Embed Size (px)
Citation preview

International Journal of Pediatric Otorhinolaryngology (2004) 68, 877—881
The age dependent relationship betweenfacial fractures and skull fractures�
James Chana, Michelle A. Putnamb, Paul J. Feustelb, Peter J. Koltai a,*
a Department of Otolaryngology and Communicative Disorders, The Cleveland Clinic Foundation,A71, 9500 Euclid Avenue, Cleveland, OH 44195 USAb Division of Otolaryngology, Albany Medical College, Albany, NY, USA
Received 12 January 2003 ; received in revised form 27 January 2004; accepted 27 January 2004
KEYWORDSPediatric facialfractures;Skull fractures;Epidemiology;Facial trauma
Summary Objective: To provide clinical evidence to support the age dependent re-lationship between facial fractures and skull fractures. Design: Retrospective chartreview of all children and adults admitted with combined facial fractures and skullfractures and skull fractures alone between January 1991 and November 1997. Setting:The Albany Medical Center Hospital, a tertiary level-one trauma center. Patients: Twohundred and one children, ages 1 month to 17 years, with skull fractures (frontal, pari-etal, or temporal), and 41 children with concurrent facial fractures were included inthis study. One hundred and thirty-nine adults, ages 18—90 years, with skull fractures,and 70 adults with concurrent facial fractures were also studied. Outcome measures:The gender, age, skull fracture, facial fracture, Glasgow coma score (GCS), mecha-nism of injury, and outcome of all patients admitted with frontal, parietal, or temporalfractures with or without facial fractures. Results: There are a significantly greater(P < 0.001) number of facial fractures associated with skull fractures among adults ascompared to children. Moreover, there is an exponential rise in facial fractures associ-ated with skull fractures between infancy and adolescence. The GCS of children withcombined facial and skull fractures is significantly lower than in those with skull frac-tures only (P < 0.001). Conclusion: The spectrum of craniofacial injuries is related tothe specific developmental stage of the craniofacial skeleton. This is demonstratedby the variable pattern of combined facial and skull fractures observed clinically inchildren and adults.© 2004 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
The clinical variation in the incidence of craniofa-cial fractures appears to be age related. This ob-servation suggests that the face, which is smallerrelative to the skull in children than in adults, ex-
� Presented at the AO ASIF Craniomaxillofacial Advanced Sym-posium, Tucson, Arizona, 22 February 2003.
*Corresponding author. Tel.: +1-216-445-5022;fax: +216-445-9409.
E-mail address: [email protected] (P.J. Koltai).
hibits facial fracture patterns that are influencedby the changing craniofacial geometry of a growingchild. If this is correct, then the incidence of facialfractures associated with skull fractures should belower in young children, and increase as the facegrows downward and outward during normal mat-uration. To test this hypothesis, the records of 340patients were reviewed with skull fractures in thefrontal, parietal, and temporal bones over a 7-yeartime span. They were then analyzed according towhether they had a skull fracture alone or a skullfracture with concomitant facial fractures.
0165-5876/$ — see front matter © 2004 Elsevier Ireland Ltd. All rights reserved.doi:10.1016/j.ijporl.2004.01.021

878 J. Chan et al.
2. Patients and methods
The information in this study is derived from a ret-rospective review of the 340 patients from the agesof first month of life to 90 years of age who wereadmitted to the Albany Medical Center Hospital be-tween January 1991 and November 1997 with a di-agnosis of skull vault fracture consisting of eitherfrontal, parietal or temporal bones. Five patientswere omitted from the study because there was noevidence of skull fracture by computed tomography(CT). The charts were then reviewed for associatedfacial fractures: orbital, nasal, maxillary, mandibu-lar, and zygomatic. The sex, age, Glasgow comascore, mechanism of injury, and outcome were allrecorded. The anatomic site of the fractures wasdetermined from CT scans as well as from operativereports.
Statistical tests were performed using softwarepackage (Minitab StatiScal: Software for WindowsRelease 12.21). For continuous data, groups werecompared using the Student’s t-test and for cat-egorical data Yates corrected Chi-square test wasused with significance accepted at the P < 0.05level.
3. Results
Of the 201 children age 0—17 years, only 41 (20.3%)had facial fractures associated with their skullfractures. Of the 139 adults age 17—90, only 70(50.4%) had facial fractures. There were a signifi-cantly greater number of facial fractures in adultsas compared to pediatric patients (P < 0.001, χ2).
