Embed Size (px)
Citation preview
The Burden And Management Of
Ischemic Heart Disease In Egypt
Dr. Sameh Shaheen M.B.B.Ch, MSc, MD, FESC, FSCAI
Prof of cardiology
Ain Shams University Cairo, Egypt
EGYPT: THE WORLD’s MOTHER
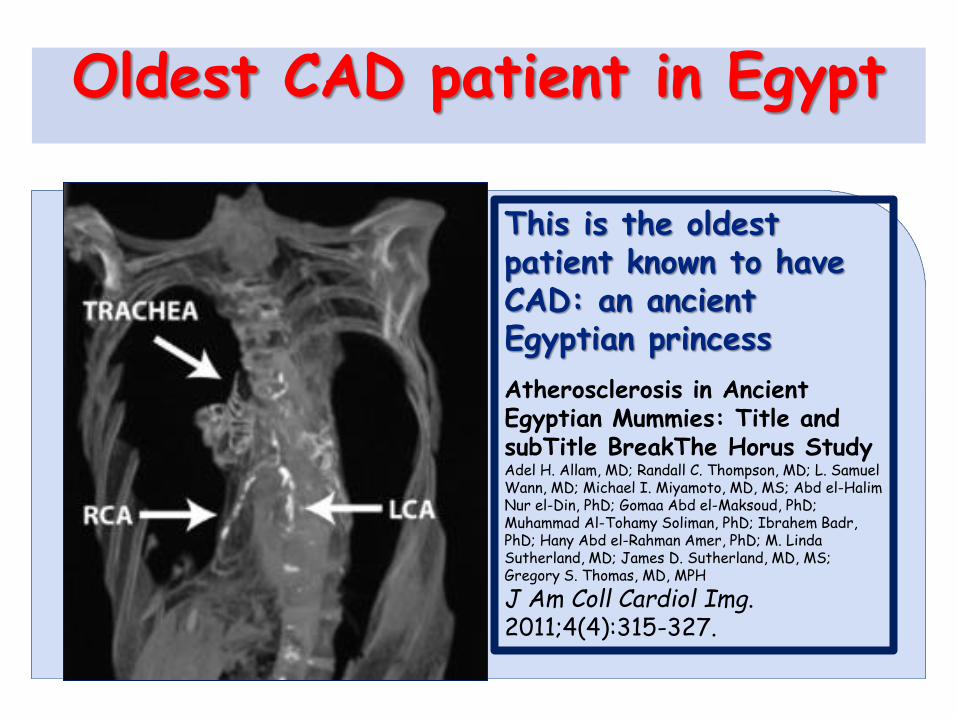
Oldest CAD patient in Egypt
This is the oldest patient known to have CAD: an ancient Egyptian princess
Atherosclerosis in Ancient Egyptian Mummies: Title and subTitle BreakThe Horus Study Adel H. Allam, MD; Randall C. Thompson, MD; L. Samuel Wann, MD; Michael I. Miyamoto, MD, MS; Abd el-Halim Nur el-Din, PhD; Gomaa Abd el-Maksoud, PhD; Muhammad Al-Tohamy Soliman, PhD; Ibrahem Badr, PhD; Hany Abd el-Rahman Amer, PhD; M. Linda Sutherland, MD; James D. Sutherland, MD, MS; Gregory S. Thomas, MD, MPH
J Am Coll Cardiol Img. 2011;4(4):315-327.

EGYPT mortality rate per 1000 in adult males World Bank Data
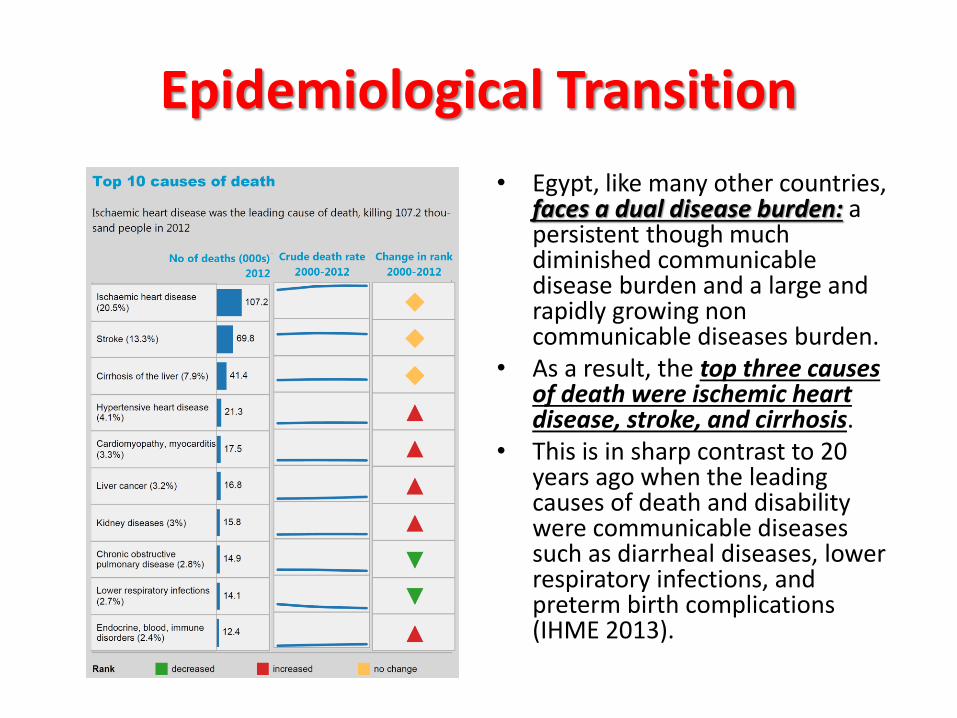
• Egypt, like many other countries, faces a dual disease burden: a persistent though much diminished communicable disease burden and a large and rapidly growing non communicable diseases burden.
• As a result, the top three causes of death were ischemic heart disease, stroke, and cirrhosis.
• This is in sharp contrast to 20 years ago when the leading causes of death and disability were communicable diseases such as diarrheal diseases, lower respiratory infections, and preterm birth complications (IHME 2013).
