Embed Size (px)
Citation preview

THE CARBOHYDRATE TOLERANCE IN CANCER PATIENTS, AND T H E EFFECT UPON I T OF ROENTGEN
RAY RADIATION
F. H. L. TAYLOR, PH.D., AND HENRY JACKSON, JR., M.D.
(Front tlae Pondville Hospital and the Thorndike Memorial Laboratory, the Second and Bourth
of Medicine, Harvard Medical School) Medical Services (Harvard) of the Boston City Hospital, and the Departmmt
There has been much investigation of the carbohydrate metabolism in malignant disease since Warburg’s (1) first publication on this subject. This author showed, and his work has since been confirmed, that a considerable increase in the utilization of glucose occurs in malignant tissue. Cori and Cori (2) have also shown by studies of lactic acid production an abnormal carbohydrate metabolism. Because of Warburg’s findings, it has been expected that in malignant disease the organism as a whole might show an abnormal carbohydrate metabo- lism. Investigations by various authors have brought forward some- what contradictory evidence.
Basing their conclusions on the return of the blood sugar content to a normal value in ninety minutes after the ingestion of 50 gm. of glucose, Slosse and Reding (3) stated that cancer patients have a diminished tolerance for carbohydrate, and Beregoff (4) arrives at the same conclusion. The presence of such diminished carbohydrate tol- erance, when occurring simultaneausly with an alkalosis, the latter author considers of diagnostic significance. Studies conducted simul- taneously on the ionized calcium and the sugar tolerance show, in the opinion of this author, an interrelationship between the level of the calcium ion and the carbohydrate metabolism.
Enocksson ( 5 ) found abnormal prolongation and elevation of the sugar curve following glucose administration in advanced cases of gastric cancer. He ascribed some diagnostic importance to this find- ing, but pointed out that equally marked disturbances may be found in other diseases resulting in cachexia.
Benso (6) found that in patients suffering from malignant disease hyperglycemia reached a higher level more quickly and decreased more slowly than in normal individuals. Following extirpation of the tumor, this author claims, the tolerance curves approach a more normal value. He also states that a return to normal tolerance for carbohydrates follows radium treatment, but he did not observe such an effect after roentgen therapy.
Romanin (7) found the rising part of the sugar tolerance curve to be normal in patients with cancer, while there existed a marked prolon- gation of the curve. This finding he interpreted as of diagnostic importance, although similar curves are obtained from patients suffer-
1 The expenses of this investigation were defrayed, in part, by a @ft to the Harvard Medical School from the Smith, Kline and French Laboratories, Philadelphia.
536

T H E CARBOHYDRATE TOLERANCE IN CANCER PATIENTS 537
ing from other diseases. Hueper, Woodward and F r y (8) found a hyperglycemia in the majority of their cases of malignant disease.
In contradistinction to these findings, DeNiord (9) and his co- workers present data showing a lowered sugar tolerance in only about one-third of their cancer cases. The altered carbohydrate metabolism is of no diagnostic significance in the opinion of these investigators. No significant changes in the carbohydrate metabolism were observed by these authors during or after roentgen ray therapy. Moreover, Pena (10) in a study of 258 cancer patients found a sugar tolerance curve similar to that encountered in normal human subjects. He did not find that the site of the tumor or its histological type bore any rela- tionship to the sugar tolerance of cancer patients. He did observe. however, a lowering of the carbohydrate tolerance as the disease pro- gressed towards the terminal stage.
The present investigation was undertaken to determine further the incidence of a lowered carbohydrate metabolism in cancer and to study the relationship, if any, of the blood calcium to the carbohydrate tolerance in cancer patients.
EXPERIMENTAL
Thirty-five patients suffering from various forms of carcinoma were studied. In each case the diagnosis was confirmed by biopsy or the malignant condition had developed to such an extent that no reasonable doubt of its nature was possible. Each patient was treated with a known dosage of roentgen-rays, a full suberythema dose being admin- istered. The voltage used was 220 kv. Sugar tolerance curves were obtained in the usual way, usiiig the improved Folin (11) micro pro- cedure. One hundred grams of glucose was used as the test meal. While the general consensus of opinion is that this amount of glucose is too great, it was, nevertheless, necessary to use this amount if results were to be compared satisfactorily with those of other investigators, the great majority of whom have used this amount of glucose. Of the original 35 patients, 27 were studied before and after x-ray treatment, and in 16 cases the study was completed by a third curve one to three months later. Distance from the clinic or death accounted for failure to obtain second and third curves on all the patients studied,
Blood calcium determinations were made simultaneously with the sugar tolerance curves on 15 patients. The blood calcium was deter- mined according to an unpublished method of Dr. Cyrus H. Fiske (12).
