Embed Size (px)
Citation preview
The Behavioral Risk Factor
Surveillance System
29 April 2010
Ali H. Mokdad, Ph.D.
Professor, Global Health
Outline
• Challenges for Surveys
• Behavioral Risk Factor Surveillance System (BRFSS)
• How BRFSS is dealing with the challenges
• Use of BRFSS for a national CVD surveillance system
Outline
• Challenges for Surveys
• Behavioral Risk Factor Surveillance System (BRFSS)
• Ways to deal with challenges
• Use of BRFSS for a national Cardiovascular Disease (CVD) surveillance system
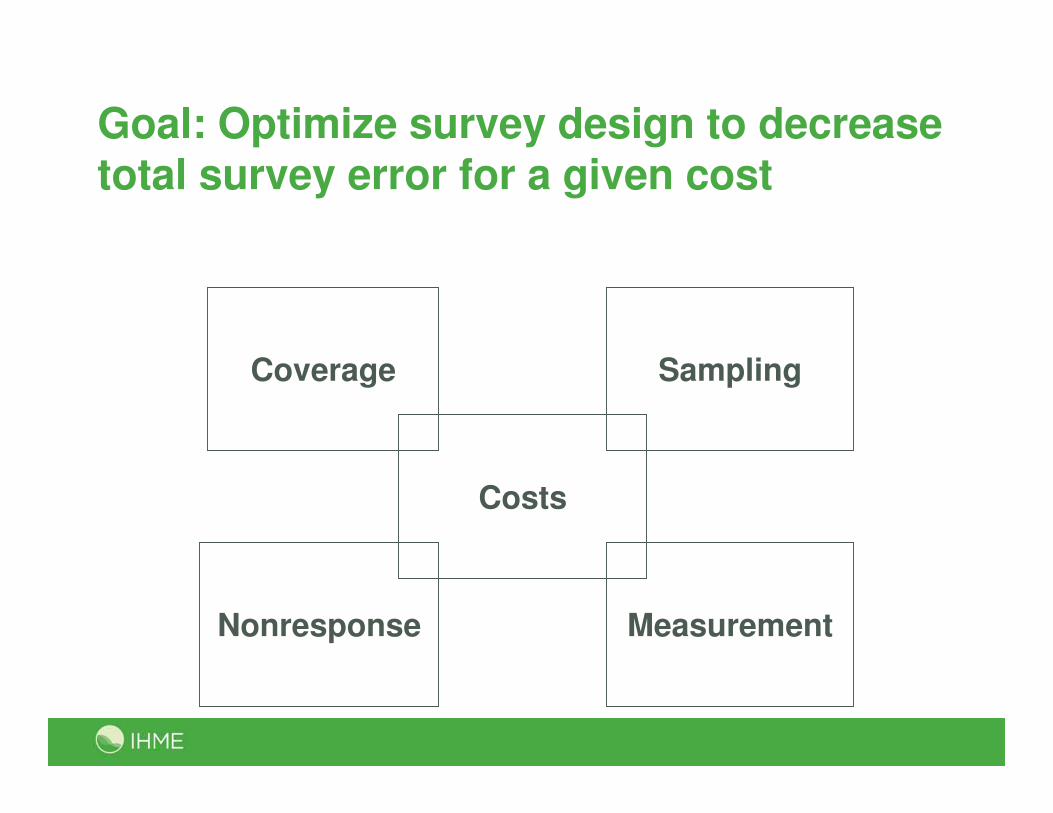
Goal: Optimize survey design to decrease total survey error for a given cost
Costs
MeasurementNonresponse
Coverage Sampling
Sampling
• Each element has a known and nonzero probability of selection from sampling frame
o Protection against selection bias
o Quantify sampling error
• Sampling by key modes:
o Face-to-face and telephone: well-developed techniques
o Mail: within-household selection techniques, quasi-random for general pop surveys
o Email: tend to be nonprobability; opt-in samples
Nonresponse
• Inability to obtain data from selected respondent:
o Unit nonresponse
o Item nonresponse
• Nonresponse by key modes:
o Highest in face-to-face
o Lowest in Internet
• Item nonresponse varies by mode and question
Measurement
• Measurement error occurs when a respondent’s answer to a question is inaccurate (departs from the
“true” value)
• Modes vary in terms of:
o Interviewer versus self-administered
o Stimuli / manner in which survey question is conveyed to respondent (and response is recorded)
05
10
15
pe
rce
nt re
spo
nd
ing
yes
Tu
rkey
Vie
tna
mK
aza
khs
tan
Sp
ain
Ge
org
iaB
os.
& H
erz
.P
aki
sta
nS
ri L
anka
Ch
ina
Lao
PD
RH
un
gar
yM
yan
ma
rU
kra
ine
Uru
gua
yS
lov
akia
Ru
ssia
n F
ed.
UA
EM
ala
ysi
aP
hill
ipin
es
Cro
atia
Cz
ech
Re
pu
blic
Gha
na
Est
oni
aM
exi
co
Ma
uriti
us
La
tvia
Par
agu
ay
Slo
ven
iaE
cuad
or
Ma
law
iZ
imb
ab
we
Na
mib
iaB
ang
lad
esh
Mau
rita
nia
Tu
nis
iaG
ua
tem
ala
Za
mbi
aE
thio
pia
So
uth
Afr
ica
Mo
roc
coD
omin
ica
n R
ep.
