Embed Size (px)
Citation preview

The association of psoriasis with autoimmune diseases
Jashin J. Wu, MD,a Thao U. Nguyen, MD,a Kwun-Yee T. Poon, MS,b and Lisa J. Herrinton, PhDc
Los Angeles, Pasadena, and Oakland, California
See related letters on pages 1076 and 1079.
From
C
Ka
of
Supp
C
an
co
da
Discl
ra
th
924
Background: Previous studies provide evidence that there is a greater frequency of autoimmune diseasesamong patients with psoriasis than in the general population.
Objective: This study examined the association between psoriasis and 21 common autoimmune diseases,specified a priori.
Methods: A retrospective cohort study was conducted among persons who were members of KaiserPermanente Southern California from 2004 to 2011. A total of 25,341 patients with 2 or more diagnosiscodes for any psoriatic disease were evaluated. Five persons not meeting this case definition were matchedto each psoriatic patient based on age, sex, and length of enrollment.
Results: Patients with psoriasis were more likely to have at least 1 other autoimmune disease (odds ratio[OR] 1.6; 95% confidence interval [CI] 1.5-1.7) and to have at least 2 other autoimmune diseases (1.9; 95% CI1.6-2.4). Of the 17 conditions evaluated, associations with 14 were found to be statistically significant. Thestrongest association was with rheumatoid arthritis (3.6; 95% CI 3.4-3.9).
Limitations: Patients with autoimmune conditions are likely to have a greater number of health careencounters, which may result in overascertainment and misascertainment of immune-mediated conditions,although the patients included in the study averaged 5.2 years of observation and the comparison subjectswere matched on length of enrollment.
Conclusions: The study suggests a genetic or environmental cause common across autoimmune diseases.Further investigation of individuals with multiple autoimmune diseases may yield important clues about theorigin and pathogenesis of the disease. ( J Am Acad Dermatol 2012;67:924-30.)
Key words: Addison disease; alopecia areata; autoimmune diseases; celiac disease; chronic glomerulo-nephritis; chronic urticaria; cohort studies; Crohn’s disease; database; giant cell arteritis; Graves disease;Hashimoto disease; hemolytic anemia; immune thrombocytopenia; multiple sclerosis; prevalence; primarybiliary cirrhosis; psoriasis; psoriatic arthritis; pulmonary fibrosis; rheumatoid arthritis; Sj€ogren syndrome;systemic lupus erythematosus; systemic sclerosis; type 1 diabetes mellitus; vitiligo; ulcerative colitis.
soriasis is one of the most prevalent systemic frequency of autoimmune diseases among patients
P inflammatory diseases, affecting approxi-mately 2% to 3% of the population and more
than 125 million patients worldwide.1-3 Previousstudies provide evidence that there is a greater
the Department of Dermatology, Kaiser Permanente Medical
enter, Los Angelesa; Department of Research and Evaluation,
iser Permanente Southern California, Pasadenab; and Division
Research, Kaiser Permanente Northern California, Oakland.c
orted in whole by Kaiser Permanente’s Regional Research
ommittee. The Regional Research Committee had no role in
y of the following: design and conduct of the study;
llection, management, analysis, and interpretation of the
ta; and preparation, review, or approval of the manuscript.
osure: Dr Wu received research funding from Abbott Labo-
tories, Amgen, and Pfizer, which were not directly related to
is study. Dr Herrinton has recent research contracts with
with psoriasis than in the general population, andmany inflammatory autoimmune diseases are a resultof derangements in multiple cytokine pathways.4-8
Chromosome 16 has been implicated to confer
Procter & Gamble, Janssen, and Genentech. Dr Nguyen and
Ms Poon have no conflicts of interest to declare.
Accepted for publication April 14, 2012.
Reprint requests: Jashin J. Wu, MD, Department of Dermatology,
Kaiser Permanente Los Angeles Medical Center, 1515 N
Vermont Ave, 5th Floor, Los Angeles, CA 90027. E-mail:
Published online June 4, 2012.
0190-9622/$36.00
� 2012 by the American Academy of Dermatology, Inc.
doi:10.1016/j.jaad.2012.04.039

J AM ACAD DERMATOL
VOLUME 67, NUMBER 5Wu et al 925
susceptibility for psoriasis, Crohn’s disease, andulcerative colitis.9 In addition, in a genomewidescan, a locus on chromosome 4 has linked psoriaticarthritis and possibly psoriasis to a host of autoim-mune diseases, including type 1 diabetes mellitus,celiac disease, and Graves disease.10 These studiesgive evidence for a genetic role in the pathogenesis
CAPSULE SUMMARY
d Psoriasis was positively associated with17 of the 21 studied autoimmunediseases, with 14 of these associationsbeing statistically significant.
d Patients with psoriatic arthritis have ahigher odds ratio for development of anautoimmune disease (except alopeciaareata, primary biliary cirrhosis, chronicurticaria, and vitiligo) when compared topatients with psoriasis only.
d The study gives evidence for a commongenetic or environmental cause amongthese autoimmune diseases.
of psoriasis.9-12
Psoriatic arthritis occursin 7% to 26% of all patientswith psoriasis.13 Althoughthere is considerable varia-tion in the association ofskin and arthritic symptoms,the genetic, epidemiologic,and therapeutic data pointto some shared patho-genic mechanisms in thesediseases.14
The study aimed to deter-mine whether patients withpsoriasis with or withoutpsoriatic arthritis were at in-creased risk for autoimmunediseases that share a com-mon autoimmune pathoge-netic mechanism. We
hypothesize that those with psoriasis are more likelyto have an autoimmune disease, while those withboth psoriasis and psoriatic arthritis are more likelyto have an autoimmune disease compared to thosewith psoriasis only.METHODSStudy population
This was a retrospective cohort study in individ-uals who were members of the Kaiser PermanenteSouthern California (KPSC) health plan from January1, 2004, to February 28, 2011. The study inception onJanuary 1, 2004, is used because KPSC started its useof electronic medical records on this date.
