Embed Size (px)
Citation preview

Journal of Clinical InvestigationVol. 46, No. 5, 1967
Testosterone and Androstenedione Blood Production Ratesin Normal Womenand WomenwithIdiopathic
Hirsutism or Polycystic Ovaries *C. WAYNEBARDIN t ANDMORTIMERB. LIPSETT
(From the Endocrinology Branch, National Cancer Institute, Bethesda, Md.)
Summary. The average plasma testosterone concentration of women witheither hirsutism or polycystic ovaries and hirsutism was higher (p < 0.01)than that of normal women although the ranges overlapped. Testosteroneblood production rates averaged 830 ± 120 SE and 1,180 ± 310 SE ,ug per dayin the two groups of hirsute women and 230 ± 33 SE ,ug per day in normalwomen. The ranges did not overlap.
The testosterone metabolic clearance rates of hirsute women (1,090 ± 140SE L per day) and of men (1,240 + 136 SE L per day) were significantlyhigher than those of normal women (590 + 44 SE L per day). These differ-ences persisted when the metabolic clearance rates were corrected for surfacearea. Wesuggest that testosterone metabolic clearance rates vary directlywith some function of testosterone production.
The mean plasma androstenedione levels (2.8 ± 0.35 SE and 2.8 + 0.30 SE,ug per L) and production rates (6,060 ± 450 SE and 7,360 + 345 SE ,ug perday) of the womenwith hirsutism or polycystic ovaries, respectively, were sig-nificantly higher than those of normal women (1.5 + 0.22 SE pg per L; 3,300+ 830 SE pg per day). The androstenedione metabolic clearance rates werethe same in each group. Plasma androstenedione was the precursor of 49%of plasma testosterone in normal womenand of 26% of plasma testosterone inhirsute women. Thus, 74% of the plasma testosterone in these subjects musthave been either secreted or derived from a precursor that did not enter theplasma androstenedione pool.
Introduction
Study of virilization and hirsutism received newimpetus with the introduction of- accurate methodsfor measuring plasma testosterone 1 levels. Inseveral series of hirsute women (1-6), the average
* Submitted for publication November 28, 1966; ac-cepted February 2, 1967.
A preliminary report of this work was presented at theForty-eighth Meeting of the Endocrine Society, June 20,1966.
t Address requests for reprints to Dr. C. WayneBardin, Endocrinology Branch, National Cancer Insti-tute, Bethesda, Md. 20014.
'The following trivial names have been used: testos-terone, 17p8-hydroxy-4-androsten-3-one; androstenedione,4-androsten-3,17-dione; dehydroepiandrosterone, 3fi-hy-droxy-5-androsten-17-one.
plasma testosterone concentration was high, butin each series some of the subjects had normallevels. The role of plasma androstenedione hasnot been evaluated in hirsute women, and there isno comprehensive study of androgen productionrates in such patients. Wehave therefore mea-sured testosterone and androstenedione plasma lev-els and production rates in normal women and inwomen with idiopathic hirsutism and hirsutismassociated with polycystic ovaries. Using themodel developed by Horton and Tait (7), we haveestimated the contribution of androstenedione pro-duction to the testosterone production rate andhave shown that the excess testosterone is secretedas well as produced from plasma androstenedione.Our finding that the blood testosterone production
891

C. WAYNEBARDIN AND MORTIMERB. LIPSETT
TABLE I
Clinical summary
UrinarySub- Body Hirsut- Ovula- Ovarian 17-keto-ject Age Weight Height surface ism* Mensest tory size steroids
years kg cm m2 cm mg/dayIa. Normal ovulatory women
1 22 59 158 1.59 N Yes N2 33 50 164 1.52 N Yes N3 21 40 165 1.39 N Yes N4 26 55 170 1.62 N Yes N5 33 55 159 1.54 N Yes N
lb. Anovulatory women6 28 61 158 1.61 N No N7 22 68 156 1.67 N No N 128 64 61 165 1.66 A No N 69 35 100 157 2.00 A No N 8
II. Womenwith idiopathic hirsutism10 24 85 163 1.89 4+ N Yes N 1811 17 54 163 1.56 2+t N Yes N 1112 18 60 165 1.65 3+ N Yes N 1113 23 66 172 1.77 2+ N Yes N 1314 31 49 153 1.43 3+ 0 No 3 X2 X3 615 20 92 165 1.97 1+ 0 No 3 X 2 X 2 616 31 72 165 1.78 1 + 0 No' N 2017 25 97 165 2.01 2+ A No 4 X2 X2 12
III. Womenwith polycystic ovaries18 33 81 164 1.86 3+t§ 0 No 4 X 6 X 4 819 35 117 164 2.18 3+ 0 No 4 X3 X3 142011 29 65 175 1.78 2+ N Yes 6 X 6 X 4 2321 25 81 172 1.93 1+ 0 No 3 X2 X2 922 35 101 162 2.02 3+t 0 No 4 X 2 X 2 10
* Facial hirsutism was graded 1+ for each portion of the face involved (side burns, upper lip, chin) and 4+ if theentire beard area was involved. All subjects had a heavy growth of hair on trunk and extremities.
t Abbreviations: N = normal; 0 = oligomenorrhea; A = amenorrhea.t Slight temporal balding.§ Clitoromegaly.11 Patient studied after wedge resection of ovaries.
rate was high in each hirsute woman is the onlyconsistent physiologic difference between normaland hirsute women that has been observed.
Methods
Subjects. The normal subjects volunteered for thesestudies. Group Ia was composed of five women withnormal ovulatory menses. Group Ib contained four non-hirsute subjects: one was receiving oral contraceptives2(Patient 6); one had received oral contraceptives 2 5months previously and was now anovulatory (Patient 7);one had carcinoma of the cervix and was postmenopausal(Patient 8); and one patient had secondary idiopathicamenorrhea (Patient 9). Group II comprised eightwomen with complaints of hirsutism. In four of themthe ovaries were assumed to be normal on the basis ofregular ovulatory menses. In three of the four patientswith irregular anovulatory cycles in whom culdoscopy
2 Norethynodrel, 5 mg per day, and mestranol, 0.075 mgper day.
was performed (Patients 14, 15, 17) the ovaries weregrossly and histologically normal. Group III containedfive hirsute patients with histologically characteristicpolycystic ovaries. When groups II and III are com-bined, they will be referred to as the hirsute subjects.These clinical data are summarized in Table I. Testos-terone metabolic clearance rates were determined in sixnormal men.
