Embed Size (px)
Citation preview

The Behavioral Approach • A treatment approach (maybe the only in
psychology) that relies heavily on others’ (paraprofessionals, civilians) implementing it.
• Everyone thinks they know how to do it because they were reared with it and continue to be shaped by it.
• Works with people and other critters. Often misunderstood. Pigeons

“If a person doesn’t know how to read, we teach. If a person doesn’t know how to swim, we teach.
If a person doesn’t know how to multiply, we teach. If a person doesn’t know how to drive, we teach.
If a person doesn’t know how to behave, We......teach?.…punish?
Why can’t we finish the last sentence as automatically as we do the others?”
Tom Herner {modified “child” to “person”} (NASDE President ) 1998

Positive Behavior Supports Edward Carr et. al., Positive Behavior Support:
Evolution of an Applied Science, Journal of Positive Behavior Interventions January 2002 vol. 4 no. 1 4-16
DDS definition: “Positive Behavioral Supports is a systematic, person-centered
approach to understanding the reasons for behavior and applying evidence-based practices for prevention, proactive intervention, teaching and responding to behavior, with the goal of achieving meaningful social outcomes, increasing learning and enhancing the quality of life across the lifespan.”

Basic Elements of PBS • PBS emphasizes operationally defined and valued
outcomes for all individuals. • PBS is based on established behavioral and biomedical
sciences that can be applied to address problem behavior. • PBS emphasizes research-validated practices to achieve
goals and outcomes. Data are used to guide the selection of practices to achieve those goals/outcomes.
• PBS gives priority to systems that support the effective and efficient selection and implementation of practices by agencies.

Philosophy of Care Can vs. Can’t (EBIG 2009)
Rather than focus on what a person can’t do (although this is often how
problem behaviors are initially defined) try to find what they can or could do and set goals, objectives and treatment around those areas.
Protecting a person from harm shouldn’t preclude them from being given
opportunities to (safely) try or fail Can vs. Can’t can help increase new behaviors and improve dignity through
risk taking A Can vs Can’t philosophy opens the door to creative and rewarding treatment
opportunities, and develops care plans that promote individual strengths

Philosophy of Care Active Treatment (EBIG 2009)
The concept of Active Treatment means providing interactions between
staff and the individual that result in increased skills and independence for the person being assisted. An acronym to guide this approach is PEARL which stands for:
P ositive - Staff are up-beat, request [not demand], encourage and prompt
(faded, errorless) E arly - Staff are on top of events, proactive, know individuals A ll - the time, across persons, places, materials, R einforcing - with sincere praise or individualized reinforcement L ook - Staff look for opportunities to teach and support

Basic Concepts

The A-B-C's of Behavior Antecedents – Behavior - Consequences
Behaviors (We all do it!!) Must be observable and measurable (not emotions, feelings) "How will we recognize it when we see it?" Adaptive vs. Maladaptive (Consider tracking both!) Physical vs. Social Examples: Aggression, SIB, Verbal abuse, Inappropriate Sexual behaviors, Social Inappropriate

Antecedents
"Any factor which precedes a behavior and influences it's probability of occurrence."
External vs. Internal Immediate vs. Remote
E.G., Noise, Med changes, Demands,
Behavior of others, Temperature, Delay or Withdrawal of Attention or other Reinforcer
Knowing them allows us to respond early, adjust conditions, or teach
alternate behavior

Controlling Caregivers as Antecedents
We can’t and shouldn’t act “normal”........ (need to act and be Better than normal)
Our
Behavior &
Attitude
Their Behavior
& Attitude
Affects

Controlling Caregivers as Antecedents (cont.)
Need to watch our voice: Tone/inflection Volume Speed/cadence and Body Language You may not notice these in yourself

Controlling Caregivers as Antecedents (cont.)
• Don’t Blame or Label the Individual • Individuals are predisposed to behave in
certain ways that are shaped by: Cognition, Perception
Memory, Pain/discomfort Embarrassment, Fear, Fatigue
• Therefore focus on the behavior, not the person per se

Controlling Caregivers as Antecedents (cont.)
Also: • We learn quickly by imitation, our moment to moment,
day by day interactions shape behavior. • Try to apply a 4:1 positive to corrective interaction ratio. • Take time out to establish a positive rapport with the
individual. • Catch folks doing well! The power of Sr+!! • The “Arms length rule” for reinforcement and
corrective feedback. • “Inappropriate” is inappropriate (use natural speech).

Bad Examples • “You need to stay here and be quiet; I’m not going
to let you get away with that (hitting me)!” • “I’ve already answered you, Don’t ask me again!” • “If you’re not quiet, you won’t be getting any
lunch.” • “I wouldn’t talk to you that way!” • “You need to apologize before I’ll let you smoke.” • “Go to your room, now!”

