Embed Size (px)
Citation preview
The advantages of carbon dioxide laser applications in orthodontic patients
Miss R HannaAssociate Specialist in Oral Surgery
King’s College Hospital NHS Foundation Trust, Department of Oral [email protected]
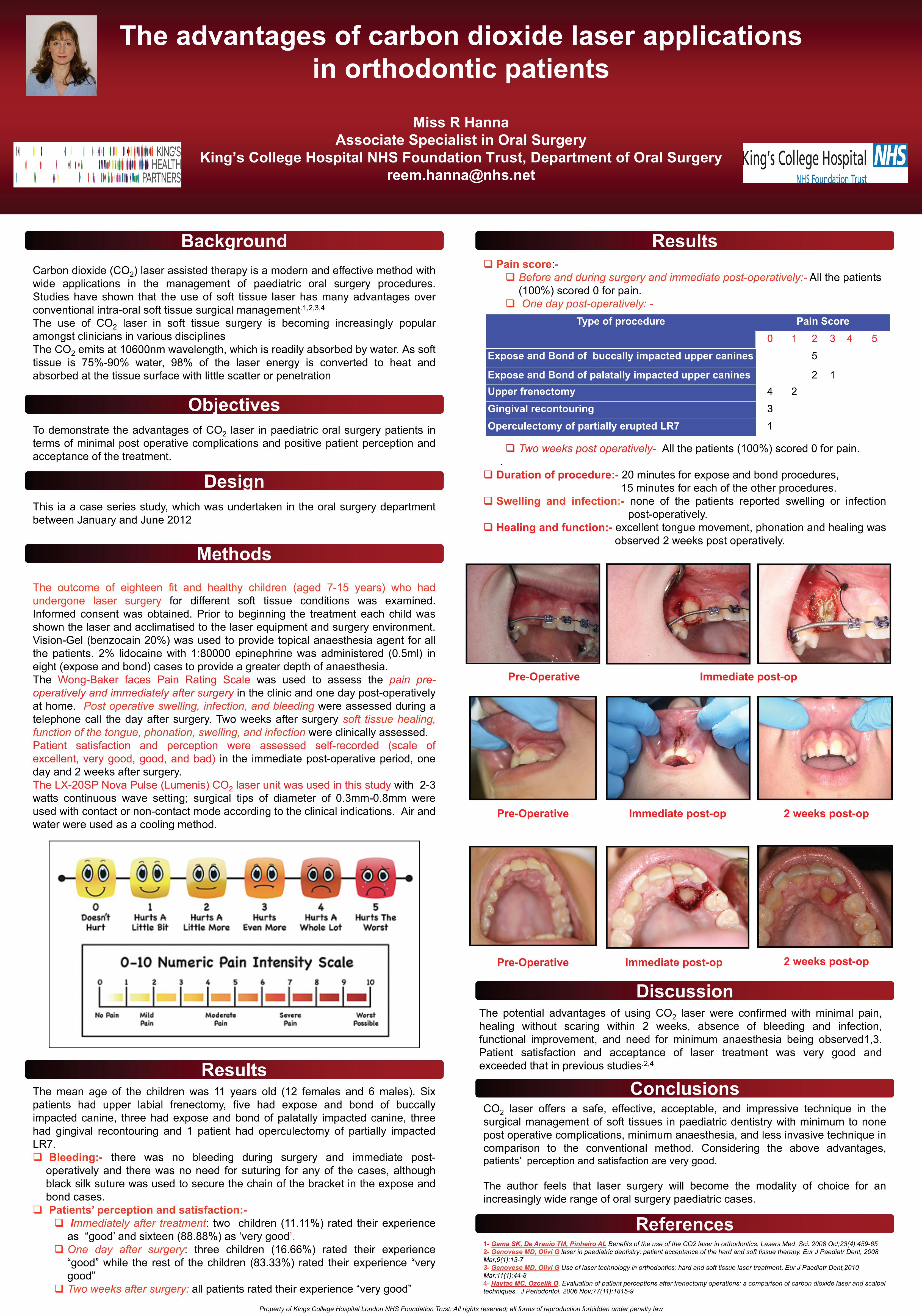
Pre-Operative Immediate post-op
Type of procedure Pain Score0 1 2 3 4 5
Expose and Bond of buccally impacted upper canines 5
Expose and Bond of palatally impacted upper canines 2 1Upper frenectomy 4 2
Gingival recontouring 3
Operculectomy of partially erupted LR7 1
Pre-Operative Immediate post-op 2 weeks post-op
Immediate post-opPre-Operative 2 weeks post-op
Carbon dioxide (CO2) laser assisted therapy is a modern and effective method withwide applications in the management of paediatric oral surgery procedures.Studies have shown that the use of soft tissue laser has many advantages overconventional intra-oral soft tissue surgical management.1,2,3,4
The use of CO2 laser in soft tissue surgery is becoming increasingly popularamongst clinicians in various disciplinesThe CO2 emits at 10600nm wavelength, which is readily absorbed by water. As softtissue is 75%-90% water, 98% of the laser energy is converted to heat andabsorbed at the tissue surface with little scatter or penetration
To demonstrate the advantages of CO2 laser in paediatric oral surgery patients interms of minimal post operative complications and positive patient perception andacceptance of the treatment.
