Embed Size (px)
Citation preview

Decades of Delayed Diagnosisin 4 Levodopa-ResponsiveYoung-Onset Monogenetic
Parkinsonism Patients
Helen Ling, BScMed, BMBS, MSc,1,2 Mark Braschinsky,MD, PhD,3 Pille Taba, MD,3 Siiri-Merike Luus, MD,3 KarenDoherty, MB, BCh, BAO, MRCP,1,2 Anna Hotter, MD,4
Werner Poewe, MD,4 and Andrew J. Lees, MD FRCP1,2*
1Reta Lila Weston Institute of Neurological Studies, Institute of
Neurology, University College London, London, United Kingdom;2Queen Square Brain Bank for Neurological Disorders and Institute
of Neurology, University College London, London, United Kingdom;3Department of Neurology, University of Tartu, Tartu, Estonia;4Department of Neurology, University Hospital of Innsbruck, Austria
ABSTRACTBackground: We report 4 patients with young-onsetmonogenetic parkinsonism, each of whom was misdiag-nosed with either a psychogenic movement disorder orchronic fatigue syndrome for 10 to 23 years after theonset of their first symptoms.
Results: Once the diagnosis was eventually made, theyall had a rapid and excellent response to levodopa, albeitwith the early appearance of interdose dyskinesias in 3.
Conclusions: We discuss possible reasons for themissed diagnosis despite the relentless progressionof their motor handicap. DAT scanning supported therevised clinical diagnosis of parkinsonism. VC 2011Movement Disorder Society
Key Words: parkin; monogenetic parkinsonism; psy-chogenic movement disorders; conversion disorder;chronic fatigue syndrome
We report 4 patients with young-onset parkinson-ism, each of whom was misdiagnosed with a motorconversion disorder for at least a decade after theirfirst specialist referral.
Case reports
Patient 1
A British woman developed gait freezing at age 31during her first pregnancy. She then became unsteadyand clumsy and complained of jerky tremulous handsand curling of the toes. She also complained of pro-found fatigue and slowness of thinking. At age 37, shestarted to have urinary urgency and to fall over. Over14 years, she was seen by 6 neurologists and hadreceived diagnoses of motor conversion disorder(MCD), chronic fatigue syndrome (CFS), and depres-sion. Her movements were described as distractible,variable, and deliberately slow. Her spontaneous move-ments were considered as strikingly normal in contrastwith those found on formal neurological examination.At age 45, she was reviewed at the National Hospitalfor Neurology and Neurosurgery in Queen Square,London, where Parkinson’s disease was suspected.In 2001, her brother committed suicide, which coin-
cided with a marked deterioration in her physical symp-toms at age 37. Three of her other 5 siblings had receivedpsychiatric treatment for depression. Her mother had alongstanding history of severe depression.On examination, she walked with 2 sticks and a nar-
row-based gait with stooped posture and postural insta-bility (Video 1a). She had a melancholic, slightly anxiousfacial expression, an asymmetrical fast resting tremorthat was also present on posture and action, and a fastsynchronous rest tremor in both legs. Her movementswere very slow. Finger tapping revealed progressivereduction in amplitude without motor arrests or fatigue.Tone was increased, which improved on distraction.DAT-SPECT showed reduced tracer uptake in the basal
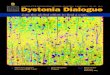
ganglia (Fig. 1a). She was found to have heterozygous de-letion of parkin exon 5 and a duplication of parkin exons2, 3, and 4. After 3 weeks of L-dopa treatment of 300 mg/day, her motor UPDRS score improved from 56 to 7. Shedeveloped limb and trunk chorea within 7 weeks of start-ing treatment (Video 1b).
Patient 2
This Irish woman presented at age 19 with symptomsof fatigue, poor balance, difficulty walking, and quietspeech. She was reviewed by an immunologist and psy-chiatrist and was informed she had CFS and depression.Her symptoms gradually deteriorated and became
------------------------------------------------------------Additional Supporting Information may be found in the online version ofthis article.
*Correspondence to: Professor Andrew J. Lees, Reta Lila WestonInstitute of Neurological Studies, Institute of Neurology, UCL, 1 WakefieldStreet, London, WC1N 1PJ, United Kingdom; [email protected].
Relevant conflicts of interest/financial disclosures: Nothing to report.This work was supported by the Reta Lila Weston Trust.Full financial disclosures and author roles may be found in the onlineversion of this article.
Received: 12 September 2010; Revised: 1 November 2010; Accepted:8 November 2010Published online 29 March 2011 in Wiley Online Library(wileyonlinelibrary.com). DOI: 10.1002/mds.23563
B R I E F R E P O R T S
Movement Disorders, Vol. 26, No. 7, 2011 1337

much worse during pregnancy at age 38. She then devel-oped right-hand tremor, limb dystonia, gait difficulty,and frequent falls. Over the next 5 years, she was fol-lowed up in a neurology clinic, but no organic causewas identified. Limb rigidity and brisk reflexes werenoted but were considered inconsistent. She wasdescribed as being anxious and agitated during consul-tations. At age 42, she was admitted to the Royal Victo-ria Hospital in Belfast, where parkinsonism wassuspected. During examination, she was very immobilewith gait freezing and postural instability and hadasymmetrical cogwheel rigidity, bradykinesia, right-foot dystonia, and stooped posture (Video 2). DAT-SPECT revealed reduced uptake in both basal ganglia(Fig. 1b). She was later confirmed to be a compoundheterozygote with parkin mutations (ARG275TRP,
GLN100X). She had an excellent response to pramipex-ole. Three years later, L-dopa was started, and peakdose dyskinesia developed within a few months.
Patient 3
At age 33, this Estonian nurse developed low mood,slowing of movements, and intermittent hand tremora year after a minor car accident. She was diagnosedwith posttraumatic stress disorder and considered tohave an obsessional, rigid personality with severedepression by psychiatrists. She developed impairmentof gait and speech 2 years later and began to requireassistance to walk. She remained on antidepressantsdespite the relentless progression of her motor symp-toms. She was twice admitted to the care of
FIG. 1. (a) [123I]FP-CIT DAT images of patient 1 show absent tracer activity in both putamen nuclei and asymmetrical markedly reduced uptake inboth caudate nuclei. (b) [123I]FP-CIT DAT images of patient 2 show markedly reduced uptake in the putamen and asymmetrical reduced uptake inthe caudate nuclei. (c) [123I]FP-CIT DAT image of patient 3 shows asymmetrical markedly reduced uptake in the putamen and caudate nuclei. (d)[123I]FP-CIT DAT image of patient 4 shows bilateral reduced tracer uptake in the putamen and caudate nuclei. [Color figure can be viewed in theonline issue, which is available at wileyonlinelibrary.com.]
L I N G E T A L .
1338 Movement Disorders, Vol. 26, No. 7, 2011

neurologists, at ages 37 and 40. Examination showedgeneralized limb rigidity and slowness of movement,with examples of paradoxical kinesis such as normalreactions in catching a ball. Her gait was described asfestinant but ‘‘atypical,’’ with knees flexed and shortstride length, and she had never fallen. Her speech wasslow and spoken in short sentences. The neurologists onboth occasions diagnosed an MCD. At age 43, shebecame bedbound and developed dysphagia, resulting insevere weight loss. She was admitted to the UniversityHospital of Tartu in Estonia, where an organic cause ofher symptoms was first suspected. Examination revealedpostural instability, severe limb rigidity with contrac-tures, and occasional limb and cervical dystonia (Video3). She had facial masking and was almost anarthric.DAT-SPECT revealed severe reduced uptake in both
basal ganglia and led to further investigation, whichrevealed exon duplication in the alpha-synuclein gene(PARK 1/4; Fig. 1c). She had excellent response to L-dopabut developed interdose dyskinesia within a week.
Patient 4
At age 28, during an inpatient treatment for pneumo-nia, this Austrian pharmacist became agitated after amarital dispute and was given 20 mg of intramusculartriflupromazine for sedation. She developed an acutedystonic reaction with right laterocollis on the follow-ing day. Cervical dystonia resolved within 48 hours,but she subsequently developed an intermittent tremorin the left leg. She was diagnosed with reactive depres-sion and was referred for psychotherapy. Subsequently,
she developed gait difficulty and a stooped posture.Over 12 years, she was reviewed by 2 neurologicalteams and psychiatrists, all of whom agreed she hadMCD. At age 40, she was referred to the Departmentof Neurology at Innsbruck Medical University, Austria,where parkinsonism was suspected for the first time.Examination revealed pill-rolling rest tremor in the lefthand, asymmetrical rigidity, and bradykinesia. Shewalked independently with small steps and had markedpostural instability. A dose of 300 mg/day of L-dopaled to complete resolution of her motor symptoms. Shedeveloped wearing-off symptoms a few years later andpeak-dose dyskinesias 15 years after L-dopa treatment.At age 63, she continues to have a good response to L-dopa with mild motor fluctuations (Video 4). Her fam-ily history was negative at the time of diagnosis, but amaternal cousin has since developed Parkinson’s diseasewith dementia. Recent DAT-SPECT revealed reducedtracer uptake (Fig. 1d). She was found to carry digenicmutations for parkin and DJ-1.
DiscussionWe report 4 patients with young-onset parkinsonism
with a delay to correct diagnosis of 10–23 years (Table1). Once organic parkinsonism was suspected, thepatients were investigated, and all were found to have aprobable monogenetic cause.1–3 It was uncertain whetherpatient 4’s digenic mutations cause her parkinsonism, buther initial extrapyramidal symptoms were probablyunmasked early by neuroleptic treatment. We believetheir distinct constellation of psychiatric, behavioral, and
Table 1. Overview of clinical characteristics of patients 1–4
Clinical characteristic Patient 1 Patient 2 Patient 3 Patient 4
Age at onset (y) 31, female 19, female 33, female 28, femaleDelay in correct diagnosis (y) 14 23 10 12Presenting complaint Gait freezing Asymmetrical
bradykinetic rigidityLow mood and slowingof movements
Neuroleptic inducedacute dystonic reactionwith subsequentdevelopment of leftleg tremor
Predominant motor features Tremulous parkinsonism,foot dystonia
Akinetic rigidity, handdystonia, gait freezing
Akinetic rigidity, festinantgait, dysphagia, anarthria
Tremulous parkinsonism,postural instability
Nonmotor features Fatigue, bradyphrenia,urinary symptoms
Fatigue, anxiety Low mood Low mood
Functional disability Walked with assistanceof 2 sticks
Severe posturalinstability requiringassistance with walking
Bedbound, contractures,dysphagia with severeweight loss
Walked independently withmarked postural instability
Genetic findings Compound heterozygoteparkin mutation
Compound heterozygoteparkin mutation
PARK1/4 duplication Compound heterozygotecarrier of parkin andDJ-1
Features mistakenly identified as supportive of a conversion disorderDistractibility and inconsistency Yes Yes Yes YesExtreme slowness/florid symptoms Yes No Yes NoParadoxical kinesis Yes No Yes NoHealth care worker No No Yes YesFamily history of psychiatric illness Yes No No NoVariable frequency and amplitudeon EMG tremor analysis
Yes Not performed Yes Not performed
D E L A Y E D D I A G N O S I S I N M O N O G E N E T I C P A R K I N S O N I S M
Movement Disorders, Vol. 26, No. 7, 2011 1339