Persons aged 0 to 100 years on January 1, 2004,and with at least 1 year of enrollment during theperiod January 1, 2004, through February 28, 2011,were eligible for the study. Eligible patients wereidentified as those with 2 or more inpatient oroutpatient diagnoses codes for psoriatic disease(International Classification of Diseases, NinthRevision [ICD-9] code 696.0-1), 2 codes for psoriasisonly (ICD-9 code 696.1), 2 codes for psoriaticarthritis (ICD-9 code 696.0), or codes for both pso-riasis and psoriatic arthritis (1 code each of 696.1 and696.0). To form the comparison group, we randomlyselected persons without psoriatic disease from theremaining population of KPSC members at a ratio of
5 to 1. Persons without psoriatic disease werematched to patients with psoriasis or psoriatic arthri-tis on gender, year of birth (61 year), and length ofenrollment (61 year) from the first date. Personswith a single code of a psoriatic disease were noteligible as control subjects.
Data collectionThe information needed
for this study included demo-graphic characteristics andinpatient and outpatientvisits. These were obtainedfrom the clinical and admin-istrative databases of KPSC.The outcomes of interestwere the following diagno-ses: Crohn’s disease, ulcera-tive colitis, type 1 diabetesmellitus, alopecia areata,hemolytic anemia, giant cellarteritis, multiple sclerosis,systemic lupus erythemato-sus, vitiligo, Graves disease,Hashimoto disease, chronicglomerulonephritis, pulmo-
nary fibrosis, Sj€ogren syndrome, Addison disease,immune thrombocytopenia, chronic urticaria, celiacdisease, primary biliary cirrhosis, rheumatoid arthri-tis, and systemic sclerosis. Each specific disease wastreated as an outcome variable except for juvenilerheumatoid arthritis, which was combined withrheumatoid arthritis because there were few studysubjects with juvenile disease.
All diagnoses for these conditions recorded fromJanuary 1, 2004, to February 28, 2011, were ascer-tained. We included only those diagnoses that wererecorded after the second recorded diagnosis forpsoriatic disease. Two or more inpatient or outpa-tient diagnoses were required for each of the auto-immune disease outcomes. The ICD-9 codes foreach disease are listed in Table I.
Statistical analysisPersons with psoriatic disease and members of the
general population without psoriatic disease weredescribed and compared in terms of demographicscharacteristics and health care use. To assessthe potential for overascertainment of immune-mediated conditions among those with psoriasis, theaverage number of health care contacts for those whohad ever received a single diagnosis code for animmune-mediated condition was calculated. The as-sociation between each autoimmune disease and thecovariates was assessed using x2 test. Conditional

Abbreviations used:
CI: confidence intervalIBD: inflammatory bowel diseasesICD-9: International Classification of Diseases
Ninth RevisionIL: interleukinKPSC: Kaiser Permanente Southern CaliforniaOR: odds ratio
J AM ACAD DERMATOL
NOVEMBER 2012926 Wu et al
logistic regression was performed to compare the riskof autoimmune disease between persons with psori-aticdisease andmatched control subjects. All statisticalanalyses were performed using software (SASEnterpriseGuide, Version 4.3, SAS Institute, Cary, NC).
RESULTSThere were 25,341 eligible members who had 21
diagnosis codes for any psoriatic disease during thestudy period (Table II). Among these, 10.6% had atleast 1 code for psoriatic arthritis. The mean age in2004 was 49 years. Of those with psoriasis only orpsoriatic arthritis, 51.6% and 51.4% were men,respectively.
The univariate analysis is shown in Table III.Patients with psoriatic arthritis had an elevated oddsratio (OR) for all of the 21 autoimmune diseasesexamined in this study. Most notable associationswere with rheumatoid arthritis, systemic lupus eryth-ematosus, Sj€ogren syndrome, systemic sclerosis, ce-liac disease, giant cell arteritis, and hemolyticanemia. Patients with psoriasis were 2 times morelikely to develop alopecia areata, celiac disease, andsystemic sclerosis. When compared with psoriasis,psoriatic arthritis had an elevated OR for develop-ment of an autoimmune disease as well, with theexception of alopecia areata, primary biliary cirrho-sis, chronic urticaria, and vitiligo.
Table IV shows OR for the association of psoriasisand psoriatic arthritis with autoimmune diseasesbased on gender and ethnicity. Female patientstended to have higher OR for having autoimmunediseases compared with male patients. White pa-tients (defined as non-Hispanic white) tended tohave similar OR for having autoimmune diseasescompared with nonwhite patients.
When combining patients with psoriasis andthose with psoriatic arthritis, we observed a signifi-cantly increased OR with most autoimmune diseases(Table V). Moreover, having at least 1, 2, or 3autoimmune diseases showed a higher OR of 1.5(95% confidence interval [CI] 1.4-1.5), 1.6 (95% CI1.5-1.7), and 1.9 (95% CI 1.6-2.4), respectively.