A complete rQsum6 of the studies on 27 patients is given in Table I. Eight patients on whom only one curve was obtained were not included in this table, but were used in determining the incidence for lowered carbohydrate tolerance in cancer patients.
Contrary t o the findings of many authors, but in agreement with DeNiord, a decreased tolerance for glucose was found in only one-third of the entire group of 35 patients prior to roentgen radiation. It is of interest that, with the exception of one patient with carcinoma of the

-
-
No.
-
2984
2541
2933
31M
302f
192t
2771
299s
30%
-
64
69
72
49
64
62
55
60
80
-
9.70
10.40
9.70
7.25
-
10.70
10.70
7.60
10.60
TA
BL
E I
(Per
iod I
= B
efor
e x-ray.
Perio
d 11
= Im
med
iate
ly a
fter
x-ray.
Perio
d I1
1 =
One
to three m
onth
s lat
er)
Car
cino
ma.
low
er
jaw
, Gr.
I
Car
cino
ma.
tong
ue,
Gr.
I
Car
cino
ma,
pro
stat
e
Car
cino
ma.
bre
asts
Car
cino
ma.
floor o
f m
outh
Car
cino
ma,
cervix,
Cla
ss C
. I. D
.
Car
cino
ma.
rec
tum
Car
cino
ma.
jaw
Car
cino
ma,
epi
glot
- ti
s, w
ith
neck
m
etas
tase
s
-
-
Dur
a-
tion
10 m
o.
11 y
r.
19 m
o
1 Yr.
-12
mo
2 yr
.
1 yr
.
3 yr.
5 m
a
-
+ + 0 + + 0 + 0 0
- D
etai
ls of R
.adil!-
tion
(r u
nite
in
air)
600
to le
ft n
eck
400
to r
ight
nec
k
1200 to
righ
t an
d le
ft neck
800
to a
nt. p
elvi
s 800
to p
ost.
pelv
is
1200 to
post
. che
st
1600 to
left
nec
k 1600 to
rig
ht n
eck
1200 to
ant.
pel
vis
1200 to
pos
t. pe
lvis
1200 to
ant.
pel
vis
1200 to
pm
t. pe
lvie
1200 to le
ft n
eck
anc
face
; 120
0 to
righ
t ne
ck. n
one to f
ace
(320 m
ch. r
adiu
m
3 mo.
prev
ious
ly)
850 to ri
ght
neck
20
0 to
left
nec
k
Clin
ical
Res
pons
e to
Rad
iatio
n
Dis
tinc
t 10-1
im
- pr
ovem
ent
Goo
d
No
mar
ked
im-
prov
emen
t
Sli
ght i
mpr
ove-
m
ent
Tem
pora
ry 1
04
impr
ovem
ent
Goo
d
Del
irit
e im
prov
e-
men
t
No
impr
ovem
ent
No
impr
ovem
ent
-
-
Pe-
,iod
-
I I1
111 I I1
111 I I1
111 I I1
111 I I1
111 I I1
111 I I1
111 I I1
111 I I1
111 -
Mg. G
luco
se per 100
m
l. bl
ood
-
&$
-
95
100
100 80
LO8
LOO 85
90
95
80
70
90
95
111 78
90
100 90
so
95
70
78
105 76
90
95
- -
?4
hr.
230
144
230
137
137
150
157
145
174
152
152
164
156
190
129
130
127
250
164
150
160
205
160
-
-
-
210
- -
1 hr.
200
144
190
100
117
132
150
145
165
107
130
123
156
185
103
200
118
115
m
150
118
118
204
110
-
200
145
- -
2 hr.
154
123
132 98
112
117
130
124
118 95
117 98
131
177
100
185
112
100
129
140 90
115
194
105
-
193
130
- -
3 hr.