motor features, monogenetic cause, female sex, and youngage of onset might have collectively contributed to the er-roneous diagnosis of MCD. All patients had an excellentresponse to L-dopa treatment, and patients 1 and 3 devel-oped dyskinesia within weeks of starting L-dopa therapy.Disability was so severe at diagnosis that L-dopa was con-sidered as the most appropriate initial therapy despite therisk of early emergence of motor fluctuations.Early instability, gait freezing, depression, and be-
havioral disturbances have been emphasised in somereports of parkin-related parkinsonism.2 Depression,anxiety, fatigue, and bradyphrenia overshadowed themotor symptoms in all our patients, and the patients’mental state had led to friction and disharmony intheir marriages. These prominent neuropsychiatric fea-tures may have played a significant role in the failureto diagnose parkinsonism.The early mislabeling of the movement disorder as psy-
chogenic also seemed to have led to an uncritical accep-tance of the diagnosis by subsequent specialists, despiteprogressive development of motor handicap. The factthat patient 1 had a strong family history of depressionand patients 3 and 4 were health care workers may havecompounded the initial error and led to an implicit butunspoken view that the patients were trying to deceivetheir physicians. A report on interviews with UK neurolo-gists indicated that many did not clearly distinguish aconversion disorder from feigning.4,5 Neurologists alsotended to adopt an ‘‘agnostic’’ stance and assume it wasno longer their problem to remedy the malady once a di-agnosis of MCD had been made.4,5 Findings frequentlycited in all 4 cases were distractibility, inconsistency inphysical signs, florid symptoms, extreme slowness, andmarriage disharmony, which led to the erroneous diagno-ses of CFS, depression, and MCD (Table 1). In patients 1and 3, the presence of kinesia paradoxica was mistakenlyconsidered incompatible with neurological disease.Psychogenic movement disorder (PMD) is a diagnosis
made by neurologists with adequate expertise in move-ment disorders,6 and once the diagnosis of PMD ismade, regular neurological follow-up is recommendedfor several years, even after psychiatric referrals. Ifrelentless deterioration in motor function occurs, a crit-ical appraisal of the diagnosis is warranted. Althoughtremor is the commonest PMD, a parkinsonian presen-tation is extremely uncommon, and therefore the diag-nosis of psychogenic parkinsonism should be madewith great caution. Other features that might poten-tially lead to the incorrect conclusion of psychogenicparkinsonism include sudden onset of symptoms afterstress or trauma, prominent pain, brief response to pla-cebo therapy, and coexisiting functional features.6
Parkinsonism can resemble the body language of re-tarded depression and CFS and was not suspected inour cases until the diagnosis was finally made. Inpatients who are chronically slow and tired, parkin-sonism should always be considered. If tremor, dysto-
nia, or signs of parkinsonism are present, atherapeutic trial of L-dopa is merited. Finger-tappingassessment can be an objective tool to differentiate or-ganic parkinsonism from PMD.7 DAT scanning mayalso help in confirming the clinical suspicion of nigro-striatal dopamine denervation.8
We have shared the lessons learned from 4 astonishingcases in the hope that the early suspicion of parkinson-ism will lead to early correct diagnosis and effectivetherapy to maximize patients, of life.Video 1a. Patient 1: Prior to treatment, moderate
bradykinesia of the left hand was demonstrated on fin-ger tapping along with right-sided resting tremor.Bilateral jerky postural tremor was observed. She washypomimic. Her gait was extremely slow with smallstride length, en bloc turning, stooped posture witharms held flexed at the elbow, absent arm swing, andintermittent resting hand tremor.Video 1b. Patient 1: Seven weeks after treatment dur-
ing ‘‘on’’ state, there was marked improvement in brady-kinesia during finger-tapping task with evidence ofchoreiform dyskinesia of the right upper and lowerlimbs. Her gait was normal in speed with good armswing. Mild right foot peak-dose dystonia was observed.Video 2. Patient 2: During ‘‘on’’ state, she could rise
easily from sitting position with her arms folded.While she was walking, start hesitation, frequent gaitfreezing, en bloc turning, poor postural stability, andbilateral hand tremor were observed.Video 3. Patient 3: Prior to treatment, she required
assistance to rise from a chair and walked very slowly,dragging her right foot with elbow and fingers heldconstantly in a flexed posture. Postural instability wasevident with striking retropulsion.Video 4. Patient 4: During the ‘‘off’’ state, there was
bilateral leg tremor at rest on distraction. There wasleft-sided bradykinesia during finger tapping. Retro-pulsion was demonstrated on pull test.
References1. Hardy J, Cai H, Cookson MR, Gwinn-Hardy K, Singleton A.
Genetics of Parkinson’s disease and parkinsonism. Ann Neurol.2006;60:389–398.
2. Khan NL, Graham E, Critchley P, et al. Parkin disease: a pheno-typic study of a large case series. Brain. 2003;126(Pt 6):1279–1292.
3. Theuns J, Van Broeckhoven C. alpha-Synuclein gene duplicationsin sporadic Parkinson disease. Neurology. 2008;70:7–9.
4. Kanaan R, Armstrong D, Barnes P, Wessely S. In the psychiatrist’schair: how neurologists understand conversion disorder. Brain.2009;132(Pt 10):2889–2896.
5. WHO.The ICD-10 Classification of Mental and Behavioural Disor-ders.Geneva, Switzerland:World Health Organisation;1992.
6. Lang AE, Koller WC, Fahn S. Psychogenic parkinsonism. ArchNeurol. 1995;52:802–810.
7. Criswell S, Sterling C, Swisher L, Evanoff B, Racette BA. Sensitivityand specificity of the finger tapping task for the detection of psycho-genic movement disorders. Parkinsonism Relat Disord. 2009;16:197–201.
8. Scherfler C, Schwarz J, Antonini A, et al. Role of DAT-SPECT inthe diagnostic work up of parkinsonism. Mov Disord. 2007;22:1229–1238.
L I N G E T A L .
1340 Movement Disorders, Vol. 26, No. 7, 2011