Ma
liC
om
oro
sB
urk
ina
Fa
soC
ote
d'Iv
oir
eS
wa
zila
nd
Ke
nya
Se
ne
gal
Ch
ad
Bra
zil
Ind
iaC
on
go
Ne
pa
l
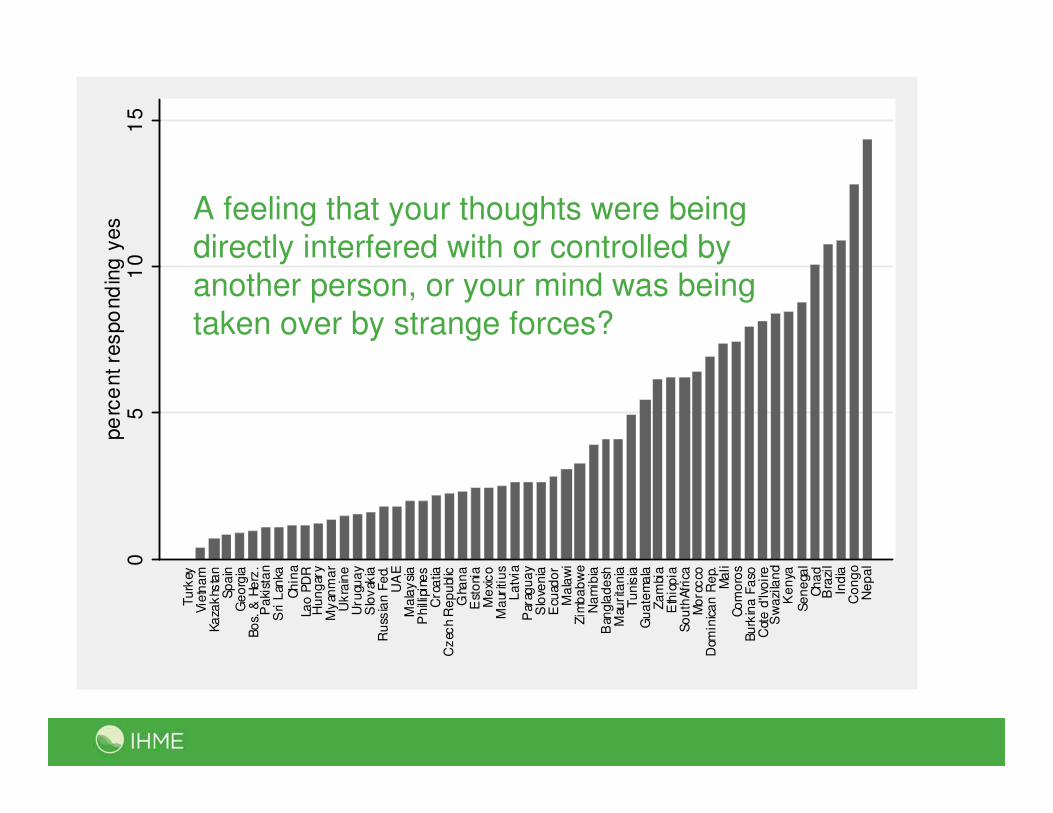
A feeling that your thoughts were being directly interfered with or controlled by
another person, or your mind was being
taken over by strange forces?
Coverage
• Sampling frame must include all units of the population of interest
o Frame coverage errors
• Coverage by key modes:
o Face-to-face: expensive to develop (lists help)
o Telephone: cell phones and number portability
o Mail: USPS list not complete, but improving
o Web: no comprehensive list
Declining response rates
• Response rates decreasing significantly in the last 10–15 years.
• Decline has occurred for most types of surveys—particularly telephone and in-person interviews.
• Evidence of trends for mail surveys not as clear due to lack of long-term trend studies.
• Web surveys are too new to provide good trend data.
• Increase in nonresponse is a global problem.
• No single or clear explanation for these trends.
Outline
• Challenges for Surveys
• Behavioral Risk Factor Surveillance System (BRFSS)
• How BRFSS is dealing with the challenges
• Use of BRFSS for a national CVD surveillance system
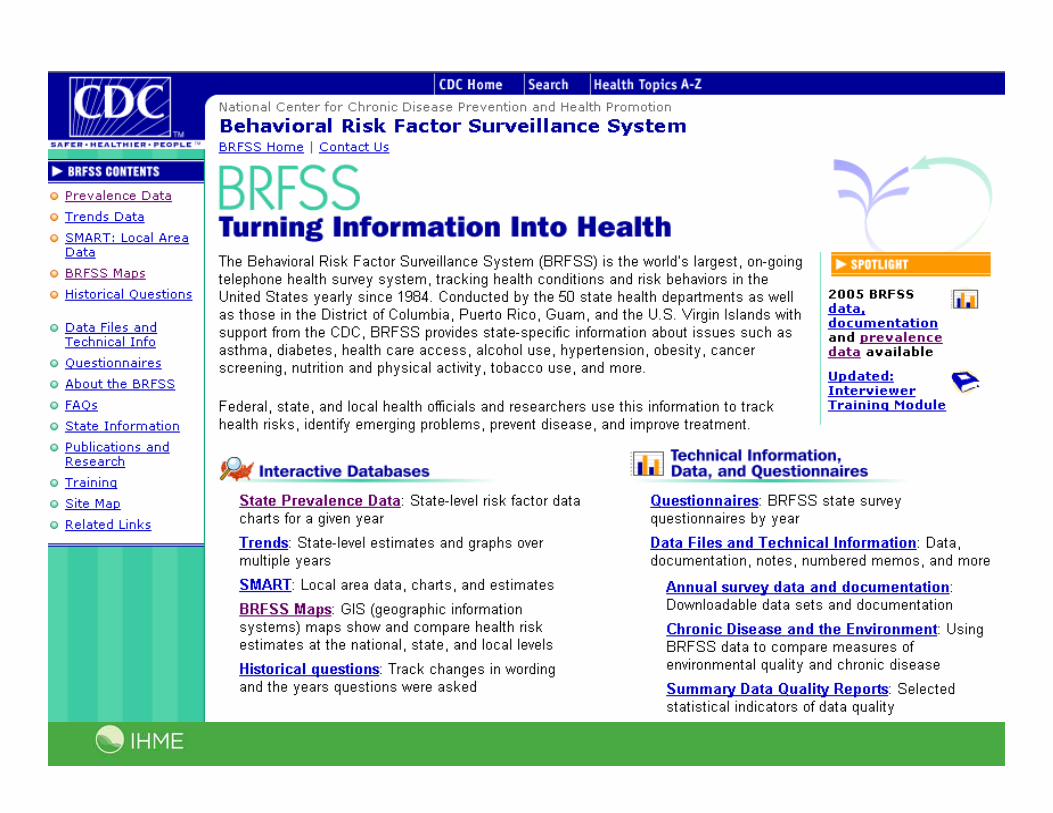
Behavioral Risk Factor Surveillance System (BRFSS)
• Monthly state-based Random Digit Dialing (RDD)
survey of health issues
• Collected by health departments in all states, District of Columbia, Puerto Rico, Guam, and Virgin Islands