143
120
130 75
110
102
123
115
113 88
100 95
117
117 97
157
112 97
111 90
85
100
133 80
-
167
120
-
Inte
rpre
tati
on o
f S
wr
Tol
eran
ce
curv
e4
Low
ered
tol
eran
oe
Pra
ctic
ally
nor
mal
L
ower
ed t
oler
ance
Nor
mal
N
orm
al
Nor
mal
Nor
mal
N
orm
al
Nor
mal
Nor
mal
N
orm
al
Nor
mal
Nor
mal
L
ower
ed t
oler
ance
N
orm
al
Low
ered
tole
ranc
e N
orm
al
Nor
mal
Low
ered
tol
eran
ce
Nor
mal
N
orm
al
Nor
mal
L
ower
ed t
oler
ance
Sl
ight
ly lo
wer
ed
tole
nrnc
e
Low
ered
tol
eran
ce
Slig
htly
low
ered
to
lera
nce
Die
d
Bio
psy
Car
cino
ma.
Gr.
I1
Epi
derm
oid
carc
i-
nom
a. G
r. I;
orig
in
papi
llom
a
Non
e
Non
e
Car
cino
ma,
epi
- de
rmoi
d. G
r. I1
Non
e
Non
e
Epi
derm
oid
carc
i- no
ma,
Gr. I1
Epi
derm
oid
carc
i-
nom
a, G
r. I
1
(Tab
le c
ont.
on p
. 54
0)

THE CARBOHYDRATE TOLERANCE IN CANCER PATIENTS 539
cervix of two years ' standing (No. 1926), all of the patients who showed a lowered sugar tolerance prior to radiation had either lost a consid- erable amount of weight or had malignant disease of the gastro-intes- tinal tract or oral cavity. It will also be noted that with three excep- tions the patients showing a lowered tolerance were above fifty-five years of age.
The data were analyzed in an attempt to discover the bearing of a lowered carbohydrate tolerance on the final outcome of the disease. The effect, if any, of roentgen radiation on both the lowered and the normal sugar tolerance in cancer patients was studied and so fa r as possible the cause of the lowered carbohydrate tolerance occurring in some patients was investigated.
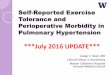
There appeared to be no consistent effect of roentgen radiation on the tolerance of a cancer patient for glucose. Sixteen patients had a
' 0 1 2 3
TIME I N HOUR8
FIG. 1. COMPOSITE CURVE OF NINE C A N C F ~ PATIENTS WITH NORMAL SUGAR TOLERANCE ORIQINALLT
0- 0 Control period 0 - - - - - 0 Immediately after roentgen therapy 0-0 One to three months later
normal tolerance for glucose before x-ray treatment (Period I). Nine or 56 per cent of these maintained a normal curve after x-ray treatment (Period 11), while in 7 or 44 per cent a slightly lowered tolerance developed. I n 9 of the 16 patients having a normal tolerance to glucose before radiation, a third curve (Period 111) was obtained one to three months later. A composite graph derived from the averages of the sugar content of the blood for the three periods of study in these nine individuals is given in Fig. 1. It will be observed, from this figure, that roentgen radiation had no marked effect on the sugar tolerance in cancer patients when the tolerance curve was normal before the institution of therapy.
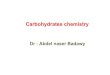
Eleven of the patients included in Table I had before roentgen radiation a lowered carbohydrate tolerance. Of these, 63 per cent showed a noticeable increase in tolerance for glucose after treatment by roentgen rays. Seven of the 11 patients were studied one to three months after radiation. Fig. 2 is a composite graph based on averages

TA
BL
E I (Continual)
Pe-
riod
I1
1x1 I1
I11 I I1
I11 I I1
1x1 I I1
111 I I1
111 I I1
111 I I1
I11 I I1
1x1
No.
-
3102
2212
1061
4119
z 0 3
m
3928
3207
2959
3754
-
-
Fsg
t mg
I8
0
60
I8
0
55
80
65
80
105
100
100
137
137
115
115
loo
100 70
75
--
loo 90
Age
&
earn
:
-
51
79
65
71
31
61
75
74
67
-
87
60
100
100
100
Dia
gnos
is
Nor
mal
N
orm
al
Low
ered
tole
ranc
e Sl
ight
ly lo
wer
ed
tole
ranc
e
2arc
inom
a. b
ucca
l m
ucoe
a
85
100
105
3arc
inom
a. lo
wer
li
p
2arc
inom
a. re
ctum
N
orm
al
Slig
htly
low
ered
Nor
mal
to
lera
nce
Zar
cino
ma.
buc
cal
muc
oea
105
105
140
185
123
122 98
115 75
85
115
110
2arc
inom
a, re
ctum
Nor
mal
L
ower
ed to
lera
nce
Nor
mal
Sl
ight
ly lo
wer
ed
Nor
mal
N
orm
al
Nor
mal
N
orm
al
Nor
mal
N
orm
al
Low
ered
tol
eran
ce
Sli
ihtl
y lo
wer
ed
Die
d
tole
ranc
e
tole
ranc
e
2arc
inom
a. lo
wer
lip
met
asta
tic
to
lym
ph n
odes
noma.
left
sca
pu-
lar
regi
on
nom
a, li
p
Zpi
dcrm
oid
carc
i-
Epi
derm
oid
earc
i-
>arc
inom
a. pr
osta
te
Dur
a-
tion
3 m
o.
