Embed Size (px)
Citation preview
ORIGINAL PAPER
The assessment of the malignant mesothelioma casesand environmental asbestos exposure in Sivas province,Turkey
Serdar Berk • Huseyin Yalcin •
Omer Tamer Dogan • Kursat Epozturk •
Ibrahim Akkurt • Zehra Seyfikli
Received: 11 September 2012 / Accepted: 25 March 2013 / Published online: 4 April 2013
� Springer Science+Business Media Dordrecht 2013
Abstract One of the most significant diseases
related to environmental asbestos exposure is malig-
nant mesothelioma (MM). Sivas province is located in
the Central Anatolia where asbestos exposure is
common. We aimed to study clinical, demographical
and epidemiologic features of the patients with MM in
Sivas, along with the history of asbestos exposure. In
total, 219 patients with MM who were diagnosed in
our hospital between 1993 and 2010 were retrospec-
tively analyzed in terms of demographical and clinical
features. Rock, soil and house plaster samples were
taken from the habitats of those patients and were
evaluated with optical microscopy and X-ray diffrac-
tion methods. The age of the patients ranged between
18 and 85 years. The male-to-female ratio was 1.4:1.
Most of the patients confirmed an asbestos exposure
history. The most frequent symptoms of the patients
were chest pain (60 %) and dyspnea (50 %). The gap
between the start of first symptoms and the diagnosis
date was approximately 4 months in average. The
plaster materials used in most of the houses were made
up of mainly carbonate and silicate minerals and some
chrysotile. Ophiolitic units contained fibrous minerals
such as serpentine (clino ? orthochrysotile) chiefly
and pectolite, brucite, hydrotalcite and tremolite/
actinolite in smaller amounts. MM is not primarily
related to occupational asbestos exposure in our
region, and hence, environmental asbestos exposure
may be indicted. Yet, single or combined roles and/or
interactions of other fibrous and non-fibrous minerals
in the etiology of MM are not yet fully understood and
remain to be investigated.
Keywords Asbestos � Chrysotile � Environmental
exposure � Malignant mesothelioma
Introduction
The most common primary malignant tumor of the
pleura is malignant mesothelioma (MM), an insidious
neoplasm with a poor prognosis arising from the
mesothelial surfaces of pleural and peritoneal cavities,
as well as from the tunica vaginalis and pericardium.
Eighty percent of all cases of mesothelioma are pleural
in origin (Sterman et al. 2008). The development of
malignant pleural mesothelioma (MPM) is related to
asbestos exposure even if some patients have no such
contact history; the proportion of asbestos-associated
mesotheliomas varies in the literature from 16 to
90 %, probably depending on the accuracy of expo-
sure history (Walker et al. 1983). Asbestos refers to
mineral groups of thin fibers including serpentine type
S. Berk (&) � O. T. Dogan � K. Epozturk �I. Akkurt � Z. Seyfikli
Department of Chest Diseases, Faculty of Medicine,
Cumhuriyet University, 58140 Sivas, Turkey
e-mail: [email protected]
H. Yalcin
Department of Geological Engineering, Cumhuriyet
University, Sivas, Turkey
123
Environ Geochem Health (2014) 36:55–64
DOI 10.1007/s10653-013-9518-y
(chrysotile) and amphibole type (riebeckite/crocido-
lite, cummingtonite-grunerite/amosite, anthophyllite,
actinolite/tremolite). Nearly, 95 % of the asbestos
consumed worldwide is chrysotile and most other
fibers are commonly used in combination with it
(Weiner and Miandoab 2009). Although its use was
widely abandoned in the Western world in the 1980s,
the long latency period between the exposure to
asbestos and the onset of mesothelioma which could
range from 15 to 60 years meant that the mortality
rates from mesothelioma have continued to rise
(Moore et al. 2008).
Our institution is a tertiary referral hospital and
patients originate mostly from Sivas and three neigh-
boring cities, namely Tokat, Erzincan and Yozgat. The
province of Sivas is located in the mid-eastern part of
Anatolia. It includes 17 districts and 1,236 villages; its
population is approximately 600,000, 34 % of which
live in rural areas. Despite a fall in its use in recent
years, asbestos-contaminated soil has been used for
many years as a whitewash and stucco (named locally
as ‘‘white’’ or ‘‘barren’’ soil) in the wall of the houses
in rural areas. After the relationship between meso-
thelioma and asbestos emerged at the beginning of
1960s (Wagner et al. 1960), many studies have been
carried out on this topic and arguments have been still
continued within the scope of medicine and medical
geology (Yang et al. 2008). Previous studies have
revealed that environmental exposure to asbestos
through the use of asbestos-contaminated soil mix-
tures caused a high risk of MPM in some parts of rural
Anatolia in Turkey (Baris 1987; Baris et al. 1979;
Metintas et al. 2002; Senyigit et al. 2000; Yazicioglu
et al. 1980). We aimed in this study to investigate the
relationships between environmental mineralogical
effects and clinical, demographical and exposure
features of patients with MM in the Sivas province.
Materials and methods
Patients
A total of 219 patients with MM who were diagnosed
in our hospital between January 1993 and December
2010 were retrospectively analyzed. Of these, 207
(95 %) were diagnosed histopathologically and 12
(5 %) were diagnosed given the clinical and radiolog-
ical features suggesting MM and the presence of
asbestos exposure history. Clinical information,
including age, sex, birthplace, history of occupational
and environmental exposure to mineral fibers, char-
acter and duration of symptoms, and clinical findings
at presentation, was extracted from the patients’ files.
The environmental exposure is expressed as the
duration of living in houses where asbestos-contam-
inated soil was used.
