Embed Size (px)
Citation preview

ORIGINAL RESEARCH
The 10 mL syringe is useful in generatingthe recommended standard of 40 mmHgintrathoracic pressure for the Valsalvamanoeuvreemm_1228 449..454
Gavin Smith1 and Malcolm J Boyle2
1Ambulance Victoria, Doncaster, and 2Department of Community Emergency Health and ParamedicPractice, Monash University, Frankston, Victoria, Australia
Abstract
Objective: The Valsalva manoeuvre (VM) continues to be first-line management for haemodynamicallystable supraventricular tachycardia in the acute setting. 40 mmHg of intrathoracic pressureis seen as an essential component of the VM. Anecdotally, blowing into a 10 mL syringe tomove the plunger is one method of pressure generation; however, to date its effectiveness hasnot been tested. The objective of the present study was to assess if blowing into a syringesufficient to move the plunger could produce the required 40 mmHg of pressure.
Methods: A two-part experimental study tested the pressure required to move the plunger, andsustain that movement for 15 s, in a Terumo syringe. Part one tested a range of syringesizes. Part two, a repeated measures study, tested the syringe to ascertain if a pressurereduction occurred after repeated use. A sphygmomanometer was attached to the syringevia a 10 cm length of tubing with another length of tubing attached to the sphygmoma-nometer enabling an investigator to blow into the syringe.
Results: In part one, the 10 mL syringe was the only size noted to provide the required 40 mmHgpressure to move the plunger. In part two, the mean for each of the three tests per syringevaried between 37.0 mmHg (95% CI 34.2–39.8) and 40.2 mmHg (95% CI 37.5–43.0). Therewas no statistically significant fall noted over three uses of the same syringe.
Conclusion: The present study has demonstrated that blowing into a 10 mL Terumo syringe, to movethe plunger, generated 40 mmHg intrathoracic pressure, thereby meeting the recommendedintrathoracic pressure for optimum VM performance.
Key words: emergency department, emergency medical services, supraventricular tachycardia, Valsalvamanoeuvre.
Correspondence: Mr Malcolm Boyle, Department of Community Emergency Health and Paramedic Practice, Monash University, P.O.Box 527, Frankston, Vic. 3199, Australia. Email: [email protected]
Gavin Smith, BParamedStud, GDipEmergHealth (MICA), MEmergHealth, MACAP, MICA Paramedic; Malcolm J Boyle, ADipBus, ADHS(Am-bOff), MICA Cert, BInfoTech, MClinEpi, MACAP, Senior Lecturer.
doi: 10.1111/j.1742-6723.2009.01228.x Emergency Medicine Australasia (2009) 21, 449–454
© 2009 The AuthorsJournal compilation © 2009 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine

Introduction
The Valsalva manoeuvre (VM) was conceived some300 years ago by renowned anatomist Antonio MariaValsalva. Its adaptation for use in terminatingsupraventricular tachycardia (SVT) has resulted invarious attempts at quantifying the application of theVM to maximize effect. Most notable has been the workof Taylor and Wong in proposing a recommended stan-dard for VM performance.1 Using the emergency medi-cine setting to illustrate compliance by a physiciansample, Taylor and Wong identified three key elementsof the VM for maximum effect:• Supine posturing• Duration of 15 s• Pressure of 40 mmHg (with an open glottis)1
The VM consists of four phases of effect.1–5 Initially,when a VM is performed, the increased intrathoracicpressure generated leads to reduced venous return anda reduction in cardiac output. The phases can best bedescribed as follows:• Phase one can be defined by a transient increase in
pressure within the thoracic aorta, coupled with acompensatory decrease in heart rate triggered by thebaroreceptors within the aortic arch. This pressureincrease results from the compressive effect of thegenerated intrathoracic pressure on the thoracic aorta
• Phase two is defined by the end of this transientperiod, resulting in decreasing aortic pressure andincreasing heart rate
• Phase three occurs at the end of the strain phase of theVM (and includes a resulting decrease in intrathoracicpressure exerted on the aorta), leading to a brief pres-sure drop within the aorta and a compensatory rise inheart rate
• Phase four occurs as a result of increased venousreturn (and a subsequent increase in preload) result-ing in increased aortic pressure as cardiac output iselevated, and a compensatory decrease in heartrate1–5
A review of the prehospital and medical literatureidentified six clinical studies of VM, including two bio-mechanical studies, which support the figure of40 mmHg of intrathoracic pressure in order to maximizethe effect of vagal tone when performing the VM.6
To generate this pressure, Wong et al. describe theuse of a sphygmomanometer attached to a tube thatenabled the patient to blow into the tube in order togenerate 40 mmHg pressure.7 This method is not usedwithin the Australian prehospital setting because ofissues associated with paramedic education and the
addition of, or modification to, existing ambulanceequipment.
