Embed Size (px)
Citation preview
8/10/2019 the case of an adult with adhd
http://slidepdf.com/reader/full/the-case-of-an-adult-with-adhd 1/21
http://ccs.sagepub.com/ Clinical Case St udies
http://ccs.sagepub.com/content/7/6/471The online version of this article can be foun d at:
DOI: 10.1177/1534650108319912 2008 7: 471 originally published online 19 June 2008Clinical Case Studies
Bradley M. Rosenfield, J. Russell Ramsay and Anthony L. RostainExtreme Makeover : The Case of a Young Adult Man With Severe ADHD
Published by:
http://www.sagepublications.com
can be found at:Clinical Case Studies Additional services and information for
http://ccs.sagepub.com/cgi/alertsEmail Alerts:
http://ccs.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
http://ccs.sagepub.com/content/7/6/471.refs.htmlCitations:
What is This? - Jun 19, 2008Proof
- Nov 10, 2008Version of Record>>
by Andreea Nicoleta Nicolae on October 12, 2011ccs.sagepub.comDownloaded from
8/10/2019 the case of an adult with adhd
http://slidepdf.com/reader/full/the-case-of-an-adult-with-adhd 2/21
Extreme Makeover
The Case of a Young Adult ManWith Severe ADHDBradley M. RosenfieldJ. Russell RamsayAnthony L. RostainUniversity of Pennsylvania School of Medicine, Philadelphia
Attention-deficit/hyperactivity disorder (ADHD) is the most prevalent behavioral disorderamong children in the United States.Many of these children continue to experience prominentfunctional difficulties through adolescence and into adulthood. Specific impairments commonto adults with ADHD have only recently come to light. The goal of this article is to discuss thecase of a young man,Ralph, who was first diagnosed with ADHD in early childhood. Althoughpharmacotherapy helped him function better at school as a child, he encountered newfounddifficulties as an adult, which reactivated his sense of rejection and failure in virtually everydomain of his life. His case illustrates the degree of impairment experienced by many adultswith ADHD and the benefit of a multimodal treatment package, which, in Ralph’s case,included pharmacotherapy, cognitive-behavioral psychotherapy, and marital therapy modifiedfor adults with ADHD.
Keywords: ADHD; attention deficit disorder; attention-deficit/hyperactivity disorder;cognitive-behavioral therapy; psychotherapy; couple’s therapy; adults; commu-nication skills; pharmacotherapy
1 Theoretical and Research Basis
Attention-deficit/hyperactivity disorder (ADHD) is a prominent developmental neu-ropsychiatric disorder characterized by the hallmark symptoms of developmentally inap-propriate levels of hyperactivity, impulsivity, and/or inattention (American PsychiatricAssociation [APA], 2000). Although there appears to be no simple, clear-cut pathophysiol-ogy, ADHD is known to be a highly heritable disorder (Nigg, 2006). Researchers are cur-rently exploring links between its observable symptoms and functional differences indifferent regions and networks in the brain (e.g., Casey & Durston, 2006). Environmentalfactors, on the other hand, have been found to contribute minimally to the risk for devel-oping ADHD ( Hudziak, Derks, Althoff, Rettew, & Boomsma, 2005) .
471
Clinical Case StudiesVolume 7 Number 6
December 2008 471-490© 2008 Sage Publications
10.1177/1534650108319912http://ccs.sagepub.com
hosted athttp://online.sagepub.com
Authors’ Note: Address correspondence to Bradley M. Rosenfield, Adult ADHD Treatment and ResearchProgram, Center for Cognitive Therapy, School of Medicine, University of Pennsylvania, 3535 Market St., 2ndFloor, Philadelphia, PA 19104; phone: 215-871-6914; fax: 215-898-1865; e-mail: [email protected].