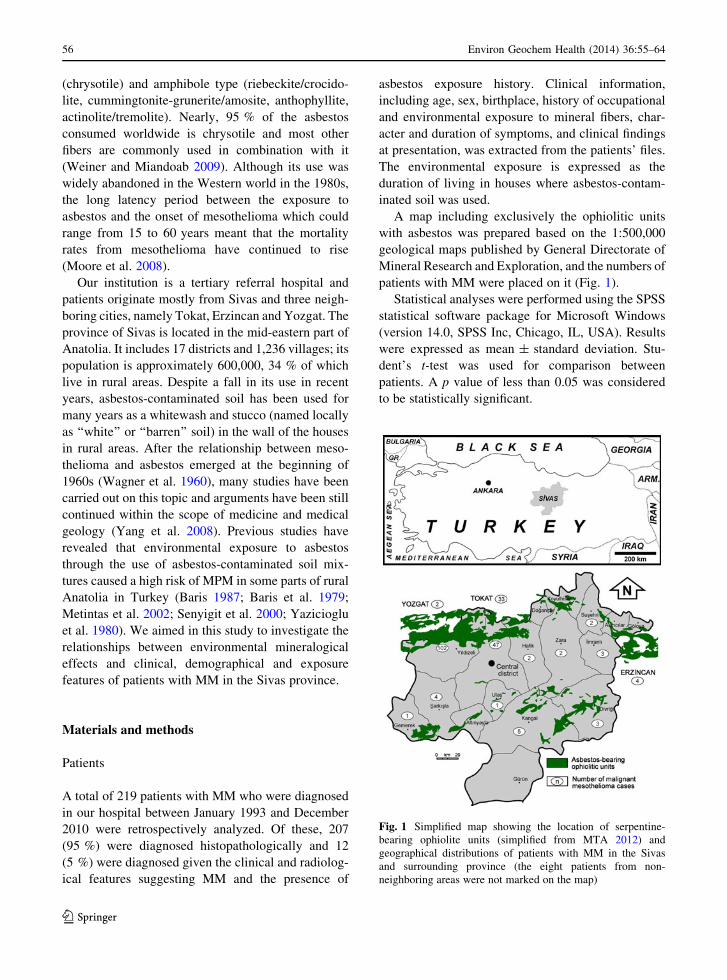
A map including exclusively the ophiolitic units
with asbestos was prepared based on the 1:500,000
geological maps published by General Directorate of
Mineral Research and Exploration, and the numbers of
patients with MM were placed on it (Fig. 1).
Statistical analyses were performed using the SPSS
statistical software package for Microsoft Windows
(version 14.0, SPSS Inc, Chicago, IL, USA). Results
were expressed as mean ± standard deviation. Stu-
dent’s t-test was used for comparison between
patients. A p value of less than 0.05 was considered
to be statistically significant.
Fig. 1 Simplified map showing the location of serpentine-
bearing ophiolite units (simplified from MTA 2012) and
geographical distributions of patients with MM in the Sivas
and surrounding province (the eight patients from non-
neighboring areas were not marked on the map)
56 Environ Geochem Health (2014) 36:55–64
123

Mineralogical investigations
Since 1990s, hundreds of samples such as rock, soil
and house plasters were collected from habitats of MM
patients and analyzed by optical microscopy and
X-ray diffraction (XRD) methods at the Geological
Engineering Department laboratory and scanning
electron microscopy (SEM) with a JEOL JSM-6490
instrument equipped with IXRF energy dispersive
spectrometry (EDS) system at the Turkish Petroleum
Corporation in Ankara, Turkey. Textural and miner-
alogical features of coarse-grained hard samples with
fibrous minerals were determined on the thin sections
by binocular optical polarizing microscopy. SEM
operating conditions were 32 s counting time and
20 kV accelerating voltage. EDS spot analyses (spot
size of 50 lm for focused electron beam) were also
used during SEM investigations to differentiate
serpentine minerals from similar constituents.
The fine-grained whole-rock and clay fraction XRD
analyses were undertaken using a Rigaku DMAX IIIC
diffractometer with the following settings: Cu-Ka,
35 kV, 15 mA, slits (divergence = 18, scatter = 18,receiving = 0.15 mm, receiving monochromator =
0.30 mm), scan speed 2�2h/min. The semiquantitative
percentages of the minerals were calculated using the
external standard method. Serpentine-bearing clay
fractions (\2 mm) from the inorganic materials were
separated by the sedimentation method and analyzed
under air-dried (at 25 �C for 16 h), ethylene-glycolat-
ed (in a desiccator at 60 �C for 16 h) and heated
(490 �C for 4 h) conditions. Serpentine polytypes for
non-oriented powder samples have been detected with
diagnostic peaks.
Results
Epidemiology and clinical findings
Of the 219 patients, 126 (57.5 %) were men and 93
(42.5 %) women. The male-to-female ratio of the
patients was 1.4:1. The age of the men ranged from 18
to 85 years (mean, 58.8 ± 12.7 years). The age of the
women ranged from 34 to 85 years (mean, 58.9 ±
13.1 years). A large proportion of the patients
(28.8 %) were in the 60–69 years age group, 23.3 %
were 70 years old or above, and 17 patients (7.8 %)
were aged less than 40 years. The youngest patient
was diagnosed at the age of 18. There was no
significant difference in the mean age between men
and women.
More than 84 % of patients were farmers and
housewives, and they had lived in a rural area all their
lives or for a long time. Four (1.8 %) patients had an
occupational history with a potential risk for asbestos
exposure (one dozer operator, one painter, one railway
worker and one working with concrete sleepers). One
hundred and ninety-six (86 %) patients had a history
of living in a house containing asbestos-contaminated
soil, for about 40 ± 20 years in average (minimum: 3,
maximum: 70 years). The most frequent symptoms of
the patients were chest pain (60.2 %) and dyspnea
(50.2 %). There were approximately 4 months in
average between the start of the first symptoms and
the diagnosis date of the disease. There was no
significant difference between men and women in the
duration of symptoms (male: 3.7 ± 3.8 months,
female: 3.9 ± 4.5 months). Table 1 displays some of
the demographical and clinical characteristics of the
patients.