Epidemiological Transition
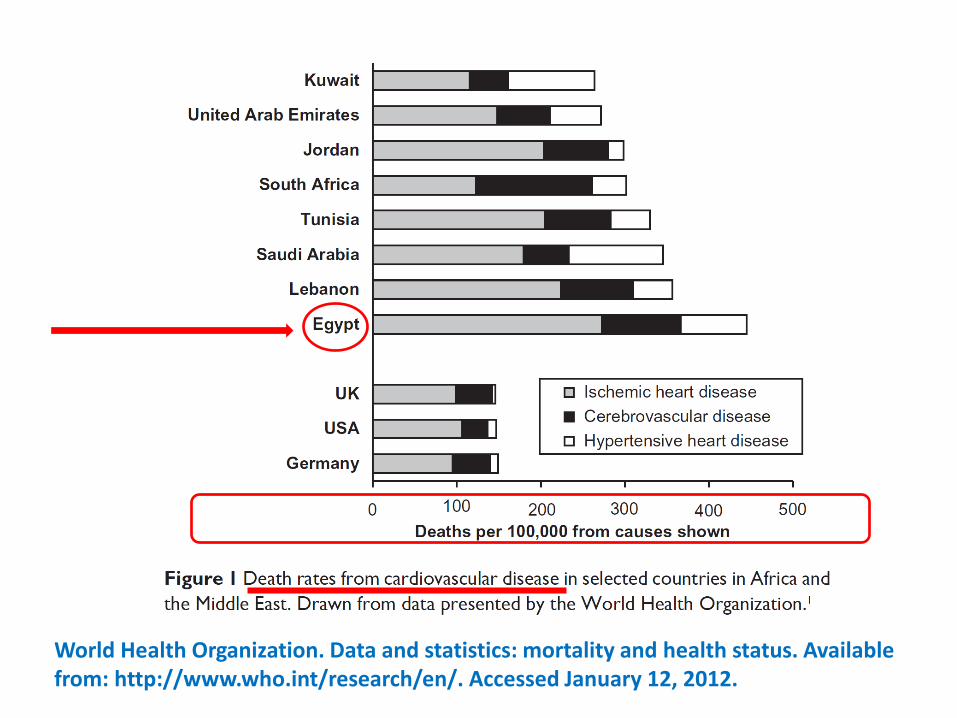
World Health Organization. Data and statistics: mortality and health status. Available from: http://www.who.int/research/en/. Accessed January 12, 2012.
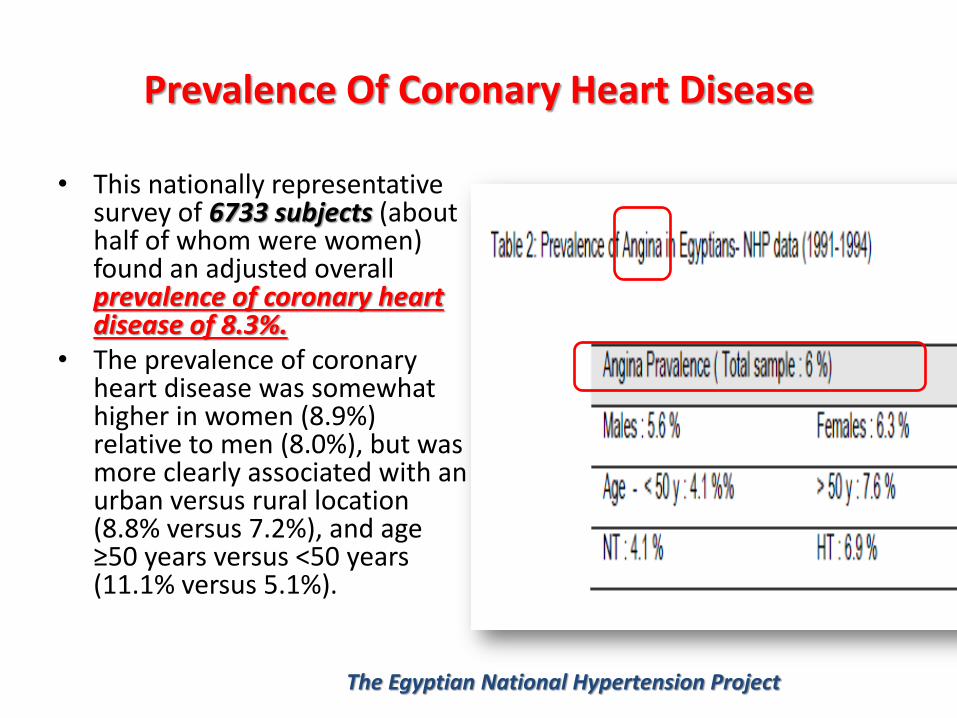
Prevalence Of Coronary Heart Disease
• This nationally representative survey of 6733 subjects (about half of whom were women) found an adjusted overall prevalence of coronary heart disease of 8.3%.
• The prevalence of coronary heart disease was somewhat higher in women (8.9%) relative to men (8.0%), but was more clearly associated with an urban versus rural location (8.8% versus 7.2%), and age ≥50 years versus <50 years (11.1% versus 5.1%).