• 420,000+ adult interviews conducted in 2008
• From 2002 to 2008:
o Completed over 2,250,000 interviews
o Dialed over 21,000,000 telephone numbers
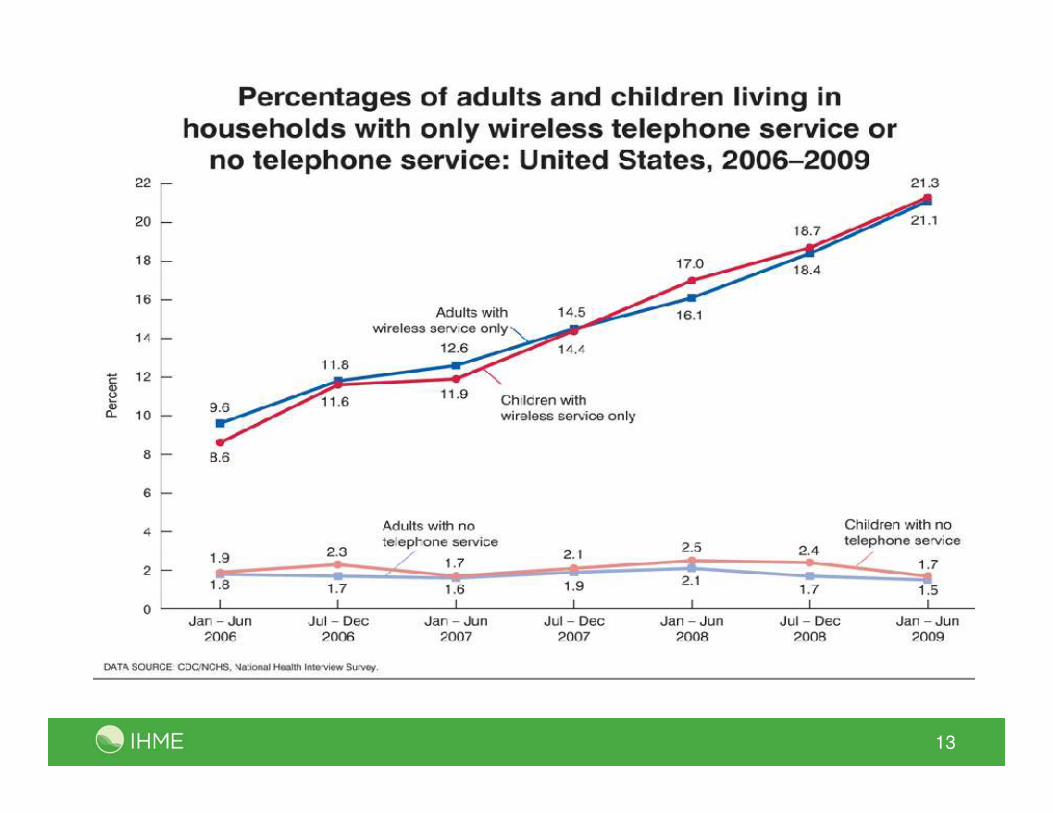
13
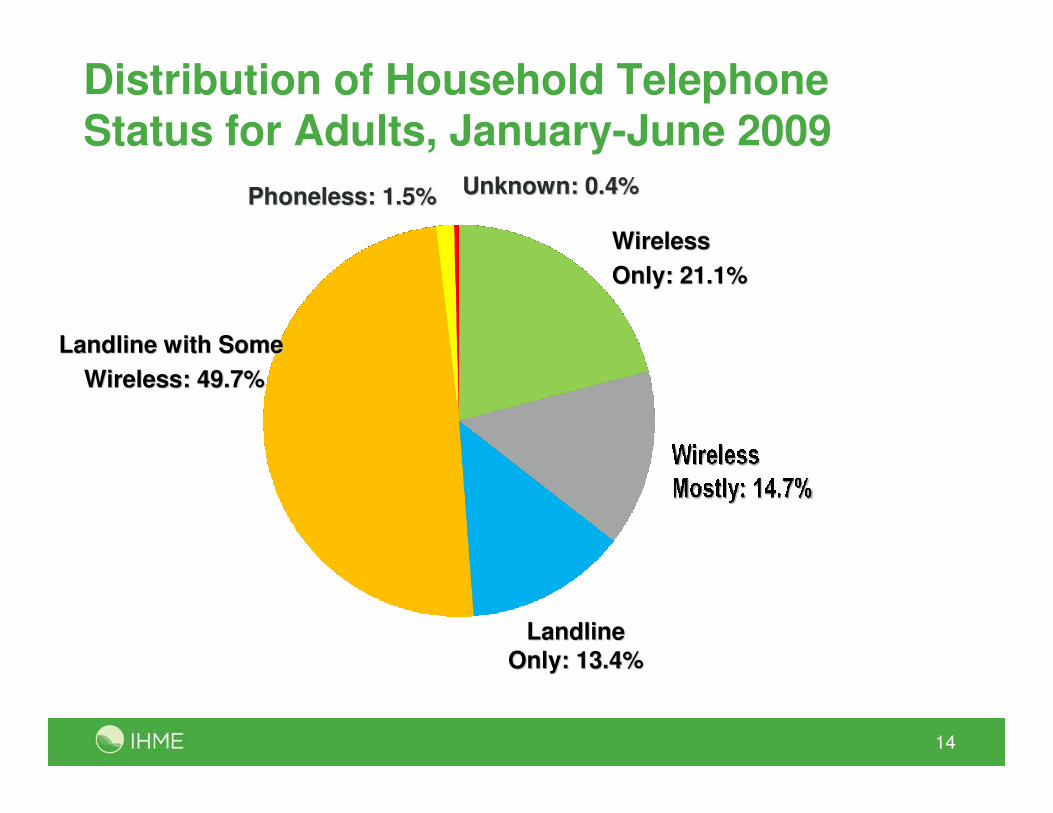
14
Distribution of Household Telephone Status for Adults, January-June 2009
Wireless Wireless
Only: 21.1%Only: 21.1%
Landline with SomeLandline with Some
Wireless: 49.7%Wireless: 49.7%
LandlineLandline
Only: 13.4%Only: 13.4%
Phoneless: 1.5%Phoneless: 1.5% Unknown: 0.4%Unknown: 0.4%
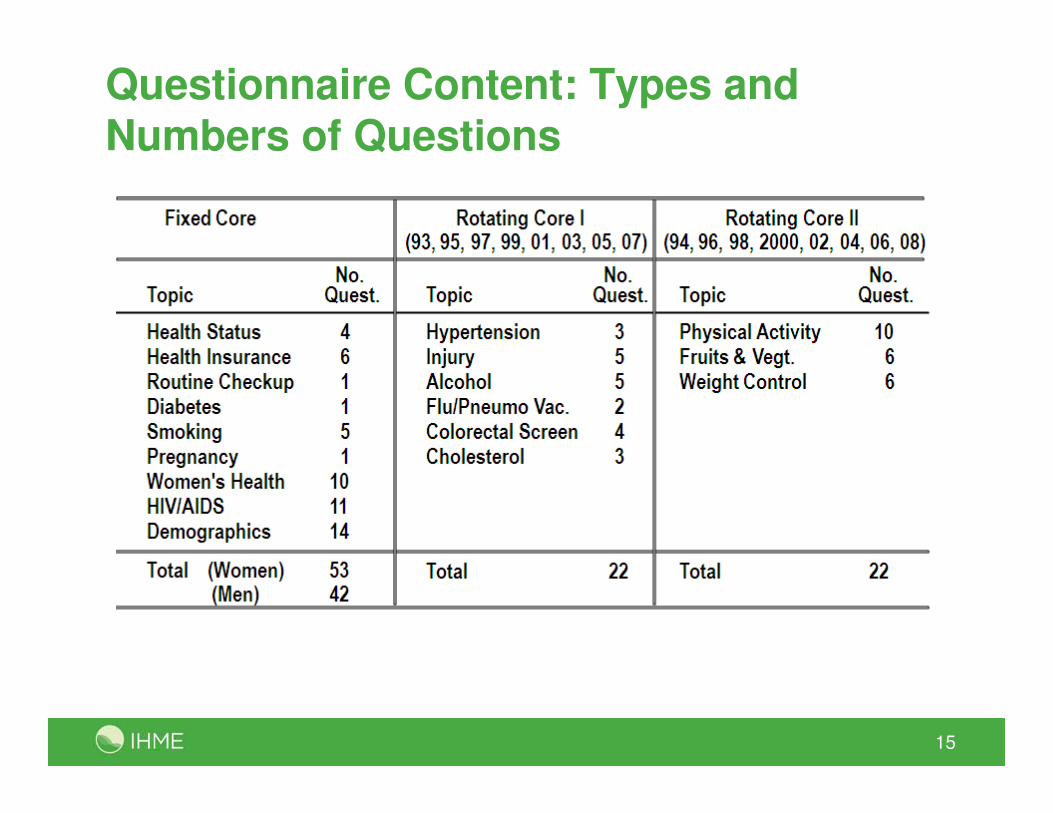
Questionnaire Content: Types and Numbers of Questions
15
CDC’s Role
• Questionnaire design and development
• Technical advice/support
• Data processing — cleaning, weighting, basic
analyses
• Analytic and epidemiologic support
• Data/information dissemination
Users of BRFSS Data
• State health departments
• CDC programs
• Department of Health and Human Services
• Other federal agencies
• Academic researchers and students
• Insurance companies
• Managed care organizations
• Nonprofit health organizations
State Health Departments and CDC
• Track health behaviors
• Identify emerging health issues
• Document health trends
• Evaluate prevention programs
• Measure progress toward health goals
• Develop programs and policies
BRFSS Strengths
• Flexible
• Timely
• Standardized
o Allows state-to-state comparisons
• Useful
• Relatively inexpensive
