Embed Size (px)
Citation preview

THE INTERNATIONAL JOURNAL OF HEALTH PLANNING AND MANAGEMENT
Int J Health Plann Mgmt (2012)Published online in Wiley Online Library(wileyonlinelibrary.com) DOI: 10.1002/hpm.2115
The accessibility of vulnerable groups tohealth services in Greece: a Delphi studyon the perceptions of health professionals
Ioanna Karamitri1,2*, Thalia Bellali3, Petros Galanis4 and Daphne Kaitelidou41General Hospital of Kalamata, Messinia, Greece2Hellenic Open University, Patras, Greece3Alexandreio Technological Educational Institute, Department of Nursing, Thessaloniki, Greece4University of Athens, Center for Health Services Management and Evaluation - Departmentof Nursing, Athens, Greece
SUMMARY
Background Problems of accessibility to healthcare services notably affect certainpopulation groups such as poor and unemployed people, migrants and minorities, thus havinga negative impact on their health. The aim of this study was to investigate these problems fromthe perspective of health professionals and to formulate empirically informed suggestions tosolve the issue.Methods Primary data were collected in 2010–2011 by using a panel of 36 experiencedhealth professionals around Greece. A two-round Delphi method was undertaken to achievethe objectives of the study. The first questionnaire investigated the factors that hinderaccessibility to health services. The second round aimed at determining the relative importanceof each of the factors emerging in the first round.Results The group of experts identified 345 factors in the first round, which were grouped in55 statements. Consensus was achieved in 22 statements. The study revealed important issues,and health professionals proposed a number of actions to eliminate the accessibility problems.Conclusions The use of medical interpreters and cultural mediators, transcultural educationand stronger linkages among medical facilities are important to reduce accessibility problems.Restructuring primary healthcare and better documenting of the beneficiaries could also improvethe quality of provided healthcare services. Copyright © 2012 John Wiley & Sons, Ltd.
KEY WORDS: accessibility; vulnerable groups; Greece; Delphi study; health professionals
INTRODUCTION
Vulnerable groups are populations at risk of poor physical, psychological and socialhealth (Aday, 1993). Despite interventions that have taken place worldwide, peopleof the lower socioeconomic groups run at least twice the risk of premature death and
*Correspondence to: Ioanna Karamitri, General Hospital of Kalamata, Messinia, Greece.E-mail: [email protected]
Copyright © 2012 John Wiley & Sons, Ltd.
I. KARAMITRI ET AL.
severe illness as of those near the top (Wilkinson and Marmot, 2003). The poorerhealth of the more vulnerable people in society can be attributed to a variety offactors such as unhealthy lifestyles, social influences and general socioeconomicconditions including unequal access to health services. Differences in healthcareutilization have been long noted among demographic groups, such as minoritiesand immigrants (Stronks et al., 2001; Williams et al., 2010), even if there has beena slight trend of improvement in recent years (Krokstad et al., 2002; Setia et al., 2011).As the global crisis deepens, the number of people belonging in the vulnerable groupsincreases and social protection becomes a necessity.Inequalities in accessibility and in other determinants in health differ within and
between countries (Makenbach et al., 2008). Thus, national policies should includespecific, realistic and obtainable goals. In Greece, vulnerable groups represent agrowing part of the population because of various historic, political and financialevents. Greece has been a destination country for immigrants for many years. Thecollapse of the Eastern European regimes in the 1990s made immigration to Greece amassive phenomenon. From 1988 to 2004, the number of immigrants increasedfivefold, and according to the 2001 Census, they represent 7.5% of the totalpopulation in Greece. Because of its geographical position, Greece is also a naturalgateway for people who want to cross over several countries in search for a betterlife. An unspecified number of illegal immigrants enter mainly by the Greek–Turkish boarders. Bilateral and international agreements exist, yet the asylum seeker/refugee problem remains unsolved. The largest ethnic minority in Europe is the Romapopulation. In Greece, formal calculations place the Roma population at about 150 000,whereas Roma associations reckon the numbers to be about 250 000–300 000(Fundación Secretariado Gitano, 2009).Vulnerable groups might differ in some of their characteristics, but they all have
difficulties in reaching health services. Accessibility to health services is a complexand multifaceted issue. Thus, researchers explore accessibility from different pointsof view. One way is to compare the usage of different groups of population. Forexample, in a cross-sectional nationwide household survey, they examine ifimmigrants are using health services equally with indigenous people for equal needs(Tountas et al., 2011). They also examine the factors of non-use, such as thelikelihood of a language barrier, a cultural obstacle or a prohibitively high medicalcost (Dias et al., 2008). Another approach is to analyze the number of admissionsin hospitals for avoidable conditions such as measles, which is a preventableimmunizable infectious disease (Pappas et al., 1997). Dixon-Woods et al. (2006)introduced the term “candidacy”, which describes the ways in which people’seligibility for medical attention is jointly negotiated between individuals and healthservices. Finally, there are two groups of people who understand accessibilityproblems: patients and health professionals. In Greece, there is little evidence aboutthe views of health professionals on the accessibility of vulnerable groups to healthservices (EUGATE, 2011).The recession deepened in 2010, and the fiscal austerity measures resulted in a
reduction of salaries and social protection allowances. In 2010, more than 200 000people lost their jobs. The unemployment rate subsequently increased and reached15.9% in March 2011 compared with the 11.7% for March 2010 and 9.3% for the
Copyright © 2012 John Wiley & Sons, Ltd. Int J Health Plann Mgmt (2012)
DOI: 10.1002/hpm

ACCESSIBILITY TO HEALTH SERVICES IN GREECE
same period in 2009 (Hellenic Statistical Authority, 2011). Risk of poverty, socialexclusion and poorer health are the consequences of this escalated unemployment.
