Embed Size (px)
Citation preview
See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/26661735
Telerehabilitation: Enabling the remote delivery of healthcare, rehabilitation,
and self management
Article in Studies in Health Technology and Informatics · February 2009
DOI: 10.3233/978-1-60750-018-6-231 · Source: PubMed
CITATIONS
163READS
5,938
3 authors, including:
Some of the authors of this publication are also working on these related projects:
Self Management View project
Smart2 View project
Sue Mawson
The University of Sheffield
65 PUBLICATIONS 948 CITATIONS
SEE PROFILE
Simon Brownsell
Durham University
55 PUBLICATIONS 1,302 CITATIONS
SEE PROFILE
All content following this page was uploaded by Sue Mawson on 02 January 2014.
The user has requested enhancement of the downloaded file.
Telerehabilitation: Enabling the Remote Delivery of Healthcare, Rehabilitation, and
Self Management
David M. BRENNANa,1, Sue MAWSONb and Simon BROWNSELLc aNational Rehabilitation Hospital, Washington DC, USA
bCentre for Health and Social Care Research, Sheffield Hallam University, UK cSchool of Health and Related Research, University of Sheffield, UK
Abstract. Telerehabilitation refers to the use of Information and Communication Technologies (ICT) to provide rehabilitation services to people remotely in their homes or other environments. By using ICT, client access to care can be improved and the reach of clinicians can extend beyond the physical walls of a traditional healthcare facility, thus expanding continuity of care to persons with disabling conditions. The concept of telecare, when telerehabilitation is used to deliver services to clients in their homes or other living environments, empowers and enables individuals to take control of the management of their medical needs and interventions by enabling personalized care, choice and personal control. A wide variety of assessment and treatment interventions can be delivered to clients using remote monitoring systems, robotic and virtual reality technologies, and synchronized collaboration with online material. This chapter will present a brief history of telerehabilitation and telecare and offer an overview of the technology used to provide remote rehabilitation services. Emphasis will be given to the importance of human factors and user-centered design in the planning, development, and implementation of telerehabilitation systems and programs. The issue of self-care in rehabilitation and self-management will be discussed along with the rationale for how telerehabilitation can be used to promote client self-care and self-management. Two case studies of real-world telerehabilitation systems will be given, with a focus on how they were planned and implemented so as to maximize their potential benefits. The chapter will close with a discussion of obstacles and challenges facing telerehabilitation and suggestions for ways to promote its growth in use and acceptance.
Keywords. telerehabilitation, telemedicine, telecare, self-care, self management
Introduction
Technology has revolutionized all aspects of medical rehabilitation. The use of robotics, virtual reality, nanotechnologies, embedded sensors, neuro-imaging, and a host of other technologies have enhanced health outcomes and allowed researchers to break new ground and expand their knowledge of the processes of neurological and musculoskeletal recovery. As this research knowledge and technology development is
1 Corresponding Author: National Rehabilitation Hospital, Center for Applied Biomechanics and
Rehabilitation Research, 102 Irving Street, NW, Washington, DC, 20010, USA; E-mail: [email protected].
Support us – Ask your institution/library/department to order our books or to apply for series
membership - ISSN 1566-7677
To order a book contact by fax or
by e-mail the offices below:
IOS Press, Inc. 4502 Rachael Manor drive Fairfax, VA 22032 U.S.A. Tel.: +1 703 323 5600 Fax: +1 703 323 3668 [email protected] IOS Press Nieuwe Hemweg 6B 1013 BG Amsterdam The Netherlands Tel: +31 20 688 3355 Fax: +31 20 620 3419 [email protected] IOS Press, c/o Ohmsha, Ltd. 3-1 Kanda Nishiki-cho Chiyoda-ku Tokyo 101 Japan Fax: +81 3 3233 2426 (Books only) IOS Press/ Gazelle Book Services Ltd White Cross Mills Hightown Lancaster LA1 4XS United Kingdom Tel.: +44 1524 68765 Fax: +44 1524 63232 [email protected]
Advanced Technology in Rehabilitation Empowering Cognitive, Physical, Social and Communicative Skills through Virtual Reality, Robots, Wearable Systems and Brain-Computer Interfaces Volume 145 Studies in Health Technology and Informatics Edited by: Gaggioli, A., Keshner, E.A., Weiss, P.L., Riva, G. June 2009, approx. 310 pp., hardcover ISBN: 978-1-60750-018-6 NEW Price: US$167 / €115 / £81 Enacting Intersubjectivity A Cognitive and Social Perspective on the Study of Interactions Volume 10 Emerging Communication: Studies on New Technologies and Practices in Communication Edited by: F. Morganti, A. Carassa and G. Riva May 2008, approx. 280 pp., hardcover ISBN: 978-1-58603-850-2 NEW Price: US$161 / €115 / £81 From Communication to Presence Cognition, Emotions and Culture towards the Ultimate Communicative Experience Festschrift in honor of Luigi Anolli Volume 9 Emerging Communication: Studies on New Technologies and Practices in Communication Edited by: G. Riva, M.T. Anguera, B.K. Wiederhold, F. Mantovani September 2006, 323 pp., hardcover ISBN: 978-1-58603-662-1 Price: US$161 / €115 / £81 Global Data Management Volume 8 Emerging Communication: Studies on New Technologies and Practices in Communication Edited by: R. Baldoni, G. Cortese, F. Davide and A. Melpignano July 2006, 376 pp., hardcover ISBN: 1-58603-629-7 Price: US$161 / €115 / £81 The Hidden Structure of Interaction From Neurons to Culture Patterns Volume 7 Emerging Communication: Studies on New Technologies and Practices in Communication Edited by: L. Anolli, G. Riva, S. Duncan Jr. and M.S. Magnusson May 2005, 304 pp., hardcover ISBN: 1-58603-509-6 Price: US$161 / €115 / £81 Ambient Intelligence The Evolution of Technology, Communication and Cognition Towards the Future of Human-Computer Interaction Volume 6 Emerging Communication: Studies on New Technologies and Practices in Communication Edited by: G. Riva, F. Vatalaro, F. Davide and M. Alcañiz January 2005, 316 pp., hardcover ISBN: 1-58603-490-1 Price: US$161 / €115 / £81 Being There Concepts, Effects and Measurements of User Presence in Synthetic Environments Volume 5 Emerging Communication: Studies on New Technologies and Practices in Communication Edited by: G. Riva, F. Davide and W.A. IJsselsteijn 2003, 344 pp., hardcover ISBN: 1-58603-301-8 Price: US$161 / €115 / £81 Say not to Say: New Perspectives on Miscommunication Volume 3 Emerging Communication: Studies on New Technologies and Practices in Communication Edited by: L. Anolli, R. Ciceri and G. Riva 2001, 288 pp., hardcover ISBN: 1-58603-215-1 Price: US$161 / €115 / £81 Towards CyberPsychology Mind, Cognition and Society in the Internet Age Volume 2 Emerging Communication: Studies on New Technologies and Practices in Communication Edited by: G. Riva and C. Galimberti 2001, 326 pp., hardcover ISBN: 1-58603-197-x Price: US$161 / €115 / £81 Communications Through Virtual Technologies Identity, Community and Technology in the Communication Age Volume 1 Emerging Communication: Studies on New Technologies and Practices in Communication Edited by: G. Riva and F. Davide 2001, 292 pp., hardcover ISBN: 1-58603-162-7 Price: US$161 / €115 / £81

translated to practice, those with disabilities have access to an ever-expanding range of cutting-edge treatments.