All subjects used in this study had normal 24-hoururinary 17-hydroxycorticoid excretion that was suppressedby 2 mg of dexamethasone daily for 3 days. Ovulationwas diagnosed either by endometrial biopsy or urinarypregnanediol excretion. Thyroid and liver functiontests were normal in all subjects. Urinary steroids mea-sured were as follows: 17-ketosteroids (8), 17-hydroxy-corticoids (9), and pregnanediol (10).
Reagents. Solvents were analytical grade and weredistilled before use. Androstenedione-1,2-8H (5 c permmole), androstenedione-4j4C (50 mc per mmole),testosterone-7ca-3H (10 c per mmole), and testosterone-4-14C (50 mc per mmole) were obtained commercially's
3-New England Nuclear Corp., Boston, Mass.
892

TESTOSTERONEAND ANDROSTENEDIONEPRODUCTIONRATES IN HIRSUTE WOMEN
TABLE II
Chromatographic systems
System Support Solvents
BM1 Silica gel Benzene: methanol (9:1)BE4 Silica gel Benzene:ethyl acetate (6:4)BE2 Silica gel Benzene:ethyl acetate (8:2)Bush A2 Paper Ligroin: methanol: water (10:7:3)
and further purified by thin layer chromatography insystems BMand BE5 (Table II). To test for purity ofthe labeled steroids, we added a portion of each to 200,ug of authentic steroid and carried through the proce-
dure outlined in Figure 1. The specific activity was esti-mated by measuring the mass of steroid by absorption at240 mA in ethanol and radioactivity by liquid scintillationspectrometry. The specific activity of each steroid re-
mained constant after successive chromatography as theacetate, free alcohol, and 17-ketone.
Chromatography. Thin layer chromatography was per-
formed on 20- X 20-cm glass plates coated with 25 mmofBrinkmann Porter silica gel GH254. Whatman 3MMwas used for paper chromatography. The chromatography
Plasma Extract
TLC - BM1
Testosterone
1. Bush A2 - 16 hrs2. Acetylation3. TLC - BE24. Specific activity5. Saponification6. TLC - BE47. Specific activity8. Oxidation9. TLC BE4
10. Specific activity
Androstenedione
1. Acetylation2. Bush A2 - 6 hrs3. Reduction to testosterone4. TLC BE45. Specific activity6. Acetylation7. TLC - BE28. Specific activity9. Saponification
10. TLC - BE211. Specific activity12. Oxidation13. TLC - BM114. Specific activity
FIG. 1. PURIFICATION OF PLASMAEXTRACTS FOR ESTI-
MATION OF ISOTOPIC TESTOSTERONEAND ANDROSTENEDIONE.
TLC= thin layer chromatography. Steps 12 and 13 were
performed on 9 samples and produced no change inspecific activity.
systems are listed in Table II. Gas-liquid chromatog-raphy and collection of the samples for radioactivitymeasurements were performed as described previously(11).
Plasma steroids. Forty ml of heparinized blood wasobtained for plasma steroid levels immediately beforedetermination of the metabolic clearance rates. Plasmatestosterone and androstenedione concentration was mea-sured by a modification (12) of the double isotope tech-nique reported from this laboratory (11). Plasma tes-tosterone and androstenedione samples of 0.007 ,ug canbe measured with theoretical precisions of 35%o and 22%,respectively. The method blanks for 20 ml of plasmawith an over-all recovery of 20% were 0.010 Aug per 100ml for testosterone and 0.0025 lug per 100 ml for andros-tenedione and have been subtracted from the reportedplasma levels.
Metabolic clearance rates. The metabolic clearancerates of testosterone (MCRT) and of androstenedione(MCRA) were measured by the technique of Horton andTait (7), and their abbreviations are used. All subjectswere studied under basal conditions. Approximately 10to 15 uc of androstenedione-8H and 0.25 to 0.5 j.c of tes-tosterone-&4C were injected intravenously in 20 ml of 5%ethanol in saline as a priming dose, and starting 30 min-utes later, double these quantities were given as a con-stant infusion for 90 minutes in 170 ml of 5%o ethanolin saline. With the infusion of androstenedione-5H andtestosterone-'4C at a disintegrations per minute ratio of30: 1, sufficient 'H and "C counts were present in 20 mlof plasma to determine the metabolic clearance of bothsteroids and the conversion ratio of androstenedione totestosterone but not the conversion ratio of testosteroneto androstenedione. In one patient (No. 8) the infusionwas extended for 12 hours. In two additional subjects(Patients 3 and 17), the isotopes were reversed, and 7 j&cof androstenedione-4-_4C and 2.5 ,uc of testosterone-7a-5Hwere given as a priming dose, and after 30 minutes twicethese quantities were infused over 90 minutes. Thesedata are presented in Table III.
The radioactive steroids were infused with a Bowmaninfusion pump equipped with a siliconized latex pumptube and Teflon tubing. The latex pump tubing wasreplaced after every fifth infusion. The tubing effluentwas monitored at frequent intervals, generally three tofive times during the infusion, and the actual rate of in-fusion of labeled steroids agreed closely with the cal-culated rate in each instance. The MCRwas calculatedfrom the rate of infusion of the isotope divided by theconcentration of isotope in the specific steroid per vol-ume of plasma.