Osteopontin PolymorphicSusceptibility Factor for
Parkinson’s Disease AmongPatients with Gaucher Disease
Avigayil Ribner, Gheona Altarescu, MD, Ari Zimran, MD, andDeborah Elstein, PhD*
Gaucher Clinic, Shaare Zedek Medical Center, Jerusalem, Israel
ABSTRACTBackground: There is an increased incidence of Par-kinson’s disease among obligate carriers of the com-mon glucocerebrosidase mutations, and amongpatients with Parkinson disease there is an increasednumber who are carriers of glucocerebrosidase muta-tions. A Gaucher mutation is considered a susceptibil-ity factor for Parkinson’s disease. Osteopontin single-nucleotide polymorphism–66 is associated with Lewybody disease and considered a susceptibility factor.The aim of this study was to ascertain whetherGaucher patients with parkinsonism carry the osteo-pontin single-nucleotide polymorphism-66 polymorphicgenotype TT to a greater extent than other Gaucherpatients.
Methods: Seventy adult patients with at least 1 allelehaving the common N370S Gaucher mutation including10 patients with Parkinson’s disease were included.
Results: There was no statistically significant differ-ence in incidence of the TT genotype in patients withclinically symptomatic Parkinson’s disease (88.9%) andother Gaucher patients (72.1%).
Conclusions: This may partly explain the increasedincidence of Parkinson’s disease associated withGaucher mutations. VC 2011 Movement Disorder Society
Key Words: osteopontin; Parkinson’s disease; Gaucherdisease; polymorphic variants
Gaucher disease, the most common autosomal re-cessive lysosomal storage disorder, is caused by muta-tions in the b-glucocerebrosidase gene, with consequentaccumulation of glucocerebroside-engorged cells caus-
------------------------------------------------------------*Correspondence to: Deborah Elstein, Gaucher Clinic, Shaare ZedekMedical Center, P.O. Box 3235, Jerusalem 91031, Israel;[email protected].
Relevant conflicts of interest/financial disclosures: Nothing to report.Full financial disclosures and author roles may be found in the onlineversion of this article.
Received: 2 August 2010; Revised: 11 November 2010; Accepted: 22November 2010Published online 5 April 2011 in Wiley Online Library(wileyonlinelibrary.com). DOI: 10.1002/mds.23595
ing a multisystem disorder. Although there are neurono-pathic forms, there is a predilection among AshkenaziJews for type 1, which has classically been termed non-neuronopathic. The hallmarks of symptomatic type 1Gaucher disease are visceral: hepatosplenomegaly, ane-mia and thrombocytopenia, bone involvement, and,sometimes, pulmonary infiltration.1
In 1996 we reported 6 patients with type 1 Gaucherdisease who had developed early-onset, aggressive Par-kinson’s disease (PD) that was refractory to standardParkinson’s therapy2,3: all had mild symptoms ofGaucher disease. This was among the earliest docu-mented reports of putative neurological findings inpatients with Gaucher genotypes including the N370S(1226G) mutation that had heretofore been consideredprotective of neuronopathic disease.More recently, evidence has accumulated showing an
increased incidence of PD among obligate carriers ofthe 6 common glucocerebrosidase mutations.4–8 as wellas evidence that among patients with PD, there is anincreased number who are carriers of a glucocerebrosi-dase mutation.9–11 The presence of a Gaucher mutationis now considered a susceptibility factor for PD.This association was also evaluated on molecular
and clinical/pathological levels.12–15 Based on autopsyfindings in patients with type 1 Gaucher disease whereunaltered brain glucosylsphingosine levels were notedbut Lewy bodies were seen, it has been suggested thatglucocerebrosidase deficiency may contribute to a vul-nerability to parkinsonism.15
There are few recognized susceptibility factors forLewy body disease associated with parkinsonism (as dis-tinct from that associated with dementia), the earliestreport being for a mitochondrial mutation16 and the mostrecent for increased levels of osteopontin (OPN) in vari-ous body fluids.17 This would also make intuitive sense toexplain a biochemical connection between Gauchermutations and Lewy body disease because in both thesedisorders, inflammation is involved in the pathophysio-logical cascade,18,19 including in the neuronopathicGaucher brain,20 and OPN is a multifunctional moleculeexpressed by activated T cells, dendritic cells, and macro-phages that is up-regulated during inflammation.21,22
Specifically, OPN single-nucleotide polymorphism(SNP)–66 was associated with the occurrence of Lewybody disease and considered a susceptibility factor.23
Therefore, the aim of this study was to ascertainwhether Gaucher patients with symptoms of parkin-sonism carry the OPN SNP-66 polymorphic genotypeto a greater extent do than other patients withGaucher disease.
Patients and MethodsA total of 70 adult patients with type 1 Gaucher dis-
ease, that is, with at least 1 allele having the N370S
O P N V A R I A N T P A R K I N S O N ’ S R I S K I N G A U C H E R
Movement Disorders, Vol. 26, No. 7, 2011 1341

mutation, of whom 10 patients had been diagnosedwith PD but not dementia, were included in the study.Zimran’s Severity Score Index (SSI) with a point
scale of 0–30 points based on Gaucher-specific param-eters24 was applied to each patient at presentation tothe clinic and is used as an indication of disease sever-ity, with <11 points considered mild disease and >20points considered severe disease.In addition to the SNP at 66, 2 other OPN SNPs, at
79525 and at 1284,26 were analyzed. TheOPN gene con-tains several common polymorphisms, distributed in 2main haplotypes, which may modulate OPN productionand/or activity, and to date these latter polymorphismshave been included as part of the major haplotype.For OPN genotyping for SNP-66, the following pri-
mers were used: sense, CCCATCCCGTAAATGAAAAA; antisense, CCAAGCCCTCCCAGAATTTA.The PCR product was digested with the restrictionenzyme FNU4HI (New England Biolabs, Ipswich, MA).The SNP 795 was diagnosed by amplifying the
DNA with the following primers: sense, CCGTGGGAAGGACAGTTATG; antisense, TTGGGGTCTACAACCAGCAT. The restriction enzyme used was AluI(New England Biolabs, Ipswich, MA).For the SNP 1284, the following primers and
restriction enzyme were used: sense, CATGGAAACTCCCTGTAAAC; antisense, ACACCACAAAAAGATAATCACA. The restriction enzyme used was AccI(New England, Biolabs, Ipswich, MA).Institutional Helsinki Committee (Shaare Zedek
Medical Center) approved this study. Specific informedconsent from the patients for the use of anonymizedDNA (and blood) samples for the purpose of clinicalresearch was received previous to advent of this study.
Statistical Analysis
Comparisons between the PD group and the non-PDgroup with regard to categorical variables (age, SSI)were analyzed using the Student t test and Levene’stest for equality of variance. Pearson’s chi-test andFisher’s exact test were applied to compare Gauchergenotypes as well as OPN genotypes between groups.Cross-tabulations were also performed to compare allnon-mutant OPN genotypes as a set between the PDgroup and the non-PD group. ANOVA was applied tocompare within groups and between groups for thepolymorphic genotypes. All tests applied were 2 tailed,and a P � 5% was considered statistically significant.
ResultsThe 10 patients in the group with PD represent all
patients with PD in our clinic other than 1 patientwho died more than a decade ago (and for whomthere was no DNA sample).The control group was chosen to include at least 1
patient age- and sex- and Gaucher genotype–matched
to a PD patient but otherwise was a random collectionof adult patients who appeared for routine clinic visitsduring the study period.The -66 SNP could not be determined for 1 patient
in each group; the 795 SNP could not be determinedin 3 non-PD patients; and the 1284 SNP could not bedetermined in 1 non-PD patient.Table 1 presents all the demographic findings and
polymorphic variable comparisons.The patients with PD had a high prevalence
(88.9%) of the TT genotype of the -66 SNP as did thenon-PD group (72.1%).There were no statistically significant differences
between the groups: not in sex, mean age, SSI, Gauchergenotype, or in the percentage of OPN polymorphic ge-notypes. Mean age and mean SSI compared with OPNgenotypes between and within groups did not differ forall the OPN polymorphic genotypes (data not shown).
DiscussionIt was shown by Maetzler et al17 that increased OPN
levels in serum and CSF are associated with Lewy bodydisease. In a subsequent study, this group also showedthere were a higher number of T alleles at the -66 SNPsite in the Lewy body disease group, so the TT genotypewas significantly associated with systemic disease.23
Finally, these researchers have suggested that there maybe a correlation between age and serum OPN levels.The initial hypothesis was that this subset of
patients would carry the TT genotype of the -66 SNPto a greater extent than would other patients withGaucher disease, thereby explaining their risk for PDas an independently sorting factor. The other 2 poly-morphic genotypes, at 795 SNP and 1284 SNP, arenot associated with any risk of Lewy body disease buthave been linked variously with immune disor-ders.25,26 Thus, these latter polymorphic genotypes
Table 1. Results of demographic and OPN polymorphicfindings among patients with Gaucher disease
diagnosed with Parkinson disease and those notdiagnosed with Parkinson disease
Parkinson (n ¼ 10) Nonparkinson (n ¼ 60)
Men 7 (70.0%) 34 (56.7%)Age (y), mean 6 SD 62 6 12.0 55.7 6 16.8SSI (points), mean 6 SD 8.6 6 6.4 10.3 6 6.3N370S/N370S 4 (40.0%) 35 (58.3%)N370S/other 6 (60.0%) 25 (41.7%)-66TT 8/9 (88.9%) 42/59 (71.2%)-66GT 1/9 (11.1%) 13/59 (22%)-66GG 0 4/59 (6.8%)795TT 0 6/57 (10.5%)795CT 6 (60.0%) 27/57 (47.4%)795CC 4 (40.0%) 24/57 (42.1%)1284AA 4 (40.0%) 28/59 (47.5%)1284CA 6 (60.0%) 27/59 (45.8%)1284CC 0 4/59 (6.8%)
R I B N E R E T A L .
1342 Movement Disorders, Vol. 26, No. 7, 2011

