Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Patrick Ziegler & Hubert Schrezenmeier & Jamil Akkad &
Ute Brassat & Lucia Vankann & Jens Panse &
Stefan Wilop & Stefan Balabanov & Klaus Schwarz &
Uwe M. Martens & Tim H. Brümmendorf
Received: 7 March 2012 /Accepted: 16 March 2012 /Published online: 4 April 2012# Springer-Verlag 2012
Abstract Telomere length (TL) both reflects and limits thereplicative life span of normal somatic cells. As a conse-quence, critically shortened telomeres are associated with avariety of disease states. Telomere attrition can be counter-acted by a nucleoprotein complex containing telomerase.Mutations in subunits of telomerase, telomerase-bindingproteins as well as in members of the shelterin complexhave been described both in inherited and acquired bonemarrow failure syndromes. Here, we report on a patient withacquired aplastic anemia and a nonsynonymous variation ofcodon 1062 of the hTERT gene (p.Ala1062Thr) whosesubstantial and maintained hematologic response to long-term androgen treatment (including complete transfusionindependence) was paralleled by a significant and continuedincrease in TL in multilineage peripheral blood cells. To our
knowledge, this represents the first case of sustained telo-mere elongation in hematopoietic stem cells induced by apharmacological approach in vivo (141 words).
Keywords Telomere . Telomerase . Bone marrow failure .
Aplastic anemia . Androgen treatment
Introduction
Acquired bone marrow failure syndromes (aBMFS) arethought to result from (e.g., auto-immune-mediated) dam-age to the hematopoietic stem cell (HSC) compartment [1].As a consequence, telomere shortening in patients withaplastic anemia (AA) was found to be significantly correlated
Patrick Ziegler and Hubert Schrezenmeier contributed equally
P. Ziegler : L. Vankann : J. Panse : S. Wilop :T. H. Brümmendorf (*)Department of Oncology, Hematology and Stem CellTransplantation, University Hospital Aachen,RWTH Aachen University,Pauwelsstraße 30,52074 Aachen, Germanye-mail: [email protected]
H. Schrezenmeier :K. SchwarzInstitut für Klinische Transfusionsmedizinund Immungenetik Ulm,DRK Blutspendedienst Baden-Württemberg – Hessen,Sandhofstraße,60528 Frankfurt, Germany
H. Schrezenmeier :K. SchwarzInstitut für Transfusionsmedizin, Universität Ulm,Helmholtzstraße 10,89081 Ulm, Germany
J. Akkad :U. M. MartensDepartment of Hematology and Oncology,Cancer Center Heilbronn-Franken, SLK Kliniken,Am Gesundbrunnen 20-26,74078 Heilbronn, Germany
U. Brassat : S. BalabanovKlinik für Onkologie, Hämatologie undKnochenmarktransplantation mit Sektion Pneumologie,Universitäres Cancer Center Hamburg (UCCH),Universitäts-Klinikum Hamburg-Eppendorf,Martinistraße 52,20246 Hamburg, Germany
Ann Hematol (2012) 91:1115–1120DOI 10.1007/s00277-012-1454-x
Telomere elongation and clinical response to androgentreatment in a patient with aplastic anemia and a heterozygoushTERT gene mutation

with the degree of pancytopenia, risk of relapse after immu-nosuppressive (IS) therapy, size of a glycosylphosphatidyli-nositol (GPI) anchor-deficient subclone [2, 3], clonalevolution, and overall survival [4–6]. Among hematopoieticdisorders associated with altered telomere maintenance [7],telomere shortening is most accelerated in cases ofinherited BMFS (iBMFS) such as dyskeratosis congenita(DKC) which are thought to result from genetic aberra-tions in the gene DKC1 or in subunits of the telomerase orshelterin complex [8].
Methods
Patient material
Patient material was obtained following informed consent.Analysis was either performed as part of routine clinical careor approved by the local institutional review board (IRB) ofthe University of Ulm.
Sequencing of the telomerase reverse transcriptase gene
Genomic deoxyribonucleic acid (DNA) was isolated fromthe respective samples using standard procedures. Polymerasechain reaction (PCR) products included the coding exons andadjacent intronic regions (±10 bp). Primer sequences areavailable upon request (e-mail: [email protected]).Products were directly sequenced with BigDye Terminatortechnology and run on an ABI PRISM 3100 genetic analyzer(both from Applied Biosystems, Carlsbad, CA, USA).