DISCUSSIONThis retrospective cohort study using the KPSC
medical health records examined 25,341 patientswith psoriatic disease and 126,705 matched controlsubjects to evaluate the relationship with autoim-mune diseases. The findings suggest that patientswith psoriatic disease are more likely than controlsubjects to be given the diagnosis of an autoimmunedisease. Present at significantly higher frequencieswere rheumatoid arthritis, alopecia areata, celiacdisease, systemic sclerosis, Crohn’s disease, Sj€ogrensyndrome, vitiligo, ulcerative colitis, chronic urti-caria, systemic lupus erythematosus, giant cell arte-ritis, Addison disease, pulmonary fibrosis, andchronic glomerulonephritis. Persons with psoriaticdisease were more likely than persons withoutpsoriatic disease to be recorded with at least 2 (1.6[95% CI 1.5-1.7]) or 3 (1.9 [95% CI 1.6-2.4]) immune-mediated diseases. This finding is consistent withprevious studies.4-7
The autoimmune disease with the highest ORwith psoriatic disease was rheumatoid arthritis. It ispossible that there may be some patients given themisdiagnosis of rheumatoid arthritis who insteadhave psoriatic arthritis. However, this issue may notoccur frequently as rheumatologists are usually thephysicians to place the initial ICD-9 code for anyinflammatory arthritic condition. KPSC rheumatolo-gists typically follow the 2010 American Collegeof Rheumatology/European League AgainstRheumatism Rheumatoid Arthritis ClassificationCriteria, which include joint involvement, serologicparameters such as positive rheumatoid factor,acute phase reactants, and duration of arthritis.KPSC rheumatologists also follow the ClassificationCriteria for Psoriatic Arthritis (CASPAR) criteria forpsoriatic arthritis, which includes evidence of cur-rent psoriasis, a personal history of psoriasis, or afamily history of psoriasis; typical psoriatic naildystrophy; a negative test result for the presenceof rheumatoid factor by any method except latex;current dactylitis or a history of dactylitis recordedby a rheumatologist; and radiographic evidence ofjuxta-articular new bone formation appearing as ill-defined ossification near joint margins (but exclud-ing osteophyte formation) on plain radiographs ofthe hand or foot.
There are several important limitations in thisstudy. Diagnostic information was obtained fromcomputerized clinical databases and the diagnosiscodes. From ongoing work, we have estimated thepositive predictive value of 2 or more psoriasis codesto be 0.59 (0.43-0.73). The inclusion of patientswithout psoriatic disease in the study population
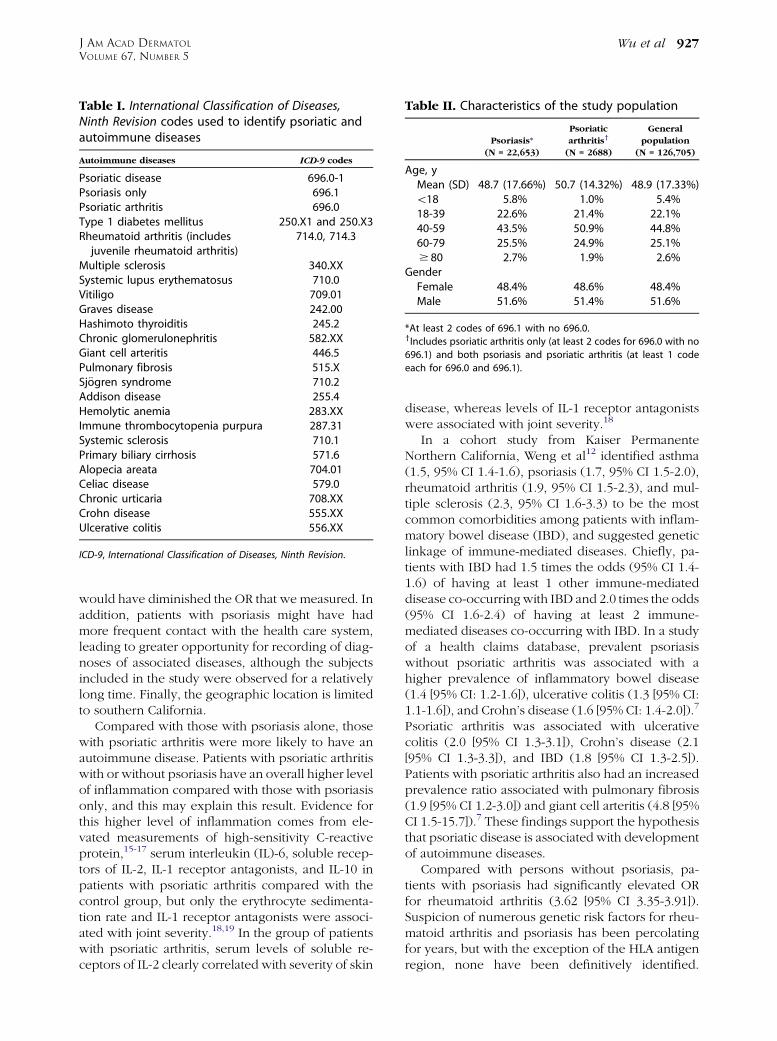
Table II. Characteristics of the study population
Psoriasis*
(N = 22,653)
Psoriatic
arthritisy
(N = 2688)
General
population
(N = 126,705)
Age, yMean (SD) 48.7 (17.66%) 50.7 (14.32%) 48.9 (17.33%)\18 5.8% 1.0% 5.4%18-39 22.6% 21.4% 22.1%40-59 43.5% 50.9% 44.8%60-79 25.5% 24.9% 25.1%$ 80 2.7% 1.9% 2.6%
GenderFemale 48.4% 48.6% 48.4%Male 51.6% 51.4% 51.6%
*At least 2 codes of 696.1 with no 696.0.yIncludes psoriatic arthritis only (at least 2 codes for 696.0 with no
696.1) and both psoriasis and psoriatic arthritis (at least 1 code
each for 696.0 and 696.1).