• Provides infrastructure for expansion and other studies
• True partnership
Flexibility
• Ability to add questions
• Ability to expand
• Ability to follow up
Timely
• States receive mid-year data reports
• States receive preliminary reports within a week of
submitting final year data
• Data files and prevalence tables are posted on the
Web site for public use within six months of the new year
Vaccine Shortage – Timeline
• Oct 5: Vaccine shortage announced
• Oct 5: Initial discussions within CDC
• Oct 19: Call with BRFSS state coordinators
• Oct 19-26: New questions developed and cognitively tested
• Oct 27: CATI specifications to states
• Nov 1: Data collection began
Morbidity and Mortality Weekly Report
• Dec 1-11: States collected December data
• Dec 13: Submitted files to CDC
• Dec 16: Dr. Gerberding holds press conference &
MMWR released on the CDC website
Standardized
• All states use same core questionnaire
• Standardized methodology for collection and analysis
• Allows for state-to-state comparisons
• Now allows for local-to-local area comparisons
Useful
• Identify emerging health problems
• Program development
• Policy development
• Tracking health risk trends
• Program evaluation

Develop Local Programs and Policies: SMART BRFSS in Fargo, ND
• Fargo, ND – 24.9% binge drinking vs. 16.4% nationwide
• Formed community coalition:
AMP (Alcohol Misuse Prevention)
• Mission: Reduce alcohol use among those under 21 in the Fargo-Moorhead area.