TL measurement
The average telomere length (TL) in peripheral blood cells ofthe patient outlined below was measured by fluorescence insitu hybridization and flow cytometry (flow-FISH) [3, 5, 9,10] and by monochrome multiplex quantitative PCR (MM-QPCR) [11]. For flow-FISH, samples were analyzed in tripli-cate both with and without hybridization with FITC–(C3TA2)3PNA. Each sample included cow thymocytes as an internalcontrol and was counterstained with the DNA dye LDS751.Subfractions of peripheral blood cells were identified based ontwo parameters: forward light scatter and LDS751 fluores-cence. TL was calculated based on Southern blot analysisperformed on cow thymocytes as described previously [9].ForMM-QPCR, whole blood DNAwas isolated using a DNAblood kit (Quiagen, Hilden, Germany). For telomere amplifi-cation, the following primers were used—telg primer 5 -ACACTAAGGTTTGGGTTTGGGTTTGGGTTTGGGTTAGTGT-3 and telc primer 5 -TGTTAGGTATCCCTATCCCTATCCCTATCCCTATCCCTAACA-3 —as a referenceserving the beta-globin gene, which was amplified using hbgu
primer 5 -CGGCGGCGGGCGGCGCGGGCTGGGCGGCTTCATCCACGTTCACCTTG-3 and hbgd primer5 -GCCCGGCCCGCCGCGCCCGTCCCGCCGGAGGAGAAGTCTGCCGTT-3 . PCR was performed on a MyIQ2two-color real-time PCR detection system (Biorad) usingsignal acquisition at 74°C (telomere amplicon) and 88°C(beta-globin amplicon). For relative quantitation, six con-centrations of standard DNA sample were prepared byserial dilution and analyzed in the same 96-well plate asthe experimental DNA. Standard and experimental DNAwere assayed in triplicate. Amplification efficiency forthe data outlined here was between 90% and 100% forboth amplicons. Melt-curve analysis confirmed the specificityof the amplification. T/S ratio for experimental DNAsamples was calculated by dividing the copy number ofthe telomere template T by the copy number of the beta-globintemplate S.
Results and discussion
We report here on a 51-year-old male patient who was firstdiagnosed in February 2006 with moderate AA. The patientdeveloped slowly progressive pancytopenia affecting pre-dominantly erythropoiesis and megakaryopoiesis. Typicalextra-hematopoietic manifestations of DKC were excluded.TL was found to be significantly reduced below the 1%percentile of normal individuals [12], both in lymphocytes(4.28±0.02 kbp) and granulocytes (4.14±0.1 kbp). Sequenc-ing of the telomerase reverse transcriptase gene (hTERT)revealed a heterozygous mutation in exon 15 (ca. 3184 G>A)with a predicted nonsynonymous aminoacid change (p.Ala1062Thr) both in peripheral blood and buccalmucosa cells(data not shown). This mutation has been demonstrated tocause reduced telomerase activity by haploinsufficiency andhas been found to be associated with the development of acutemyeloid leukemia [8, 13]. Telomerase RNA subunit (hTERC)and DKC1 genes were found to be wild-type.