When the places of residence of 219 patients were
assessed, it was determined that 172 (78.5 %) patients
were residing in Sivas and the rest in other provinces.
Nearly, half of the patients came from Yildizeli district
(see Fig. 1).
According to the data from local civil registry
office, it was determined that 34 % of the total
population and 82 % of the population in Yildizeli
particularly were residing in rural areas (Table 2).
Geological and mineralogical findings
Ophiolites are parts of the Earth’s lithosphere that
surfaced above sea level and are often made of green
rocks such as serpentine. Ophiolitic units bearing
serpentine group of mainly Cretaceous age and their
transported products into soils are widespread and
extend hundreds of kilometer in Turkey and particu-
larly in Sivas region based on the map of MTA (2012)
(see Fig. 1). In the Ulas district of southeastern Sivas,
the dark green unaltered peridotitic ultramafic rocks
are preserved as lens-like forms of 1–5 m within the
serpentinites which are cut by thin-coarse grained and
grayish green-black pyroxenite, gabbro and diorite
dykes of commonly 1–2 m (partly 20–30 m) in
thickness. The host rocks of asbestos are layers of
approximately 100 m thick and brecciated
Environ Geochem Health (2014) 36:55–64 57
123
serpentinites of 10–20 m thick. Of these, first is of
blackish green to brown-honey-colored, mesh-tex-
tured, soapy, slippery and abundant cracks, and the
other is similar to layered ones but made up of angular
to sub-angular grains ranging a few mm to 15 cm in
size.
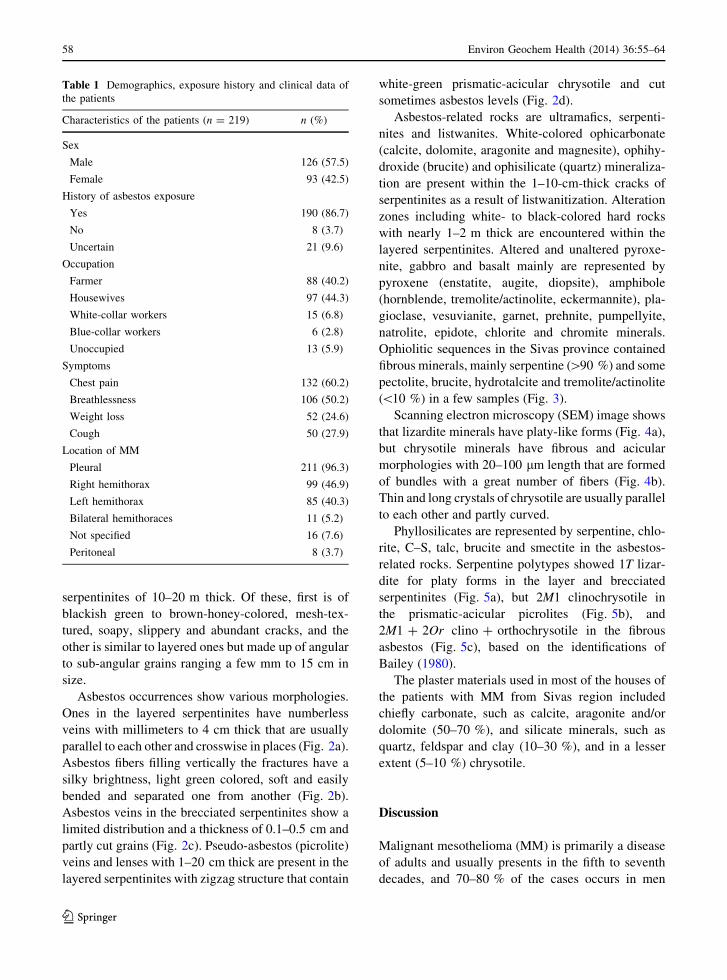
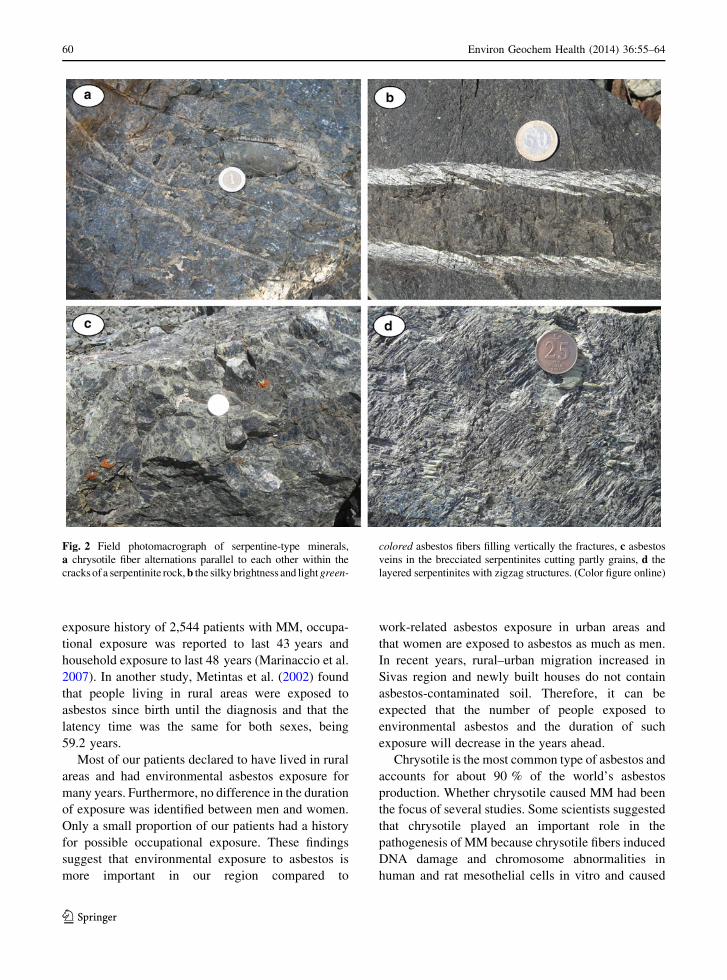
Asbestos occurrences show various morphologies.
