Embed Size (px)
Citation preview

Testimony
of the
American Hospital Association
before the
Subcommittee on Antitrust, Competition Policy and Consumer Rights
of the
Committee on the Judiciary
of the
U.S. Senate
“Examining Consolidation in the Health Insurance Industry and its Impact on Consumers”
September 22, 2015
I am Rick Pollack, president and CEO of the American Hospital Association (AHA). On behalf
of our nearly 5,000 member hospitals, health systems and other health care organizations, and
our 43,000 individual members, I thank you for the opportunity to testify.
Both of the recently proposed commercial health insurance deals – Anthem’s acquisition of
Cigna and Aetna’s acquisition of Humana – could be a blow to millions of health care
consumers, as well as the hospitals, doctors and others who are working to improve quality and
efficiency while making care more affordable to patients. The unprecedented level of
consolidation these deals threaten could make health insurance more expensive and less
accessible for consumers. This applies to health insurance purchased in the commercial market
as well as Medicare Advantage (MA) plans. These deals also could further entrench the power of
the Blues plans, which currently dominate the market in nearly every state.
Another likely casualty of these deals is the momentum hospitals have established to move the
nation’s health care system forward. Despite the commercial insurers’ recent claims that they are
fostering innovation, they continue to benefit financially from letting hospitals do most of the
hard work of reducing readmissions, improving (rigorously measured) patient quality,

2
experimenting with accountable care organizations (ACOs) and bundling programs, instituting
population health programs and numerous other efforts designed to turn a system predicated on
volume to one measured by value. There is no reason to believe that allowing these insurers to
become even larger and more immune from competitive forces would alter their incentive to sit
mostly on the sidelines and reap the considerable financial rewards of providers’ innovation.
Neither of the proposed acquisitions should be permitted to move forward until federal and state
antitrust and insurance authorities can offer assurances that they are procompetitive, will not
leave consumers with fewer and more expensive options for coverage or diminish insurers’
willingness to be innovative partners with providers to move our health care system beyond silos
to a continuum of care that is responsive to consumers’ needs.
SERIOUS CONCERNS ABOUT HEALTH INSURANCE CONSOLIDATION
The AHA recently shared with the Department of Justice’s Antitrust Division (Department) our
serious concerns about the recently announced acquisitions; the two letters are attached.1 These
deals would eliminate two of the largest national health insurance companies, leaving just three
dominant providers of health insurance, and an even more consolidated health insurance
market. Recent American Medical Association (AMA) data on health insurance concentration
confirms that consolidation is widespread – 70 percent of health insurance markets are “highly
concentrated.”2
Concentration Matters. A recent study3 in Technology Science highlighted why this increasing
concentration should be of particular concern. It found that the largest issuer in each state not
only raised premiums by higher amounts, but also raised premiums on more of their plans than
other issuers in the same state.
Anthem’s Acquisition of Cigna Threatens to Reduce Competition on a Massive Scale.
The potential harm to consumers from the loss of competition that could result
from the Anthem/Cigna transaction is large and durable. Because the two
companies generate more than $100 billion in revenue, even a modest price
increase would cost consumers billions of dollars in higher health care costs.4
The geographic reach of the transaction would be sweeping. It threatens to reduce competition
for commercial health insurance in at least 817 markets across the U.S. that serve 45 million
consumers. In each of these markets the transaction would produce a Herfindahl-Hirschman
Index (HHI) score of 2,500 or more, which the merger guidelines indicate either raise serious or
virtually insurmountable competitive issues.
The parties’ attempt to explain away the substantial competition between them by creating
artificial “submarkets” (by, we assume, customer category and/or policy type) should be viewed
with great skepticism. Typically, when companies go to such lengths, it is to obscure competitive
overlaps in a desperate effort to demonstrate that a market is competitive. In fact, both
companies acknowledge in their public statements that they compete vigorously for the same

3
group of customers, including large group customers. Moreover, even if such market
stratification were valid and the companies do not actually compete in the regions in which they
both actively sell commercial insurance, it would reflect enormously high entry barriers and raise
questions about anticompetitive coordination (which also should be investigated) and, of course,
underscore the deal’s enormous anticompetitive potential.
The durability of the anticompetitive impact is enhanced because of the high barriers to entry in
the health insurance market. A former Acting Assistant Attorney General modestly described
entry as “difficult,” particularly in concentrated markets like those at issue in this
transaction. One of the very few new companies to even attempt entry described it as “quite
daunting.”5 Just last week, the New York Times reported on the demise of a number of health
insurance start-ups, concluding that “the [health insurance] marketplace is proving hostile to
newcomers trying to break into the industry dominated by powerfully entrenched businesses.”6
Claims of offsetting efficiencies cannot ameliorate the competitive harm from this deal. Insurers
have a dismal track record of passing any savings from an acquisition on to consumers, and there
is no reason to believe that this transaction would be any different.7 In addition, neither of the
legislated controls on excessive premium hikes – medical loss ratio (MLR) or rate review – are
sufficient to prevent Anthem from raising rates to consumers above competitive levels.
The MLR measures how much of the premium dollar goes to pay for medical claims and quality
activities instead of administrative costs and marketing. Despite its seeming promise, the MLR
will not be effective in controlling premium cost increases because: the MLR requirements apply
to fewer than 50 percent of Americans under age 65 with health insurance coverage; the rules for
reporting MLRs may mask differences in premiums rate increases; and the MLR does not
address the level of the premium increase, only the percentage used for claims and quality
activities.
Likewise, insurance rate review will not prevent rate hikes. Neither the Department of Health
and Human Services nor most states have the power to prevent a rate hike. For example, an
article in the August 27 Wall Street Journal8 reported that officials had “greenlighted” hikes in
health insurance rates of more than 36 percent in Tennessee, 25 percent in Kentucky and 23
percent in Idaho.
Another concern is that Anthem’s affiliation with the Blue Cross and Blue Shield (Blue) system
raises some particular competitive concerns. An August 2015 letter9 from Joe R. Whatley, Jr., to
the Department described the Blue Cross Blue Shield Association’s license agreement that
prevents the individual Blue plans from directly competing against one another, and also
prevents their non-Blue subsidiaries from competing even slightly vigorously against other Blue
companies. The letter stated:
Because Anthem cannot expand its non-Blues business, an evaluation of the
effects of its merger with Cigna must include not only those geographic markets
in which Cigna competes with Anthem, but also those geographic markets where
Cigna competes (or would compete) with any other insurers. In each of those
markets … Cigna can no longer compete for new business in any market unless it

4
decreases its business by an offsetting amount in another market. The net effect is
that Cigna’s effectiveness as a competitor … will be impaired.
The letter may only have partially captured the extensive interconnections between Anthem and
the other BlueCard members that appear likely to eliminate competition between Cigna and
every Blue plan in every state. In fact, the letter may understate the coordination likely to result
between Cigna and the non-Anthem Blues plans.
As a result of the folding of Cigna into the overall Blue system through Anthem’s Blues
affiliation, this deal may augment the already considerable power of the Blue plan in every
state. The AMA data report that Blues plans tend to be the most dominant plan in virtually every
state in which they operate. Because of the way in which the Blue system operates, Blues plans
nationwide may now be able to control Cigna lives – particularly for BlueCard members,
including national employer accounts – as their own when they negotiate with providers for
rates, terms and conditions under which coverage is available to consumers. If so, this would
give these Blues plans even more market power to block entry into their local markets and to
constrict plan design and reimbursement rates by, for example, further narrowing provider
networks available to consumers and/or driving down rates for those in the network below
competitive levels and causing some to decline to participate in any network. The Blues’ control
over provider reimbursement would increase their ability to put new plans and those hoping to
expand at a competitive disadvantage by depriving providers of the flexibility and options to
work effectively with those new insurance competitors.
At a time of rising health insurance premiums, the Department and state Attorneys General
should examine closely how this acquisition could increase Blue plan dominance
nationwide. Blue Cross dominance has been an issue the Department has been concerned with in
previous health insurance consolidations. In a speech by former Assistant Attorney General
Christine Varney10, she noted that local health plan dominance (i.e., Blue plan dominance)
creates barriers to entry. And, the department has challenged two Blue plan mergers that would
have increased that dominance. Given the size and scope of this deal and the dominance of the
Blue plans nationwide, the Department should thoroughly investigate how the addition of Cigna
to the Blues’ arrangement could further entrench that widespread dominance and decrease
competition, reduce the number of participating providers and lead to higher consumer
premiums.
While it may have been sufficient in the past, it is unlikely that divestitures, no matter how
numerous, could rescue this deal. As we noted in our letter to the Department, in “the 817 at-risk
markets, over half of the lives that need to be divested reside across 368 MSAs (metropolitan
statistical areas) and rural counties [where there is] no divestiture possibility that is likely to
preserve” the benefits of competition. Significantly, it has been reported that the divestitures
required for two deals overseen by the Federal Trade Commission (FTC) are floundering. That is
significant because the divestitures for both deals were much less numerous than those likely to
be required for an Anthem/Cigna combination.11 The report highlighted the problems the
antitrust agencies face in trying to turn “smaller firms into large competitors capable of
absorbing major divestitures.”

5
Further, the deal could eliminate an irreplaceable source of competition for national accounts and
large regional customers. The FTC recently prevailed in a case where it found a national market
despite the parties’ claims the market was more segmented and localized.12 Both Cigna and
Anthem serve national accounts (large multi-state employers) and large regional customers. As
recently as the first quarter of 2015, Anthem’s president and CEO told investors it was
“optimistic” about the 2016 outlook for national accounts and had closed on two new large
accounts serving several hundred thousand lives.13 In its second quarter 2015 earnings call with
investors, Anthem’s chief financial officer and executive vice president suggested its Blues
affiliation was an “instrumental part” of its success with national accounts.14
Aetna’s Acquisition of Humana Could Further Concentrate MA Markets Already
Suffering from a Lack of Competitive Alternatives. Nearly 18 million people obtain their
health insurance through MA, and that number is growing rapidly: “The total Advantage
population is up 7.3 percent from … this time last year, according to the latest CMS data.”15
More than 2.7 million seniors are enrolled in MA plans operated by these insurers in more than
1,000 markets that would become highly concentrated if Aetna is permitted to acquire Humana
(this estimate uses the HHI). The deal would not only eliminate current competition between
Aetna and Humana in the MA market, it also would eliminate the possibility of future
competition between them. Humana is the second-largest MA insurer with 3.23 million members
(an 11.4 percent increase over last year), and Aetna the fourth largest with 1.27 million
members.16 As recently as 2014, Aetna appeared to believe it was capable of growing its MA
business substantially without this acquisition.17
This is particularly concerning as there is almost a complete lack of competition in MA markets,
according to an August 2015 report by the Commonwealth Fund18, which found that 97 percent
of MA markets in U.S. counties are “highly concentrated.” This confirms the findings of a recent
report by the Kaiser Family Foundation19 that also described MA markets as highly
concentrated. That report also noted that, while the MA program has continued to grow in
virtually all states, MA plans now provide less financial protection for enrollees and average out-
of-pocket expenses have continued to climb; this is not an unexpected development in such
highly-concentrated markets.
A somewhat perplexing new report from Avalere20 suggests that both the Commonwealth Fund
and Kaiser are wrong. The report claims there is new market entry and growth, as well as
diversification in MA markets. These new entrants mainly comprise a Blue plan and 15 provider-
owned plans. While provider-owned plans offer seniors an excellent choice in the geographic
areas they cover, they cannot begin to replace the loss of competition in more than 1,000 markets
in 38 states for the 2.7 million seniors that are at risk because of this transaction. Furthermore,
some skepticism should be applied to any characterization of a Blue plan as a new entrant into a
health insurance market.
The Department has viewed MA as a separate product market because of its unique
characteristics. Both lower out-of-pocket costs and a more extensive benefit design have
distinguished it from traditional Medicare. While payments to MA plans have moderated, the
financial protection and greater range of benefits offered by MA plans continue to attract seniors
in large numbers, despite predictions that lowered payments would have the opposite effect.