However, it is not only the interventions themselves that benefit from advanced technologies, but also the way in which the interventions are delivered. Physical distance between a client and a clinic is no longer an insurmountable obstacle to care. Information and Communication Technologies (ICT) can be used to extend the reach of clinicians far beyond the physical walls of a healthcare facility to local clinics, community health care facilities, or in some cases, directly to clients in their homes. Beyond basic videoconferencing, a wide variety of assessment and treatment interventions can be delivered to clients using remote monitoring systems, inertial sensors, robotic and haptic devices, and synchronized collaboration with online material.
Using ICT to deliver rehabilitation services improves access to care for people who live in rural locales (or in areas without specialty-trained clinicians) and for clients with mobility impairments who have difficulty travelling. It can also substantially reduce practitioner travel time and therefore increase the number of client consultations possible in a day. Finally, the use of ICT in delivering rehabilitation services can greatly expand continuity of care to persons with disabling conditions and enable them to take control of the management of their medical needs and therapy interventions by promoting personalized care, choice, and personal autonomy.
Having stated the opportunities that ICT affords in rehabilitation, it is worth providing a brief introduction to the related terminology. For the purposes of this chapter, telemedicine is used, in a broad sense, to refer to the transfer or exchange of medical and healthcare information using ICT. Telerehabilitation refers specifically to the delivery of rehabilitation services via telemedicine methods and techniques. Telecare refers to the specific instances where health or care services are provided to people in their homes or other supervised living settings [1, 2]. It is hoped the reader will appreciate it is not so much the specific definition of each term that is essential, but rather the concepts behind the terms. The reader is also encouraged to keep in mind that no matter what term is used, telerehabilitation and its related applications are not new clinical disciplines or specialties, rather they represent a new way to deliver treatment to the client and improve access to care, while perhaps offering opportunities to enhance the rehabilitation process.
This chapter will present a brief history of telerehabilitation and telecare and discuss how they fit within the broad scope of telemedicine. It will offer an overview of the technology used to provide remote rehabilitation services as well as discuss the importance of human factors and user-centered design in the planning, development, and implementation of telerehabilitation systems and programs. The importance of self-care in rehabilitation will be discussed along with the rationale for how telecare can be used to promote client self-care. Two case studies of real-world telerehabilitation will be given, with a focus on how they were planned and implemented so as to maximize their potential benefits. The chapter will close with a discussion of obstacles and challenges facing telerehabilitation and suggestions of ways to promote its growth.
1. Origins of Telemedicine
Some have suggested that telemedicine can trace its origins to the use of bonfires and smoke signals, carrier pigeons, and horseback-riding letter carriers to transfer

information related to disease outbreaks, military casualty lists, and requests for medical assistance [1]. These instances are obviously dwarfed by the scope and speed of modern telemedicine applications, yet they demonstrate the rationale and potential for health data to be transmitted from one location to another.
The formal history of telemedicine is directly tied to advancements in technology. The original "no-tech" methods, described above, were gradually replaced, first by the telephone and telegraph, and later by radio-transmission, closed-circuit television signals, and satellite communication. The mid- to late-1990's brought about what some consider to be the 'modern' era of telemedicine with the advent of digital communications, growth of electronic medical records, and rapid proliferation of the Internet – all of which continue to be significant driving forces for telemedicine [1, 2]. Figure 1 offers an approximate timeline illustrating when various ICT was first used for transmitting medical information.
Today, telemedicine has grown to include a broad research knowledge base, a mounting body of evidence on efficacy and effectiveness, and a rising level of acceptance among clinicians and clients [1]. Radiology, pathology, and other primarily image-driven diagnostic specialties have strongly embraced telemedicine as a way to deliver services faster, more efficiently, more accurately (for example, when advanced image processing techniques or algorithms are applied), and to a greater number of people [3]. Videoconferencing consults from larger specialty clinics to rural healthcare providers are becoming increasingly commonplace around the globe, extending the reach of clinicians and improving client care [2]. Advancements in ICT coupled with the rapid development of software, sensors, robotics, digital medical records, and other equipment have helped telemedicine develop into a key component in the evolution of modern healthcare.
2. Origins of Telerehabilitation
Much as the earliest examples of telemedicine were opportunistic and often driven by innovative clinicians making use of equipment that existed for another purpose [2], telerehabilitation sprang from the application of existing telemedicine tools and
Figure 1. Timeline of ICT Telemedicine Utilization

techniques to individual rehabilitation disciplines. From the first demonstration projects, the motivation for telerehabilitation has been a desire to improve the delivery of rehabilitation services, enhance the continuum of care, and promote client involvement and participation in treatment. These are essential components of the long-term dynamic process of rehabilitation and are directly related to the functional outcomes and level of recovery a client can achieve.
Early telerehabilitation efforts were structured mostly as pilot projects that were small in sample size and proof-of-concept in nature, yet they demonstrated that some rehabilitation assessment and treatment techniques could be delivered to clients located in physically separate locations, thus overcoming obstacles of distance and lack of access to trained providers. In some of the first telerehabilitation projects, clinicians used the telephone to provide client follow-up and caregiver support, and to administer client self-assessment measures [4, 5]. By the late 1980's, this approach expanded to include the use of closed-circuit television and pre-recorded video material to provide visual interaction with clients [6, 7].
As ICT advanced, telerehabilitation applications expanded in scope. Projects began to employ live interactive videoconferencing, with an emphasis on rehabilitation interventions that relied mostly on audio-visual interaction (e.g. neuropsychology, speech-language pathology, counseling, etc.) and for which a lack of physical contact presented less of a barrier to treatment. In cases where a higher-speed connection was available, clinicians were able to use high-quality video transmission to provide consultations, diagnostic assessments, delivery of treatment interventions, and distance learning and supervision via telerehabilitation [8, 12]. Other projects made use of slower analog public switched telephone network (PSTN) connections that were more limited in the speed of the videoconferencing they could provide. Yet despite lower-quality video transmission, telerehabilitation was shown to be a feasible method for delivering a range of rehabilitation treatment and assessment interventions [13, 17].
These projects pointed to the potential benefits of telerehabilitation with results demonstrating efficacy and yielding high levels of client and clinician satisfaction. Feasibility of telerehabilitation was shown not only in controlled laboratory or clinic settings, but also across long distances, bringing therapy and assessment to remote and rural populations.
The recent development of advanced sensor and remote monitoring technologies has enabled an increasing number of telerehabilitation applications to be deployed into the home. While early telecare projects looked to provide basic follow-up services and caregiver support [18, 19], more recent work has developed and deployed systems to provide home-based exercise monitoring, diet and medication compliance tracking, robotic-based treatment, and other more dynamic interventions [20, 23].