In Victoria, Australia, vagal manoeuvres by para-medics in the prehospital setting are the first-linemanagement tool for the patient suffering haemody-namically stable SVT. Several cultural practices havebeen identified within Victorian paramedic practice inorder to generate the required pressure. These include,but are not limited to:• Placing the thumb in the mouth and blowing against
it• Bearing down• Placing a hand on the abdomen and pushing
against it• Attempting to blow the plunger out of a 10 mL
syringe (when blowing into the small end)As the only currently popular method that provides a
means of identifying the intrathoracic pressure gener-ated, the syringe method needs to be the subject of astudy in order to determine its effectiveness in generat-ing the appropriate pressure according to the recom-mended standard. The objective of the present studywas to assess if blowing into a syringe sufficient tomove the plunger could produce the required 40 mmHgof pressure.
Methods
Design
A two-part experimental study was conducted, testingthe pressure required to move the plunger in a standardselection of Terumo brand syringes (Terumo, Binan,Laguna, Philippines). The first part of the studyattempted to ascertain what pressure (mmHg) would berequired to commence movement of the plunger, andmaintain this movement for a duration of 15 s. Part twoof the study attempted to ascertain if the syringe wouldmaintain its effective pressure requirement over threeconsecutive uses, reflecting repeated attempts in theclinical setting.
Materials
The syringes tested in the present study were manufac-tured by the Terumo company, and are at this time theonly brand stocked and utilized by Ambulance Victoriaacross its area of operations.
Part one of the study used a variety of Terumosyringes (1 mL, 3 mL, 5 mL, 10 mL, 20 mL, and 50 mL)
G Smith and MJ Boyle
450 © 2009 The AuthorsJournal compilation © 2009 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine

commonly used by the ambulance service and a major-ity of hospitals in Victoria, Australia.
A selection of five syringes of each size was randomlychosen from a freshly opened box of 100 syringes forPart one of the study. For part two of the study, werandomly selected eight syringes by picking a syringefrom each row in the box. Two syringes were randomlyselected from each of four previously unopened boxes.Each unopened box contained 100 syringes.
Procedure
Pressure testThe syringes were tested by a single author (GS), withthe author blowing into each syringe being tested. Thetesting was conducted in a non-laboratory setting over aperiod of 3 days in June 2009. The author (GS) was notblinded to the syringe size being tested as this was notpracticable using the apparatus and device being tested.The device used to measure pressure was a standardcombination gauge/bulb sphygmomanometer (ana-logue dial gauge type) manufactured by ABN Health-care Systems (Jawa Barat, Indonesia) and calibrated at2 mmHg increments, with a lower limit of 0 mmHg andan upper limit of 300 mmHg. It was a new sphygmoma-nometer having passed a standard calibration test by anAmbulance Victoria-approved biomedical tester.
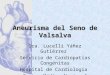
Each syringe plunger was moved to the fully closedposition to ensure that movement was possible beforetesting. The sphygmomanometer was attached to thesyringe via a 10 cm length of plastic tubing, and anairtight seal ensured. The rubber bulb was removedfrom the sphygmomanometer and a 20 cm length ofplastic tubing was attached to enable the author to blowinto this. No leak was required within the circuit createdto prevent potential deleterious side-effects, as theplunger of each syringe provided a quantifiablemaximum resistance, which was the subject of testing.The syringes were assessed for the minimum pressurerequired to commence movement of the plunger, and tomaintain this movement over a period of 15 s. Figure 1demonstrates the apparatus and syringe sizes tested.
Each syringe used for the testing was labelled from 1to 5 for data recording purposes (and 1–8 for part twotesting), and the Terumo production batch numbersrecorded separately for reference. A period of 5 min wasallowed between tests to reflect the practical applicationof the procedure in the prehospital setting.
Sample size calculationAs there have been no previous studies investigatingthe pressure generated by blowing into a syringe, we
used the mean and standard deviation for the 10 mLsyringe from test one and test three listed in Table 1.With the data from Table 1 and using an alpha of 0.05and a power of 0.9, eight syringes would be required todemonstrate if there was a statistically significantdecrease in pressure over the three tests.
Analysis
Data were analysed using SPSS (version 17.0, SPSS,Chicago, IL, USA). The mean and standard deviationwere used to summarize the results of each test, andone-way ANOVA used to compare differences in the pres-sure recorded for each syringe and for each test in parttwo of the study. The results were considered statisti-cally significant if the P-value was <0.05. All confidenceintervals (CI) are 95%.
Results
Part one
A series of three tests were conducted on each syringesize, with a 5 min rest between each test. No instances of
Figure 1. Sphygmomanometer apparatus and syringesamples.