In our study, we tried to detect, to record and to analyze the possible barriers toaccess to health services for vulnerable groups, which are related to problems anddeficiencies of service facilities, or are connected with their particular living conditionsand their socioeconomic and cultural characteristics. Thus, the purpose of this studywas twofold: to examine the difficulties faced by the professionals, when in contactwith vulnerable groups, and to identify the particular needs of these people from theprofessionals’ perspectives. This is a qualitative substudy performed as part of a largerproject on the accessibility of vulnerable groups to healthcare services in Greece. Thequantitative approach substudy investigated the views of members of the vulnerablegroups, and it will be presented in a forthcoming paper.
METHOD
A two-round Delphi method was undertaken to achieve the objectives of the study. TheDelphi technique is widely applied in health research as a tool for solving problems inhealthcare settings. It is in essence a series of sequential questionnaires or “rounds” thataim to gain the most reliable consensus of a group of experts (Linstone and Turoff,1975). Its main characteristics are use of experts, anonymity of the responses,multiplied rounds, controlled feedback and statistical analysis (Clayton, 1997). It ischosen for this study to support (i) the ability of each participant to express viewsanonymously, while providing information generated by an entire group ofparticipants, (ii) the need of heterogeneity of the participants to insure validity and(iii) the lack of geographical limitations because the questionnaires are usuallycompleted by mail (Linstone and Turoff, 1975; Fink et al., 1984).
Panel selection
The success of a Delphi study rests on the combined expertise of the purposelyselected participants and not on the representativeness of the sampling for statisticalpurposes (Powell, 2002). There are no universal rules about the minimum ormaximum number of participants. The heterogeneous panel of professionals selectedfor our study, consisting of academics, nurses, physicians, social workers andadministrative staff, working in hospitals or health centers in areas where there is ahigh concentration of vulnerable groups required an increased number of participants.The selection criterion for participants was a minimum of 3 years of experienceworking with vulnerable groups. For the academics, the sole inclusion criterion wasthe publication of at least one article about vulnerable groups. Diverse geographicregions (urban, suburban and rural) were represented in the panel.
Initially, 36 individuals (14 physicians, 8 nurses, 6 social workers, 5 hospitaladministrative officers and 3 members of the academic society) were approachedin writing per mail and invited to participate. They all agreed. This number wasadopted to allow dropouts at each stage and still fulfill the requirement of having aminimum of 25 experts by the end of the study to increase reliability. Both rounds
Copyright © 2012 John Wiley & Sons, Ltd. Int J Health Plann Mgmt (2012)