o Anti-binge drinking campaign
o Policy change sanctioning facilities
o Intervention with ER doctors
WEAT Startup Screen
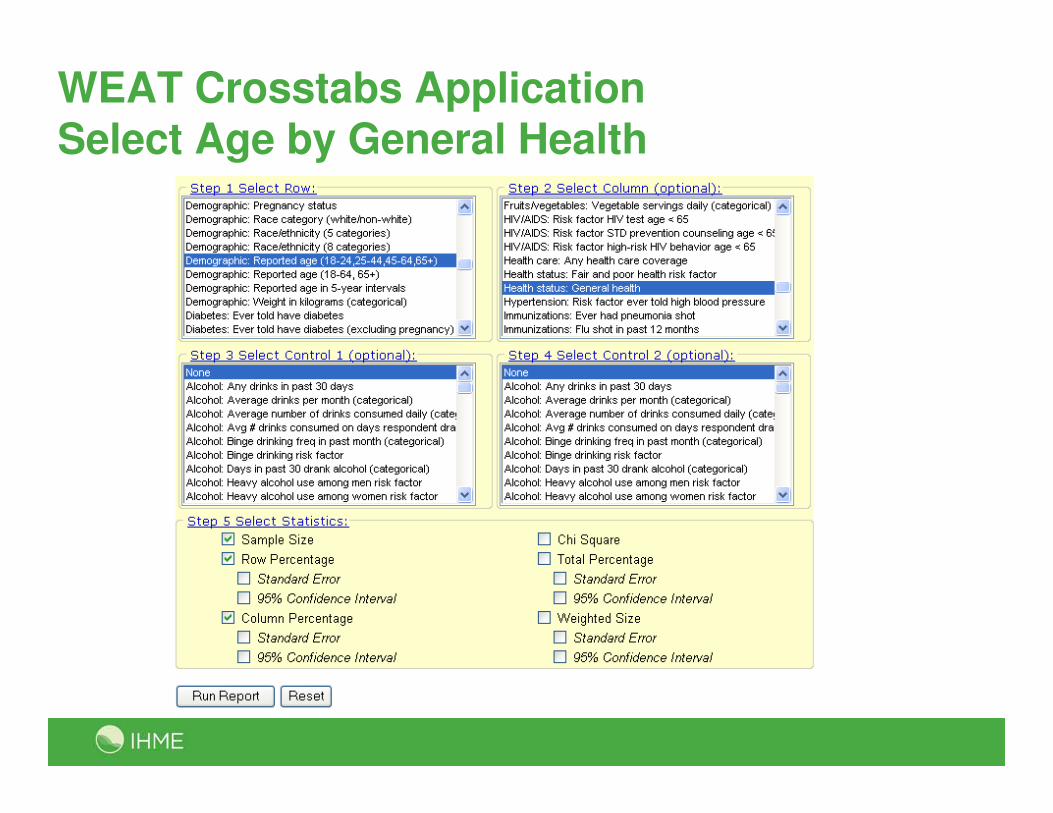
WEAT Crosstabs Application Select Age by General Health
Challenges
• Gathers self-reported information only
• Increasing number of questions being added to survey
• Telephone undercoverage
• Increase in cell phone usage
• Competition from telemarketers
• Rising demand for data at the state and local levels
Outline
• Background
• Challenges for Surveys
• Behavioral Risk Factor Surveillance System (BRFSS)
• Ways to deal with challenges
• Use of BRFSS for a national CVD surveillance system
Ensuring Validity of BRFSS Estimates
• Monitoring data collection process
• Refining post-survey adjustments
• Benchmarking to other studies
• Testing alternative ways of collecting data
o Cell phone interviewing
o Address-based sampling (ABS)
Monitoring the Data Collection Process
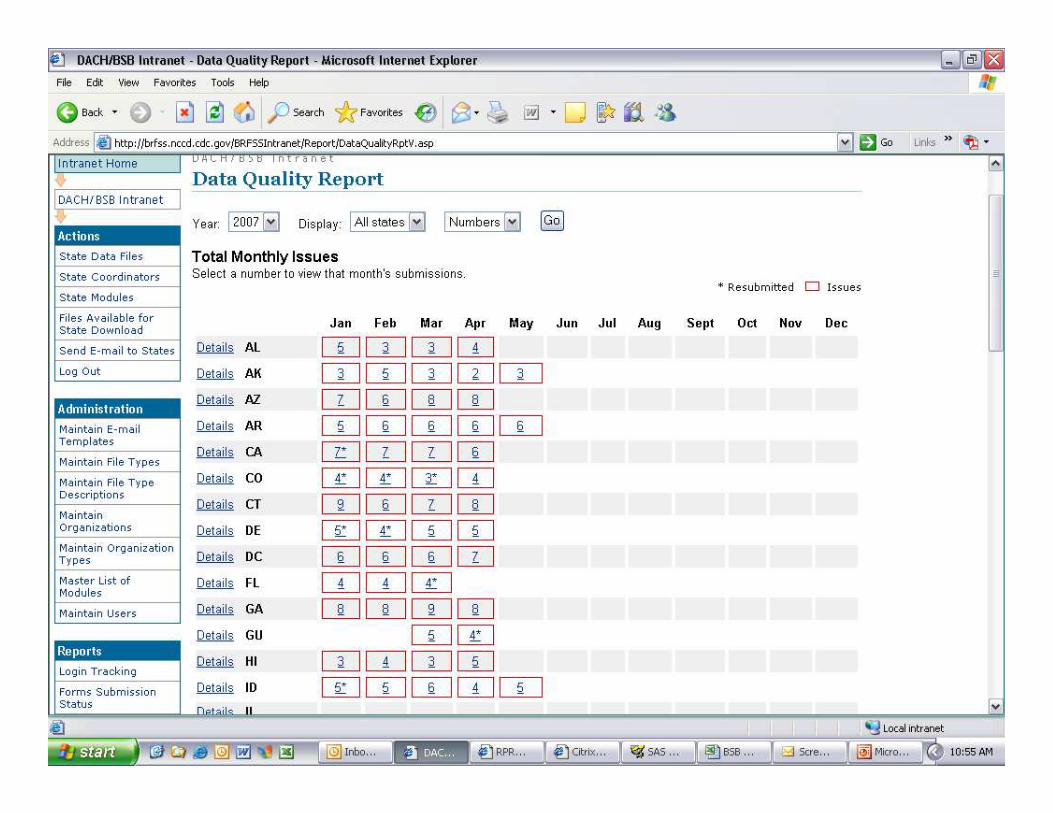
What did we learn?
• Estimates are only as valid as the process in which the data were collected
