Embed Size (px)
Citation preview

TEVAR For Acute Aortic Syndromes
Luis A. Sanchez, MD FACS Gregorio A. Sicard Distinguished Professor of Surgery and Radiology
Chief, Section of Vascular Surgery Washington University School of Medicine, St. Louis MO

Disclosures
¨ Consultant § Cook Inc. § Medtronic Vascular § W.L. Gore § Aptus
§ Trivascular II § Endologix

Acute Aortic Syndromes
¨ Acute Dissection ¨ Intramural Hematoma ¨ Penetrating Aortic Ulcers ¨ Acute Transection ¨ Aortic Rupture – aneurysms, other
pathology

Suspected Acute Aortic Syndrome MDCT in 373 Emergency Evaluation
¨ N=365 patients; men: 56%; women: 44% ¨ Mean age: 61 years (range 21 to 96); men: 61; women: 69 ¨ 67 cases (18%) positive for acute aortic disorders (n=112)
¤ 23 (34%) acute aortic dissections; A=13 (19%), B=10 (15%) ¤ 14 (21%) acute aortic IMH; A=1 (2%), B=13 (19%) ¤ 20 (30%) acute penetrating ulcer; A=3 (5%), B=17 (25%) ¤ 44 (67%) new or enlarging aortic aneurysms ¤ 11 (17%) acute aortic ruptures
Hayter RG, Radiology 2006; 238:841-852

PUA, IMH, and Dissections
¨ Traditional thinking ¨ Differences in clinical presentation exist
¤ PAU n Older than AD n Exhibit atherosclerotic disease n Cratered intima
¤ Symptomatic vs Asymptomatic ¤ Ascending vs Descending
Spectrum of Disease
IMH Dissection PAU
Sundt T et al., Ann Thor Surg 2007

Penetrating Aortic Ulcer
¨ Evaluated 198 patients ¤ 15 (7.6%) were found to have PAU
n 86.7% in the DTA n Risk of rupture: 40% while observed in ICU
n Most had Type B dissections
¨ Postulated that prognosis may be more serious
Coady et al. J Vas Surg 1998; 27: 1006-16.

Penetrating Aortic Ulcer
¨ Initial treatment with antihypertensive medication, after load reduction
¨ At Risk ¤ Persistent pain, recurrent pain, hemodynamic instability,
enlargement ¤ Ascending aortic ulcers?
¨ Saccular aneurysms, dissections may be the end result

Intramural Hematoma & Penetrating Ulcers
Focal pathology amenable to TEVAR

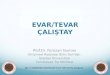
IMH and Thoracic Aneurysm
74 yo female presents with chest pain
Intramural hematoma and thoracic aneurysm TEVAR

Aortic dissections • Type A dissections
• Type B dissections ü Acute
o Complicated / symptomatic
o Uncomplicated /asymptomatic
ü Chronic
Aortic Arch Pathology

Important Historical Data
¨ Indicators of aneurysmal enlargement
¤ Initial Aortic Diameter
n > 4 cm @ 3 months: 70% enlarge
n < 4 cm @ 3 months: 30% enlarge
¤ Patency of False Lumen
¤ Uncontrolled HTN

Aortic dissections
• Type A dissections
ü Open surgical repair
ü Future endografts
Aortic Arch Pathology

Aortic dissections • Type B dissections
ü Acute complicated
o Open surgery vs TEVAR ü Acute uncomplicated
o Medical therapy vs TEVAR ü Chronic
o Open surgery vs hybrid/TEVAR
Aortic Arch Pathology

Acute Aortic Dissection
Goals of therapy → seal the entry point, improve distal perfusion, and prevent early & late complications

Aortic Dissection
47 y.o. presents with chest pain & h/o chronic dissection
• Hypertension
• CXR – left chest whiteout
• CT evaluation
Ø Ruptured Type B dissection

Aortic Dissection
47 y.o. presents with chest pain & h/o chronic dissection
• Hypertension
• CXR – left chest whiteout
• CT evaluation Ø Ruptured Type B dissection

Clinical Trials Type B Aortic Dissection
¨ Completed Trials ¤ INSTEAD - Medtronic (Europe) ¤ TAG (High Risk) - Gore (USA) ¤ ADSORB – Gore (Europe) ¤ CTAG – Gore (USA) ¤ VALIANT - Medtronic
¨ Ongoing Trials ¤ STABLE - Cook

INSTEAD TRIAL • 140 patients with uncomplicated Type B dissections • Best medical therapy (68) vs BMT + endograft (72) • Results at 2 years:
Ø No difference in survival (95.6 vs 88.9%), aortic related deaths or progression of disease Ø Significant difference in aortic remodeling (19.4 vs 91.3%) Ø Continuing patient follow-up
Nienaber et al. Circulation 2009
ADSORB TRIAL • 250 patients with acute uncomplicated Type B dissections • Randomized to BMT vs BMT + endograft
European Dissection Trials

Clinical Trials Acute Complicated Type B Aortic Dissections
CTAG and STABLE TRIALS
TAG 08-01 SVS-CPC STABLE
Subjects 50 (%) 85 (%) 40 (%) Adverse Events 20 (40) 32 (37.6) n/a
Death 4 (8) 9 (10.6) 2 (5) MI 2 (4) 1 (1.2) n/a
Stroke 7 (14) 8 (9.4) 3 (7.5) Renal Failure (+HD) 3 (6) 8 (9.4) 5 (12.5)
Paralysis/paraparesis 3 (6) 8 (9.4) 1 (2.5) Bowel Ischemia 2 (4) 3 (3.5) 0
Post implant Type A dissection 5 (10) 8 (9.4) 2 (5)
Cambria RP et al., J Vasc Surg 2012; Lombardi JV et al, J Vasc Surg 2012