6 m
o.
2 yr
.
1 yr
.
6 w
k.
3 m
o.
18 m
o.
0 m
o.
7 m
o.
aeg
O!
Weig
b
-
+ + + + 0
0
0
0 4-
Det
aib
of R
Bdi
F
tion
(r m
ta i
n an
)
800
to l
eft
face
So
me
radi
um 2 m
o.
prev
ious
ly
1200 to
laio
n in
jam
(r
adiu
m 357
mch
3
mo.
pre
viou
sly)
1200 to
post
. pe
lvh
1200 to
ant
. pel
vis
1200 to
righ
t an
d le
ft n
eck
1200 t
o p
ost.
pelv
if
to a
nt. p
elvi
s
to le
ft n
eck
400
to r
ight
nec
k
2400
to l
eft s
capu
- la
r re
gion
1600 to
left
nec
k 1400 to
rig
ht n
eck
loo0 to
low
er d
orsa
l sp
me
Clin
ical
Res
pone
e to
Rsd
ist1
on
No
impr
ovem
ent
No
impr
ovem
ent
No
mar
ked
im-
prov
emen
t
Slig
ht or no im
- pr
ovem
ent
Slig
ht o
r no im
- pr
ovem
ent
No
impr
ovem
ent
No
impr
ovem
ent
Goo
d
Slig
ht o
r no im
- pr
ovem
ent
1 M
g.
Glu
cose
per 100
1 d. bloo
d -
M
hr.
120 70
210
145
210
133
152
155
120
167
200
220
188
136
113
190
-
152
125
215
148
-
-
1 hr.
100 64
208
108
198 90
140
140
120
165
-
165
215
168
130
108
152
130
118
215
148
-
2 hr. 95
64
140
105
150 85
125
120
108
162
-
157
192
125
125
108
124 87
100
213
148
Inte
rpre
tati
on o
f Sugar
Tol
eran
ce
3 br.
Bio
psy
Epi
derm
oid
carc
i-
nom
a. G
r. I
Non
e
Ade
noea
rcin
oma.
re
ctum
Nec
ropa
y co
nfir
ma
epid
erm
oid
csrc
i- no
m8.
Gr.
I1
Ade
noca
rcin
oma.
G
r. 1
11
Non
e
Epi
derm
oid
aarc
i- no
ma.
GI. I
Epi
derm
oid
Nec
ropy
(m
icro
- m
op.=
). ad
eno-
ca
rcm
oma.
pro
s-
tate
(Tab
le c
ont. OR p
. 543)

THE CARBOHYDRATE TOLERANCE IN CANCER PATIENTS 54 1
of the values obtained in these 7 patients. On the whole, the suc- cessive curves show a tendency towards an increased tolerance for carbohydrate.
Seven of the 10 patients not studied a third time were dead six months after the initial investigation. Five of these 7 patients had previously a normal carbohydrate tolerance. Of the patients who lived long enough for the final tolerance curve to be obtained, none showed an improvement in tolerance for carbohydrate when a lowered tolerance for glucose was originally present. It would seem impos- sible, from a consideration of the carbohydrate tolerance in period one, to determine how long the patient would survive. A progressive de- crease of tolerance for carbohydrate would be a distinctly unfavorable sign, but thc presence or absence of a lowered tolerance for glucose before or after treatment does not offer an aid to prognosis.
I 2 3
TIME IN HOURS
FIG. 2. CONPOSITE CURVE OF SEVEN CANCER PATIENTS WITH A DECREASED SUGAR TOLERANCE ORIQINALLY
0- 0 Control period 0 - - - - - 0 .----. Immcdiately after roeiitgeii therapy
One to three months later
From a study of the data obtained from sugar tolerance curves one to three months after treatment by x-ray, some interesting facts emerge. More than 75 per cent of those patients presenting a lowered tolerance for glucose at this time had shown the same abnormality prior to roentgen therapy. Clinical improvement following radiation does not appear to change the picture. Of the patients in whom radiation brough about clinical improvement, two-thirds had a normal carbohy- drate tolerance prior to treatment, and the same incidence appears in those patients in whom radiation brought about no clinical improve- ment.