Blowing into a syringe to generate pressure
451© 2009 The AuthorsJournal compilation © 2009 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine

the plunger ejecting from the syringe were recorded.The 10 mL syringe consistently provided pressure mea-sures between the desired 30 to 50 mmHg. The 5 mLsyringe did provide some pressures in the desired range;however, the majority of pressures were outside of thisrange. The remaining syringes produced pressuresbelow or above the desired pressure range. See Table 1for all results.
Part two
Analysis of the eight 10 mL syringes occurred with a5 min rest period between tests. There were no instancesof the plunger being ejected from the barrel of thesyringe during the 15 s duration of each test. The 10 mLsyringe required a mean pressure of 40.2 mmHg (CI37.5–43.0) on the first attempt, and 37.2 mmHg (CI 35.3–39.2) on the third attempt (Table 2 and Figure 2). Therewas no significant difference between the three testmeans (F(2) = 2.82, P = 0.082).
Discussion
Intrathoracic pressure generation during the VM, andspecifically the figure of 40 mmHg, has been demon-strated to provide the optimum pressure for maximumvagal tone, which in turn provides an environment formaximizing effect while minimizing the potential onsetof deleterious side-effects, such as rebound tachycar-dia’s and bradycardia’s.1,3–5,8,9 The use of a standardTerumo syringe to promote intrathoracic pressure gen-eration is an effective method of offering the patient asimple physical device to focus their efforts on, whilealso providing a defined resistance pressure in order toavoid potentially harmful side-effects resulting fromhigh intrathoracic pressures, strain pressures andclosed glottis straining.5,7,10
As a result of the comparative testing, both the 50and 20 mL syringes were excluded from further testingas neither syringe size was able to demonstrate pres-sures above 30 mmHg, and pressure generation below
Table 1. Syringe pressure requirement test results (all sizes)
Syringe size Test number Mean (standard deviation) 95% confidence intervals Range
1 mL 1 76.4 (5.0) 70.2–80.6 68–802 78.8 (4.4) 73.4–84.2 72–843 76.4 (5.0) 70.2–82.6 68–80
3 mL 1 57.2 (2.3) 54.4–60.0 54–602 54.8 (2.7) 51.5–58.1 52–583 54.8 (2.3) 52.0–57.6 52–58
5 mL 1 51.6 (5.2) 45.2–58.0 46–582 51.6 (5.5) 44.7–58.5 46–583 51.2 (4.6) 45.5–56.9 48–58
10 mL 1 42.4 (1.7) 40.3–44.5 40–442 39.2 (1.1) 37.8–40.6 38–403 38.8 (1.1) 37.5–40.2 38–40
20 mL 1 26.0 (2.0) 23.5–28.5 24–282 25.2 (1.8) 23.0–27.4 24–283 24.8 (1.1) 23.5–26.2 24–26
50 mL 1 19.2 (1.1) 17.8–20.6 18–202 18.8 (1.1) 17.4–20.2 18–203 17.6 (1.7) 15.5–19.7 16–20
Five syringes of each size were tested.
Table 2. Syringe pressure requirement test results (10 mL syringe)
Test number Mean (standard deviation) 95% confidence intervals Range
1 40.2 (3.3) 37.5–43.0 36–442 37.0 (3.4) 34.2–39.8 32–403 37.2 (2.4) 35.3–39.2 34–40
Eight 10 mL syringes were tested.
G Smith and MJ Boyle
452 © 2009 The AuthorsJournal compilation © 2009 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine

30 mmHg has been demonstrated within the literatureto prove insufficient in providing adequate vagal toneresponse.5 Similarly, the 1, 3 and 5 mL syringes wereexcluded from further testing, as the literature suggeststhat intrathoracic pressures above 50 mmHg are likelyto result in deleterious side-effects manifesting withinpatients.5
The 5 mL syringes demonstrated mean pressuresabove the acceptable range of 30–50 mmHg, yet thelower range value from the first test (46 mmHg) andthird test (48 mmHg) was within the acceptable safepressure range. The likelihood of excessive pressuregeneration, however, adds an unacceptable risk elementto the use of this syringe size.
Given that the literature supports intrathoracic pres-sure generation of between 30 and 50 mmHg, and thatthe recommended standard suggests an intrathoracicpressure of 40 mmHg to achieve maximum vagalresponse from the VM,1,5 the 10 mL syringe has beendemonstrated to be the most suitable size for thispurpose. In part two of the testing process, the 10 mLsyringe demonstrated mean pressures between37 mmHg (CI 34.2–39.8) and 40.2 mmHg (CI 37.5–43.0)over the three tests. The mean pressure generated for a10 mL syringe in part one and part two of the studydemonstrates an approximation of the recommendedstandard of 40 mmHg, and the overall mean ranges arewell within defined safe intrathoracic pressure levels.