Ones in the layered serpentinites have numberless
veins with millimeters to 4 cm thick that are usually
parallel to each other and crosswise in places (Fig. 2a).
Asbestos fibers filling vertically the fractures have a
silky brightness, light green colored, soft and easily
bended and separated one from another (Fig. 2b).
Asbestos veins in the brecciated serpentinites show a
limited distribution and a thickness of 0.1–0.5 cm and
partly cut grains (Fig. 2c). Pseudo-asbestos (picrolite)
veins and lenses with 1–20 cm thick are present in the
layered serpentinites with zigzag structure that contain
white-green prismatic-acicular chrysotile and cut
sometimes asbestos levels (Fig. 2d).
Asbestos-related rocks are ultramafics, serpenti-
nites and listwanites. White-colored ophicarbonate
(calcite, dolomite, aragonite and magnesite), ophihy-
droxide (brucite) and ophisilicate (quartz) mineraliza-
tion are present within the 1–10-cm-thick cracks of
serpentinites as a result of listwanitization. Alteration
zones including white- to black-colored hard rocks
with nearly 1–2 m thick are encountered within the
layered serpentinites. Altered and unaltered pyroxe-
nite, gabbro and basalt mainly are represented by
pyroxene (enstatite, augite, diopsite), amphibole
(hornblende, tremolite/actinolite, eckermannite), pla-
gioclase, vesuvianite, garnet, prehnite, pumpellyite,
natrolite, epidote, chlorite and chromite minerals.
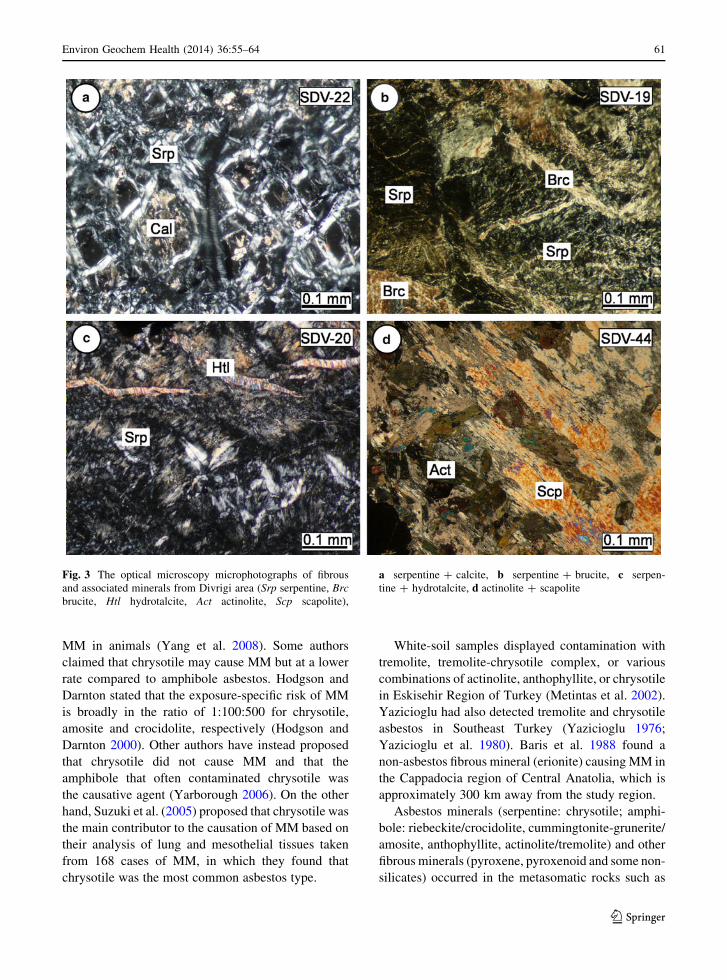
Ophiolitic sequences in the Sivas province contained
fibrous minerals, mainly serpentine ([90 %) and some
pectolite, brucite, hydrotalcite and tremolite/actinolite
(\10 %) in a few samples (Fig. 3).