by Andreea Nicoleta Nicolae on October 12, 2011ccs.sagepub.comDownloaded from
8/10/2019 the case of an adult with adhd
http://slidepdf.com/reader/full/the-case-of-an-adult-with-adhd 3/21
It is increasingly clear that children with ADHD do not invariably “grow out of it” onreaching adulthood. On the contrary, research of the persistence of symptoms of ADHDindicates that up to 90% of these individuals continue to experience some degree of func-
tional impairment into adulthood ( Biederman, Mick, & Faraone, 2000 ). Results from anational survey of psychiatric comorbidity in the United States indicated that 36.3% of individuals diagnosed with childhood ADHD (established by retrospective self-report) con-tinued to meet full Diagnostic and Statistical Manual of Mental Disorders ( DSM-IV-TR ;APA, 2000) criteria as adults (Kessler et al., 2005). This percentage is likely an underesti-mation of the true persistence of symptoms because the diagnostic criteria were originallydeveloped for children ages 4 to 17 years old and do not currently include developmentallyappropriate criteria for adults (McGough & Barkley, 2004). Barkley, Murphy, and Fischer(2008) compiled an empirically derived set of nine symptoms of ADHD that differentiateadults with ADHD from both a non-ADHD clinical sample of adults and a nonclinical con-
trol sample of adults. Relevant to the current case, these symptoms include the following:is often easily distracted by extraneous stimuli; often has difficulty stopping activities orbehavior when he or she should do so; often has difficulty sustaining attention in tasks orleisure activities; and often has difficulty organizing tasks and activities. It is further pro-posed that the age of onset be modified to specify that “some symptoms that caused impair-ment were present before age 16 years ” (Barkley et al., 2008, p. 192).
Regarding functional impairment, longitudinal and cross-sectional studies indicate thatindividuals with ADHD, when compared with non-ADHD controls, report lower levels of educational attainment, a higher incidence of psychiatric comorbidity than would be
expected by chance, increased risk for substance abuse, greater discord in relationships,poorer driving records, and not surprisingly, more negative outlooks and higher levels of pessimism (Barkley et al., 2008; Barkley, Fischer, Smallish, & Fletcher, 2006; Biedermanet al., 2006; Biederman & Faraone, 2005; Murphy & Barkley, 1996a, 1996b; Wilens,Biederman, & Spencer, 2002). Working adults with ADHD were paid lower salaries, hadmore conflict with supervisors, were less punctual, produced lower quality work, had lowerscores on ratings of work performance, and were more likely to be disciplined by superi-ors than both clinical and community samples (Barkley et al., 2008).
A variety of studies has established the prevalence rate of adult ADHD at around 4% of the adult population in the United States, with a recent national survey estimating that 4.4%
of adults in the United States fulfill diagnostic criteria for adult ADHD, representing about8 million adults. Prevalence rates of ADHD found in international samples are strikinglysimilar to those found in the United States, with a recent study of countries in the Americas,Europe, and Middle East reporting an international prevalence of 3.4% (Fayyad et al.,2007), indicating that ADHD is not a uniquely “American” disorder (Kessler et al., 2006).
Increasing numbers of adults are seeking evaluation and treatment for issues related toADHD, though, unfortunately, it is estimated that only 11% of adults with ADHD receivespecialized treatment (Kessler et al., 2006). These individuals seek help either after havingbeen diagnosed with ADHD in childhood and seeking treatment to cope with issues inadulthood, or after learning about ADHD as adults and recognizing that their longstandingdifficulties that previously had been attributed to character flaws, laziness, or other pejora-tive explanations may have neurobiological underpinnings and, what is more, are treatable.
472 Clinical Case Studies
by Andreea Nicoleta Nicolae on October 12, 2011ccs.sagepub.comDownloaded from
8/10/2019 the case of an adult with adhd
http://slidepdf.com/reader/full/the-case-of-an-adult-with-adhd 4/21
Medications, particularly the psychostimulants, have been well researched in the treat-ment of ADHD in patients of all ages, establishing pharmacotherapy as an effective firstline of treatment (e.g., Dodson, 2005). Although medications may lessen core symptoms of
ADHD, these improvements, though impressive, do not necessarily produce positive resultsin important domains of functioning, such as social skills, organization, time management,and confidence. Thus, medications alone may be insufficient treatment for many adultswith ADHD, particularly those with moderate to severe symptoms and complex clinicalpresentations.