It is well documented that use of the VM for termi-nating SVT often requires multiple attempts to achievesuccess, although the rationale for this is, as yet, unex-plained. As a result, any reduction in pressure genera-tion required to move the plunger after an initialattempt might result in a potentially similar reduction inefficiency in generating optimal intrathoracic pressurewhile performing the VM. There was a non-statisticallysignificant decrease in the mean pressure over the threetests; even with the lowest recorded value of 32 mmHg,this is still within the desirable limits identified in theliterature.5
The reduction of pressure, as demonstrated by therange, across three tests does not suggest overall inef-ficiency of the syringe after repeated use, yet mighthave an, as yet, unquantifiable effect on reversionsuccess in the clinical setting. The literature indicatingpressures of 30–50 mmHg are within the safe limits ofVM practice; however, there is a lack of clinical evidenceto support the effectiveness of the lower pressure.
There is a need for further studies in the clinicalsetting to determine the lowest pressure during the VMthat produces the desired effect. There is also a need todetermine the best time frame between each VMattempt.
The present study has several potential limitations tothe practical setting. The testing conducted within thepresent study was not designed to reproduce the clinicalsetting, and as such is a measure only of pressure gen-eration using the Terumo syringe, and therefore, theresults obtained reflect only the performance of thisbrand of syringe within the described testing procedure.Other practical variables that might adversely influencepressure generated in the clinical setting, and thusreduce the overall efficiency and effectiveness of the VMare:• Respiratory disease• Age (specifically paediatric and elderly patients)• A variety of patient/procedure communication and
comprehension difficulties• The ability of the patient to make and maintain an
appropriate seal around the syringe for the durationof the attempt.
Conclusion
The present study has demonstrated that a 10 mLTerumo syringe will generate an intrathoracic pressureof approximating 40 mmHg, by blowing, to move the
Figure 2. Pressure variation for each test and each 10 mLsyringe. ( ) Test one. ( ) Test two. ( ) Test three.
Blowing into a syringe to generate pressure
453© 2009 The AuthorsJournal compilation © 2009 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine

plunger. This in turn meets the requirements of therecommended standard of intrathoracic pressure foroptimum VM performance.
Author contributions
GS, conceived the idea of the project, conducted thetesting and compiled the manuscript; MB, undertook thestatistical analysis and compiled the manuscript. Bothauthors have read and approved the final version of themanuscript.
Competing interests
No conflict of interest is declared for either author.
Accepted 10 September 2009
References
1. Taylor MD, Wong LF. Incorrect instruction in the use of theValsalva manoeuvre for paroxysmal supra-ventricular tachycar-dia is common. Emerg. Med. Australas. 2004; 16: 284–7.
2. Dawson SL, Panerai RB, Potter JF. Critical closing pressureexplains cerebral hemodynamics during the Valsalva maneuver.J. Appl. Physiol. 1999; 86: 675–80.
3. Waxman MB, Wald RW, Sharma AD, Huerta F, Cameron DA.Vagal techniques for termination of paroxysmal supraventricu-lar tachycardia. Am. J. Cardiol. 1980; 46: 655–64.
4. Nishimura RA, Tajik AJ, Nishimura RA, Tajik AJ. The Valsalvamaneuver-3 centuries later. Mayo Clin. Proc. 2004; 79: 577–8.
5. Looga R. The Valsalva manoeuvre – cardiovascular effects andperformance technique: a critical review. Respir. Physiol. Neuro-biol. 2004; 147: 39–49.
6. Smith G, Morgans A, Boyle M. Use of the Valsalva manoeuvre inthe prehospital setting: a review of the literature. Emerg. Med. J.2009; 26: 8–10.
7. Wong LF, Taylor MD. Vagal response varies with Valsalvamaneuver technique: A repeated-measures clinical trial inhealthy subjects. Ann. Emerg. Med. 2004; 43: 477–82.
8. Mehta D, Wafa S, Ward DE, Camm AJ. Relative efficacy ofvarious physical manoeuvres in the termination of junctionaltachycardia. Lancet 1988; 331: 1181–5.
9. Taylor MD, Auble TF, Yealy DM. First-line management ofparoxysmal supraventricular tachycardia (letter). Am. J. Emerg.Med. 1999; 17: 214–16.
10. Greenland HP, Hosker GL, Smith ARB. A valsalometer can beeffective in standardising the Valsalva manoeuvre. Int. Urogy-necol. J. 2007; 18: 499–502.
G Smith and MJ Boyle
454 © 2009 The AuthorsJournal compilation © 2009 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine