Embed Size (px)
Citation preview
• •
• B
UL
LE
TIN
• •
•B i m o n t h l y u p d a t e t o t h e Te x a s M e d i c a i d P r o v i d e r P r o c e d u r e s M a n u a l
Texas MedicaidSome specials we are offering in this bulletin include:• An article on Emergency Diagnosis Code changes on page 4• A reminder of Medicare Crossovers on page 9• An article about Pulse Oximeter Changes on page 12Be sure to help yourself.
November/December 2003 No. 176
Bulletin Contents, No. 176
All Providers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
New Texas Medicaid Claims and Primary Care Case Management (PCCM) Administrator .......... 2CLIA Waived Test Update ..................................................................................................... 2Changes to Outpatient Professional Evaluation and Management (E/M) Services .................... 2Emergency Diagnosis .......................................................................................................... 4Federal Matching Percentage Rate Changes .......................................................................... 7Injection Progesterone ......................................................................................................... 7Mental Health and Mental Retardation (MHMR) Service Coordination Reimbursement .............. 7Modifier 55 Clarification ...................................................................................................... 8Pegfilgrastim ....................................................................................................................... 8Programmable Implantable Pumps ........................................................................................ 8Recommendations to Enhance Compliance with Texas Medicaid Fee-for-Service Hospital Billing .................................................................................................................... 8Reminder of Medicare Crossovers ........................................................................................ 9Revised Influenza Vaccine Recommendations ........................................................................ 9SHARS Rates SFY03 ......................................................................................................... 10Tracheostomy Tube and Oxygen Changes ............................................................................ 10
Health Insurance Portability and Accountability Act (HIPAA) Update . . . . . . . . . . . . 11
Attention Home Health Agencies HIPAA Update ................................................................... 11HIPAA Information Regarding Authorizations ........................................................................ 11HIPAA Special Bulletin No. 170 Clarification ......................................................................... 11Federally Qualified Health Centers (FQHCs) and Rural Health Clinics (RHCs) Revenue Code .... 11
THSteps - CCP Providers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
Pulse Oximeter Changes .................................................................................................... 12
THSteps Providers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
THSteps Policy Clarification ................................................................................................ 13
Excluded Providers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
Forms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
Enrolling in the Electronic Funds Transfer Program ............................................................... 16NHIC Electronic Funds Transfer Authorization Agreement ...................................................... 17Pulse Oximeter Form ......................................................................................................... 18Provider Information Change Form ...................................................................................... 19
www.eds-nhic.comNational Heritage Insurance Company (NHIC) is the insurer and contract administrator for the Texas Medicaid
Program under contract with the Texas Health and Human Services Commission (HHSC)
Indicates updated information
All Providers
New Texas Medicaid Claims and Primary Care Case Management (PCCM) Administrator
Effective January 1, 2004, a coalition of contractors called the Texas Medicaid & Healthcare Partnership (TMHP), headed by Affiliated Computer Services, Inc. (ACS), will assume Medicaid Claims Administrator duties for the State of Texas, under contract with the Health and Human Services Commission (HHSC). TMHP will also be the administrator for the Medicaid Managed Care Primary Care Case Management (PCCM) model known as the Texas Health Network. Providers will continue to use the same telephone numbers they currently use to commununicate with NHIC and the Texas Health Network. Additionally, providers will continue to use the same post office box addresses to communicate with NHIC.
Note: The Texas Health Network addresses will be changing. The new addresses will be published in future TMHP transition bulletins. The Texas Health Network mail will be forwarded from the existing addresses for a short period of time to ensure a smooth transition.
Refer to: October 2003 TMHP Transition Bulletin, No. 1, sent to your office in October for more information.
Future TMHP transition bulletins are scheduled for distri-bution in November and December 2003 and will provide transition updates. ■
CLIA Waived Test Update
Effective December 8, 2000, Clinical Laboratory Improvement Amendments (CLIA) waived test 82962, Blood glucose by glucose monitoring devices cleared by the Food and Drug Adminstration (FDA) for home use, is not a benefit because of its home use specification by clinical laboratory providers. ■
Changes to Outpatient Professional Evaluation and Management (E/M) Services
Effective for dates of service on or after September 1, 2003, the following outpatient profes-sional E/M services changes are in place:
• Procedure code 94760 is denied as part of another procedure when billed on the same day by the same provider as an office (99201 through 99205 and 99211 through 99215) or outpatient consultation visit (99241 through 99245)
• Procedure codes 99050 and 99056 are reimbursed only once per day when billed by the same provider
• Procedure codes 99354 and 99355 are denied within precare days when billed by the same provider
• Procedure codes 99354 and 99355 are denied within extended postcare days with a related diagnosis when billed by the same provider
• Procedure codes 99354 and 99355 are denied within 90 days of surgery for a related diagnosis when billed by a different provider unless billed with modifier 55
• Procedure codes 99050, 99056, 99354, and 99355 are denied within six weeks following surgery for the same diagnosis when billed by the same provider
• Procedure codes 99050, 99056, 99354, and 99355 are denied within six weeks following anesthesia service for a related diagnosis when billed by the same provider
Procedure codes 99204, 99205, 99215, 99243, 99244, 99245, 99354, and 99355 are denied as part of another procedure when billed for the same date of service the same provider as procedure codes 92002, 92004, 92012, 92014, 92265, 92270, 92275, 92285, 92286, 92287, 95930, 95930-26, and 95930-TC:
Procedure Code Description
92002 Ophthalmological services: medical examination and evaluation with initiation of diagnostic and treatment program; intermediate, new patient
92004 Ophthalmological services: medical examination and evaluation with initiation of diagnostic and treatment program; comprehensive, new patient, one or more visits
92012 Ophthalmological services: medical examination and evaluation, with initiation or continuation of diagnostic and treatment program; intermediate, established patient
92014 Ophthalmological services: comprehensive, established patient, one or more visits
Texas Medicaid Bulletin, No. 176 2 November/December 2003
92265 Needle oculeolectromyography, one or more extraocular muscles, one or both eyes, with interpretation and report
92270 Electro-oculography with interpretation and report
92275 Electroretinography with interpretation and report
92285 External ocular photography with interpretation and report for documentation of medical progress (e.g., close-up photography, slit lamp photography, goniophotography, stereo-photography)
92286 Special anterior segment photography with interpretation and report; with specular endothelial microscopy and cell count
92287 Special anterior segment photography with interpretation and report; with fluorescein angiography
94760 Noninvasive ear or pulse oximetry for oxygen saturation; single determination
95930 Visual evoked potential (VEP) testing central nervous system, checkerboard or flash
95930-26 Visual evoked potential (VEP) testing central nervous system, checkerboard or flash – professional component
95930-TC Visual evoked potential (VEP) testing central nervous system, checkerboard or flash – technical component
99050 Services requested after office hours in addition to basic service
99056 Services provided at request of patient in a location other than physician’s office which are normally provided in the office
99201 Office or other outpatient visit for the evaluation and management of a new patient, which requires these three components:
• a problem-focused history • a problem-focused examination• straightforward medical decision making
99202 Office or other outpatient visit for the evaluation and management of a new patient, which requires these three components:
• an expanded problem-focused history • an expanded problem-focused examination• straightforward medical decision making
99203 Office or other outpatient visit for the evaluation and management of a new patient, which requires these three components:
• a detailed history • a detailed examination• medical decision making of low complexity
Procedure Code Description
99204 Office or other outpatient visit for the evaluation and management of a new patient, which requires these three components:
• a comprehensive history• a comprehensive examination• medical decision making of moderate
complexity
99205 Office or other outpatient visit for the evaluation and management of a new patient, which requires these three components:
• a comprehensive history • a comprehensive examination• medical decision making of high complexity
99211 Office or other outpatient visit for the evaluation and management of an established patient, that may not require the presence of a physician. Usually, the presenting problem(s) are minimal. Typically, five minutes are spent performing or supervising these services.