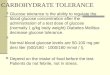
Four typcs of abnormal glucosc tolerance curves were encountered during the investigation. No one type could be considered predomi- nantly characteristic of malignant clisease. These types are shown in Fig. 3.

Tas
m I
(C
ontin
ued)
pets
ils o
f R
adia
- ti
on (
r un
ita in
air)
1400
to a
nt. p
elvi
s 14
00 to
post
. pe
lvis
1600
.to a
nt. s
tern
al
regi
on
1400
to
left
neck
lo00
to a
nt. p
elve
lo
00 to
pos
t. pe
lvls
No.
C
linic
al Re
aponrre
to R
adia
tion
Exc
elle
nt
No m
arke
d im
- pr
ovem
ent
Fair
res
pons
e
No
impr
ovem
ent
3819
3967
3822
3169
en * I9
3955
3671
3913
3800
3658
-
Fast
- m
g
loo
115
135 90
90
140
140
173 85
lo(!
10
0 90
90
140 85
68
115 90
150 95
95
95
82
100
59
72
70
63
56
79
78
67
70
-
?4
hr.
--
-
-
183
205
134
205
200
210
210
125
125
185
128
190
150
160
212
154
194
295
235
275
135
90200
122
8.90
-
-
7.78
-
8.03
-
-
8.50
1200
to le
ft b
reas
t 12
00 to
left
axi
lls
1600
to ri
ght f
acc
Dur
a-
tion
Goo
d re
apon
se
Gra
dual
impr
ove-
m
ent
Car
cino
ma,
cer
vix,
C
lsss
B.
Gr.
I1
1500
to
left
neck
1500
to
righ
t ncc
k
2400
to
righ
t neck
Rad
ium
652m
ch.
and
chin
and
chin
Car
cino
m~.
esop
h-
agus
Loc
al im
prov
e-
men
t
Slig
ht im
prov
e-
men
t
Car
cino
ma.
left
pa
rotid
gla
nd
Cw
3nom
a, to
nsil
Car
cino
ma,
pro
stat
e
Car
cino
ma,
cer
vix
2 w
k.
1 yr.
Car
cino
ma,
bre
ast
1!XW
to p
ost
. pe
l+
1200
to
ant.
pel-
3960 m
ch. r
adiu
m
1 m
onth
bef
ore)
6 m
o.
6 w
k.
4r
8 m
o.
3 yr
. K.i.
8 m
o.
Goo
d re
spon
se
Car
cino
ma,
buc
cal
2 yr.
mu-
I
Car
cino
ma,
Boo
r of
mou
th
5 m
o.
Lose
of
wei
gh1
+ + 0 + + + 0 0 0
-
-
Pe-
riod
-
I I1
111 I I1
111 I I1
111 I I1
I11 I I1
111 I I1
III I I1
I11 I I1
111 I I1
I11 -
Mg.
Glu
cose
per
100
m
l. bl
ood
-
1 hr.
125
168
163
195
125
185
200
200
148
110
110
145
128
165
140
150
200
148
205
197
197
242
125
167
114
-
- -
2 hr.
123
1.54
163
157
118
-
170
160
200
130
106
106
127
123
166
125
150
155
125
155
177
177
217
115
137
108 - -
3 hr.
115
133
135
105
105
-
145
150
175
110
102
102 92
113
166
100
150
137
100
135
125
175
135 90
125
Inte
rpre
tatio
n of
Suga
r Tolerance
curv
es
Low
ered
tole
ranc
e N
orm
al
Die
d
Low
ered
tol
eran
ce
Low
ered
tol
eran
ce
Low
ered
tol
eran
ce
Slightly l
ower
ed
tole
ranc
e N
orm
al
(not o
ount
ed)
Nor
mal
N
orm
al
Slin
fitIY
ione
red
tder
once
Nor
mal
Lo
wer
ed to
lera
nce
Low
ered
tole
rane
e Lo
wer
ed
Nor
mal
to
lera
nce
Low
ered
tole
ranc
e Lo
wer
ed to
lera
nce
Low
ered
tole
ranc
e
Npr
mal
S
Ilgh
tIy lo
wer
ed
Nor
mal
tv
lera
ncs
Bio
pey
Epi
derm
oid
carc
i-
nom
a, C
law
B. G
r. I1
Non
e
Car
cino
ma,
typeIlI.