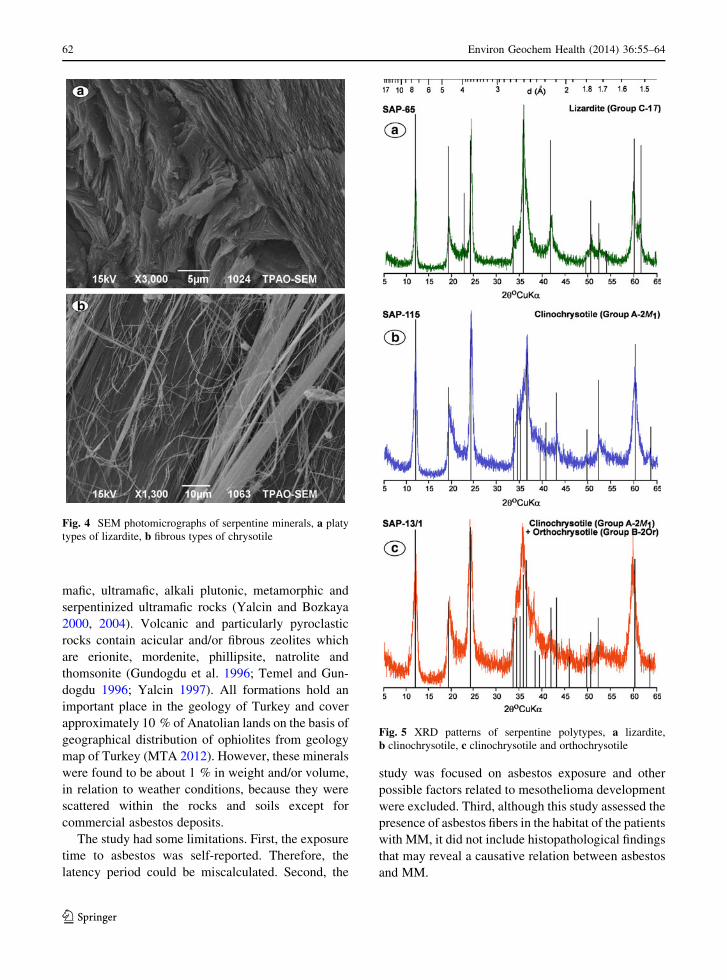
Scanning electron microscopy (SEM) image shows
that lizardite minerals have platy-like forms (Fig. 4a),
but chrysotile minerals have fibrous and acicular
morphologies with 20–100 lm length that are formed
of bundles with a great number of fibers (Fig. 4b).
Thin and long crystals of chrysotile are usually parallel
to each other and partly curved.
Phyllosilicates are represented by serpentine, chlo-
rite, C–S, talc, brucite and smectite in the asbestos-
related rocks. Serpentine polytypes showed 1T lizar-
dite for platy forms in the layer and brecciated
serpentinites (Fig. 5a), but 2M1 clinochrysotile in
the prismatic-acicular picrolites (Fig. 5b), and
2M1 ? 2Or clino ? orthochrysotile in the fibrous
asbestos (Fig. 5c), based on the identifications of
Bailey (1980).
The plaster materials used in most of the houses of
the patients with MM from Sivas region included
chiefly carbonate, such as calcite, aragonite and/or
dolomite (50–70 %), and silicate minerals, such as
quartz, feldspar and clay (10–30 %), and in a lesser
extent (5–10 %) chrysotile.
Discussion
Malignant mesothelioma (MM) is primarily a disease
of adults and usually presents in the fifth to seventh
decades, and 70–80 % of the cases occurs in men
Table 1 Demographics, exposure history and clinical data of
the patients
Characteristics of the patients (n = 219) n (%)
Sex
Male 126 (57.5)
Female 93 (42.5)
History of asbestos exposure
Yes 190 (86.7)
No 8 (3.7)
Uncertain 21 (9.6)
Occupation
Farmer 88 (40.2)
Housewives 97 (44.3)
White-collar workers 15 (6.8)
Blue-collar workers 6 (2.8)
Unoccupied 13 (5.9)
Symptoms
Chest pain 132 (60.2)
Breathlessness 106 (50.2)
Weight loss 52 (24.6)
Cough 50 (27.9)
Location of MM
Pleural 211 (96.3)
Right hemithorax 99 (46.9)
Left hemithorax 85 (40.3)
Bilateral hemithoraces 11 (5.2)
Not specified 16 (7.6)
Peritoneal 8 (3.7)
58 Environ Geochem Health (2014) 36:55–64
123
(Moore et al. 2008). Occupational asbestos exposures
were more frequent in men, whereas environmental
asbestos exposure was found to be nearly as frequent
in men and women (Senyigit et al. 2000). In a study
from Turkey, for the environmental asbestos exposure
series of Selcuk, the average age was 50 years, with
one-fourth of the patients being less than 40 years old,
and the male-to-female sex ratio of the patients was
one (Selcuk et al. 1992). Rarely, MM occurs in
patients younger than 20 years (Fraire et al. 1988).
The reasons for such cases were suggested to be
related to genetic predisposition and other unknown
factors other than asbestos exposure. In our series, the
average age at the time of diagnosis was 59 and the
male-to-female ratio was 1.4:1. The youngest patient
was diagnosed at the age of 18 and had no asbestos
exposure.
Malignant pleural mesothelioma (MPM) is more
commonly found to be unilateral (95 %) and located in
the right chest (60 %). The initial clinical presentation
for most patients with MPM is progressive dyspnea
and/or steady chest wall pain. The symptoms may be
insidious and non-specific such that the time from
initial presentation until diagnosis is often 3–6 months
(Ismail-Khan et al. 2006). Our study revealed that
unilateral hemithorax (mostly right hemithorax) was
involved in 87.2 % of the patients, in accordance with
the current literature. The most frequent symptoms of
the patients were chest pain (60 %) and shortness of
breath (50 %). The average time between the onset of
symptoms and the diagnosis was 4 months.
Earlier studies reported various numbers (about
5–30 %) for the frequency of malignant peritoneal
mesothelioma among all MM cases (Bridda et al.
2007; Marinaccio et al. 2007). This variation was
thought to result from confusing peritoneal mesothe-
lioma with abdominal neoplasms, such as peritoneal
serous carcinoma and ovarian serous carcinoma
(Marinaccio et al. 2010). In our series, less than 4 %
of the patients had peritoneal involvement. This
slightly smaller percentage could be the result of
encoding flaws in records.