The Egyptian National Hypertension Project
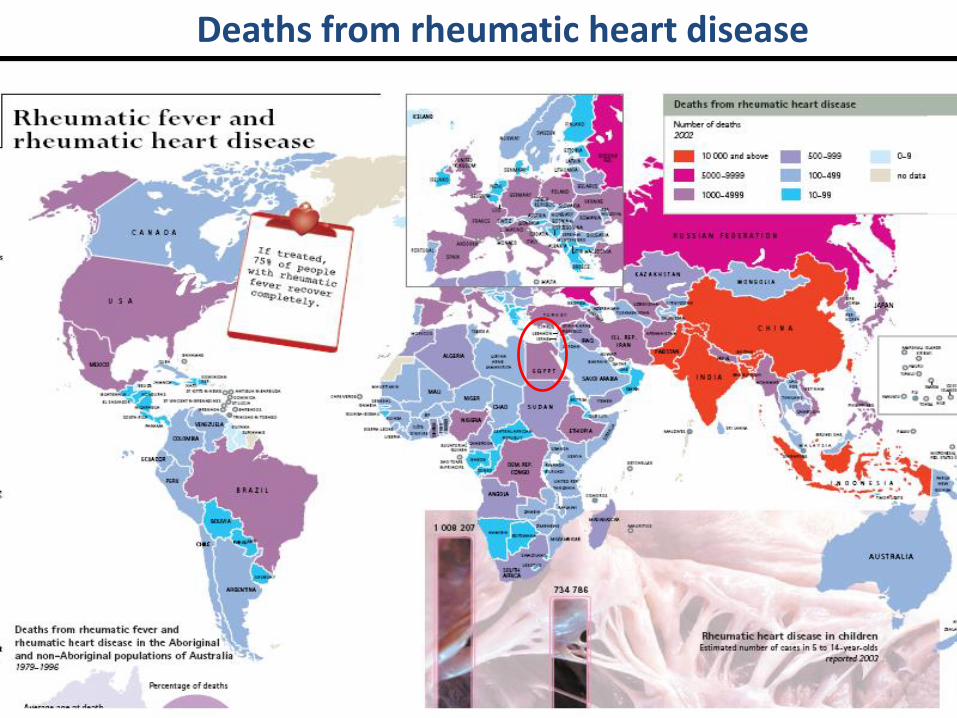
Deaths from rheumatic heart disease
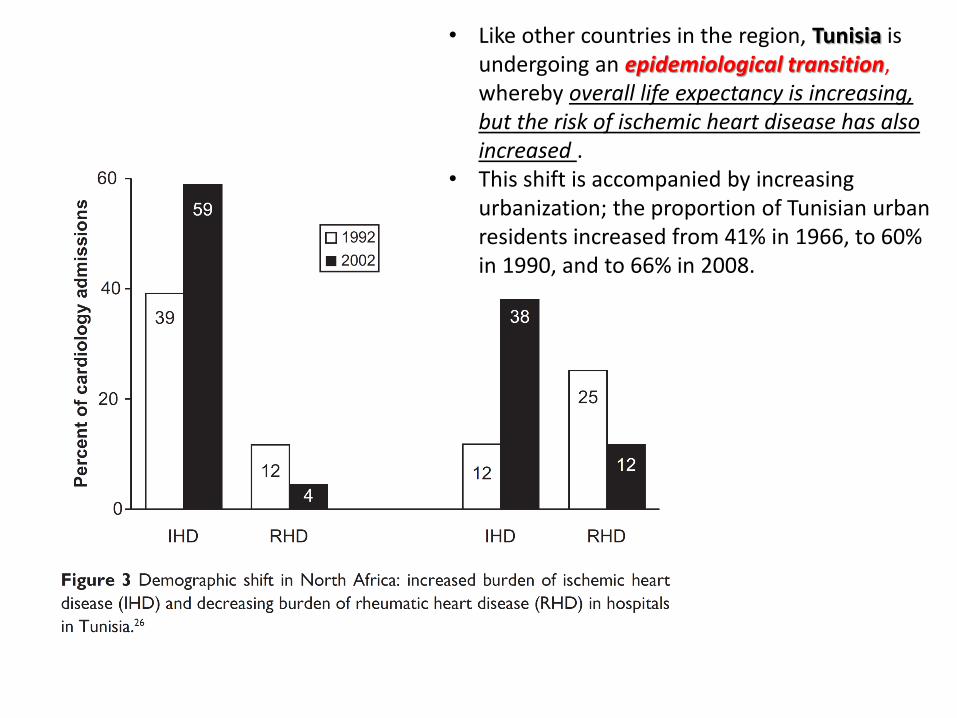
• Like other countries in the region, Tunisia is undergoing an epidemiological transition, whereby overall life expectancy is increasing, but the risk of ischemic heart disease has also increased .
• This shift is accompanied by increasing urbanization; the proportion of Tunisian urban residents increased from 41% in 1966, to 60% in 1990, and to 66% in 2008.
Differing Trends: age at presentation
• In developed countries, despite the overall increase in CHD burden, the age-adjusted death rates for CHD are declining. Thus the average age of death from CVD continues to climb and as a result affects a larger population in retirement.
• In the developing countries the age-adjusted death rates for coronary heart disease are increasing; and a relatively younger population is afflicted by CHD. Thus the increase number of deaths in the working age population.