6
The high barriers to market entry and lack of efficiencies present in the Anthem deal are present
here as well. The remedy the Department has relied on in previous health insurance deals – a
series of MA plan divestitures – is unlikely to be sufficient to remediate the likely competitive
harm from this deal. The difficulty of implementing successfully this structural remedy should
not be underestimated – a suitable acquirer would need to be identified in 1,083 counties in 38
states serving more than 2.7 million current Aetna and Humana members. Even if it were
feasible, which it likely is not, it would be a staggering task to develop, implement and supervise
these divestitures in a manner that did not further erode the competitive equilibrium in these
markets and harm seniors, as well as the promise of the MA program itself.
WHY HOSPITAL DEALS ARE DIFFERENT
Hospitals’ Realignment. Hospitals have shouldered much of the heavy burden of reshaping the
nation’s health care system to meet the laudable goals of improving quality and efficiency and
making care more affordable for patients and families. And hospitals have made significant
strides toward meeting all of those goals. A July 2015 study, reported in the Journal of the
American Medical Association, described it as a “medical hat trick:”21
In this comprehensive analysis of the hospital trends in the Medicare fee-for-
service populations aged 65 years and older, there were marked reductions in all-
cause mortality rates, all-cause hospitalization rates, and inpatient expenditures, as
well as improvements in outcomes during and after hospitalization.
Unlike the insurance deals, which appear motivated by top-line profits, hospital realignment is a
procompetitive response to the major forces reshaping the health care system:
Widespread recognition, especially among those in the hospital field, of the need to
replace a “siloed” health care system with a continuum of care that improves
coordination and quality and reduces costs for patients;
Changes in reimbursement models to reward value and encourage population health;
Increased capital requirements; and
Competition that is rapidly changing how services are delivered.
Building a Continuum of Care. Building a continuum demands that providers be more
integrated. Integration can take many forms – hospitals, physicians, post-acute care providers
and others in the health care chain can integrate clinically or financially, horizontally or
vertically, and the relationships can range from loose affiliations to complete mergers – and it is
happening across the country. For example, a large teaching hospital in Virginia is partnering
with other hospitals in the state to form a regional health care system; a New Orleans health
system is partnering with four other hospitals across the state to launch a network to provide
patients with access to 25 medical facilities and more than 3,000 physicians; and hospitals in
Michigan partnered to create a regional affiliation allowing a critical access hospital’s patients
access to the full array of services offered by the larger system. In addition, two prestigious
teaching hospitals in California have teamed up with a local acute rehabilitation hospital to

7
develop a world-class regional center for treating complex rehabilitation cases from around the
nation.
Hospitals and patients benefit when a hospital realigns. The most common benefits are improved
coordination across the care continuum, increased operational efficiencies, greater access to cash
and capital for smaller or financially distressed hospitals, and support for innovation, including
payment alternatives that entail financial risk. For financially struggling hospitals, finding a
partner can make all the difference. For example:
A health system in Ohio acquired a small, community hospital in bankruptcy with closure
impending; it expanded access to care in the rural area, increased technological
efficiencies and saved 250 community jobs.
An acquisition by a nearby hospital system of a hospital that was struggling financially
led to it being transformed into a much-needed regional children’s hospital, which
provided improved access and services for area children.
Regulatory Barriers Persist for Integration. While innovative partnerships and integrative
arrangements abound throughout the country, permanent arrangements, such as mergers, offer
the most protection from a staggering array of outdated regulatory barriers that make integration
risky when Medicare or Medicaid patients are involved. Despite the AHA having identified the
five main barriers to clinical integration more than 10 years ago, to date, only one regulatory
barrier has been addressed. The following barriers remain:
Lack of antitrust guidance on clinical integration (current guidance applies only to
arrangements that are part of ACOs);
Restrictions on arrangements that base payments on achievements in quality and
efficiency instead of just hours worked (Stark Law);
Restrictions on financial incentives to physicians that could be construed as influencing
care provided, even if the goal of the incentive is to adopt proven protocols and
procedures to improve care (Anti-kickback law); and
Uncertainty about how the Internal Revenue Service will view payments from tax-
exempt hospitals to non-tax exempt physicians working together in clinically integrated
arrangements.
It is notable that all these barriers to clinical integration had to be addressed to allow the ACO
program to move forward. Yet, the federal agencies responsible for administering these laws and
regulations have yet to modernize them, with one limited exception, to support even more
progress toward building a continuum of care through innovative arrangements like those
described above.
MOVING TO A VALUE-BASED REIMBURSEMENT SYSTEM
Increasingly, reimbursement models are being recast to compensate providers based on
outcomes, not the volume of services provided. The outcomes being rewarded include keeping

8
patients well (population health) and providing high-quality services when patients are in the
hospital.
Many hospitals, health systems and payers are adopting delivery system reforms with the goal of
better aligning provider incentives to achieve higher-quality care at lower costs. These reforms
include forming ACOs, bundling services and payments for episodes of care, developing new
incentives to engage physicians in improving quality and efficiency, and testing payment
alternatives for vulnerable populations. The Centers for Medicare & Medicaid Services (CMS)
recently announced a goal of moving 30 percent of Medicare payments to alternative models of
reimbursement that reward value by 2016 and to 50 percent of payments by 2018. In its
announcement, CMS recognized that achieving these goals would require hospitals to “make
fundamental changes in their day-to-day operations that improve the quality and reduce the cost
of health care.”
Hospitals have supported these efforts and often take the lead in testing and improving them. In
addition, hospitals are collaborating with and learning from each other in order to improve the
quality of care they deliver to patients. For example, the Health Research & Educational Trust
(HRET), an AHA affiliate, was awarded a contract by CMS to support the Partnership for
Patients campaign, a three-year, public-private partnership designed to improve the quality,
safety and affordability of health care for all Americans. The AHA/HRET Hospital Engagement
Network project helped hospitals adopt new practices with the goal of improving patient care and
reducing readmissions by 20 percent. The project, which included a network of nearly 1,500
hospitals across 31 states, focused on several areas of impact and produced cost savings of $988
million through improved care. Some additional highlights include: a 61 percent reduction in
early elective deliveries across 800 birthing hospitals; a 48 percent reduction in venous
thromboembolism (blood clot in a vein) across 900 hospitals; and a 54 percent reduction in
pressure ulcers across 1,200 hospitals.
Meanwhile, many hospitals report that it has been difficult to work with commercial insurers in
moving to new payment models. We recently surveyed members of AHA’s nine regional policy
boards, which represent hundreds of hospitals around the nation, about their experience working
with commercial insurers on new payment models. About 80 percent reported it was a challenge
to work with insurers on new payment models, and more than 40 percent described it as a major
challenge.
INCREASED CAPITAL REQUIREMENTS
The fundamental restructuring that CMS anticipates in response to its alternative reimbursement
models will undoubtedly come with a high cost that will be particularly difficult to bear for small
and stand-alone hospitals. Already, the field is under serious financial pressure from the need for
capital expenditures, particularly those for health information technology (IT) and electronic
health records (EHRs). In fact, the AHA estimates that hospitals collectively spent $47 billion on
IT, including EHRs, each and every year between 2010 and 2013.

9
EHRs are essential to improving care and, consequently, succeeding in value-based
reimbursement models. Every hospital is expected to meet a constantly evolving set of standards
for having and using EHRs for their patients. And a portion of Medicare and Medicaid
reimbursement is conditioned on EHR adoption and use. Estimates are that EHRs will cost a
hospital between $20 and $200 million depending on their size. For smaller, rural and stand-
alone hospitals, these costs can be ruinous without a partner to absorb some of the cost and
provide the necessary technical expertise.
For many hospitals, the credit markets are already difficult to access. The most recent
FitchRating report confirms this; starting in 2011, the profitability “metrics” for the lowest-rated
hospitals have declined.22 The lowest-rated hospitals tend to be smaller or stand-alone. The debt
burden for the lowest-rated hospitals also has continued to grow, and the hospitals’ operating
margins are razor thin. For these hospitals, accessing the credit markets for capital
improvements, including technology, will be difficult, if at all possible. Without a partner, these
hospitals will continue to decline until they are forced to close their doors, with potentially
devastating repercussions for the communities they serve.
NEW COMPETITION FOR HOSPITAL SERVICES
Rapid changes in the health care market are providing consumers with an increased array of
options for their health care, including services that hospitals provide.
CVS, Walgreens and Wal-Mart, among others, are changing where consumers go for their health
care needs. The retailers offer an array of health care services, including primary care,
immunizations, blood pressure monitoring and routine blood tests, all of which were formerly
available only in a doctor’s office or hospital outpatient clinic or emergency room. Meanwhile,
many of the retailers plan to provide even more sophisticated care and services at their thousands
of convenient locations. These developments challenge hospitals to become more integrated with
physicians and other providers so that they too can offer convenient and more affordable care
that is attractive to patients.
In addition, telehealth promises to revolutionize how an incredible array of health care services
are provided to consumers and to change the competitive landscape entirely. Telehealth is
already delivering services as different as dermatology and mental health to patients across town
and across the country. A hospital in Arlington, Va., has an arrangement with the Mayo Clinic,
which is based in Rochester, Minn., that allows its patients access to Mayo’s expertise without
leaving the neighborhood. In addition, a hospital system in California was able to cover its need
for physician intensivists at one of its satellite facilities using mobile telehealth devices instead of
hiring new doctors, with positive clinical and patient satisfaction outcomes. Increasingly, patients
are able to consult doctors using their computers, laptops and smartphones, and this is becoming
a more common expectation of patients when they seek care. For their part, insurers too are
increasingly relying on telehealth to reduce costs and meet network adequacy requirements. All
of this changes the competitive landscape for hospitals. Now, competitors for even specialized
services do not have to be in the same neighborhood, city or state to connect with patients who
might otherwise have sought care at their local hospital.

10
The rapid growth of telehealth illustrates how quickly the competitive landscape can change for
hospitals and the importance of having adequate financial resources and access to capital.
Without those resources, hospitals cannot keep up with the demands of new technology or the
opportunities they present.
CONCLUSION
Consumers and the entire health care system are threatened by the potential consequences of the
unprecedented consolidation that would result from Anthem’s acquisition of Cigna and Aetna’s
acquisition of Humana. These health insurance deals, which would affect at least one form of
health insurance in every state, could mean fewer choices for consumers for commercial
insurance and MA plans, narrower networks of providers in what few choices remain and higher
prices for premiums or more out-of-pocket costs. The deals also could diminish insurers’
willingness to be innovative partners with providers, as well as jeopardize the momentum
hospitals have led to improve quality and efficiency while making care more affordable for
patients and families.
Some have compared the insurance deals to those in the telecommunications arena because of
their size and the enduring ability to contort the market and harm consumers. The Department
was ready to challenge the telecommunications deals, and it also should be ready to challenge the
insurance deals, if, as we expect, its intensive investigation confirms that these transactions
threaten the growth and vitality of our health care system and the health and welfare of
consumers across the nation.
1 www.aha.org/letters 2 Competition in Health Insurance A comprehensive study of U.S. markets, American Medical Association, 2015
Update, https://commerce.ama-
assn.org/store/catalog/productDetail.jsp?product_id=prod2680007&navAction=push#usage-tab. 3 Wang E, Gee G. Larger Issuers, Larger Premium Increases: Health insurance issuer competition post-ACA.
Technology Science. 2015081104. August 11, 2015. http://techscience.org/a/2015081104. 4 AHA letter to the Honorable William Baer, August 5, 2015. 5 This $1.5 billion Startup is Making Health Insurance Suck Less, Wired, March, 20, 2015
http://www.wired.com/2015/04/oscar-funding/. 6 Tough Going for Co-Ops, New York Times, September 15, 2015. 7 Testimony of Professor Thomas L. Greaney, Before the House of Representatives Subcommittee on Regulatory
Reform, Commercial and Antitrust Law, September 10, 2015. 8 Insurers Win Big Health-Rate Increases, Wall Street Journal, August 27, 2015.
http://www.wsj.com/articles/insurers-win-big-health-rate-increases-1440628848. 9 Joe R. Whatley, Jr., letter to the Honorable William Baer, August 13, 2015. 10Remarks of Christine Varney, then Assistant Attorney General of the DOJ’s Antitrust Division, at a joint
American Bar Association/American Health Lawyers Association Antitrust in Healthcare Conference, May 24,
2010, available at http://www.justice.gov/atr/speech/antitrust-andhealthcare 11Reporting on divestitures ordered in the car rental and grocery store industries. Divestitures required were 58 on-
airport locations and a line of business for the Hertz deal and 168 supermarkets in 130 locations for Albertsons.
http://pipeline.thedeal.com/tdd/ViewArticle.dl?s=dd&id=13291361&cmpid=em:DA091715#ixzz3m1SYWNdc

11
12 FTC v. Sysco Corp, (D.D.C.) June 23, 2015 at https://www.ftc.gov/system/files/documents/cases/150623syscomemo.pdf 13 Anthem Quarter 1 Earnings Call with Investors, April 29, 2015, http://www.thestreet.com/story/13131183/1/anthem-antm-earnings-report-q1-2015-conference-call-transcript.html. 14 Anthem Quarter 2 Earnings Call with Investors, July 29, 2015, http://phx.corporate-ir.net/External.File?item=UGFyZW50SUQ9NTg4NjExfENoaWxkSUQ9Mjk2ODg1fFR5cGU9MQ==&t=1. 15 Medicare Advantage membership nearly 18 million ahead of annual enrollment, Modern Healthcare, September 17, 2015 (Modern). 16 Modern. 17 AHA letter to the Honorable William Baer and Secretary Burwell, September 1, 2015 (see chart page 16). 18 Brian Biles, Giselle Casillas, and Stuart Guterman, Competition Among Medicare’s Private Health Plans: Does It
Really Exist?, The Commonwealth Fund August 2015,
www.commonwealthfund.org/publications/issue-briefs/2015/aug/competition-medicare-private-plans-does-it-exist. 19 Gretchen Jacobson, Anthony Damico and Marsha Gold, Kaiser Family Foundation Issue Brief, Medicare
Advantage 2015 Spotlight: Enrollment Market Update, June 30, 2015, http://kff.org/medicare/issuebrief/medicare-
advantage-2015-spotlight-enrollment-market-update/. 20 New Market Entrants: Growth and Diversification in U.S. Health Insurance, Avalere, September 2015. 21 ‘Jaw-dropping’: Medicare deaths, hospitals AND costs reduced, USA Today, July 28, 2015. Reporting on
“Mortality, Hospitalizations, and Expenditures for the Medicare Population Aged 65 Years and Older, 1999-2013”,
Krumholz, Nuti, Downing, Normand & Wang, JAMA, July 28, 2015, Vol. 312, No. 4. 22 FitchRatings, 2015 Medium Ratios for Nonprofit Hospitals and Health Systems, Special Report, August 10, 2015.