DOI: 10.1002/hpm
I. KARAMITRI ET AL.
were completed by 28 participants (78% responsiveness). The experts were mostlyfemale (61%), had a mean (SD) of 13.28 (�8.48) year experience with vulnerablegroups and originated from four areas: Athens, Thessaloniki (the second biggestcity), Kalamata (medium-size urban city) and Messini (a rural town) (Table 1).To initiate the study, an invitation letter and the round 1 questionnaire were sent on
15 November 2010 to the expert panel. The invitation letter explained the objective ofthe study and the method to be followed. The first round aimed at identifying whichfactors are important relative to the research question. The questionnaire consisted ofthree open-ended questions and a fourth part for comments and additional suggestions.All the questions in the first round of the Delphi study were pretested by experts, andfeedback was sought on comprehensibility, question order effects, readability and wordordering. Modifications were made when needed. Following the suggestion of the pilotstudy participants, we provided a definition of “vulnerable groups” relevant to the studyat the top of the questionnaire and there was an explanation of the subgroups thatcomposed the target group of the study. These subgroups included unemployedpeople, poor people, immigrants, refugees and the Roma population.The first questionnaire included three open-ended questions that are presented in
Table 2. We asked the panel of experts to give three to five answers to our questionsto maximize the chance of pinpointing important issues while avoiding unlimitedresponses that could create an excessive volume of data for analysis (Schmidt,1997). The participants had a 3-week period in their disposal to send back thecompleted questionnaires via e-mail or fax.The results of the first round were analyzed with the purpose of creating the
second round questionnaire. The 345 items, which ensued from the first round, weresummarized, analyzed and sorted by content. Answers describing the same variable
Table 1. Sociodemographic characteristics of the group of experts
n % Min Max Mean SD
GenderMale 11 39Female 17 61Total 28 100
OccupationPhysicians 8 29Nurses 6 21Social workers 6 21Administrative staff 5 18Academics 3 11Total 28 100
Location of workAthens 16 57Thessaloniki 6 21Kalamata 3 11Rural areas 3 11Total 28 100
Age 26 60 40.42 9.56Years of experience 3 30 12.46 8.83
Copyright © 2012 John Wiley & Sons, Ltd. Int J Health Plann Mgmt (2012)
DOI: 10.1002/hpm

Table 2. The first questionnaire
Questions Number ofresponses
1. Name the things that make your contact with the members ofvulnerable groups more difficult
110
2. In your opinion, what are the problems that vulnerable groups facewhen dealing with the health services of the National Health System?
108
3. Name at least 3 things that could improve the rendering of healthservices to members of vulnerable groups
112
Comments 15
Total 345
ACCESSIBILITY TO HEALTH SERVICES IN GREECE
were grouped into one item, and there were also cases that a response that includedtwo different issues was split, according to the topic. Finally, the 345 items wereconsolidated into 55 statements. The 55 statements were divided into threethematic sections: (i) difficulties of experts, (ii) difficulties of vulnerable groupsand (iii) proposals for improvement. To minimize the possible ambiguity orvagueness, the questionnaire was once again pretested by experts who did notparticipate in the study, and feedback was sought on word ordering, question ordereffects and readability. Consequently, modifications were made when needed.
The second questionnaire was sent to the group of experts to determine therelative importance of each of the factors identified. A thank you letter forparticipating in the first round was also sent with some information about the numberof responses of the first round and brief instructions for the completion of the secondquestionnaire. The panelists were requested to rate each of the 55 items on the basisof their significance. They were asked how essential or necessary each item was on afive-point Likert scale (1=strongly disagree, 2=disagree, 3=neither agree nordisagree, 4=agree, 5=strongly agree).
Consensus
Consensus among the panelists was considered a priori the representation of >70%agreement to each data element (Hasson et al., 2000). Agreement was expressed asthe percentage of respondents scoring either 4 (agree) or 5 (strongly agree). It wasdecided that beside the convergence, there would be a reference to other interestingoutcomes such as controversies and polarization of answers.
Number of rounds
In the classic Delphi approach, four rounds are used, although in previous studies,two or three rounds are preferred (Hasson et al., 2000). Our research group decideda priori to use two rounds because most of our experts were first-line medicalpractitioners and nurses under time pressure, and we wanted to avoid reduction inresponse rates because of participant fatigue.
Copyright © 2012 John Wiley & Sons, Ltd. Int J Health Plann Mgmt (2012)
DOI: 10.1002/hpm
I. KARAMITRI ET AL.
Ethical considerations
Verbal and written confirmation of guaranteed anonymity was given to the experts.Informed consent to participate in the Delphi study was determined by the completionof the questionnaire.
Data analysis
Throughout the study, data handling was limited to two researchers and the collectedmaterial was coded prior to analysis. Results from open-ended questions included inthe first questionnaire were assembled into appropriate categories and synthesizedfor use in the second questionnaire. Quantitative analysis included the assessmentof the frequency of item selection and the calculation of answer scores. All data wereanalyzed with IBM SPSS 18.0 software.
RESULTS
Round 1
The numbers of responses per question are presented in Table 2.Some issues concerned many participants, and several proposals for improvement
were identical. For instance, 35 of 36 participants named language barriers as afactor that makes contact with vulnerable groups more difficult, and it is apparentin the following verbatim quotations:
Communication difficulties associated with non-comprehension of the Greeklanguage (Physician, 34). Difficulty in understanding medical advice and theseverity of their condition (Nurse, 26). Verbal communication with people whodon’t speak Greek or English without the use of an interpreter (Social Worker, 30).