Exposure to asbestos is identified in 50–90 % of the
patients with MM (Metintas et al. 1999). The latency
period between the time of initial exposure and the
diagnosis is about 30 years and ranges from 20 to
50 years (Carbone et al. 2002). A meta-analysis
involving 21 studies was published in 1992 and the
latency period was calculated as 32 years (Lanphear
and Buncher 1992). In a study evaluating the asbestos
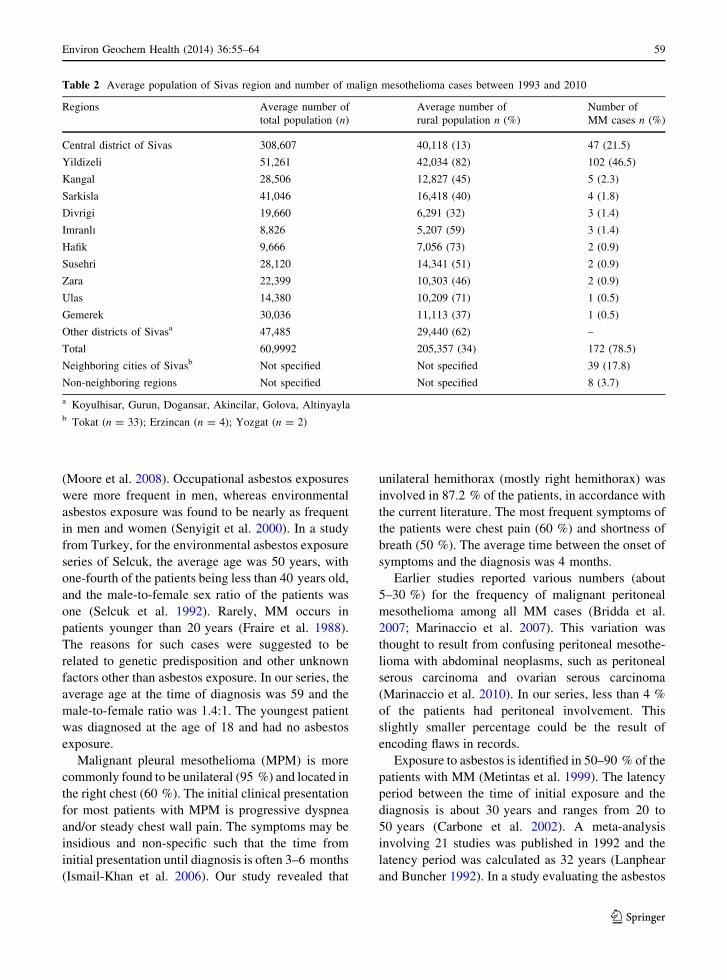
Table 2 Average population of Sivas region and number of malign mesothelioma cases between 1993 and 2010
Regions Average number of
total population (n)
Average number of
rural population n (%)
Number of
MM cases n (%)
Central district of Sivas 308,607 40,118 (13) 47 (21.5)
Yildizeli 51,261 42,034 (82) 102 (46.5)
Kangal 28,506 12,827 (45) 5 (2.3)
Sarkisla 41,046 16,418 (40) 4 (1.8)
Divrigi 19,660 6,291 (32) 3 (1.4)
Imranlı 8,826 5,207 (59) 3 (1.4)
Hafik 9,666 7,056 (73) 2 (0.9)
Susehri 28,120 14,341 (51) 2 (0.9)
Zara 22,399 10,303 (46) 2 (0.9)
Ulas 14,380 10,209 (71) 1 (0.5)
Gemerek 30,036 11,113 (37) 1 (0.5)
Other districts of Sivasa 47,485 29,440 (62) –
Total 60,9992 205,357 (34) 172 (78.5)
Neighboring cities of Sivasb Not specified Not specified 39 (17.8)
Non-neighboring regions Not specified Not specified 8 (3.7)
a Koyulhisar, Gurun, Dogansar, Akincilar, Golova, Altinyaylab Tokat (n = 33); Erzincan (n = 4); Yozgat (n = 2)
Environ Geochem Health (2014) 36:55–64 59
123
exposure history of 2,544 patients with MM, occupa-
tional exposure was reported to last 43 years and
household exposure to last 48 years (Marinaccio et al.
2007). In another study, Metintas et al. (2002) found
that people living in rural areas were exposed to
asbestos since birth until the diagnosis and that the
latency time was the same for both sexes, being
59.2 years.
Most of our patients declared to have lived in rural
areas and had environmental asbestos exposure for
many years. Furthermore, no difference in the duration
of exposure was identified between men and women.
Only a small proportion of our patients had a history
for possible occupational exposure. These findings
suggest that environmental exposure to asbestos is
more important in our region compared to
work-related asbestos exposure in urban areas and
that women are exposed to asbestos as much as men.
In recent years, rural–urban migration increased in
Sivas region and newly built houses do not contain
asbestos-contaminated soil. Therefore, it can be
expected that the number of people exposed to
environmental asbestos and the duration of such
exposure will decrease in the years ahead.
Chrysotile is the most common type of asbestos and
accounts for about 90 % of the world’s asbestos
production. Whether chrysotile caused MM had been
the focus of several studies. Some scientists suggested
that chrysotile played an important role in the
pathogenesis of MM because chrysotile fibers induced
DNA damage and chromosome abnormalities in
human and rat mesothelial cells in vitro and caused
Fig. 2 Field photomacrograph of serpentine-type minerals,
a chrysotile fiber alternations parallel to each other within the
cracks of a serpentinite rock, b the silky brightness and light green-
colored asbestos fibers filling vertically the fractures, c asbestos
veins in the brecciated serpentinites cutting partly grains, d the
layered serpentinites with zigzag structures. (Color figure online)
60 Environ Geochem Health (2014) 36:55–64
123
MM in animals (Yang et al. 2008). Some authors
claimed that chrysotile may cause MM but at a lower
rate compared to amphibole asbestos. Hodgson and
Darnton stated that the exposure-specific risk of MM
is broadly in the ratio of 1:100:500 for chrysotile,
amosite and crocidolite, respectively (Hodgson and
Darnton 2000). Other authors have instead proposed
that chrysotile did not cause MM and that the
amphibole that often contaminated chrysotile was
the causative agent (Yarborough 2006). On the other
hand, Suzuki et al. (2005) proposed that chrysotile was
the main contributor to the causation of MM based on
their analysis of lung and mesothelial tissues taken
from 168 cases of MM, in which they found that
chrysotile was the most common asbestos type.