Isotopic testosterone and androstenedione concentra-tions were determined by reverse isotope dilution on 40ml of heparinized blood obtained at 50, 70, and 86 minutesof the infusion. The plasma was separated within 30minutes, and 200 ,ug each of testosterone and androstene-dione was added to the plasma. The plasma sampleswere extracted twice with 2 vol of ether: chloroform(3: 1) after the addition of 1 ml of 1 N NaOHper 20ml of plasma. The extracts were washed with water,
893

C. WAYNEBARDIN AND MORTIMERB. LIPSETT
TABLE III
Infusion rates and plasma concentration of isotopic steroids
Infusion Plasma* Infusion Plasma*Andros- Andros- Andros- Andros-
Sub- tenedione- Testos- tenedione- Testos- tenedione- Testos- tenedione- Testos-ject 3H terone-14C 3H terone-14C Subject aH terone-"4C 8H terone-14C
dpm/hr dpm/hr dpm/L dpm/L dpm/hr dpm/hr dpm/L dpm/LX 107 X 106 X 106 XO' X1OT XJos X10f X1&
1 4.31 1.41 6.9 6.40 12 5.38 1.69 5.43 6.052 5.99 1.31 4.78 5.23 13 4.74 1.46 5.55 3.143t 1.82 6.80 1.93 21.4 14 4.39 1.44 7.06 5.874 4.21 1.42 5.96 6.45 15 5.38 1.69 5.08 2.515 4.08 1.59 4.78 7.05 16 4.00 1.59 4.46 3.756 2.68 1.17 2.76 7.67 17t 1.82 6.80 1.68 9.317 5.04 2.35 4.00 6.00 18 4.85 2.60 3.10 3.948 0.434 1.73 19 5.85 1.32 4.18 3.009 18.0 34.0 20 4.70 1.79 3.32 5.26
10 4.75 2.51 3.83 6.06 21 4.90 1.55 6.29 4.9811 2.50 1.45 2.78 3.72 22 4.76 1.63 4.83 2.94
* Mean of the three values obtained at 50, 70, and 86 minutes of the infusion.t Androstenedione-14C and testosterone-3H were infused in these patients.
dried, and purified by chromatography and derivativeformation as outlined in Figure 1. Oxidation was car-ried out with 0.2% chromic acid in glacial acetic acidfor 10 minutes and reduction with freshly prepared 2%potassium borohydride in water for 20 seconds. Acetyla-tion was performed with acetic anhydride in pyridine andsaponification with 0.15 N NaOH in 80% methanol un-der Ne overnight. After chromatography of each deriva-tive (Figure 1) the specific activity of both plasma ster-oids was determined as outlined above. The plasmaconcentrations of isotopes in testosterone and andros-tenedione were calculated from the recovery of addedunlabeled steroid.
Evidence that the infused steroids reached equilibriumduring the 90-minute infusion was provided by the con-stant level of radioactive testosterone and androstenedi-one observed in the plasma samples at 50, 70, and 86 min-utes. In one patient (No. 8), continuing the infusionfor 12 hours produced no change in the observed radio-active testosterone levels. In each subject the meanplasma concentrations for both testosterone and andros-tenedione were calculated, and the per cent deviation ofeach sample from the mean was determined. After infu-sion of testosterone-'C and androstenedione-8H the devia-tion of individual samples from the mean was + 1.1%for "C in testosterone, + 2% for 'H in androstenedione,and ± 6% for 'H in testosterone. These analyses demon-strated no significant trend in the plasma isotopic steroidlevels.
H/I"C of urinary testosterone glucuronoside. Aftereach infusion, urine was collected for 2 days and pooled.One-tenth of the pool from each of six subjects was ex-tracted with 2 vol of ether and then hydrolyzed withbeef liver glucuronidase (Ketodase). The freed steroidswere extracted with 6 vol of dichloromethane after ad-dition of 50 Atg of testosterone. The extracts were washedwith 0.1 N NaOH and water and then partitioned be-tween heptane and 80% ethanol. The heptane was dis-carded; the ethanol concentration was reduced to 20%,
and the testosterone was extracted with 8 vol of carbontetrachloride. These extracts were purified as in Fig-ure 1. One-third of the sample was counted at steps 4and 10, and the 'H/"C of the remaining one-third wasdetermined on the effluent after gas-liquid chromatog-raphy. The 'H/"C ratios were the same at step 10 andafter gas-liquid chromatography.
Radioactivity measurement. Counting was performedwith a Packard Tri-Carb liquid scintillation spectrometer,model 4322, operating at 25% efficiency for 3H and at 50%efficiency for 'C. Discriminator and gain settings weresuch that less than 0.1% of the 'H was counted in the'C channel, and 13% of the "C was counted in the 'Hchannel. With a single isotope, sufficient counts wereaccumulated to -give standard errors of less than 2%.When two isotopes were measured, the samples werecounted four times for 50 minutes, and the standard er-rors for 'H and 'C were less than 2%o. The standarderror of the 'H/"C ratio of urinary testosterone glu-curonoside was less than 4%.
Calculations. The symbols and calculations for theseveral parameters of the testosterone-androstenedionesystem are those of Horton and Tait (7). The super-scripts indicate the steroid, the subscripts the compart-ment. The symbol z refers to the isotope in testosteroneand x to the isotope in androstenedione. The formulasused are as follows:
MCRT= RzT/zT and MCRA- RxA/xA,
where RzT is the disintegrations per minute of testosteroneinfused per unit time and zT is the concentration of isotopein testosterone in disintegrations per minute per unitvolume of plasma. The androstenedione expressions areanalogous.
PBT = MCRTX iT and PBA = MCRAX iA,
where PBT is the blood testosterone production rate and iTis the blood testosterone concentration.