99212 Office or other outpatient visit for the evaluation and management of an established patient, which requires at least two of these three components:
• a problem-focused history • a problem-focused examination • straightforward medical decision making
99213 Office or other outpatient visit for the evaluation and management of an established patient, which requires at least two of these three components:
• an expanded problem-focused history • an expanded problem-focused examination • medical decision making of low complexity
99214 Office or other outpatient visit for the evaluation and management of an established patient, which requires at least two of these three components:
• a detailed history • a detailed examination • medical decision making of moderate
complexity
99215 Office or other outpatient visit for the evaluation and management of an established patient, which requires at least two of these three components:
• a comprehensive history • a comprehensive examination • medical decision making of high complexity
99241 Office consultation for a new or established patient, which requires these three key components:
• a problem-focused history • a problem-focused examination• straightforward medical decision making
99242 Office consultation for a new or established patient, which requires these three key components:
• an expanded problem-focused history • an expanded problem-focused examination• straightforward medical decision making
Procedure Code Description
November/December 2003 3 Texas Medicaid Bulletin, No. 176
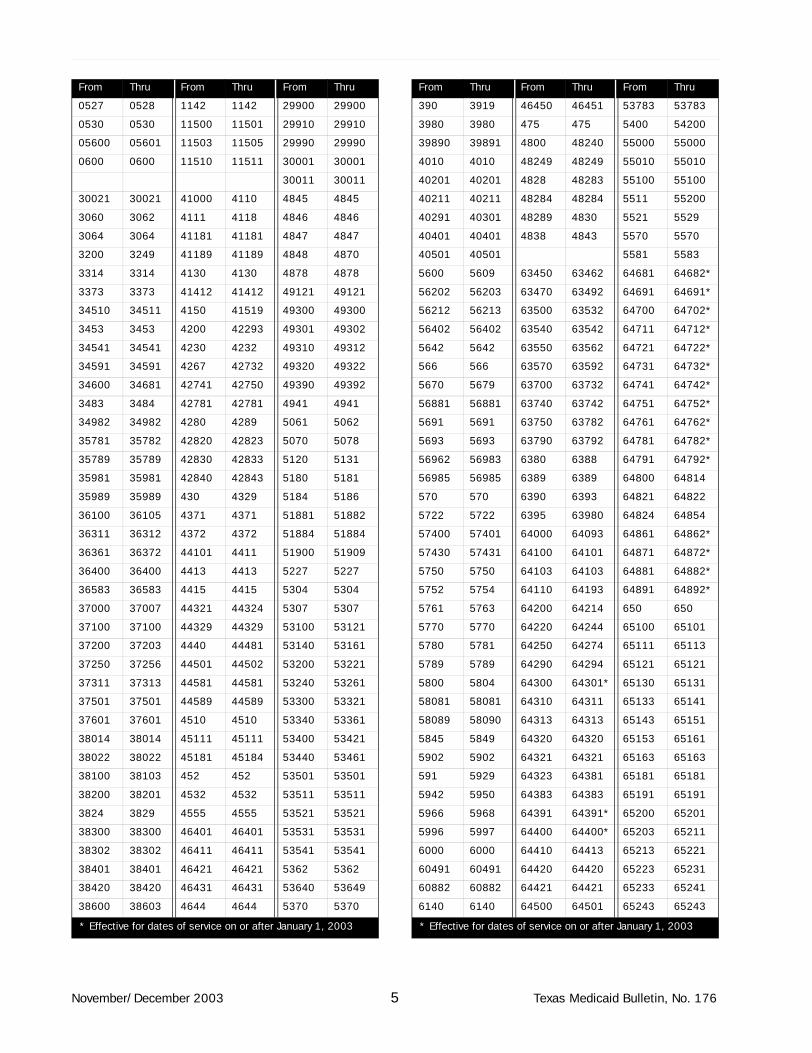
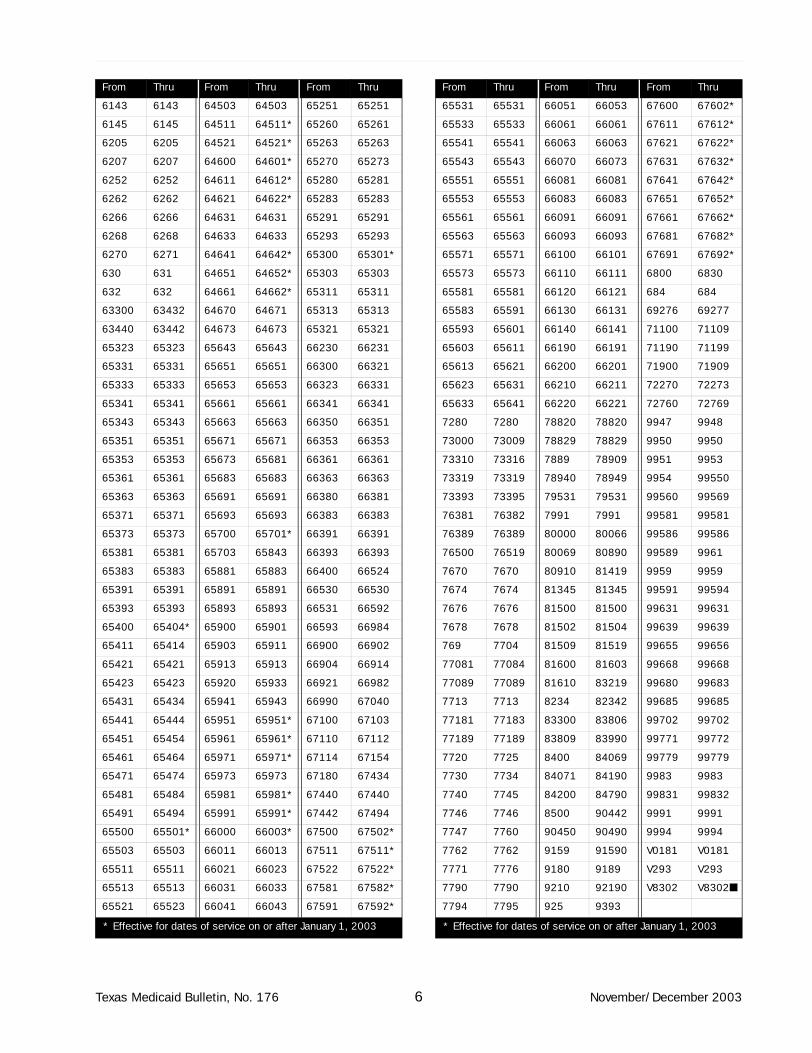
Emergency Diagnosis
The Texas Medicaid Program limits reimbursement of some categories to services based on documentation of an emergency medical condition. Emergency medical condition is defined on page 1-6 of the 2003 Texas Medicaid Provider Procedures Manual. Reimbursement is limited to emergency medical conditions for the following:
• Medical treatment provided to a lock-in (limited) client without a referral from the designated physician on page 1-5 of the 2003 Texas Medicaid Provider Procedures Manual
• Medical treatment provided to clients with “emergency only” coverage on page 1-4 of the 2003 Texas Medicaid Provider Procedures Manual
Following is a list of diagnoses that are considered emergency medical conditions by the Texas Medicaid Program. Those diagnoses indicated with an asterisk (*) are effective for dates of service on or after January 1, 2003.
99243 Office consultation for a new or established patient, which requires these three key components:
• a detailed history • a detailed examination • medical decision making of low complexity
99244 Office consultation for a new or established patient, which requires these three key components:
• a comprehensive history • a comprehensive examination• medical decision making of moderate
complexity
99245 Office consultation for a new or established patient, which requires these three key components:
• a comprehensive history • a comprehensive examination • medical decision making of high complexity
99354 Prolonged physician service in the office or other outpatient setting requiring direct (face-to-face) patient contact beyond the usual service (e.g., prolonged care and treatment of an acute asthmatic patient in an outpatient setting); first hour (List separately in addition to code for office or other outpatient Evaluation and Management service)
99355 Prolonged physician service in the office or other outpatient setting requiring direct (face-to-face) patient contact beyond the usual service (e.g., prolonged care and treatment of an acute asthmatic patient in an outpatient setting); each additional 30 minutes (List separately in addition to code for prolonged physician service) ■
Procedure Code Description
From Thru From Thru From Thru
0010 0020 061 0632 11513 11515
0021 0030 0638 0659 1160 1160
0031 0031 0661 0661 1171 1171
00320 0050 0664 0664 1175 1175
0051 00581 0700 0700 1221 1221
00589 0060 07020 07023 1300 1300
0069 0069 07041 07049 1303 1304
0090 0093 0706 0706 1362 1363
01710 01716 071 071 24201 24201
01800 0200 0721 0722 24211 24211
0202 0205 0730 0730 24221 24221
0212 0212 0741 0741 24231 24231
0221 0221 07420 07423 24241 24241
0223 0223 075 075 24281 24281
0230 0233 0786 0786 24291 24291
0260 0261 07981 07981 2450 2450
0270 0270 080 0819 2463 2463
0272 0272 0820 0839 25010 25033
0310 0310 0848 0848 2510 2510
0320 0320 0860 0860 2521 2521
0321 03284 0863 0863 27702 27703
03289 0330 0865 0865 27709 27709
0331 0341 09041 09042 28262 28262
035 035 0913 0913 2832 2832
0360 0369 09181 09181 2851 2851
037 03811 0930 09324 29011 29012
03819 03819 09381 09382 29020 29020
0382 03849 09389 09389 2903 2903
0391 0391 0942 0942 29041 29042
0400 0400 09487 09487 2910 2910
04082 04082 0951 0952 2913 2913
04500 04503 0980 09817 29211 29212
04510 04510 09840 09843 29281 29281
04512 04593 09882 09886 2930 2930
0463 0463 1000 1000 29540 29540
0470 0470 10081 10081 29604 29604
0479 0479 10089 1009 29624 29624
0491 0491 1124 1125 29644 29644
0512 0512 11280 11283 29654 29654
0520 0521 1140 1140 2983 2983
* Effective for dates of service on or after January 1, 2003
Texas Medicaid Bulletin, No. 176 4 November/December 2003
0527 0528 1142 1142 29900 29900
0530 0530 11500 11501 29910 29910
05600 05601 11503 11505 29990 29990
0600 0600 11510 11511 30001 30001
30011 30011
30021 30021 41000 4110 4845 4845
3060 3062 4111 4118 4846 4846
3064 3064 41181 41181 4847 4847
3200 3249 41189 41189 4848 4870
3314 3314 4130 4130 4878 4878
3373 3373 41412 41412 49121 49121
34510 34511 4150 41519 49300 49300
3453 3453 4200 42293 49301 49302
34541 34541 4230 4232 49310 49312
34591 34591 4267 42732 49320 49322
34600 34681 42741 42750 49390 49392
3483 3484 42781 42781 4941 4941
34982 34982 4280 4289 5061 5062
35781 35782 42820 42823 5070 5078
35789 35789 42830 42833 5120 5131
35981 35981 42840 42843 5180 5181
35989 35989 430 4329 5184 5186
36100 36105 4371 4371 51881 51882
36311 36312 4372 4372 51884 51884
36361 36372 44101 4411 51900 51909
36400 36400 4413 4413 5227 5227
36583 36583 4415 4415 5304 5304
37000 37007 44321 44324 5307 5307
37100 37100 44329 44329 53100 53121
37200 37203 4440 44481 53140 53161
37250 37256 44501 44502 53200 53221
37311 37313 44581 44581 53240 53261
37501 37501 44589 44589 53300 53321
37601 37601 4510 4510 53340 53361
38014 38014 45111 45111 53400 53421
38022 38022 45181 45184 53440 53461
38100 38103 452 452 53501 53501
38200 38201 4532 4532 53511 53511
3824 3829 4555 4555 53521 53521
38300 38300 46401 46401 53531 53531
38302 38302 46411 46411 53541 53541
38401 38401 46421 46421 5362 5362
38420 38420 46431 46431 53640 53649
38600 38603 4644 4644 5370 5370
From Thru From Thru From Thru