• The INTERHEART study (an international case-control analysis of the risk factors for a first myocardial infarction conducted in more than 15,000 patients presenting with myocardial infarction in 52 countries) showed that the median age at presentation with myocardial infarction was 51 years in the middle east; this was lower than the median age at presentation in nine other regions, and was 12 years lower than the median age at presentation in western Europe
Yusuf S, Hawken S, Ounpuu S, et al. Effect of potentially
modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study.
Lancet. 2004;364: 937–952

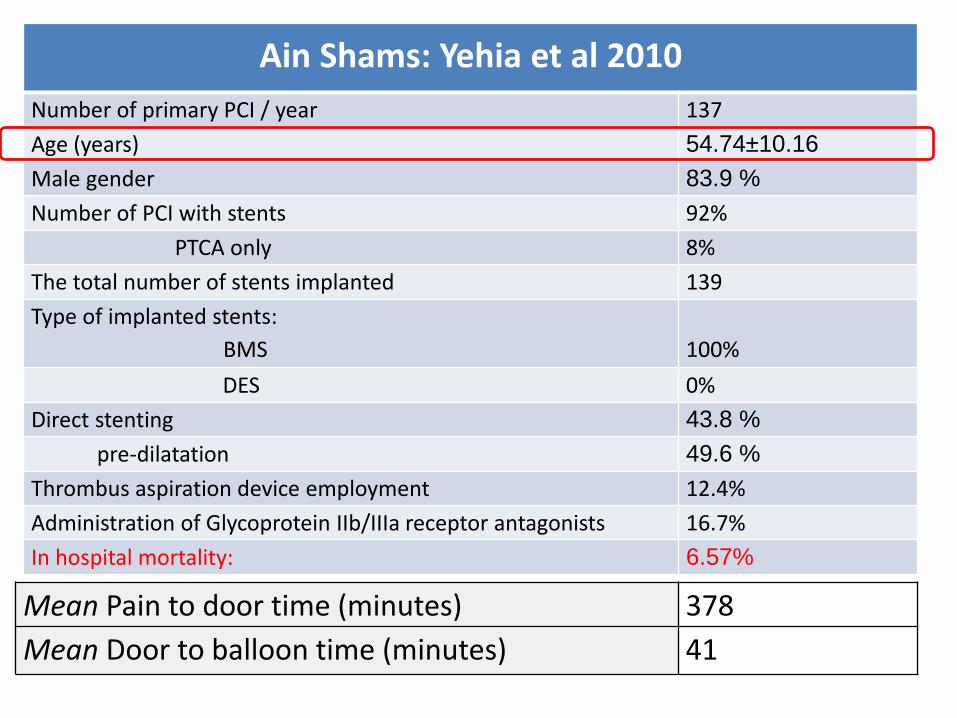
Ain Shams: Yehia et al 2010
Number of primary PCI / year 137
Age (years) 54.74±10.16
Male gender 83.9 %
Number of PCI with stents 92%
PTCA only 8%
The total number of stents implanted 139
Type of implanted stents:
BMS
100%
DES 0%
Direct stenting 43.8 %
pre-dilatation 49.6 %
Thrombus aspiration device employment 12.4%