• Tools for monitoring the quality of data collection and collecting valid data are only good:
o … if they are actually used
o … and if they are understood
o … and initiate follow-up action
Refining post-survey adjustments
Goals and limits of weighting
• Weighting and other post-survey adjustments are used to correct for imbalances in the data due to issues of:
o Coverage
o Sampling
o Nonresponse
• Weighting methodology affects the estimates produced
• Can only weight data you have
o Assumes no difference between respondents and nonrespondents on variables of interest
• Can only weight to external standards that exist
o Typically limits weighting to a handful of demographic variables, not “substantive” variables
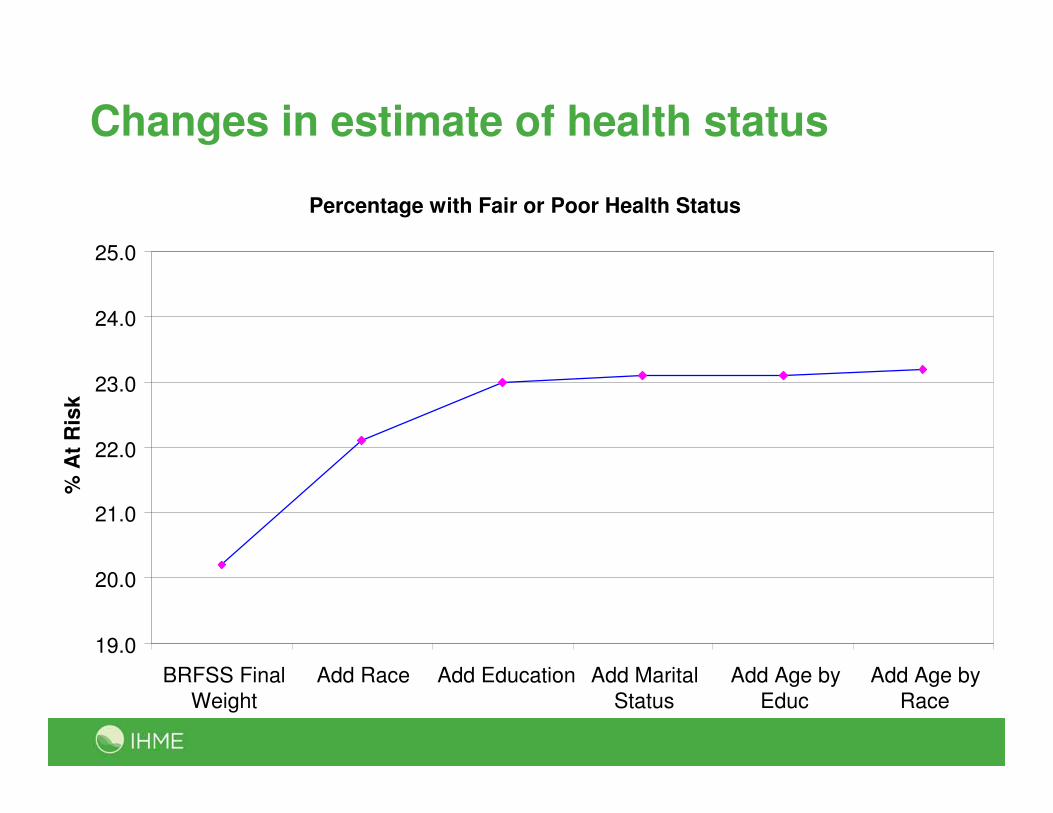
Changes in estimate of health status
Percentage with Fair or Poor Health Status
19.0
20.0
21.0
22.0
23.0
24.0
25.0
BRFSS Final
Weight
Add Race Add Education Add Marital
Status
Add Age by
Educ
Add Age by
Race
% A
t R
isk
What did we learn?