Furthermore, 21 of 36 participants raised the issue of discrimination with commentssuch as,
Due to stereotypes they are treated negatively by the health care providers, whichresults in difficulty in adaptation (Physician, 39). They are feeling like a statistic(Social Worker, 40). National origin discrimination (Academic, 50).
With regard to possible solutions, 20 participants proposed the planning of traininginitiatives. An expert suggested,
Regular educational activities with the purpose of providing information onhandling and dealing with issues related to vulnerable groups (Social Worker, 30).
Moreover, 17 experts identified general issues of increasing the quality of healthservices such as better staffing levels.
Round 2
As described in the Method section, the results of Round 1 were utilized to produce thequestions of Round 2. In the second round, 28 experts completed the questionnaire
Copyright © 2012 John Wiley & Sons, Ltd. Int J Health Plann Mgmt (2012)
DOI: 10.1002/hpm

ACCESSIBILITY TO HEALTH SERVICES IN GREECE
(78% response rate), and 22 out of 55 items achieved over 70% agreement. The expertsagreed on three items that create difficulties to the health professionals and to themembers of vulnerable groups (Table 3). The experts acknowledged that the inabilityof some members of vulnerable groups to understand paperwork creates problems ofaccess and that because of a probable lack of health insurance, they cannot alwaysafford the cost of health services. The panelists also recognized that some membersof vulnerable groups confront the healthcare system with prejudice and distrust, whichis a barrier to establishing a therapeutic relationship between the health professionaland the patient.
Many statements (n: 19) involved proposals to ameliorate the existing accessibilityconditions and to diminish accessibility problems to health services overall (Table 4).Notable proposals seemed to be the necessity of reduction of time-consumingbureaucratic procedures and the creation of support systems for housing and recordingvulnerable groups. Other proposals included primary healthcare restructuring tominimize patient crowding in hospitals, strengthening referral links between primaryand secondary healthcare, increasing staffing and planning health promotion and healtheducation programs. Furthermore, the experts agreed on recommendations that refer tothe particular challenges the members of vulnerable groups such as migrants confrontwhen seeking medical attention. For example, the translation of leaflets about healthservices in the languages of immigrant groups might help non-Greek speakers to learnabout their rights and obligations. Regarding the language barrier issue, there wereother suggestions, such as using medical interpreters and training members ofvulnerable groups as cultural mediators. A consensus was also apparent as to the needof organizing regular educational activities for employees with the purpose ofproviding information on handling issues related to vulnerable groups.
Many proposals for improvement also achieved consensus and can be categorizedin three core clusters: (i) quality improvement in healthcare services; (ii) training ofhealthcare professionals; and (iii) planning interventions for vulnerable groups(Table 5).
There was an apparent disagreement among the participants in three cases: theneed for safeguarding hospital areas and the creation of specific waiting rooms orpolyclinics for vulnerable groups. These solutions might endorse marginalizationrather than integration and were felt as discriminatory from some members of theexpert panel (Table 6).
Table 3. Results of the second round—difficulties
Statements Percentage ofagreement
The inability to understand the paperwork creates problems of access 75.00%Lack of health insurance. The cost of health care services is not alwayslow for the members of vulnerable groups
71.42%
Some members of vulnerable groups confront the health care systemwith prejudice and distrust