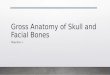
The mean age of all children (age 19 days to17 years) with skull fractures was (mean ± S.E.)4.07 ± 0.36 and the median age was 3 years. Themean age of the 41 children with skull fracturesand facial fractures was 7.62 ± 0.82 (mean ± S.E.).Children with facial fractures were statistically sig-
0%10%20%30%40%50%60%70%80%
< 1 Y
R3 Y
R6 Y
R9 Y
R12
YR
15 Y
R18
YR
21-2
5 YR
36-4
0 YR
56-6
5 YR
76-9
0 YR
AGE IN YEARS
FA
CIA
L F
RA
CT
UR
E P
ER
SK
UL
L F
RA
CT
UR
E
(PE
RC
EN
TA
GE
)
Fig. 1 Incidence of facial fractures with age.
nificantly older than those without facial fractures(P < 0.001, t-test).
The mean age of adult’s (age 18—90 years) was39.3 ± 2.3 (mean ± S.E.), and the median age was34 years. The mean age of the 139 adults with skullfractures and facial fractures was 37.7 ± 2.2 (mean± S.E.). Age was not different between those withand without facial fractures in the adult population(P = 0.64, t-test) (Fig. 1).
Of the 201 children, 116 [57.7 ± 0.35%, (95% con-fidence interval 0.508—0.646)] were boys and 85(42.3%) were girls (ratio, 1.3:1). Among the 139adults, 110 (79.1%) were boys and 29 (20.9%) weregirls (ratio 3.8:1). In our study population, therewasa preponderance of males. Adult males were signif-icantly more likely to sustain a facial fracture withskull fracture than their associated female counter-parts (P < 0.001, χ2).
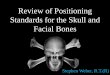
The mechanisms of injury were: motor vehicleaccidents (MVA) in 21 children (10.4%), falls in 109children (54.2%), assault/explosion/abuse in 34children (16.9%), MVA versus pedestrian in 30 chil-dren (14.9%), motorcycle/all terrain vehicle (ATV)in 7 children (3.5%). The mechanisms of injuryleading to concomitant facial fractures were: MVAin 8 children (19.5%), falls in 14 children (34.1%),assault/explosion/abuse in 3 children (7.3%), MVAversus pedestrian in 11 children (26.8%), motorcy-cle/ATV in 5 children (12.2%) (Fig. 2).
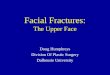
The mechanisms of injury were: MVA in 49adults (35.2%), falls in 25 adults (18.0%), assault/explosion/abuse in 32 adults (23.0%), MVA versuspedestrian in 17 adults (12.2%), motorcycle/ATV in16 adults (11.5%). The mechanisms of injury lead-ing to concomitant facial fractures in adults were:MVA in 33 adults (47.1%), falls in 10 adults (14.2%),assault/explosion/abuse in 15 adults (21.4%), MVAversus pedestrian in 6 adults (8.6%), motorcy-cle/ATV in 6 adults (8.6%) (Fig. 3).
Of the 41 children with skull fractures and fa-cial fractures, the mean Glasgow coma score (GCS)

Age dependent relationship of craniofacial fractures 879
020406080
100120
MV
A
FA
LL
S
AS
SA
UL
T
MV
A V
S.
PE
DE
ST
RIA
N
OF
F R
OA
DV
EH
ICL
E
MECHANISM
NU
MB
ER
OF
FR
AC
TU
RE
S
SKULL FRACTURES
FACIAL FRACTURES
Fig. 2 Mechanism of injury in children <17 years of age.
0102030405060
MV
A
FA
LL
S
AS
SA
UL
T
MV
A V
S.
PE
DE
ST
RIA
N
OF
F R
OA
DV
EH
ICL
E
MECHANISM
NU
MB
ER
OF
FR
AC
TU
RE
S
SKULL FRACTURES
FACIAL FRACTURES
Fig. 3 Mechanism of injury of adults >17 years of age.
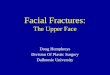
was 10.98 ± 0.70 (mean ± S.E.). The mean GCSof children with skull fractures without associatedfacial fractures was 13.43 ± 0.25 (mean ± S.E.).Facial fractures in children are significantly morelikely to result in a greater severity of injury, basedon the lower GCS, than those children with skullfractures alone (P < 0.001, t-test). Of the 70 adultswith skull fractures and concomitant facial frac-tures, the mean GCS was 10.71 ± 0.52 (mean ±S.E.). The mean GCS of the 69 adults with skull frac-tures without associated facial fractures was 9.58± 0.52 (mean ± S.E.). Facial fractures in adults arenot significantly likely to result in a greater severityof injury (P = 0.15, t-test) (Fig. 4).