Acute Complicated Dissection
5 year treatment of acute complicated type B dissections • Experience from 2005 to 2012 – 50 patients
• 20% rupture, 48% malperfusion, 34% pain/impending rupture
• 20% adjunctive procedures
• Results – mean follow up of 33.8 months ü Mortality – 0%, Stroke – 2%, Paraplegia – 2%, Hemodialysis – 4%
ü Type I endoleak – 10%, pressurized false lumen – 8%
ü Retrograde Type A – 2%
ü Reinterventions – 26%
Hanna JM et al., JVS 2013

Uncomplicated Type B Dissection: Long-Term Data
Fattori et al., JACC Cardiovasc Interv 2013
IRAD Data Medical TEVAR Patients 853 276
In-hospital mortality 8.7% 10.9%
1 year mortality 9.8% 8.1%
5 year survival 29% 15.5%
INSTEAD Medical TEVAR Patients -140 68 72
2-5 yr All cause mortality 16.9% 0%
2-5 yr Aortic specific mortality 16.9% 0%
2-5 yr Progression 28.1% 4.1%
5 yr All cause mortality 19.3% 11.1%
5 yr Aortic specific mortality 19.3% 6.9%
5 yr Progression 46.1% 27%
Nienaber CA et al., Circ Cardiovasc Interv 2013

Complex Aortic Dissections
• Involve the aortic arch
• Associated with
complex arch/thoracic
aneurysms

Complex Aortic Dissections
• Similar treatment considerations as arch aneurysms:
> Debranching with ascending aortic inflow
> Elephant trunk procedure

Complex Aortic Dissections
• Debranching and elephant trunk techniques:
> can be useful in this patient population
> preference for the elephant trunk technique § allows repair of arch/branch involvement
§ provides an excellent proximal seal landing zone for TEVAR
§ Can be performed in a single stage

Complex Aortic Dissections
1 Stage Treatment of TA with Elephant trunk 68 yo female with arch aneurysm

Complex Aortic Dissections

Aortic Dissection Case
¨ 55 yo male presented hypertension, abdominal and chest pain.
• Dissection extending to the iliacs
• True lumen narrowing at celiac/SMA
• Infrarenal aortic occlusion
• Right iliac occlusion
• Limited flow to right kidney

Aortic Dissection Case
¨ 55 yo male presented hypertension, abdominal and chest pain.

Aortic Dissection Case
¨ 55 yo male presented hypertension, abdominal and chest pain.
• After thoracic aortic endograft:
ü Better flow into the right kidney
ü Persistent infrarenal narrowing
ü Persistent right EIA occlusion

Aortic Dissection Case
¨ 55 yo male presented hypertension, abdominal and chest pain.
Aortic stent Renal stent
Right EIA stent

Aortic Dissection Case
¨ 55 yo male presented hypertension, abdominal and chest pain.
Kissing iliac stents

Aortic Dissection Case ¨ 55 yo male presented with HTN,
abdominal and chest pain.

Complex Aortic Dissections
• Other complications: > Type A retrograde dissection
> Endoleaks –
> Type IA or B –
> Type II -
> Type III –
> Continued false lumen flow and expansion

Acute Aortic Syndromes
Conclusions: • TEVAR: ü is the treatment of choice for suitable
patients with symptomatic intramural hematomas, penetrating ulcers and traumatic lesions.
ü is the treatment of choice for acute complicated Type B dissections.
ü has a role in selected patients with chronic dissections.
ü may have an increasing role in the treatment of acute uncomplicated Type B dissections but more data is needed.
ü has a potential future role in the treatment of Type A dissections.

Thank you


Approved Device options
• C-TAG graft ü 22-45mm, 200mm long
• Valiant graft ü 22-46mm, up to 200mm long ü Captivia delivery system
Endovascular Grafts

Thoracic Aneurysms
§ Most commonly treated lesion
§ Other patients, like those with
an acute aortic syndrome, can
potentially benefit
§ Aortic trauma, dissections,
rupture, penetrating ulcers,
intramural hematomas

Indications for Intervention
¨ Acute Symptomatic/Complicated Dissections ¤ Presence of malperfusion ¤ Presence of rupture ¤ Persistent symptoms – uncontrolled pain
¨ Subacute ¤ Presence of enlargement/aneurysmal degeneration
n >6 cm
¨ Chronic ¤ 3 months to years
n Aneurysmal dilatation (>6cm thoracic, 5.5cm abdominal)

Aortic Dissection
46 y.o. presents with chest pain • Hypotension (80/50)
• LE weakness
• CT evaluation Ø Ruptured Type B dissection

Acute Aortic Type B Dissection
46 y.o. with ruptured dissection • Emergent endovascular repair
Ø Hemodynamic stability
Ø Resolution of LE symptoms

Acute Aortic Type B Dissection
46 y.o. with ruptured dissection
• Secondary procedure
Ø Additional TAG
Ø Aortic stent
Ø Carotid stent
• Additional intervention
Ø Right renal covered stent

Penetrating Aortic Ulcer
¨ Presentation similar to dissection and many times confused with AD ¤ Focal outpouching of contrast
¨ Older patients ¨ More common in descending TA ¨ Focal area of dissection limited by existing
atherosclerotic disease

Complex Aortic Dissections
• Technical details: > Standard elephant trunk procedure with specific size graft to match
the chosen endograft
> Antegrade wire introduction into the true lumen
> Evaluation with TEE and/or IVUS
> Femoral access to the true lumen if needed
> Reevaluation distal flow after TEVAR