3. Technology
All telemedicine applications, while unique in their purpose, involve the exchange of medical or healthcare information. The people involved in the session (e.g. clinician-to-clinician in a tele-consultation, or clinician-to-client in a treatment encounter), the type of information collected, and the ways in which it is transmitted and displayed, varies significantly according to the intervention being delivered. Figure 2 illustrates the typical information exchange in telemedicine. In a live session, the information transmission occurs in real-time, while in store-and-forward telemedicine information
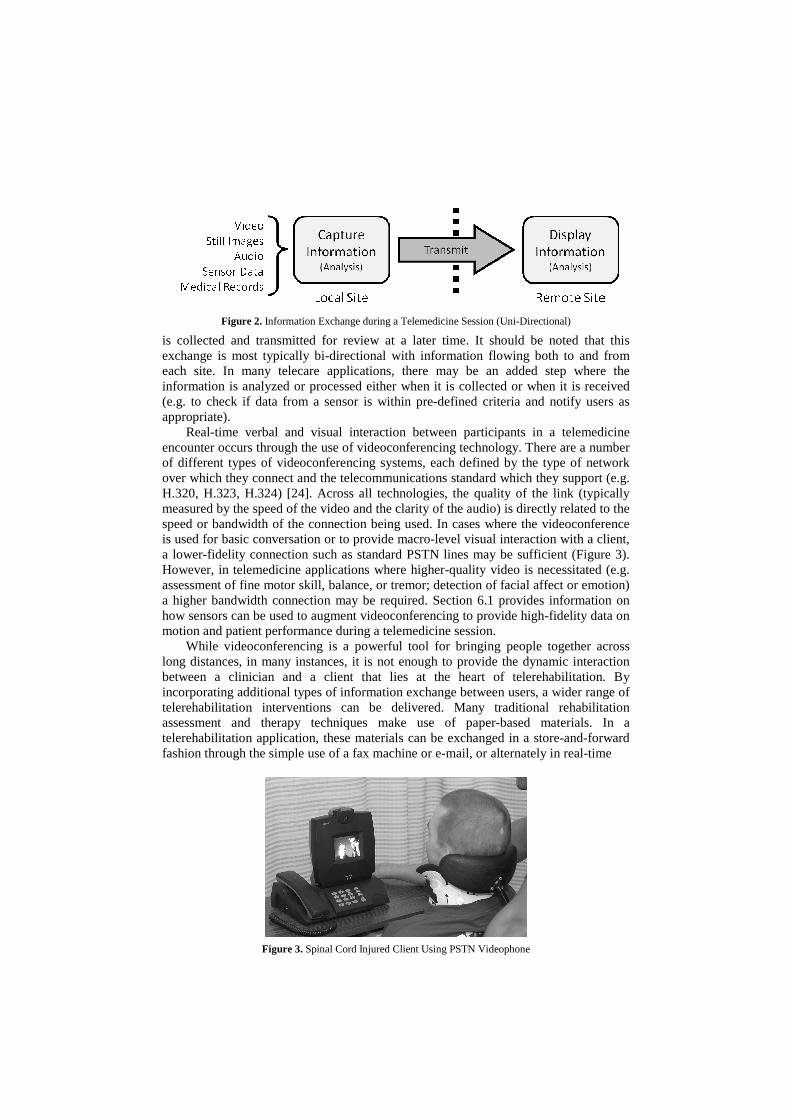
Figure 2. Information Exchange during a Telemedicine Session (Uni-Directional)
is collected and transmitted for review at a later time. It should be noted that this exchange is most typically bi-directional with information flowing both to and from each site. In many telecare applications, there may be an added step where the information is analyzed or processed either when it is collected or when it is received (e.g. to check if data from a sensor is within pre-defined criteria and notify users as appropriate).
Real-time verbal and visual interaction between participants in a telemedicine encounter occurs through the use of videoconferencing technology. There are a number of different types of videoconferencing systems, each defined by the type of network over which they connect and the telecommunications standard which they support (e.g. H.320, H.323, H.324) [24]. Across all technologies, the quality of the link (typically measured by the speed of the video and the clarity of the audio) is directly related to the speed or bandwidth of the connection being used. In cases where the videoconference is used for basic conversation or to provide macro-level visual interaction with a client, a lower-fidelity connection such as standard PSTN lines may be sufficient (Figure 3). However, in telemedicine applications where higher-quality video is necessitated (e.g. assessment of fine motor skill, balance, or tremor; detection of facial affect or emotion) a higher bandwidth connection may be required. Section 6.1 provides information on how sensors can be used to augment videoconferencing to provide high-fidelity data on motion and patient performance during a telemedicine session.
While videoconferencing is a powerful tool for bringing people together across long distances, in many instances, it is not enough to provide the dynamic interaction between a clinician and a client that lies at the heart of telerehabilitation. By incorporating additional types of information exchange between users, a wider range of telerehabilitation interventions can be delivered. Many traditional rehabilitation assessment and therapy techniques make use of paper-based materials. In a telerehabilitation application, these materials can be exchanged in a store-and-forward fashion through the simple use of a fax machine or e-mail, or alternately in real-time
Figure 3. Spinal Cord Injured Client Using PSTN Videophone
via computer-based data sharing methods where on-screen material can be used interactively by participants (as illustrated by the interactive telerehabilitation system described in Section 6.2).
Today, an increasing number of projects are moving beyond basic videoconferencing to include the types of remote ‘hands-on’ interaction that was once viewed as being impossible for telerehabilitation. Multi-axial position and force sensors (the latest of which are small in size with wireless communication and low-power requirements) provide a tangible measure of physical performance and function of a remote client. Haptic and robotic technologies let therapists ‘feel’ a client and impart forces and motion. Environmental sensors, and other ‘Smart Home’ equipment, monitor a living space and collect information on a client’s interaction with the environment. The data from these devices can be used as part of a remote monitoring application and transmitted in real-time (with or without a simultaneous videoconference) or be collected, processed, and analyzed using store-and-forward methods.
Despite the ever-evolving potential that advanced technologies afford clinicians and researchers, it is imperative that the presence of technology has no negative impact on the interaction between clinician and client. Telerehabilitation technologies must be developed and implemented such that they facilitate the treatment interventions being delivered and are usable and accepted by both the clients (and their caregivers) who will receive the services and the clinicians who will provide them.
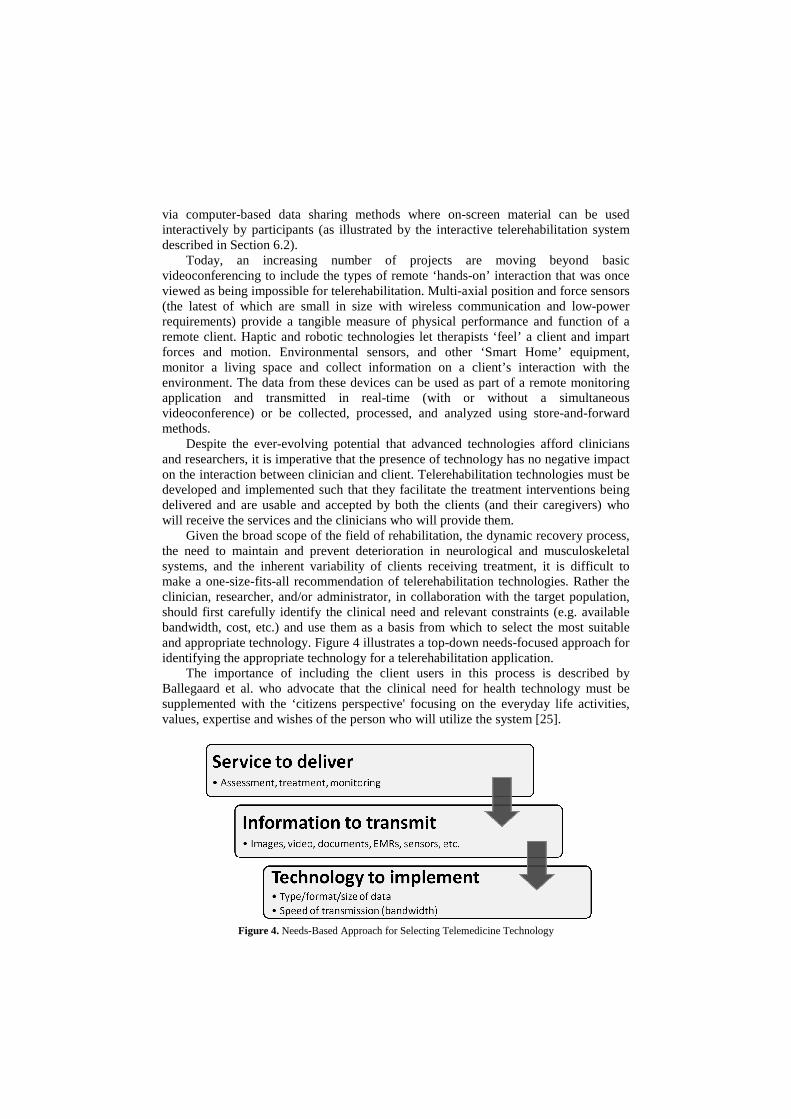
Given the broad scope of the field of rehabilitation, the dynamic recovery process, the need to maintain and prevent deterioration in neurological and musculoskeletal systems, and the inherent variability of clients receiving treatment, it is difficult to make a one-size-fits-all recommendation of telerehabilitation technologies. Rather the clinician, researcher, and/or administrator, in collaboration with the target population, should first carefully identify the clinical need and relevant constraints (e.g. available bandwidth, cost, etc.) and use them as a basis from which to select the most suitable and appropriate technology. Figure 4 illustrates a top-down needs-focused approach for identifying the appropriate technology for a telerehabilitation application.