3
5
7
9
11
13
15
CHILDREN (<17YEARS OF AGE)
ADULTS (>17 YEARSOF AGE)
PATIENT POPULATION
GC
S
SKULL FRACTURE ONLY
SKULL FRACTURE PLUSFACIAL FRACTURE
Fig. 4 GCS comparison.
4. Comments
4.1. Epidemiology
Pediatric facial fractures account for 5 to 15% ofall maxillofacial injuries. Children 7 years of ageand younger have a substantially lower risk, and itis not until late adolescence, with the maturationof the face and adoption of a fast-paced lifestyle,that the frequency and the distribution of facialfractures evolves into the pattern seen in adults. Insome reports, a male predominance becomes ap-parent in older children and is interpreted to reflectthe more aggressive risk-taking behavior of preteen

880 J. Chan et al.
and adolescent boys [1—7]. Our study concurs withthese reports and demonstrates an age dependant,increasing ratio of males to females.
Nasal fractures are the most common facial boneinjuries in children. Many of these are treated in anoutpatient setting, and therefore, their true fre-quency is difficult to determine. Mandible fracturesare the most common facial fractures in childrenrequiring hospitalization and account for approx-imately 30% of injuries [1,8,9]. Middle and upperfacial fractures have traditionally been consid-ered uncommon in children; nevertheless, recentreports have consistently shown an incidence oforbital fractures ranging from 10 to 30% [1,10,11]These high figures reflect the variable classificationof orbital injuries. Skeletal components of the face,such as the nasoethmoid region, zygomaticomalarcomplex, and frontal bone are contiguous with andhave fractures that extend to the orbit [1].
4.2. Craniofacial development
Two distinct but related factors of facial growthaffect the changing pattern of facial fractures inchildren. The first of these is growth of the face inrelationship to the cranium and the changing geom-etry between the two. The second is the expansionof the paranasal sinuses that surround the orbit.The size of the human newborn’s head is a finebalance between the diameter of the birth canal,a disproportionately large brain, and a face that issufficiently developed to allow for respiration andalimentation. The craniofacial ratio at birth is 8:1,and spatially, the face is recessed under the rela-tively large skull. Initially, the cranium grows fasterthan the face, reaching 80% of its mature size bythe age of 2 years. Brain and ocular growth are nearcompletion by age 7 years. Facial growth, however,continues into the second decade of life and byadulthood, the craniofacial ratio is 2:1 [1,11,12].
The architectural changes of facial enlargementstem from bone growth and mineralization, as wellas pneumatization of the paranasal sinuses. Atbirth, all the sinuses are present as buds of mucosawithin a matrix of cancellous bone covered by thincortical plates. The ethmoid air cells, which are themain structure affecting intraorbital dimension,expand at a steady rate so that by 7 years of age,70% of the interorbital width is reached [13]. In thenewborn, the maxillary sinus is medial to the globeso that the alveolar margin is close to the inferiororbital rim. Its rate of pneumatization varies, how-ever by 7 years of age, the sinus has widened pastthe mid-pupillary line and lengthened to occupyhalf of the lateral nasal wall. The frontal sinusesare initially indistinct from the anterior ethmoid
air cells, but a slow expansion brings them abovethe superior orbital rim around seven yeas of age[14]. Therefore, it appears that before the ageof 7 years, the large cranium is more likely to beexposed to trauma than the proportionally smallerface. The present study provides clinical evidenceto support this, as skull fractures alone were morecommon in the pediatric population compared to ahigher incidence of concomitant facial fractures inadults.
The unfolding of the face from beneath the pro-tective overhanging cranium, a consequence ofcontinued growth of the maxilla, results in the ex-posure of the face to an increased risk of trauma.Fundamental to this process and an integral partof pneumatization, is the remodeling of the elasticcancellous bone of the infant’s face into the adultform of compact and dense bony buttresses con-nected by thin and brittle membranous bony plates[1].