were examined to highlight the index polymorphicgenotype at the -66 SNP because it has been positedthat ethnicity may be a factor.25
The current cohort of Gaucher patients with PD issmall but includes all diagnosed patients in a Gaucherclinic with more than 500 adult patients. A very recentsurvey of 444 patients with type 1 Gaucher diseaserevealed 11 patients over a 12-year period,27 approxi-mately comparable to the percentage in our single-centercohort with the same approximate number of adultpatients. In addition, they estimated the risk of PD inpatients with type 1 Gaucher disease to be 21.4 (95%confidence interval [95% CI], 10.7–38.3), higher amongmen (which is also true in the general population). Theobverse situation was also shown in a study of 420 Is-raeli Ashkenazi Jewish patients with PD,28 where thecarrier frequency of a glucocerebrosidase gene mutationwas 17.9% relative to 4.2% in elderly controls and6.35% in young controls. The proportion of carriers of asevere glucocerebrosidase gene mutation among the PDpatients was 29%, increasing the risk of developing PDby 13.6-fold versus an increased risk of 2.2-fold amongcarriers of a milder mutation.28 Interestingly, this esti-mated risk is approximately that predicted among first-degree relatives of patients with PD29 who carry a copyof the mutated parkin gene (odds ratio compared withnoncarriers, 2.8; 95% CI, 1.5–5.3; P ¼ .002), a well-characterized risk factor for PD.The unexpected finding in the current study was that
in the control cohort of Gaucher patients there was nostatistically significant difference in the incidence of theTT genotype of the -66 OPN polymorphism relative tothat found in patients with clinically symptomatic PD.This should be considered in the context of the hypothe-sis that patients with Gaucher disease (and carriers) areat risk for PD.7–14 If indeed—and in contradistinction topossible other genetic and epigenetic factors that impactGaucher symptoms and signs such as thrombocytopeniaand bone density—the OPN genotype is an unique riskfactor for PD and if indeed many patients (and carrierspotentially) with Gaucher disease have the at-risk poly-morphic genotype, this may be a possible link underlyingthe increased incidence of PD in Gaucher disease.
References1. Beutler E, Grabowski GA. Gaucher disease. In: Scriver CR,Valle
D, Beudet A, Sly WS, eds .The Metabolic and Molecular Bases ofInherited Diseases. New York: McGraw-Hill; 2001:3635–3668.
2. Neudorfer O. MD Thesis: Occurrence of parkinsonianism amongpatients and carriers of type I Gaucher disease. Hebrew University-Hadassah Medical School; 1994.
3. Neudorfer O, Giladi N, Elstein D, et al. Occurrence of Parkinson’ssyndrome in type I Gaucher disease. QJM 1996;89:691–694.
4. Machaczka M, Rucinska M, Skotnicki AB, Jurczak W. Parkinson’ssyndrome preceding clinical manifestation of Gaucher’s disease.Am J Hematol 1999;61:216–217.
5. Varkonyi J, Simon Z, Soos K, Poros A. Gaucher disease type Icomplicated with Parkinson’s syndrome. Haematologia (Budap)2002;32:271–275.
6. Bembi B, Zambito Marsala S, Sidransky E, et al. Gaucher’s diseasewith Parkinson’s disease: clinical and pathological aspects. Neurol-ogy 2003;61:99–101.
7. Goker-Alpan O, Schiffmann R, LaMarca ME, Nussbaum RL, McI-nerney-Leo A, Sidransky E. Parkinsonism among Gaucher diseasecarriers. J Med Genet 2004;41:937–940.
8. Halperin A, Elstein D, Zimran A. Increased incidence of Parkinsondisease among relatives of patients with Gaucher disease. BloodCells Mol Dis 2006;36:426–428.
9. Lwin A, Orvisky E, Goker-Alpan O, LaMarca ME, Sidransky E.Glucocerebrosidase mutations in subjects with parkinsonism. MolGenet Metab 2004;81:70–73.
10. Aharon-Peretz J, Rosenbaum H, Gershoni-Baruch R. Mutations inthe glucocerebrosidase gene and Parkinson’s disease in AshkenaziJews. N Engl J Med 2004;351:1972–1977.
11. Clark LN, Nicolai A, Afridi S, et al. Pilot association study of thebeta-glucocerebrosidase N370S allele and Parkinson’s disease insubjects of Jewish ethnicity. Mov Disord 2005;20:100–103.
12. Tayebi N, Callahan M, Madike V, et al. Gaucher disease and par-kinsonism: a phenotypic and genotypic characterization. MolGenet Metab 2001;73:313–321.
13. Tayebi N, Walker J, Stubblefield B, et al. Gaucher disease with parkin-sonian manifestations: does glucocerebrosidase deficiency contribute toa vulnerability to parkinsonism?Mol Genet Metab 2003;79:104–109.
14. Sidransky E. Gaucher disease: complexity in a ‘‘simple’’ disorder.Mol Genet Metab 2004;83:6–15.
15. Wong K, Sidransky E, Verma A, et al. Neuropathology providesclues to the pathophysiology of Gaucher disease. Mol Genet Metab2004;82:192–207.
16. Egensperger R, Kosel S, Schnopp NM, Mehraein P, Graeber MB.Association of the mitochondrial tRNA(A4336G) mutation withAlzheimer’s and Parkinson’s diseases. Neuropathol Appl Neurobiol1997;23:315–321.
17. Maetzler W, Berg D, Schalamberidze N, et al. Osteopontin is ele-vated in Parkinson’s disease and its absence leads to reduced neuro-degeneration in the MPTP model. Neurobiol Dis 2007;25:473–482.
18. Campeau PM, Rafei M, Boivin MN, Sun Y, Grabowski GA, Gali-peau J. Characterization of Gaucher disease bone marrow mesen-chymal stromal cells reveals an altered inflammatory secretome.Blood 2009;114:3181–3190.
19. Roodveldt C, Christodoulou J, Dobson CM. Immunological fea-tures of alpha-synuclein in Parkinson’s disease. J Cell Mol Med2008;12:1820–1829.
20. Hong YB, Kim EY, Jung SC. Upregulation of proinflammatorycytokines in the fetal brain of the Gaucher mouse. J Korean MedSci 2006;21:733–738.
21. Morimoto J, Kon S, Matsui Y, Uede T. Osteopontin; as a targetmolecule for the treatment of inflammatory diseases. Curr DrugTargets 2010;11:494–505.
22. Lund SA, Giachelli CM, Scatena M. The role of osteopontin ininflammatory processes. J Cell Commun Signal 2009;3:311–322.
23. Maetzler W, Michelis J, Tomiuk J, et al. A single-nucleotidepolymorphism of the osteopontin gene may contribute to asusceptibility to Lewy body disease. J Neural Transm 2009;116:599–605.
24. Zimran A, Sorge J, Gross E, Kubitz M, West C, Beutler E. Predic-tion of severity of Gaucher’s disease by identification of mutationsat DNA level. Lancet 1989;2:349–352.
25. Mas A, Martınez A, de las Heras V, et al. The 795CT polymorphismin osteopontin gene is not associated with multiple sclerosis in a Span-ish population. Mult Scler 2007;13:250–252.
26. Caillier S, Barcellos LF, Baranzini SE, et al. Osteopontin polymor-phisms and disease course in multiple sclerosis. Genes Immun2003;4:312–315.
27. Bultron G, Kacena K, Pearson D, et al. The risk of Parkinson’s diseasein type 1 Gaucher disease. J Inherit Metab Dis 2010;33:167–173.
28. Gan-Or Z, Giladi N, Rozovski U, et al. Genotype-phenotype corre-lations between GBA mutations and Parkinson disease risk andonset. Neurology 2008;70:2277–2283.
29. Marder KS, Tang MX, Mejia-Santana H, et al. Predictors of par-kin mutations in early-onset Parkinson disease: the consortium onrisk for early-onset Parkinson disease study. Arch Neurol 2010;67:731–738.
O P N V A R I A N T P A R K I N S O N ’ S R I S K I N G A U C H E R
Movement Disorders, Vol. 26, No. 7, 2011 1343