The importance of including the client users in this process is described by Ballegaard et al. who advocate that the clinical need for health technology must be supplemented with the ‘citizens perspective' focusing on the everyday life activities, values, expertise and wishes of the person who will utilize the system [25].
Figure 4. Needs-Based Approach for Selecting Telemedicine Technology

4. Human Factors and User-Centered Design in Telerehabilitation
Technology plays a vital role in telerehabilitation as it is responsible for all aspects of the transfer of medical information. Yet as important as technology is, in order for telerehabilitation to ultimately be successful and move forward, it must remain focused on the users. This emphasis on user-centered design (UCD) is important at all phases of telerehabilitation planning, development, and implementation. Through careful involvement and consideration of users, technology designers can produce systems that are more user-friendly and less error-prone; researchers can collect more targeted and appropriate outcomes on satisfaction, effectiveness, and cost efficiency; and administrators can improve staff comfort levels and adoption of telerehabilitation procedures. The UK Department of Health has suggested that, “systematically and rigorously finding out what people want and need from their services is a fundamental duty of both the commissioners and the providers of services. It is particularly important to reach out to those whose needs are greatest but whose voices are often least heard” [26, p. 157].
In telemedicine applications, the list of users is quite broad and includes clients, clinicians, support staff, caregivers, and administrators. In considering the users of a telerehabilitation system, one must look beyond the factors of age, education, and technology experiences and account for possible impairments in cognitive, gross and fine motor function, and visual and language skills [27]. These additional considerations should be reflected in the telerehabilitation service delivery (e.g. accessibility of treatment space, training materials, consent documentation; disability-specific training for staff) as well as in the technology that is utilized (e.g. high usability, accessible controls).
Mainstream designers have become increasingly aware of the need for UCD, as can be evidenced by the recent trends in commercial products towards design emphasizing usability, ergonomics and aesthetics. While there are a number of existing methods and tools for UCD that can be used, it has been argued that new paradigms such as a ‘user-sensitive inclusive design’ should be used by developers of health care devices [28]. The purpose is to gain an understanding of the users’ experience of not only the technology to be designed but also the social and cultural context in which users live with their disability and in which they will engage with the technology [29, 31].
In the advancing world of telecare and telerehabilitation, the need to utilize such design techniques is paramount. Given the unique nature of the telerehabilitation population and the requirement for clients and caregivers to often directly interact with the technology, all aspects of telerehabilitation devices and systems must emphasize ease of use, consistency, and reliability. This relates to physical input and control functions such as buttons, switches, and connection ports/jacks; the use and placement of sensors and other peripherals such as sensor arm bands, blood pressure cuffs, and cameras; and on-screen graphical user interfaces of videoconferencing systems, in-home telehealth messaging devices, and sensors and other monitoring equipment.
By involving users throughout each stage of the development process, there is a greater likelihood that the final product will meet its design goals, be completed on-time, have lower development costs, and be more usable for its target population [32, 33]. To work towards this goal, developers of telerehabilitation devices may wish to employ UCD techniques such as ‘story-boarding’ which involves conducting observational fieldwork, semi-structured interviews, and cultural probes, to develop
‘personas’ for each of the targeted users of a system. For example, in a telerehabilitation system for clients with stroke, the persona would identify physical and cognitive abilities, social environments, personal life goals and networking needs and then map that storyboard to a new or emerging technology. In this way the design is derived from both the clinical need and the future user’s needs. Other valuable UCD methods that can be used include iterative paper prototyping (a method of having users test early iterations of a GUI through low-fidelity mock-ups), video acting, and workshop dissemination processes.
Well-designed and developed devices are clearly essential for successful telerehabilitation. However, there are other human factors considerations that must also be taken into account, especially with regard to how the telerehabilitation system integrates into the existing organization and clinical or research environment. These considerations include such dimensions as stakeholder support and buy-in, user training, equipment maintenance, scheduling, and technical support.
5. The self management and self-care agenda
As telerehabilitation will likely be a key component in the evolution of healthcare, it is important to understand the scope and potential of telerehabilitation systems to meet as full a range as possible of user needs. One such avenue for future exploration, from both a service-delivery and research perspective, is client self-care, defined as the practices undertaken by individuals towards maintaining health and managing illness [34]. Home-based telecare programs have the potential to promote self-care in numerous ways. Sensor-based systems could monitor performance and provide clients with feedback on their progress or display to them pre-established therapy and educational content (delivered by computer screen), all without the direct real-time involvement of a therapist. Clients would perhaps feel empowered to take an active role in their own rehabilitation, conducting self-care whenever they feel appropriate. Self-care, therefore, provides both the opportunity to receive treatment at the time and place of the client’s choosing, and to achieve improved health outcomes through self-managed additional rehabilitation sessions. In recognition of the fact that self-care could promote long-term wellness and a reduction in future healthcare demand, the UK Department of Health has identified self-care as one of the key building blocks for future client-centered health service [35].
The concept of self-management is closely linked to that of self-care. However, there are some distinctions in relation to rehabilitation, with clear key elements of the self-management concept that dictate a more dynamic process with the users. The elements within the self-management paradigm are goal identification, information acquisition, problem solving, decision-making, and self reaction, which in rehabilitation terms, should result in changes in motor control and subsequent functional ability. The SMART case study (Section 6.1) demonstrates that it is possible to use ICT and sensor technology to enable the key elements of the self management process to take place, the ultimate goal being to promote self managed recovery of motor function following a stroke.
Arguably most of the attention to date on self-care has centered on the management of long-term conditions (LTC) such as Chronic Heart Failure, Chronic Obstructive Pulmonary Disease, and Congestive Heart Failure. While self-care is encouraged in many countries at the policy level (including the use of telecare

technologies), a recent Cochrane review involving 17 studies with a total of 7,442 participants reported that while self-care programs for LTCs led by lay leaders, "may lead to modest, short-term improvements in patients confidence to manage their condition and perceptions of their own health." The, "programmes did not improve quality of life, alter the number of times patients visited their doctor or reduce the amount of time spent in hospital" [36, p. 2].
While the clinical outcomes of self-care approaches are inconclusive at this point, such results should perhaps be interpreted in the light that currently the process and imputed relationship between self-care education skills and health service contact, the human factors, are poorly understood [37]. Indeed, a noticeable cultural shift from both clients and clinicians is likely to be necessary before the full extent of the effectiveness of self-care can be quantified. Historically, the ‘balance of power’ has been with the medical practitioners who would use their expertise and knowledge to respond reactively to a client. Self-care promises increased knowledge for clients which can be used to empower them to pro-actively care for themselves; moving the balance of power, and in some instances sharing the decision making, between client and clinician. Thus, a paradigm shift is required where service providers, rather than strictly providing medical interventions, create an environment where people feel supported in their self-care decision making.