Has
had
his
tory
of
carc
inom
a fo
r 4 y
r.
P.I
. 8 m
onth
s
Adc
noca
rcin
oma
Car
cino
ma simplex.
(sci
rrhu
a) p
apil-
lo
ma
Non
e
Papi
llom
a
Epi
derm
oid carci-
nom
a, Gr. I1
Non
e

T H E CARBOHYDRATE TOLERANCE IN CANCER PATIENTS 543
Six patients had a lowered tolerance for glucose, giving a high maximum in thirty minutes but returning to a normal value within three hours (Fig. 3, Group A). Five patients showed a lowered tol- erance for glucose, giving a high maximum but failing to return to a normal value in three hours (Group B). In 6 patients only a normal elevation of the blood sugar occurred, but the blood sugar level failed to return to normal in three hours (Group C). In 4 patients a plateau appeared (Group D). While it is not particularly safe to ascribe any particular type of sugar tolerance curve to any definite disease, the general consensus of opinion would attribute Groups A and B to con- ditions generally associated with malnutrition and cachexia, while groups C and D are generally considered (13, 14, 15, 16) to occur in
a Y 0.
Y
3 3 -I u f a
GROUP A
300-
GROUP A 300
i
I 2 3 L I
I 2 3
J = 0 0
o! c
L I 8 3
CROUP c 300
200 -. tOQ
I 2 3 TIME I N HOURS
QROUP I 3001 1
TIME I N HOURS
FIQ. 3. T Y m s OF ABNORMALITIES I N 8UQAR TOLERANCE CURVEB ENCOUNTERED I N CANCEn PATIENTS
patients showing a poor absorption of glucose from the gastro-intestinal tract. There is no question, also, that some of the prolongation of the curves found in this series, and by other workers, may be due to the effect (17, 18, 19, 20) of an excessive amount of glucose used in the test meal. Consideration of this fact was given in the interpre- tation of normal and lowered tolerance in this study. It was generally found that when a hyperglycemia was present originally, the sugar values fell, not necessarily to the original value but to a more normal value. A high percentage of such abnormalities as shown by groups A and B is not inconsistent with the loss of body weight and appetite so characteristic of advanced malignant disease. The occurrence of a large number of plateau curves in the period immediately after roentgen treatment may be accounted for by gastro-intestinal dis- turbances due to roentgen-ray sickness in the patients a t this period.

544 F. H. L. TAYLOR AND HENRY JACKSON
It has been previously shown (21) that a hypocalcemia occurs in a certain number of cancer patients and that roentgen radiation had no effect on the level of the blood serum calcium. As has been men- tioned previously, a lowered blood serum calcium has been considered by some authors to be linked in some way to a lowered sugar t,olerance. In an attempt to discover if such a relationship exists, simultaneous calcium and sugar tolerance determinations were made on 15 patients. The serum calcium values taken before, during, and some months after x-ray treatment were averaged. This average figure is given in Table I. In confirmation of a previous report (loc. cit.) one notes that a hypocalcemia occurred in only 34 per cent of the 15 patients.
Examination of the data obtained on those patients in whom a normal sugar tolerance existed shows an average calcium value of 9.3 mg. per 100 ml. of blood serum. The extremes encountered were 7.25 and 10.50 mg. of calcium per 100 ml. of blood serum. In those patients showing a decreased tolerance for glucose the average calcium value was 9.84 mg. per 100 ml. of blood serum, the extremes being 7.78 and 10.50 mg. per 100 ml. Definite hypocalcemia was found to be present in 30 per cent of patients having a normal carbohydrate tolerance and in 28 per cent of those having a decreased tolerance. No direct relationship, therefore, seems to exist between the sugar tolerance in cancer patients and the level of the total serum calcium.