Consequently, many adults seek adjunctive psychosocial treatment for help managingthe day-to-day effects of living with ADHD. Though there has been comparatively littleresearch of psychosocial treatments, cognitive-behavioral therapy (CBT) approachesadapted for adult ADHD have emerged with the strongest evidence base (Ramsay &Rostain, 2007). Although ADHD is not the result of negative or distorted thoughts, many
individuals who grew up with (often undiagnosed) ADHD may have developed maladap-tive beliefs and cognitions that interfere with the implementation of effective coping strate-gies. CBT for adult ADHD helps individuals to appreciate how ADHD affects their lives,develop effective coping strategies, and identify and modify cognitions that interfere withimplementation of these coping strategies to enhance resilience and overall well-being(Ramsay & Rostain, 2008).
The purpose of this article is to discuss the case of a young man, Ralph, who was diag-nosed with ADHD and treated with medications in childhood. However, Ralph experiencednewfound difficulties functioning in adulthood when his symptoms directly led to a num-
ber of life crises affecting his ability to function at work and in his marriage. The goal of presenting Ralph’s case is to illustrate the degree of impairment experienced by manyadults with ADHD and to describe a coordinated, multimodal intervention approach com-posed of pharmacotherapy, individual CBT, and marital therapy to address diverse andcomplex problem areas in his life.
2 Case Presentation
Ralph is a 30-year-old married, Caucasian man who sought an evaluation at the authors’
specialty clinic for adult ADHD. He made the appointment at the behest of his wife, June,who is a middle school teacher. June was exasperated because her husband had been firedfrom nine different jobs during the first 5 years of their marriage, followed by a 2-year periodof total unemployment preceding his evaluation. Ralph lamented, “My wife says I’m drivingher crazy with my irresponsibility (i.e., unemployment) and social embarrassments.”
Ralph presented as a rather cheerful but admittedly “socially awkward” young manwhose manner made him seem considerably younger than his stated age. He was friendlyand cooperative through the interview process, but had a tendency to blurt out answers toquestions before the examiner could complete them. Consequently, his answers oftenmissed the mark and periodically spiraled into loosely related tangents. His eye contact wasminimal and he requested the window blinds be drawn as “the light reflection through theblinds is very distracting.”
Rosenfield et al. / Young Man With Severe ADHD 473
by Andreea Nicoleta Nicolae on October 12, 2011ccs.sagepub.comDownloaded from

8/10/2019 the case of an adult with adhd
http://slidepdf.com/reader/full/the-case-of-an-adult-with-adhd 5/21
Ralph said that his goal for the evaluation and for eventual treatment was to save his mar-riage by finding better ways to manage his ADHD, especially to enable him to secureemployment. He agreed to seek treatment only after his wife threatened to divorce him.
Ralph said that June complained that he did not listen to her and his lack of reliability andfollow-through on promises made her feel disrespected. He said these complaints were sim-ilar to those voiced by his parents when he was younger. Ralph had at times briefly soughttreatment in the past but, considering the gravity of his current situation, he now viewedtreatment as his “last chance.”
3 Presenting Complaints
Apart from responding to his wife’s ultimatum that he seek treatment, Ralph confided
that he was highly motivated to learn how to find and keep a job for personal reasons. Hesaid that it bothered him to have been fired from every job he had had in adulthood, usu-ally because of some combination of recurrent tardiness, inability to follow directions, for-getting important projects, inefficiency, procrastination, and clashes with peers andsupervisors. Although he reported minimal emotional distress, Ralph’s expectation that hewould “fail” in his endeavors, based in no small part on his realistic experiences of beingfired, spurred brief, though intense feelings of dysphoria and hopelessness. He said that,when stressed, he distracted himself by becoming engrossed on the computer or by “put-tering around the house,” adopting an attitude that “everything is going to work out.” He
made plans for finding a new job, but did not follow through on steps to achieve this goal.Ralph effectively avoided short-term distress but was left “feeling like a failure,” com-pounded by resulting financial stress and his wife’s view of him as a “lazy underachiever.”