Pupillary Unrest Correlates WithArousal Symptoms and MotorSigns in Parkinson Disease
Samay Jain, MD, MS,1,2* Greg J. Siegle, PhD,1
Chen Gu, MS,1 Charity G. Moore, PhD,1
Larry S. Ivanco, MSW,1 Stephanie Studenski, MD, MPH,1
J. Timothy Greenamyre, MD, PhD,1,2,3
and Stuart R. Steinhauer, PhD1,3
1University of Pittsburgh School of Medicine, Pittsburgh,
Pennsylvania, USA; 2Pittsburgh Institute for Neurodegenerative
Diseases, Pittsburgh, Pennsylvania, USA; 3VA Pittsburgh Healthcare
System, Pittsburgh, Pennsylvania, USA
ABSTRACTBackground: Arousal symptoms (e.g., sleepiness) arecommon in Parkinson’s disease, and pupillary unrest(spontaneous changes in pupil diameter) is positivelyassociated with sleepiness. We explored pupillaryunrest in Parkinson’s disease.
Methods: Arousal symptoms (Epworth sleepiness scaleand sleep/fatigue domain of the nonmotor symptoms scalefor Parkinson’s disease) and pupillary unrest wereassessed in 31 participants (14 patients with Parkinson’sdisease, 17 controls). Effect sizes and t tests comparedpatients with Parkinson’s disease with control participants.Correlation coefficients were calculated among arousalsymptoms, pupillary unrest, and Unified Parkinson DiseaseRating Scale Part III. Linear regression was performed witharousal symptoms or pupillary unrest as outcome.
Results: Participants with Parkinson’s disease reportedmore arousal symptoms than controls. Pupillary unrest,arousal symptoms, and Unified Parkinson Disease Rat-ing Scale Part III were positively correlated. The associ-ation between nonmotor symptoms scale-sleep scoreand pupillary unrest was higher in participants with Par-kinson’s disease than controls and higher in those withmore Parkinsonian motor signs. Unified Parkinson Dis-ease Rating Scale Part III was positively associatedwith pupillary unrest.
Conclusions: Pupillary unrest correlates with motorand nonmotor features associated with Lewy-relatedpathology, suggesting it may be a nonmotor marker ofprogression in Parkinson’s disease. VC 2011 MovementDisorder Society
Key Words: nonmotor features; Parkinson’s disease;pupil; sleep disorders; autonomic dysfunction
There is a great need for earlier recognition of Parkin-son’s disease (PD) and nonmotor markers of disease pro-gression so that agents that alleviate motor symptoms
------------------------------------------------------------*Correspondence to: Samay Jain, Assistant Professor of Neurology,Clinical Director, Movement Disorders Division, Department of Neurology,University of Pittsburgh Medical Center, 3471 Fifth Ave., Suite 811,Kaufmann Medical Building, Pittsburgh, PA 15213-3232, USA;[email protected].
Funding agencies: This study was funded by NIH grants KL2RR024154, KMH082998, MH55762, UL1 RR024153, and P30 AG-024827, the Department of Veterans Affairs, and the American ParkinsonDisease Association Center for Advanced Research at the University ofPittsburgh.Relevant conflicts of interest/financial disclosures: Nothing to report.Full financial disclosures and author roles may be found in the onlineversion of this article.
Received: 19 July 2010; Revised: 4 December 2010; Accepted: 14December 2010Published online 19 April 2011 in Wiley Online Library(wileyonlinelibrary.com). DOI: 10.1002/mds.23628
may be evaluated for neuroprotective effects. Nonmotorfeatures have a prevalence of 90% in PD.1 They may pre-date motor signs and include dysautonomia and disordersof arousal such as daytime sleepiness and sleep disorders.2
Pupillary unrest refers to the extent of spontaneouschanges in pupil diameter in darkness that reflectspontaneous fluctuations in autonomic tone. In mid-dle-aged healthy adults, pupillary unrest is positivelyassociated with sleepiness.3 Consequently, the applica-tion of pupillary unrest in PD may address the needfor nonmotor markers of PD progression, as it maymeasure dysautonomia and disorders of arousal. Theobjectives of this exploratory study were to determinewhether pupillary unrest can be measured in PD, tocharacterize differences in pupillary unrest betweenPD and control groups, and to investigate the extentto which pupillary unrest correlates with sleepiness orparkinsonism in an elderly population.
Participants and MethodsParticipants were recruited from the University of Pitts-
burgh Medical Center. PD participants fulfilled the UKPD Society Brain Bank Clinical Criteria, scoring Hoehnand Yahr stage (HY) < 5, taking either no antiparkinso-nian medication, carbidopa/levodopa, or dopamine ago-nists. Controls were age- and sex matched to PDparticipants. Exclusion criteria included pyramidal and/orcerebellar signs, any other organic brain disorder, prior in-tracranial surgery, uncorrectable eyesight, bilateral cata-ract surgery, diabetes, uncontrolled hypertension, inabilityto participate due to motor disability (HY ¼ 5), takingmedications affecting autonomic measures that could notbe safely withheld, and history of polyneuropathy or fail-ure to pass a toxicology screen for substances that couldinfluence results (alcohol, opiates, cocaine, cannabis, ben-zodiazepines, and amphetamines).
Design and Measures
Baseline measures included age, sex, HY stage, andUnified Parkinson Disease Rating Scale Part III—Motor
J A I N E T A L .
1344 Movement Disorders, Vol. 26, No. 7, 2011

signs (UPDRS-III). Arousal measures were the EpworthSleepiness Scale and the sleep/fatigue domain of thenonmotor symptoms scale for PD (NMS-Sleep). Bothscales have established validity and reliability. TheEpworth is an index of sleepiness (0–3) in 8 situations(range, 0–24).4 The NMS-Sleep has 4 items: daytimesleepiness, fatigue, restless legs, and insomnia. Severity(0–3) and frequency (1–4) are scored and then multi-plied, and items are summed (range, 0–48).5 In bothmeasures, higher scores indicate more symptoms.Testing sessions began at 9:00 AM. Pupillary unrest
was assessed as in the Pupillary Sleepiness Test,6 usinginfrared video pupillography, which digitized measure-ment of the horizontal pupil diameter of 1 eye (ISCANRK726 sampling at 60 Hz with a resolution of 0.04mm). Participants were seated in front of a computermonitor in darkness (illumination ¼ 0.027 foot candleswith monitor on) resting comfortably on a head-and-chin rest. They were instructed to stare at a dim redfixation point (intensity < 0.03 candelas/m2) at eyelevel at a distance of 28.7500 subtending a visual angleof 0.25� for 11 minutes. Because of concerns aboutwhether PD participants could remain adequately stilloff antiparkinsonian medication, the first 5 PD partici-pants were tested without antiparkinsonian medica-tions being withheld. Once feasibility was established,antiparkinsonian medications were withheld for at least12 hours prior to testing.
Signal Processing and Statistical Analyses
As described by Ludtke et al,6 pupillary unrest wasquantified employing a fast Fourier transform and sum-ming spectral power from 0 to 0.8 Hz for an 82-secondsegments of data. Because several participants were
unable to stay awake and keep their eyes open for 11minutes, pupillary unrest was quantified as the spectralpower for the first 164 seconds of pupil signal collected.Two-sided t tests or Wilcoxon rank-sum tests com-
pared PD versus controls group (a ¼ 0.1). Effect sizes(Cohen’s d) and their 95% confidence intervals werecalculated. The Shapiro-Wilk normality test showedpupillary unrest was not normally distributed. Thiswas normalized by logarithmic (base 10) transforma-tion for correlations and regression analyses. Pearsoncorrelation coefficients were used to determine linearassociations among arousal measures (Epworth andNMS-Sleep), pupillary unrest, and Parkinsonian motorsigns (UPDRS-III). A 1-sided t test for the differencebetween 2 dependent correlations compared associa-tions of arousal measures (Epworth or NMS-Sleep)with UPDRS-III. Linear regressions were performed totest if associations between arousal (outcome) andpupillary unrest were different for PD and controlsbased on a PD diagnosis (categorical) or UPDRS-IIIscore (continuous); test for interaction, a ¼ 0.1. A uni-variate model with log(pupillary unrest) as outcomeand UPDRS-III as the predictor was also tested. Giventhe sample size, regression models were limited to nomore than 3 predictors. A secondary analysis com-pared those PD participants in whom antiparkinsonianmedications were withheld with those in whom theywere not. Analyses were performed with Stata (Stata-Corp LP, version 10) or R (version 2.11).7
ResultsPD and control participants were of similar age
(mean [SD]): 64.5 (3.2) versus 59.4 (3.3) years,
Table 1. Participant characteristics, arousal-related measures, pupillary unrest, and correlations
Participant characteristics PD (n ¼ 14) Controls (n ¼ 17)
Age 64.5 (3.2) 59.4 (3.3)No. of women (%) 9 (52.9) 4 (28.8)Hoehn and Yahr 1.7 (0.6) 0UPDRS-III 10.1 (3.7) 0
Arousal measures and pupillary unrest PD Controls P value Effect size 95% CI
Epworth 8.6 (4.4) 5.7 (3.4) .05 0.71 0.01–1.41NMS-Sleep 3.9 (4.3) 0.24 (0.75) .007 1.07 0.34–1.80Pupillary unrest (� 10�2 s2/Hz)a 8.0 (7.6) 2.7 (3.3) .07 0.90 0.23–1.57Log(pupillary unrest) �1.5 (0.8) �1.9 (0.6) .12 0.56 0.16–1.2
Pearson correlations r P value
Log(pupillary unrest) and Epworth 0.39 .03Log(pupillary unrest) and NMS-Sleep 0.41 .02UPDRS-III and Epworth 0.38 .04UPDRS-III and NMS-Sleep 0.66 .001UPDRS-III and log(pupillary unrest) 0.32 .08aSpectral power.
P U P I L L A R Y U N R E S T , A R O U S A L & M O T O R S I G N S I N P D
Movement Disorders, Vol. 26, No. 7, 2011 1345