Administration of Glycoprotein IIb/IIIa receptor antagonists 16.7%
In hospital mortality: 6.57%
Mean Pain to door time (minutes) 378
Mean Door to balloon time (minutes) 41

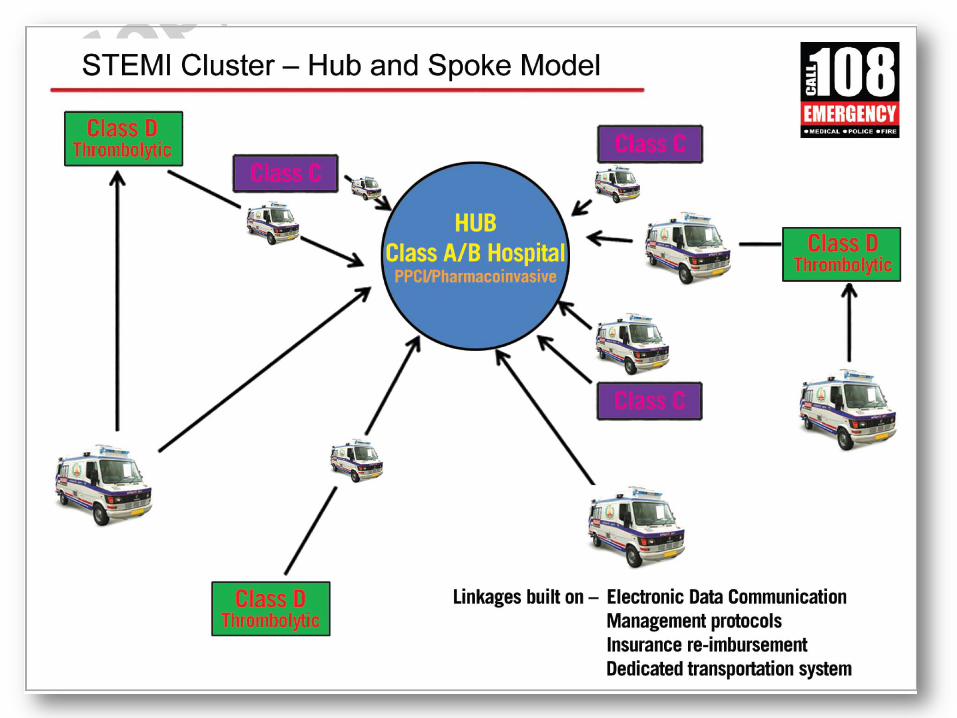
STEP to STEMI
ST Elevation Program
STEP to STEMI
Alignment Meeting October 14, 2014
Cairo Egypt
Dr. Sameh Shaheen MD, FESC Prof. of Cardiology
Ain Shams University
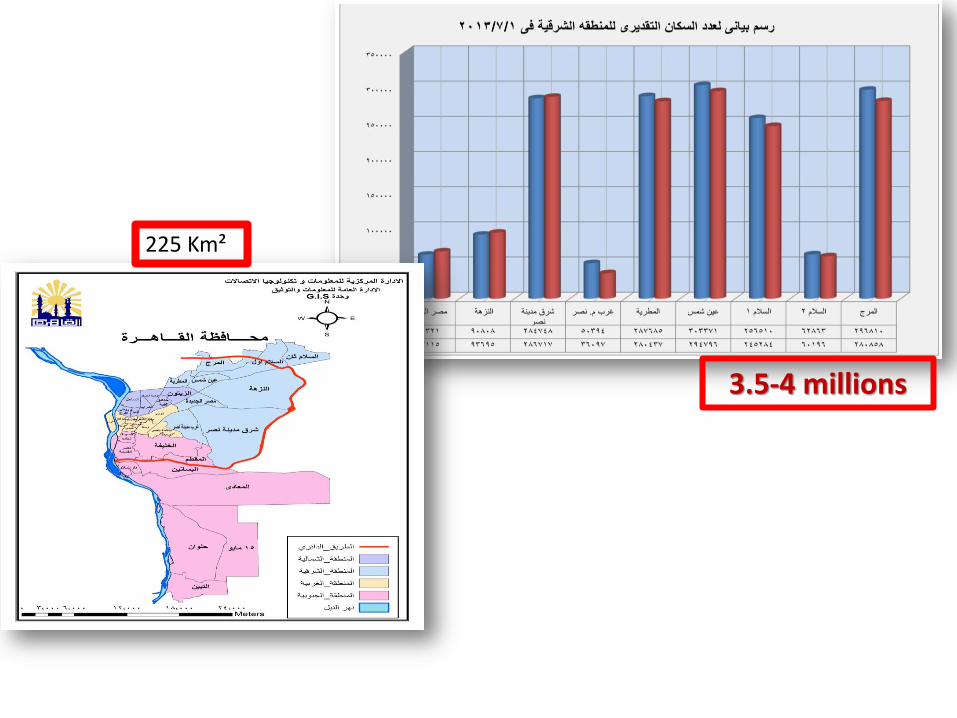
3.5-4 millions
225 Km²
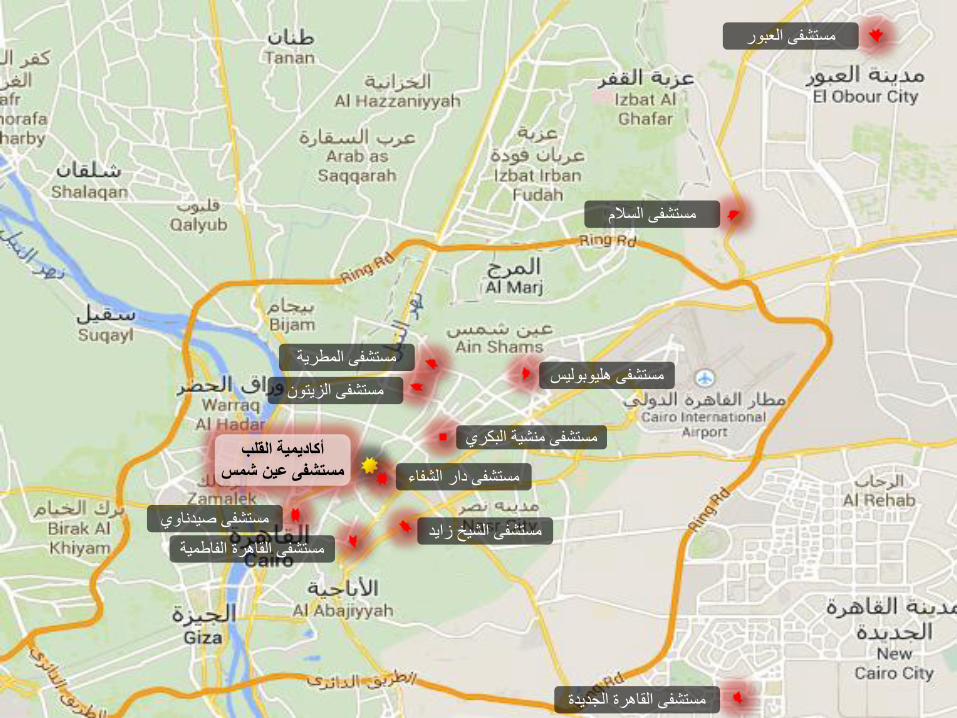
أكاديمية القلب مستشفى عين شمس
مستشفى صيدناوي مستشفى الشيخ زايد
مستشفى القاهرة الفاطمية
مستشفى دار الشفاء
مستشفى منشية البكري
مستشفى هليوبوليس مستشفى الزيتون
مستشفى المطرية
مستشفى السالم
مستشفى العبور
مستشفى القاهرة الجديدة
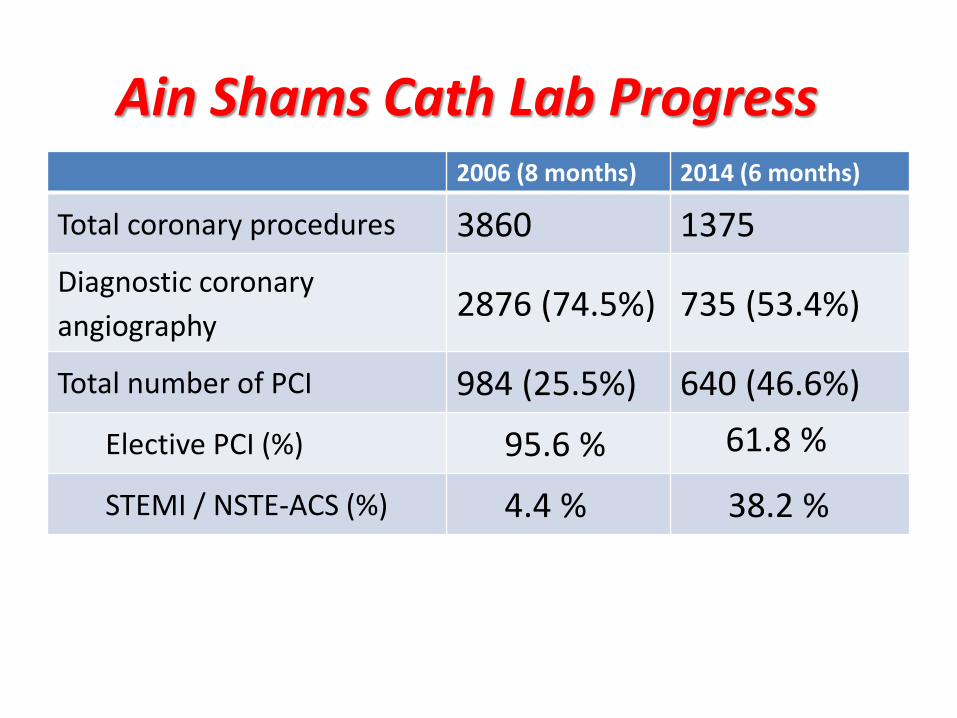
2006 (8 months) 2014 (6 months)
Total coronary procedures 3860 1375
Diagnostic coronary
angiography 2876 (74.5%) 735 (53.4%)
Total number of PCI 984 (25.5%) 640 (46.6%)
Elective PCI (%) 95.6 % 61.8 %
STEMI / NSTE-ACS (%) 4.4 % 38.2 %
Ain Shams Cath Lab Progress

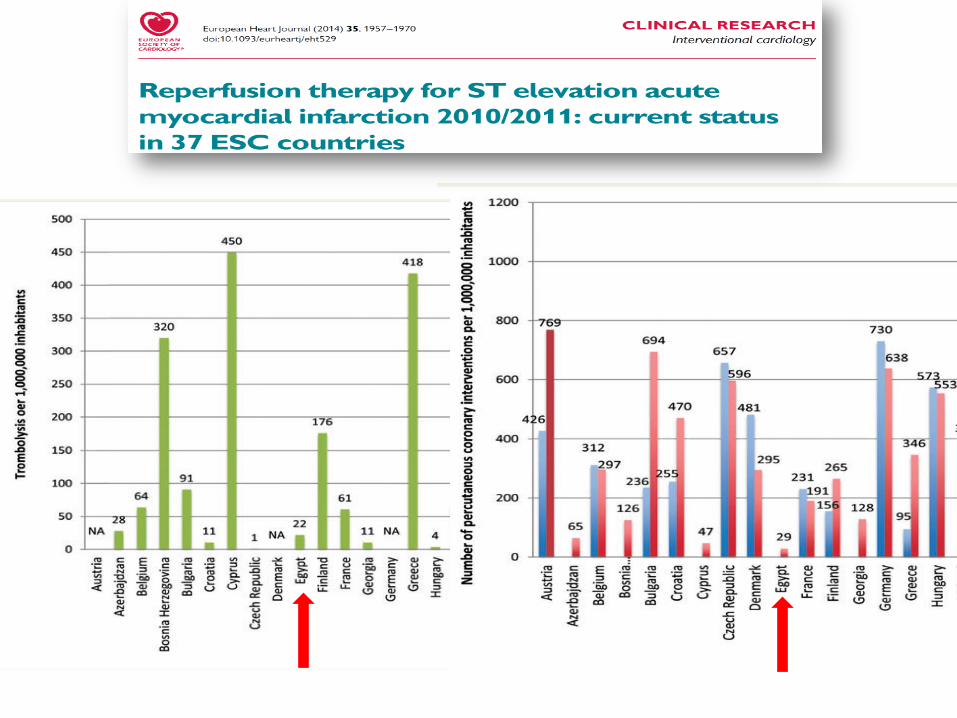