Ralph hoped to improve his relationship with his wife but it seemed that the harder hetried, the more mistakes he would make. He bemoaned that his wife felt embarrassed tosocialize with other couples because of his numerous social “blunders.” For example, theyattended a formal fundraising event for the school district in which June worked and he toldan inappropriate, off-color joke to the superintendent and his wife. In another instance hereduced a restaurant hostess to tears when he made a joke about her weight, thinking shewas out of earshot. The cumulative effect of these various experiences was that Ralph was
left feeling incompetent and pessimistic about his ability to make changes in his life,though he desperately clung to the notion that things could magically work out for the bestif he found the “right” job and the “right” medication.
4 History
It is good practice, whenever possible, to gather corroborative data about developmentalhistory and childhood symptoms of ADHD from other observers and sources (e.g., parentsor sibling, medical records, and old report cards). However, Ralph said that he did not getalong well with his parents and tried to keep contact to a minimum, thus the assessors reliedon his report of developmental information and his wife’s recollection of stories told to herby his parents about Ralph as a child.
474 Clinical Case Studies
by Andreea Nicoleta Nicolae on October 12, 2011ccs.sagepub.comDownloaded from
8/10/2019 the case of an adult with adhd
http://slidepdf.com/reader/full/the-case-of-an-adult-with-adhd 6/21
Ralph was the only child born to his parents. His mother’s pregnancy and delivery of himwere reportedly uncomplicated, as was his early development. His father and mother, a car-penter and a stay-at-home parent, respectively, were frequently called by teachers regard-
ing his behavior difficulties in school and were similarly aggravated by his behavior athome. Ralph remembered having behavior problems as far back as early elementary school,including “getting in trouble for not sitting still and talking out of turn.” He said that hisrelationship with his parents was “always terrible. I never wanted to sleep and I was all overthe place from the time I could stand up. The only thing I could do for an extended timewas play video games. They told me over and over that I was a handful.” He grudginglyacknowledged that they had exhibited some degree of parental concern because they hadsought treatment for him in childhood.
Ralph remembered severe problems from the very beginning of first grade, including“excruciating boredom” with classroom activities, inability to focus attention, squirming in
his seat, excessive talking, and blurting out answers in class. Such behaviors resulted inrecriminations from his teachers and parents, though what he recalled as being most frus-trating for him was that “they thought I was a bad kid for not listening, but I really could-n’t do what they wanted and I couldn’t make them understand.” Ralph also recalled havingno friends in elementary school because other children found him to be “annoying.” Suchannoyances were the sum result of missing social cues, perseverating on topics when a con-versation had obviously moved on, his inability to stop playful teasing, and “always sayingthe wrong thing.”
After being diagnosed with ADHD by a school psychologist, Ralph was prescribed the
psychostimulant methylphenidate in second grade by a pediatrician. Soon thereafter he wasable to start to develop his first friendships, “but, kids still got annoyed with (him) a lot.”He responded well to his prescribed dose and his hyperactivity and impulsivity improved,allowing him to “finally concentrate in school and be less annoying to others.” By fourthgrade he said that he felt more “normal” and his grades and social circumstances continuedto improve, though he continued to characterize sitting in class and doing homework as“agonizing boredom.”
Ralph was maintained on a stable dose of methylphenidate for the duration of ele-mentary school, middle school, and into high school. By all accounts, he continued torespond well to pharmacotherapy in terms of improved attention and concentration and
he was considered an average student. During his senior year of high school, unbe-knownst to his parents, he started to skip doses of his medications, only taking it whenhe needed to study. Ralph’s grades tailed off in many classes. He graduated from highschool with his class but grew increasingly anxious about school toward the end. He hadself-doubts that were similar to those he had in elementary school, though he attributedhis lower grades to “senior-itis.”