respectively (Table 1). The PD group had HY ¼ 1.7(0.6) and UPDRS-III ¼ 10.1 (3.7). The PD group scoredhigher in measures of arousal-related symptoms(Epworth effect size [ES], 0.71; P ¼ .05; NMS-Sleep ES,1.07; P ¼ .007) and pupillary unrest (ES, 0.90; P ¼.07). There were no significant differences in any out-come measure between the PD participants in whomantiparkinsonian medications were withheld and thosein whom they were not.Positive correlations were seen between arousal-
related measures and pupillary unrest (Epworth: r ¼0.39, P ¼ .03; NMS-Sleep: r ¼ 0.41, P ¼ .02) as well asarousal-related measures and UPDRS-IIII (Epworth: r¼ 0.38, P ¼ .04; NMS-Sleep: r ¼ 0.66, P ¼ .001). Cor-relation was higher with UPDRS-III for NMS-Sleepthan for Epworth scores (r ¼ 0.66 vs 0.38, P ¼ .06).UPDRS-III was positively associated with pupillaryunrest (r ¼ 0.32, P ¼ .08).Epworth scores were positively associated with PD
diagnosis (R2 ¼ 0.13, P ¼ .05), log(pupillary unrest)(R2 ¼ 0.15, P ¼ .03), and UPDRS-IIII (R2 ¼ 0.14, P
¼ .04) in univariate models but not in a simultaneousregression. Multiple linear regression (Fig. 1) demon-strated that the association between pupillary unrestand NMS-Sleep score was higher for PD than for con-trols, with a difference in slope between the PD andcontrol groups of 1.07 (P ¼ .09). The associationbetween NMS-Sleep score and pupillary unrest washigher with more severe Parkinsonian motor signs(difference in simple slopes of 0.85 [P ¼ .10] forUPDRS-III one standard deviation above and belowthe mean).
DiscussionPupillary unrest has not been previously evaluated
in PD. Compared with controls, the PD group hadmore severe arousal symptoms, which were positivelycorrelated with pupillary unrest. A positive interactionon NMS-Sleep scores was seen involving PD diagnosis(PD diagnosis � log[pupillary unrest]) and severity ofParkinsonian motor signs (UPDRS-III � log[pupillary
FIG. 1. Regression models and interactions on arousal-related measures (PU, pupillary unrest).
J A I N E T A L .
1346 Movement Disorders, Vol. 26, No. 7, 2011

unrest]). Parkinsonian motor signs were also positivelyassociated with pupillary unrest.This study found an association between pupillary
unrest and arousal in older adults with PD. The pupilsympathetic pathway integrates input from frontal,limbic hippocampal-amygdaloid, and thalamic sour-ces. The pupil parasympathetic pathway integrates in-formation in the Edinger-Westphal nucleus (cranialnerve III) from ascending reticular fibers and descend-ing fibers from cortical regions.3 Therefore, pupillaryunrest is influenced by neural structures that underliearousal. Although the possibility of processes periph-eral to the Edinger-Westphal nucleus contributing topupillary unrest has not been excluded (glaucoma maybe associated with higher parasympathetic tone result-ing in less pupillary unrest3), this is unlikely given theexclusion criteria for participants. The correlation ofpupillary unrest with Parkinsonian motor signs washigher for NMS-Sleep scores versus Epworth scores(r ¼ 0.66 vs 0.41, P ¼ .06), possibly because theEpworth scale assesses only daytime sleepiness,whereas the NMS-Sleep scale captures additionalsymptoms that coexist in PD.The positive correlation between arousal symptoms
or pupillary unrest and parkinsonism suggests eitherthat one contributes to the other or that both motorfunction and arousal are affected by the same under-lying process in PD. Although it is possible that par-kinsonism contributes to symptoms such as daytimesleepiness or that fatigue could lead to bradykinesia,this does not explain why arousal disorders (eg, REMsleep behavior disorder) predate motor signs.2 Fur-thermore, neuropathologic studies in PD have dem-onstrated Lewy-related pathology in the structuresthat influence the pupillary autonomic pathwaysdetailed above.8,9 Thus, a possible explanation is thathigher UPDRS-III scores and pupillary unrest areboth measures that reflect impairments due to PDneuropathology. The UPRDS-III reflects motorimpairment of the basal ganglia, whereas pupillaryunrest may reflect disorders of arousal involving thereticular activating system. Because PD pathologyalso involves structures that influence pupillary unrestbut not arousal, pupillary unrest may not only reflectdisorders of arousal as seen in healthy adults, but
additional PD pathology as well. This may explainthe significant positive interactions observed betweenPD diagnosis or parkinsonian motor signs and pupil-lary unrest.Limitations of this study include its small sample
size, limited range of PD severity (HY ¼ 1.7 [0.6]),limited range of arousal symptoms, and cross-sec-tional design. Nonetheless, results demonstrate thefeasibility of measuring pupillary unrest in PD andsuggest that pupillary unrest is a marker of disordersof arousal. As such disorders can occur prior tomotor signs,10 pupillary unrest may increase in PDprior to parkinsonism becoming apparent. In later-stage PD, the correlation between pupillary unrestand motor signs may be higher as motor signs andarousal symptoms accumulate. Longitudinal investi-gation of pupillary unrest in a more heterogeneousPD population and in those at risk for PD (REMsleep behavior disorder) is needed to assess the poten-tial of pupillary unrest as an objective nonmotormarker of PD progression.
References1. Weintraub D, Comella CL, Horn S. Parkinson’s disease—Part 1:
Pathophysiology, symptoms, burden, diagnosis, and assessment.Am J Manag Care 2008;14(2 Suppl):S40–S48.
2. Postuma RB, Gagnon JF, Vendette M, Fantini ML, Massicotte-Marquez J, Montplaisir J. Quantifying the risk of neurodegenera-tive disease in idiopathic REM sleep behavior disorder. Neurology2009;72:1296–1300.
3. Loewenfeld IE. The Pupil: Anatomy, Physiology, and Clinical Appli-cations. 1st ed. Detroit, MI: Wayne State University Press; 1993.
4. Johns MW. A new method for measuring daytime sleepiness: theEpworth sleepiness scale. Sleep 1991;14:540–545.
5. Chaudhuri KR, Martinez-Martin P, Brown RG, et al. The metricproperties of a novel non-motor symptoms scale for Parkinson’sdisease: results from an international pilot study. Mov Disord2007;22:1901–1911.
6. Ludtke H, Wilhelm B, Adler M, Schaeffel F, Wilhelm H. Mathe-matical procedures in data recording and processing of pupillaryfatigue waves. Vision Res 1998;38:2889–2896.
7. Getting Started with Stata for Macintosh Release 10. College Sta-tion, TX: Stata Press; 2007.
8. Hunter S. The rostral mesencephalon in Parkinson’s disease andAlzheimer’s disease. Acta Neuropathol 1985;68:53–58.
9. Braak H, Ghebremedhin E, Rub U, Bratzke H, Del Tredici K.Stages in the development of Parkinson’s disease-related pathology.Cell Tissue Res 2004;318:121–134.
10. Chaudhuri KR, Healy DG, Schapira AH. Non-motor symptoms ofParkinson’s disease: diagnosis and management. Lancet Neurol2006;5:235–245.
P U P I L L A R Y U N R E S T , A R O U S A L & M O T O R S I G N S I N P D
Movement Disorders, Vol. 26, No. 7, 2011 1347

