Embed Size (px)
Citation preview
The alternatives: in defence
of naso-gastric tubes
Tracy Earley
Consultant Nurse
Lancashire Teaching Hospitals NHS Foundation Trust.
NGT’s Friend Or Foe?
Indications for NGT Feeding
For short to medium term feeding
Decreased appetite
Inability to feed
Gastro-intestinal disease
Increased nutritional requirements
When PEG cannot be placed safely
Positive Aspects of NGT’s Inexpensive
Low risk of complications
Can be used as a supplement to oral intake or to provide complete
nutritional requirements
Nasogastric tube insertion is a relatively simple and safe procedure
Contraindications
Absolute and Relative Recent Nasal surgery or mid face trauma
Fractured base of skull
Oesophageal disease
– Varices
– Carcinomas
– Pouches
Nasal Tumours
Nasal septum deviation
Congenital abnormalities to the nose
Severe gastric reflux or vomiting
Negative Aspects of NGT’s
Negative Aspects of NGT’s
Short to medium term usage only
Can be displaced
Can be prone to blockage
Very Obvious
Requires testing to confirm position each
day prior to usage
Resource
Implications for NGT’s
Time consuming to replace
Difficult to keep secured in some patients
Night time displacement a problem often !
Traumatic to replace for patients (and staff
sometimes !)

Successful NGT placement is
an achievement which both
patients and staff are relieved
and elated by
Now we just need to ensure it doesn't come out !!!!!!!
What are the Options?
Short term – NGT
Short term / Medium term + Community – NGT / PEG
Medium to Long term + Community – PEG
PEG is usually always preferable, however – these options may not always be possible or practical
Why PEG may
not be Possible Patient Choice
Severe contractures
Gastric surgery
Short life expectancy (and patient choice to
continue feeding)
The alternative
LTHTR model :
Offer Nasal Bridle to secure NGT in displaced tubes or short – medium term patients in community.
Training for nursing homes to re-pass their own tubes
Rapid access nutrition nursing service service mon - fri
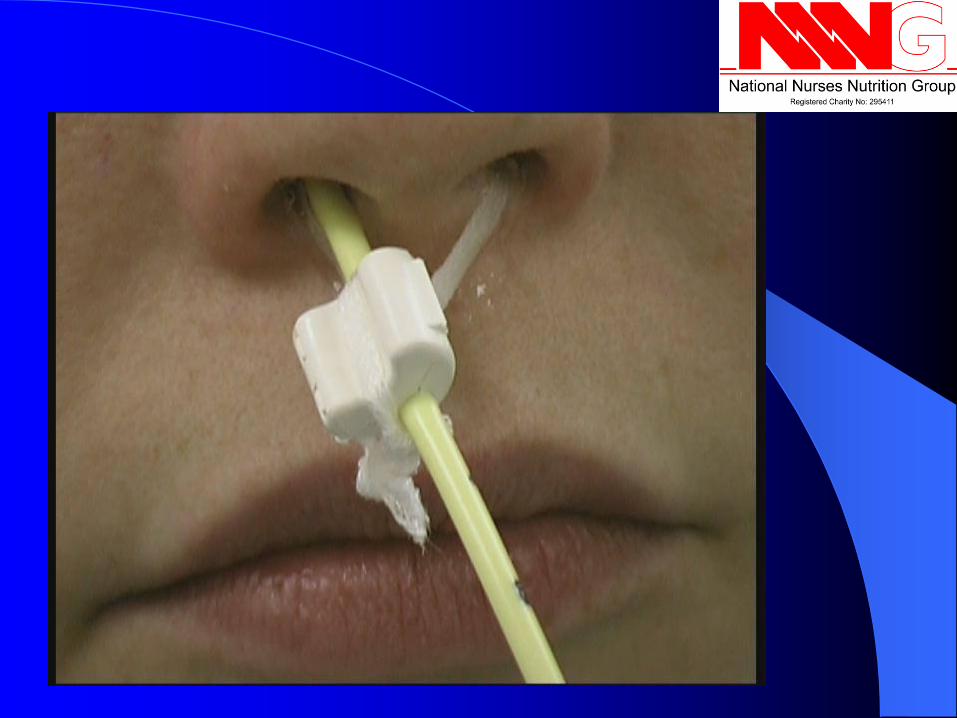
Nasal Bridle
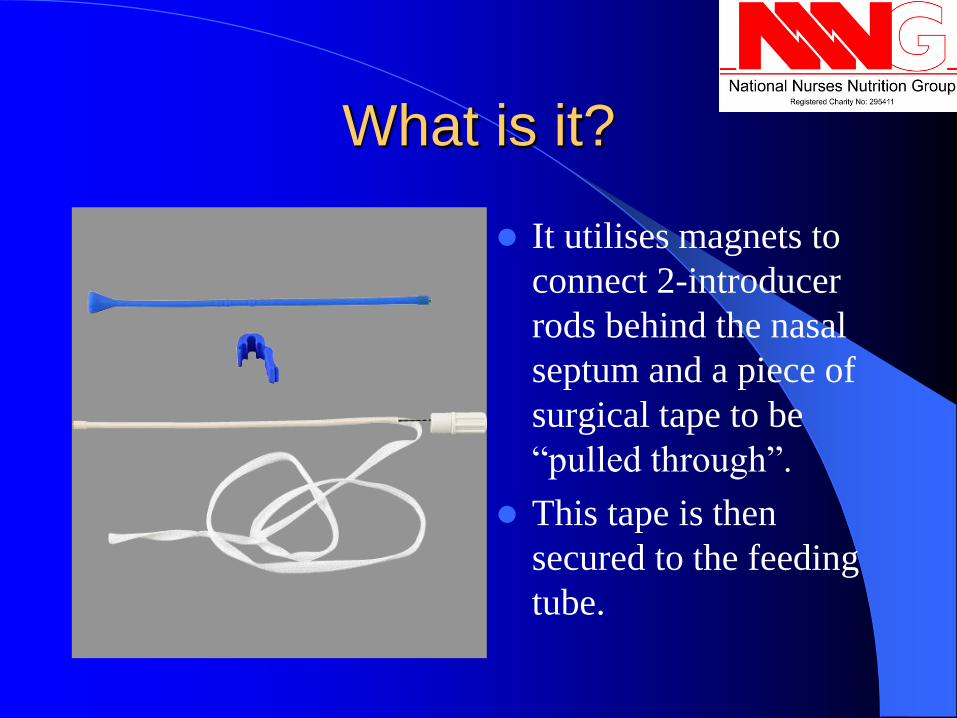
What is it?
It utilises magnets to
connect 2-introducer
rods behind the nasal
septum and a piece of
surgical tape to be
“pulled through”.
This tape is then
secured to the feeding
tube.
Introduction
1st described in 19801
Safe & effective2,3
Traditional uses
– Head & neck malignancy
– Critical care
– Paediatric intensive care
1. McGuirt WF, Strout JJ, „Securing of Intermediate Duration Feeding Tubes‟ Laryngoscope 1980; 90: 2046-48.
2.Levenson R, Dyson A, Turner W, „Feeding tube anchor‟ Nutr Support Serv 1985; 5: 40-42.
3.Barrocas A, Jastram C, St Romain C, „The Bridle: increasing the use of nasoenteric feeding‟ Nutr Support Serv 1982; 2: 8-10.