Ralph abruptly stopped taking his medication altogether soon after arriving at college,ostensibly because he reported increased anxiety but he also admitted that he wanted to “doit on [his] own.” Although he had been nervous about college, he found college lecturesmore interesting than in high school. Ralph joined a choral group and thrived on the structureand camaraderie that it offered. He received study tips, free tutoring, and class notes from “thesmartest guys” in the choir. He also was careful to not schedule morning classes because hehad difficulty waking up and getting to early lectures on time. Ralph acknowledged that,
Rosenfield et al. / Young Man With Severe ADHD 475
by Andreea Nicoleta Nicolae on October 12, 2011ccs.sagepub.comDownloaded from
8/10/2019 the case of an adult with adhd
http://slidepdf.com/reader/full/the-case-of-an-adult-with-adhd 7/21
despite these steps, college was not easy for him. He was somewhat disorganized in hisapproach to completing assignments but was proud to graduate with a solid C average.
During his final year of college, during a period of relative stability, Ralph met June. She
said that she found his “energy” and willingness to “express his outrageous opinions” to beattractive. Neither he nor his wife had much dating experience when they met, and neitherhad been in a serious romantic relationship. However, they reportedly fell in love and wereengaged to be married within 6 months, not long after their graduation and to the chagrinof both families. June said that their first heated arguments occurred when Ralph would for-get or not follow through on his various responsibilities in planning their wedding.
Ralph’s entrance to the “real world” of the workplace was a rude awakening for him. Therigidity of schedules, lack of individualized guidance and supervision, emphasis on per-sonal organization, time management, planning, and personal accountability for perfor-mance resulted in repeated poor performance evaluations. There was also no end of the
semester to provide an opportunity to start over with a “clean slate.”Ralph tended to respond to superiors’ corrective feedback by becoming defensive, mak-
ing excuses, and blurting out convoluted explanations that ranged from blame to angry out-bursts. Such behaviors invariably led to reprimands, strained interactions, and, ultimately,termination of employment. His conflicts at work were compounded by his inability to fol-low rules, misreading social cues, and stubbornness with supervisors. For instance, he oftenarrived early or stayed late to compensate for his admitted procrastination and inefficiencyat work. However, these extra hours raised concerns because his employers were legallyobligated to pay him overtime. Although Ralph offered to waive his overtime pay, such
appeals ended in arguments when Ralph was unable to accept “no” for an answer. Theseinteractions resulted in him being labeled as “high maintenance.” Ralph also refused to dis-close to his employers the fact he had ADHD because he was ashamed of his “condition.”Being unable to keep a job corroded Ralph’s confidence and sense of self, confirming hiscore belief that he was “inadequate.”
June and Ralph’s first major marital rift arose when Ralph was fired from his first jobduring their first year of marriage. His occupational problems over the years were com-pounded by escalating marital conflicts stemming from Ralph forgetting to pay bills, notfollowing through on chores, and “getting stuck” on topics in conversations, all leading tohis wife’s perception that he was insensitive to her. Ralph said her frustration with him cul-
minated a few weeks before he scheduled his evaluation when June tearfully pronouncedhim “an embarrassing underachiever” and banished him to sleep on the couch. Ralph saidthat he realized his wife had grown increasingly frustrated with the chaos in their marriage,but hearing that she was considering divorce took him by surprise. He said he now recog-nized the need to get help.
5 Assessment
Ralph received a comprehensive psychiatric evaluation that included various measuresof adult ADHD. In addition to an extensive history-gathering interview that included hiswife’s input on various forms (although she was unable to attend in-person) and psychiatricrecords, Ralph was administered the Structured Clinical Interview for DSM-IV Axis I
476 Clinical Case Studies
by Andreea Nicoleta Nicolae on October 12, 2011ccs.sagepub.comDownloaded from
8/10/2019 the case of an adult with adhd
http://slidepdf.com/reader/full/the-case-of-an-adult-with-adhd 8/21
Disorders (First, Spitzer, Gibbon, & Williams, 1997), the Brown Attention Deficit DisorderScale for Adults (BADDS; Brown, 1996), the Conners’ Adult ADHD Rating Scales(CAARS; Conners, Erhardt, & Sparrow, 1999), the Beck Depression Inventory II (BDI-II;
Beck, Steer, & Brown, 1996), the Beck Anxiety Inventory (BAI; Beck & Steer, 1990), theBeck Hopelessness Scale (BHS; Beck & Steer, 1989), and ADHD symptom checklists forboth childhood and adult symptoms, including both self-report and observer report forms(Barkley & Murphy, 2006). No school records were available.