Table I. International Classification of Diseases,Ninth Revision codes used to identify psoriatic andautoimmune diseases
Autoimmune diseases ICD-9 codes
Psoriatic disease 696.0-1Psoriasis only 696.1Psoriatic arthritis 696.0Type 1 diabetes mellitus 250.X1 and 250.X3Rheumatoid arthritis (includesjuvenile rheumatoid arthritis)
714.0, 714.3
Multiple sclerosis 340.XXSystemic lupus erythematosus 710.0Vitiligo 709.01Graves disease 242.00Hashimoto thyroiditis 245.2Chronic glomerulonephritis 582.XXGiant cell arteritis 446.5Pulmonary fibrosis 515.XSj€ogren syndrome 710.2Addison disease 255.4Hemolytic anemia 283.XXImmune thrombocytopenia purpura 287.31Systemic sclerosis 710.1Primary biliary cirrhosis 571.6Alopecia areata 704.01Celiac disease 579.0Chronic urticaria 708.XXCrohn disease 555.XXUlcerative colitis 556.XX
ICD-9, International Classification of Diseases, Ninth Revision.
J AM ACAD DERMATOL
VOLUME 67, NUMBER 5Wu et al 927
would have diminished the OR that we measured. Inaddition, patients with psoriasis might have hadmore frequent contact with the health care system,leading to greater opportunity for recording of diag-noses of associated diseases, although the subjectsincluded in the study were observed for a relativelylong time. Finally, the geographic location is limitedto southern California.
Compared with those with psoriasis alone, thosewith psoriatic arthritis were more likely to have anautoimmune disease. Patients with psoriatic arthritiswith or without psoriasis have an overall higher levelof inflammation compared with those with psoriasisonly, and this may explain this result. Evidence forthis higher level of inflammation comes from ele-vated measurements of high-sensitivity C-reactiveprotein,15-17 serum interleukin (IL)-6, soluble recep-tors of IL-2, IL-1 receptor antagonists, and IL-10 inpatients with psoriatic arthritis compared with thecontrol group, but only the erythrocyte sedimenta-tion rate and IL-1 receptor antagonists were associ-ated with joint severity.18,19 In the group of patientswith psoriatic arthritis, serum levels of soluble re-ceptors of IL-2 clearly correlated with severity of skin
disease, whereas levels of IL-1 receptor antagonistswere associated with joint severity.18
In a cohort study from Kaiser PermanenteNorthern California, Weng et al12 identified asthma(1.5, 95% CI 1.4-1.6), psoriasis (1.7, 95% CI 1.5-2.0),rheumatoid arthritis (1.9, 95% CI 1.5-2.3), and mul-tiple sclerosis (2.3, 95% CI 1.6-3.3) to be the mostcommon comorbidities among patients with inflam-matory bowel disease (IBD), and suggested geneticlinkage of immune-mediated diseases. Chiefly, pa-tients with IBD had 1.5 times the odds (95% CI 1.4-1.6) of having at least 1 other immune-mediateddisease co-occurring with IBD and 2.0 times the odds(95% CI 1.6-2.4) of having at least 2 immune-mediated diseases co-occurring with IBD. In a studyof a health claims database, prevalent psoriasiswithout psoriatic arthritis was associated with ahigher prevalence of inflammatory bowel disease(1.4 [95% CI: 1.2-1.6]), ulcerative colitis (1.3 [95% CI:1.1-1.6]), and Crohn’s disease (1.6 [95% CI: 1.4-2.0]).7
Psoriatic arthritis was associated with ulcerativecolitis (2.0 [95% CI 1.3-3.1]), Crohn’s disease (2.1[95% CI 1.3-3.3]), and IBD (1.8 [95% CI 1.3-2.5]).Patients with psoriatic arthritis also had an increasedprevalence ratio associated with pulmonary fibrosis(1.9 [95% CI 1.2-3.0]) and giant cell arteritis (4.8 [95%CI 1.5-15.7]).7 These findings support the hypothesisthat psoriatic disease is associated with developmentof autoimmune diseases.
Compared with persons without psoriasis, pa-tients with psoriasis had significantly elevated ORfor rheumatoid arthritis (3.62 [95% CI 3.35-3.91]).Suspicion of numerous genetic risk factors for rheu-matoid arthritis and psoriasis has been percolatingfor years, but with the exception of the HLA antigenregion, none have been definitively identified.