DISCUSSION On the basis of the foregoing experimental evidence there seems to
be no direct relationship between a decreased sugar tolerance and cancer per se. There is some evidence that the decreased tolerance for carbohydrate encountered in about one-third of the patients studied was due in part to the general malnutrition and cachexia commonly found in cancer. Some patients with a lowered sugar tolerance had definite involvement of the gastro-intestinal tract. Even in those patients where a lowered sugar tolerance was found, as determined by the usual criteria, it was not certain that such decreased tolerance curves were not due to delayed utilization of glucose caused by the large amount of this material ingested. It is interesting that, while no one type of tolerance curve was characteristic of the disease, yet most, of the abnormalities found were consistent with the types found following the feeding of carbohydrate in non-diabetic patients suffering from starvation or malnutrition. It is, of course, appreciated that involvement of certain specialized areas such as the pancreas, the para- thyroids, and the hypophysis by malignant disease may alter the tol- erance curve entirely (22). Some of the curves which have been considered normal show some elevation above the base line after three hours. As stated above, we have borne in mind that with an original hypoglycemia the return of the sugar level to a normal value, even if this value is above the original base line, is not indicative of an ab- normal sugar tolerance. We have in the interpretation of curves con-

THE CARBOHYDRATE TOLERANCE IN CANCER PATIENTS 545
sidered the hyperglycemia produced and the duration of this hyper- glycemia above a normal figure. Recognition of the reported effect of age on the glucose tolerance (23) has been made. All except two of the patients were over fifty and most were over sixty years of age. It is believed that in comparative studies of glucose tolerance the individuals sliould be in the same general age group.
In short, it was found that about one-third of the patients studied show a lowered tolerance for glucose, the presence of which was not inconsistent with the malnutrition accompanying the malignant state. This relationship may be further modified when one considers the in- cidence of a lowered glucose tolerance in non-diabetic persons between fifty-five and seventy years of age. It seems rather difficult to account for a lowered carbohydrate tolerance in cancer in terms of Warburg’s theory. The presence of an actively growing malignant tissue having a high rate of carbohydrate utilization would tend to cause a more rapid, and not a less rapid removal of carbohydrate from the blood stream.
The lack of direct relationship between cancer and the sugar toler- ance of individuals was still further shown by a consideration of the effect of roentgen radiation. Radiation by roentgen rays did not pro- duce any marked changes in the carbohydrate metabolism. When the tolerance for glucose was normal a t the outset, over half of the patients studied showed an unchanged sugar tolerance following roentgen ray treatment. Of those patients who did show a change, the same number showed a trend toward normal as showed a further decrease in toler- ance for glucose. There was, however, a tendency among patients originally possessing a lowered tolerance for glucose for the tolerance curves to become more normal. In this connection i t is noteworthy that Lennox (24) has shown that with marked abnormality of sugar tolerance, repeated tests, even after considerable intervals of time, produce tolerance curves which are somewhat flatter and more close to normal.
It was found impossible to predict from an analysis of initial sugar tolerance curves whether the outcome would be favorable or unfavor- able. In patients who originally showed a normal tolerance for car- bohydrate, the development of a progressively decreasing tolerance strongly indicated an unfavorable prognosis.
It has been found impossible to show any relationship between the decreased sugar tolerance found in some cases of cancer and the total serum calcium. That a lowered blood serum calcium is encountered in diabetic malnutrition in some instances and increases in calcium are observed during insulin therapy is well known. It does not follow, however, that in these conditions the rise in the blood sugar, together with the fall in the blood serum calcium, or in the second instance the fall in the blood mgar with a rise in the blood serum calcium, has any causal relationship. In the temporary hypercalcemia following insulin therapy, the changes in the blood serum calcium are probably secondary to the removal of phosphate ion to form hexose phosphate,

546 F. H. L. TAYLOR AND H E N R Y JAUESON
as glucose utilization is accelerated. In the hypocalcemia of diabetes and malnutrition, as in other cachectic states, the lowered serum calcium is probably associated with the lowered serum proteins particularly of the albumen fraction.
CONCLUSIONS I. I n only one-third of 35 cancer patients studied was a decreased
tolerance for glucose found, prior to the institution of roentgen therapy. 11. Consideration must be given to the fact that a lowered tolerance
for glucose is not an uncommon tendency in persons between fifty-five and seventy years of age, particularly if they are suffering from malnutrition.
111. The presence of a lowered carbohydrate tolerance in cancer is not diagnostic nor is it of assistance in prognosis. However, progres- sively increased abnormality of the carbohydrate tolerance may be regarded as an unfavorable sign.
IV. Roentgen radiation has no consistent effect on the sugar toler- ance of cancer patients.
V. No relationship has been found between the decreased sugar tolerance occurring in some cases of cancer and the total serum calcium.
Note: The authors express their appreciation of the co-operation of the S W of the Pondville Hospital during the progress of this investigation. They acknowledge in par- ticular the technical assistance of Miss Eleanor R. Shea, A.B., and Mr. Roderick Dwyer.
BIBLIOGRAPHY 1. WARBURG, 0. : Verbesserte Methode zur Messung der Atmung und Glykolyze, Biochem.