Ralph presented with minimal levels of self-reported anxiety and depression, which wassurprising given his precarious domestic and vocational circumstances. Ralph’s scores onthe BDI-II, BAI, and BHS all fell in the minimal range for depression, anxiety, and hope-lessness, respectively. Thus, these self-report instruments did not accurately reflect thedegree of functional impairment Ralph exhibited. In effect, he was disturbingly “under-whelmed” by the problems he was facing as a result of various avoidance strategies.
Although he endorsed items on the BDI-II indicating that he was troubled by indecision,believed he had failed more than he should have, and that he had lost confidence in him-self, each of these items was endorsed only as “mild.” He seemed to find comfort byattributing his difficulties to his childhood diagnosis of ADHD, seemingly using the diag-nosis to explain away his current problems and to deflect the suggestion that he coulddevelop ways to cope more adaptively.
The BADDS is a 40-item clinician-administered rating scale of ADHD symptom severityin various life domains. Ralph’s BADDS total score fell in the “ADD highly probable” rangeand he had clinically elevated scores for the Activation and Attention subscales, reflecting that
he has difficulties getting started on tasks and maintaining focus on various projects.The CAARS: Long Version is a 66-item self-report instrument that measures a wide varietyof symptoms of ADHD in adult patients. Among the subscale scores are three devoted to DSM-
IV criteria ( DSM-IV Inattentive Symptoms, DSM-IV Hyperactive-Impulsive Symptoms, and DSM-IV ADHD Symptoms Total). Ralph’s responses indicated clinical elevations for bothhyperactivity/impulsivity and inattentive symptoms and for subscales measuring emotionallability, inattention, and memory problems, and problems with self-concept.
Ralph’s recall of his behavior during childhood, corroborated by a copy of the evalua-tion report written by the school psychologist who assessed him in first grade, indicated thepresence of sufficient impairment to indicate that he had met diagnostic criteria for ADHD,
Combined Type in childhood. His self-report of his current ADHD symptoms indicated adevelopmental pattern of sustained problems of inattention, impulsivity, and poor self-man-agement. Likewise, these impressions were corroborated by his wife’s responses on anobserver checklist of current symptoms, with June even adding a note, “And this is withmedications [ sic ] !!!” Thus, there was sufficient convergent evidence from a variety of sources that Ralph had struggled with ADHD since childhood and his current symptomscontinued to play a direct and causal role in his current difficulties.
The structured diagnostic interview revealed a history of brief reactive episodes of depressed mood, including varying symptoms dysphoria, anhedonia, weight loss, insom-nia, and psychomotor agitation that were precipitated by “being fired.” However, Ralph’sdescription of his current emotional state fell short of meeting full diagnostic criteria forseverity and chronicity for any mood or anxiety disorder, although he described some resid-ual depressive symptoms. Consequently, the diagnostic impression based on the structured
Rosenfield et al. / Young Man With Severe ADHD 477
by Andreea Nicoleta Nicolae on October 12, 2011ccs.sagepub.comDownloaded from
8/10/2019 the case of an adult with adhd
http://slidepdf.com/reader/full/the-case-of-an-adult-with-adhd 9/21
interviews, the BADDS, and CAARS results was that his symptoms fulfilled diagnostic cri-teria for ADHD, Combined Type with comorbid Depressive Disorder, Not OtherwiseSpecified (i.e., minor depressive episodes). There was no evidence to suggest that his symp-
toms could be better explained by other psychiatric disorders or a medical condition.Results of the assessment were reviewed with Ralph and his wife during an assessmentfeedback session. In addition to psychoeducation about the effects of ADHD on his func-tioning, time was spent reviewing the effects of his impulsivity on his relationship at work and at home, as these interpersonal issues contributed to his impairment as much as his dis-organization and avoidance did. Thus, it was recommended that he start concurrent phar-macotherapy and CBT, with therapy sessions also addressing issues related to hisinterpersonal functioning. Considering the level of marital stress, marital therapy with atherapist specializing in ADHD issues was also mentioned as a possible component of thetreatment plan. Ralph and June said they wanted to discuss this option further, though they
agreed for Ralph to start the combined pharmacotherapy–CBT treatment.