Thalamic Neuronal and EMGActivity in Psychogenic DystoniaCompared with Organic Dystonia
Kazutaka Kobayashi, MD PhD,1,2,3 Anthony E. Lang, MD,FRCPC,4 Mark Hallett, MD,5 andFrederick A. Lenz, MD, PhD, FRCSC1*
1Department of Neurosurgery, Johns Hopkins Hospital, Baltimore,
Maryland, USA; 2Department of Neurological Surgery, Nihon
University School of Medicine, Tokyo, Japan; 3Division of Applied
Systems Neuroscience, Department of Advanced Medical Science,
Nihon University School of Medicine, Tokyo, Japan; 4Division of
Neurology, University Health Network and University of Toronto,
Toronto, Ontario, Canada; 5Human Motor Control Section, NINDS,
NIH, Bethesda, Maryland, USA
ABSTRACTBackground: This is a retrospective analysis of thalamicneuronal and electromyogram activities between subjectswith organic dystonia and a subject with psychogenicdystonia in whom a thalamotomy was carried out beforethe diagnosis of psychogenic dystonia was made.
Results: The signal-to-noise ratio in the lowest fre-quency band (dystonia frequency < 0.76 Hz) in theelectromyogram was not significantly different by diag-nosis or muscle. The coherence at dystonia frequencyfor wrist flexors X biceps electromyograms was signifi-cantly higher in organic dystonia, whereas the phasewas not apparently different from zero for either diag-nosis. In a thalamic pallidal relay nucleus (ventral oralposterior), neuronal firing rates were not apparently dif-ferent between psychogenic and organic dystonia. Theneuronal signal-to-noise ratio in ventral oral posteriorwas significantly higher in organic dystonia than in psy-chogenic dystonia, whereas both were greater than incontrols with chronic pain. Spike X electromyogram co-herence apparently was not different between psycho-genic and organic dystonia. The proportion of thalamiccells responding to joint movements was higher in thecerebellar relay nucleus (ventral intermediate) of psy-chogenic dystonia than in organic dystonia.
Conclusions: These results suggest that some fea-tures, such as firing rates and thalamic reorganization,are similar in psychogenic and organic dystonia. Otherfeatures differ, such as the coherence between theelectromyograms from different muscles and the tha-lamic neuronal signal-to-noise ratio, which may reflectpathophysiological factors in organic dystonia. VC 2011Movement Disorder Society
Key Words: psychogenic dystonia; organic dystonia;human thalamus; neuronal activity; plasticity; dystonia-related activity
------------------------------------------------------------*Correspondence to: Frederick A. Lenz, Department of Neurosurgery,Johns Hopkins Hospital, Meyer Building 8-181, 600 North Wolfe Street,Baltimore, MD 21287-7713, USA; [email protected].
Relevant conflicts of interest/financial disclosures: Nothing to report.This work was supported by the National Institutes of Health—NationalInstitute of Neurological Disorders and Stroke Intramural and ExtramuralPrograms (RO1 NS38493 and ROL NS40059 to F.A.L.).Full financial disclosures and author roles may be found in the onlineversion of this article.
Received: 27 May 2010; Revised: 9 November 2010; Accepted: 11November 2010Published online 15 April 2011 in Wiley Online Library(wileyonlinelibrary.com). DOI: 10.1002/mds.23565
The pathophysiology of psychogenic dystonia (PsyD)is not well understood, and some of the same physiologi-cal abnormalities identified in organic dystonia have alsobeen found in PsyD.1 It is possible that some physiologicalabnormalities do not cause the dystonic movements, butresult either from the movements or from some othercommon pathophysiological factor. Reorganized fore-brain sensory and motor maps have been suggested toresult from repetitive movements both in patients withdystonia and in a monkey model of dystonia.2–4 This con-cept is consistent with studies demonstrating that repeti-tive motor activity can lead to reorganization ofthalamocortical sensory and motor maps in monkeys.5,6
In addition, the activity of thalamic neurons often showssignificant peaks of activity at the frequency of dystonicmovements (dystonia frequency < 0.76 Hz).4
We have previously reported reorganized thalamicmaps and altered dystonia frequency activity inpatients undergoing thalamotomy for dystonia.4 Sub-sequent to surgery, 1 of these patients was diagnosedas having PsyD. This situation provided a unique op-portunity to report descriptively how thalamic neuro-nal activity in PsyD differs from that recorded inpatients with organic dystonia and in ‘‘controls’’ oper-ated on for treatment of chronic pain.
Patients and MethodsResults of surgery in the patient with PsyD were
included in a report of 9 patients with organic dystonia.4
At that time, our patient with PsyD was diagnosed withorganic dystonia. Thalamic activity in the psychogenicpatient could be analyzed only for the first operationbecause of the poor quality of recordings in the previ-ously operated thalamic nuclei.4 The electromyogram(EMG) was sampled from myohyoid, deltoid, biceps,and wrist flexors in the psychogenic patient versus flex-ors and extensors of the elbow and wrist in the other 9patients. Therefore, the thalamic spike X EMG cross-correlation was not previously compared with the otherpatients.4 These results were also compared with those in3 patients with chronic pain secondary to thoracic spinalcord injury. None of these patients had pain or altered
K O B A Y A S H I E T A L .
1348 Movement Disorders, Vol. 26, No. 7, 2011

motor function in the upper extremity; clinical detailswere reported in a previous publication.7
All the methods used in this study have been previ-ously described in detail.8–10 Deep sensory cellsresponded reliably to rapid joint movements and/orsqueezing of muscles or tendons but did not respondto stimulation of the skin deformed by these stimuli.Dystonic movements prevented the subclassificationof deep sensory cells and the identification of cellsresponding during active movements.4 Therefore, cellsresponding to cutaneous stimuli provided our mostreliable physiological landmark; putative nuclearlocation was estimated by moving the atlas mapsalong the anterior commissure–posterior commissure(AC–PC) line to align the anterior border of Vc withthe most anterior cell in the region, where the major-ity of cells respond to cutaneous stimulation.4
Postoperative Analysis
The action potentials of single neurons were discrimi-nated and digitized at 10 kHz by a standard shape-fittingpackage (Explorer, Brainwave, Thornton, CO). Thespike train was converted into an equivalent analog sig-nal using the French-Holden algorithm, a standard tech-nique that preserves the time resolution of the actionpotentials in the spike train.10–12 The EMG signals werehigh-pass-filtered (6 dB) at 20 Hz to eliminate low-fre-quency movement artifact while preserving the rawEMG signal. We had data epochs that were long enoughto be analyzed by a standard spectral analysis techniquerather than by a multitapper technique that would havebeen required for shorter epochs.13 Standard techniques
were used to take, process, and interpret the spectralanalysis of the neuron and EMG signals.4,10,12
Patient with Psychogenic Dystonia
The patient was a 33-year-old woman with a 2-yearhistory of dystonia at the time of the first surgery. Thedystonia involved the left oromandibular structures andthe left upper and lower extremities. She had failed treat-ment with trihexyphenidyl (40 mg/day) and with levo-dopa/carbidopa. Marked postoperative improvementlasted only 2 months. Following a second, right-sidedthalamotomy 18 months after the first, dystonia pro-gressed to involve the other side of the body. Six monthslater, she was seen by a movement disorders neurologist(AEL). The diagnosis of PsyD was subsequently madebased on: (1) inconsistencies on examination such assevere tongue involvement only when speech was for-mally assessed, extreme slowness in performing finger-to-nose testing, but normal speed of similar voluntarymovements outside the context of the examination; and(2) incongruities with organic dystonia including markedacute exaggeration of generalized dystonic postures,such as severe axial extension triggered when she wasasked to look upward, and the rapid progression to gen-eralized involvement in an adult without other neurolog-ical abnormalities. At that time, she had severegeneralized dystonia involving her face and all limbs andaxial muscles and required assistance to walk.The patient was informed that she might improve
considerably with admission to hospital, physiotherapy,and withdrawal of the anticholinergic medication.Within days of hospitalization, the dystonia had almost
Table 1. Summary of results
Group Psychogenic Organic Pain
Segments with EMG peak < 0.76 Hz amongsegments per epoch.
85%, ND, Mann–Whitney 81% —NA
Wrist flexor � biceps EMG coherence 0.23, P < .01, Mann–Whitney 0.39 —EMG phase 5.3, ND, Mann–Whitney �7.9 —
Vop neuron firing rate 14.2 Hz, ND, Mann–Whitney 15.1 Hz 18.3 Hz, ND in both groupsVop neurons SNR 2.1, P < .01, Mann–Whitney 3.8 1.2, P < .001 for both groupsProportion of Vop neurons with high spike XEMG coherence
59% for WF 25% for WF —32% for biceps 58% for bicepsND for both muscles, chi square
Proportion of Vop neurons withphase lead
69% for WF 100% for WF —43% for biceps 43% for bicepsND for both muscles, chi square.
Proportion of cells in Vim and Vop respond-ing to joint movement
26/50 lumped, P < .00001 74/334 lumped —23/31 Vim, P < .00001 62/222 Vim3/19 Vop, ND, chi-square 12/112 Vop
Vim and Vop sensory reorganization 0.7 mm, ND, Mann–Whitney 1.1 mm 0.6 mm, P < .05, Mann–Whitneyfor the Organic group only
P values in the Psychogenic column indicate differences with the Organic group. P values in the Pain column indicate differences with 1 or both of the othergroups, as specified in that column. ND indicates that the variable is not significantly different by patient group but does not in any way prove that the 2groups are the same. Abbreviations: EMG, electromyogram; SNR, signal-to-noise ratio; Vim and Vop, thalamic nuclei ventralis intermedius and oralis posterior,respectively. Other conventions are as in the text.
T H A L A M I C N E U R O N A C T I V I T Y I N P S Y C H O G E N I C D Y S T O N I A
Movement Disorders, Vol. 26, No. 7, 2011 1349

completely resolved. At the time of discharge, she hadonly minimal posturing in the left hand, and that subse-quently resolved. In view of the rapid and sustained
remission, the diagnosis of PsyD was clear. Sheremained stable on further follow-up, and so psychiat-ric assessment and treatment was not actively pursued.
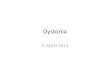
FIG. 1. Sagittal map of thalamic neuronal location relative to the AC–PC line (horizontal line, PC as indicated) and nuclear boundaries in the patientwith psychogenic dystonia. Electrode trajectories (P3, P2, and P1) are shown by oblique lines. Locations of recording sites are indicated by ticks tothe right of each trajectory. Long tics indicate the locations of neurons that responded during sensory stimulation or active movement or both; shorttics indicate unresponsive neurons. A symbol at a long tic indicates a neuron responding during active movement (cross), cutaneous stimulation(circle), and deep stimulation (triangle), as described in the Patients and Methods section. Sites are numbered sequentially, and numbers are indi-cated for every fifth tick. Scale as indicated. Lower panels P1, P2, and P3 show the site number, and receptive field (RF). RF is indicated to the rightand below the site number. Note that many cells responded to movement of 2 joints. For example, 1 cell responded to the extension of bothshoulder and elbow. Shading on the figure indicates the part of the body where there was mechanical stimulation-evoked cellular activity. All shadedfigures indicate cutaneous stimulation, except for neurons 22–24 and 35, for which cellular activity was evoked by manipulation of muscle not bymanipulation of the overlying skin. The maximum size of the representation of a part of the body was estimated from the lengths of single-electrodetrajectories along which all RFs included a single joint, as in a previous study.7 For example, in electrode trajectory P2, passive shoulder movementsare represented by neurons 52–55, a distance of 2.5 mm.
K O B A Y A S H I E T A L .
1350 Movement Disorders, Vol. 26, No. 7, 2011