CBBAT = XT/XA,
894

TESTOSTERONEANDANDROSTENEDIONEPRODUCTIONRATES IN HIRSUTE WOMEN
TABLE IV
Concentrations, production rates, and interconversion of plasma testosterone and androstenedione*
PlasmaPlasma andros- [P]BBATPBA
Subject testosterone MCRT pBT tenedione MCRA PBA XT/XA EP]BBAT pBT
pg/L L/day pg/day pg/L L/day pg/dayIa. Normal ovulatory women
1 0.25 5302 0.36 6003 0.36 7604 0.39 5305 0.62 540
130 1.1 1,500220 2.1 3,000260 0.9 2,120210 1.7 1,700330 1.8 2,050
590 230 1.5±98 ± 73 40.50±44 ±33 40.22
lb. Anovulatory women6 0.53 370 2007 1.4 940 1,3208 0.32 600 1909 0.90 1,270 1,140
II. Womenwith idiopathic hirsutism10 0.90 990 89011 1.08 920 99012 1.01 670 68013 0.71 1,100 78014 0.99 590 58015 0.35 1,610 56016 0.54 1,020 55017 0.90 1,750 1,580
1,080±-410±145
830±340±120
1.62.40.9
2,070±577±260
1,7006,3001,8902,9003,700
3,300±1,860
±830
0.0930.160.110.0950.12
0.12±0.025±0.011
2,330 3,700 0.253,020 7,250 0.085
1.9 2,9803.5 2,2502.3 2,3802.2 2,0505.1 1,4901.8 2,5202.9 2,1502.7 2,610
2.840.98±0.35
2,30044404160
III. Womenwith polycystic ovaries18 0.5119 1.2120 0.7021 0.8222 1.98
1,5801,060
820750
1,330
1,110±350±155
8101,280
570620
2,640
1,180±700±-310
2.2 3,7202.3 3,3101.9 3,4003.4 1,8703.4 2,360
2.8 2,930±0.7 ±775±0.3 ±350
5,5107,7005,4304,5207,6004,5406,1007,040
6,060± 1,280
±450
8,1007,6006,7006,4008,000
7,360±770±345
0.0580.0960.0840.0450.0920.0400.0750.068
0.070±t0.017±0.006
0.0650.1200.1700.0540.053
0.0330.0320.0390.0300.032
0.033±0.00340.001
0.0400.026
0.0190.0400.0240.0240.0360.0260.0360.046
0.031±0.009±0.003
0.0280.0390.0410.0220.030
0.092 0.032±0.052 ±0.008±0.023 ±0.003
0.450.930.280.410.35
0.49±0.29±0.11
0.760.15
0.120.310.190.140.470.210.400.20
0.26±0.13±0.04
0.280.230.460.220.09
0.26±0.13±0.06
* MCRTand MCRA= metabolic clearance rate of testosterone and androstenedione; PBT and PBA = bloodproduction rate of testosterone and androstenedione; xT/xA = conversion ratio of labeled testosterone to androstene-dione; [P]BBAT = fraction of blood androstenedione pool converted to blood testosterone pool.
where CEBATis the conversion ratio of androstenedione to since the product of the two [p] values is approximatelytestosterone in blood.
[p]BBAT = (MCRT/MCRA) X (xT/xA),
where EP]BBAT is the fraction of the blood androstenedionepool converted to the blood testosterone pool.
([PIBBAT X PBA)/PBT = (XT/XA) X (iA/iT),
where the expression is the fraction of the blood testoster-one production that is derived from blood androstenedioneproduction. A similar expression can be derived forandrostenedione production from testosterone. The cor-
rection factor, 1 - [p]BBAT X [P]BBTA, for the amountof precursor originating from product has been ignored,
0.03.Errors of the method. The errors of the rates of radio-
active steroid infusions determined from the countingerrors and from the observed variability of pump tubingeffluent were ±4% for RZT and 5% for RxA. The theo-retical errors of the radioactive steroid levels in plasmacalculated from counting errors and specific activitydeterminations were ±4%, ±i4%, and ±11% for thesedeterminations (±3.0, ±4.4, and ±9.9%). The errors
of the calculated values were as follows: MCRT, ±5.7%;MCRA, ±6.0%; PBT, ±35%; PBA, ±18%; XT/XA,±11.8%; [P]BBAT, ±14.4%. The larger error of PsT was
calculated for plasma testosterone levels in normal women.
MeanSDSE
0.40±0.13±0.06
MeanSDSE
0.81+0.75±0.09
MeanSDSE
1.04±0.61±0.27
895

C. WAYNEBARDIN AND MORTIMERB. LIPSETT
This error is 21 %when the plasma testosterone level is inthe range of 0.1 jg per 100 ml.
Results
Plasma steroids. The mean plasma testosteroneconcentration of 0.40 jug per L in the five normalovulatory women (Table IV) was the same as
that of 20 normal women previously reportedfrom this laboratory (0.37 + 0.02 SE jtg per L;range, 0.20 to 0.70 jg per L) (12). The mean
plasma levels in women with idiopathic hirsutism(0.81 + 0.09 SE ug per L) and with polycysticovaries (1.04 0.27 SE jug per L) were higherthan the normal levels (p < 0.01). Despite thisdifference four of the 13 hirsute women hadplasma testosterone levels in the normal range.
The mean plasma androstenedione level in thefive normal women (1.5 0.22 SE Mg per L) was
not different from the mean of 20 normal women
previously reported (1.67 + 0.09 SE Mg per L;range, 0.9 to 2.1 ug per L) (12). The andros-tenedione levels in both hirsute groups were sig-nificantly greater than those of normal women
(p < 0.05). As with the testosterone levels, theranges overlapped.
Metabolic clearance rates. The primary datafrom all the studies are summarized in Table III.Adequate amounts of tritium and 14C were presentin each steroid, and the counting ratios were satis-factory. The mean MCRTof normal women mea-
sured by the constant infusion technique was sig-nificantly less than the means of the subjects with
120 r
1101
100 F
* Hirsute
0 Normal
0 0
0
90 F
'-80x
iw
70
601_ 0
50 _
0
0
0
o0 *
00
0
500 900 1300METABOLIC CLEARANCE-L/doy
1700
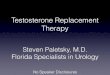
FIG. 2. CORRELATIONOF THE TESTOSTERONEMETABOLICCLEARANCERATE (MCRT) WITH BODY WEIGHT. The r
equals 0.79 with 95% confidence limits of 0.5 to 0.9.