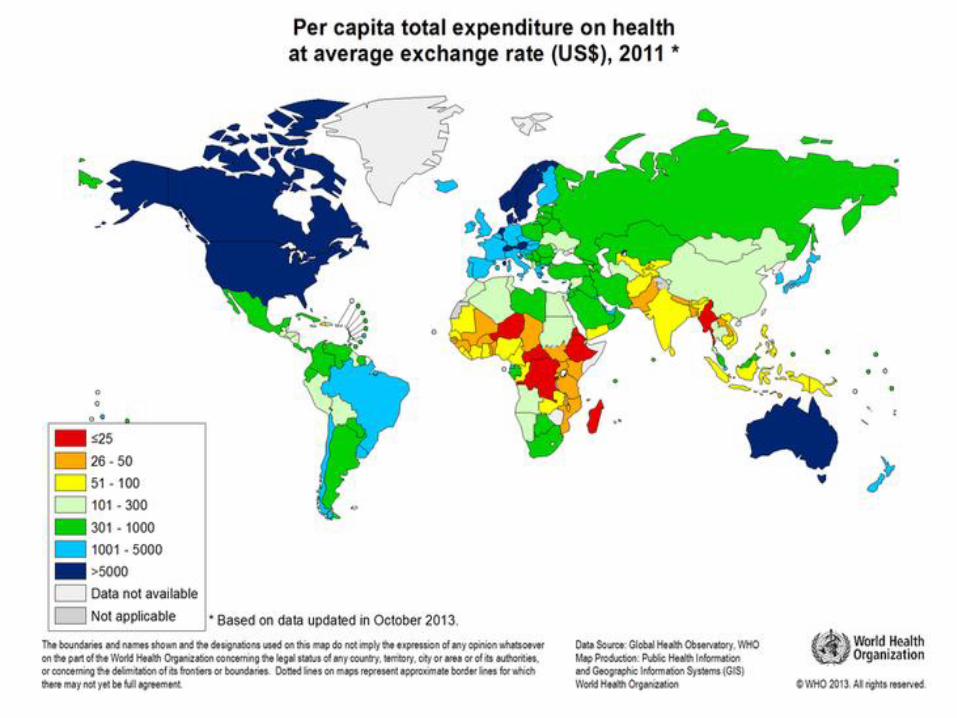
Egypt=64
A major difference between developed and developing countries is the amount of resources devoted to CVD care. For example, there is about a fifty fold difference in what the United States and South Africa spends on CVD care.
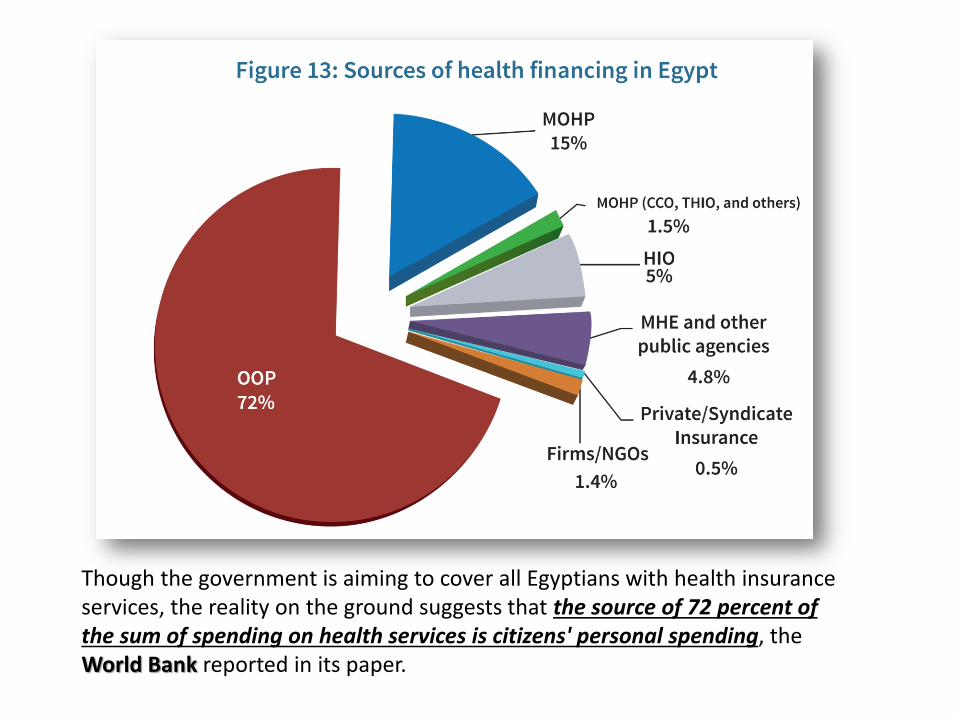
Though the government is aiming to cover all Egyptians with health insurance services, the reality on the ground suggests that the source of 72 percent of the sum of spending on health services is citizens' personal spending, the World Bank reported in its paper.
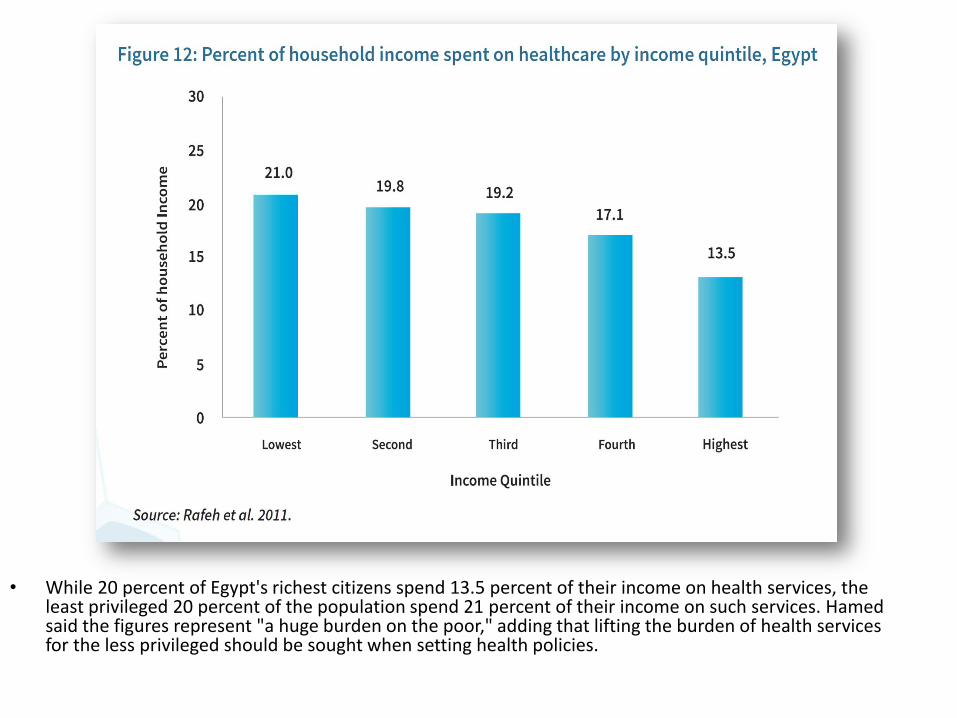
• While 20 percent of Egypt's richest citizens spend 13.5 percent of their income on health services, the least privileged 20 percent of the population spend 21 percent of their income on such services. Hamed said the figures represent "a huge burden on the poor," adding that lifting the burden of health services for the less privileged should be sought when setting health policies.