* Effective for dates of service on or after January 1, 2003
390 3919 46450 46451 53783 53783
3980 3980 475 475 5400 54200
39890 39891 4800 48240 55000 55000
4010 4010 48249 48249 55010 55010
40201 40201 4828 48283 55100 55100
40211 40211 48284 48284 5511 55200
40291 40301 48289 4830 5521 5529
40401 40401 4838 4843 5570 5570
40501 40501 5581 5583
5600 5609 63450 63462 64681 64682*
56202 56203 63470 63492 64691 64691*
56212 56213 63500 63532 64700 64702*
56402 56402 63540 63542 64711 64712*
5642 5642 63550 63562 64721 64722*
566 566 63570 63592 64731 64732*
5670 5679 63700 63732 64741 64742*
56881 56881 63740 63742 64751 64752*
5691 5691 63750 63782 64761 64762*
5693 5693 63790 63792 64781 64782*
56962 56983 6380 6388 64791 64792*
56985 56985 6389 6389 64800 64814
570 570 6390 6393 64821 64822
5722 5722 6395 63980 64824 64854
57400 57401 64000 64093 64861 64862*
57430 57431 64100 64101 64871 64872*
5750 5750 64103 64103 64881 64882*
5752 5754 64110 64193 64891 64892*
5761 5763 64200 64214 650 650
5770 5770 64220 64244 65100 65101
5780 5781 64250 64274 65111 65113
5789 5789 64290 64294 65121 65121
5800 5804 64300 64301* 65130 65131
58081 58081 64310 64311 65133 65141
58089 58090 64313 64313 65143 65151
5845 5849 64320 64320 65153 65161
5902 5902 64321 64321 65163 65163
591 5929 64323 64381 65181 65181
5942 5950 64383 64383 65191 65191
5966 5968 64391 64391* 65200 65201
5996 5997 64400 64400* 65203 65211
6000 6000 64410 64413 65213 65221
60491 60491 64420 64420 65223 65231
60882 60882 64421 64421 65233 65241
6140 6140 64500 64501 65243 65243
From Thru From Thru From Thru
* Effective for dates of service on or after January 1, 2003
November/December 2003 5 Texas Medicaid Bulletin, No. 176
6143 6143 64503 64503 65251 65251
6145 6145 64511 64511* 65260 65261
6205 6205 64521 64521* 65263 65263
6207 6207 64600 64601* 65270 65273
6252 6252 64611 64612* 65280 65281
6262 6262 64621 64622* 65283 65283
6266 6266 64631 64631 65291 65291
6268 6268 64633 64633 65293 65293
6270 6271 64641 64642* 65300 65301*
630 631 64651 64652* 65303 65303
632 632 64661 64662* 65311 65311
63300 63432 64670 64671 65313 65313
63440 63442 64673 64673 65321 65321
65323 65323 65643 65643 66230 66231
65331 65331 65651 65651 66300 66321
65333 65333 65653 65653 66323 66331
65341 65341 65661 65661 66341 66341
65343 65343 65663 65663 66350 66351
65351 65351 65671 65671 66353 66353
65353 65353 65673 65681 66361 66361
65361 65361 65683 65683 66363 66363
65363 65363 65691 65691 66380 66381
65371 65371 65693 65693 66383 66383
65373 65373 65700 65701* 66391 66391
65381 65381 65703 65843 66393 66393
65383 65383 65881 65883 66400 66524
65391 65391 65891 65891 66530 66530
65393 65393 65893 65893 66531 66592
65400 65404* 65900 65901 66593 66984
65411 65414 65903 65911 66900 66902
65421 65421 65913 65913 66904 66914
65423 65423 65920 65933 66921 66982
65431 65434 65941 65943 66990 67040
65441 65444 65951 65951* 67100 67103
65451 65454 65961 65961* 67110 67112
65461 65464 65971 65971* 67114 67154
65471 65474 65973 65973 67180 67434
65481 65484 65981 65981* 67440 67440
65491 65494 65991 65991* 67442 67494
65500 65501* 66000 66003* 67500 67502*
65503 65503 66011 66013 67511 67511*
65511 65511 66021 66023 67522 67522*
65513 65513 66031 66033 67581 67582*
65521 65523 66041 66043 67591 67592*
From Thru From Thru From Thru
* Effective for dates of service on or after January 1, 2003
65531 65531 66051 66053 67600 67602*
65533 65533 66061 66061 67611 67612*
65541 65541 66063 66063 67621 67622*
65543 65543 66070 66073 67631 67632*
65551 65551 66081 66081 67641 67642*
65553 65553 66083 66083 67651 67652*
65561 65561 66091 66091 67661 67662*
65563 65563 66093 66093 67681 67682*
65571 65571 66100 66101 67691 67692*
65573 65573 66110 66111 6800 6830
65581 65581 66120 66121 684 684
65583 65591 66130 66131 69276 69277
65593 65601 66140 66141 71100 71109
65603 65611 66190 66191 71190 71199
65613 65621 66200 66201 71900 71909
65623 65631 66210 66211 72270 72273
65633 65641 66220 66221 72760 72769
7280 7280 78820 78820 9947 9948
73000 73009 78829 78829 9950 9950
73310 73316 7889 78909 9951 9953
73319 73319 78940 78949 9954 99550
73393 73395 79531 79531 99560 99569
76381 76382 7991 7991 99581 99581
76389 76389 80000 80066 99586 99586
76500 76519 80069 80890 99589 9961
7670 7670 80910 81419 9959 9959
7674 7674 81345 81345 99591 99594
7676 7676 81500 81500 99631 99631
7678 7678 81502 81504 99639 99639
769 7704 81509 81519 99655 99656
77081 77084 81600 81603 99668 99668
77089 77089 81610 83219 99680 99683
7713 7713 8234 82342 99685 99685
77181 77183 83300 83806 99702 99702
77189 77189 83809 83990 99771 99772
7720 7725 8400 84069 99779 99779
7730 7734 84071 84190 9983 9983
7740 7745 84200 84790 99831 99832
7746 7746 8500 90442 9991 9991
7747 7760 90450 90490 9994 9994
7762 7762 9159 91590 V0181 V0181
7771 7776 9180 9189 V293 V293
7790 7790 9210 92190 V8302 V8302■
7794 7795 925 9393
From Thru From Thru From Thru
* Effective for dates of service on or after January 1, 2003
Texas Medicaid Bulletin, No. 176 6 November/December 2003
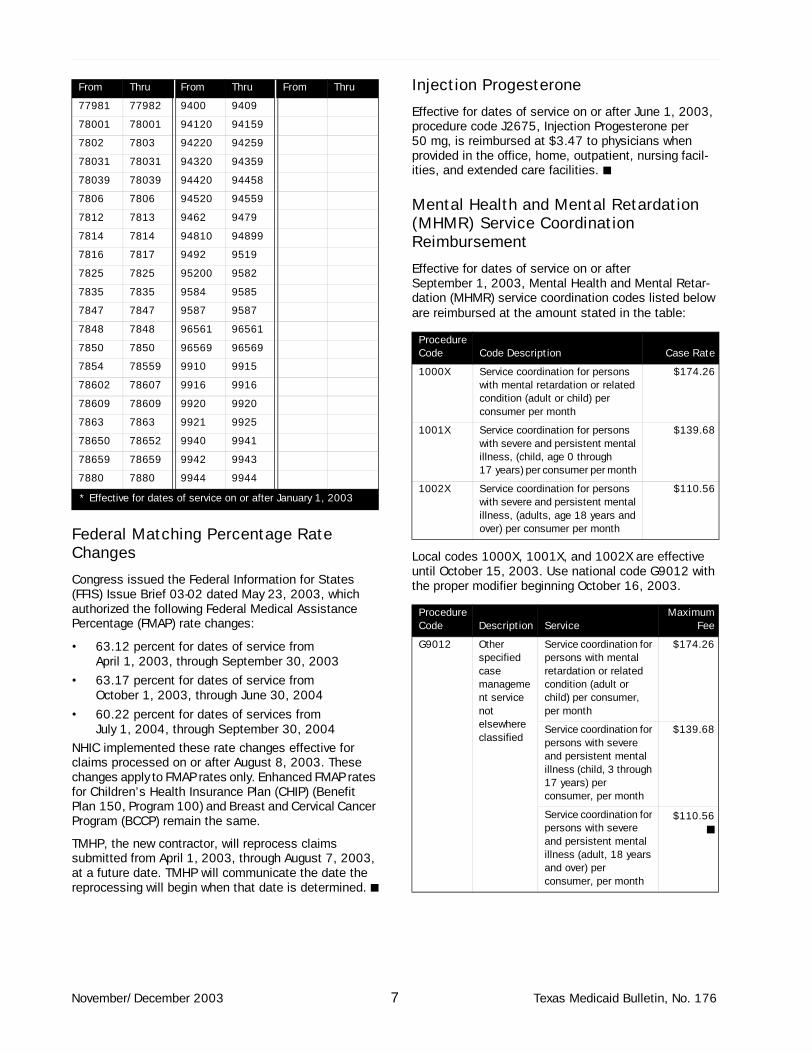
Federal Matching Percentage Rate Changes
Congress issued the Federal Information for States (FFIS) Issue Brief 03-02 dated May 23, 2003, which authorized the following Federal Medical Assistance Percentage (FMAP) rate changes:
• 63.12 percent for dates of service from April 1, 2003, through September 30, 2003
• 63.17 percent for dates of service from October 1, 2003, through June 30, 2004
• 60.22 percent for dates of services from July 1, 2004, through September 30, 2004
NHIC implemented these rate changes effective for claims processed on or after August 8, 2003. These changes apply to FMAP rates only. Enhanced FMAP rates for Children’s Health Insurance Plan (CHIP) (Benefit Plan 150, Program 100) and Breast and Cervical Cancer Program (BCCP) remain the same.
TMHP, the new contractor, will reprocess claims submitted from April 1, 2003, through August 7, 2003, at a future date. TMHP will communicate the date the reprocessing will begin when that date is determined. ■
Injection Progesterone
Effective for dates of service on or after June 1, 2003, procedure code J2675, Injection Progesterone per 50 mg, is reimbursed at $3.47 to physicians when provided in the office, home, outpatient, nursing facil-ities, and extended care facilities. ■
Mental Health and Mental Retardation (MHMR) Service Coordination Reimbursement
Effective for dates of service on or after September 1, 2003, Mental Health and Mental Retar-dation (MHMR) service coordination codes listed below are reimbursed at the amount stated in the table:
Local codes 1000X, 1001X, and 1002X are effective until October 15, 2003. Use national code G9012 with the proper modifier beginning October 16, 2003.