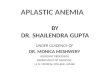
Based on the clinical presentation (i.e., moderate AAwithisolated red blood cell transfusion dependency) in conjunc-tion with a heterozygous hTERT mutation associated withsubstantial telomere shortening, we decided to initiate tes-tosterone undecanoat (Andriol® 80 mg tid) as first linetreatment rather than to initiate IS treatment with antithy-mocyte globulin (ATG) and cyclosporin (CSA) in April2007. Androgen treatment was well tolerated, and eventu-ally, after 12 months of treatment, the patient became redblood cell transfusion-independent (Fig. 1A). In parallel tohis hemoglobin levels rising to above 12 g/dl, the patient’splatelet count increased steadily and significantly over morethan 4 years (Fig. 1B). During this time period, the patientremained free of somatic symptoms and without apparentadverse events. Excitingly, this clinical and hematological
1116 Ann Hematol (2012) 91:1115–1120

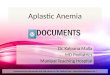
improvement was mirrored by a steady increase of TL inmultilineage peripheral blood cells (Fig. 2A–B), suggestingthat continuous telomere lengthening has occurred invivo in the multipotent hematopoietic stem and progenitorcompartment. Whereas telomeres in granulocytes typicallyloose an average of about 30–50 bp/year in adulthood(reviewed in Drummond et al. [7]), we found a mean increaseof >400 bp/year during the treatment period. Results obtainedby two independent methods, i.e., flow FISH and MM-QPCRcorrelated well (Fig. 2C). To our knowledge, this representsthe first case of sustained telomere elongation in HSCsinduced by a pharmacological approach in vivo. However,more than 5 years after first diagnosis of AA, the patientsblood counts began to drop again and four months later, thepatient developed acute myelogeneous leukemia (AML) with
a 50% infiltration of the bone marrow with CD13+CD33+,CD34+, CD117+, HLA-DR+leukemic blasts. Cytogeneticsrevealed monosomy 7, molecular markers NPM1 and FLT3were negative. Following induction chemotherapy, blastswere cleared from the patient’s bone marrow at day 22.However, due to persistent bone marrow aplasia and lackof hematopoietic recovery probably reflecting limitedbone marrow reserve due to his underlying BMFS, thepatient proceeded to allogeneic stem cell transplantationfrom a matched related donor. Within the first 100 dayspostallogeneic stem cell transplantation, the patient diedfrom acute graft versus host disease accompanied byinfectious complications.
Telomerase reverse transcriptase (hTERT) and its RNAtemplate (hTERC) are core components of the telomerase
8
10
12
14
16
40
80
120
160
200/6
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40 42 44 46 48 50 52 54 56 58 60 62 64 660.0
1.0
2.0
3.0
4.0
5.0
6.0/0
Andriol 80 mg tid
A hemoglobin
B plateletsplatelets
C wbc
Months
g/d
lX
103 /
µlX
103 /
µl
Fig. 1 Clinical response uponandrogen treatment. Timecourse of hemoglobin values(A), platelets (B), and whiteblood cell (wbc, C) counts in apatient before and duringtreatment with Andriol for redblood cell transfusion-dependent AA prior todiagnosis of secondary AML.Black arrows indicate packedred blood cell transfusions
Ann Hematol (2012) 91:1115–1120 1117

AML
AML
3 4 5 6 7 8
0.5
1.0
1.5
2.0
Granulocytes
3 4 5 6 7 8
0.5
1.0
1.5
2.0
Lymphocytes
A Flow-FISH
B MM-QPCR
C Correlation: MM-QPCR/flow-FISH
0 4 8 12 16 20 24 28 32 36 40 44 48 52 56 60 64 680
1
2
3
4
5
6
7
8
9
10/0
72
1
2
3
4
5
6
7
8
9
10
AML
Andriol
Andriol
MNCs
0 4 8 12 16 20 24 28 32 36 40 44 48 52 56 60 64 680.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
1.6
1.8
2.0
72
Tel
omer
e le
ngth
kbp
Rel
ativ
e T
/S r
atio
Months
Months
Telomere length kbp
Rel
ativ
e T
/S r
atio
Lymphocyte gate: + 438 bp/year
Granulocyte gate:+ 463 bp/year
R2=0.86 R2=0.86
Fig. 2 Telomere elongation invivo upon androgen treatment.Gain in telomere length(bp/year) in granulocytes andlymphocytes from peripheralblood during androgentreatment of a patient withacquired aplastic anemia and anonsynonmous mutation in thetelomerase gene measured byflow-FISH (A) and MM-QPCR(B). Correlation of the relativeT/S ratios obtained byMM-QPCR in whole bloodDNA samples with telomerefluorescence values determinedby flow-FISH
1118 Ann Hematol (2012) 91:1115–1120

complex together with other proteins [14]. Mutations in sev-eral telomere maintenance genes, including dyskerin (DKC1)[15], hTERC [16], hTERT, TINF2, NOP10 and NHP2, resultin inherited aBMFS such as DKC. Patients with DKC havebeen shown to have ultra-short telomeres associated with ahighly increased risk of developing iBMFS before the age of30 years [16]. Heterozygous hTERT mutations compromisetelomerase function mostly by haploinsufficiency and rarely,by a dominant negative effect [17]. Interestingly, hTERTcatalytic activity has been shown to be responsive to stimula-tion by sex hormones via upregulation of hTERTmRNA [18].Recently, hematopoietic cells from patients carrying muta-tions within the telomerase complex have been shown torespond to androgen treatment in vitro [19]. Obviously, sincebone marrow specimens were not available under treatment,we cannot provide formal proof of increased telomerase ac-tivity under andriol treatment eventually leading to elongationof TL in hTERT-mutated HSCs. However, the gradual natureof improvement in blood counts over more than 4 yearsparalleled by continued elongation of TL in peripheral bloodgranulocytes and lymphocytes is in support of this hypothesis.Alternatively, TL increase can be explained by favorableactivity of androgen treatment on subclone(s) with particularlylong telomeres [20] eventually leading to clonal selection ofsuch HSC(s). Whereas TL in peripheral blood cells amountedto 7.3 kb 5 months before diagnosis of AML, it was dramat-ically reduced in bone marrow blasts retrieved from the timepoint of AML diagnosis (3.7 kb). As expected [10], despite ofsignificantly reduced TL, TA was found to be significantlyincreased in myeloid leukemic blasts (not shown).