ADDRESSING NCDS in EGYPT
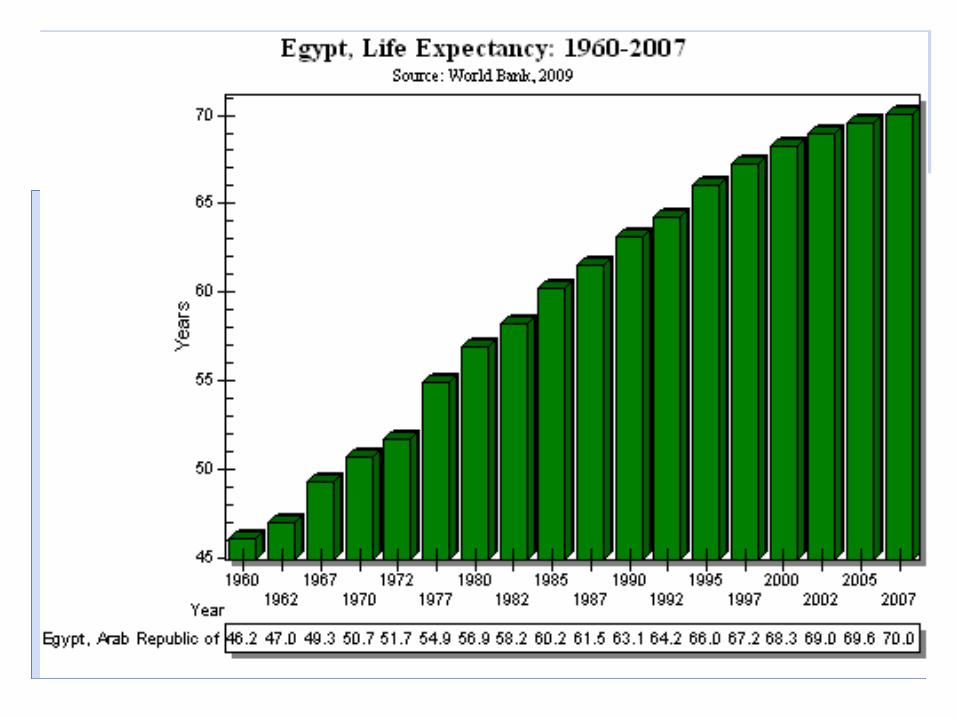
• Despite an improvement in Egyptians' health during the past 20 years noted by the World Bank and represented in an increase in life expectancy from 64.5 years to 70.5 years, such an improvement was not achieved with equality.
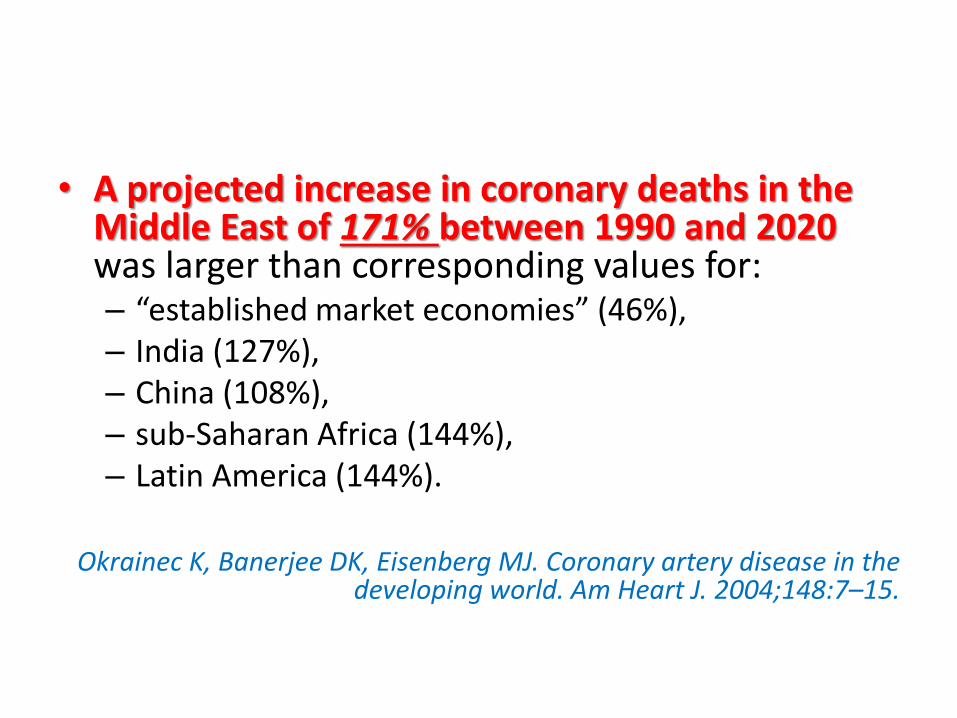
• A projected increase in coronary deaths in the Middle East of 171% between 1990 and 2020 was larger than corresponding values for: – “established market economies” (46%), – India (127%), – China (108%), – sub-Saharan Africa (144%), – Latin America (144%).
Okrainec K, Banerjee DK, Eisenberg MJ. Coronary artery disease in the
developing world. Am Heart J. 2004;148:7–15.