77981 77982 9400 9409
78001 78001 94120 94159
7802 7803 94220 94259
78031 78031 94320 94359
78039 78039 94420 94458
7806 7806 94520 94559
7812 7813 9462 9479
7814 7814 94810 94899
7816 7817 9492 9519
7825 7825 95200 9582
7835 7835 9584 9585
7847 7847 9587 9587
7848 7848 96561 96561
7850 7850 96569 96569
7854 78559 9910 9915
78602 78607 9916 9916
78609 78609 9920 9920
7863 7863 9921 9925
78650 78652 9940 9941
78659 78659 9942 9943
7880 7880 9944 9944
From Thru From Thru From Thru
* Effective for dates of service on or after January 1, 2003
Procedure Code Code Description Case Rate
1000X Service coordination for persons with mental retardation or related condition (adult or child) per consumer per month
$174.26
1001X Service coordination for persons with severe and persistent mental illness, (child, age 0 through 17 years) per consumer per month
$139.68
1002X Service coordination for persons with severe and persistent mental illness, (adults, age 18 years and over) per consumer per month
$110.56
Procedure Code Description Service
MaximumFee
G9012 Other specified case management service not elsewhere classified
Service coordination for persons with mental retardation or related condition (adult or child) per consumer, per month
$174.26
Service coordination for persons with severe and persistent mental illness (child, 3 through 17 years) per consumer, per month
$139.68
Service coordination for persons with severe and persistent mental illness (adult, 18 years and over) per consumer, per month
$110.56■
November/December 2003 7 Texas Medicaid Bulletin, No. 176
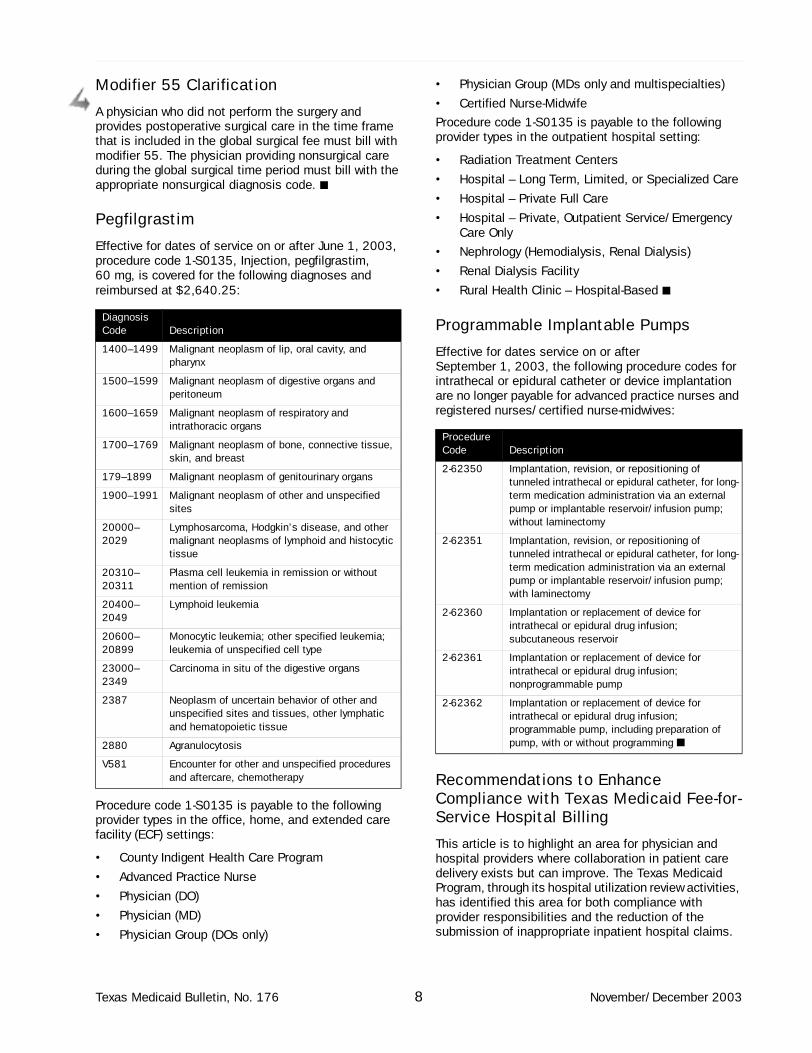
Modifier 55 Clarification
A physician who did not perform the surgery and provides postoperative surgical care in the time frame that is included in the global surgical fee must bill with modifier 55. The physician providing nonsurgical care during the global surgical time period must bill with the appropriate nonsurgical diagnosis code. ■
Pegfilgrastim
Effective for dates of service on or after June 1, 2003, procedure code 1-S0135, Injection, pegfilgrastim, 60 mg, is covered for the following diagnoses and reimbursed at $2,640.25:
Procedure code 1-S0135 is payable to the following provider types in the office, home, and extended care facility (ECF) settings:
• County Indigent Health Care Program
• Advanced Practice Nurse
• Physician (DO)
• Physician (MD)
• Physician Group (DOs only)
• Physician Group (MDs only and multispecialties)
• Certified Nurse-Midwife
Procedure code 1-S0135 is payable to the following provider types in the outpatient hospital setting:
• Radiation Treatment Centers
• Hospital – Long Term, Limited, or Specialized Care
• Hospital – Private Full Care
• Hospital – Private, Outpatient Service/Emergency Care Only
• Nephrology (Hemodialysis, Renal Dialysis)
• Renal Dialysis Facility
• Rural Health Clinic – Hospital-Based ■
Programmable Implantable Pumps
Effective for dates service on or after September 1, 2003, the following procedure codes for intrathecal or epidural catheter or device implantation are no longer payable for advanced practice nurses and registered nurses/certified nurse-midwives:
Recommendations to Enhance Compliance with Texas Medicaid Fee-for-Service Hospital Billing
This article is to highlight an area for physician and hospital providers where collaboration in patient care delivery exists but can improve. The Texas Medicaid Program, through its hospital utilization review activities, has identified this area for both compliance with provider responsibilities and the reduction of the submission of inappropriate inpatient hospital claims.
Diagnosis Code Description
1400–1499 Malignant neoplasm of lip, oral cavity, and pharynx
1500–1599 Malignant neoplasm of digestive organs and peritoneum
1600–1659 Malignant neoplasm of respiratory and intrathoracic organs
1700–1769 Malignant neoplasm of bone, connective tissue, skin, and breast
179–1899 Malignant neoplasm of genitourinary organs
1900–1991 Malignant neoplasm of other and unspecified sites
20000–2029
Lymphosarcoma, Hodgkin’s disease, and other malignant neoplasms of lymphoid and histocytic tissue
20310–20311
Plasma cell leukemia in remission or without mention of remission
20400–2049
Lymphoid leukemia
20600–20899
Monocytic leukemia; other specified leukemia; leukemia of unspecified cell type
23000–2349
Carcinoma in situ of the digestive organs
2387 Neoplasm of uncertain behavior of other and unspecified sites and tissues, other lymphatic and hematopoietic tissue
2880 Agranulocytosis
V581 Encounter for other and unspecified procedures and aftercare, chemotherapy
Procedure Code Description
2-62350 Implantation, revision, or repositioning of tunneled intrathecal or epidural catheter, for long-term medication administration via an external pump or implantable reservoir/infusion pump; without laminectomy
2-62351 Implantation, revision, or repositioning of tunneled intrathecal or epidural catheter, for long-term medication administration via an external pump or implantable reservoir/infusion pump; with laminectomy
2-62360 Implantation or replacement of device for intrathecal or epidural drug infusion; subcutaneous reservoir
2-62361 Implantation or replacement of device for intrathecal or epidural drug infusion; nonprogrammable pump
2-62362 Implantation or replacement of device for intrathecal or epidural drug infusion; programmable pump, including preparation of pump, with or without programming ■
Texas Medicaid Bulletin, No. 176 8 November/December 2003

HHSC is required to operate a utilization review program that controls the utilization of Medicaid inpatient hospital services for hospitals reimbursed under the prospective payment system. An admission review of paid, inpatient hospital claims is conducted retrospec-tively to evaluate the medical necessity of inpatient admissions. For utilization review purposes, medical necessity means the patient has a condition requiring treatment that can be safely provided only in the inpatient setting. When medical necessity is not estab-lished, the hospital inpatient claim is denied and the inappropriate payment to the hospital is recovered.
To enhance compliance with Texas Medicaid fee-for-service hospital billing and decrease the submission of inappropriate inpatient hospital claims, HHSC’s Utili-zation Review Department is offering the following suggestions:
• Physicians and hospital personnel (primarily case managers, utilization review, billing) should become familiar with the Hospital Inpatient Screening Criteria used by the HHSC staff in performing reviews of hospital medical records related to paid, inpatient hospital claims. The criteria provide guide-lines for review staff to assist with the determination of medical necessity of inpatient stays. The criteria may be found on the HHSC Web site, www.hhsc.state.tx.us/OIE/index.html, Medicaid Hospital Inpatient Screening Criteria.
• Consideration should be given to initially admitting patients in observation status if the physician feels that it is reasonable to expect that the patient may be able to be discharged within 24 hours. In the Texas Medicaid Program, if the patient is initially admitted in observation status (per physician order), the stay is more than 24 hours, and the hospital submits an inpatient claim, the hospital is given the opportunity to rebill the first 24 hours of services on an outpatient claim if the inpatient claim is subsequently denied per retrospective utili-zation review.
• When a patient is admitted to the hospital as an inpatient and is discharged in less than 24 hours, the hospital may request that the physician change the admission order from inpatient status to outpa-tient observation status. This billing practice is acceptable under the Texas Medicaid Program when the physician makes the changes to the admitting order from inpatient status to outpatient obser-vation status before the hospital submits the claim for payment.
This correction in admission status avoids errors in billing and the potential need for a more lengthy appeal process. If the physician admitting orders do not accurately reflect the services provided, the hospital inpatient claim may be denied and the inappropriate payment recovered from both the hospital and the admitting physician.
HHSC encourages physician and hospital providers to consider these recommendations and support appro-priate utilization of inpatient hospital services. ■
Reminder of Medicare Crossovers
If a claim for a Medicare/Medicaid client does not electronically crossover to NHIC within 60 days of Medicare’s payment, the Medicare crossover must be filed on paper. This policy applies to all Medicare claims, including Medicare adjustments.
Refer to: Section 1, Paragraph 1.5.1 of the 2003 Texas Medicaid Provider Procedures Manual for specific instructions on filing a Medicare crossover on paper to NHIC. ■
Revised Influenza Vaccine Recommendations
Note: This article was run previously under a different title.
The Centers for Disease Control and Prevention (CDC) has announced an expansion of the routine recommen-dations for influenza vaccine during the 2003 through 2004 influenza season. All children eligible for the Texas Vaccines for Children Program (TVFC) must be vacci-nated in accordance with the revised Advisory Committee on Immunization Practices (ACIP) and the Federal Vaccines for Children Program resolution. (A copy of the resolution can be downloaded from www.cdc.gov/mmwr/PDF/rr/rr5208.pdf.) Eligible groups are identified as:
• Children age 6 months through 23 months*
• Children and adolescents age 6 months through 18 years with chronic disorders of the pulmonary or cardiovascular systems, including asthma
• Children and adolescents age 6 months through 18 years who have required regular medical follow-up or hospitalization during the preceding year because of chronic metabolic diseases (including diabetes mellitus), renal dysfunction, hemoglolbino-pathies, or immunosuppression (including immunosuppression caused by medications)
• Children and adolescents age 6 months through 18 years who are receiving long-term aspirin therapy and may therefore be at risk for developing Reye syndrome after influenza
• Children and adolescents age 2 through 18 years who are household contacts of persons in high-risk groups (e.g., people aged 65 years or older, trans-plant recipients, people with AIDS, and children younger than age 2 years)
November/December 2003 9 Texas Medicaid Bulletin, No. 176
• Children and adolescents age 6 months through 18 years who are residents of nursing facilities and other chronic-care facilities that house people at any age who have chronic medical conditions
• Adolescent females younger than age 19 years who are in the second or third trimester of pregnancy during influenza season
Influenza vaccine orders for Medicaid children and all TVFC-eligible children are placed in September and follow the TVFC vaccine ordering procedures currently in place for routine childhood vaccines. Vaccines were delivered in October.
Contact the nearest public health region (PHR) immuni-zation program manager with questions regarding influenza vaccine recommendations. For influenza vaccines ordering information call Lisa Davis at 800-252-9152 or 512-458-7284.