This ia a case series study, which was undertaken in the oral surgery departmentbetween January and June 2012
The outcome of eighteen fit and healthy children (aged 7-15 years) who hadundergone laser surgery for different soft tissue conditions was examined.Informed consent was obtained. Prior to beginning the treatment each child wasshown the laser and acclimatised to the laser equipment and surgery environment.Vision-Gel (benzocain 20%) was used to provide topical anaesthesia agent for allthe patients. 2% lidocaine with 1:80000 epinephrine was administered (0.5ml) ineight (expose and bond) cases to provide a greater depth of anaesthesia.The Wong-Baker faces Pain Rating Scale was used to assess the pain pre-operatively and immediately after surgery in the clinic and one day post-operativelyat home. Post operative swelling, infection, and bleeding were assessed during atelephone call the day after surgery. Two weeks after surgery soft tissue healing,function of the tongue, phonation, swelling, and infection were clinically assessed.Patient satisfaction and perception were assessed self-recorded (scale ofexcellent, very good, good, and bad) in the immediate post-operative period, oneday and 2 weeks after surgery.The LX-20SP Nova Pulse (Lumenis) CO2 laser unit was used in this study with 2-3watts continuous wave setting; surgical tips of diameter of 0.3mm-0.8mm wereused with contact or non-contact mode according to the clinical indications. Air andwater were used as a cooling method.
The mean age of the children was 11 years old (12 females and 6 males). Sixpatients had upper labial frenectomy, five had expose and bond of buccallyimpacted canine, three had expose and bond of palatally impacted canine, threehad gingival recontouring and 1 patient had operculectomy of partially impactedLR7.
Bleeding:- there was no bleeding during surgery and immediate post-operatively and there was no need for suturing for any of the cases, althoughblack silk suture was used to secure the chain of the bracket in the expose andbond cases.Patients’ perception and satisfaction:-
Immediately after treatment: two children (11.11%) rated their experienceas “good’ and sixteen (88.88%) as ‘very good’.One day after surgery: three children (16.66%) rated their experience“good” while the rest of the children (83.33%) rated their experience “verygood”Two weeks after surgery: all patients rated their experience “very good”
Background
Objectives
Design
Methods
Results
Pain score:-Before and during surgery and immediate post-operatively:- All the patients (100%) scored 0 for pain.One day post-operatively: -
Two weeks post operatively- All the patients (100%) scored 0 for pain..
Duration of procedure:- 20 minutes for expose and bond procedures,15 minutes for each of the other procedures.
Swelling and infection:- none of the patients reported swelling or infectionpost-operatively.
Healing and function:- excellent tongue movement, phonation and healing wasobserved 2 weeks post operatively.
The potential advantages of using CO2 laser were confirmed with minimal pain,healing without scaring within 2 weeks, absence of bleeding and infection,functional improvement, and need for minimum anaesthesia being observed1,3.Patient satisfaction and acceptance of laser treatment was very good andexceeded that in previous studies.2,4
CO2 laser offers a safe, effective, acceptable, and impressive technique in thesurgical management of soft tissues in paediatric dentistry with minimum to nonepost operative complications, minimum anaesthesia, and less invasive technique incomparison to the conventional method. Considering the above advantages,patients’ perception and satisfaction are very good.
The author feels that laser surgery will become the modality of choice for anincreasingly wide range of oral surgery paediatric cases.
1- Gama SK, De Arauio TM, Pinheiro AL Benefits of the use of the CO2 laser in orthodontics. Lasers Med Sci. 2008 Oct;23(4):459-65. 2- Genovese MD, Olivi G laser in paediatric dentistry: patient acceptance of the hard and soft tissue therapy. Eur J Paediatr Dent, 2008 Mar;9(1):13-73- Genovese MD, Olivi G Use of laser technology in orthodontics; hard and soft tissue laser treatment. Eur J Paediatr Dent,2010 Mar;11(1):44-84- Haytac MC, Ozcelik O. Evaluation of patient perceptions after frenectomy operations: a comparison of carbon dioxide laser and scalpel techniques. J Periodontol. 2006 Nov;77(11):1815-9
Results
Discussion
Conclusions
References
Property of Kings College Hospital London NHS Foundation Trust: All rights reserved; all forms of reproduction forbidden under penalty law