6 Case Conceptualization
The symptoms of ADHD are considered to be the downstream consequences of execu-tive dysfunction stemming from impaired neurobiological functioning. The symptoms neg-atively affect various aspects of self-control, planning, concentration, memory, andbehavioral activation. Not surprisingly, the aforementioned difficulties create many func-
tional problems in the day-to-day lives of affected adults. Ralph’s symptoms, which basi-cally had gone untreated in adulthood, created significant impairment in his life and hiscould be considered a severe case of ADHD.
Considering the severity of his symptoms and life impairment, it was clear that Ralphwould require multiple modes of treatment. His treatment plan started with concurrentpharmacotherapy and CBT focused on achieving symptom reduction and functionalimprovements in behavioral coping.
At the time of his initial evaluation, according to Ralph and medical records, his previouspsychiatrist had prescribed a combination of extended-release methylphenidate and extended-release bupropion, with minimal effectiveness. After reviewing treatment options, it was
decided to switch his stimulant medication to mixed amphetamine salts (immediate release)and to evaluate how this regimen would help his core symptoms of poor concentration andinattentiveness, overactivation, and impulsivity. After titrating the dose to a moderate level, hereported noticeable improvement ( > 50%) in these symptoms at which point he was switchedto the extended-release form to improve adherence. Although he was pleased with the initialresponse to mixed amphetamine salts, by the 8th week of CBT, Ralph began to complain thathe was extremely unfocused in the evenings and mornings and that these symptoms were con-tinuing to cause significant impairment in his marital relationship and in his ability to carry outmorning and evening self-care routines. After reviewing treatment options, it was decided tobegin a trial of atomoxetine as an augmentation strategy, with the expectation that this med-ication would be effective in the evenings and mornings, and that it would also enhance theefficacy of the mixed amphetamine salts. Within a month, Ralph reported that both treatmentobjectives were met, and he was very pleased with the results. Not only were mornings and
478 Clinical Case Studies
by Andreea Nicoleta Nicolae on October 12, 2011ccs.sagepub.comDownloaded from
8/10/2019 the case of an adult with adhd
http://slidepdf.com/reader/full/the-case-of-an-adult-with-adhd 10/21
evenings easier for him to manage (especially from the standpoint of marital interactions), buthe also found his ability to focus and complete tasks during work hours was significantlyimproved ( > 70% greater than baseline). He has maintained his progress on this combination
regimen (mixed amphetamine salts, atomoxetine, and bupropion) throughout the duration of treatment with no side effects.A CBT case conceptualization provides a detailed template for understanding a patient’s
belief system and the influence of this belief system on automatic thoughts, emotions,physiological responses, and behaviors. One of the myths about CBT is that it ignoresdevelopmental information to exclusively focus on the “here and now.” On the contrary, animportant aspect of developing a case conceptualization is to identify specific develop-mental learning experiences that may have provided the original “evidence” for certain corebeliefs; beliefs that may have once been relevant in a specific developmental context.However, those beliefs may have become obsolete or maladaptive in current settings.
ADHD has pernicious effects on many domains of life that are central for one’s self-concept, such as school, work, relationships, and global sense of self-efficacy. Maladaptivebeliefs, although often rooted in documented frustrations in these life domains, have becomeovergeneralized and create undue stumbling blocks to pursuing reasonable personal goals(Ramsay & Rostain, 2008).