Telecare can be a key tool in enabling such a cultural shift and realizing the proposed clinical benefits of self-care. It can allow the ‘balance of power’ to be facilitated in a more agreeable environment as clinicians have access to frequently entered data (gathered manually and automatically) from the home and can maintain ‘contact’ with clients, particularly those with significant needs. At the same time, the client is empowered to self-care and receive additional therapy sessions in the knowledge that the clinician is keeping a ‘watching brief’ on their progress. Therefore, the telerehabilitation system, by its very nature, encourages a sharing of responsibility and communication. The SMART case study (Section 6.1) demonstrates the feasibility of a system that fosters a supportive client environment such that self-care educational material and the self-management of the therapy sessions can be targeted directly to the client (either as a consequence of the system automatically observing changes in client-entered data, or from direct clinician involvement); thus improving the client’s knowledge base, ability to self-care, and therapy outcomes.
While such innovations are currently small in scale there is an appetite for such a paradigm shift in service. The European Commission Information Society and Media (2006) suggest that, "the way healthcare is presently delivered has to be deeply reformed… The situation is becoming unsustainable and will only worsen in the future as chronic diseases and the demographic change place additional strains on healthcare systems around Europe." They call for a, "new healthcare delivery model based on preventative and person-centred health systems. This new model can only be achieved through proper use of ICT, in combination with appropriate organizational changes and skills" [38, p. 11]. The ability to generate reliable evidence for service commissioners to make informed decisions will be important to deliver this paradigm shift.

6. Telerehabilitation Case Studies
Stroke is the largest cause of severe disability in the western world. It is estimated that over 900,000 people in the UK and close to 2.5 million people in the United States are living with moderate to severe impairments as a result of stroke, affecting their independence and quality of life [39, 40]. In response to this need, and faced with a growing prevalence of stroke and other chronic diseases, rehabilitation specialists are investigating innovative models of health care delivery using technologies to improve access to care and enable the self management of long-term conditions.
6.1. Self-management of rehabilitation: the SMART study
Evidence suggests that 30% to 60% of stroke survivors regain no functional use in the arm at 6 months post-stroke [41]. Targeted rehabilitation is known to promote re-organization of the central nervous system with the intensity and frequency of the training [42], as well as the level of the client’s active participation and engagement [43], shown to be crucial factors in the recovery process.
The SMART rehabilitation project, a collaborative initiative with partners from Sheffield Hallam University, University of Sheffield, University of Ulster, University of Essex, and University of Bath, aimed to explore the use of innovative technologies to promote the self-management of progressive, repetitive, functional task-specific activities to motivate stroke survivors to engage in the rehabilitation process. The project examined the scope, effectiveness and appropriateness of systems to support home-based rehabilitation for stroke survivors and their caregivers focusing on upper limb home-based rehabilitation.
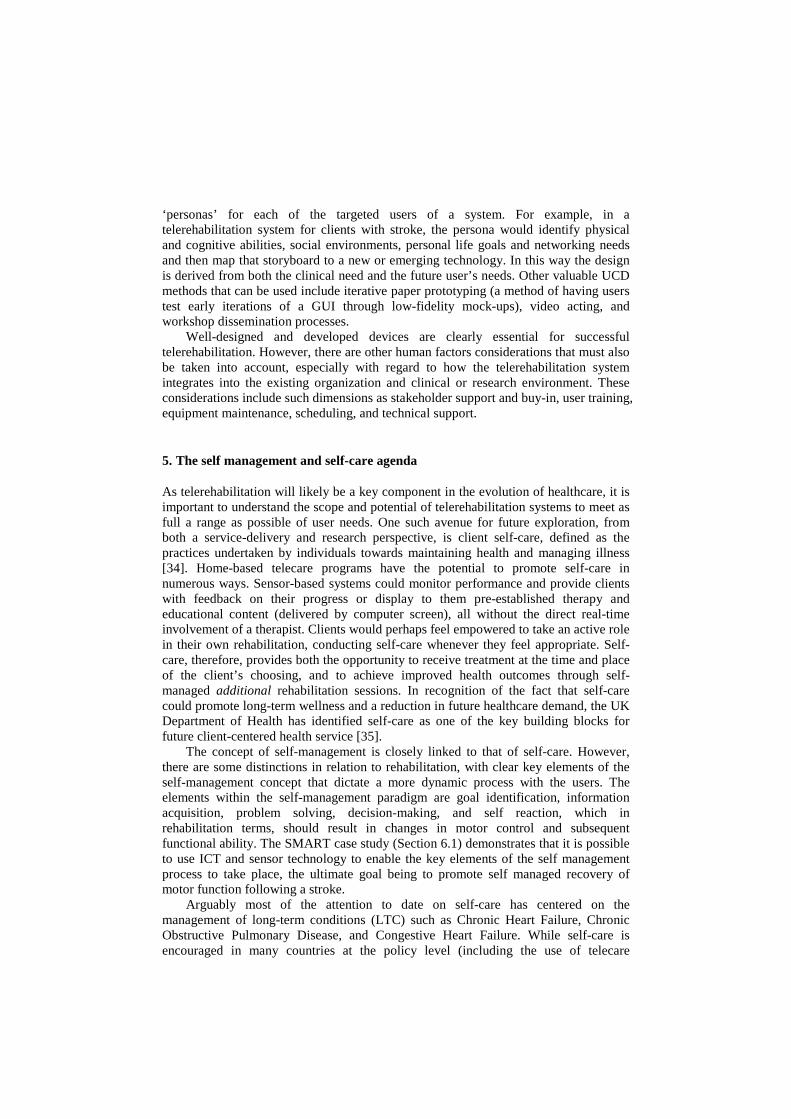
The SMART rehabilitation system (Figure 5) consists of three components: a movement tracking system (consisting of two small inertial sensors attached to the arm), a personal computer and a web-server unit [44, 20, 43]. The client attaches the sensors, selects a specific functional goal such as drinking or reaching, and repeats the task a number of times. The sensors record changes in the client's arm position resulting from movement of the elbow and shoulder joints. The information collected by the sensors is analyzed and provided as feedback to the client (and caregiver) in the form of on-screen 3D avatars showing the client's movement compared to the targeted "normal" movement. Summative kinematic data on frequency of use, angle ranges, and cycle time can also be viewed.
In this way the SMART system enables users to self-manage their rehabilitation by choosing which goal (exercise) to undertake, deciding when and how often to perform the task, observing and problem-solving their movements in comparison to a normal movement, and self-reacting by changing the way they move in response to feedback given [46, 47]. Clinicians can assess and monitor movements remotely via the Internet by accessing the central server, or provide comments/instructions over the web-based system when they have viewed the summative kinematic data.
Figure 5. Infrastructure of the SMART remote rehabilitation system.