71.42%
Copyright © 2012 John Wiley & Sons, Ltd. Int J Health Plann Mgmt (2012)
DOI: 10.1002/hpm
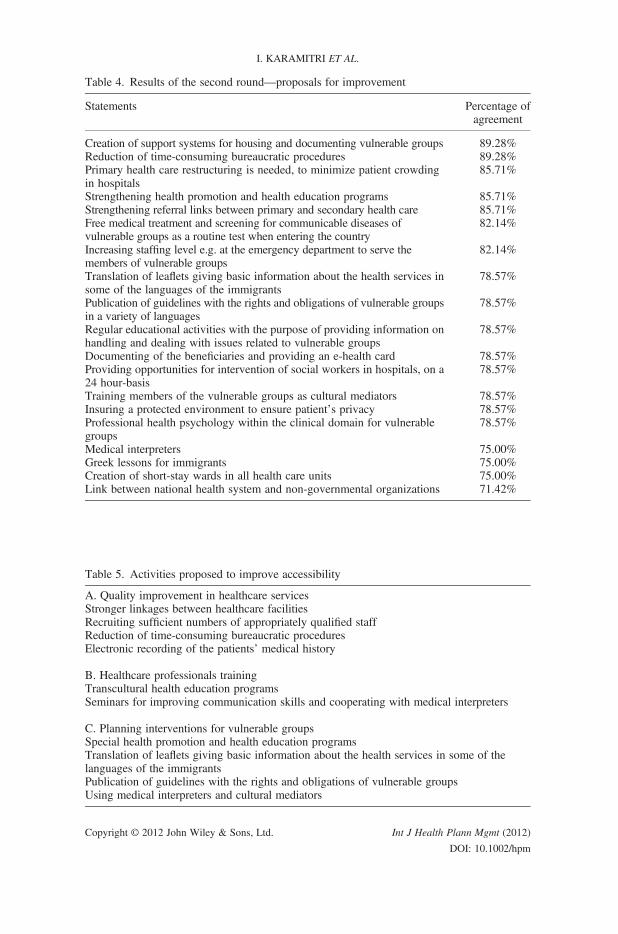
Table 4. Results of the second round—proposals for improvement
Statements Percentage ofagreement
Creation of support systems for housing and documenting vulnerable groups 89.28%Reduction of time-consuming bureaucratic procedures 89.28%Primary health care restructuring is needed, to minimize patient crowdingin hospitals
85.71%
Strengthening health promotion and health education programs 85.71%Strengthening referral links between primary and secondary health care 85.71%Free medical treatment and screening for communicable diseases ofvulnerable groups as a routine test when entering the country
82.14%
Increasing staffing level e.g. at the emergency department to serve themembers of vulnerable groups
82.14%
Translation of leaflets giving basic information about the health services insome of the languages of the immigrants
78.57%
Publication of guidelines with the rights and obligations of vulnerable groupsin a variety of languages
78.57%
Regular educational activities with the purpose of providing information onhandling and dealing with issues related to vulnerable groups
78.57%
Documenting of the beneficiaries and providing an e-health card 78.57%Providing opportunities for intervention of social workers in hospitals, on a24 hour-basis
78.57%
Training members of the vulnerable groups as cultural mediators 78.57%Insuring a protected environment to ensure patient’s privacy 78.57%Professional health psychology within the clinical domain for vulnerablegroups
78.57%
Medical interpreters 75.00%Greek lessons for immigrants 75.00%Creation of short-stay wards in all health care units 75.00%Link between national health system and non-governmental organizations 71.42%
Table 5. Activities proposed to improve accessibility
A. Quality improvement in healthcare servicesStronger linkages between healthcare facilitiesRecruiting sufficient numbers of appropriately qualified staffReduction of time-consuming bureaucratic proceduresElectronic recording of the patients’ medical history
B. Healthcare professionals trainingTranscultural health education programsSeminars for improving communication skills and cooperating with medical interpreters
C. Planning interventions for vulnerable groupsSpecial health promotion and health education programsTranslation of leaflets giving basic information about the health services in some of thelanguages of the immigrantsPublication of guidelines with the rights and obligations of vulnerable groupsUsing medical interpreters and cultural mediators
I. KARAMITRI ET AL.
Copyright © 2012 John Wiley & Sons, Ltd. Int J Health Plann Mgmt (2012)
DOI: 10.1002/hpm

Table 6. Results of the second round—controversial statements
Controversial statements Agree Disagree Neither agreenor disagree
Safeguarding hospital areas 13 12 3Creating specific waiting rooms for the vulnerablegroup members
12 13 3
Creating special polyclinics for migrants and the Romapopulation
13 10 5
ACCESSIBILITY TO HEALTH SERVICES IN GREECE
DISCUSSION
Our study indicates consensus among experts in identifying difficulties that healthprofessionals and members of the vulnerable groups face. Bureaucracy is interwovenwith public administration since the restoration of democracy in 1974 in Greece, andit is considered one of the main weaknesses of the Greek Health System (Maniouand Iakovidou, 2009). The proposal of the experts in this study to diminish theexcessive bureaucratic procedures is not connected to their general consequencesfor productivity or to the phenomenon of corruption of public servants. It refers tothe simplification of procedures to render health services accessible to vulnerablegroups. In a study about Balkan immigrants in Thessaloniki, 16% of Albaniansand 21.4% of Bulgarians mentioned bureaucracy as a problem in Greek hospitals(Hatziprokopiou, 2004).