Behavior Precursors
Early elements of a behavioral sequence; What the individual does
"Oh Oh here it comes!" E.G.; Pacing, Glaring, Clenched Fists,
Noticeable Change in Behavior ↓↑
Knowing them allows us to respond early, teach alternate behaviors, Redirect, or Use Crisis Intervention before things escalate

Consequences
(not what you’d think!) • When staff say“Well, aren’t you going to give them a consequence?”, what do they want you to do? • Most likely punishment • How do they want to punish? Usually by taking something away
The real definition is: "Any factor which follows a behavior and influences
it's probability of occurrence.“ Must be immediate, consistent, meaningful, contingent and
persistent to work.

Two Kinds: Reinforcement & Punishment
•Reinforcement: Any event following a behavior which increases the probability of the behavior occurring again, increases it's intensity or increases it's duration in the future. •Positive reinforcement: NOT BRIBES!! PAA-LEEEZ
•Primary reinforcers: Food, water, shelter, companionship, beer. •Secondary reinforcers: The stuff you cash-in to buy the primaries.

Negative Reinforcement (often confused with Punishment)
Definition: The removal of an aversive stimulus, contingent on a response, that increases the
strength of that response. Example: Seatbelt buzzer. To make the buzzer
stop you buckle seatbelt thereby reinforcing strength of seatbelt use.

Positive vs. Negative Reinforcement Explained (finally)
POSITIVE REINFORCEMENT NEGATIVE REINFORCEMENT
BBUUYY 11 GGEETT 11 FFRREEEE!!

Punishment • Any event following a behavior which decreases
the probability of the behavior occurring again, decreases it's intensity or decreases it's duration in the future.
• Type I = Apply an aversive: spanking, petting a sleeping hamster
• Type II = Withdraw a reinforcer: speeding ticket,
“No soup for you!”

Why Punishment’s Not the Way to Go
1. Tends to work temporarily 2. Tends to work only under conditions of where and who
originally presented (i.e., doesn’t generalize) 3. Elicits counter-attack and ruins therapeutic rapport 4. Person doesn’t want to learn from and in-turn avoids person
who’s punishing 5. Is easily abused 6. Makes person delivering the punishment feel lousy 7. Needs to be delivered all the time to work and can actually
increase behavior 8. Is unethical and disallowed by regulatory agencies

Setting Events
• A Setting Event (Kantor, 1959) is any biological factor that alters an individual’s response to a given environmental context.
• Sleep Disturbance • Poor Diet • Metabolic Disorders • Menses • Otitis Media • Fatigue (prolonged physical exertion, sleep disturbance,
temperature extremes, lack of sugar, salt, or water)

Antecedent (A) – Behavior (B) – Consequence (C)
– Basic unit of analysis for operant behavior – All ABA procedures involve the
manipulation of one or more components of the 3-term contingency
The Three Term Contingency

The Four-Term Contingency
• MO: Antecedent Behavior Consequence • Now, all ABA procedures involve the
manipulation of one or more components of the 4-term contingency.

• This fourth-term Motivating Operation (MO) is a relatively recent addition.
• MO: Antecedent-Behavior-Consequence • In sum, MOs have two defining effects. They alter (a) the effectiveness of consequences (the value-altering effect) and (b) the frequency of operant response classes related to those consequences (the behavior altering effect). Let me give you some examples, common and peculiar to individuals with brain injury….
Familiar and Unfamiliar Terms

ASSESSMENT

Functional Assessment What are the possible functions of a behavior? or......."What's the payoff?“ The ABC form (run lots) Possible functions: a. Increase Attention b. Terminate Demands/Decrease Attention c. Seek Assistance/Help d. Access to Reinforcement (delay or withdrawal situations) e. Self-stimulation (automatic reinforcement)

Behavior Analysis Form Patient: _________________ Objectively enter antecedents (what happened in the environment before the behavior i.e., what pt. said, you said, things happening around pt.): clear def. of behavior: and consequence (what you did, others reactions etc.)
Date Time Antecedents Behavior Consequences Setting Comments

Also Assess: Person’s skills: Communication, motor ability, ADL's Family/client history Mediator analysis (people in contact with client) Ecological Factors (lighting, noise etc.) Positive Programming (what programming is happening for skill acquisition) Look at the behaviors course, strength, cycle etc. Medication influences Etiology/diagnosis Conduct a reinforcer Inventory Involve person in behavior support plan as much as possible

TREATMENT

"Many behaviors can be viewed viewed as
serving a communicative function."

Effective Behavior
Programming Behavioral treatment can only work if all
interventions are: • Consistent (use the same approach), • Contingent (reinforcement occurs for the targeted behaviors and not for others), • Persistent (sticking with the program to see results), and • Adaptable (behavior programs are continuously modified to promote success)

Social/Physically Maladaptive
Behavior
Antecedents
Precursors
Payoff/Consequence
Alternate Response Training

Treatment Strategies
“Good behavioral programming requires; teaching new skills, rigorous data collection, tight contingency control, trained staff, safe
environments, and demands/tasks tailored to the individuals needs.”
Use a Multi-Element Approach

Treatment Strategies (cont.)
Proceed from the least to most restrictive intervention.
Favor antecedent management over consequences
"Teach the behavior away"

D.R.O. Differential Reinforcement of Other Behaviors
Person is reinforced after a specified period of no occurrence of the target behavior. If the behavior occurs the interval is reset. Advantages: Useful on all kinds of behaviors, flexible duration (down to seconds if needed). Drawbacks: Non-specific reinforcement, risk reinforcing behavior at the time of DRO delivery.