idiopathic hirsutism or polycystic ovaries (p <0.01) (Table IV). Because the higher clearancerates occurred in heavier women, we examinedMCRTas a function of body weight (Figure 2)and found the r to be 0.79 with 95% confidencelimits of 0.5 to 0.9. In view of these findings andsince the calculated metabolic clearance rate de-pends not only on rate of steroid metabolism buton its volume of distribution, it is appropriate tocorrect MCRTfor body size before comparing itamong groups. We have elected to express
TABLE V
The metabolic clearance rates of testosterone and androstenedione
Subjects MCRT/m2No. Surface area MCRT MCRT/m2 log PBT MCRA MCRA/m2
ma2 L/day L/dayNormal women
5 1.53 i 0.04* 590 =1: 44 390 :1: 40 161 i 15 2,070 260 1,360 i 185
Idiopathic hirsutism8 1.75 + 0.15t 1,080 145t 600 ±t 60t 202 i1 18 2,300 -t 160 1,240 4 53
Polycystic ovaries5 1.95 i 0.07t 1,110 ± 155t 568 ± 84 185 :1 26 2,930 4t 350 1,550 :1: 96
All hirsute women13 1.83 ±t 0.06t 1,090 + 140t 588 d 47t 196 4 12 2,540 =1 178 1,360 d 65
Normal men6 1.98 I 0.12t 1,240 i 136t 627 4 60t 162 ± 16
* Mean 4 standard error.t Significantly different from normal women (p < 0.01).t Significantly different from normal women (p < 0.05).
896

TESTOSTERONEAND ANDROSTENEDIONEPRODUCTIONRATES IN HIRSUTE WOMEN
MCRTas a function of surface area. Even withthis correction, MCRT per square meter washigher in the hirsute patients than in the normalwomen (p < 0.05) (Table V). Calculationsbased on body weight rather than surface areagave similar results. These data suggested thatsome factor in addition to body size influencedthe MCRTof hirsute women.
Wetherefore examined the relationship betweenMCRT and several parameters of testosteronemetabolism. The logarithm of the blood testos-terone production rate (log PBT) was correlatedpositively with MCRT (r = 0.65) and withMCRTper square meter (r = 0.55) with ratherwide confidence limits. When the MCRTwascorrected for surface area and log PBT, then theresulting expression MCRTper square meter perlog PBT was the same for all groups (Table V).
Since we found that the MCRTof men (TableV) was twice that of women, we calculated the ef-fects of correction for surface area and testosteroneproduction rate on MCRT. When the MCRTwascorrected for surface area, the MCRTper squaremeter of men remained significantly greater thanthat of women. When the expression MCRTpersquare meter per log PBT was calculated, however,the values were the same in men and women.
The MCRTof the women in group Ib was con-sistent with that of the other groups with thecorrection factors just outlined. Of interest werePatients 7 and 9, who had high plasma testos-terone levels and MCRT. When the MCRTwascorrected by surface area and log PBT, the MCRTper square meter per log PBT was the same as inthe other groups.
The MCRAand MCRAper square meter aresummarized in Table V. Although there was nosignificant difference between the MCRAof nor-mal and hirsute womenat the 0.05 level, the MCRAof the obese women was greater than that of thenormal women. The variances of the means of theMCRAfor each group were reduced markedly bycorrection for surface area.
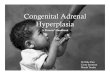
Blood production rates. The blood productionrates of testosterone and androstenedione fromTable IV are summarized in Figures 3 and 4, re-spectively. Both PBT and PBT per square meterwere two to four times greater in the hirsutegroups than in the normal. The ranges did notoverlap although some hirsute patients had plasma
26001
1400_
1200 _
1000
ox4a%
- PT/mIT
800_
600 -
400k_
200I
NORALDIl Uv IvrI MRInew ;T I~a, K;sNORMAL'~ HIRSUTISM OVARIES
FIG. 3. TESTOSTERONEBLOOD PRODUCTIONRATES (PBT)AND BLOOD PRODUCTIONRATES PER SQUAREMETEROF BODYSURFACE (PBT/m2) IN NORMALAND HIRSUTE WOMEN.Mean and range.
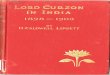
testosterone levels within the normal range. Simi-larly, PBA and PBA per square meter were twice asgreat in the hirsute women.
Conversion ratios, [pI values, and fraction ofPBT from PBA. The conversion ratios of labeledandrostenedione to testosterone, xT/xA, duringthe infusion of radioactive androstenedione aresummarized in Table IV. Ratios of XT/XA werethe same in the normal and polycystic ovarygroups, but xT/xA was significantly lower in thenormal than in the idiopathic hirsutism group(p < 0.01). Despite this, the fraction of the bloodandrostenedione converted to blood testosterone,[p] BBAT, was the same in the three groups, themeans ranging from 0.031 to 0.033. Since PBAwas greater in the hirsute subjects, the amount ofblood testosterone produced from blood andros-tenedione (l[P] BBAT X PBA) was higher. It is ap-parent that since the fractional conversion rate,[p] BBT, was the same among all groups, the percent of blood testosterone derived from blood
897
ninPATWlir D" Vf'VQTlt'

C. WAYNEBARDIN AND MORTIMERB. LIPSETT
i4 T
2L
IDIOPATHIC POLYCYSTICNORMAL HIRSUTISM OVARIES
FIG. 4. ANDROSTENEDIONEBLOOD PRODUCTION RATES
(PBA) ANDBLOODPRODUCTIONRATES PER SQUAREMETEROF
BODYSURFACE(PBA/M2) IN NORMALAND HIRSUTE WOMEN.
Mean and range.
androstenedione is directly proportional to PBA/PBT. In normal subjects, this ratio was 14.3, and49%o of blood testosterone was derived from bloodandrostenedione. In the idiopathic hirsutism andpolycystic ovary groups, PBA/PBT were 7.3 and6.2, respectively, so that a smaller per cent of blood
testosterone originated from blood androstene-dione (Table IV). Thus the hirsute subjectsmust have had either a greater secretion of tes-tosterone or a larger synthesis from some precur-
sor that did not enter the plasma androstenedionepool.