By Email and Courier
September 1, 2015
The Honorable William Baer
Assistant Attorney General
United States Department of Justice Antitrust Division
950 Pennsylvania Avenue, N.W.
Washington, D. C. 20530
The Honorable Sylvia Burwell
Secretary
Department of Health & Human Services
200 Independence Avenue, S.W.
Washington, D.C. 20201
Dear Assistant Attorney General Baer and Secretary Burwell:
I’m writing on behalf of nearly 5,000 member hospitals, health systems and other health care
organizations, and 43,000 individual members of the American Hospital Association (AHA)
regarding the proposed acquisition involving two of the five major commercial health insurance
companies in the United States: Aetna’s proposed acquisition of Humana. We previously wrote
to the Department of Justice’s Antitrust Division (Department) on August 5, 2015, about the
proposed acquisition of Cigna by Anthem. That letter is attached.
Our concerns about the proposed Aetna/Humana deal are similar in many respects. Both have the
very real potential to reduce competition substantially, increase the cost of premiums, and
diminish the insurers’ willingness to be innovative partners with providers and consumers in
transforming health care. Viewed in tandem the two deals would reduce the number of major
health insurers from five to three and adversely impact millions of consumers.
The proposed Aetna/Humana deal raises particular concerns about an adverse impact on the
Medicare Advantage program. More than 2.7 million seniors are enrolled in Medicare advantage
plans operated by the companies in more than 1,000 markets that would become highly
concentrated. In previous investigations the Department has viewed Medicare Advantage
markets as distinct from traditional Medicare, “[d]ue in large part to the lower out-of-pocket

The Honorable William Baer
The Honorable Sylvia Burwell
September 1, 2015
Page 2 of 20
costs and richer benefits that many Medicare Advantage plans offer seniors over traditional
Medicare.” United States v. UnitedHealth Group Inc. and Sierra Health Services, Inc.1
Yet, some of the benefits Medicare Advantage plans offer may be eroding. This erosion is not
the result of legislative changes to the program in the Affordable Care Act but is due in
significant part to the lack of robust competition among Medicare Advantage plans. A recent
Kaiser Family Foundation report described Medicare Advantage markets as “highly concentrated
among large firms.” It also cautioned that while enrollment in the Medicare Advantage program
has continued to grow and increase in virtually all states, Medicare Advantage plans “provide
less financial protection to Medicare enrollees than they have in the past ….[and] [a]verage out-
of-pocket spending limits have continued to rise.”2 The almost complete absence of competition
in Medicare Advantage markets was highlighted in a report just issued by the Commonwealth
Fund. The report studied the state of competition in every Medicare Advantage market and found
“97 percent of markets in U.S. counties are highly concentrated and therefore lacking in
significant Medicare Advantage plan competition.”3
The substantial barriers to entry in the health insurance sector make it extraordinarily unlikely
that existing firms could replicate the size and scope of the insurers involved in this proposed
transaction. This strongly suggests that the acquisition likely would serve only to exacerbate
problematic coverage and cost trends as well as produce other adverse impacts on access and
innovation. Significantly, it appears doubtful that divestitures alone would remedy the loss of
competition threatened by this acquisition.
The attached analysis details the competitive issues that the Department will consider as it
reviews this deal and the precedents that suggest it is, and should be, at risk. We understand that
the Department will work closely with the Department of Health and Human Services (HHS) in
understanding fully the potential anticompetitive impacts of the deal on the Medicare Advantage
program. We look forward to working with both agencies throughout the course of this
investigation. To that end, we will be contacting representatives of both agencies to request
meetings with top officials and staff to discuss more fully our concerns and ways in which we
can be of assistance.
For more information, you can contact me directly at [email protected] or (202) 626-2336.
1 Competitive Impact Statement, United States v. UnitedHealth Group Inc. and Sierra Health Services, Inc., No. 08-
cv-322 (D.D.C. Feb. 25, 2008), available at www.justice.gov/atr/case/us-v-unitedhealth-group-inc-and-sierra-
health-services-inc. 2 Gretchen Jacobson, Anthony Damico and Marsha Gold, Kaiser Family Foundation Issue Brief, Medicare
Advantage 2015 Spotlight: Enrollment Market Update, (June 30, 2015), available at http://kff.org/medicare/issue-
brief/medicare-advantage-2015-spotlight-enrollment-market-update/. 3 Brian Biles, Giselle Casillas, and Stuart Guterman, Competition Among Medicare’s Private Health Plans: Does It
Really Exist?, The Commonwealth Fund (August 25, 2014), available at
www.commonwealthfund.org/publications/issue-briefs/2015/aug/competition-medicare-private-plans-does-it-exist.

The Honorable William Baer
The Honorable Sylvia Burwell
September 1, 2015
Page 3 of 20
Sincerely,
/s/
Melinda Reid Hatton
Senior Vice President & General Counsel
cc: Andy Slavitt, Acting Administrator for the Centers for Medicare & Medicaid Services
Attachment

The Honorable William Baer
The Honorable Sylvia Burwell
September 1, 2015
Page 4 of 20
Detailed Analysis of the Aetna/Humana Merger
Submitted by the American Hospital Association
On behalf of the nearly 5,000 members of the American Hospital Association, we urge that the
Department of Justice’s Antitrust Division (Department) thoroughly investigate Aetna’s
proposed $37 billion acquisition of Humana.4 The transaction is likely to lessen competition
substantially in violation of Section 7 of the Clayton Act.5 The harm the transaction threatens to
consumers—and particularly to senior citizens and other vulnerable populations who depend on
Medicare Advantage programs for their health care—is large and durable. Almost one in three
Medicare beneficiaries, amounting to 16.8 million people, obtain their health care through a
Medicare Advantage plan.6 Yet, as the Kaiser Family Foundation observed in a recent report,
“Medicare Advantage enrollment … tends to be highly concentrated among a small number of
firms.”7 Humana and Aetna are leaders in this critical market. Their merger will increase already
high levels of concentration even further, making the combined company the largest Medicare
Advantage insurer in the country with one million more members than the current largest insurer,
UnitedHealthcare.8 The resulting loss of competition will harm seniors by making it considerably
more difficult for them to obtain affordable, comprehensive health care coverage.
1. The Parties
A. Aetna
Aetna is one of the nation’s largest health insurance companies, with $58 billion in revenues in
2014.9 The company is financially strong, and boasted of “strong growth” in its “core
businesses” in 2014, when it set records in both operating revenues and operating earnings.10
4 Aetna news release, available at https://news.aetna.com//aetna-to-acquire-humana/. 5 15 U.S.C. § 18. 6 Gretchen Jacobson, Anthony Damico, and Marsha Gold, Kaiser Family Foundation Issue Brief, Medicare
Advantage 2015 Spotlight: Enrollment Market Update, (June 30, 2015), Figure 1, available at
http://kff.org/medicare/issue-brief/medicare-advantage-2015-spotlight-enrollment-market-update/ (hereafter “KFF
June 2015 Issue Brief”). 7 Id. at 13. In fact, in a report released just days ago, The Commonwealth Fund found that 2,852 of the 2,933
counties studied (97 percent) have “highly concentrated” MA markets, using the definition for that term set forth in
the Department of Justice’s merger guidelines. Brian Biles, Giselle Casillas, and Stuart Guterman, Competition
Among Medicare’s Private Health Plans: Does It Really Exist?, The Commonwealth Fund (August 25, 2014),
available at www.commonwealthfund.org/publications/issue-briefs/2015/aug/competition-medicare-private-plans-
does-it-exist. 8 KFF June 2015 Issue Brief at Fig. 14; see also Anna Wilde Mathews, Liz Hoffman, Dana Mattioli, With Merger
Deal, Aetna, Humana Get Ahead of the Pack, Wall Street Journal (July 6, 2015) (the combined companies “would
have about a million more members in Medicare Advantage … than their next-closest competitor, UnitedHealth”),
available at www.wsj.com/articles/with-merger-deal-aetna-humana-get-ahead-of-the-pack-1436143581. 9 Aetna Annual Report (2014) at 2, available at http://phx.corporate-
ir.net/External.File?item=UGFyZW50SUQ9NTc0OTUyfENoaWxkSUQ9Mjc4NDQyfFR5cGU9MQ==&t=1. $55
billion are derived from Aetna’s health care businesses. 10 Id.

The Honorable William Baer
The Honorable Sylvia Burwell
September 1, 2015
Page 5 of 20
Aetna offers a full range of health care insurance products. In 2014, 23.5 million people received
medical coverage through Aetna. These included people for whom Aetna provided medical
insurance and those who received coverage through self-insured employers that contracted with
Aetna for administrative services.11 Aetna added approximately 1.4 million medical members
between 2013 and 2014, thereby growing its membership at a rate of about 6 percent.12
“One of the keys” to Aetna’s results in 2014, its chairman reported in his annual letter to
shareholders, “was the strength of our Government business, which now represents over 40
percent of Aetna’s total health premiums.”13 Premiums in the company’s government business
grew dramatically in 2014, “primarily driven by Medicare Advantage membership growth of
almost 18 percent” and by strong Medicare Supplement growth as well.14 The company has
Medicare Advantage enrollees in every state in the country, other than North Dakota.
B. Humana
Humana also is one of the largest health insurers in the U.S., with more than $48 billion in total
revenues in 2014.15 It has almost 14 million medical members.16
The company has long been a leader in Medicare products. The company offers at least one
Medicare product in every state.17 Humana today is the second largest Medicare Advantage
insurer in the U.S., just behind UnitedHealthcare.18 Fully 54 percent of Humana’s revenues
derive from Medicare Advantage products.19 Total Medicare Advantage membership increased
18 percent between 2013 and 2014.20 Humana claims that its strength in Medicare Advantage
provides it “with greater ability to expand our network of PPO and HMO providers” and so it is
well positioned to maintain and expand its strength in Medicare Advantage markets.21
2. Application of the Antitrust Laws to this Transaction
As noted in the analysis of the Anthem/Cigna transaction we provided on August 5, 2015,22
health insurance competition is vital if the promise of increased access to affordable health
insurance coverage, embodied in the Affordable Care Act (ACA), is to be realized. The
11 Aetna Annual Report (2014) at 10. 12 Id. 13 Mark T. Bertolini, Chairman and CEO, Letter to shareholders (April 2015), available at http://phx.corporate-
ir.net/External.File?item=UGFyZW50SUQ9NTc0OTUyfENoaWxkSUQ9Mjc4NDQyfFR5cGU9MQ==&t=1. 14 Id. 15 Humana 10-K for YE 2014 (attached to 2014 Annual Report), at 81, available at http://phx.corporate-
ir.net/External.File?item=UGFyZW50SUQ9NTcyNjgzfENoaWxkSUQ9Mjc0NTQ3fFR5cGU9MQ==&t=1. 16 Id. at 12; see also id. at 38. 17 Id. at 5. 18 KFF June 2015 Issue Brief at Fig. 14. 19 Humana 10-K for YE 2014 (attached to 2014 Annual Report), supra, at 5. 20 2014 Annual Report, supra, at 3. 21 Humana 10-K for YE 2014 (attached to 2014 Annual Report), supra, at 5. 22 Letter from Melinda Reid Hatton to William Baer, at 7 (August 5, 2015), available at
http://www.aha.org/advocacy-issues/letter/2015/150805-let-acquisitions.pdf.

The Honorable William Baer
The Honorable Sylvia Burwell
September 1, 2015
Page 6 of 20
Department, which has reviewed carefully every health insurance merger in recent years, has
been adamant that competition must be preserved among insurers. The Acting Assistant Attorney
General in charge of the Antitrust Division remarked three years ago that “the division has
brought a number of enforcement actions against health insurance mergers” as part of its
“commitment to carefully review mergers in the health insurance industry and challenge those
mergers that may substantially lessen competition in properly defined markets.”23
To fulfill this commitment to protect competition in health insurance markets, the Department
has filed many actions against insurers seeking to merge or otherwise act anticompetitively.24
Significantly, in two of the cases filed over the last several years involving mergers of health
insurers, the Department recognized the particular importance of preserving competition in the
Medicare Advantage market:
In 2008, after UnitedHealth proposed to acquire Sierra Health Services, the Department
sued to protect competition in the provision of Medicare Advantage plans in Las Vegas.25
The Department noted Congress created Medicare Advantage “as a private market
alternative” to the traditional Medicare program. “In establishing the Medicare
Advantage program, Congress intended that vigorous competition among private
Medicare Advantage insurers would lead insurers to offer seniors richer and more
affordable benefits than traditional Medicare, provide a wider array of health-insurance
choices, and be more responsive to the demands of seniors.” The Department alleged the
proposed merger would end all competition between UnitedHealth and Sierra, thereby
“eliminating the pressure that these close competitors place on each other to maintain
attractive benefits, lower prices, and high-quality health care.”26 The Department settled
the complaint through entry of a consent decree that required the merged company to
preserve competition in the market for Medicare Advantage in Las Vegas by divesting
individual Medicare Advantage lives in the two counties encompassing that city.27
23 Sharis A. Pozen, Acting Assistant Att’y Gen., Dep’t of Justice Antitrust Div., Competition and Health Care: A
Prescription for High-Quality, Affordable Care (Mar. 19, 2012), at 4, 6, available at
www.justice.gov/atr/speech/competition-and-health-care-prescription-high-quality-affordable-care. Less than two
year earlier, Christine Varney, then Assistant Attorney General of the DOJ’s Antitrust Division, made a similar point
in remarks given to a joint American Bar Association/American Health Lawyers Association
Antitrust in Healthcare Conference, (May 24, 2010), available at http://www.justice.gov/atr/speech/antitrust-and-
healthcare. 24 Several cases brought by the Department to protect competition in health insurance markets are discussed in the
Pozen speech, supra n.8. Others are identified in the AHA’s August 5 letter, supra n.6, at 7 n.19. 25 Complaint, United States v. UnitedHealth Group Inc. and Sierra Health Services, Inc., No. 08-cv-322 (D.D.C.
Feb. 25, 2008), available at www.justice.gov/atr/case/us-v-unitedhealth-group-inc-and-sierra-health-services-inc. 26 Id. at ¶ 3. 27 Final Judgment United States v. UnitedHealth Group Inc. and Sierra Health Services, Inc., No. 08-cv-322
(D.D.C. Sept. 24, 2008), available at www.justice.gov/atr/case/us-v-unitedhealth-group-inc-and-sierra-health-
services-inc; see also Competitive Impact Statement (Feb. 25, 2008) (available at same website).