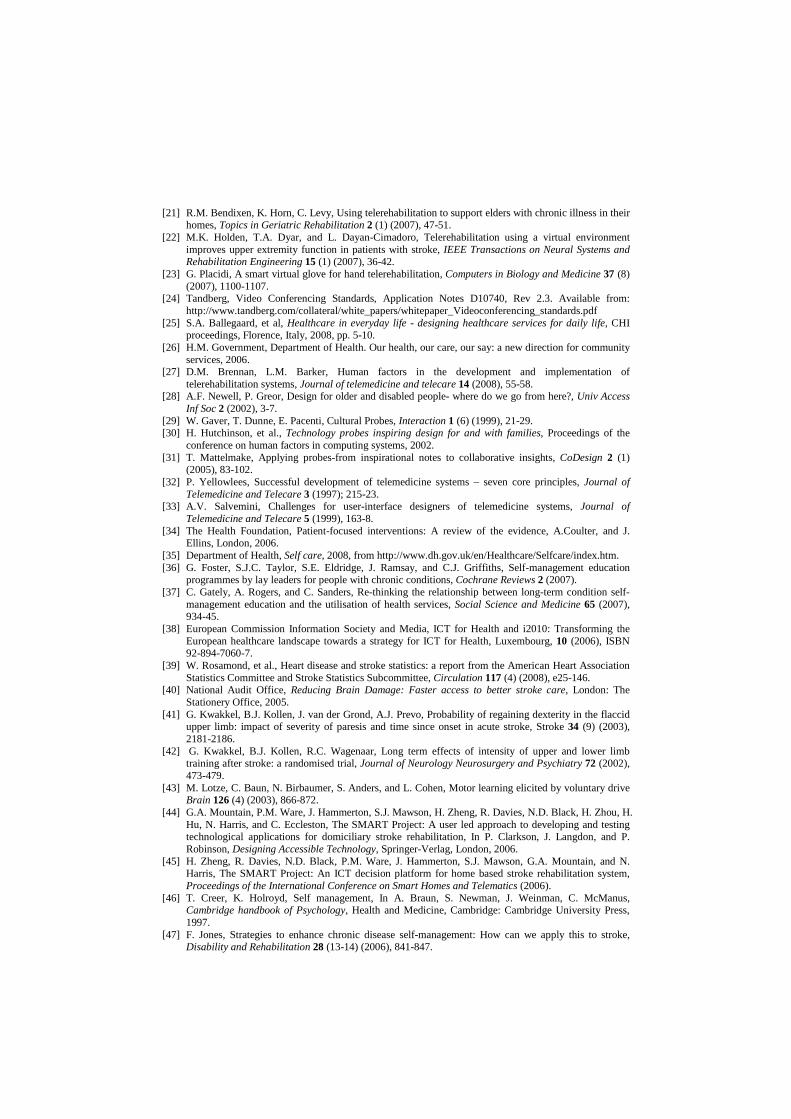
The project used an iterative UCD approach to develop a series of prototypes of the system’s user interface that were evaluated via task analysis, cognitive walkthroughs, and formal usability testing sessions. The final system was deployed and tested in the homes of four stroke survivors for two weeks as a proof of concept research study (Figure 6). Results indicated that the system could be effective at promoting functional improvement and encouraging compliance. Qualitative data provided anecdotal evidence of both the motivational aspects of the SMART system and the way it facilitated self-management of rehabilitation by enabling users to problem solve their movement strategies and self-react to the feedback provided. Figure 7 offers comments from two participants on their experience with the system.
Figure 6. Study Participant Using the SMART System at Home
"What I liked about it was that he was so eager to do it. He'd ask me 'shall I do it again? Shall I do it again?...It's really amazing that he really wanted to do these exercises much more..."
"Having viewed it visually I'm aware that this elbow swings out...people can see the difference between what they can do and what they should be doing"
Figure 7. Qualitative Feedback from Home Users of the SMART System

The results provided valuable guidance for further development of the system and proof of the concept that a robust rehabilitation system can be managed at home and used to provide useful and motivating feedback within the daily routine of a stroke survivor. Future projects will expand the SMART system and methodology to develop a personalized remote therapy system for chronic pain, stroke and chronic heart failure.
6.2. Interactive videoconferencing for remote cognitive-communicative treatment
Following stroke or brain injury, many clients often exhibit some degree of cognitive-communicative impairments. Treatment of these impairments by a speech-language pathologist (SLP) typically involves skill-based exercises that are largely based on drill-and-practice, repetition, and the use of treatment materials such as worksheets and flash cards. Given the highly verbal and visual nature of this treatment, it is well-suited for delivery using telerehabilitation technology [48]. While early work in the field pointed to the significant potential for telerehabilitation to deliver numerous cognitive-communicative interventions to remote clients [6, 9, 11, 12, 49], there was a clear need for technology that could enhance and expand the ways in which clinicians could interact with their remote clients.
Work at the National Rehabilitation Hospital, in Washington, DC, investigated use of a customized telerehabilitation system that combined videoconferencing with interactive data sharing features (Figure 8). The goal was to develop a system that could augment and extend interaction during a telerehabilitation session so as to enable a wide range of therapeutic interventions to be delivered to remote clients. In addition to the basic verbal and visual communication afforded by the videoconferencing connection, data collaboration functions were designed to serve as a ‘virtual desktop’ on which the client and clinician were able to work together in real-time using on-screen material (e.g. word processing documents, scanned worksheets, computer applications, or digital drawing whiteboards) just as they would use physical treatment materials in a traditional face-to-face session (Figure 9).
Development of the overall system was based on a UCD framework, which emphasized effective and usable interface design in addition to traditional software/system development goals of quality, budget, expandability, and timeliness. The design of the system GUIs were achieved through iterative prototyping that progressed from low-fidelity designs (e.g. drawings, sketches, and storyboards) to
Figure 8. Telerehabilation Interaction Incorporating Videoconferencing and Data Sharing

Figure 9. Videoconferencing Interaction with Barrier Drawing Task (NOTE: in this example, the client and the clinician share an on-screen drawing whiteboard, such that the clinician can view the client’s drawing via the touchscreen in real-time)
increasingly higher-fidelity functional models. The members of a cross-disciplinary project team worked in close collaboration with users (both stroke survivors and SLP clinicians) at all stages of the project through focus groups, brainstorming sessions, ad hoc task-centered cognitive walkthroughs, and formal usability testing sessions to ensure that the final design met the usability requirements of the target population.
Through a series of case studies, this system was evaluated as a method for delivering cognitive-communicative treatment to clients following stroke. Upon completion of a six-week treatment protocol, all clients achieved improvement in their functional communication at a level consistent with expectations for an equivalent period of traditional face-to-face treatment. In addition to a high level of overall client satisfaction, the data sharing features were found to be a highly valuable component of the system and were viewed favorably by both clients and clinicians as making treatment significantly more engaging and motivating [50, 51].
7. Obstacles, barriers and recommendations
Although telerehabilitation has been emerging for some time, it is still in its relative infancy. In order for telerehabilitation to achieve the long-term goal of improving health outcomes, empowering clients, and serving as a cost-effective mainstream tool for all, obstacles related to reliable evidence, technology, policy and reimbursement, organizational change, and workforce development and operational delivery must be addressed. Table 1 highlights each of these obstacles and offers recommendations as to how the telerehabilitation community - through the mutual efforts of researchers, clinicians, administrators, and policymakers - can overcome them for the benefit of client and clinician alike. For example, in order to address a lack of reliable evidence, well-designed studies with appropriate research methodologies must be conducted to evaluate both clinical and cost effectiveness of telerehabilitation programs as well as the impacts on client care delivery systems, training programs, and healthcare organizations.

Table 1. Obstacles to mainstream deployment of telerehabilitation and recommendations to overcome them
Obstacle Recommendations
Reliable evidence: While service innovators embrace change believing improvements will result, the majority of decision makers and service commissioners are typically more cautionary. Consequently requiring reliable evidence so as to compare costs and clinical outcomes of one service innovation against another before they will embrace the opportunity.
1. The academic community should produce reliable evidence, at a variety of different levels, to support service commissioners’ decision making for sustainable services. Particular attention should be given to clinical and cost effectiveness which compares against existing forms of service delivery.
2. Research funding bodies should review the potential benefits of telerehabilitation and make the appropriate levels of funding available to support sustainable research programs that deliver solutions over the short, medium and long-term.
3. While the risks of undertaking a new service innovation are often highlighted, the associated risks of rejecting opportunities and staying with the ‘status quo’ are rarely recognized. Consideration of these should therefore be highlighted.