• Modifications to post-survey adjustments can improve
the quality of the estimates produced
• Sometimes need to be innovative in the use of external data in developing population estimates
Benchmarking to external standards
Importance and challenges of benchmarking
• True standards rarely exist in health surveys – relative standards
o Better coverage, response
• No two studies are identical
o Populations
o Modes / procedures
o Wording / question order
o Post-survey adjustments / population standards
What did we learn?
• There are no “gold standards” in health statistics
• All comparisons are relative
o Surveys can vary in terms of back-end processing just as much as on front-end design and operational issues
• Determining if BRFSS compares favorably with
other surveys is a matter of perspective
Finding new ways of collecting data:
Cell phonesand
Address-based sampling
Cell phones and telephone surveys
• Reliance on cell phones is increasing
• Conducting surveys via cell phones can be operationally challenging:
o Cell phone sampling frame very inefficient
o Cannot use autodialers
o Charges for incoming calls/minutes used
o Safety concerns
o Potential mode effects / measurement errors
What did we learn?
• The part of the population we are missing due to
cell phones is different from those we interview ---and we cannot ignore them
• Missing critical information needed to integrate
landline and cell phone samples at the subnational level
o No reliable external standards denoting telephone usage at subnational level
Address-based sampling
BRFSS 2006 Address-based sample (ABS)mixed-mode pilot survey
• Six states: CA, FL, MA, MN, TX, and SC
• Address-based sampling frame: USPS Delivery Sequence File (sample provided by Marketing Systems Group)
• Mixed mode data collection:
o Initial mail survey
o Postcard reminder
o Second mail survey (to nonrespondents)
o Telephone survey follow-up (of nonrespondents)
• 75 questions from BRFSS core questionnaire
• Field period: June 20-Oct 4, 2006
• Compared to monthly RDD surveys from same time frame
Within household randomization
• Mail survey (3 approaches tested):
oMost recent birthday (25%)
– One questionnaire
oNext birthday (25%)
– One questionnaire
oAll adults in household (50%)
– Three questionnaires
– Toll-free number for additional questionnaire
• Telephone follow-up survey:
o Used BRFSS protocol – number of males / number of females
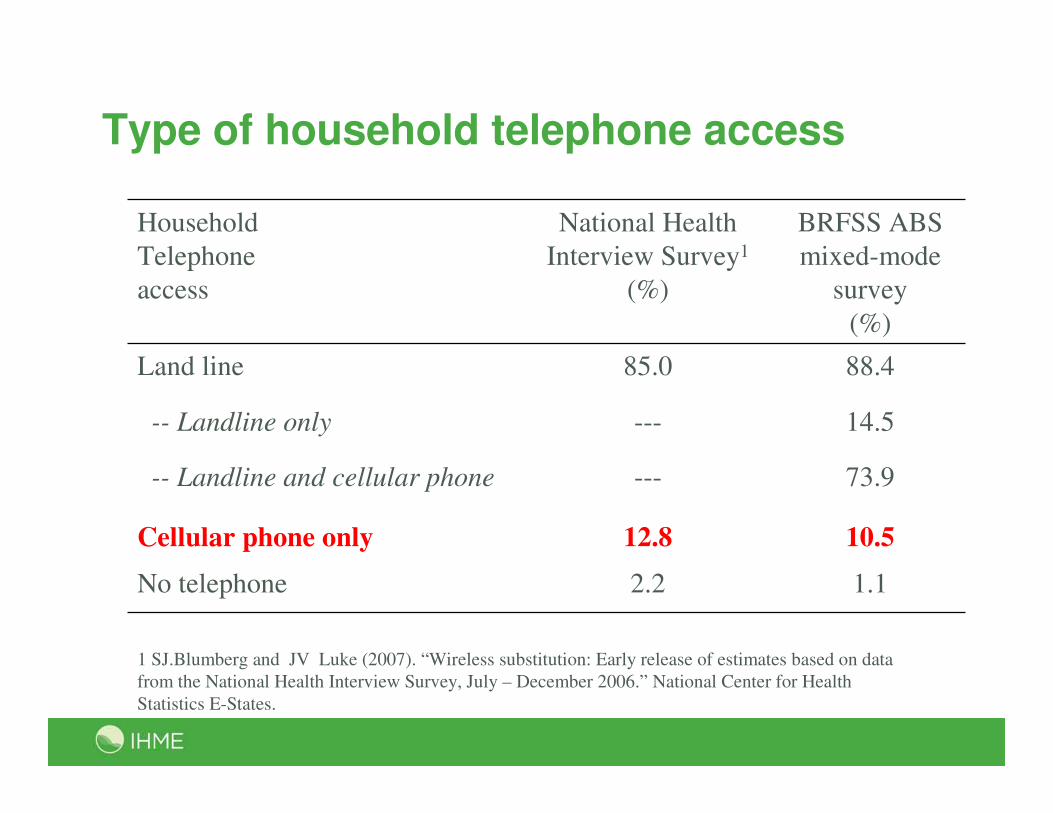
Type of household telephone access
1 SJ.Blumberg and JV Luke (2007). “Wireless substitution: Early release of estimates based on data
from the National Health Interview Survey, July – December 2006.” National Center for Health
Statistics E-States.