The Honorable William Baer
The Honorable Sylvia Burwell
September 1, 2015
Page 7 of 20
In 2012, the Department sued to block the proposed acquisition by Humana Inc. of
Arcadian Management Services, Inc.28 The Department charged the proposed acquisition
would “significantly lessen competition among Medicare Advantage plans and eliminate
substantial head-to-head competition between Humana and Arcadian in the provision of
such plans” in 45 relevant geographic markets.29 The competition between the two
companies, the Department noted, “has significantly benefited thousands of seniors” who
look to Medicare Advantage plans to obtain “greater benefits than those available under
traditional Medicare.”30 The Department resolved the complaint when the merging
companies agreed to divest individual Medicare Advantage business in each of the
relevant geographic markets.31 Without the divestitures, the Department warned, “[t]he
loss of competition from the acquisition likely would result in higher premiums and
reduced benefits and services in these markets.”32
A. Relevant Product Market
1. The Medicare Advantage Program
a. Medicare Advantage Before The Passage Of The ACA
The Department demonstrated a thorough understanding of the Medicare Advantage market in
the complaints and competitive impact statements filed in the UnitedHealth/Sierra and
Humana/Arcadian transactions.33 As the Department noted there, in the traditional, government-
operated Medicare program, a beneficiary generally receives coverage for hospital services under
Part A of the program for free if he or she worked and paid Medicare taxes. A beneficiary may
elect to receive coverage for physician and other outpatient services under Part B upon payment
of a premium. To receive prescription drug coverage a beneficiary enrolled in traditional
Medicare program must enroll in a Medicare prescription drug plan under Medicare’s Part D for
an additional monthly premium.
28 Complaint, United States v. Humana Inc. and Arcadian Management Services, Inc., No. 12-cv-464 (D.D.C.,
March 27, 2012), available at www.justice.gov/atr/case/us-v-humana-inc-and-arcadian-management-services-inc. 29 Id. at ¶ 4. 30 Id. 31 Final Judgment, United States v. Humana Inc. and Arcadian Management Services, Inc., No. 12-cv-464 (D.D.C.,
Sept. 21, 2012), available at www.justice.gov/atr/case/us-v-humana-inc-and-arcadian-management-services-inc.;
see also Competitive Impact Statement (March 27, 2012) (available at same website). 32 Competitive Impact Statement, United States v. Humana, supra, at 1. 33 United States v. UnitedHealth Group Inc. and Sierra Health Services, Inc., No. 08-cv-322, available at
www.justice.gov/atr/case/us-v-unitedhealth-group-inc-and-sierra-health-services-inc.; United States v. Humana Inc.
and Arcadian Management Services, Inc., No. 12-cv-464, available at www.justice.gov/atr/case/us-v-humana-inc-
and-arcadian-management-services-inc.

The Honorable William Baer
The Honorable Sylvia Burwell
September 1, 2015
Page 8 of 20
The Part B premium for most beneficiaries in 2015 is $104.90 per month.34 The cost of a stand-
alone Part D plan varies widely, but in 2015 averages about $38.80 per month.35 Assuming a
beneficiary obtains covered medical services, he or she may incur substantial additional costs:
The deductible for hospitalization under Medicare Part A is $1,260 in 2015. If a hospital
stay lasts longer than 60 days, prescribed coinsurance amounts must be paid by the
beneficiary.36
The deductible for Medicare Part B this year is $147.37
o Once beneficiaries meet the deductible, they typically must pay 20 percent of the
Medicare allowed amounts.
There is no annual limit on out-of-pocket costs incurred under either Part A or Part B. “If
beneficiaries want to limit potentially catastrophic out-of-pocket costs, they need to
purchase a separate Medicare Supplement plan.”38
Medicare Advantage plans must provide all Medicare-covered services (Parts A and B).
Beneficiaries pay a premium established by the plan and are responsible as well for the Part B
premium. From the point of view of beneficiaries, there are many differences between Medicare
Advantage and traditional Medicare. Some of the critically important differences include:
Additional benefits. Medicare Advantage plans may (and usually do) provide benefits
not provided by Medicare. These additional services often include dental and vision
benefits, and may include hearing and health and wellness programs.39
Prescription drug coverage. The overwhelming majority of Medicare Advantage
enrollees (88 percent) participate in a plan (an MA-PD) that includes a prescription drug
benefit.40
34 Medicare.gov, Medicare 2015 costs at a glance, available at www.medicare.gov/your-medicare-costs/costs-at-a-
glance/costs-at-glance.html. Beneficiaries with modified adjusted gross incomes above $85,000 for individuals and
$170,000 for joint filers are charged higher amounts. Id. 35 See Jack Hoadley et al., Medicare Part D: A First Look at Plan Offerings in 2015, Kaiser Family Foundation (Oct.
10, 2014), available at http://kff.org/report-section/medicare-part-d-a-first-look-at-plan-offerings-in-2015-key-
findings/; see also Medicare.gov, Monthly Premium for Drug Plans, www.medicare.gov/part-d/costs/part-d-
costs.html. 36 These can be substantial: $315 per day for days 61-90 and $630 after that for a prescribed number of “lifetime
reserve days” after which the beneficiary must pay the entire amount incurred. Medicare 2015 costs at a glance,
supra. 37 Medicare 2015 costs at a glance, supra. 38 Competitive Impact Statement, United States v. UnitedHealth, supra, at 5. 39 See generally Medicare.gov, Medicare Advantage plans cover all Medicare services, available at
www.medicare.gov/what-medicare-covers/medicare-health-plans/medicare-advantage-plans-cover-all-medicare-
services.html. 40 KFF June 2015 Issue Brief at 7.

The Honorable William Baer
The Honorable Sylvia Burwell
September 1, 2015
Page 9 of 20
o The standard Part D benefit design has a $320 deductible and requires 25 percent
coinsurance up to $2,960 in drug costs.41 At that expenditure level, a “donut
hole” opens: beneficiaries are responsible for 45 percent of the cost of the drug
(in 2015) until their out-of-pocket hits $4,700, after which they pay 5 percent of
their drug costs.42
o Enrollees in MA-PDs generally have better coverage than do those who must buy
a Part D plan directly: fully 58 percent of MA-PD enrollees participate in plans
that have no Part D deductible.43 Such no-deductible drug plans are more
common in Medicare Advantage than in Part D plans available to traditional
Medicare enrollees.44 And, almost half (45 percent) of MA-PD enrollees are in
plans that close some of the “donut hole” in Part D’s drug coverage.45
Premium cost. The average enrollee in a MA-PD plan in 2015 pays a monthly plan
premium of about $38.46 Medicare Advantage plans may use savings to reduce—
sometimes to zero—the premiums they charge for coverage. In 2015, 78 percent of all
MA-PD enrollees had a choice of at least one plan that charged nothing for Medicare
Advantage coverage, leaving enrollees responsible only for their Part B premium.47
Almost one-half of all MA-PD enrollees participate in these “zero-premium” plans.48
Some plans go even further, and use their savings to reduce the Part B premium.49
Out-of-pocket limits. Medicare Advantage plans must limit out-of-pocket expenditures
for Part A and Part B services.50 The out-of-pocket limit in 2015 can be no greater than
$6,700 per Medicare Advantage enrollee annually. In fact, the average out-of-pocket
limit in 2015 is less: $5,041 per enrollee.51
Medicare Advantage plans are sold predominantly to individuals and less frequently to groups.52
Almost 64 percent of Medicare Advantage enrollees participate in a health maintenance
41 KFF June 2015 Issue Brief at 11. 42 Id. 43 Id. 44 Gretchen Jacobson, Anthony Damico, Tricia Neuman, and Marsha Gold, Kaiser Family Foundation Issue Brief,
Medicare Advantage 2015 Data Spotlight: Overview of Plan Changes, (Dec. 10, 2014), at 11, available at
http://files.kff.org/attachment/data-spotlight-medicare-advantage-2015-data-spotlight-overview-of-plan-changes 45 KFF June 2015 Issue Brief at 11. 46 KFF June 2015 Issue Brief at 8. 47 Id. at 8. 48 Id. 49 Medicare Payment Advisory Commission (“MedPAC”), Report to the Congress: Medicare Payment Policy,
(March 2015), Ch. 13, available at www.medpac.gov/documents/reports/chapter-13-the-medicare-advantage-
program-status-report-(march-2015-report).pdf?sfvrsn=0 . 50 Id. 51 KFF June 2015 Issue Brief at 10. 52 According to MedPAC, as of February 2015, about 3 million enrollees were in employer group plans, or about 19
percent of all Medicare Advantage enrollees. About 2 million were in special needs plans. MedPAC, A Data Book,

The Honorable William Baer
The Honorable Sylvia Burwell
September 1, 2015
Page 10 of 20
organization (HMO).53 Preferred provider organizations (PPOs) provide coverage to 31 percent
of the enrollees. Just 5 percent of all Medicare Advantage enrollees obtain services through
private fee-for-service plans,54 and that proportion has “fallen precipitously” since 2008.55
Consistent with the usual way in which HMOs and PPOs operate, enrollees in these plans usually
obtain care from a more limited network than offered by traditional Medicare, and these plans
(and in particular, the HMOs) typically manage the care provided.56
b. Changes To The Medicare Advantage Program Made By The ACA
An insurer wishing to offer a Medicare Advantage plan in a county must submit a bid to the
Centers for Medicare & Medicaid Services (CMS). The bid covers the insurer’s projected cost to
provide required Medicare benefits under Part A and Part B to a beneficiary. CMS compares the
bid (plus an amount for profit) to a local payment benchmark intended to reflect, in part, the cost
of providing care through the traditional Medicare system.57 Through 2011, Medicare retained 25
percent of the amount (if any) by which the benchmark exceeded the bid.58 The balance (75
percent) was rebated to the bidder and used to provide supplemental benefits or lower premiums
(including Part B premiums).59 The Department has recognized that this structure “encourages
insurers to compete against each other to attract Medicare beneficiaries by providing low prices
and more benefits.”60
Before the ACA, Medicare Advantage plans were being paid, on average, 114 percent of
Medicare fee-for-service costs per enrollee.61 The ACA seeks to change this structure so as to
reduce, if not entirely eliminate, the payment difference per enrollee. The ACA does this in two
ways: first, it gradually reduces the benchmarks. Second, it reduces the amount rebated from 75
percent of the difference between a bid and the benchmark to an amount ranging from 50 percent
to 70 percent (depending on plan quality).62
Health Care Spending and the Medicare Program, Ch. 9 (June 2015) available at
www.medpac.gov/documents/data-book/jun15databooksec9.pdf?sfvrsn=0. 53 In 2015, 64 percent (10.7 million) of the 16.8 million Medicare Advantage enrollees were in HMO plans. KFF
June 2015 Issue Brief at 3. 54 Id. Most of the PPO enrollees (4 million) participate in local (i.e., countywide) PPOs; a much smaller number
(1.2 million) enrollees participate in regional PPOs. Id. 55 Id. 56 MedPAC, Report to the Congress, supra, Ch. 13, at 319. 57 See Competitive Impact Statement, United States v. Humana, supra, at 4. 58 Id. 59 Id. 60 See Competitive Impact Statement, United States v. UnitedHealth, supra, at 6; see also Competitive Impact
Statement, United States v. Humana, supra, at 4-5 (the rebate causes Medicare Advantage plans to “compete for
enrollment by lowering costs, lowering premiums, increasing benefits, and improving performance”). 61 This was the figure in 2009. See U.S. Department of Health and Human Services, Office of the Assistant
Secretary for Planning and Evaluation, The Medicare Advantage Program in 2014, (April 7, 2014) at 9, available at
http://aspe.hhs.gov/sites/default/files/pdf/76846/ib_MedicareAdvantage.pdf. 62 MedPAC, Medicare Advantage Program Payment (rev’d Oct. 2014), available at
www.medpac.gov/documents/payment-basics/medicare-advantage-program-payment-system-14.pdf?sfvrsn=0.

The Honorable William Baer
The Honorable Sylvia Burwell
September 1, 2015
Page 11 of 20
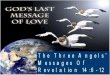
Not surprisingly, before the ACA took effect the Congressional Budget Office (CBO) projected
that these changes would reduce enrollment.63 Those predictions were wrong: enrollment in
Medicare Advantage plans has increased, not decreased, since passage of the ACA. A table
included in a recent issue brief published by the Kaiser Family Foundation shows this:64
This enrollment increase has occurred at the same time that CMS has ratcheted down the
payments to Medicare Advantage plans from the average of 114 percent of the amount expended
per fee-for-service enrollee in 2009,65 to just 102 percent in 2015.66 And, while total Medicare
Advantage enrollment has been growing quickly, and is projected to continue to grow to 25
million over the next 10 years,67 the number of Medicare Advantage plans is declining.68
2. Medicare Advantage Constitutes A Separate Relevant Product Market
In each of the two recent cases in which the Department focused on the market for Medicare
Advantage plans, it identified Medicare Advantage plans sold to individuals as the relevant
product market. As the Department stated in the UnitedHealth/Sierra merger, Medicare
63 CBO estimated 35 percent less enrollment in 2019 than otherwise would have been the case—about 4.8 million
fewer enrollees. See CBO, Comparison of Projected Enrollment in Medicare Advantage Plans and Subsidies for
Extra Benefits Not Covered by Medicare, at 2, available at www.cbo.gov/sites/default/files/111th-congress-2009-
2010/costestimate/macomparisons.pdf 64 KFF June 2015 Issue Brief at 2 (Fig. 1). 65 Kaiser Family Foundation, The Role of Medicare Advantage, Slide 4 (Ex. 3), available in
http://kff.org/slideshow/the-role-of-medicare-advantage/. 66 MedPAC, Report to the Congress: Medicare Payment Policy, at 325 (March 2015) available at
www.medpac.gov/documents/reports/chapter-13-the-medicare-advantage-program-status-report-(march-2015-
report).pdf?sfvrsn=0 (Table 13-4). 67 The Role of Medicare Advantage, supra, Slide 2 (Ex. 1). 68 Gretchen Jacobson, Tricia Neuman, and Anthony Damico, Kaiser Family Foundation Issue Brief, What’s In and
What’s Out? Medicare Advantage Market Entries and Exits for 2015 (Oct. 23, 2014) at 2, available at
http://files.kff.org/attachment/medicare-advantage-market-entries-and-exits-for-2015-issue-brief/.