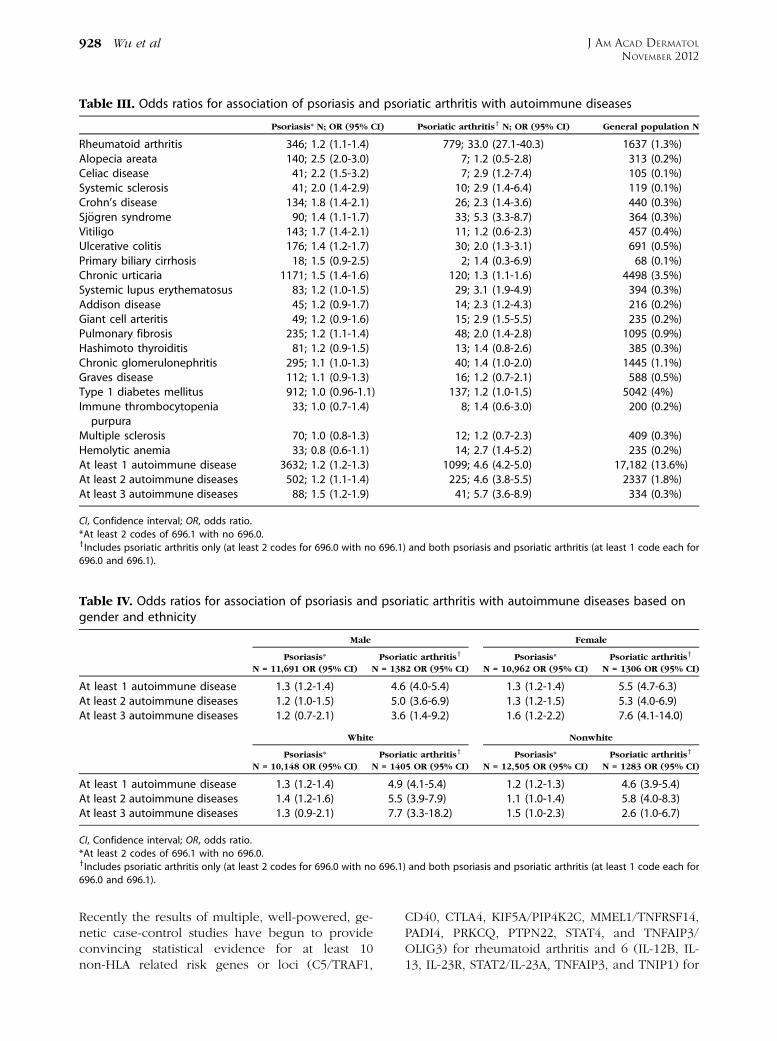
Table IV. Odds ratios for association of psoriasis and psoriatic arthritis with autoimmune diseases based ongender and ethnicity
Male Female
Psoriasis*
N = 11,691 OR (95% CI)
Psoriatic arthritisy
N = 1382 OR (95% CI)
Psoriasis*
N = 10,962 OR (95% CI)
Psoriatic arthritisy
N = 1306 OR (95% CI)
At least 1 autoimmune disease 1.3 (1.2-1.4) 4.6 (4.0-5.4) 1.3 (1.2-1.4) 5.5 (4.7-6.3)At least 2 autoimmune diseases 1.2 (1.0-1.5) 5.0 (3.6-6.9) 1.3 (1.2-1.5) 5.3 (4.0-6.9)At least 3 autoimmune diseases 1.2 (0.7-2.1) 3.6 (1.4-9.2) 1.6 (1.2-2.2) 7.6 (4.1-14.0)
White Nonwhite
Psoriasis*
N = 10,148 OR (95% CI)
Psoriatic arthritisy
N = 1405 OR (95% CI)
Psoriasis*
N = 12,505 OR (95% CI)
Psoriatic arthritisy
N = 1283 OR (95% CI)
At least 1 autoimmune disease 1.3 (1.2-1.4) 4.9 (4.1-5.4) 1.2 (1.2-1.3) 4.6 (3.9-5.4)At least 2 autoimmune diseases 1.4 (1.2-1.6) 5.5 (3.9-7.9) 1.1 (1.0-1.4) 5.8 (4.0-8.3)At least 3 autoimmune diseases 1.3 (0.9-2.1) 7.7 (3.3-18.2) 1.5 (1.0-2.3) 2.6 (1.0-6.7)
CI, Confidence interval; OR, odds ratio.
*At least 2 codes of 696.1 with no 696.0.yIncludes psoriatic arthritis only (at least 2 codes for 696.0 with no 696.1) and both psoriasis and psoriatic arthritis (at least 1 code each for
696.0 and 696.1).