Technology: Currently many hardware configurations work in isolation to one another, therefore requiring existing systems to be replaced when additional functionality is required. This can also limit the functionality of the ‘technology’ as an individual manufacturer may not have all of the ‘technology’ required to meet a specific users need.
Much of the technology is not as aesthetically pleasing as it might be. This can result in some users refusing or abandoning the technology as they consider it a badge of dependency. This issue is equally important in the growing consumer or self purchase market.
Finally the features of much of the technology are rather simplistic when compared to some other fields. Greater efforts are required for monitoring, analysis and data presentation.
1. Interoperable technology standards for communication, operation and interface should be developed to increase the flexibility of end-user solutions and facilitate easy user operation when utilizing the products from different manufacturers*.
2. Greater efforts should be made to understand why users reject or abandon ‘technology’ and efforts made to redesign equipment to maximize benefit for all – including the aesthetics of the technology.
3. In a research and development capacity greater collaboration between different disciplines should be encouraged due to the cross-organizational nature of solutions required. Collaboration and joint initiatives with industry should also ensure the minimum time delay between research demonstration and translation to available market product.
Policy and reimbursement: The supportive strength of national policy is variable throughout many different countries. As is the healthcare environment and the way in which services are funded. Even where policy is strong the funding is often unclear, sometimes resulting in greater financial benefits for those not contributing to the purchasing costs of such systems than those actually paying for it. As such, where direct benefit is not returned to the purchaser, there can be little motivation to invest at a micro level, even though the macro level benefits may be understood.
1. International comparison and collaboration at a policy level should be sought to share learning, evidence and encourage service innovation/technological developments by international companies*.
2. Holistic views of the financial costs and associated benefits are required. Alternatively understanding of the benefits throughout operational systems is required to share the costs and benefits accordingly.
Organizational change: Challenging cultural attitudes and the established ways in which organizations function is a considerable task that can take significant time. However, if the
1. Evidence should be presented, including consultation with end users, such that the requirement for change and the anticipated benefits can be described – in effect justifying the business case.

whole organization is not committed to the service redesign then the benefits are likely to be less than possible or anticipated.
2. The process of change should be project-managed accordingly with sufficient resource provided to enable the best possible chances of success.
3. Throughout the process, consultation and evaluation should be conducted to provide a feedback loop to reinforce the benefits and lessons learnt.
Workforce development and operational delivery: A variety of new skills may well be required on service delivery aspects, including the ‘balance of power’, technological aspects, equipment installation and maintenance, etc. Operational codes of practice, competencies and standards will also be required to ensure practitioners have the appropriate skills and abilities to offer services to a demonstrable level of performance.
1. Additional training courses are required to provide the necessary knowledge and competencies so the workforce can effectively deliver recognizable components of the overall system.
2. National occupational standards should be encouraged so clear career paths can be established.
3. Government organizations, trade associations and the voluntary sector should be encouraged to establish local, national, and possibly international, operational standards.
* Note: The efforts of the Continua Health Alliance [52], aimed at promoting interoperable personal telehealth solutions, are welcomed.
8. Conclusion
The need for evolving the delivery of rehabilitation services and incorporating aspects of self-care and remote monitoring is somewhat magnified in light of the shift in global demographics to an older population and the increasing prevalence of chronic health conditions. Telerehabilitation holds significant potential to meet this need and to provide services that are more accessible to more people, while having the ability to offer a more affordable enhanced level of care.
Despite all of its potential, the evolution of telerehabilitation is not inevitable and it will not occur on its own. Greater adoption of telerehabilitation will likely occur as a result of the shift towards user-focused and technology-enabled healthcare, and as an increased emphasis is placed on preventative and continuous care, rather than traditional episodic and reactive care. Additionally, there is a crucial need for a greater body of evidence on clinical effectiveness and cost efficiency of telerehabilitation programs. Research should look to analyze the behavior change that can and does occur as a result of telerehabilitation interventions and the impact it has on long-term health outcomes.
The last decade has seen tremendous growth of telerehabilitation, and this trend is likely to continue. While most of the past and current focus in telerehabilitation has been on modifying face-to-face treatment methods for remote delivery, future work will explore the potential for telerehabilitation to enhance and perhaps even improve care. While this growth occurs and new approaches for remote service delivery are explored, great care must be taken to ensure that the planning, design, and implementation of telerehabilitation technologies, systems, and services is strongly focused on user-centered human factors principles. Telerehabilitation must never be a result of 'technology push' alone, rather it must be driven by clinical need and a desire to improve healthcare.

Acknowledgments
The SMART Consortium (www.thesmartconsortium.org) is funded by the Engineering and Physical Sciences Research Council (www.fp.rdg.ac.uk/equal). Consortium members include Sheffield Hallam University, University of Sheffield, University of Bath, University of Essex and the University of Ulster.
References
[1] J. Craig, and V. Patterson, Introduction to the practice of telemedicine, In R. Wootton, J. Craig, and V. Patterson, Introduction to Telemedicine, Second Edition, London: The Royal Society of Medicine Press, Ltd, 2006, pp.3-14.
[2] A.C. Norris, Essentials of Telemedicine and Telecare, West Sussex: John Wiley and Sons, Ltd, 2002. [3] V. Della Mea, Prerecorded telemedicine, In R. Wootton, J. Craig, and V. Patterson, Introduction to
Telemedicine, Second Edition, London: The Royal Society of Medicine Press, Ltd, 2006, pp. 3-14. [4] G.R. Vaughn, Tel-communicology: health-care delivery system for persons with communicative
disorders, ASHA 18 (1) (1976), 13-17. [5] N. Korner-Bitensky, S. Wood-Dauphinee, Barthel Index information elicited over the telephone. Is it
reliable?, American Journal of Physical Medicine and Rehabilitation 74 (1) (1995), 9-18. [6] R. Wertz, N. Dronkers, E. Bernstein-Ellis, Y. Shubitowski, R. Elman, G. Shenaut, R. Knight, and J.
Deal, Appraisal and diagnosis of neurogenic communication disorders in remote settings, In R.H. Brookshire, Clinical Aphasiology, Minneapolis: BRK Publishers, 1987, pp. 117-123.
[7] R. Wertz, N. Dronkers, E. Bernstein-Ellis, L. Sterling, Y. Shubitowski, R. Elman, G. Shenaut, R. Knight, and J. Deal, Potential of telephonic and television technology for appraising and diagnosing neurogenic communication disorders in remote settings, Aphasiology 6 (2) (1992), 195-202.
[8] J.R. Duffy, G.W. Werven, and A.E. Aronson, Telemedicine and the diagnosis of speech and language disorders, Mayo Clinic Proceedings 72 (12) (1997), 1116-1122.
[9] A. McCullough, Viability and effectiveness of teletherapy for pre-school children with special needs, International Journal of Language & Communication Disorders 36 (1) (2001), 321-326.
[10] L. Savard, A. Borstad, J. Tkachuck, D. Lauderdale, and B. Conroy, Telerehabilitation consultations for clients with neurologic diagnoses: cases from rural Minnesota and American Samoa, NeuroRehabilitation 18 (2) (2003), 93-102.
[11] D. Theodoros, T.G. Russell, A. Hill, L. Cahill, and K. Clark, Assessment of motor speech disorders online: a pilot study, Journal of Telemedicine & Telecare 9 (2) (2003), S66-68.
[12] D. Brennan, A. Georgeadis, C. Baron, L. Barker, The effect of videoconference-based telerehab on story retelling performance by brain injured subjects and its implications for remote speech-language therapy, Telemedicine Journal and e-Health 10 (2) (2004), 147-154.