The Honorable William Baer
The Honorable Sylvia Burwell
September 1, 2015
Page 12 of 20
Advantage plans “offer lower co-payments, lower co-insurance, caps on total yearly out-of-
pocket spending, prescription drug coverage, vision coverage, health club memberships, and
other benefits that traditional Medicare does not cover.”69 Similarly, in the Humana/Arcadian
merger, the Department found Medicare Advantage plans:
Offer substantially richer benefits at lower costs to enrollees than
traditional Medicare does with or without a Medicare Supplement
or Medicare prescription drug plan, including lower copayments,
lower coinsurance, caps on total yearly out-of-pocket costs,
prescription drug coverage, and supplemental benefits that
traditional Medicare does not cover, such as dental and vision
coverage, and health club memberships.70
The fact that Medicare Advantage plans combine in one product benefits that an enrollee in
traditional Medicare must assemble from a variety of sources is yet another significant feature
that distinguishes these plans from traditional Medicare. As the Department observed in the
Humana/Arcadian merger, “Seniors enrolled in Medicare Advantage plans also often value that
they can receive all of these benefits through a single plan and that Medicare Advantage plans
manage care in ways that traditional Medicare does not.”71 One-stop shopping is of real value in
many markets,72 but particularly here, where consumers are older, the products they must
compare differ widely, and pricing comparisons are extremely difficult, not least because
consumers frequently do not know what services they will require in the year ahead.73 The cap
on financial risk similarly distinguishes Medicare Advantage products from traditional Medicare.
The sum of these features translates into a strong preference by many seniors for Medicare
Advantage plans. As the Department concluded in the UnitedHealth/Sierra merger:
Due in large part to the lower out-of-pocket costs and richer
benefits that many Medicare Advantage plans offer seniors over
traditional Medicare, seniors in the Las Vegas area would not
likely switch away from Medicare Advantage plans to traditional
69 Competitive Impact Statement, United States v. UnitedHealth, supra, at 7; see also Competitive Impact
Statement, United States v. Humana, supra, at 4. 70 Competitive Impact Statement, United States v. Humana, supra, at 5. 71 Id. 72 See ABA Section of Antitrust Law, Antitrust Law Developments (7th ed. 2012) at 595-99 (broad recognition of
cluster markets in industries including hospital services, financial services, office supply superstores, and others). 73 See generally Gretchen Jacobson, Christina Swoope, Michael Perry, Mary Slosar, How are seniors choosing and
changing health insurance plans?, Henry J. Kaiser Family Foundation (May 2014) at 12 (“Seniors say they have
tried to compare the costs, coverage, and provider networks of plans, but find it frustrating and confusing”),
available at https://kaiserfamilyfoundation.files.wordpress.com/2014/05/8589-how-are-seniors-choosing-and-
changing-health-insurance-plans.pdf.

The Honorable William Baer
The Honorable Sylvia Burwell
September 1, 2015
Page 13 of 20
Medicare in sufficient numbers to make an anticompetitive price
increase or reduction in quality unprofitable.74
Based on the same differentiating factors, the Department similarly concluded in the
Humana/Arcadian merger that individual Medicare Advantage plans constituted a relevant
product market.75
Despite the changes to the Medicare Advantage program made by the ACA, the elements that
supported the Department’s conclusions in 2008 and 2012 that Medicare Advantage plans
constitute a distinct relevant product market still are in place today: Medicare Advantage plans
continue to offer richer benefits at lower costs than does traditional Medicare, even when the
latter is supplemented by Medigap policies and Part D plans.76 Moreover, the ACA did nothing
to reduce the complexity that faces a senior as he or she attempts to weave together coverage for
inpatient care, outpatient care, physician care, prescription drugs, vision care, dental care, and
other necessary health care, from the various items on the traditional Medicare menu including
Part A, Part B, Part D, and Medigap and other supplemental insurance policies. To further
complicate matters, seniors simultaneously must attempt to select coverage in a way that does
not leave the senior exposed to large deductibles, high coinsurance on Part B, and no out-of-
pocket limits for those unfortunate enough to incur substantial heath care expenses in a given
year.
Not only has passage of the ACA not weakened the argument that Medicare Advantage plans
constitute a separate relevant product market, subsequent events have strengthened the argument.
As noted above, costs for the average Medicare Advantage enrollee are being brought in line
with costs for the average traditional Medicare enrollee. The CBO predicted that with fewer
dollars available, relative to traditional Medicare, Medicare Advantage plans could expect
enrollment to decline as seniors opted out of Medicare Advantage and into traditional
Medicare.77 But as this differential has narrowed, enrollment—instead of declining—has
grown.78
It appears the vast majority of individuals enrolled in Medicare Advantage plans have stayed in
Medicare Advantage plans, even as the dollars expended on them relative to expenditures on
74 Competitive Impact Statement, United States v. UnitedHealth, supra, at 4-5. 75 Competitive Impact Statement, United States v. Humana, supra, at 6 (“a small but significant increase in
Medicare Advantage plan premiums or reduction in benefits is unlikely to cause a sufficient number of seniors in the
relevant geographic markets to switch to traditional Medicare such that the price increase or reduction in benefits
would be unprofitable”). 76 See generally KFF June 2015 Issue Brief at 8-12. 77 CBO, Comparison of Projected Enrollment in Medicare Advantage Plans and Subsidies; see generally KFF June
2015 Issue Brief at 1; Gretchen A. Jacobson, Patricia Neuman, Anthony Damico, At Least Half Of New Medicare
Advantage Enrollees Had Switched From Traditional Medicare During 2006–11, 34 Health Affairs 48, 49 (Jan.
2015), available at http://content.healthaffairs.org/content/34/1/48.full.pdf. 78 Id.

The Honorable William Baer
The Honorable Sylvia Burwell
September 1, 2015
Page 14 of 20
traditional Medicare beneficiaries have declined by about 10 percent.79 One study confirmed that
in any given year the odds of seniors switching between Medicare Advantage and traditional
Medicare are small (and fewer switch from Medicare Advantage to the traditional program than
vice versa).80 Significantly, seniors are far less likely to switch from Medicare Advantage to
traditional Medicare when other Medicare Advantage alternatives are available.81 “And the odds
of switching from Medicare Advantage to traditional Medicare were higher in counties with
fewer plans, less experienced plans, or lower Medicare Advantage penetration rates.”82
These data suggest strongly that Medicare Advantage enrollees prefer a Medicare Advantage
product to traditional Medicare. So long as other Medicare Advantage alternatives are available,
they generally do not switch to traditional Medicare. Similarly, in each of the
UnitedHealth/Sierra and Humana/Arcadian mergers, the Department found Medicare Advantage
constitutes a relevant product market separate from traditional Medicare because seniors would
not switch away from Medicare Advantage to traditional Medicare in sufficient numbers to
defeat a small but significant price increase or quality decrease in Medicare Advantage.83 The
same is true today. The only difference is that the evidence that such switching will not occur is
far stronger now than it was in 2008 or 2012.
B. Relevant Geographic Market
Consistent with the Department’s practice in the UnitedHealth/Sierra84 and Humana/Arcadian85
mergers, the relevant geographic markets in which to evaluate the proposed Aetna/Humana
merger are at the county (or parish) level. CMS approves Medicare Advantage plans on a
county-by-county basis,86 and the vast majority of seniors may only enroll in a Medicare
Advantage plan in the county in which they live.87
79 As discussed earlier, in 2009, on average, the government expended 14 percent more on Medicare Advantage
enrollees than it did on traditional Medicare beneficiaries. By 2015, that average had shrunk to 102 percent – a
reduction in the differential of 10.5 percent. 80 Gretchen A. Jacobson, Patricia Neuman, Anthony Damico, At Least Half Of New Medicare Advantage Enrollees
Had Switched From Traditional Medicare During 2006–11, 34 Health Affairs 48, 51 (Jan. 2015), available at
http://content.healthaffairs.org/content/34/1/48.full.pdf. 81 Id. at 53. 82 Id. 83 Competitive Impact Statement, United States v. UnitedHealth, supra, at 7; Competitive Impact Statement, United
States v. Humana, supra, at 6. 84 Competitive Impact Statement, United States v. UnitedHealth, supra, at 6. 85 Competitive Impact Statement, United States v. Humana, supra, at 7. 86 CMS examines network adequacy on a county-by-county basis. See “CY2015 MA HSD Provider and Facility
Specialties and Network Adequacy Criteria Guidance,” available at www.cms.gov/Medicare/Medicare-
Advantage/MedicareAdvantageApps/Downloads/CY2015_MA_HSD_Network_Criteria_Guidance.pdf 87 Almost 88 percent of all Medicare Advantage enrollment is in HMOs and local PPOs. See KFF June 2015 Issue
Brief at 3. Seniors enroll in these at the county level. Regional PPOs (just 7 percent of all enrollment) may provide
coverage on a regional basis, but their beneficiaries can enroll in a plan only in the service area in which they live.
CMS, Medicare Managed Care Manual, Ch. 2, Medicare Advantage Enrollment and Disenrollment, § 20.2,
www.cms.gov/Medicare/Health-Plans/HealthPlansGenInfo/downloads/mc86c02.pdf .

The Honorable William Baer
The Honorable Sylvia Burwell
September 1, 2015
Page 15 of 20
C. Competitive Effects
Under the Merger Guidelines, a “highly concentrated market” is one where the Herfindahl-
Hirschman Index (HHI) is 2500 or more.88 “Mergers resulting in highly concentrated markets
that involve an increase in the HHI of between 100 points and 200 points potentially raise
significant competitive concerns and often warrant scrutiny. Mergers resulting in highly
concentrated markets that involve an increase in the HHI of more than 200 points will be
presumed to be likely to enhance market power.”89 Consistent with this approach, our analysis
identifies counties where (1) both Aetna and Humana have Medicare Advantage membership,
(2) the post-merger HHI is at least 2,500, and (3) the merger produces an increase of at least 100
points.
The table below shows the substantial impact the Aetna acquisition of Humana would have on
Medicare Advantage competition across the nation.90 In 1,083 markets, the transaction would
increase the HHI by at least 100 points and the post-merger HHI will top 2,500. In 924 of these
markets, the transaction would increase the HHI by more than 200 points.
Table 1. Counties in which the Post-Merger HHI Exceeds 2,500
and Change in HHI Exceeds 100 for Medicare Advantage Lives
HHI Delta Screen
>200 >100
Number of Counties 924 1,083
Aetna Membership 784,167 842,864
Humana Membership 1,612,941 1,878,082
Total Aetna/Humana
membership
Membership to Divest
(smaller plan)
2,397,108
581,050
2,720,946
610,278
Source: Centers for Medicare & Medicaid Services, June 2015 MA Enrollment by Contract/Plan/State/County.91
88 Horizontal Merger Guidelines, U.S. Department of Justice and Federal Trade Commission (August 19, 2010) at §
5.3, available at www.justice.gov/atr/horizontal-merger-guidelines-08192010. 89 Id. 90 We exclude Special Needs Plans, as the Department did in both UnitedHealth/Sierra and Humana/Arcadian. 91 Available at www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-
Reports/MCRAdvPartDEnrolData/Monthly-Enrollment-by-Contract-Plan-State-County-Items/Monthly-Enrollment-
by-CPSC-2015-06.html.

The Honorable William Baer
The Honorable Sylvia Burwell
September 1, 2015
Page 16 of 20
Aetna and Humana today provide health care coverage through Medicare Advantage for more
than 4.3 million people.92 More than 2.7 million of these seniors—almost two-thirds of both
companies’ enrollees—live in relevant geographic markets that are or will be highly
concentrated and in which the HHI increase will be at least 100 points. The proposed
acquisition threatens serious and widespread competitive harm.
The deal will not just eliminate current competition between Humana and Aetna, it will eliminate
future competition between them. Humana is the second largest insurer of Medicare Advantage
lives in the country.93 Aetna is the fourth largest.94 Aetna has promised investors it will continue
to grow its Medicare Advantage business, as this chart from an Aetna investor conference held in
December 2014 makes clear:95
The merger would eliminate the possibility of competition between Aetna and Humana in
markets which Aetna plans to enter. The Department should study carefully Aetna’s (and
Humana’s) expansion plans to determine the degree to which both current and future competition
will be sacrificed should this deal be completed.
92 CMS, June 2015 MA Enrollment by Contract/Plan/State/County, available at www.cms.gov/Research-Statistics-
Data-and-Systems/Statistics-Trends-and-Reports/MCRAdvPartDEnrolData/Monthly-Enrollment-by-Contract-Plan-
State-County-Items/Monthly-Enrollment-by-CPSC-2015-06.html. 93 Anna Wilde Mathews, Liz Hoffman, Dana Mattioli, With Merger Deal, Aetna, Humana Get Ahead of the Pack,
Wall Street Journal (July 6, 2015), available at www.wsj.com/articles/with-merger-deal-aetna-humana-get-ahead-
of-the-pack-1436143581 94 KFF June 2015 Issue Brief at Fig. 14. (The BCBS figure shown there adds together shares for the different Blue
Cross and Blue Shield affiliates in the U.S.) 95 Aetna, 2014 Investor Conference (Dec. 11., 2014), at slide 72 available at http://phx.corporate-
ir.net/External.File?item=UGFyZW50SUQ9NTYzNTQ0fENoaWxkSUQ9MjYzODg0fFR5cGU9MQ==&t=1; see
also Aetna, 2013 Investor Conference (Dec. 12., 2013) at slide 107 (“Medicare Has Been a Growth Driver for
Aetna”), available at www.aetna.com/investors-aetna/assets/documents/2013%20Investor%20Conference/2013-
Investor-Conference-Presentation.pdf.