*Correction Note: In the September/October 2003 Texas Medicaid Bulletin, No. 175, the age range was incorrectly listed as 6 months through 23 years. ■
SHARS Rates SFY03
The correct state fiscal year (SFY) 2003 School Health and Related Services (SHARS) rates for SFY03 listed in the original memorandum was effective September 1, 2002, rather than July 1, 2003, or May 1, 2003. ■
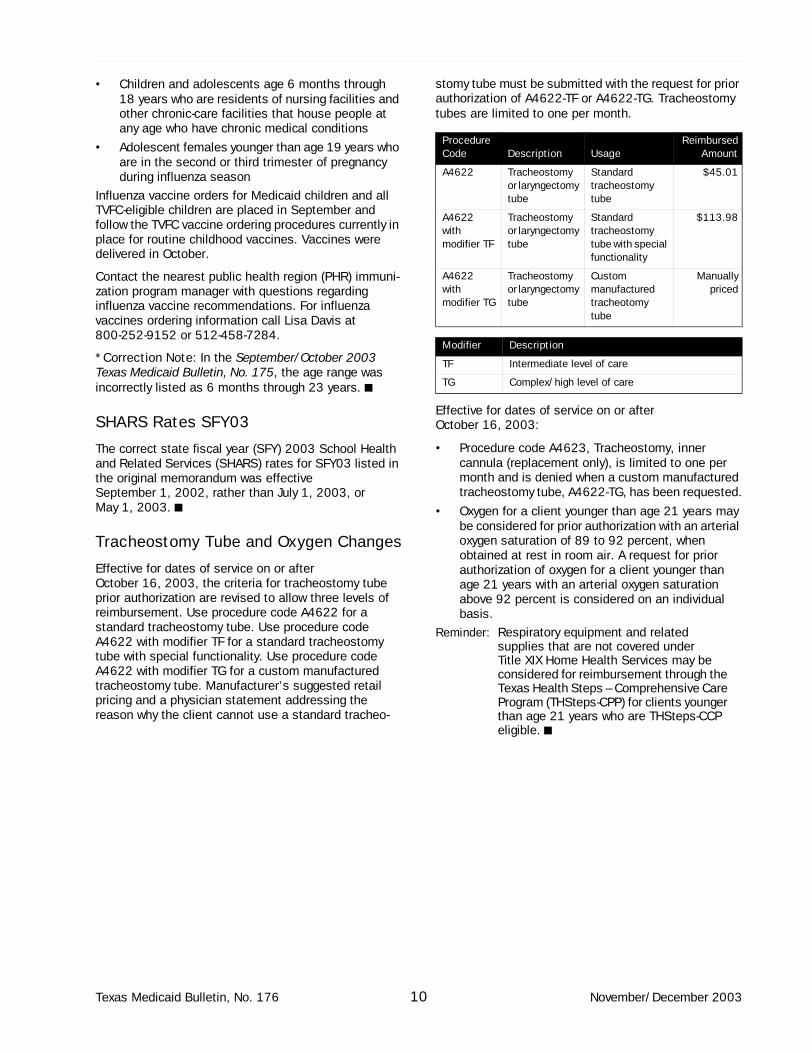
Tracheostomy Tube and Oxygen Changes
Effective for dates of service on or after October 16, 2003, the criteria for tracheostomy tube prior authorization are revised to allow three levels of reimbursement. Use procedure code A4622 for a standard tracheostomy tube. Use procedure code A4622 with modifier TF for a standard tracheostomy tube with special functionality. Use procedure code A4622 with modifier TG for a custom manufactured tracheostomy tube. Manufacturer’s suggested retail pricing and a physician statement addressing the reason why the client cannot use a standard tracheo-
stomy tube must be submitted with the request for prior authorization of A4622-TF or A4622-TG. Tracheostomy tubes are limited to one per month.
Effective for dates of service on or after October 16, 2003:
• Procedure code A4623, Tracheostomy, inner cannula (replacement only), is limited to one per month and is denied when a custom manufactured tracheostomy tube, A4622-TG, has been requested.
• Oxygen for a client younger than age 21 years may be considered for prior authorization with an arterial oxygen saturation of 89 to 92 percent, when obtained at rest in room air. A request for prior authorization of oxygen for a client younger than age 21 years with an arterial oxygen saturation above 92 percent is considered on an individual basis.
Reminder: Respiratory equipment and related supplies that are not covered under Title XIX Home Health Services may be considered for reimbursement through the Texas Health Steps – Comprehensive Care Program (THSteps-CPP) for clients younger than age 21 years who are THSteps-CCP eligible. ■
Procedure Code Description Usage
ReimbursedAmount
A4622 Tracheostomy or laryngectomy tube
Standard tracheostomy tube
$45.01
A4622 with modifier TF
Tracheostomy or laryngectomy tube
Standard tracheostomy tube with special functionality
$113.98
A4622 with modifier TG
Tracheostomy or laryngectomy tube
Custom manufactured tracheotomy tube
Manuallypriced
Modifier Description
TF Intermediate level of care
TG Complex/high level of care
Texas Medicaid Bulletin, No. 176 10 November/December 2003

Health Insurance Portability and Accountability Act (HIPAA) Update
Attention Home Health Agencies HIPAA Update
All home health agencies must provide a revenue code in addition to the national procedure code T1015 on the electronic 837I claim transaction. The revenue code entered is not used in claims processing but is required for the claim to be HIPAA-compliant. If you use TDHconnect to file your electronic claims, you may enter the appropriate HCPCS procedure code in the procedure code field and leave the revenue code field blank, as TDHconnect 3.0 populates a revenue code automati-cally for you. If you do not use TDHconnect to file your electronic claims, check with your software vendor to determine if you need to enter the revenue code along with the appropriate HCPCS procedure code. ■
HIPAA Information Regarding Authorizations
For most of the current authorizations that contain local procedure codes for dates of service on or after October 16, 2003, NHIC will be able to convert the existing authorization to the appropriate national procedure code (and modifier, when appropriate). However, NHIC cannot convert 68 local procedure codes on the provider’s behalf (refer to HIPAA Special Bulletin Update, No. 174, Traditional, Managed Care, and MCO SSI Authorizations on page 28). Providers with an approved authorization for one of those 68 local procedure codes for a date of service on or after October 16, 2003, must resubmit the original paperwork and indicate the national procedure code (and modifier, when appropriate) that are used for dates of service on or after October 16, 2003. Providers may begin resub-mitting authorization requests for one of those 68 local procedure codes and new authorization requests on September 2, 2003. ■
HIPAA Special Bulletin No. 170 Clarification
Effective for dates of service on or after October 16, 2003, all federally qualified health centers (FQHCs) and rural health clinics (RHCs) will use national procedure code T1015, Clinic visit, encounter, all inclusive, for encounters. The appropriate national modifier must be used with T1015 to indicate the rendering providers: AM, Physician; SA, Nurse practi-
tioner; U7, Physician Assistant; TE, Visiting Nurse if LPN or LVN; TD, Visiting Nurse if RN; AJ, Social Worker; or TH, Obstetrical treatment for postpartum services.
Refer to: HIPAA Special Bulletin, No. 170, Appendix B, Local Modifier to National Modifier Table.
Modifier AJ is a national modifier and is not listed in Appendix B and was inadvertently omitted from the article titled Encounters in the FQHC section of the HIPAA Special Bulletin, No. 170. ■
Federally Qualified Health Centers (FQHCs) and Rural Health Clinics (RHCs) Revenue Code
All FQHCs and RHCs must provide a revenue code in addition to the national procedure code T1015 on the electronic 837I claim transaction. The revenue code entered is not used in claims processing but is required for the claim to be HIPAA-compliant.
All FQHCs must bill THSteps medical services on the HIPAA-compliant 837P claim transaction and THSeps dental services on the HIPAA-complaint 837D, which do not require a revenue code.
All RHCs must bill the following services on the HIPAA-compliant 837P claim transaction, which does not require a revenue code: THSteps medical, immuniza-tions outside THSteps medical checkup, family planning services (including implantable contraceptive capsules provision, insertion, or removal), outpatient hospital (including emergency room services), and inpatient hospital.
If you use TDHconnect to file your electronic claims, you may enter the appropriate Healthcare Comon Procedure Code System (HCPCS) procedure code in the procedure code field and leave the revenue code field blank, as TDHconnect 3.0 populates a revenue code behind the scenes for you. If you do not use TDHconnect to file your electronic claims, check with your software vendor to determine if you need to enter the revenue code along with the appropriate HCPCS procedure code. ■
November/December 2003 11 Texas Medicaid Bulletin, No. 176
THSteps - CCP Providers
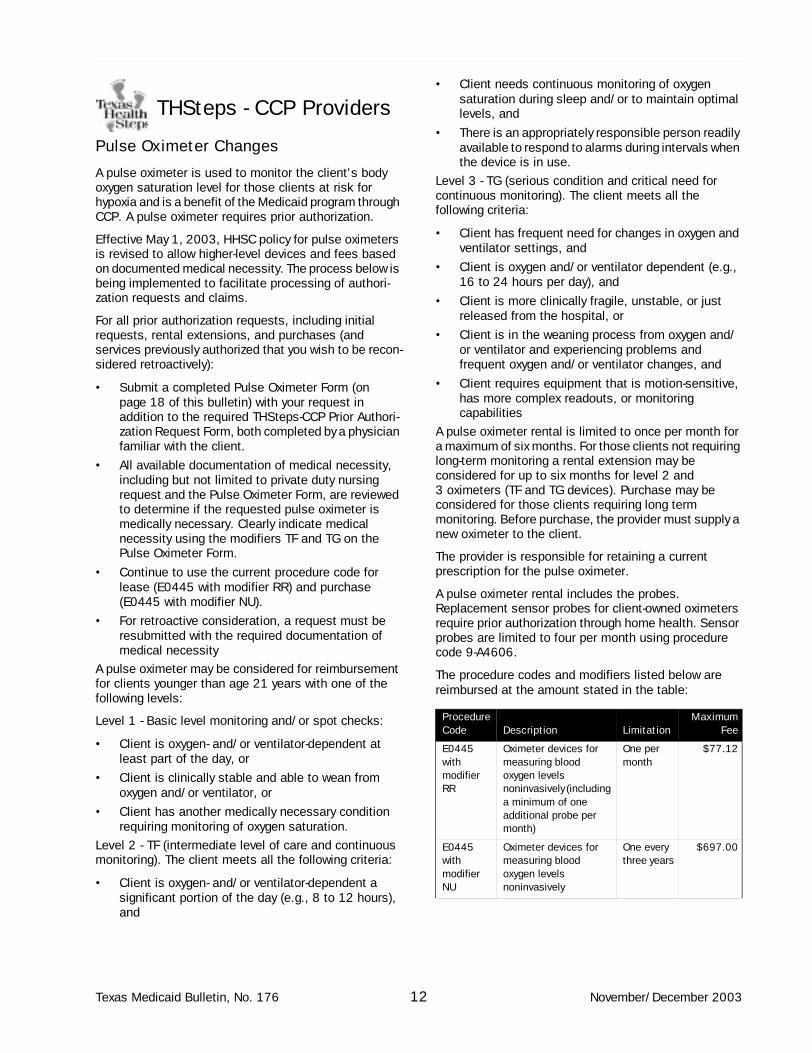
Pulse Oximeter Changes
A pulse oximeter is used to monitor the client’s body oxygen saturation level for those clients at risk for hypoxia and is a benefit of the Medicaid program through CCP. A pulse oximeter requires prior authorization.
Effective May 1, 2003, HHSC policy for pulse oximeters is revised to allow higher-level devices and fees based on documented medical necessity. The process below is being implemented to facilitate processing of authori-zation requests and claims.
For all prior authorization requests, including initial requests, rental extensions, and purchases (and services previously authorized that you wish to be recon-sidered retroactively):
• Submit a completed Pulse Oximeter Form (on page 18 of this bulletin) with your request in addition to the required THSteps-CCP Prior Authori-zation Request Form, both completed by a physician familiar with the client.
• All available documentation of medical necessity, including but not limited to private duty nursing request and the Pulse Oximeter Form, are reviewed to determine if the requested pulse oximeter is medically necessary. Clearly indicate medical necessity using the modifiers TF and TG on the Pulse Oximeter Form.
• Continue to use the current procedure code for lease (E0445 with modifier RR) and purchase (E0445 with modifier NU).