Ztschr. 51: 152, 1924. 2. CORI, C. F., AND Cow, 0. T.: On the carbohydrate metabolism of malignant tumors,
Proc. SOC. Exper. Med. & Biol. 22: 254, 1924. 3. SLOSBE, A., AND REDING, R.: fitude des althrations humhrales dans le cancer et le
prBcancer, Bull. Acad. roy. de mBd. de Belgique 7: 405, 1927. Also in Cancer, Bruxelles 4: 442, 1927.
4. BEREOOPP, PAULINE : Changes in the blood chemistry in malignant disease with special reference to carbohydrate tolerance and alkalosis, J. Cancer Research 14: 559,1930.
5. ENOCKSBON, B.: Carbohydrate metabolism in gastric cancer, Svenska lak. 27: 729, 1930. Abst. in Am. J. Cancer 15: 365, 1931.
6. BENSO, F.: Le xantoprotein, i lipoide, il glucosio nel siero di sangue dei cancerosi, Tumori 4 : 425, 1930.
7. ROMANIN, V. : Apparato glicoregolatore e tono vegetativo nei tumori maligni, Minerva med. 1 : 870, 1931. Abst. in Cancer Review 7 : 151, 1932.
8. HUEPER, W. C., WOODWARD, G. E., AND FRY, E. 0.: Interrelations between histologic structure and blood chemical findings in cancer, Am. J. Cancer 15: 2666, 1931.
9. DE NIORD, R. N., SCHREINER, B. F., AND DE NIORD, H. H. : The effect of roentgen rays on the metabolism of cancer patients, Arch. Int. Med. 25: 32, 1920.
10. PENA, FAUSTINO A.: La glicemia en el cancer, Bol. Inst. de med. exper. para el estud. y trat. del cheer 7 : 1258, 1930. Abst. in Am. J. Cancer 15: 1654, 1931.
11. FOLIN, O., AND SVEDBERQ, A.: Micro methods for the determination of non-protein nitrogen, urea, uric acid, and sugar in unlaked blood, J. Biol. Chem. 88: 85, 1930.
12. FISKE, CYRUS H., AND LOGAN, M. A.: Unpublished calcium method. 13. LEHMANN, W. L. : Het arsenigzuur als geneesmiddel bij diabetes mellitus, Amsterdam,
1873. Abst. in Arch. exper. Path. u. Pharm. 2: 463, 1874.

THE CARBOHmBATE TOLERANCE IN CANCER PATIENTS 547
14. Du VIQNEAUD, V., AND KARR, W. 0.: Carbohydrate utilization. 1. The rate of dis- appearance of d-glucose from the blood, J. Biol. Chem. 66: 281, 1925.
15. LENNOX, W. G., O’CONNOR, M., AND BELLINQER, M.: Chemical changes in the blood during fasting in the human subject, Arch. Int. Med. 38: 553, 1926.
16. MOROULIS, S., AND EDWARDS, A. C. : Chemical changes in the blood during fasting and subsequent refeeding.
17. CORI, C. I?.: The fate of sugar in the animal body. I. The rate of absorption of hexoses and pentoses from the intestinal tract, J. Biol. Chem. 66 : 691, 1925.
18. FADER, K.: Benign glycosuria due to disturbances in the blood sugar regulating mechanism, J. Clin. Investigation 3: 203, 1926.
19. HANSEN, K. M.: Investigations on the blood sugar in man. Conditions of oscilla- tions, rise, and distribution, Arta med. srand. Supplement 4, pp. 1-221, 1923.
20. STAtrB, H. : Untersuchungen iiber den Zuckerstoffwechsel des Menschen, Ztschr. f. klin. Med. 93: 89-140, 1922.
21. JACKSON, HENRY, JR., AND TAYLOR, F. H. L.: The calcium, potassium and inorganic phosphate content of the serum in cancer patients, Am. J. Cancer 19: 379, 1933.
22. WILDER, R. M., ET A L : Carcinoma of the islands of the pancreas: hyperinsulinism and hypoglycemia, J. A. M. A. 89: 348, 1927.
23. SPENCE, J. C.: Some observations on sugar tolerance with special reference to varia- tions found a t different ages, Quart. J . Med. 14: 314, 1921.
24. LENNOX, W. 0.: Stimulation of the sugar regulating mechanism as shown by dupli- cate blood sugar curves, J. Biol. Chem. 73: 237, 1927.
Experiments on dogs, Am. J. Physiol. 68: 477, 1924.