The Honorable William Baer
The Honorable Sylvia Burwell
September 1, 2015
Page 17 of 20
D. Aetna/Humana Will Not Show Efficiencies Overcome The Merger’s Anticompetitive
Effects
1. The Aggregation of Buyer Power Is Not An Efficiency And Will Harm Seniors
Aetna and Humana may argue that by merging they will obtain market power with which they
can force hospitals and physicians to further lower their prices to the benefit of consumers.96
The argument lacks merit.
Courts and commentators distinguish between monopsony power and countervailing power.97
Monopsony power is the mirror image of monopoly power: a single buyer has monopsony power
when it faces off against competitive suppliers who lack market power.98 (And a small group of
buyers in the same situation have oligopsoly power.)99 A monopsonist maximizes profits by
depressing prices below competitive levels. Suppliers react by reducing output. As the
Department recognized in a prior acquisition by Aetna, the exercise of monopsony power by an
insurer harms consumers because it depresses the supply of providers (and potentially of other
health care resources) below competitive levels.100 Countervailing power is the use of buyer
power against a supplier with market power. Some argue countervailing power may cause a
supplier with market power to lower its price closer to the competitive level.101 But, as one law
professor who has written extensively on buyer power notes, “the exercise of countervailing
power is not always procompetitive.”102 As this commentator points out:
[A] merger that is large enough to increase buyer power materially
may harm competition in multiple ways. First, it may create
monopsony power and enable the merged firm to exploit small,
relatively powerless providers. Second, the merger may create
downstream market power, which could offset the desirable effects
of countervailing power and raise premiums to consumers. Finally,
96 Several commentators have made this argument. See, e.g., Victor Fuchs, Peter Lee, A Health Side of Insurer
Mega-Mergers, Wall Street Journal (Aug. 26, 2015), available at www.wsj.com/articles/a-healthy-side-of-insurer-
mega-mergers-1440628597. Whether Aetna would make this argument is less clear: the company’s CEO is on
record saying so long as a market evolves toward capitation and away from fee-for-service, “a [provider] monopoly
or oligopoly in a marketplace is a good thing.” Aetna, 2014 Investor Conference (Dec. 11, 2014) (statement made on
audio portion at slide 35) available at http://edge.media-server.com/m/p/eebugf92/lan/en. 97 See, e.g., John B. Kirkwood, Powerful Buyers and Merger Enforcement, 92 B.U. L. REV. 1485, 1493-1512 (2012). 98 See Improving Health Care: A Dose of Competition, Department of Justice & Federal Trade Commission,
Improving Health Care: A Dose of Competition 29 (July 2004), Ch. 6 at 13, available at
www.justice.gov/sites/default/files/atr/legacy/2006/04/27/204694.pdf. 99 Id. at n.84. 100 Complaint, United States v. Aetna Inc. and The Prudential Insurance Co., No. 3-99CV 1398-H, at ¶¶ 30-33 (June
21, 1999), Competitive Impact Statement at 9-12 (July 16, 1999), available at www.justice.gov/atr/case/us-v-aetna-
and-prudential-insurance-company; see also United States v. UnitedHealth Group, Inc., and PacifiCare Health
Systems, Inc., Civil Action No. 1:05CV02436, Complaint ¶ 5 (Dec. 20, 2005, D.D.C. 2005), available at
http://www.justice.gov/atr/case/us-v-unitedhealth-group-inc-and-pacificare-health-systems-inc. 101 Dose of Competition, Ch. 6 at 14, n.86. 102 John B. Kirkwood, Buyer Power and Healthcare Prices, Wash. L. Rev. (forthcoming) at 10 n.32.

The Honorable William Baer
The Honorable Sylvia Burwell
September 1, 2015
Page 18 of 20
the merger might create countervailing power but the merged firm
might exercise it in anticompetitive ways, harming consumers or
small providers. Because a merger of large insurance companies
is likely to produce at least one of these anticompetitive
outcomes, allowing major insurers to combine does not appear to
be a promising way of lowering healthcare prices.103
This conclusion simply reinforces the wisdom of the position taken by the antitrust enforcement
agencies a decade ago, when they published their seminal study on competition in health care:
“Countervailing power should not be considered an effective response to disparities in
bargaining power between payors and providers.”104
2. Entry
As observed in our analysis of the Anthem/Cigna merger, any argument that entry is sufficient to
overcome the otherwise anticompetitive effects of a health insurer merger should be considered
(in the words of a former Acting Assistant Attorney General in charge of the Division) “carefully
and with some skepticism.”105
The Department recognized in the Michigan MFN case that effective entry into a commercial
health insurance market requires that “a health insurer contract with broad provider networks and
obtain hospital prices and discounts at least comparable to the market’s leading incumbents.”106
The same applies to an insurer seeking to enter a Medicare Advantage market. In fact, even if the
103 Id. at 7-8 (emphasis added and footnotes omitted). 104 Dose of Competition, Executive Summary at 27 (8th Observation). Although this was discussed primarily in the
context of provider pleas that they be allowed to exercise countervailing power in negotiations with insurers, the
logic applies equally against an assertion by insurers that they be allowed to merge to obtain power to use against
providers. In fact, the enforcement agencies have responded to the argument that providers ought to have
countervailing power to offset situations where insurers gain monopsony power by asserting “antitrust enforcement
to prevent the unlawful acquisition … of monopsony power by insurers is a better solution than allowing providers
to exercise countervailing power.” Id. Ch. 3 at 21. 105 Pozen at 7. See also remarks of Christine Varney, then Assistant Attorney General of the DOJ’s Antitrust
Division, at a joint American Bar Association/American Health Lawyers Association
Antitrust in Healthcare Conference, (May 24, 2010), available at http://www.justice.gov/atr/speech/antitrust-and-
healthcare. 106 Complaint, U.S. v. Blue Cross and Blue Shield of Michigan, No. 2:10-cv-14155-DPH-MKM (Oct. 18, 2010) at ¶
35, available at www.justice.gov/atr/case/us-and-state-michigan-v-blue-cross-blue-shield-michigan. The
Department also noted that entry was difficult (in fact, efforts to enter were demonstrably unsuccessful) in the
complaint filed against a payer and five hospitals for colluding to lessen competition in the health insurance market
in Montana. U.S. and State of Montana v. Blue Cross and Blue Shield of Montana, et. al., Case No.1:11-cv-00123-
RFC (Nov. 8, 2011), available at www.justice.gov/atr/case/us-and-state-montana-v-blue-cross-blue-shield-montana-
inc-et-al. See also United States v. Aetna Inc. and Prudential Insurance Co. of Am., Complaint at ¶ 23 (finding that it
was unlikely that new companies would enter or that existing insurers providing other products would shift
resources to provide products competitive with the newly formed Aetna/Prudential in Houston and Dallas “because
of the costs and difficulties of doing so”).

The Honorable William Baer
The Honorable Sylvia Burwell
September 1, 2015
Page 19 of 20
insurer already has a commercial product in the same relevant geographic market, entering the
Medicare Advantage market may present some challenges.
In the Analysis to Aid Public Comment filed in the Humana/Arcadian merger, the Department
took note that competition from existing Medicare Advantage plans and new entrants “is
unlikely to prevent anticompetitive effects in each relevant geographic market. Entrants face
substantial cost, reputation, and distribution disadvantages that will likely make them unable to
prevent Humana from profitably raising premiums or reducing benefits in the relevant
geographic markets.”107 The very same allegation was made earlier in the UnitedHealth/Sierra
merger.108
E. Remedies
Aetna and Humana may argue that divestitures will remedy the competitive problems identified
by the Department. Both the UnitedHealth/Sierra and Humana/Arcadian mergers were permitted
to proceed on condition that the parties divest portions of their individual Medicare Advantage
lines of business. In those cases, however, the mergers threatened competitive harm in only a few
relevant geographic markets. UnitedHealth’s proposed acquisition of Sierra affected Medicare
Advantage patients in just two counties. In the Humana/Arcadian transaction, the Department
identified 45 counties in which the merger would lessen competition, affecting approximately
50,000 Medicare Advantage enrollees. Here, by contrast, the proposed transaction between
Aetna and Humana would substantially lessen competition in 1,083 counties with over 2.7
million Aetna and Humana members. (See Table 1.)
Even if it were feasible, it would be a staggering task to develop, implement and supervise a
divestiture package that would remedy harm to competition over such a broad area. Our analysis
shows the 1,083 affected counties are in 38 states.
The Department has never before been faced with a merger that threatens to destroy competition
in the Medicare Advantage market to the extent promised by this transaction. The scope of the
likely competitive harm here is so broad and so deep that the amount of divestitures required to
preserve and grow competition may not be feasible from a practical standpoint or even preserve
the purported business benefits of the transaction.109
107 Competitive Impact Statement, United States v. Humana, at 8. 108 Competitive Impact Statement, United States v. UnitedHealth, at 8-9. 109 The federal antitrust enforcement agencies have opposed mergers where the divestitures that might otherwise
have been required to preserve competition were so numerous as to cast serious doubt on the use of divestitures as a
remedy. See, e.g., FTC v. Sysco Corp., No. 15-cv-256-APM, 2015 U.S. Dist. LEXIS 83482, at *76–78 (D.D.C. June
23, 2015); United States v. AT&T Inc. and T-Mobile, Case: 1:11-cv-01560 (D.D.C. Aug. 31, 2011), available at
www.justice.gov/atr/case/us-and-plaintiff-states-v-att-inc-et-al; Press Release, Department of Justice, Blue Cross
Blue Shield of Michigan and Physicians Health Plan of MidMichigan Abandon Merger Plans: Decision to Abandon
Deal Follows Justice Department’s Decision to Challenge the Acquisition (Mar. 8, 2010).
www.justice.gov/opa/pr/blue-cross-blue-shield-michigan-and-physicians-healthplan-mid-michigan-abandon-
merger-plans.

The Honorable William Baer
The Honorable Sylvia Burwell
September 1, 2015
Page 20 of 20
3. Conclusion
The proposed Aetna/Humana merger threatens substantial and irreversible harm to competition
in critically important markets for Medicare Advantage plans across the country. In the earlier
acquisition of Arcadian by Humana, the Department recognized that Medicare Advantage
insurers “compete against each other by offering plans with frequently low or no premiums,
reducing copayments, eliminating deductibles, lowering annual out-of-pocket maximum costs,
managing care, improving drug coverage, offering desirable benefits, and making their provider
networks more attractive to potential members.”110 The Department warned that if the merger
proposed there were completed, the loss of “competition likely would result in higher premiums
and reduced benefits for seniors enrolled in Medicare Advantage plans in the relevant geographic
markets.”111
The same consequences would follow here if Aetna and Humana are permitted to close the
transaction. Today, however, unlike the “thousands of seniors” who would have been affected
had the Department not intervened in the Humana/Arcadian merger,112 millions of seniors will be
adversely affected should the Aetna/Humana merger proceed as proposed.
110 Competitive Impact Statement, United States v. Humana, at 8. 111 Id. 112 Complaint, United States v. Humana at ¶ 4.

By Email and Courier
August 5, 2015
The Honorable William Baer
Assistant Attorney General
United States Department of Justice Antitrust Division
950 Pennsylvania Avenue, N.W.
Washington, D.C., 20530
Dear Assistant Attorney General Baer:
I am writing on behalf of the nearly 5,000 member hospitals, health systems and other health
care organizations, and 43,000 individual members of the American Hospital Association (AHA)
regarding the proposed acquisitions involving four of the five major commercial health insurance
companies in the United States: Anthem’s proposed acquisition of Cigna and Aetna’s proposed
acquisition of Humana. Because the size and scope of these proposed acquisitions is so
enormous and their potential anticompetitive impact on access, affordability and innovation is so
profound, we will address them in separate letters in the knowledge that the Antitrust Division of
the Department of Justice (Department) has indicated it will likely consider them collectively.
This letter will focus on the proposed Anthem/Cigna deal.
We endorse the Department’s often stated position that reforms in the health insurance industry
are dependent on vigorous antitrust enforcement, particularly those involving significant
commercial insurers where there is the very real potential for those deals to substantially reduce
competition and substantially diminish the insurers’ willingness to be innovative partners with
providers and consumers in transforming care. We believe the announced deals cited above have
that potential and, therefore, merit the closest scrutiny to determine whether remedies, such as
divestitures, have any chance of ameliorating the enduring damage they could do as a result of
the loss of such significant competition.
While some are comparing these acquisitions to those in the hospital sector, we submit that the
antitrust issues for these transactions are fundamentally different. The size, scope and enduring
impact of the announced deals far surpass any hospital merger. These transactions will combine
four of the five national health insurance companies, with effectively no possibility that existing firms could replicate their size and scope. As the Department has long recognized,
there are substantial barriers to entry in the health insurance sector (United States and the State of

The Honorable William Baer
August 5, 2015
Page 2 of 13
Michigan v. Blue Cross Blue Shield of Michigan and Remarks by Sharis A. Pozen on
Competition and Health Care: A Prescription for High-Quality Affordable Care, March 19,
2012). Moreover, the seeming underlying business case for them – increasing “top-line”
revenues and profits through acquisition rather than competition without offsetting demonstrable
efficiencies – is fundamentally different than that for transactions in the hospital sector. The
hospital sector is undergoing profound structural changes, driven by the need to take on risk as
the field moves away from fee-for-service payments toward population health, offer integrated
clinical care, and provide financially failing facilities with the resources they require to survive
and continue to serve their communities. Yet despite those pressures, the growth in hospital
spending is at historic lows, which is entirely inconsistent with claims from commercial insurers
about the impact of hospital transactions (Bureau of Labor Statistics Producer Price Index data,
2014-2015, for Hospitals (622)).
The attached analysis details the competitive issues that the Department will consider as it
reviews these deals and the precedents that suggest both are, and should be, at risk. Regulations
in the Affordable Care Act, such as the Medical Loss Ratio (MLR), do not warrant scaled-back
application of the antitrust laws. A keystone component of that act is competition, and the MLR
requirements do nothing to prevent the combined firms from increasing prices or reducing
competition in service, quality, plan design and the like.
We look forward to working with the Department throughout its investigation of these insurance
deals. To that end, we will be contacting the Department to request meetings with staff and top
officials to more fully discuss our concerns and ways in which we can be of assistance.
For more information, you can contact me directly at [email protected] or (202) 626-2336.
Sincerely,
/s/
Melinda Reid Hatton
Senior Vice President & General Counsel
Attachment