White-soil samples displayed contamination with
tremolite, tremolite-chrysotile complex, or various
combinations of actinolite, anthophyllite, or chrysotile
in Eskisehir Region of Turkey (Metintas et al. 2002).
Yazicioglu had also detected tremolite and chrysotile
asbestos in Southeast Turkey (Yazicioglu 1976;
Yazicioglu et al. 1980). Baris et al. 1988 found a
non-asbestos fibrous mineral (erionite) causing MM in
the Cappadocia region of Central Anatolia, which is
approximately 300 km away from the study region.
Asbestos minerals (serpentine: chrysotile; amphi-
bole: riebeckite/crocidolite, cummingtonite-grunerite/
amosite, anthophyllite, actinolite/tremolite) and other
fibrous minerals (pyroxene, pyroxenoid and some non-
silicates) occurred in the metasomatic rocks such as
Fig. 3 The optical microscopy microphotographs of fibrous
and associated minerals from Divrigi area (Srp serpentine, Brc
brucite, Htl hydrotalcite, Act actinolite, Scp scapolite),
a serpentine ? calcite, b serpentine ? brucite, c serpen-
tine ? hydrotalcite, d actinolite ? scapolite
Environ Geochem Health (2014) 36:55–64 61
123
mafic, ultramafic, alkali plutonic, metamorphic and
serpentinized ultramafic rocks (Yalcin and Bozkaya
2000, 2004). Volcanic and particularly pyroclastic
rocks contain acicular and/or fibrous zeolites which
are erionite, mordenite, phillipsite, natrolite and
thomsonite (Gundogdu et al. 1996; Temel and Gun-
dogdu 1996; Yalcin 1997). All formations hold an
important place in the geology of Turkey and cover
approximately 10 % of Anatolian lands on the basis of
geographical distribution of ophiolites from geology
map of Turkey (MTA 2012). However, these minerals
were found to be about 1 % in weight and/or volume,
in relation to weather conditions, because they were
scattered within the rocks and soils except for
commercial asbestos deposits.
The study had some limitations. First, the exposure
time to asbestos was self-reported. Therefore, the
latency period could be miscalculated. Second, the
study was focused on asbestos exposure and other
possible factors related to mesothelioma development
were excluded. Third, although this study assessed the
presence of asbestos fibers in the habitat of the patients
with MM, it did not include histopathological findings
that may reveal a causative relation between asbestos
and MM.
Fig. 4 SEM photomicrographs of serpentine minerals, a platy
types of lizardite, b fibrous types of chrysotile
Fig. 5 XRD patterns of serpentine polytypes, a lizardite,
b clinochrysotile, c clinochrysotile and orthochrysotile
62 Environ Geochem Health (2014) 36:55–64
123
The mineralogical analyses obtained in this study
showed that MM disease was common in northern
regions of Sivas (especially Yildizeli district) where
serpentine-bearing ophiolite complexes were abun-
dant. On the other hand, the relationship between MM
and the distance of ophiolites could be correlated, as
evidenced by Bayram et al. (2012).
This finding questions the previous opinions
regarding the roles of different asbestos types in the
etiology of MM. However, the unique or combined
effect and/or interactions of other fibrous and non-
fibrous minerals on the development of MM are not
fully known yet and remain to be proven.
Acknowledgments The authors would like to thank the villagers
for their help in the field study, patients and their families for their
patience and department staff for their contribution.
References
Bailey, S. W. (1980). Structures of layer silicates. In G.
W. Brindley & G. Brown (Eds.), Crystal structures of clay
minerals and their X-ray identification (pp. 1–123). Lon-
don: Mineralogical Society.
Baris, Y. I. (1987). Asbestos and erionite related chest diseases.
Ankara: Semih Ofset Mat Com.
Baris, Y. I., Artvinli, M., & Sahin, A. A. (1979). Environmental
mesothelioma in Turkey. Annals of the New York Academy
of Sciences, 330, 423–432.
Baris, Y. I., Bilir, N., Artvinli, M., Sahin, A. A., Kalyoncu, A. F.,
& Sebastien, P. (1988). An epidemiological study in an
Anatolian village environmentally exposed to tremolite
asbestos. British Journal of Industrial Medicine, 45,
838–840.
Bayram, M., Dongel, I., Bakan, N. D., Yalcin, H., Cevit, R.,
Dumortier, P., et al. (2012). High risk of malignant meso-
thelioma and pleural plaques in subjects born close to
ophiolites. Chest, 143, 164–171.
Bridda, A., Padoan, I., Mencarelli, R., & Frego, M. (2007).
Peritoneal mesothelioma: A review. Medscape General
Medicine, 9(2), 32.
Carbone, M., Kratzke, R. A., & Testa, J. R. (2002). The path-
ogenesis of mesothelioma. Seminars in Oncology, 29,
2–17.
Fraire, A. E., Cooper, S., Greenberg, S. D., Buffler, P., &
Langston, C. (1988). Mesothelioma of childhood. Cancer,
62, 838–847.
Gundogdu, M. N., Yalcin, H., Temel, A., & Clauer, N. (1996).
Geological, mineralogical and geochemical characteristics
of zeolite deposits associated with borates in the Bigadic,
Emet and Kirka Neogene lacustrine basins, Western Tur-
key. Mineralium Deposita, 31, 492–513.
