failure to doo might result in the balloon prolapsing into the aneurysm,ith loss of proximal occlusion. If open surgical conversion iseeded subsequent to stent-graft deployment, the exact ap-roach should be tailored to the type of stent graft, ie, theype of proximal and distal fixation and presence of suprare-al versus infrarenal stents or barbs.
onclusionndovascular repair of ruptured AAA is evolving and offers
he potential for improved patient survival. During emergentVAR, the time for preoperative planning is limited and often
maging is less than ideal. Under these circumstances, oneften has to get creative and utilize more of a problem-solvingpproach to address challenging issues. A standardized mul-idisciplinary approach can be instrumental in organizingathways that can accommodate individual practices andospital infrastructure, and facilitate a seamless transition ofhese hemodynamically unstable patients from diagnosis touccessful EVAR. There are several important technical as-ects that include the choice of anesthesia, percutaneous ver-us femoral cut-down approach, use of aortic occlusion bal-oons, use of bifurcated versus aorto-uniiliac stent grafts, anddjunctive procedures that need to be understood as oneerforms these procedures.
eferences. Ohki T, Veith FJ: Endovascular grafts and other image guided catheter
based adjuncts to improve the treatment of ruptured aortoiliac aneu-
Catheter Length (cm)Maximum Balloon
Diameter (mm)
100 46100-120 32, 4065, 110 20, 27, 33, 40
e (Fr)
rysms. Ann Surg 232:466-479, 2000

2
3
4
5
6
7
8
186 M. Mehta
. Veith FJ, Ohki T, Lipsitz EC, Suggs WD, Cynamon J: Endovascular graftsand other catheter-directed techniques in the management of rupturedabdominal aortic aneurysms. Semin Vasc Surg 16:326-331, 2003
. Dgorova N, Giacovelli J, Greco G, Gelijns A, Kent CK, McKinsey JF:National outcomes of treatment of ruptured AAA: comparison of openversus endovascular repair. J Vasc Surg 48:1092-1100, 2008
. Mehta M, Taggert J, Darling RC III, et al: Establishing a protocol forendovascular treatment of ruptured abdominal aortic aneurysms: out-comes of a prospective analysis. J Vasc Surg 44:1-8, 2006
. Lloyd GM, Bown MJ, Norwood MG, et al: Feasibility of preoperative
computed tomography in patients with ruptured AAA: A time todeath study in patients without operation. J Vasc Surg 39:788-791,2004
. Starnes BW, Andersen CA, Ronsivalle JA, Stockmaster NR, Mullenix PS,Statler JD: Totally percutaneous aortic aneurysm repair: experience andprudence. J Vasc Surg 43:270-276, 2006
. Kim JK, Noll RE Jr, Tonnessen BH, Sternbergh WC 3rd: A technique forincreased accuracy in the placement of the “giant” Palmaz stent for treat-ment of type 1A endoleak after EVAR. J Vasc Surg 48:755-757, 2008
. Mehta M, Darling RC III, Roddy SP, et al: Factors associated with abdominalcompartment syndrome complicating endovascular repair of ruptured ab-
dominal aortic aneurysms. J Vasc Surg 42:6:1047-1051, 2005