Table III. Odds ratios for association of psoriasis and psoriatic arthritis with autoimmune diseases
Psoriasis* N; OR (95% CI) Psoriatic arthritisy N; OR (95% CI) General population N
Rheumatoid arthritis 346; 1.2 (1.1-1.4) 779; 33.0 (27.1-40.3) 1637 (1.3%)Alopecia areata 140; 2.5 (2.0-3.0) 7; 1.2 (0.5-2.8) 313 (0.2%)Celiac disease 41; 2.2 (1.5-3.2) 7; 2.9 (1.2-7.4) 105 (0.1%)Systemic sclerosis 41; 2.0 (1.4-2.9) 10; 2.9 (1.4-6.4) 119 (0.1%)Crohn’s disease 134; 1.8 (1.4-2.1) 26; 2.3 (1.4-3.6) 440 (0.3%)Sj€ogren syndrome 90; 1.4 (1.1-1.7) 33; 5.3 (3.3-8.7) 364 (0.3%)Vitiligo 143; 1.7 (1.4-2.1) 11; 1.2 (0.6-2.3) 457 (0.4%)Ulcerative colitis 176; 1.4 (1.2-1.7) 30; 2.0 (1.3-3.1) 691 (0.5%)Primary biliary cirrhosis 18; 1.5 (0.9-2.5) 2; 1.4 (0.3-6.9) 68 (0.1%)Chronic urticaria 1171; 1.5 (1.4-1.6) 120; 1.3 (1.1-1.6) 4498 (3.5%)Systemic lupus erythematosus 83; 1.2 (1.0-1.5) 29; 3.1 (1.9-4.9) 394 (0.3%)Addison disease 45; 1.2 (0.9-1.7) 14; 2.3 (1.2-4.3) 216 (0.2%)Giant cell arteritis 49; 1.2 (0.9-1.6) 15; 2.9 (1.5-5.5) 235 (0.2%)Pulmonary fibrosis 235; 1.2 (1.1-1.4) 48; 2.0 (1.4-2.8) 1095 (0.9%)Hashimoto thyroiditis 81; 1.2 (0.9-1.5) 13; 1.4 (0.8-2.6) 385 (0.3%)Chronic glomerulonephritis 295; 1.1 (1.0-1.3) 40; 1.4 (1.0-2.0) 1445 (1.1%)Graves disease 112; 1.1 (0.9-1.3) 16; 1.2 (0.7-2.1) 588 (0.5%)Type 1 diabetes mellitus 912; 1.0 (0.96-1.1) 137; 1.2 (1.0-1.5) 5042 (4%)Immune thrombocytopeniapurpura
33; 1.0 (0.7-1.4) 8; 1.4 (0.6-3.0) 200 (0.2%)
Multiple sclerosis 70; 1.0 (0.8-1.3) 12; 1.2 (0.7-2.3) 409 (0.3%)Hemolytic anemia 33; 0.8 (0.6-1.1) 14; 2.7 (1.4-5.2) 235 (0.2%)At least 1 autoimmune disease 3632; 1.2 (1.2-1.3) 1099; 4.6 (4.2-5.0) 17,182 (13.6%)At least 2 autoimmune diseases 502; 1.2 (1.1-1.4) 225; 4.6 (3.8-5.5) 2337 (1.8%)At least 3 autoimmune diseases 88; 1.5 (1.2-1.9) 41; 5.7 (3.6-8.9) 334 (0.3%)
CI, Confidence interval; OR, odds ratio.
*At least 2 codes of 696.1 with no 696.0.yIncludes psoriatic arthritis only (at least 2 codes for 696.0 with no 696.1) and both psoriasis and psoriatic arthritis (at least 1 code each for
696.0 and 696.1).
J AM ACAD DERMATOL
NOVEMBER 2012928 Wu et al
Recently the results of multiple, well-powered, ge-netic case-control studies have begun to provideconvincing statistical evidence for at least 10non-HLA related risk genes or loci (C5/TRAF1,
CD40, CTLA4, KIF5A/PIP4K2C, MMEL1/TNFRSF14,PADI4, PRKCQ, PTPN22, STAT4, and TNFAIP3/OLIG3) for rheumatoid arthritis and 6 (IL-12B, IL-13, IL-23R, STAT2/IL-23A, TNFAIP3, and TNIP1) for
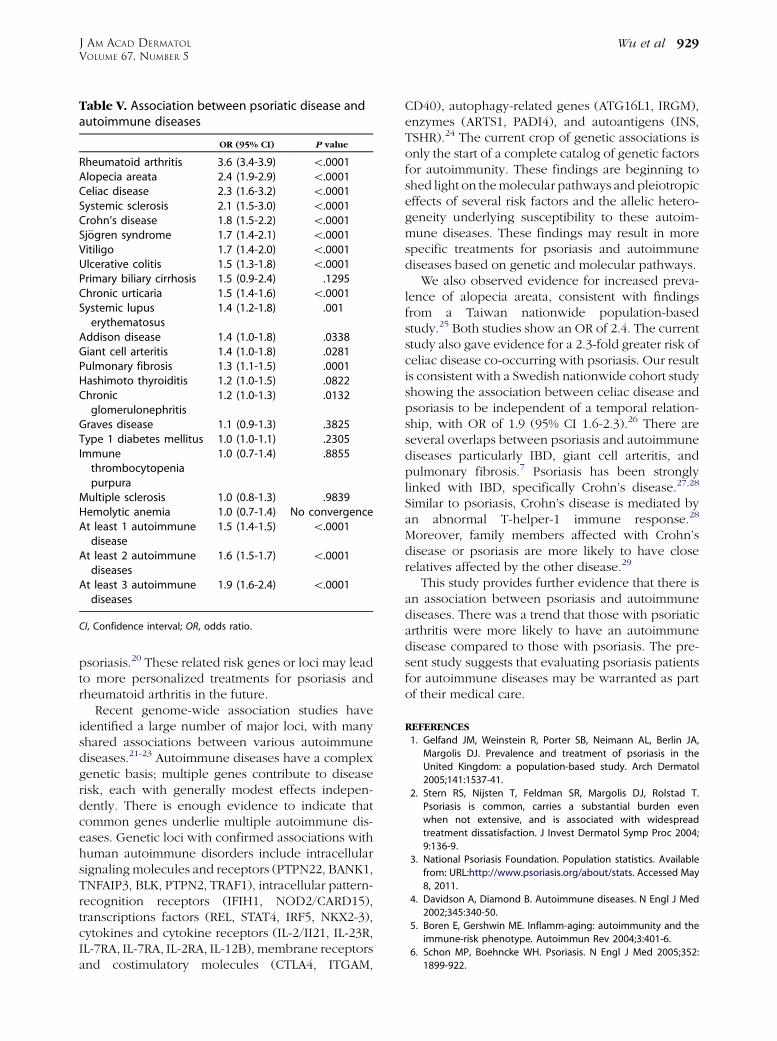
Table V. Association between psoriatic disease andautoimmune diseases
OR (95% CI) P value
Rheumatoid arthritis 3.6 (3.4-3.9) \.0001Alopecia areata 2.4 (1.9-2.9) \.0001Celiac disease 2.3 (1.6-3.2) \.0001Systemic sclerosis 2.1 (1.5-3.0) \.0001Crohn’s disease 1.8 (1.5-2.2) \.0001Sj€ogren syndrome 1.7 (1.4-2.1) \.0001Vitiligo 1.7 (1.4-2.0) \.0001Ulcerative colitis 1.5 (1.3-1.8) \.0001Primary biliary cirrhosis 1.5 (0.9-2.4) .1295Chronic urticaria 1.5 (1.4-1.6) \.0001Systemic lupuserythematosus
1.4 (1.2-1.8) .001
Addison disease 1.4 (1.0-1.8) .0338Giant cell arteritis 1.4 (1.0-1.8) .0281Pulmonary fibrosis 1.3 (1.1-1.5) .0001Hashimoto thyroiditis 1.2 (1.0-1.5) .0822Chronicglomerulonephritis
1.2 (1.0-1.3) .0132
Graves disease 1.1 (0.9-1.3) .3825Type 1 diabetes mellitus 1.0 (1.0-1.1) .2305Immunethrombocytopeniapurpura
1.0 (0.7-1.4) .8855
Multiple sclerosis 1.0 (0.8-1.3) .9839Hemolytic anemia 1.0 (0.7-1.4) No convergenceAt least 1 autoimmunedisease
1.5 (1.4-1.5) \.0001
At least 2 autoimmunediseases
1.6 (1.5-1.7) \.0001
At least 3 autoimmunediseases
1.9 (1.6-2.4) \.0001
CI, Confidence interval; OR, odds ratio.