The Honorable William Baer
August 5, 2015
Page 3 of 13
Detailed Analysis of the American Hospital Association
On behalf of the nearly 5,000 members of the American Hospital Association (AHA), we
urge that the Antitrust Division of the Department of Justice (Department) thoroughly investigate
Anthem, Inc.’s (Anthem) planned $54 billion acquisition of Cigna Corporation. There is a
material risk that the transaction is likely to substantially reduce competition, in violation of
Section 7 of the Clayton Act.1 The potential harm to consumers from this loss of competition is
large and durable. Because the two companies generate more than $100 billion in combined
revenues, even a modest price increase would cost consumers billions of dollars in higher health
care costs.
The geographic breadth of the transaction’s potential anticompetitive effects and the
number of consumers at risk are also sweeping. The transaction threatens to reduce competition
in the sale of commercial health insurance in at least 817 relevant geographic markets, defined as
Metropolitan Statistical Areas (MSAs) or rural counties. In 600 of these markets, the transaction
would result in a Herfindahl-Hirschman Index (HHI) in excess of 2,500 and a greater than 200-
point HHI increase, which under the Department’s and the Federal Trade Commission’s (FTC)
Horizontal Merger Guidelines (Merger Guidelines, or Guidelines) are market concentration
levels and increases that the Department “presume[s] to be likely to enhance market power.”2 In
an additional 217 markets, the transaction would result in a post-merger HHI in excess of 2,500
and a 100-200 point HHI increase, which the Guidelines say “potentially raise[s] significant
competitive concerns.”3 In these 817 at-risk markets the parties collectively serve 45 million
consumers.
The risk of harm to these tens of millions of consumers is further enhanced because new
entry is unlikely to prevent, or even partially offset, the transaction’s potential anticompetitive
effects. The Department has repeatedly stated in its court filings and in statements by the
Department’s leadership that there are substantial barriers to entry in the health insurance sector,
including obtaining the necessary scale to form a full-service, cost-competitive provider network.
As former Acting Assistant Attorney General Sharis Pozen explained, the Department
“undertook an extensive review of entry and expansion in the health insurance industry” in 2011,
and found that entry in the health insurance sector was often difficult, particularly in already
concentrated markets, as is the case in many of the markets at issue here.4
The parties will no doubt argue that the transaction would produce offsetting efficiencies,
but this is not likely. And it is even less likely that the combined companies would “pass
through” any cost savings to consumers. As numerous economists have found, demand for health
1 15 U.S.C. § 18. 2 Merger Guidelines § 5.3. 3 Id. 4 Sharis A. Pozen, Acting Assistant Att’y Gen., Dep’t of Justice Antitrust Div., Competition and Health Care:
A Prescription for High-Quality, Affordable Care 7 (Mar. 19, 2012) [hereinafter Pozen, Competition and Health
Care], available at http://www.justice.gov/atr/speech/competition-and-health-care-prescription-high-quality-
affordable-care.

The Honorable William Baer
August 5, 2015
Page 4 of 13
insurance is inelastic,5 which reduces the incentive for large health insurance companies to pass
through cost savings. The incentives to pass savings on to consumers are further reduced due to
the opaqueness of the insurance markets and the fact that costs and benefits are not fully
internalized by consumers.
Anthem and Cigna also will undoubtedly urge that the Department approve the merger
after the parties agree to divestitures. It is far from clear that the parties could ever put forth a
divestiture package that would reduce the transaction’s likely anticompetitive effects. First, the
Department has been rightly concerned that the acquirer of any divested lives be well-positioned
to compete effectively in the local area. An existing presence in the market can often facilitate
the success of a buyer. Accordingly, we have examined to what extent it is possible to eliminate
the potentially anticompetitive overlaps through sales to an existing competitor without causing
an increase in market concentration. Significantly, in the 817 at-risk markets, over half of the
lives that need to be divested reside across 368 MSAs and rural counties with no divestiture
possibility that is likely to preserve the pre-merger market structure.
Second, even if the parties somehow managed to maintain the structural status quo, the
Department also must require, as it has in its recent enforcement actions, Anthem and Cigna to
ensure that the buyers of any divested contracts have a provider network of comparable cost and
breadth to that of the parties.6 Indeed, the Department has repeatedly recognized that in order for
a health insurer to compete effectively, it must have a full-service, cost-competitive network of
hospitals, physicians, and other health care providers.7
Third, the Department also should view any remedy proposal carefully because,
regardless of the “fix” the parties ultimately propose, the transaction will inevitably eliminate a
national health insurance company. The parties are two of only five national health insurance
companies that remain today, and two of the other three (Aetna and Humana) also have entered
into a consolidation agreement. Recent enforcement actions suggest that all possible relevant
markets must be examined closely, particularly in a transaction of this magnitude, which can be
challenged on the basis of reduced competition in a market for national customers.8 In particular,
the Department should carefully investigate how this permanent loss of national competitors
would affect competition for contracts with national and large regional employers. Obvious
sources of evidence that the Department should analyze are the parties’ “bid” files reflecting
competition between them for these accounts.
5 See M. Kate Bundorf et al., Pricing and Welfare in Health Plan Choice 32 (Stanford Inst. for Economic
Policy Research Discussion Paper No. 07-47, 2008), http://www-siepr.stanford.edu/papers/pdf/07-47.pdf; Su Liu &
Deborah Chollet, Price and Income Elasticity of the Demand for Health Insurance and Health Care Services: A
Critical Review of the Literature ix (Mathematic Policy Research Ref. No. 6203-042, 2006), http://www.mathematica-
mpr.com/publications/pdfs/priceincome.pdf. 6 See Competitive Impact Statement at 17, United States v. Blue Cross-Blue Shield of Montana, No. 11-cv-
123-RFC (D. Mont. Nov. 8, 2011). 7 See id. 8 See FTC v. Sysco Corp., No. 15-cv-256-APM, 2015 U.S. Dist. LEXIS 83482, at *76–78 (D.D.C. June 23,
2015).

The Honorable William Baer
August 5, 2015
Page 5 of 13
Finally, while the competitive overlap between the parties appears somewhat smaller in
the sale of Medicare Advantage plans than in the commercial insurance market, the Department
also should investigate carefully the transaction’s effect on competition in the Medicare
Advantage sector. Starting with the Department’s challenge to UnitedHealthcare’s acquisition of
Sierra Health Services in 2008,9 the Department (working with the Center for Medicare &
Medicaid Services) has scrutinized carefully the effect of consolidation of Medicare Advantage
providers in order to preserve the benefits of competition for senior citizens that the program was
designed to bring. The Department should continue this policy of protecting competition for the
sale of Medicare Advantage plans both in its investigation of the Anthem/Cigna transaction, as
well in its investigation of Aetna’s proposed acquisition of Humana, which we will address in a
separate letter.
1. The Parties
A. Anthem
Anthem is one of the largest health insurance companies in the United States. In 2014,
Anthem generated approximately $73 billion in revenues.
Anthem is investor-owned and publicly-traded, and operates plans under the Blue Cross
(BCBS) brand in 14 states. The Anthem companies serve members as the Blue Cross licensee for
California, and as the Blue Cross and Blue Shield licensee for Colorado, Connecticut, Georgia,
Indiana, Kentucky, Maine, Missouri (excluding 30 counties in the Kansas City area), Nevada,
New Hampshire, New York (as the Blue Cross Blue Shield licensee in 10 New York City
metropolitan and surrounding counties and as the Blue Cross or Blue Cross Blue Shield licensee
in selected upstate counties), Ohio, Virginia (excluding the northern Virginia suburbs of
Washington, D.C.) and Wisconsin.
Anthem also conducts business through arrangements with other BCBS licensees in
South Carolina and Texas; and through its Amerigroup subsidiary in Florida, Georgia, Kansas,
Louisiana, Maryland, Nevada, New Jersey, New Mexico, New York, Tennessee, Texas and
Washington. The company is licensed to conduct insurance operations in all 50 states through its
subsidiaries.
Anthem has been strikingly successful on its own. In 2014, the company grew its
membership by 1.8 million new members, including more than 700,000 members from the
Public Exchanges, and surpassed 5 million members in its Medicaid business. In 2014 Anthem
increased its revenues by nearly $3 billion, or approximately 5 percent over the previous year.
Moreover, the company “made and [is] continuing to make substantial investments in new
capabilities that better serve [its] members and will help drive future growth [and it is] confident
that by remaining disciplined, consistent and accountable for delivering results, [it] will achieve
[its] goals.”10
9 See Complaint, United States v. UnitedHealth Group Inc., No. 08-cv-322 (D.D.C. Feb. 25, 2008). 10 Anthem, Inc., 2014 Annual Report 9 (2015).

The Honorable William Baer
August 5, 2015
Page 6 of 13
Anthem reported 38.5 million members in its medical plans, as of June 30, 2015. Of
these, 5.8 million were in Medicaid plans, 1.4 million in Medicare Advantage, 1.6 million in
FEP, and 1.8 million in individual products. Approximately 29 million are commercial group
members.11
B. Cigna
Cigna also is one of the largest health insurance companies in the United States, with
15 million members in all 50 states. In 2014, Cigna generated approximately $35 billion in
revenues. Like Anthem, Cigna provides a wide range of commercial plans and has more than
14.2 million commercial members.12
Cigna also has been very successful on its own. Cigna’s 2014 Annual Report states that
in 2014 the company increased revenue by 8 percent and earnings per share by 9 percent last
year. And over the last five years, Cigna “delivered compound annual growth of 14 percent for
revenues and 14 percent for adjusted income from operations on a per share basis.”13 Moreover,
the 2014 Annual Report (which was issued months before the announcement of its transaction
with Anthem) states that, on its own, Cigna expected to achieve substantial growth, such as:
“Growing revenues by eight to ten percent in 2015;
Doubling the size of [its] business over the next seven to eight years[;] and
Delivering on [its] long-term Earnings Per Share objective of 10 to 13 percent compound
growth on an annual basis.”14
2. The Antitrust Laws Applied to Health Insurance Mergers
As noted in the 2004 report, Improving Health Care: A Dose of Competition, the federal
antitrust agencies, for decades, have had a bipartisan “commitment to vigorous competition on
both price and non-price parameters [ ] in health care.”15 As the Agencies have explained, in this
sector “[p]rice competition generally results in lower prices and, thus, broader access to health
care products and services. Non-price competition can promote higher quality and encourage
innovation.”16
11 Press Release, Anthem, Inc., Anthem Reports Second Quarter 2015 Results (July 29, 2015)
http://ir.antheminc.com/phoenix.zhtml?c=130104&p=irol-newsArticle&ID=2072061. 12 Press Release, Cigna Corp., Cigna Reports Strong Second Quarter 2015 Results, Affirms Increased Outlook
(July 30, 2015) http://newsroom.cigna.com/NewsReleases/Cigna-Reports-Strong-Second-Quarter-2015-Results--
Affirms-Increased-Outlook.htm. 13 Cigna Corp., 2014 Annual Report 3 (2015) (footnote omitted). 14 Id. 15 Dep’t of Justice & Federal Trade Comm’n, Improving Health Care: A Dose of Competition 29 (July 2004),
http://www.justice.gov/sites/default/files/atr/legacy/2006/04/27/204694.pdf. 16 Id. at 4.

The Honorable William Baer
August 5, 2015
Page 7 of 13
The Affordable Care Act (ACA) has not diminished the importance of antitrust
enforcement in the commercial health insurance sector. To the contrary, the Department’s
leadership has made clear that:
The success of health care reform will depend as much upon healthy competitive
markets as it will upon regulatory change. If health care reform is to produce
more efficient systems, bring health care costs under control, and provide higher-
quality health care delivery, then we must vigorously combat anticompetitive
mergers and conduct that harm consumers with responsible antitrust
enforcement.17
The Department has primary responsibility for enforcing the antitrust laws in the health
insurance sector.18 In this capacity, the Department has challenged transactions that cause a
significant increase in market concentration and loss of localized head-to-head competition.19 In
its enforcement actions, the Department has set forth a clear analytical framework for evaluating
transactions, which it should apply rigorously in reviewing this transaction of unprecedented size
and scope. We summarize that framework and then apply it to the Anthem/Cigna transaction to
demonstrate the substantial risk that the transaction presents to competition and consumers.
A. Relevant Product Market
The Department has consistently recognized that group commercial health insurance is a
well-defined antitrust-relevant product market. The Department has explained that, for
individuals who obtain commercial health insurance through their employers, there are no
reasonable competitive alternatives to group health insurance. This is because the closest
alternative—individual health insurance—is typically much more expensive than group health
insurance, in part because, while group health insurance is purchased using pre-tax dollars,
individual health insurance is not.20
The Department also has determined that individual (and relatedly, small group)
insurance is a relevant antitrust product market. As the Department has found, “individual health
insurance is the only product available to individuals without access to group coverage or
17 Pozen, Competition and Health Care at 19. 18 The FTC conducts the bulk of the antitrust investigations that involve hospitals. 19 See, e.g., Complaint, United States v. Humana Inc., 12-cv-464 (D.D.C., Mar. 27, 2012) (Medicare
Advantage); Complaint, United States v. Blue Cross Blue Shield of Montana, No. 11-cv-123-RFC (D. Mont. Nov. 8,
2011) (group commercial and individual insurance); Complaint, United States v. UnitedHealth Group Inc., No. 08-
cv-322 (D.D.C. Feb. 25, 2008) (Medicare Advantage); Complaint, United States v. UnitedHealth Group Inc., No.
05CV02436 (Dec. 20, 2005) (large group commercial insurance; small group commercial health insurance);
Complaint, United States v. Aetna, Inc., No. 99 CV 1398-H (June 21, 1999) (commercial plans.) These enforcement
actions reflect the Department’s experience in the insurance sector, including its understanding that, unlike many
industries, health insurance is characterized by strong and durable barriers to entry. See Complaint at ¶ 35, United
States v. Blue Cross Blue Shield of Michigan, No. 10-cv-14155-DPH-MKM (E.D. Mich. Oct. 18, 2010). 20 See Complaint at ¶¶ 21–24, Blue Cross Blue Shield of Montana.