• For retroactive consideration, a request must be resubmitted with the required documentation of medical necessity
A pulse oximeter may be considered for reimbursement for clients younger than age 21 years with one of the following levels:
Level 1 - Basic level monitoring and/or spot checks:
• Client is oxygen- and/or ventilator-dependent at least part of the day, or
• Client is clinically stable and able to wean from oxygen and/or ventilator, or
• Client has another medically necessary condition requiring monitoring of oxygen saturation.
Level 2 - TF (intermediate level of care and continuous monitoring). The client meets all the following criteria:
• Client is oxygen- and/or ventilator-dependent a significant portion of the day (e.g., 8 to 12 hours), and
• Client needs continuous monitoring of oxygen saturation during sleep and/or to maintain optimal levels, and
• There is an appropriately responsible person readily available to respond to alarms during intervals when the device is in use.
Level 3 - TG (serious condition and critical need for continuous monitoring). The client meets all the following criteria:
• Client has frequent need for changes in oxygen and ventilator settings, and
• Client is oxygen and/or ventilator dependent (e.g., 16 to 24 hours per day), and
• Client is more clinically fragile, unstable, or just released from the hospital, or
• Client is in the weaning process from oxygen and/or ventilator and experiencing problems and frequent oxygen and/or ventilator changes, and
• Client requires equipment that is motion-sensitive, has more complex readouts, or monitoring capabilities
A pulse oximeter rental is limited to once per month for a maximum of six months. For those clients not requiring long-term monitoring a rental extension may be considered for up to six months for level 2 and 3 oximeters (TF and TG devices). Purchase may be considered for those clients requiring long term monitoring. Before purchase, the provider must supply a new oximeter to the client.
The provider is responsible for retaining a current prescription for the pulse oximeter.
A pulse oximeter rental includes the probes. Replacement sensor probes for client-owned oximeters require prior authorization through home health. Sensor probes are limited to four per month using procedure code 9-A4606.
The procedure codes and modifiers listed below are reimbursed at the amount stated in the table:
Procedure Code Description Limitation
MaximumFee
E0445 with modifier RR
Oximeter devices for measuring blood oxygen levels noninvasively (including a minimum of one additional probe per month)
One per month
$77.12
E0445 with modifier NU
Oximeter devices for measuring blood oxygen levels noninvasively
One every three years
$697.00
Texas Medicaid Bulletin, No. 176 12 November/December 2003
THSteps Providers
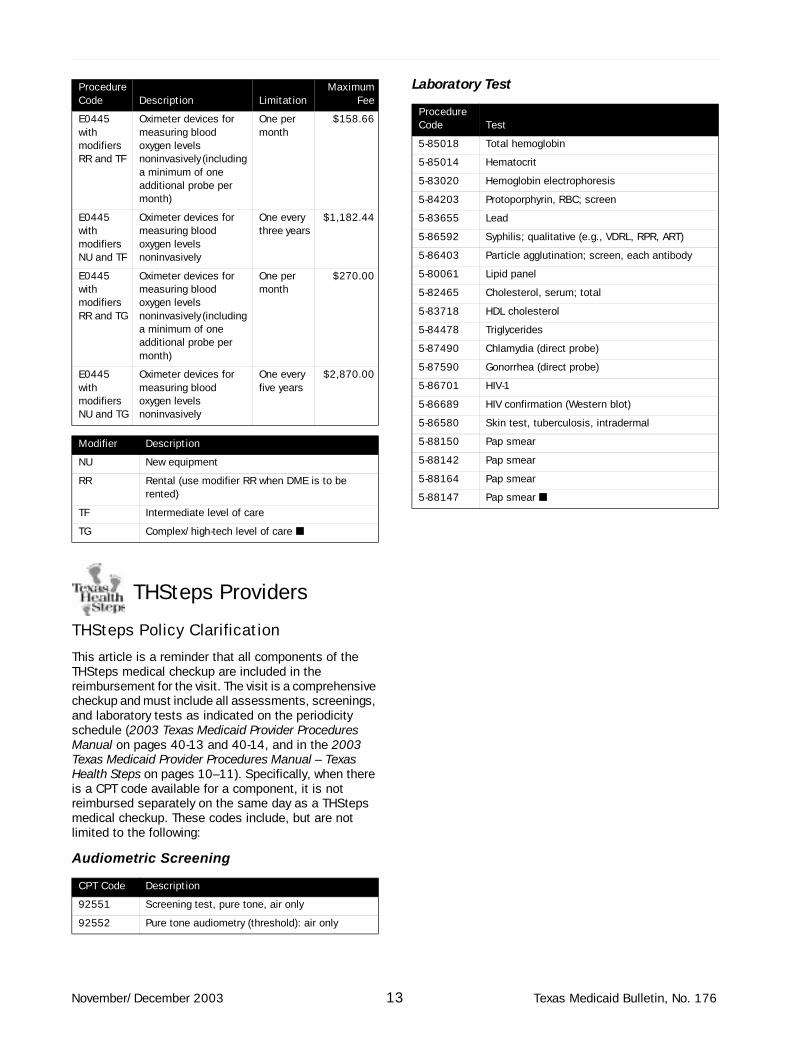
THSteps Policy Clarification
This article is a reminder that all components of the THSteps medical checkup are included in the reimbursement for the visit. The visit is a comprehensive checkup and must include all assessments, screenings, and laboratory tests as indicated on the periodicity schedule (2003 Texas Medicaid Provider Procedures Manual on pages 40-13 and 40-14, and in the 2003 Texas Medicaid Provider Procedures Manual – Texas Health Steps on pages 10–11). Specifically, when there is a CPT code available for a component, it is not reimbursed separately on the same day as a THSteps medical checkup. These codes include, but are not limited to the following:
Audiometric Screening
Laboratory Test
E0445 with modifiers RR and TF
Oximeter devices for measuring blood oxygen levels noninvasively (including a minimum of one additional probe per month)
One per month
$158.66
E0445 with modifiers NU and TF
Oximeter devices for measuring blood oxygen levels noninvasively
One every three years
$1,182.44
E0445 with modifiers RR and TG
Oximeter devices for measuring blood oxygen levels noninvasively (including a minimum of one additional probe per month)
One per month
$270.00
E0445 with modifiers NU and TG
Oximeter devices for measuring blood oxygen levels noninvasively
One every five years
$2,870.00
Modifier Description
NU New equipment
RR Rental (use modifier RR when DME is to be rented)
TF Intermediate level of care
TG Complex/high-tech level of care ■
CPT Code Description
92551 Screening test, pure tone, air only
92552 Pure tone audiometry (threshold): air only
Procedure Code Description Limitation
MaximumFee
Procedure Code Test
5-85018 Total hemoglobin
5-85014 Hematocrit
5-83020 Hemoglobin electrophoresis
5-84203 Protoporphyrin, RBC; screen
5-83655 Lead
5-86592 Syphilis; qualitative (e.g., VDRL, RPR, ART)
5-86403 Particle agglutination; screen, each antibody
5-80061 Lipid panel
5-82465 Cholesterol, serum; total
5-83718 HDL cholesterol
5-84478 Triglycerides
5-87490 Chlamydia (direct probe)
5-87590 Gonorrhea (direct probe)
5-86701 HIV-1
5-86689 HIV confirmation (Western blot)
5-86580 Skin test, tuberculosis, intradermal
5-88150 Pap smear
5-88142 Pap smear
5-88164 Pap smear
5-88147 Pap smear ■
November/December 2003 13 Texas Medicaid Bulletin, No. 176
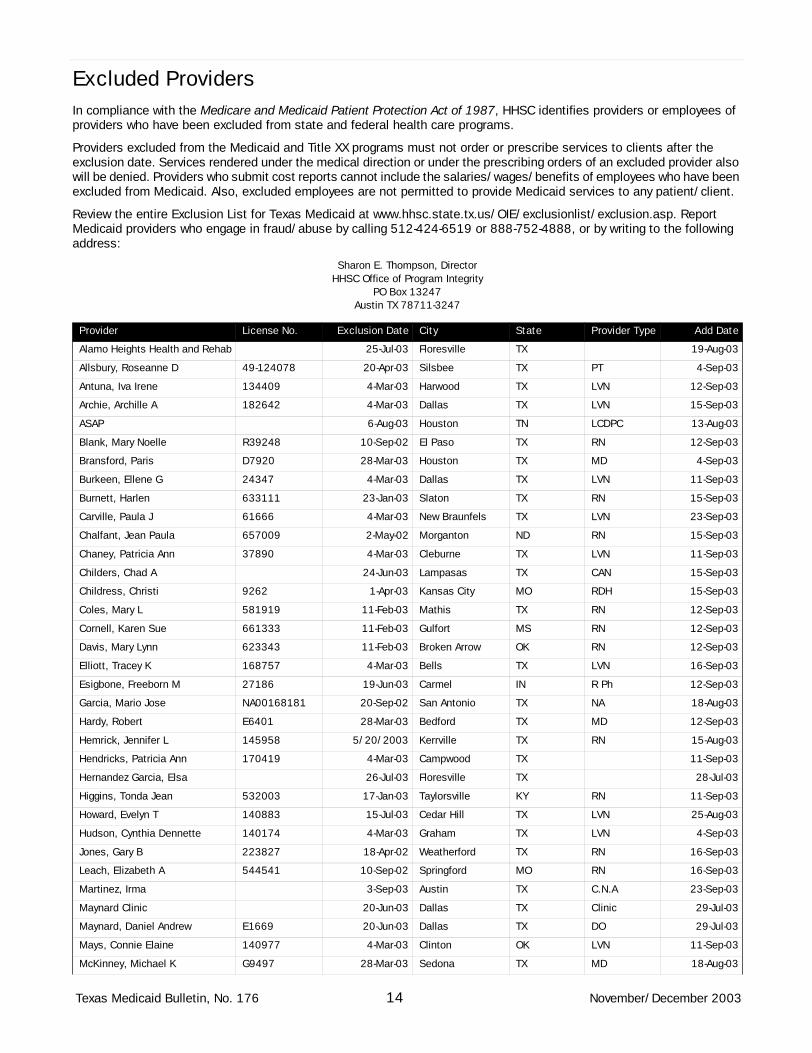
Excluded ProvidersIn compliance with the Medicare and Medicaid Patient Protection Act of 1987, HHSC identifies providers or employees of providers who have been excluded from state and federal health care programs.
Providers excluded from the Medicaid and Title XX programs must not order or prescribe services to clients after the exclusion date. Services rendered under the medical direction or under the prescribing orders of an excluded provider also will be denied. Providers who submit cost reports cannot include the salaries/wages/benefits of employees who have been excluded from Medicaid. Also, excluded employees are not permitted to provide Medicaid services to any patient/client.