Comparison of 3H/14C ratios of plasma and tes-tosterone and urinary testosterone glucuronide. Ithas been shown (7, 13) that only a small fractionof testosterone synthesized from blood androstene-dione reaches the blood testosterone pool, and itwas found that the fractional conversion of bloodandrostenedione to urinary testosterone glucurono-side ([p] BUAT) was greater than [p] BBAT. Thelarge differences between the 3H/14C ratios ofplasma testosterone and urinary testosterone glu-curonoside (Table VI) re-emphasize this. Theratios of the 3H/14C of testosterone glucuronosideto the 3H/14C of plasma testosterone were not thesame in all patients (column 6, Table VI). Thisdemonstrates that [p] BBAT has no constant rela-tionship to [p] BUAT. This is in accord with thesuggestion (7) that most of the synthesis ofplasma testosterone from androstenedione takesplace in peripheral tissues other than the liver.
Discussion
Testosterone. The development of methods forthe measurement of plasma testosterone levelspromised solutions to several problems associatedwith virilization and hirsutism. Indeed, to our
knowledge, whenever plasma testosterone has beendetermined in virilized women, the levels havebeen high. However, the promise of a relation-ship between plasma testosterone and hirsutism
TABLE VI
Isotopic ratios in urinary testosterone glucuronoside and free plasma testosterone after the infusion ofandrostenedione-3H and testosterone-14C
(6)(4) Ratio of
(3) 31-1/14C (5) column 4(1) SH/14C of urinary 3H/"4C divided by
Subject (2) of isotopes testosterone of plasma ratio ofno. Diagnosis given glucuronoside testosterone column 5
dpm3 Normal 25.0 10.9 0.84 135 Normal 28.2 10.9 0.79 14
12 Idiopathic hirsutism 32.8 10.2 0.79 1315 Idiopathic hirsutism 32.8 15.9 0.78 2020 Polycystic ovary 31.9 20.1 1.12 1822 Polycystic ovary 32.1 7.25 0.89 8
898

TESTOSTERONEANDANDROSTENEDIONEPRODUCTIONRATES IN HIRSUTE WOMEN
has proved illusory. In several studies of hirsutewomen, plasma testosterone levels ranged fromnormal to high (1-6). Our data are similar tothose previously reported; that is, although themean plasma testosterone level differed signifi-cantly between the normal and hirsute groups,not all the patients had abnormal testosteronelevels.
In contrast to the normal levels of plasma tes-tosterone reported in various studies in hirsutesubjects, testosterone production rates were higherthan normal in each hirsute patient. This some-what unexpected finding made us consider thatsome aspects of testosterone production or clear-ance in addition to plasma levels may be of sig-nificance in the development of hirsutism. Therecent reports of testosterone metabolism by skin(14) may be pertinent to the clearance of testos-terone, but meaningful estimates of the fractionof testosterone metabolized by skin cannot bemade as yet.
The thesis has been advanced that hirsutismmay be a manifestation of increased end-organsensitivity to normal androgen levels (15). Thiswas based on the obvious differences in the rateof development of hirsutism by women receivingtestosterone. This thesis was supported furtherby the occurrence of normal plasma testosteronelevels in some hirsute women. Our findings of auniformly increased testosterone production ratedo not support the hypothesis that differences inend-organ sensitivity are the sole determinants ofhirsutism. Although this is a relatively smallseries, it is the only one in which'a consistent bio-chemical difference was observed in hirsutism.
It should not be inferred, however, that an in-creased testosterone production rate will be nec-essarily associated with hirsutism. End-organsensitivity may be the determinant in these in-stances. Two of our subjects, Patients 7 and 9,had high testosterone production rates but nohirsutism.
These results differ from those previously re-ported from our laboratory (5) when testosteroneproduction rates were being measured by isotopedilution into urinary metabolites. The reasonsfor the overestimates of testosterone productionrates by this method have been discussed fully(13, 16). The differing results emphasize theimportance of using the metabolic clearance tech-
nique for meaningful assessments of testosteroneproduction.
The extrapolation of testosterone productionrates obtained by the metabolic clearance techniqueto estimates of 24-hour production rates shouldbe cautious. Our patients were studied in thebasal state before arising in the morning. Underthese conditions, the testosterone metabolic clear-ance technique would be maximal; it has beenshown to decrease by as much as 35 %upon stand-ing (17). Changes in metabolic clearance couldthus affect plasma testosterone levels. Further,circadian variations in plasma testosterone levelsin women have not been examined, and signifi-cant changes in these levels would alter the calcu-lated 24-hour production rate. These considera-tions emphasize that all patients should be stud-ied under similar metabolic conditions if com-parisons are to be made.
Androstenedione. Although androstenedionehas been recognized as an androgen, its quantita-tive importance as a precursor of plasma testos-terone in women was demonstrated only recently(7). Mahesh and Greenblatt (18) reported highandrostenedione levels in ovarian vein blood fromwomen with polycystic ovaries. These studiesmake it imperative that any examination of an-drogen overproduction include an analysis of an-drostenedione production and conversion to tes-tosterone.
Plasma androstenedione levels and productionrates in patients with hirsutism or polycysticovaries were about twice those of normal women.This excess androstenedione may be of ovarianorigin in women with polycystic ovaries (18),but its source is unknown in patients with idio-pathic hirsutism. Suppression of the adrenalcortex in a large group of hirsute womenpermittedJayle, Scholler, Mauvais-Jarvis, and Metay (19)to distinguish between adrenal cortical and ovar-ian hirsutism. The more recent demonstration(20) that adrenal suppression markedly decreasesurinary testosterone excretion in most hirsutewomen points to the role of the adrenal cortex inthe secretion of testosterone or its precursors.
Horton and Tait (7) found that 60% of theplasma testosterone of normal women was derivedfrom plasma androstenedione. In our control group49% of the testosterone was so derived, which is inreasonable agreement with the former investigators.
899

C. WAYNEBARDIN AND MORTIMERB. LIPSETT
However, the fractional conversion of androstene-dione to testosterone, [p]BBAT, was lower than thatobserved by Horton and Tait (7). This discrep-ancy is due to the lower MCRTobserved in our
study. It should be noted that this difference inthe MCRTaffects only the calculation of PBT and[PI BBAT. The [p] BBAT was the same in all of our
subjects. Therefore, the higher testosterone pro-
duction rate of the hirsute patient cannot be dueto increased rate of synthesis of testosterone fromplasma androstenedione in the liver or other pe-
ripheral tissue. In the hirsute patients, 26% ofthe plasma testosterone was derived from plasmaandrostenedione. Thus 74% of the 830 /Lg ofplasma testosterone in women with idiopathichirsutism and 1,180 jug in subjects with polycysticovaries must have been either secreted or derivedfrom precursors that did not enter the plasma an-
drostenedione pool.Testosterone secretion from the polycystic ovary
has been demonstrated by several investigators(3, 6, 18). In addition, the adrenal cortex hasbeen shown to secrete testosterone in hirsutewomen (4).