The Honorable William Baer
August 5, 2015
Page 8 of 13
government programs that allows them [(1)] to reduce the financial risk of adverse health
conditions and [(2)] to have access to health care at the discounted prices negotiated by
commercial health insurers.” The Department has explained that “[t]here are no reasonable
alternatives to individual health insurance for individuals who lack access to group health
insurance” because “[p]urchasing hospital services directly, rather than through a commercial
insurer, is typically prohibitively expensive and [therefore] is not a viable substitute for group or
individual health insurance.”21
Regardless of how the Department ultimately defines the product market, the
Anthem/Cigna transaction is likely to reduce competition in the sale of commercial health
insurance. As shown above and discussed further below, the transaction would produce
substantial increases in concentration in the sale of commercial health insurance in substantial
portions of the country. Moreover, the transaction is likely to have particularly large and wide-
ranging anticompetitive effects in the sale of health insurance to employers who self-insure
because both parties are particularly strong in the sale of such plans.
B. Relevant Geographic Market
To date, the Department has largely defined local relevant geographic markets in the
health insurance sector. The rationale is that patients typically seek medical care close to their
homes or workplaces and consequently “strongly prefer health‐insurance plans with networks of
hospitals and physicians that are close to their homes and workplaces.”22 As a practical matter,
consumers will not select commercial health insurers that do not have a network of providers
close to where they work and live.23
The Department’s investigation of the Anthem/Cigna transaction should focus closely on
the deal’s impact on local markets throughout the country. However, as discussed below, this
transaction also raises substantial competitive concerns for reductions in competition for national
and large regional customers.
C. Competitive Effects
Consistent with modern antitrust enforcement principles, the Department’s competitive
effects analysis of health insurance transactions examines both market structure and direct
evidence of competition in the markets.
Market structure analysis focuses on the number of competitors, market shares, and
market concentration ratios, usually the HHI. The HHI is calculated by squaring the market share
of each firm competing in the market and then summing the resulting numbers. The Merger
Guidelines provide that a market whose HHI is above 2,500 is “Highly Concentrated.” The
21 Complaint at ¶¶ 22–23, Blue Cross Blue Shield of Michigan; see also Complaint at ¶¶ 25–26, Blue Cross
Blue Shield of Montana. 22 Complaint at ¶ 27, Blue Cross Blue Shield of Montana. 23 See id.at ¶¶ 27–29.

The Honorable William Baer
August 5, 2015
Page 9 of 13
Guidelines further provide that “[m]ergers resulting in highly concentrated markets that involve
an increase in the HHI of more than 200 points will be presumed to be likely to enhance market
power.”24 Mergers resulting in highly concentrated markets that involve an increase in the HHI
of between 100 points and 200 points potentially raise significant competitive concerns and often
warrant scrutiny.25
The structural evidence strongly suggests that the Anthem/Cigna transaction will reduce
competition in many geographic markets. Table 1 depicts the substantial increases in
concentration that the transaction would produce.
Table 1
MSAs and Rural Counties in which the Post-Merger HHI Exceeds 2,500
for Commercial Lives
HHI Delta Screen Share Screen
>200 > 100 > 50% > 35%
All Commercial Lives
Number of MSAs 600 817 355 498
Total Commercially Insured
Population 31,231,334 45,034,730 11,325,952 23,692,558
Anthem Membership 10,472,094 12,405,109 5,723,016 9,747,303
Cigna Membership 3,706,219 4,755,399 1,254,867 2,613,582
Membership to Divest (smaller
plan) 2,942,351 3,721,670 1,191,751 2,288,825
Membership with no Potential
Acquirer 1,675,275 2,040,397 954,116 1,156,554
In 600 markets, the transaction will produce a post-merger HHI of more than 2,500 with
a 200-point increase, generating a presumption that the transaction will result in an increase in
the parties’ market power. Significantly, the parties insure approximately 31.2 million lives in
these markets. In 217 markets, covering an additional 14 million commercially insured
individuals, the transaction will produce a post-merger HHI of 2,500 with a 100-200 point
increase, indicating that the transaction raises significant competitive concerns for these
consumers.26
24 Merger Guidelines § 5.3. 25 See id. 26 The calculations are based on data from January 2015 obtained from HealthLeaders-Interstudy Managed
Market Surveyor, which provides information on the number of individuals who are enrolled in different health plan
products by county and plan. Following Department precedent in previous investigations, we have calculated shares
and HHI measures at the MSA level or, in the case of rural counties that are not part of an MSA, at the county level.

The Honorable William Baer
August 5, 2015
Page 10 of 13
The competitive picture is equally concerning if one focuses on market shares. In 355
markets, the combined company would have a market share of at least 50 percent, and in 498
MSAs and counties, their combined share would exceed 35 percent.27
Because the Department often focuses on the degree of head-to-head competition
between the merging parties, we also have examined the transaction’s effects on competition in
the sale of commercial health insurance to self-insured employers, which is the area of greatest
competitive overlap. The antitrust concerns are not lower for consolidations of health insurers
that sell policies to self-insured employers (often called Administrative Services Only plans, or
ASO). Again, an essential service that health insurers provide is access to a provider network at
competitive rates. Increasing the market power of a provider of self-insured products would
allow the carrier to increase the administrative and other service fees that self-insured employers
need to pay in order to obtain access to the carrier’s provider network and raises other
competitive concerns that negatively impact consumers.
As shown in Table 2, the competitive picture is even worse when one focuses on the sale
of commercial insurance to self-insured employers.
Table 2
MSAs and Rural Counties in which the Post-Merger HHI Exceeds 2,500
for Commercial ASO Lives
HHI Delta Screen Share Screen
>200 > 100 > 50% > 35%
Commercial ASO Lives
Number of MSAs 1,009 1,177 460 730
Total Commercially Insured
Population 38,336,781 43,919,746 14,928,252 24,741,274
Anthem Membership 10,915,580 11,314,078 6,818,499 9,275,512
Cigna Membership 6,385,014 6,960,004 2,450,874 4,265,669
Membership to Divest (smaller
plan) 4,358,445 4,679,006 2,053,778 3,247,357
Membership with no Potential
Acquirer 2,762,697 3,009,489 1,830,490 2,245,286
Limiting the analysis to self-insured lives, there are 1,009 MSAs and rural counties in
which the merger would result in an HHI exceeding 2,500 with an HHI increase of at least 200,
covering 38.3 million self-insured commercial lives who reside in these markets. And there are
1,177 local geographic areas, with nearly 44 million self-insured lives, for which the HHI
increase exceeds 100 (and the post-merger HHI is at least 2,500). In 460 of these markets, the
combined Anthem-Cigna share of self-insured commercial business would be at least 50 percent.
27 We also apply the HHI > 2500 threshold to these calculations.

The Honorable William Baer
August 5, 2015
Page 11 of 13
D. Entry
The parties will no doubt argue that changes in the health care landscape would prompt
entry if they were to attempt to exercise market power. Former Acting Assistant Attorney
General Pozen appropriately cautioned that the Department should review such claims “carefully
and with some skepticism.”28 This is in part because smaller entrants and incumbents often lack
the volume to obtain prices from providers that are comparable to insurers with large market
positions. The Department’s challenge to Blue Cross Blue Shield of Michigan’s use of most-
favored nation clauses clearly set forth this market dynamic:
Blue Cross’ market power in each of the alleged markets is durable because entry
into the alleged [commercial health insurance] markets is difficult. Effective entry
into or expansion in commercial health insurance markets requires that a health
insurer contract with broad provider networks and obtain hospital prices and
discounts at least comparable to the market’s leading incumbents.29
Indeed, one of the central insights of antitrust analysis of the health insurance markets
over the last several decades is that Judge Easterbrook was likely incorrect at the time (and is
certainly incorrect today) in characterizing the key input of the health insurance market as
“capital” for spreading financial risk.30 Instead, as the Department has argued in its court filings,
“the core component of health insurance products today is access to a local network of health
care providers at rates far lower [than] those that an individual could negotiate directly.”31
Brand also is a substantial entry barrier in the commercial health insurance markets.
Because of the importance of health insurance, and the often substantial transition costs from
switching plans, employers and individuals are often very reluctant to switch to a company that
lacks an established brand in the relevant geographic market. Even companies with strong
positions in other regions can founder in markets in which they lack a strong track record of
providing high-quality services.32
28 Pozen, Competition and Health Care at 7. 29 Complaint at ¶ 35, United States v. Blue Cross Blue Shield of Michigan. 30 Ball Mem’l Hosp. v. Mut. Hosp. Ins. Inc., 784 F.2d 1325, 1335 (7th Cir. 1986) (affirming district court finding
“that insurers need only a license and capital, and that firms such as Aetna and Prudential have both[, and that] [t]here
are no barriers to entry”). 31 Plaintiff United States of America’s Memorandum In Opposition to Defendant Blue Cross Blue Shield of
Michigan’s Motion to Dismiss the Complaint With Prejudice at 13, United States v. Blue Cross Blue Shield of
Michigan, No. 10-cv-14155-DPH-MKM (E.D. Mich. Oct. 18, 2010). Moreover, the Tenth Circuit disagreed with Ball
Memorial and recognized the importance of Blue Cross of Kansas’s provider network, including direct contracts with
local hospitals, as a source of competitive advantage over other insurers that could not until recently contract directly.
Reazin v. Blue Cross and Blue Shield of Kansas, 899 F.2d 951, at 971–72 & n.32 (10th Cir. 1990). 32 See Pozen, Competition and Health Care at 7 (“brokers typically are reluctant to sell new health insurance
plans, even if those plans have substantially reduced premiums, unless the plan has strong brand recognition or a good
reputation in the geographic area where the broker operates.”)

The Honorable William Baer
August 5, 2015
Page 12 of 13
E. Remedies
The parties also will no doubt propose to solve any overlaps that the Department views as
problematic through one-off divestiture remedies. The Department should view such remedies
with skepticism. Indeed, the Department has blocked outright health insurance transactions when
it doubted that a remedy could reliably fix the lost competition, as it did when Blue Cross Blue
Shield of Michigan attempted to purchase Physicians Health Plan of Mid-Michigan.33
Our analysis demonstrates that it will be, at best, challenging for Anthem and Cigna to
devise remedies that will maintain the competitive status quo. First, Table 1 provides estimates
of the number of lives that would need to be divested to maintain the current market structure.
Recognizing the Department’s concern that the acquirer of any divested lives be equipped to
compete effectively in the local area, without at the same time raising additional structural
concerns, we have identified those local areas in which there is no potential acquirer who
currently accounts for at least 5 percent of the covered lives and would not result in a post-
acquisition HHI of 2,500 with a change in HHI of at least 100. Based on these minimal criteria,
there is no viable divestiture candidate for approximately 55 percent of the lives to be divested
(or 2 million consumers), who reside across 368 MSAs and rural counties.
Second, even assuming that one could solve the “nominal” structural problem through the
divestitures, the Department must still ensure, as it has in the past, that the divesting parties
guarantee that the purchaser of any divested assets has a cost-competitive comparable network
of hospitals and physicians. As the Department explained in its Competitive Impact Statement
for its challenge to the Blue Cross-Blue Shield of Montana/New West transaction:
Most importantly, Sections IV(G)–(I) [of the Final Judgment] ensure that the
acquirer has a cost‐competitive health‐care provider network. To compete
effectively in the sale of commercial health insurance, insurers need a network of
health‐care providers at competitive rates because hospital and physician
expenses constitute the large majority of an insurer’s costs. By requiring New
West and the hospital defendants to help to provide the acquirer with a cost‐competitive provider network, Sections IV(G)–(I) help ensure that the acquirer
will be able to compete as effectively as New West before the parties entered the
Agreement.34
In the Blue Cross-Blue Shield of Montana case, because of the importance of ensuring
that the acquirer had a cost-competitive network, the Department required that the hospital
defendants, which owned New West, enter into three-year contracts with the buyer of the
33 See Press Release, Dep’t of Justice, Blue Cross Blue Shield of Michigan and Physicians Health Plan of Mid-
Michigan Abandon Merger Plans: Decision to Abandon Deal Follows Justice Department’s Decision to Challenge the
Acquisition (Mar. 8, 2010), http://www.justice.gov/opa/pr/blue-cross-blue-shield-michigan-and-physicians-health-
plan-mid-michigan-abandon-merger-plans. 34 Competitive Impact Statement at 17, Blue Cross-Blue Shield of Montana, No. 11-cv-123-RFC (D. Mont.
Nov. 8, 2011) (emphasis added).

The Honorable William Baer
August 5, 2015
Page 13 of 13
divested assets that were “substantially similar to their existing contractual terms with New
West.” The Department declared these contractual guarantees to be “vital” to ensuring the
effectiveness of the remedy: “Because these three‐year contracts provide the acquirer with a cost
structure comparable to New West’s costs, they position the acquirer to be competitive selling
commercial health insurance in all four geographic markets.”35
F. Medical Loss Ratio
Finally, Anthem and Cigna may argue that the Department should lower the antitrust bar
because of the margin restrictions imposed by the ACA’s Medical Loss Ratio (MLR) provisions,
which require that fully insured health plans spend a minimum percentage of their premiums
(less taxes, licenses, and regulatory fees) on medical services and quality improvement
initiatives. In particular, the ACA requires that large group insurers spend at least 85 percent of
their net premium dollars on these items, while small group and individual insurers must devote
at least 80 percent of them.36
The Department should reject this argument, as it has in the past. First, MLR
requirements only apply to fully insured products. They do not cover at all the substantial
competition between the parties for self-insured products. Second, the MLR requirements are not
price-caps. Nothing in the requirements prevents an insurance company from increasing its costs,
in order to increase prices and margins. Third, the requirements do not prevent health insurance
companies from exercising market power by restricting provider networks or reducing service
levels so long as they meet the minimum MLR thresholds.
3. Conclusion
A competitive commercial health insurance market is essential for access, affordability
and innovation in the health care sector. Anthem’s proposed acquisition of Cigna presents a
substantial risk to such competition on an unprecedented national scope. The AHA is confident
that the Department will work to protect consumers by vigorously investigating the transaction.
35 Id. at 17–18. 36 See ACA, Pub. L. No. 111-148, § 10101(f), 124 Stat. 119, 886 (2010) (amending Public Health Service Act
§ 2718(b)(1)(A), 42 U.S.C. 300gg-18).