Review the entire Exclusion List for Texas Medicaid at www.hhsc.state.tx.us/OIE/exclusionlist/exclusion.asp. Report Medicaid providers who engage in fraud/abuse by calling 512-424-6519 or 888-752-4888, or by writing to the following address:
Sharon E. Thompson, Director HHSC Office of Program Integrity
PO Box 13247Austin TX 78711-3247
Provider License No. Exclusion Date City State Provider Type Add Date
Alamo Heights Health and Rehab 25-Jul-03 Floresville TX 19-Aug-03
Allsbury, Roseanne D 49-124078 20-Apr-03 Silsbee TX PT 4-Sep-03
Antuna, Iva Irene 134409 4-Mar-03 Harwood TX LVN 12-Sep-03
Archie, Archille A 182642 4-Mar-03 Dallas TX LVN 15-Sep-03
ASAP 6-Aug-03 Houston TN LCDPC 13-Aug-03
Blank, Mary Noelle R39248 10-Sep-02 El Paso TX RN 12-Sep-03
Bransford, Paris D7920 28-Mar-03 Houston TX MD 4-Sep-03
Burkeen, Ellene G 24347 4-Mar-03 Dallas TX LVN 11-Sep-03
Burnett, Harlen 633111 23-Jan-03 Slaton TX RN 15-Sep-03
Carville, Paula J 61666 4-Mar-03 New Braunfels TX LVN 23-Sep-03
Chalfant, Jean Paula 657009 2-May-02 Morganton ND RN 15-Sep-03
Chaney, Patricia Ann 37890 4-Mar-03 Cleburne TX LVN 11-Sep-03
Childers, Chad A 24-Jun-03 Lampasas TX CAN 15-Sep-03
Childress, Christi 9262 1-Apr-03 Kansas City MO RDH 15-Sep-03
Coles, Mary L 581919 11-Feb-03 Mathis TX RN 12-Sep-03
Cornell, Karen Sue 661333 11-Feb-03 Gulfort MS RN 12-Sep-03
Davis, Mary Lynn 623343 11-Feb-03 Broken Arrow OK RN 12-Sep-03
Elliott, Tracey K 168757 4-Mar-03 Bells TX LVN 16-Sep-03
Esigbone, Freeborn M 27186 19-Jun-03 Carmel IN R Ph 12-Sep-03
Garcia, Mario Jose NA00168181 20-Sep-02 San Antonio TX NA 18-Aug-03
Hardy, Robert E6401 28-Mar-03 Bedford TX MD 12-Sep-03
Hemrick, Jennifer L 145958 5/20/2003 Kerrville TX RN 15-Aug-03
Hendricks, Patricia Ann 170419 4-Mar-03 Campwood TX 11-Sep-03
Hernandez Garcia, Elsa 26-Jul-03 Floresville TX 28-Jul-03
Higgins, Tonda Jean 532003 17-Jan-03 Taylorsville KY RN 11-Sep-03
Howard, Evelyn T 140883 15-Jul-03 Cedar Hill TX LVN 25-Aug-03
Hudson, Cynthia Dennette 140174 4-Mar-03 Graham TX LVN 4-Sep-03
Jones, Gary B 223827 18-Apr-02 Weatherford TX RN 16-Sep-03
Leach, Elizabeth A 544541 10-Sep-02 Springford MO RN 16-Sep-03
Martinez, Irma 3-Sep-03 Austin TX C.N.A 23-Sep-03
Maynard Clinic 20-Jun-03 Dallas TX Clinic 29-Jul-03
Maynard, Daniel Andrew E1669 20-Jun-03 Dallas TX DO 29-Jul-03
Mays, Connie Elaine 140977 4-Mar-03 Clinton OK LVN 11-Sep-03
McKinney, Michael K G9497 28-Mar-03 Sedona TX MD 18-Aug-03
Texas Medicaid Bulletin, No. 176 14 November/December 2003
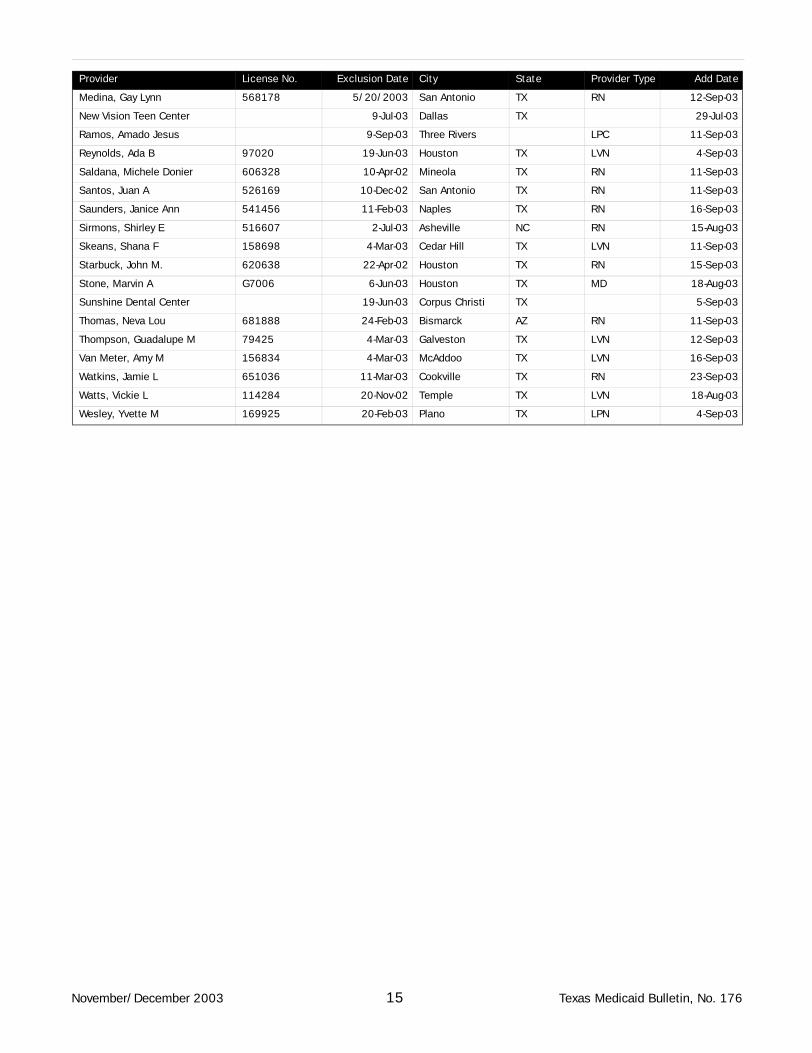
Medina, Gay Lynn 568178 5/20/2003 San Antonio TX RN 12-Sep-03
New Vision Teen Center 9-Jul-03 Dallas TX 29-Jul-03
Ramos, Amado Jesus 9-Sep-03 Three Rivers LPC 11-Sep-03
Reynolds, Ada B 97020 19-Jun-03 Houston TX LVN 4-Sep-03
Saldana, Michele Donier 606328 10-Apr-02 Mineola TX RN 11-Sep-03
Santos, Juan A 526169 10-Dec-02 San Antonio TX RN 11-Sep-03
Saunders, Janice Ann 541456 11-Feb-03 Naples TX RN 16-Sep-03
Sirmons, Shirley E 516607 2-Jul-03 Asheville NC RN 15-Aug-03
Skeans, Shana F 158698 4-Mar-03 Cedar Hill TX LVN 11-Sep-03
Starbuck, John M. 620638 22-Apr-02 Houston TX RN 15-Sep-03
Stone, Marvin A G7006 6-Jun-03 Houston TX MD 18-Aug-03
Sunshine Dental Center 19-Jun-03 Corpus Christi TX 5-Sep-03
Thomas, Neva Lou 681888 24-Feb-03 Bismarck AZ RN 11-Sep-03
Thompson, Guadalupe M 79425 4-Mar-03 Galveston TX LVN 12-Sep-03
Van Meter, Amy M 156834 4-Mar-03 McAddoo TX LVN 16-Sep-03
Watkins, Jamie L 651036 11-Mar-03 Cookville TX RN 23-Sep-03
Watts, Vickie L 114284 20-Nov-02 Temple TX LVN 18-Aug-03
Wesley, Yvette M 169925 20-Feb-03 Plano TX LPN 4-Sep-03
Provider License No. Exclusion Date City State Provider Type Add Date
November/December 2003 15 Texas Medicaid Bulletin, No. 176
Forms
Enrolling in the Electronic Funds Transfer Program
NHICATTN: Provider Enrollment
PO Box 200795Austin TX 78720-0795
FAX: 512-514-4214
Electronic Funds Transfer (EFT) is a payment method that deposits funds for claims approved for payment directly into a provider’s bank account. These funds can be credited to either checking or savings accounts provided the bank selected accepts Automated Clearinghouse (ACH) transactions. EFT also avoids the risks associated with mailing and handling paper checks, ensuring funds are directly deposited into a specified account.
The following items are specific to EFT:
• EFT funds are available to providers when banks open on Wednesday mornings or Thursday if a bank holiday occurs.
• Applications are processed within five working days of receipt.
• Prenotification to the bank takes place on the cycle following the application processing.
• Ten days after prenotification, future deposits are received electronically.
• The Remittance and Status (R&S) report furnishes the details of individual credits made to the provider’s account during the weekly cycle.
• Specific deposits and associated R&S reports are cross-referenced by both provider number and R&S number.
• The availability of R&S reports is unaffected by EFT, and they continue to arrive in the same manner and time frame as currently received.
NHIC provides the following notification according to ACH guidelines:
Most receiving depository financial institutions receive credit entries on the day before the effective date, and these funds are routinely made available to their depositors as of the opening of business on the effective date. The effective date for EFT under the Texas Medicaid Program is Wednesday (or Thursday) of each week.
However, because of geographic factors, some receiving depository financial institutions do not receive their credit entries until the morning of the effective day, and the internal records of these financial institutions will not be updated. As a result, tellers, bookkeepers, or automated teller machines (ATMs) may not be aware of the deposit, and the customers’ withdrawal request may be refused. When this occurs, customers or companies should discuss the situation with the ACH coordinator of their institution who, in turn, should work out the best way to serve their customers’ needs.
In all cases, credits received should be posted to the customers’ account on the effective date and thus be made available to cover checks or debits that are presented for payment on the effective date.
To enroll in the EFT program, providers should complete the Electronic Funds Transfer Authorization Agreement. A voided check or deposit slip must be returned with the agreement to the NHIC address indicated on the form.