ResultsAnalysis of EMG was carried out and demonstrated
no apparent difference in signal-to-noise ratio (SNR)between diagnoses of dystonia (Table 1). The EMG XEMG cross-correlation function could only be com-pared for wrist flexors � biceps (see Patients andMethods section). In patients with organic versus psy-chogenic dystonia, more synchronous EMG activitywas observed between these muscles (Table 1).Although RF maps were recorded for cells in the
ventral intermediate nucleus (Vim), records of activityduring involuntary movements were only available forneurons in the ventral oral posterior (Vop) in thepatient with PsyD. Therefore, analysis of spike trainsand spike X EMG functions was limited to Vop,whereas analysis of somatic sensory propertiesincluded neurons in both Vim and Vop. The Vopspike SNR at dystonia frequency was significantlyhigher in organic dystonia than in PsyD, and bothwere greater than in patients with chronic pain (Table1). Neither firing rates nor ISIs appeared to be differ-ent between these diagnostic groups.The proportion of neurons with spike X EMG coher-
ence > 0.42 and maximum SNR at dystonia frequencydid not appear to differ between PsyD and organic dys-tonia for either wrist flexors or biceps. The phase didnot appear to differ between dystonia diagnoses.Figure 1 shows the thalamic map of neuronal location
and stimulation sites for the patient with PsyD. It is re-markable for the large number of cells with deep receptivefields, which was significantly greater than that in patientswith chronic pain. The size of the representations of indi-vidual joints in Vim (see Fig. 1) did not appear differbetween the dystonia diagnoses, although these lengthswere less in chronic pain than in organic dystonia.
DiscussionThe patient with PsyD has a secure diagnosis
because her dystonia remitted with suggestion andphysiotherapy, fulfilling Fahn and Williams’ criteriafor documented psychogenic dystonia.14 We believe thatit is unlikely that she had organic dystonia originally, fol-lowed by PsyD postsurgery, because the appearance ofthe dystonia was very similar throughout her clinicalcourse and because the pattern of clinical remission wasconsistent with PsyD. The results reported in this articlewere obtained from this 1 patient, and the number ofcells studied was limited, so the conclusions must be con-sidered tentative until confirmed.The physiological results suggest that Vop neuronal
activity is characterized by higher SNR in organicthan in psychogenic dystonia, whereas both are higherthan that in patients with chronic pain (Table 1). Thisfinding suggests that SNR is an abnormal feature in
both types of dystonia, which differs in degreebetween the 2 diagnoses. The increased SNR in PsyDmay be a consequence of dystonic movements, a riskfactor that predisposes to the development of dystoniaduring repetitive movements, or both.2,15 The originof this change could be related to grouped GPi neuro-nal discharges in dystonia patients,16,17 which increasewith increasing duration and severity of dystonia.16,18
GPi projects to Vop and lesions of either of thesestructures may interrupt dystonia.4,19 Thalamic neuro-nal activity was often correlated with EMG activityin both diagnoses and so may drive movement forboth, whether it is a consequence of dystonic move-ments or a risk factor for the development of thesemovements.The large number of deep sensory cells in PsyD may
also be a result of plastic change in the sensory represen-tation resulting from dystonic movements. Specifically,cortical plasticity associated with sensory protocolsincluding associative conditioning leads to greater corti-cal reorganization than do protocols in which sensorystimuli are not related to conditioning.20,21
The present study also points to differences betweenthe 2 types of dystonia. EMG coherence between armmuscles has previously been described in organic dys-tonia,22,23 except for focal hand dystonia.24 EMG co-herence was lower in PsyD (Table 1). This may be auseful measure to distinguish psychogenic from or-ganic dystonia. Paired associative magnetic stimulationtesting of cortical plasticity may also differentiatethese conditions.25 Such noninvasive measures may bepractical biomarkers for distinguishing psychogenicfrom organic dystonia, especially given the difficultydifferentiating them on clinical grounds alone.
Acknowledgments: We thank Lance Rowland for excellent technicalassistance.
References1. Espay AJ, Morgante F, Purzner J, et al. Cortical and spinal
abnormalities in psychogenic dystonia. Ann Neurol. 2006;59:825–834.
2. Byl NN, Merzenich MM, Jenkins WM. A primate genesis modelof focal dystonia and repetitive strain injury: I. learning-induceddedifferentiation of the representation of the hand in the primary soma-tosensory cortex in adult monkeys. Neurology. 1996;47:508– 520.
3. Lenz FA, Byl NN. Reorganization in the cutaneous core of thehuman thalamic principal somatic sensory nucleus (Ventral caudal)in patients with dystonia. J Neurophysiol. 1999;82:3204–3212.
4. Lenz FA, Jaeger CJ, Seike MS, et al. Thalamic single neuron activ-ity in patients with dystonia: dystonia- related activity and somaticsensory reorganization. J Neurophysiol. 1999;82:2372–2392.
5. Kaas JH. Plasticity of sensory and motor maps in adult mammals.Annu Rev Neurosci. 1991;14:137–167.
6. Nudo RJ, Milliken GW, Jenkins WM, et al. Use-dependent altera-tions of movement representations in primary motor cortex ofadult squirrel monkeys. J Neurosci. 1996;16:785–807.
7. Lenz FA, Kwan HC, Martin R, et al. Characteristics of somato-topic organization and spontaneous neuronal activity in the regionof the thalamic principal sensory nucleus in patients with spinalcord transection. J Neurophysiol. 1994;72:1570–1587.
T H A L A M I C N E U R O N A C T I V I T Y I N P S Y C H O G E N I C D Y S T O N I A
Movement Disorders, Vol. 26, No. 7, 2011 1351

8. Hua SE, Lenz FA. Posture-related oscillations in human cerebellarthalamus in essential tremor are enabled by voluntary motor cir-cuits. J Neurophysiol. 2005;93:117–127.
9. Lenz FA, Dostrovsky JO, Kwan HC. Techniques for micro-stimulation and recordings of single units and evoked poten-tials during stereotactic surgery. J Neurosurg. 1988;68:630–634.
10. Lenz FA, Tasker RR, Kwan HC, et al. Single unit analysis of thehuman ventral thalamic nuclear group: correlation of thalamic‘‘tremor cells’’ with the 3–6 Hz component of parkinsoniantremor. J Neurosci. 1988;8:754–764.
11. French AS, Holden AV. Alias-free sampling of neuronal spiketrains. Kybernetic. 1971;8:165–171.
12. Glaser EM, Ruchkin DS.Principles of Neurobiological Signal Ana-lysis.New York, New York:Academic Press;1976.
13. Percival DB, Walden AT.Spectral Analysis of Physical Applica-tions.New York, NY:Cambridge University Press;1993.
14. Fahn S, Williams DT. Psychogenic dystonia. Adv Neurol. 1988;50:431–455.
15. Hallett M. The neurophysiology of dystonia. Arch Neurol. 1998;55:601–603.
16. Lenz FA, Suarez JI, Metman LV, et al. Pallidal activity during dys-tonia: somatosensory reorganisation and changes with severity. JNeurol Neurosurg Psychiatry. 1998;65:767–770.
17. Vitek JL, Zhang J, Evatt M. et al. GPi pallidotomy for dystonia:clinical outcome and neuronal activity. Adv Neurol. 1998;78:211–219.
18. Starr PA, Rau GM, Davis V, et al. Spontaneous pallidal neuronalactivity in human dystonia: comparison with Parkinson’s diseaseand normal macaque. J Neurophysiol. 2005;93:3165–3176.
19. Ondo WG, Desaloms JM, Jankovic J, et al. Pallidotomy for gener-alized dystonia [see comments]. Mov Disord. 1998;13:693– 698.
20. Recanzone GH, Merzenich MM, Jenkins WM. Frequency discrimi-nation training engaging a restricted skin surface results in anemergence of a cutaneous response zone in cortical area 3a. J Neu-rophysiol. 1992;67:1057–1070.
21. Recanzone GH, Merzenich MM, Jenkins WM, et al. Topographicreorganization of the hand representation in cortical area 3b ofowl monkeys trained in a frequency-discrimination task. J Neuro-physiol. 1992;67:1031–1056.
22. Tijssen MA, Munchau A, Marsden JF, et al. Descending control ofmuscles in patients with cervical dystonia. Mov Disord. 2002;17:493–500.
23. Grosse P, Edwards M, Tijssen MA, et al. Patterns of EMG-EMGcoherence in limb dystonia. Mov Disord. 2004;19:758–769.
24. Cordivari C, Lees AJ, Misra VP, et al. EMG-EMG coherence inwriter’s cramp. Mov Disord. 2002;17:1011–1016.
25. Quartarone A, Rizzo V, Terranova C, et al. Abnormal sensorimo-tor plasticity in organic but not in psychogenic dystonia. Brain.2009;132:2871–2877.
K O B A Y A S H I E T A L .
1352 Movement Disorders, Vol. 26, No. 7, 2011