J AM ACAD DERMATOL
VOLUME 67, NUMBER 5Wu et al 929
psoriasis.20 These related risk genes or loci may leadto more personalized treatments for psoriasis andrheumatoid arthritis in the future.
Recent genome-wide association studies haveidentified a large number of major loci, with manyshared associations between various autoimmunediseases.21-23 Autoimmune diseases have a complexgenetic basis; multiple genes contribute to diseaserisk, each with generally modest effects indepen-dently. There is enough evidence to indicate thatcommon genes underlie multiple autoimmune dis-eases. Genetic loci with confirmed associations withhuman autoimmune disorders include intracellularsignaling molecules and receptors (PTPN22, BANK1,TNFAIP3, BLK, PTPN2, TRAF1), intracellular pattern-recognition receptors (IFIH1, NOD2/CARD15),transcriptions factors (REL, STAT4, IRF5, NKX2-3),cytokines and cytokine receptors (IL-2/II21, IL-23R,IL-7RA, IL-7RA, IL-2RA, IL-12B), membrane receptorsand costimulatory molecules (CTLA4, ITGAM,
CD40), autophagy-related genes (ATG16L1, IRGM),enzymes (ARTS1, PADI4), and autoantigens (INS,TSHR).24 The current crop of genetic associations isonly the start of a complete catalog of genetic factorsfor autoimmunity. These findings are beginning toshed light on themolecular pathways and pleiotropiceffects of several risk factors and the allelic hetero-geneity underlying susceptibility to these autoim-mune diseases. These findings may result in morespecific treatments for psoriasis and autoimmunediseases based on genetic and molecular pathways.
We also observed evidence for increased preva-lence of alopecia areata, consistent with findingsfrom a Taiwan nationwide population-basedstudy.25 Both studies show an OR of 2.4. The currentstudy also gave evidence for a 2.3-fold greater risk ofceliac disease co-occurring with psoriasis. Our resultis consistent with a Swedish nationwide cohort studyshowing the association between celiac disease andpsoriasis to be independent of a temporal relation-ship, with OR of 1.9 (95% CI 1.6-2.3).26 There areseveral overlaps between psoriasis and autoimmunediseases particularly IBD, giant cell arteritis, andpulmonary fibrosis.7 Psoriasis has been stronglylinked with IBD, specifically Crohn’s disease.27,28
Similar to psoriasis, Crohn’s disease is mediated byan abnormal T-helper-1 immune response.28
Moreover, family members affected with Crohn’sdisease or psoriasis are more likely to have closerelatives affected by the other disease.29
This study provides further evidence that there isan association between psoriasis and autoimmunediseases. There was a trend that those with psoriaticarthritis were more likely to have an autoimmunedisease compared to those with psoriasis. The pre-sent study suggests that evaluating psoriasis patientsfor autoimmune diseases may be warranted as partof their medical care.
REFERENCES
1. Gelfand JM, Weinstein R, Porter SB, Neimann AL, Berlin JA,
Margolis DJ. Prevalence and treatment of psoriasis in the
United Kingdom: a population-based study. Arch Dermatol
2005;141:1537-41.
2. Stern RS, Nijsten T, Feldman SR, Margolis DJ, Rolstad T.
Psoriasis is common, carries a substantial burden even
when not extensive, and is associated with widespread
treatment dissatisfaction. J Invest Dermatol Symp Proc 2004;
9:136-9.
3. National Psoriasis Foundation. Population statistics. Available
from: URL:http://www.psoriasis.org/about/stats. Accessed May
8, 2011.
4. Davidson A, Diamond B. Autoimmune diseases. N Engl J Med
2002;345:340-50.
5. Boren E, Gershwin ME. Inflamm-aging: autoimmunity and the
immune-risk phenotype. Autoimmun Rev 2004;3:401-6.