Texas Medicaid Bulletin, No. 176 16 November/December 2003
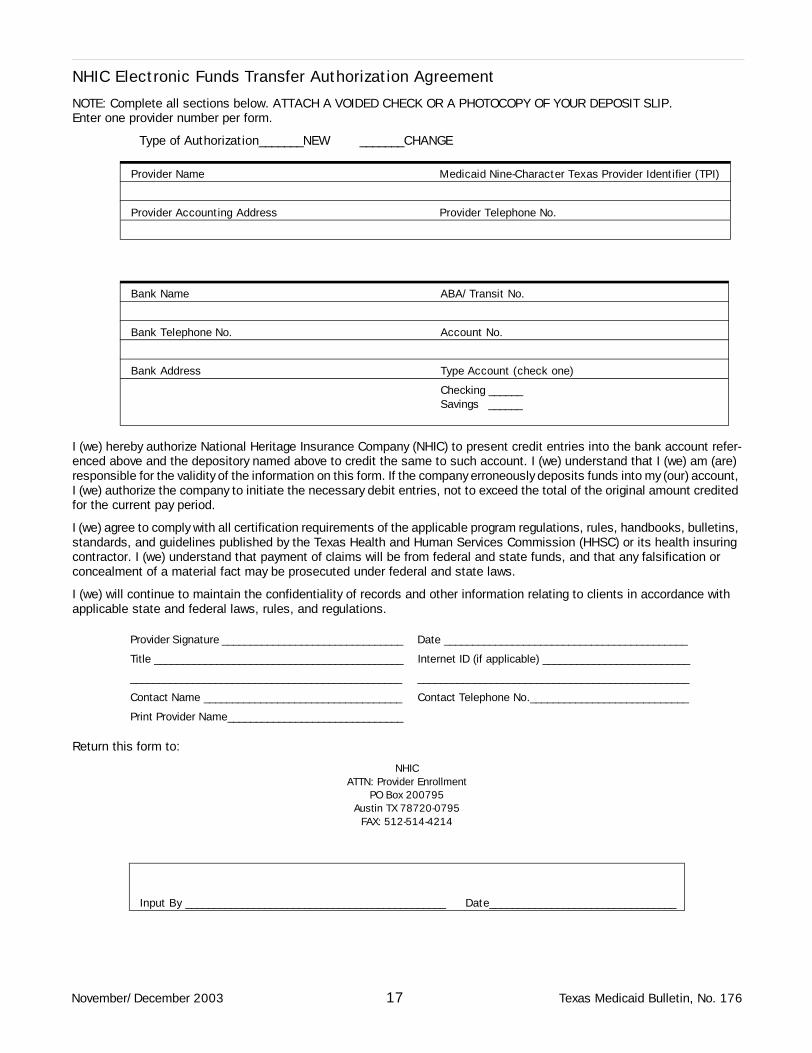
NHIC Electronic Funds Transfer Authorization Agreement
NOTE: Complete all sections below. ATTACH A VOIDED CHECK OR A PHOTOCOPY OF YOUR DEPOSIT SLIP. Enter one provider number per form.
Type of Authorization_______NEW _______CHANGE
I (we) hereby authorize National Heritage Insurance Company (NHIC) to present credit entries into the bank account refer-enced above and the depository named above to credit the same to such account. I (we) understand that I (we) am (are) responsible for the validity of the information on this form. If the company erroneously deposits funds into my (our) account, I (we) authorize the company to initiate the necessary debit entries, not to exceed the total of the original amount credited for the current pay period.
I (we) agree to comply with all certification requirements of the applicable program regulations, rules, handbooks, bulletins, standards, and guidelines published by the Texas Health and Human Services Commission (HHSC) or its health insuring contractor. I (we) understand that payment of claims will be from federal and state funds, and that any falsification or concealment of a material fact may be prosecuted under federal and state laws.
I (we) will continue to maintain the confidentiality of records and other information relating to clients in accordance with applicable state and federal laws, rules, and regulations.
Return this form to:
NHICATTN: Provider Enrollment
PO Box 200795Austin TX 78720-0795
FAX: 512-514-4214
Provider Name Medicaid Nine-Character Texas Provider Identifier (TPI)
Provider Accounting Address Provider Telephone No.
Bank Name ABA/Transit No.
Bank Telephone No. Account No.
Bank Address Type Account (check one)
Checking ______Savings ______
Provider Signature ________________________________ Date ___________________________________________
Title ____________________________________________ Internet ID (if applicable) __________________________
________________________________________________ ________________________________________________
Contact Name ___________________________________ Contact Telephone No.____________________________
Print Provider Name_______________________________
Input By ______________________________________________ Date_________________________________
November/December 2003 17 Texas Medicaid Bulletin, No. 176

Pulse Oximeter Form
Client Name: ______________________________ Client Medicaid No:_____________________________
DME Provider Name and Address Provider TPI No:________________________________
_____________________________________ Provider Phone No:______________________________
_____________________________________ Provider Fax No:________________________________
_____________________________________
HCPCS Code Product Name and Model Number Retail Price
___________ ________________________________________ __________________________
___________ ________________________________________ __________________________
New device provided for purchase Yes_____No_____
**** Equipment designated for clinical use only is not considered appropriate for use in the home****
Oxygen dependent is defined as ongoing, regular need for use of supplemental oxygen for a significant portion of
the day to maintain oxygen saturation. This does not include: PRN use; when only used when sick; when only
used when suctioning; when desaturation occurs only when crying; when desaturation occurs only with seizure
activity
****The following information must be completed by the physician ****
Diagnosis and Basis for Medical Necessity of requested services: ___________________________________________
________________________________________________________________________________________________
Dates of Service requested for Prior Authorization: From ________________ To____________________
___ Client is ventilator and/or oxygen dependent
Client is ventilator dependent __________________________ hours per day
Client is oxygen dependent ____________________________ hours per day
___ Client is weaning from oxygen and/or a ventilator ___________________________________________________
___ Anticipated length of monitor need: Months________1-3 years _______ More than 3 years_________________
___Who will respond to monitor alarm? ______________________________________________________
___Can the patient’s medical needs be meet with intermittent “spot check” of oxygen saturations? Yes_____ No_____
___What is the medical basis for need of continuous monitoring?___________________________________________
____________________________________________________________________________________________
___Is the client receiving any nursing services such as PDN, Home Health Vists, MDCP, CBA, Private Insurance
Please indicate services________________________Number of hours/vists__________________
Signature of prescribing physician_________________________________Date _____________________________
Printed or typed name of physician________________________________Phone No. _________________________
Physician License number_________________________Physician Medicaid TPI ____________________________
Must be submitted with a THSteps – CCP Prior Authorization Request Form
Texas Medicaid Bulletin, No. 176 18 November/December 2003
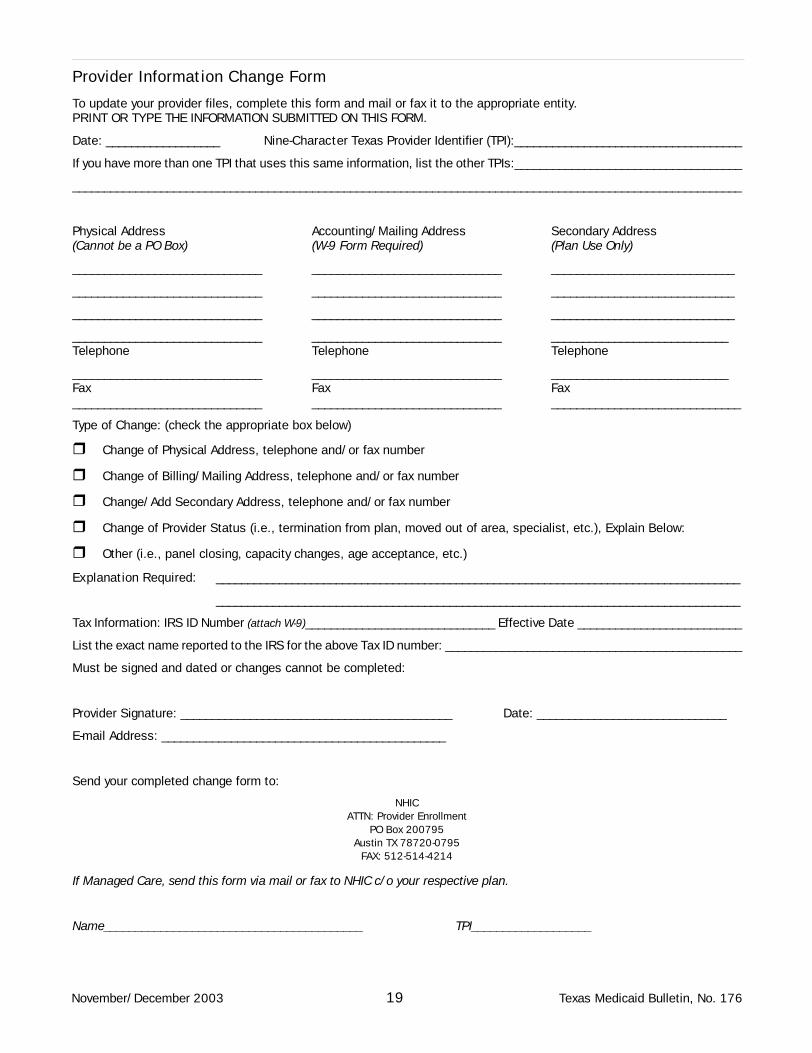
Provider Information Change Form
To update your provider files, complete this form and mail or fax it to the appropriate entity. PRINT OR TYPE THE INFORMATION SUBMITTED ON THIS FORM.
Date: __________________ Nine-Character Texas Provider Identifier (TPI):____________________________________
If you have more than one TPI that uses this same information, list the other TPIs:____________________________________
__________________________________________________________________________________________________________
Physical Address Accounting/Mailing Address Secondary Address (Cannot be a PO Box) (W-9 Form Required) (Plan Use Only)
______________________________ ______________________________ _____________________________
______________________________ ______________________________ _____________________________
______________________________ ______________________________ _____________________________
______________________________ ______________________________ ____________________________Telephone Telephone Telephone
______________________________ ______________________________ ____________________________Fax Fax Fax______________________________ ______________________________ ______________________________
Type of Change: (check the appropriate box below)
��Change of Physical Address, telephone and/or fax number
��Change of Billing/Mailing Address, telephone and/or fax number
��Change/Add Secondary Address, telephone and/or fax number
��Change of Provider Status (i.e., termination from plan, moved out of area, specialist, etc.), Explain Below:
��Other (i.e., panel closing, capacity changes, age acceptance, etc.)
Explanation Required: ___________________________________________________________________________________
___________________________________________________________________________________
Tax Information: IRS ID Number (attach W-9)______________________________ Effective Date __________________________
List the exact name reported to the IRS for the above Tax ID number: _______________________________________________
Must be signed and dated or changes cannot be completed:
Provider Signature: ___________________________________________ Date: ______________________________
E-mail Address: _____________________________________________
Send your completed change form to:
NHICATTN: Provider Enrollment
PO Box 200795Austin TX 78720-0795
FAX: 512-514-4214
If Managed Care, send this form via mail or fax to NHIC c/o your respective plan.
Name_________________________________________ TPI___________________
November/December 2003 19 Texas Medicaid Bulletin, No. 176
ATTENTION: BUSINESS OFFICE
PRESORTED STANDARDUS POSTAGE PAID
AUSTIN TXPERMIT NO 156
Click the following link titles at www.eds-nhic.com for important information:
• Medicaid Workshop Schedules and FAQs
• TDH-NHIC 2003 Publications—includes the Texas Medicaid Provider Procedures Manual, Texas Medicaid Provider Procedures Manual - Texas Health Steps, and Texas Medicaid Bulletins
• TDH-NHIC 2002 Publications—includes previous manuals and bulletins
• Regional Support—lists NHIC Training Specialists
NHICan EDS companyNational Heritage Insurance Co.12545 Riata Vista CircleAustin TX 78727-6524





