D.R.L. Differential Reinforcement of
Low Rates of Behavior Person is reinforced after a specified interval of time if the behavior occurs at a pre-set level or less. Initial criterion is set at baseline level. Advantages: Errorless, uses icons or markers, good w/impaired memory, can be arranged in full or partial intervals. Drawbacks: Uses response cost, peer pressure, gradual results.

Shaping & Chaining Shaping The gradual modification and differential
reinforcement of successive approximations to a desired behavior. E.g., student raising hand to get attention.
Chaining A procedure that involves teaching a complete
sequence of behaviors that must be performed in a particular order. Uses a Task Analysis. E.g., tooth brushing

Shaping • To help the person achieve their highest level of
independence, staff should use the smallest amount of help needed to do the task.
Most • Hand over hand (physically assisting) should be paired with verbal
information • Touch prompt (light physical prompt) should be paired with verbal
information • Full Verbal cue (tell rt. what to do) can be paired with gesture • Partial Verbal cue (some information “what should you do next?”
or phonetic cue e.g., “T” sound when the answer is ‘Tom’) • Modeling (demonstrate what to do so that rt. copies or imitates you) • Gesture (point to next step or action)
Least

Ignore/Extinction Withdrawal or withholding the reinforcer maintaining a
behavior. "Ignore the behavior but not the individual."
Difficult to carry out because demands perfect consistency. Behavior may get worse before better (Extinction Burst) Not possible on many behaviors (e.g., SIB, Aggression)

Redirection
Providing the person an alternate activity including the cues set-up and follow-through to complete the
redirection.
A temporary "reactive" strategy. Good during antecedent situations.

Token Economies
Providing a secondary (conditioned) reinforcers (e.g., money, tokens, points)
that’s later exchanged for a primary reinforcer (e.g., edible, activity, item)
Good for immediate delivery
Remember: Don’t use to punish (i.e., no fines) Can tailor primary reinforcer to the individual
Can be tough to fade

Crisis Intervention
Mediators should have good non-aversive crisis intervention training like:
Non-Violent Crisis Intervention (CPI)
PAC NAPPI

Keep things calm!
Time
Inte
nsity
Rationality
Precursors Antecedents
Recovery
Crisis
Successful de-escalation

Measurement and Evaluation
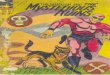
Anecdotal vs. Empirical Frequency: How often it happens, difficult with high rate behaviors Interval: Occurrence/Non-occurrence (+ or -) during an interval of time Duration: How long a behavior lasts Graphing: Line, Bar, Grid Analysis Reliability: Do verbal reports, notes and graphs match?

Sample Graph
0123456789
10
Mon Tue Wed Thur Fri Sat Sun
Days
Num
ber
Swearing Interrupting
Payoff < 2

0
5
10
15
20
25
30
35
40
45
M 2231Ju152230Ju152231 A 152231 S 152231 O 152231 N 152231 D 152231Ja152231Fe152228 M 152231 A 152230 M 152231Ju152230
Wee
k E
ndin
g
# Episodes
Non-Comp Inapp Soc Verbal AbusePhysical Abuse Elope Inapp. Sex.
Mellaril Dc’d, numerous
alternates tried
Mellaril restarted
Psychopharmacology use

Individual: __John D. Calm = � Swearing = X Hitting= ■ Month:_____Sept .08___________
9:00
8:00 X
7:00 X X X
6:00 X X X X X X X X X X
5:00 X X X X 4:00
3:00
2:00
1:00
12:00pm
11:00
10:00 X
X 9:00 X X X X X X X X X X
X X 8:00 X
X X 7:00am
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 Comments:
Inte
rval
end
ing
at:

Agitated Behavior Scale 1 = absent, 2 = slight degree, 3 = moderate degree 4 = extreme degree
AM/PM _____ 1. Short attention span, easy distractibility, inability to concentrate. _____ 2. Impulsive, impatient, low tolerance for pain or frustration. _____ 3. Uncooperative, resistant to care, demanding. _____ 4. Violent and or threatening violence toward people or property. _____ 5. Explosive and/or unpredictable anger. _____ 6. Rocking, rubbing, moaning or other self-stimulating behavior. _____ 7. Pulling at tubes, restraints, etc. _____ 8. Wandering from treatment areas. _____ 9. Restlessness, pacing, excessive movement. _____ 10. Repetitive behaviors, motor and/or verbal. _____ 11. Rapid, loud or excessive talking. _____ 12. Sudden changes of mood. _____ 13. Easily initiated or excessive crying and/or laughter. _____ 14. Self-abusiveness, physical and/or verbal. Total Score= 14-56

Generalization and Maintenance
(often missed, resulting in failure)
Generalization: Program to treat behavior across diverse settings, people, materials, conditions Maintenance: Fade treatment to where behavioral results are maintained over time, under natural contingencies and generalized conditions