Lack of health insurance, which was also named as a barrier by the panelists, cancreate two kinds of problems. Physicians are reluctant to order essential diagnostictests, and uninsured people forego preventative and postpone necessary care. Therole of health insurance is mentioned in many studies (Derose et al., 2009; Siddiqiet al., 2009). For example, in a study comparing the United States and Canada withregard to the role of health insurance as primary explanation of disparities in health,it was found that the existence or inexistence of health insurance coverage correlateswith access to health services (Siddiqi et al., 2009).
In general, the quality of healthcare services could improve with variousinterventions according to the experts. Organized cooperation between primaryand secondary healthcare settings as well as with non-governmental organizationsseemed to be a priority because the participants expressed variously this requeston the first round and the relative statement attained a high score on the second.Members of vulnerable groups mostly visit emergency departments and healthcenters, but comorbidity or multimorbidity is often present, requiring personalizedtreatment. Recruiting sufficient numbers of appropriately qualified staff is a proposalfor general quality improvement, but it is significant to the vulnerable groupsbecause they are among the main users of the public health system. Betterstaffing is ranked as a high priority among other studies because it is a maincause of burnout syndrome in hospitals (Iakovidou et al., 2008). Also, digitalmonitoring improves quality. E-health is part of a broader digital Agenda for theEuropean Union because it can improve the quality of care and reduce medical costs(European Commission, 2010).
Copyright © 2012 John Wiley & Sons, Ltd. Int J Health Plann Mgmt (2012)
DOI: 10.1002/hpm

I. KARAMITRI ET AL.
The group of experts agreed on the need for continuing education on topics relatedto vulnerable groups such as transcultural healthcare. In a study involving 18 focusgroups on the issue in the UK, health professionals emphasized that they were anxiousof appearing discriminatory, being culturally inappropriate or causing affront (Kaiet al., 2007). As it is shown in a qualitative study in New SouthWales, Australia, aboutthe accessibility of young people, adequate training is important for providinghealthcare successfully to people with particular characteristics (Kang et al., 2003).Suggestions of the experts refer also to the initiatives that focus on the needs of
vulnerable groups. General health promotion policies and programs might not havethe expected results for vulnerable group members. Qualitative research in theUnited Kingdom suggested that there are several constraints on the developmentof health promotion relative to deprivation and poverty (Daykin and Naidoo,1997). Lack of time and inadequate information might additionally negatively affectproject outcomes; therefore, careful planning is required for maximizing the positiveeffects on the target group.Translation of leaflets is a basic method for providing information to foreign
speakers worldwide. This method has been criticized because low literacy patientsare unable to comprehend the medical instructions given (Schaafsma et al., 2003).Thus, the extended use of graphs and pictograms is proposed. Evaluation onreadability, comprehensibility, communicative effectiveness and pilot testing of theleaflets is important prior to applying to the public (Garner et al., 2011).The medical interpreter issue was essential in both rounds of the Delphi study. The
quality of the relationship between the health professional and the patient has themost positive effect on satisfaction and influences health outcomes (Raposo et al.,2009). A systematic review about the use of professional interpreters in health (from1966 to 2005) reports benefits on communication, utilization, satisfaction andclinical outcomes (Karliner et al., 2007). Speaking the same language is a necessarybut not sufficient condition to build a successful therapeutic relationship. Lack ofawareness of the value systems of patients and the family expectations about rolesand relationships might lead to serious ethical dilemmas with deleterious outcomes(Donnelly, 2000). The proposal of the experts for training people belonging tothe vulnerable groups and using them as cultural mediators can be characterizedas innovative.
Strengths and limitations of the study
The Delphi method has been methodologically criticized mainly for not adhering toaccepted scientific principles such as psychometric validity (Mullen, 2003). Onthe other hand, Goodman (1987) reported that, “If a Delphi panel is broadlyrepresentative of the population and the area of knowledge, then content validitycan be assumed”. Our study included experts from different educationalbackgrounds as well as from different job positions, originating from variousgeographical areas in Greece. Delphi has also been criticized for producing resultsthat reflect the opinions of the selected participants only (Hasson et al., 2000). Atest–retest reliability analysis could possibly be applied, but a group of experts isnot always tolerant to this procedure. A third round for ranking the most important
Copyright © 2012 John Wiley & Sons, Ltd. Int J Health Plann Mgmt (2012)
DOI: 10.1002/hpm

ACCESSIBILITY TO HEALTH SERVICES IN GREECE
statements could further complete the study, but repeated rounds might lead toparticipant fatigue and dropouts. Parallel data collection and analysis is justified herebecause it not only reflects the primary purpose of seeking consensus about theparticular issue but also provides insight into methodological issues of credibilityand reliability (Powell, 2002). Finally, it is difficult to contrast our study withprevious ones because no research was identified examining the exact same topic.However, in a European Delphi project of 16 countries about the identification of “bestpractice” in the delivery of healthcare to immigrants, some suggestions (intersectorialcollaboration, culturally sensitive healthcare, transcultural education and access tointerpretation assistance) were identical to our findings (EUGATE, 2011).