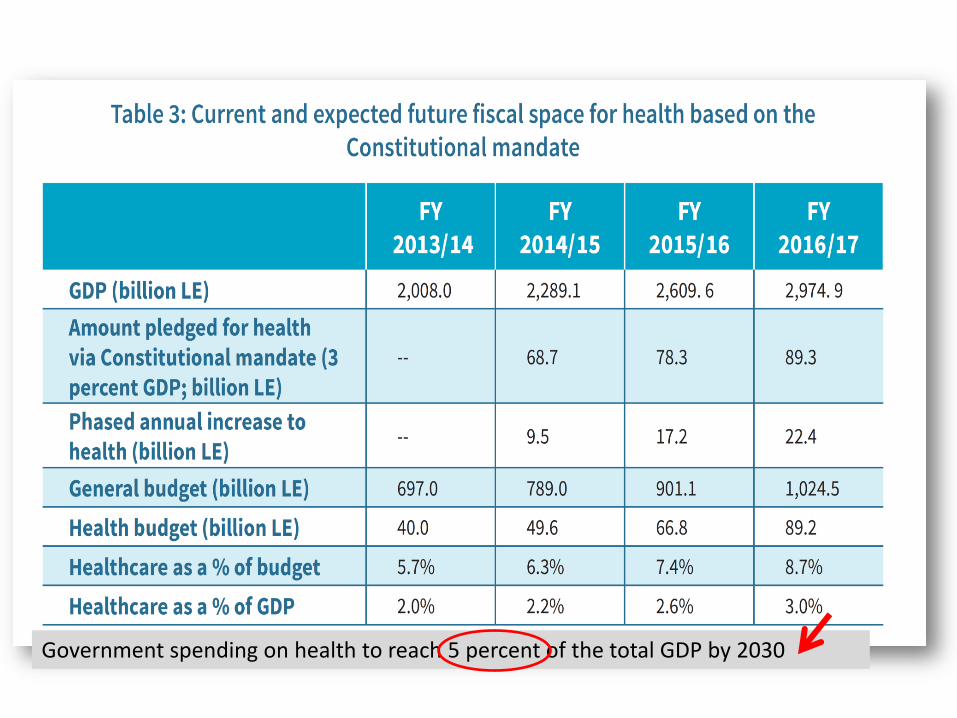
Government spending on health to reach 5 percent of the total GDP by 2030
CONCLUSION
• Egypt is undergoing an epidemiological transition as it faces a dual disease burden
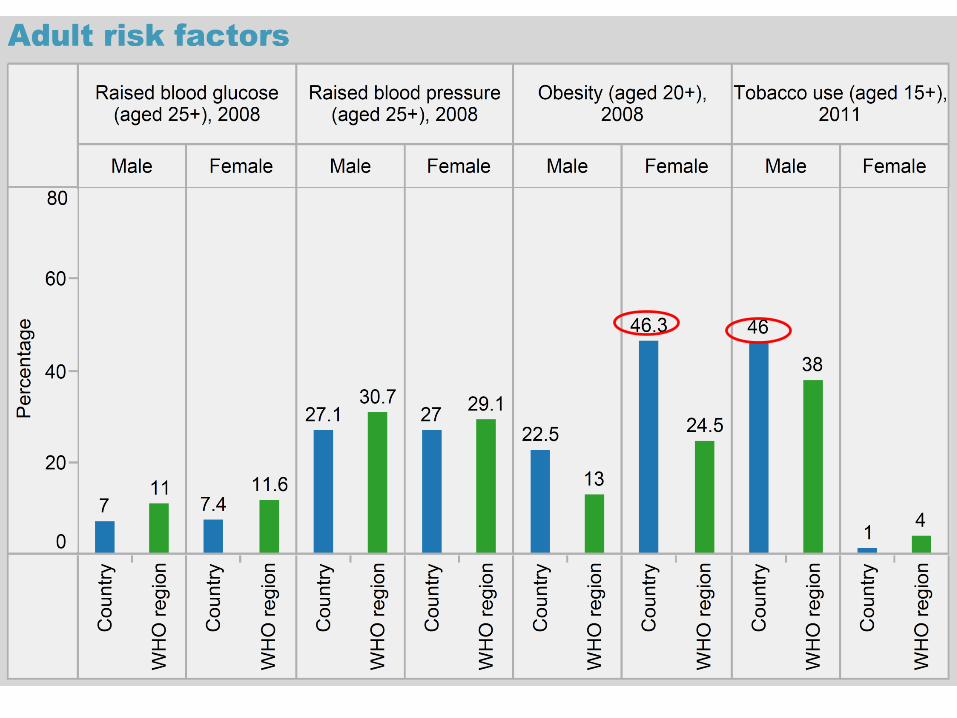
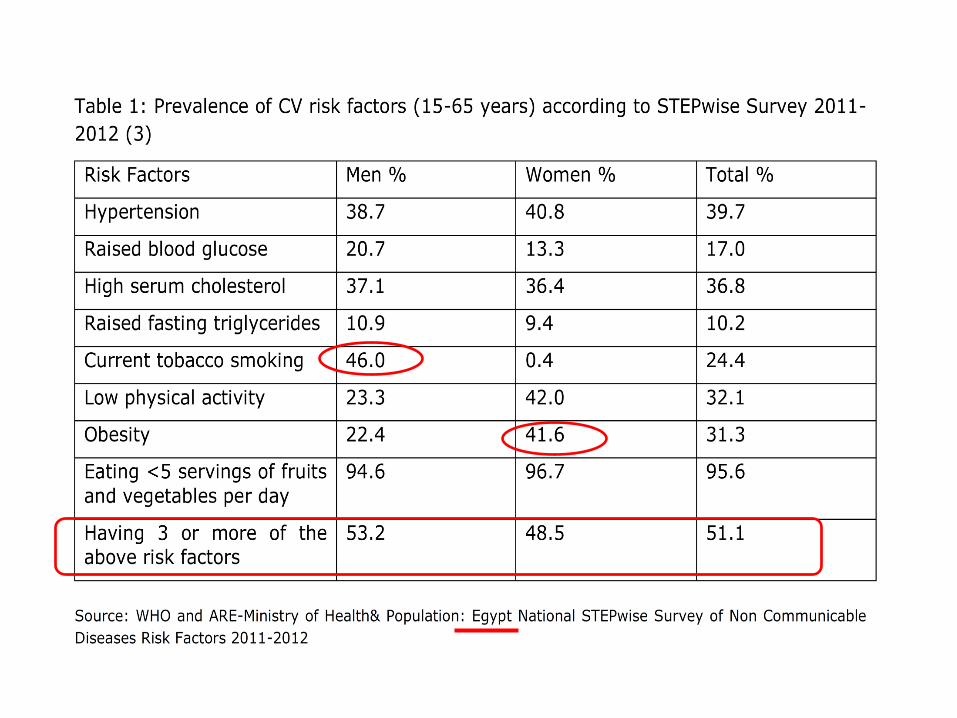
• Egypt has a high prevalence of CAD risk factors especially tobacco use and obesity
• CAD is affecting younger patients in Egypt • Despite several gains in healthcare in previous
decades, Egypt has much to do in terms of prevention and management of CAD
• Egypt is still to ensure that social justice is realized in healthcare.