Taken together, these findings seem to suggest that evolutionto secondary AML occurred in a subclone of HSCs that eitherwas primarily unresponsive to androgen treatment (and there-fore telomeres remained short) or developed secondary resis-tance at some point during the years of andriol treatment leadingto accelerated telomere shortening and genetic instability.
Clinically, patients with AA refractory to IS treatmentrequire alternate treatment strategies such as allogeneic stemcell transplantation, a treatment option that is associatedwith significant risk and considerable comorbidities and(given the age distribution of the patients) not readily avail-able for all patients [21]. Alternatively, in addition to sup-portive care, corticosteroids and particularly syntheticandrogenic steroids have been used in individual caseseffectively. Recently, a Japanese study successfully investi-gated Danazol in Japanese individuals with AA refractory toIS [22]. Moreover, Danazol was used as first line treatmentin patients who were not eligible for allogeneic stem celltransplantation and did not have access to standard first linetreatment with ATG and CSA in Mexico [23]. In this study,the response rate in the Danazol arm was 46% (17 out of 37patients treated) and tolerability at a dose of 300–600 mg(median 400 mg) was favorable.
The role of androgen treatment in AA, in general, and in“telomeropathies,” in particular, will have to be tested pro-spectively and studies addressing this issue are alreadyongoing (ClinicalTrials.gov identifier: NCT01441037).Nevertheless and in line with these strategies, we feel thatevidence is increasing that screening TL analysis should beincorporated into the routine clinical work-up of patientswith BMFS to date and might not only serve as a valuableprognostic but eventually also as an important predictivebiomarker for patients receiving treatment with androgenderivatives in this disease.
Ann Hematol (2012) 91:1115–1120 1119
References
1. Young NS, Maciejewski J (1997) The pathophysiology of acquiredaplastic anemia. N Engl J Med 336(19):1365–1372
2. Beier F, Balabanov S, Buckley T, Dietz K, Hartmann U, RojewskiM, Kanz L, Schrezenmeier H, Brummendorf TH (2005) Acceler-ated telomere shortening in glycosylphosphatidylinositol (GPI)-negative compared with GPI-positive granulocytes from patientswith paroxysmal nocturnal hemoglobinuria (PNH) detected byproaerolysin flow-FISH. Blood 106(2):531–533
3. Baerlocher GM, Sloand EM, Young NS, Lansdorp PM (2007)Telomere length in paroxysmal nocturnal hemoglobinuria corre-lates with clone size. Exp Hematol 35(12):1777–1781
4. Ball SE, Gibson FM, Rizzo S, Tooze JA, Marsh JC, Gordon-SmithEC (1998) Progressive telomere shortening in aplastic anemia.Blood 91(10):3582–3592
5. Brummendorf TH, Maciejewski JP, Mak J, Young NS, LansdorpPM (2001) Telomere length in leukocyte subpopulations ofpatients with aplastic anemia. Blood 97(4):895–900
6. Scheinberg P, Cooper JN, Sloand EM, Wu CO, Calado RT, YoungNS (2010) Association of telomere length of peripheral bloodleukocytes with hematopoietic relapse, malignant transformation,and survival in severe aplastic anemia. JAMA 304(12):1358–1364
7. Drummond MW, Balabanov S, Holyoake TL, Brummendorf TH(2007) Concise review: telomere biology in normal and leukemichematopoietic stem cells. Stem Cells 25(8):1853–1861