CONCLUSION
This research provides a starting point for assessing possible factors of accessibilityproblems of vulnerable groups to health services. The experts agreed on several topicssimilar to the suggestion of other studies worldwide, such as the need of medicalinterpreters, cultural mediators and transcultural education. Our study also points outgeneral everyday problems of the Greek Health System, for instance, the importanceof restructuring primary healthcare, better documenting of the beneficiaries and strongerlinkages amongmedical facilities. Future studies should recruit subgroups of populationsubgroups with particular needs but not necessarily of a lower socioeconomic groupsuch as non-Greek speakers or adolescents and examine their specific accessibilityproblems from the viewpoints of both health service users and health professionals.
AUTHORS’ CONTRIBUTIONS
IK analyzed the data, interpreted the results and wrote the manuscript. TB wasinvolved in the conception and design of the study and the data collection. Shedrafted sections of the manuscript and revised drafts of the manuscript. PG andDK were involved in conception and design of the study and the data collection.All authors critically reviewed and approved the final manuscript.
ACKNOWLEDGEMENTS
The authors would like to thank all 36 participants in the Delphi study for theirvaluable contribution to this project. The authors have no competing interests.
REFERENCES
Aday LA. 1993. At Risk in America: The Health and
Health Care Needs of Vulnerable Populations in the
United States. Jossey-Bass: San Francisco.
Copyright © 2012 John Wiley & Sons, Ltd.
Clayton MJ. 1997. Delphi: a technique to harness expert
opinion for critical decision-making tasks in education.
Educ Psychol 17(4): 373–386.
Int J Health Plann Mgmt (2012)
DOI: 10.1002/hpm
I. KARAMITRI ET AL.
Daykin N, Naidoo J. 1997. Poverty and health promotion
in primary health care: professionals’ perspectives.
Health Soc Care Comm 5(5): 309–317.
Derose KP, Escarce JJ, Lurie N. 2009. Immigrants and
health care: access, quality and cost. Med Care Res
Rev 66(4): 355–409.
Dias SF, Severo M, Barros H. 2008. Determinants of
health care utilization by immigrants in Portugal.
BMC Health Serv Res 8: 207.
Dixon-Woods M, Cavers D, Agarwal S, et al. 2006.
Conducting a critical interpretive synthesis of the
literature on access to healthcare by vulnerable groups.
BMCl Health Res Methodol 6: 35.
Donnelly PL. 2000. Ethics and cross-cultural nursing.
J Transcult Nurs 11(2): 119–126.
EUGATE. 2011. Work Package n� 7: Identification of
best practice models Project Report on Delphi process
on best practice of health care for Immigrants,
European Best Practices in Access. Quality and
Appropriateness of Health Services for Immigrants,
EUGATE A/800175.
European Commission. 2010. Communication from The
Commission to The European Parliament, the Council,
the European Economic and Social Committee and the
Committee of the Regions: a Digital Agenda for
Europe. COM(2010) 245 final/2, Brussel.
Fink A, Kosecoff J, Chassin M, Brook RH. 1984.
Consensus methods: characteristics and guidelines for
use. Am J Public Health 74(9): 979–983.
Fundación Secretariado Gitano. 2009. Health and the
Roma Community, analysis of the situation in Europe.
Bulgaria, Czech Republic, Greece, Portugal, Romania,
Slovakia, Spain. Fundación Secretariado Gitano,
Ministerio de Sanidad y Política Social: Madrid.
Garner M, Ning Z, Francis J. 2011. A framework for the
evaluation of patient information leaflets. Health
Expect. DOI: 10.1111/j.1369-7625.2011.00665.x
Goodman CM. 1987. The Delphi technique: a critique.
J Adv Nurs 12(6): 729–734.
Hasson F, Keeney S, McKenna H. 2000. Research
guidelines for the Delphi survey technique. J Adv Nurs
32(4): 1008–1015.
Hatziprokopiou P. 2004. Balkan immigrants in the Greek
city of Thessaloniki: local processes of incorporation
in an international perspective. Eur Urban Reg Stud
11(4): 321–338.