The question of other precursors has not beenexamined thoroughly as yet. The secretion ofpossible precursors such as dehydroepiandros-terone, its sulfate, and 5-androsten-3,3, 17ft-diolhas been reported (21). Wehave estimated thatas much as 50 ,ug per day of blood testosteroneproduction could be derived from the secretion of10 mg per day of dehydroepiandrosterone (22).Tait and Horton (23) have discussed fully thequestion of testosterone precursors other thanandrostenedione and concluded that their quan-
titative importance is small. If these considera-tions are correct, then the increased testosteroneproduction rates in hirsutism are due, in largepart, to testosterone secretion. Differential sup-
pression of the adrenal cortex and ovary will benecessary to assess the relative roles of each glandin the secretion of testosterone and androstene-dione. In preliminary studies in patients withhirsutism, we have observed that dexamethasonecaused a significant reduction of plasma testos-terone in five of nine patients and of plasma an-
drostenedione in all nine patients.Metabolic clearance rates and methodology.
The concept (24) and methods (25) of measuring
metabolic clearances have been clearly outlined byTait and his co-workers. In a study of three menand two women (7), the testosterone metabolicclearance rates were reported to be the same, al-though those of the women were less than thoseof the men. Hudson, Dulmanis, Coghlan, andWintour (26) reported that metabolic clearancerates of testosterone of men and women were thesame, but the details of the infusion technique werenot given. Southren, Tochimoto, Carmody, andIsurugi (27), using the single injection technique,found that men had a greater testosterone meta-bolic clearance than women and in a subsequentabstract (28) stated that the clearance rate byconstant infusion in men was twice that in women.Our studies are in accord with these findings.
The reasons for the discrepancies among thegroups are not immediately apparent, but severalimportant features of this study should be empha-sized.
1) Teflon tubing was used for each infusion,and the rate of infusion of isotope entering the pa-tient was checked by monitoring the infusion ata stopcock behind the infusion needle. Levin,Friedrich, and Labotsky (29) have noted thatpolyethylene tubing may adsorb testosterone andandrostenedione.
2) The purification of the plasma steroids wasextensive in this study, each sample being puri-fied by derivative formation and chromatographyuntil specific activities and 3H/14C ratios agreedwithin 5%o on the last two and generally threemeasurements.
3) In spite of the marked differences in MCGRTamong the groups studied, the MCRAwas thesame in each group and agreed closely with thosereported by Horton and Tait (7). This is goodevidence against systematic errors in the methodfor measuring testosterone metabolic clearancerates.
Therefore, after failing to find methodologic er-rors, we have accepted as fact that testosteronemetabolic clearance rates are higher in men thanin women and that they are higher in women withhirsutism or polycystic ovaries than in normalwomen. The possible reasons for this are of someinterest.
Since the MCRis obtained by dividing the rateof infusion of the radioactive steroid by the plasma
900

TESTOSTERONEAND ANDROSTENEDIONEPRODUCTIONRATES IN HIRSUTE WOMEN 9
radioactivity of that steroid, the MCRwill dependon the volume of distribution and the turnoverrate. In the simplest case, the one compartmentsystem, MCR= Vy where y is the turnover rate(30). Because of this, to compare the actual clear-ance of steroids from the plasma, one must correctthe MCRby some factor proportional to volumeof distribution. Wehave used the calculated sur-face area for this correction. Even after this cor-rection, however, the MCRper square meter washigher in men and in the hirsute women than innormal women.
The linear regression of MCRTper square me-ter with the log PBT is demonstrated by the factthat the function MCRTper square meter per logPBT was the same for each group. This correla-tion suggested the typical dose-response curvecharacteristic of most biologic assays where theresponse is linear only when plotted against thelogarithm of the dose.
The explanation of this phenomenon can be onlyspeculative at present. There are many studiesdemonstrating that hepatic enzyme systems ca-pable of metabolizing androgens are altered bytestosterone. Recently, the presence of a plasmatestosterone-binding protein has been reported(31), and it was suggested that its level washigher in women than in men. This testosterone-binding protein was also observed to increase inpregnancy. Whether the presence of such a bind-ing protein would alter testosterone metabolicclearance rates would depend on the bindingaffinity and capacity of the protein in relation tothe plasma testosterone level. If significantamounts of testosterone were bound, the decreasein metabolic clearance rate would be analogous tothe slowed cortisol turnover rates seen in womenwith increased levels of cortisol-binding globulin.It is of note that the patient with the lowest tes-tosterone metabolic clearance in this study wastaking norethynodrel, 5 mg per day, and mestra-nol, 0.075 mg per day. Our data could thus beinterpreted as being consistent with a depressionof a testosterone-binding protein by increased tes-tosterone production.
AcknowledgmentsWe gratefully acknowledge the technical assistance of
David Collins and Amel French.
References1. Forchielli, E., G. Sorcini, M. S. Nightingale, N.
Brust, R. I. Dorfman, W. H. Perloff, and G.Jacobson. Testosterone in human plasma. Analyt.Biochem. 1963, 5, 416.
2. Hudson, B., J. Coghlan, A. Dulmanis, M. Wintour,and I. Ekkel. The estimation of testosterone inbiological fluids. 1. Testosterone in plasma.Aust. J. exp. Biol. med. Sci. 1963, 41, 235.
3. Dignam, W. J., R. J. Pion, E. J. Lamb, and H. H.Simmer. Plasma androgens in women. II. Pa-tients with polycystic ovaries and hirsutism.Acta endocr. (Kbh.) 1964, 45, 254.