8. Calado RT, Young NS (2009) Telomere diseases. N Engl J Med361(24):2353–2365
9. Baerlocher GM, Vulto I, de Jong G, Lansdorp PM (2006) Flowcytometry and FISH to measure the average length of telomeres(flow FISH). Nat Protoc 1(5):2365–2376
10. Hartmann U, Brummendorf TH, Balabanov S, Thiede C, Illme T,Schaich M (2005) Telomere length and hTERT expression inpatients with acute myeloid leukemia correlates with chromosomalabnormalities. Haematologica 90(3):307–316
11. Cawthon RM (2009) Telomere length measurement by a novelmonochrome multiplex quantitative PCR method. Nucleic AcidsRes 37(3):e21
12. Rufer N, Brummendorf TH, Kolvraa S, Bischoff C, Christensen K,Wadsworth L, Schulzer M, Lansdorp PM (1999) Telomere fluo-rescence measurements in granulocytes and T lymphocyte subsetspoint to a high turnover of hematopoietic stem cells and memory Tcells in early childhood. J Exp Med 190(2):157–167
13. Yamaguchi H, Calado RT, Ly H, Kajigaya S, Baerlocher GM,Chanock SJ, Lansdorp PM, Young NS (2005) Mutations in TERT,
Conflict of interest None

14. Martinez P, Blasco MA (2011) Telomeric and extra-telomeric rolesfor telomerase and the telomere-binding proteins. Nat Rev Cancer11(3):161–176
15. Knight SW, Heiss NS, Vulliamy TJ, Greschner S, Stavrides G, PaiGS, Lestringant G, Varma N, Mason PJ, Dokal I, Poustka A (1999)X-linked dyskeratosis congenita is predominantly caused by mis-sense mutations in the DKC1 gene. Am J Hum Genet 65(1):50–58
16. Vulliamy TJ, Knight SW, Mason PJ, Dokal I (2001) Veryshort telomeres in the peripheral blood of patients with X-linked and autosomal dyskeratosis congenita. Blood Cells Mol Dis27(2):353–357
17. Xin ZT, Beauchamp AD, Calado RT, Bradford JW, Regal JA,Shenoy A, Liang Y, Lansdorp PM, Young NS, Ly H (2007)Functional characterization of natural telomerase mutations foundin patients with hematologic disorders. Blood 109(2):524–532
18. Kyo S, Takakura M, Kanaya T, Zhuo W, Fujimoto K, Nishio Y,Orimo A, Inoue M (1999) Estrogen activates telomerase. CancerRes 59(23):5917–5921
19. Calado RT, Yewdell WT, Wilkerson KL, Regal JA, Kajigaya S,Stratakis CA, Young NS (2009) Sex hormones, acting on theTERT gene, increase telomerase activity in human primary hema-topoietic cells. Blood 114(11):2236–2243
20. Bartolovic K, Balabanov S, Berner B, Buhring HJ, Komor M,Becker S, Hoelzer D, Kanz L, Hofmann WK, Brummendorf TH(2005) Clonal heterogeneity in growth kinetics of CD34+CD38-human cord blood cells in vitro is correlated with gene expressionpattern and telomere length. Stem Cells 23(7):946–957
21. Marsh JC, Ball SE, Cavenagh J, Darbyshire P, Dokal I, Gordon-Smith EC, Keidan J, Laurie A, Martin A, Mercieca J, Killick SB,Stewart R, Yin JA (2009) Guidelines for the diagnosis and man-agement of aplastic anaemia. Br J Haematol 147(1):43–70
22. Chuhjo T, Yamazaki H, Omine M, Nakao S (2008) Danazol herapyfor aplastic anemia refractory to immunosuppressive therapy. Am JHematol 83(5):387–389
23. Jaime-Perez JC, Colunga-Pedraza PR, Gomez-Ramirez CD,Gutierrez-Aguirre CH, Cantu-Rodriguez OG, Tarin-Arzaga LC,Gomez-Almaguer D (2011) Danazol as first-line therapy for aplas-tic anemia. Ann Hematol 90(5):523–527
1120 Ann Hematol (2012) 91:1115–1120
the gene for telomerase reverse transcriptase, in aplastic anemia. NEngl J Med 352(14):1413–1424