Hodgson, J. T., & Darnton, A. (2000). The quantitative risks of
mesothelioma and lung cancer in relation to asbestos
exposure. Annals of Occupational Hygiene, 44, 565–601.
Ismail-Khan, R., Robinson, L. A., Williams, C. C., Jr., Garrett,
C. R., Bepler, G., & Simon, G. R. (2006). Malignant pleural
mesothelioma: A comprehensive review. Cancer Control,
13, 255–263.
Lanphear, B. P., & Buncher, C. R. (1992). Latent period for
malignant mesothelioma of occupational origin. Journal of
Occupational Medicine, 34, 718–721.
Marinaccio, A., Binazzi, A., Cauzillo, G., Cavone, D., De Zotti,
R., Ferrante, P., et al. (2007). Analysis of latency time and
its determinants in asbestos-related malignant mesotheli-
oma cases of the Italian register. European Journal of
Cancer, 43, 2722–2728.
Marinaccio, A., Binazzi, A., Di Marzio, D., Scarselli, A., Ver-
ardo, M., Mirabelli, D., et al. (2010). Incidence of extra-
pleural malignant mesothelioma and asbestos exposure,
from the Italian national register. Occupational and Envi-
ronmental Medicine, 67(11), 760–765.
Metintas, M., Ozdemir, N., Hillerdal, G., Ucgun, I., Metintas, S.,
Baykul, C., et al. (1999). Environmental asbestos exposure
and malignant pleural mesothelioma. Respiratory Medi-
cine, 93, 349–355.
Metintas, S., Metintas, M., Ucgun, U., & Oner, U. (2002).
Malignant mesothelioma due to environmental exposure to
asbestos: follow-up of a Turkish cohort living in a rural
area. Chest, 122, 2224–2229.
Moore, A. J., Parker, R. J., & Wiggins, J. (2008). Malignant
Mesothelioma. Orphanet Journal of Rare Diseases, 3, 34.
MTA (2012) http://www.mta.gov.tr/v2.0/daire-baskanliklari/
jed/images/urunler/yeni500/buyuk/SIVAS.pdf. Accessed
07 August, 2012.
Selcuk, Z. T., Coplu, L., Emri, S., Kalyoncu, A. F., Sahin, A. A.,
& Baris, Y. I. (1992). Malignant pleural mesothelioma due
to environmental mineral fiber exposure in Turkey: Anal-
ysis of 135 cases. Chest, 102, 790–796.
Senyigit, A., Coskunsel, M., Topcu, F., Isik, R., & Babayigit, C.
(2000). Malignant pleural mesothelioma: Evaluation of
clinical, radiological and histological features in 136 cases.
Tuberk Toraks, 48, 26–34.
Sterman, D. H., Litzky, L. A., & Albelda, S. M. (2008).
Malignant mesothelioma and other primary pleural tumors.
In A. P. Fishman & J. A. Elias (Eds.), Fishman’s pul-
monary diseases and disorders (4th ed., pp. 1535–1552).
Philadelphia: McGraw-Hill.
Suzuki, Y., Yuen, S. R., & Ashley, R. (2005). Short, thin
asbestos fibers contribute to the development of human
malignant mesothelioma: pathological evidence. Interna-
tional Journal of Hygiene and Environmental Health, 208,
201–210.
Temel, A., & Gundogdu, M. N. (1996). Zeolite occurrences and the
erionite-mesothelioma relationship in Cappadocia, central
Anatolia, Turkey. Mineralium Deposita, 31, 539–547.
Wagner, T. C., Sleggs, C. A., & Marckand, P. (1960). Diffuse
pleural mesothelioma and asbestos exposure in north
western Cape Province. British Journal of Industrial
Medicine, 17, 160–171.
Walker, A. M., Loughlin, J. E., Friedlander, E. R., Rothman, K.
J., & Dreyer, N. A. (1983). Projections of asbestos-related
disease 1980–2009. Journal of Occupational Medicine, 25,
409–425.
Weiner, S. J., & Miandoab, N. S. (2009). Pathogenesis of
malignant pleural mesothelioma and the role of
Environ Geochem Health (2014) 36:55–64 63
123

environmental and genetic factors. Journal of Cancer
Research and Clinical Oncology, 135, 15–27.
Yalcin, H. (1997). Central North Anatolian zeolite occurrences
related to Eocene submarine volcanism in Turkey. Bulletin
of Faculty of Engineering Cumhuriyet University Series
A-Earth Sciences, 14, 43–56. (article in Turkish).
Yalcin, H., & Bozkaya, O. (2000). Mineralogy and geochem-
istry of ultramafic- and sedimentary-hosted talc deposits of
Paleocene in the southern part of the Sivas basin, Turkey.
Clays and Clay Minerals, 54, 333–350.
Yalcin, H., & Bozkaya, O. (2004). Ultramafic-rock-hosted vein
sepiolite occurrences in the Ankara ophiolitic melange,
Central Anatolia, Turkey. Clays and Clay Minerals, 52,
227–239.
Yang, H., Testa, J. R., & Carbone, M. (2008). Mesothelioma
epidemiology, carcinogenesis and pathogenesis. Current
Treatment Options in Oncology, 9, 147–157.
Yarborough, C. M. (2006). Chrysotile as a cause of mesotheli-
oma: An assessment based on epidemiology. Critical
Reviews in Toxicology, 36, 165–187.
Yazicioglu, S. (1976). Pleural calcification associated with
exposure to chrysotile asbestos in southeast Turkey. Chest,
70, 43–47.
Yazicioglu, S., Ilcayto, R., Balci, K., Sayli, B. S., & Yorulmaz,
B. (1980). Pleural calcification, pleural mesotheliomas and
bronchial cancers caused by tremolite dust. Thorax, 35,
564–569.
64 Environ Geochem Health (2014) 36:55–64
123