[13] R.P. Hauber, M.L. Jones, A.J. Temkin, S. Vesmarovich, V.L. Phillips, Extending the Continuum of Care After Spinal Cord Injury Through Telerehabilitation, Topics in Spinal Cord Injury Rehabilitation 5 (3) (1999),11-20.
[14] N.C. Dreyer, K.A. Dreyer, D.K. Shaw, and P.P. Wittman, Efficacy of telemedicine in occupational therapy: a pilot study, Journal of Allied Health 30 (1) (2001), 39-42.
[15] E.D. Lemaire, Y. Boudrias, and G. Greene, Low-bandwidth, Internet-based videoconferencing for physical rehabilitation consultations, Journal of Telemedicine and Telecare 7 (2) (2001), 82-89.
[16] P.G. Clark, S.J. Dawson, C. Scheideman-Miller, and M.I. Post, Telerehab: Stroke teletherapy and management using two-way interactive video, Neurology Report 26 (2002), 87-93.
[17] T.G. Russell, P. Buttrum, R. Wootton, and G.A. Jull, Low-bandwidth telerehabilitation for patients who have undergone total knee replacement: preliminary results, Journal of Telemedicine & Telecare 9 (2) (2003), S44-47.
[18] V.L. Phillips, S. Vesmarovich, R. Hauber, E. Wiggers, A. Egner, Telehealth: reaching out to newly injured spinal cord patients, Public Health Reports 116 (1) (2001), 94-102.
[19] B.Q. Tran, K.M. Buckley, and C.M. Prandoni, Selection & use of telehealth technology in support of homebound caregivers of stroke patients, CARING Magazine 21 (3) (2002), 16-21.
[20] H. Zheng, R.J. Davies, N.D. Black, Web-based monitoring system for home based rehabilitation with stroke patients, Proceedings of 18th IEEEE International Symposium on computer based medical systems 2005.
[21] R.M. Bendixen, K. Horn, C. Levy, Using telerehabilitation to support elders with chronic illness in their homes, Topics in Geriatric Rehabilitation 2 (1) (2007), 47-51.
[22] M.K. Holden, T.A. Dyar, and L. Dayan-Cimadoro, Telerehabilitation using a virtual environment improves upper extremity function in patients with stroke, IEEE Transactions on Neural Systems and Rehabilitation Engineering 15 (1) (2007), 36-42.
[23] G. Placidi, A smart virtual glove for hand telerehabilitation, Computers in Biology and Medicine 37 (8) (2007), 1100-1107.
[24] Tandberg, Video Conferencing Standards, Application Notes D10740, Rev 2.3. Available from: http://www.tandberg.com/collateral/white_papers/whitepaper_Videoconferencing_standards.pdf
[25] S.A. Ballegaard, et al, Healthcare in everyday life - designing healthcare services for daily life, CHI proceedings, Florence, Italy, 2008, pp. 5-10.
[26] H.M. Government, Department of Health. Our health, our care, our say: a new direction for community services, 2006.
[27] D.M. Brennan, L.M. Barker, Human factors in the development and implementation of telerehabilitation systems, Journal of telemedicine and telecare 14 (2008), 55-58.
[28] A.F. Newell, P. Greor, Design for older and disabled people- where do we go from here?, Univ Access Inf Soc 2 (2002), 3-7.
[29] W. Gaver, T. Dunne, E. Pacenti, Cultural Probes, Interaction 1 (6) (1999), 21-29. [30] H. Hutchinson, et al., Technology probes inspiring design for and with families, Proceedings of the
conference on human factors in computing systems, 2002. [31] T. Mattelmake, Applying probes-from inspirational notes to collaborative insights, CoDesign 2 (1)
(2005), 83-102. [32] P. Yellowlees, Successful development of telemedicine systems – seven core principles, Journal of
Telemedicine and Telecare 3 (1997); 215-23. [33] A.V. Salvemini, Challenges for user-interface designers of telemedicine systems, Journal of
Telemedicine and Telecare 5 (1999), 163-8. [34] The Health Foundation, Patient-focused interventions: A review of the evidence, A.Coulter, and J.
Ellins, London, 2006. [35] Department of Health, Self care, 2008, from http://www.dh.gov.uk/en/Healthcare/Selfcare/index.htm. [36] G. Foster, S.J.C. Taylor, S.E. Eldridge, J. Ramsay, and C.J. Griffiths, Self-management education
programmes by lay leaders for people with chronic conditions, Cochrane Reviews 2 (2007). [37] C. Gately, A. Rogers, and C. Sanders, Re-thinking the relationship between long-term condition self-
management education and the utilisation of health services, Social Science and Medicine 65 (2007), 934-45.
[38] European Commission Information Society and Media, ICT for Health and i2010: Transforming the European healthcare landscape towards a strategy for ICT for Health, Luxembourg, 10 (2006), ISBN 92-894-7060-7.
[39] W. Rosamond, et al., Heart disease and stroke statistics: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee, Circulation 117 (4) (2008), e25-146.
[40] National Audit Office, Reducing Brain Damage: Faster access to better stroke care, London: The Stationery Office, 2005.
[41] G. Kwakkel, B.J. Kollen, J. van der Grond, A.J. Prevo, Probability of regaining dexterity in the flaccid upper limb: impact of severity of paresis and time since onset in acute stroke, Stroke 34 (9) (2003), 2181-2186.
[42] G. Kwakkel, B.J. Kollen, R.C. Wagenaar, Long term effects of intensity of upper and lower limb training after stroke: a randomised trial, Journal of Neurology Neurosurgery and Psychiatry 72 (2002), 473-479.
[43] M. Lotze, C. Baun, N. Birbaumer, S. Anders, and L. Cohen, Motor learning elicited by voluntary drive Brain 126 (4) (2003), 866-872.
[44] G.A. Mountain, P.M. Ware, J. Hammerton, S.J. Mawson, H. Zheng, R. Davies, N.D. Black, H. Zhou, H. Hu, N. Harris, and C. Eccleston, The SMART Project: A user led approach to developing and testing technological applications for domiciliary stroke rehabilitation, In P. Clarkson, J. Langdon, and P. Robinson, Designing Accessible Technology, Springer-Verlag, London, 2006.
[45] H. Zheng, R. Davies, N.D. Black, P.M. Ware, J. Hammerton, S.J. Mawson, G.A. Mountain, and N. Harris, The SMART Project: An ICT decision platform for home based stroke rehabilitation system, Proceedings of the International Conference on Smart Homes and Telematics (2006).
[46] T. Creer, K. Holroyd, Self management, In A. Braun, S. Newman, J. Weinman, C. McManus, Cambridge handbook of Psychology, Health and Medicine, Cambridge: Cambridge University Press, 1997.
[47] F. Jones, Strategies to enhance chronic disease self-management: How can we apply this to stroke, Disability and Rehabilitation 28 (13-14) (2006), 841-847.

[48] D. Brennan, A. Georgeadis, C. Baron, Telerehabilitation tools for the provision of remote speech-language treatment, Topics in Stroke Rehabilitation 8 (4) (2002), 71-78.
[49] A. Georgeadis, D. Brennan, L. Barker, C. Baron, Telerehabilitation and its effect on story retelling by adults with neurogenic impairments, Aphasiology 18 (5/6/7) (2004), 639-652.
[50] D. Brennan, L. Barker, A model of client-clinician interaction for telemedicine in speech-language pathology, Telemedicine Journal and e-Health 11 (2) (2005), 218-219.
[51] D. Brennan, A. Georgeadis, The use of data sharing in speech-language telemedicine following stroke, Telemedicine Journal and e-Health 12 (2) (2006), 226.
[52] http://www.continuaalliance.org/home
View publication statsView publication stats





