Hellenic Statistical Authority. 2011. Facts about unemploy-
ment rates (accessed 17/07/2011) http://www.statistics.
gr/portal/page/portal/ESYE/PAGE-themes?p_param=
A0101
Iakovidou E, Maniou M, Palli E, Kostopoulos E,
Zaragas S, Katsanevas T. 2008. Services of health
in Greece: measurement of the satisfaction of the
health care personnel in private and public sector
Copyright © 2012 John Wiley & Sons, Ltd.
that concerns the provided services. Vima-Asklipiou
7(4): 344–359.
Kai J, Beavan J, Faull C. 2007. Professional uncertainty
and disempowerment responding to ethnic diversity
in health care: a qualitative study. PLoS Med 4(11):
e323:1766–1775.
Kang M, Bernard D, Booth M, et al. 2003. Access to
primary health care for Australian young people:
service provider perspectives. Brit J Gen Pract
53(497): 947–952.
Karliner LS, Jacobs EA, Chen A, Mutha S. 2007. Do
professional interpreters improve clinical care? A
systematic review of the literature. Health Serv Res
42(2): 727–754.
Krokstad S, Kunst AE, Westin S. 2002. Trends in health
inequalities by educational level in a Norwegian total
population study. J Epidemiol Commun H 56: 375–380.
Linstone HA, Turoff M (eds). 1975. The Delphi
Method: Techniques and Applications. Addison-
Wesley Publishing Company: Massachusetts.
Mackenbach JP, Stirbu I, Roskam AJ, et al. 2008. Socio-
economic inequalities in health in 22 European
countries. N Engl J Med 358: 2468–2481.
Maniou M, Iakovidou E. 2009. The current situation in the
public and private hospitals in Greece. Vima-Asklipiou
8(4): 381–400.
Mullen PM. 2003. Delphi: myths and reality. J Health
Organ Manag 17(1): 37–52.
Pappas G, Hadden W, Kosak L, Fisher G. 1997. Potentially
avoidable hospitalizations: Inequality in rates between
US socioeconomic groups. Am J Public Health 87(5):
811–816.
Powell C. 2002. The Delphi technique: myths and
realities. J Adv Nurs 41(4): 376–382.
Raposo ML, Alves HM, Duarte PA. 2009. Dimensions of
service quality and satisfaction in healthcare: a
patient’s satisfaction index. Serv Bus 3: 85–100.
Schaafsma E, Raynor T, de Jong-van den Berg L. 2003.
Accessing medication information by ethnic minorities:
barriers and possible solutions. Pharm World Sci 25(5):
185–190.
Schmidt RC. 1997. Managing Delphi surveys using
nonparametric statistical techniques. Decision Sci 28(3):
763–774.
Setia MS, Quesnel-Vallee A, AbrahamowiczM, Tousignant
P, Lynch J. 2011. Access to health-care in Canadian
immigrants: a longitudinal study of the National
Population Health Survey. Health Soc Care Comm 19(1):
70–79.
Siddiqi A, Zuberi D, Nguyen QC. 2009. The role of
health insurance in explaining immigrant versus
non-immigrant disparities in access to health care:
comparing the United States to Canada. Soc Sci Med
69(10): 1452–1459.
Int J Health Plann Mgmt (2012)
DOI: 10.1002/hpm
ACCESSIBILITY TO HEALTH SERVICES IN GREECE
Stronks K, Ravelli ACJ, Reijneveld SA. 2001. Immigrants
in the Netherlands: equal access for equal needs? J
Epidemiol Commun H 55: 701–707.
Tountas Y, Oikonomou N, Pallikarona G, et al. 2011.
Sociodemographic and socioeconomic determinants
of health services utilisation in Greece: the Hellas
Health I study. Health Serv Manag Res 24(1): 8–18.
Copyright © 2012 John Wiley & Sons, Ltd.
Wilkinson R, Marmot M (eds). 2003. Social Determinants
of Health: The Solid Facts, (2nd ed). World Health
Organization Regional Office for Europe: Copenhagen.
Williams DR, Mohammed SA, Leavell J, Collins C. 2010.
Race, socioeconomic status, and health: complexities,
ongoing challenges, and research opportunities. Ann
NY Acad Sci 1186(1): 69–101.
Int J Health Plann Mgmt (2012)
DOI: 10.1002/hpm









![Vulnerable Populations Perceive Their Health as at …...Vulnerable Populations Perceive Their Health as at Risk from Climate Change Karen L. Akerlof 1 , ... respectively) [11]. Moreover,](https://img.pdfslide.net/doc/110x75/5f06019b7e708231d415d293/vulnerable-populations-perceive-their-health-as-at-vulnerable-populations-perceive.jpg)