Household
Telephone
access
National Health
Interview Survey1
(%)
BRFSS ABS
mixed-mode
survey
(%)
Land line 85.0 88.4
-- Landline only --- 14.5
-- Landline and cellular phone --- 73.9
Cellular phone only 12.8 10.5
No telephone 2.2 1.1
Key findings fromABS mixed-mode design
• In states with low response rates, the address-based mixed-mode survey approach can yield response rates superior to RDD rates
• Approach reaches households without landline telephones
o Alternative to sampling from cell phone directories
• Mixed-mode data collection may result in cost savings
o Dependent on complexity of infrastructure put into place to integrate the approaches
What did we learn?
• We can reach cell phone population
• We can reach households with no telephones
Operational considerations
MULTIMODE
• May allow for total survey error for given cost
BUT
• Added complexity may produce mistakes and unexpected
consequences
Assessing Mode Effects – Key Enabler Is “Overlap”
MODE 1MODE 2
Outline
• Background
• Challenges for Surveys
• Behavioral Risk Factor Surveillance System (BRFSS)
• Ways to deal with challenges
• Use of BRFSS for a national CVD surveillance system
Surveillance System: Goals
• Surveillance of disease incidence and prevalence, functional health outcomes, measured risks, and public health and clinical response for the different Americas.
• Quantify the contribution of the major NCD risk factors to patterns and trends in disparities across the US
• Demonstrate an innovative model for surveillance that empowers local decision-makers with information in a decentralized health system that could be subsequently implemented on a wider basis
• Create an environment for conducting rigorous implementation research and evaluating the effectiveness of new health intervention programs
57
Basic Design
• Implement at the county level using an integrated multimode surveillance system.
• Each county would collect self-reported data, examination data, vital events, and provider data.
• Record linkage and repeat surveying of the same individuals would maximize the information content of the data collected.
• Surveillance data would be available for researchers in the public domain, with appropriate safeguards for privacy.
58
Surveillance System: Components
• Health and health care survey data
o Mixed-mode (telephone, cell phone, mail, in-person) interview survey
o Physical examination survey
• Administrative data
o Mortality data by cause from the vital registration system
o Health service provider data from hospitals, emergency rooms, and clinics
59
Role of BRFSS
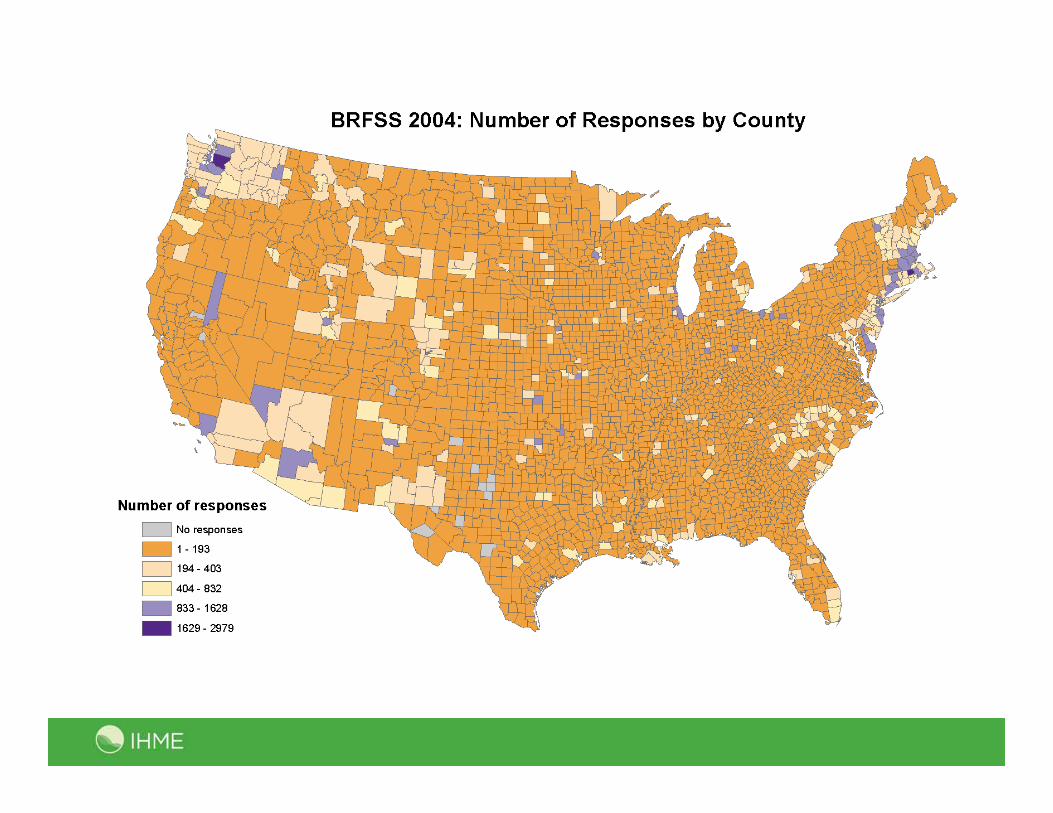
• Provides local data (over 300 counties)
• Mixed-mode experience (use ABS as a starting point)
• Physical examination survey (pilots in 3 states in 2008, 2 states in 2010)
• Administrative data (advantage has been a state-based surveillance)
61
Ali H. Mokdad, [email protected]





