Patient Review
with Nasal Bridle If In- Patient – Review within two weeks of
commencing feed to assess. PEG if appropriate
If discharged with NGT / Bridle then Review by
HEF dietitian in three months to assess if enteral
route still required
Return to Rapid access clinic for replacement of
NGT / Bridle as needed.
Continued regular review.
Benefits of NGT
and Nasal Bridle
Increased security of NGT
Increased Comfort for Patients with NGT
Able to enterally feed those patients who
require short term feeding without having to
resort to PEG.
Able to enterally feed a large population
who cannot have PEG placed.

NGT replacement
in Community Targeted replacement in some nursing homes, but
not yet nasal bridle
Support from nutrition nursing team
Initial trainee in nursing home selected and then
competency assessed by Nutrition nurses
They then become cascade trainers
Rapid access nutrition nursing service mon – fri
for advice and support

Rapid Access
Nutrition Nursing
Service
Based at Royal Preston Hospital site.
Open week days except bank holidays
Dedicated telephone helpline.
Service Now:
Runs days mornings (sessions) per week based in Endoscopy
Six slots per session (follow up / day case / new patient)
Widened access gates – existing patients with enteral / Parenteral
feeding devices problems are referred via GP’s, District Nurses,
patients, carer’s.
New referrals for assessment of patient’s suitability for feeding
device, for paediatrics undergoing transition, or patients new to the
area.
Central telephone number for all referrals.
Nurse led with wide skill set for assessing and treating patients
Templated on Trust system so financial revenue as a result
Protocols accepted by Trust for band 6 and 7 nutrition nurses
Nurse led discharge
Clinic letter given to patient / carer at the end of appointment
Formal letters out to GP within 5 days
Benefits
See > 500 patient episodes annually
Patients seen by clinical specialists equipped to
trouble shoot / replace their devices.
Discharge >98% patients home the same day.
Avoids hospital admissions
Relieves pressure on IP / OP services
Liaise directly with other colleagues should the
need arise.
Summary
Where possible in medium – long term
patients who require enteral feeding place a
PEG.
However, NGT feeding in short to medium
term needs NGT with Nasal Bridle can be
successful with targeted training for
community colleagues AND support of
local hospital for trouble shooting.





