4. Burger, H. G., J. R. Kent, and A. E. Kellie. Deter-mination of testosterone in human peripheral andadrenal venous plasma. J. clin. Endocr. 1964, 24,432.
5. Korenman, S. G., M. A. Kirschner, and M. B. Lip-sett. Testosterone production in normal and viri-lized women and in women with the Stein-Leven-thal syndrome or idiopathic hirsutism. J. clin.Endocr. 1965, 25, 798.
6. Lloyd, C. W., J. Lobotsky, E. J. Segre, T. Kobayashi,M. L. Taymor, and R. E. Batt. Plasma testos-terone and urinary 17-ketosteroids in women withhirsutism and polycystic ovaries. J. clin. Endocr.1966, 26, 314.
7. Horton, R., and J. F. Tait. Androstenedione pro-duction and interconversion rates measured inperipheral blood and studies on the possible site ofits conversion to testosterone. J. clin. Invest. 1966,45, 301.
8. Peterson, R. S., and C. E. Pierce. Methodology ofurinary 17-ketosteroids in Lipids and the SteroidHormones in Clinical Medicine, F. W. Saundersand F. W. Saunders, Jr., Eds. Philadelphia, J. B.Lippincott, 1960, p. 147.
9. Wilson, H., and M. B. Lipsett. Use of periodate oxi-dation in the clinical analysis of urine corticoids.Analyt. Biochem. 1963, 5, 217.
10. Kirschner, M. A., and M. B. Lipsett. The analysisof urinary steroids using gas-liquid chromatog-raphy. Steroids 1964, 3, 277.
11. Kirschner, M. A., M. B. Lipsett, and D. R. Collins.Plasma ketosteroids and testosterone in man: astudy of the pituitary-testicular axis. J. clin. In-vest. 1965, 44, 657.
12. Bardin, C. W., and M. B. Lipsett. Estimation oftestosterone and androstenedione in human periph-eral plasma. Steroids 1967, 9, 71.
13. Korenman, S. G., and M. B. Lipsett. Is testosteroneglucuronoside uniquely derived from plasma tes-tosterone? J. clin. Invest. 1964, 43, 2125.
14. Rongone, E. L. Testosterone metabolism by humanmale mammary skin. Steroids 1966, 7, 489.
15. Kennedy, B. J., and I. T. Nathanson. Effect ofintensive sex steroid hormone therapy in advancedbreast cancer. J. Amer. med. Ass. 1953, 152, 1135.
901

C. WAYNEBARDIN AND MORTIMERB. LIPSETT
16. Tait, J. F., and R. Horton. Some theoretical con-siderations -on the significance of the discrepancyin urinary and blood production rate estimates ofsteroid hormones, particularly in those of testos-terone in young women. Steroids 1964, 4, 365.
17. Lipsett, M. B., H. Wilson, M. A. Kirschner, S. G.Korenman, L. M. Fishman, G. A. Sarfaty, andC. W. Bardin. Studies on Leydig cell physiologyand pathology: secretion and metabolism of tes-tosterone. Recent Progr. Hormone Res. 1966, 22,245.
18. Mahesh, V. B., and R. B. Greenblatt. Steroid se-cretions of the normal and polycystic ovary. Re-cent Progr. Hormone Res. 1964, 20, 341.
19. Jayle, M. F., R. Scholler, P. Mauvais-Jarvis, and S.Metay. Excretion des steroides chez des femmespresentant un virilisme pilaire associe a destroubles du cycle menstruel. Acta Endocr. (Kbh.)1961, 36, 375.
20. Nichols, T., C. A. Nugent, and F. H. Tyler. Gluco-corticoid suppression of urinary testosterone ex-cretion in patients with idiopathic hirsutism. J.clin. Endocr. 1966, 26, 79.
21. Wieland, R. G., C. De Courcy, R. P. Levy, A. P.Zala, and H. Hirschmann. C1902 steroids and someof their precursors in blood from normal humanadrenals. J. clin. Invest. 1965, 44, 159.
22. Korenman, S. G., and M. B. Lipsett. Direct periph-eral conversion of dehydroepiandrosterone to tes-tosterone glucuronoside. Steroids 1965, 5, 509.
23. Tait, J. F., and R. Horton. The in vivo estimation ofblood production and interconversion rates of an-drostenedione and testosterone and the calculationof their secretion rates in Steroid Dynamics, G.
Pincus, T. Nakao, and J. F. Tait, Eds. New York,Academic Press, 1966, p. 393.
24. Tait, J. F. Review: the use of isotopic steroids forthe measurement of production rates in vivo. J.clin. Endocr. 1963, 23, 1285.
25. Tait, J. F., B. Little, S. A. S. Tait, and C. Flood.The metabolic clearance rate of aldosterone inpregnant and nonpregnant subjects estimated byboth single-injection and constant-infusion meth-ods. J. clin. Invest. 1962, 41, 2093.
26. Hudson, B., A. Dulmanis, J. P. Coghlan, and M.Wintour. The measurement of androgen produc-tion in normal subjects. Aust. Ann. Med. 1966,15, 236.
27. Southren, A. L., S. Tochimoto, N. C. Carmody, and-K. Isurugi. Plasma production rates of testosteronein normal adult men and women and in patientswith the syndrome of feminizing testes. J. clin.Endocr. 1965, 25, 1441.
28. Southren, A. L., G. G. Gordon, and S. Tochimoto.Plasma production rates of testosterone in nor-mal men and women; a physiological study usingboth a single injection and constant infusion tech-nique. J. cdin. Invest. 1966, 45, 1075.
29. Levin, J., E. H. Friedrich, and J. Lobotsky. Steroidadsorption with polyethylene tubing. J. clin. En-docr. 1965, 25, 1519.
30. Tait, J. F., and S. Burstein. In vivo studies ofsteroid dynamics in man in The Hormones, G.Pincus, K. V. Thimann, and E. B. Astwood, Eds.New York, Academic Press, 1964, vol. 5, p. 441.
31. Pearlman, W. H., and 0. Crepy. Steroid-protein in-teraction with particular reference to testosterone-binding by human serum. J. biol. Chem. 1967, 242,182.
902