4.3. Injury severity
The combination of paranasal sinus pneumatizationand increasing mineralization of the facial bonesprovide protection to the cranium. This reflects thelower GCS score that was observed in children withconcomitant facial fractures in this study. In chil-dren, it appears that facial fractures imply a higherenergy injury. This likely relates to the lack of pro-tection of the brain by the pneumatized sinuses andmineralized, developed, bony buttresses that arepresent in adults. In adults, the GCS score was notsignificantly different between those who sufferedskull fractures alone as compared to those with as-sociated facial fractures. There appears to be a re-verse relationship in the adult population, howevernot statistically significant, of a higher GCS in theconcomitant facial fracture group compared to thegroup with skull fractures alone. This suggests thatthe adult face may provide an absorption barrier tothe cranium transmitting energy to the facial bonesand away from the central nervous system.
4.4. Clinical implications
The age dependant relationship between skull frac-tures and facial fractures lends clinical support tothe idea that fracture patterns are related to cran-iofacial development. The lower GCS in childrenwith concomitant facial fractures imply that inves-tigation of central nervous system injuries should bepursued in children with combined skull and facialfractures. Furthermore, development of protectivedevices should take into account the severity of fa-cial injuries in children.

Age dependent relationship of craniofacial fractures 881
5. Conclusion
The pattern of craniofacial fractures in children andadults is age dependent and developmentally spe-cific. The age distribution of facial fractures, reflectthe high craniofacial ratio of the young child, thevulnerability of the large cranium to trauma, andthe lack of pneumatization of the paranasal sinuses.The exponential rise in the incidence of facial frac-tures associated with skull fractures in children, re-flect the growth and development of the face thatunfolds from beneath the overhanging cranium andbecomesmore vulnerable to trauma. The lower GCSin children sustaining facial fractures suggests thata higher energy injury may be required for com-bined skull and facial fractures in the pediatric pop-ulation. Our review of the literature supports amalepreponderance of facial fractures in children andadults, however there is a trend toward 50:50 inthe younger population changing to an obvious malepredominance in the older adult population.
References
[1] P.J. Koltai, I. Amjad, D. Mayer, P.J. Feustel, Orbital frac-tures in children, Arch Otolaryngol Head Neck Surg. 121(1995) 1375—1379.
[2] P.J. Koltai, Maxillofacial injuries in children, in: J.D.Smith, R. Brumstead (Eds.), Pediatric Facial Plastic and
Reconstructive Surgery, Raven Press, New York, NY, 1993,pp. 283—316.
[3] N.L. Rowe, Fracture of the facial skeleton in children, J.Oral. Surg. 26 (1967) 505—515.
[4] L.B. Kaban, Diagnosis and treatment of fractures of thefacial bones in children 1943—1993, J. Oral. Maxillofac.Surg. 51 (1993) 722—729.
[5] G.S. Gussck, A. Lutterman, K. Rodgers, R.W. Powell, M.Ramenofsky, Pediatric maxillofacial trauma: unique fea-tures in diagnosis and treatment, Laryngoscope 97 (1987)925—930.
[6] M.A. Fortunato, A.F. Fielding, L.H. Gurensey, Facial bonefractures in children, Oral. Surg. Oral. Med. Oral. Pathol.53 (1982) 225—231.
[7] B.L. McGraw, R.R. Cole, Pediatric maxillofacial trauma,Arch. Otolaryngol. Head Neck. Surg. 116 (1990) 41—45.
[8] R.K. Hall, Injuries of the face and jaws in children, Int. J.Oral. Surg. (1972) 65—75.
[9] L.B. Kaban, J.B. Mulliken, J.E. Murray, Facial fractures inchildren an analysis of 122 fractures in 109 patients, Plast.Reconstr. Surg. 59 (1977) 15—20.
[10] J.C. Posnick, M. Wells, G.E. Pron, Pediatric facial fractures:evolving patterns of treatment, J. Oral. Maxillofac. Surg.51 (1993) 836—844.
[11] J.M. Converse, Facial injuries in children, in: V.H. Kazan-jian, J.M. Converse (Eds.), The Surgical Treatments of Fa-cial Injuries, second ed., Williams & Wilkins, Baltimore,MD, 1959, pp. 299—315.
[12] D.H. Endlow, Facial Growth, third ed., WB Saunders Co.,Philadelphia, PA, 1990, pp. 1—24.
[13] J.D. Morin, J.C. Hill, J.E. Anderson, R.M. Grainger, A studyof growth in the interorbital region, Am. J. Ophthalmol.56 (1963) 895—901.
[14] A. Onodi, Accessory Sinuses of the Nose in Children,William Wood & Co., New York, NY, 1911, plates 4—90.