6. Schon MP, Boehncke WH. Psoriasis. N Engl J Med 2005;352:
1899-922.

J AM ACAD DERMATOL
NOVEMBER 2012930 Wu et al
7. Makredes M, Robinson D Jr, Bala M, Kimball AB. The burden of
autoimmune disease: a comparison of prevalence ratios in
patients with psoriatic arthritis and psoriasis. J Am Acad
Dermatol 2009;61:405-10.
8. Prey S, Paul C, Bronsard V, Puzenat E, Gourraud PA, Aractingi S,
et al. Assessment of risk of psoriatic arthritis in patients with
plaque psoriasis: a systematic review of the literature. J Eur
Acad Dermatol Venereol 2010;24(Suppl 2):31-5.
9. Nair RP, Henseler T, Jenisch S, Stuart P, Bichakjian CK, Lenk W,
et al. Evidence for two psoriasis susceptibility loci (HLA and
17q) and two novel candidate regions (16q and 20p) by
genome-wide scan. Hum Mol Genet 1997;6:1349-56.
10. Liu Y, Helms C, Liao W, Zaba LC, Duan S, Gardner J, et al. A
genome-wide association study of psoriasis and psoriatic
arthritis identifies new disease loci. PLoS Genet 2008;4:
e1000041.
11. Langley RG, Krueger GG, Griffiths CE. Psoriasis: epidemiology,
clinical features, and quality of life. Ann Rheum Dis 2005;
64(Suppl): ii18-25.
12. Weng X, Liu L, Barcellos LF, Allison JE, Herrinton LJ. Clustering
of inflammatory bowel disease with immune mediated dis-
eases among members of a northern California-managed care
organization. Am J Gastroenterol 2007;102:1429-35.
13. Jamshidi F, Bouzari N, Seirafi H, Farnaghi F, Firooz A. The
prevalence of psoriatic arthritis in psoriatic patients in Tehran,
Iran. Arch Iran Med 2008;11:162-5.
14. Ciocon DH, Kimball AB. Psoriasis and psoriatic arthritis: sepa-
rate or one and the same? Br J Dermatol 2007;157:850-60.
15. Strober B, Teller C, Yamauchi P, Miller JL, Hooper M, Yang YC,
et al. Effects of etanercept on C-reactive protein levels in
psoriasis and psoriatic arthritis. Br J Dermatol 2008;159:
322-30.
16. Tam LS, Tomlinson B, Chu TT, Li M, Leung YY, Kwok LW, et al.
Cardiovascular risk profile of patients with psoriatic arthritis
compared to controlsethe role of inflammation. Rheumatol-
ogy (Oxford) 2008;47:718-23.
17. Chandran V, Cook RJ, Edwin J, Shen H, Pellett FJ, Shanmugar-
ajah S, et al. Soluble biomarkers differentiate patients with
psoriatic arthritis from those with psoriasis without arthritis.
Rheumatology (Oxford) 2010;49:1399-405.
18. Elkayam O, Yaron I, Shirazi I, Yaron M, Caspi D. Serum levels of
IL-10, IL-6, IL-1ra, and sIL-2R in patients with psoriatic arthritis.
Rheumatol Int 2000;19:101-5.
19. Ritchlin CT, Qureshi AA, de Vlam K, Pitzalis C, Helliwell PS,
Mease PJ, et al. Biomarkers in psoriasis and psoriatic arthritis:
GRAPPA 2008. J Rheumatol 2010;37:462-7.
20. Li Y, Begovich AB. Unraveling the genetics of complex
diseases: susceptibility genes for rheumatoid arthritis and
psoriasis. Semin Immunol 2009;21:318-27.
21. Invernizzi P, Gershwin ME. The genetics of human autoim-
mune disease. J Autoimmun 2009;33:290-9.
22. Criswell LA, Pfeiffer KA, Lum RF, Gonzales B, Novitzke J, Kern
M, et al. Analysis of families in the multiple autoimmune
disease genetics consortium (MADGC) collection: the PTPN22
620W allele associates with multiple autoimmune phenotypes.
Am J Hum Genet 2005;76:561-71.
23. Zenewicz LA, Abraham C, Flavell RA, Cho JH. Unraveling the
genetics of autoimmunity. Cell 2010;140:791-7.
24. Gregersen PK, Olsson LM. Recent advances in the genetics of
autoimmune disease. Annu Rev Immunol 2009;27:363-91.
25. Chu SY, Chen YJ, Tseng WC, Lin MW, Chen TJ, Hwang CY, et al.
Comorbidity profiles among patients with alopecia areata: the
importance of onset age, a nationwide population-based
study. J Am Acad Dermatol 2011;65:949-56.
26. Ludvigsson JF, Lindelof B, Zingone F, Ciacci C. Psoriasis in a
nationwide cohort study of patients with celiac disease.
J Invest Dermatol 2011;131:2010-6.
27. Gupta G, Gelfand JM, Lewis JD. Increased risk for demyelin-
ating diseases in patients with inflammatory bowel disease.
Gastroenterology 2005;129:819-26.
28. Najarian DJ, Gottlieb AB. Connections between psoriasis and
Crohn’s disease. J Am Acad Dermatol 2003;48:805-21; quiz
22-4.
29. Lee FI, Bellary SV, Francis C. Increased occurrence of psoriasis
in patients with Crohn’s disease and their relatives. Am J
Gastroenterol 1990;85:962-3.





