The CBT model of adult ADHD recognizes that the disorder is fundamentally neurobi-ological in nature (e.g., Seidman, Valera, & Makris, 2005), resulting in downstream deficitsin executive functioning, self-control, and behavior (Nigg, 2006). Despite their neurobio-logical origin, it is easy to understand how the neurocognitive deficits of adult ADHD con-
tribute to both emotional distress and functional impairment. The effects of ADHD onfunctioning are comparable to the notion of temperament, affecting individuals to somedegree throughout their lives and playing an important role in the reciprocal interactionsbetween oneself and the social environment beginning at an early age. These experiences,in turn, affect one’s self-perception and the personal meanings attributed to new experi-ences, which, in turn, affect how one constructs core beliefs about oneself, the world, andone’s view of the future (Beck, 1976). In this manner, the individual’s core beliefs influ-ence cognitive, emotional, and behavioral responses that then elicit consequences in theexternal environment, which serve to maintain the ADHD belief system, in a self-perpetu-ating cycle (Ramsay & Rostain, 2008).
Based on information gathered during the diagnostic interview and early sessions of CBT, Ralph’s case conceptualization seemed to be organized around three principal mal-adaptive schema (Young, 1999): failure (“I’ve failed at everything important in life.”),defectiveness/shame (“I’m a social embarrassment.”), and entitlement (“People shouldknow I have ADHD and accommodate me because I cannot change.”). As is common whenconstructing a case conceptualization, these beliefs “make sense” considering that theyarose from recurring, often painful early life experiences, including the sense that he haddisappointed his parents and teachers, primarily because of the effects of his ADHD symp-toms. Although he had a positive response to medications and had many affirming experi-ences in high school and college, his schema lay dormant until triggered by stressful lifecircumstances associated with the effects of residual ADHD in adulthood.
To compound matters, Ralph learned that he could immediately reduce his distress by engag-ing in various forms of avoidance, be it cognitive, emotional, or behavioral. For example, he
Rosenfield et al. / Young Man With Severe ADHD 479
by Andreea Nicoleta Nicolae on October 12, 2011ccs.sagepub.comDownloaded from
8/10/2019 the case of an adult with adhd
http://slidepdf.com/reader/full/the-case-of-an-adult-with-adhd 11/21
recalled, “I could not stand not being able to concentrate on my reading assignments, so Ifound excuses to do everything but reading.” The benefits of avoidance are immediate, pro-viding quick escape from discomfort (i.e., negative reinforcement). However, costs of avoid-
ance of uncomfortable thoughts and feelings are great, such as dodging important problemsthat inevitably must be faced. Ralph’s avoidance cycle also prevented him from attemptingmore adaptive behaviors and coping strategies that could help him to have more satisfyingexperiences. In CBT parlance, such behaviors that are an apparent effort to manage a corebelief but that end up insidiously strengthening them in a self-defeating manner are deemedcompensatory strategies and are an important target for intervention.
It soon became apparent that Ralph also avoided stress by engaging in magical thinking(e.g., “It will all work out”), coupled with externalizing thoughts in the form of using thediagnosis of ADHD to disproportionately emphasize the need for external accommodations(e.g., “They should cut me a break because I have ADHD”). These cognitive distortions
served to deflect focus away from the adaptive changes he could make to his coping reper-toire. Thus, his tendency to avoid facing various issues in his life out of concern he would“fail” was an important aspect of his CBT case conceptualization. These issues would beimportant to address as Ralph attempted to make behavioral changes in his life to improvehis functioning and his well-being and, ultimately, to revise his beliefs about himself.
7 Course of Treatment and Assessment of Progress
CBT sessions lasting 50 minutes were held on a weekly basis. During the first CBT ses-sion with his individual therapist (BR), the primary agenda item was for Ralph to identifyspecific, operationalized treatment goals gleaned from his ambiguous, though understand-able objectives, which were to “save [his] marriage and find a job.” Ralph’s ambitions werereworked into specific behavioral goals, including (a) to learn and use different communi-cation skills with his wife to increase intimacy and deescalate (rather than trying to “win”)arguments, (b) to spend 3 nights per week doing specific “couples things together,” and(c) to research potential jobs for which he could apply, paying particular attention to issuesrelated to compatibility and how his attitudes affect his job search and work performance.
Even with well-defined and reasonable treatment goals, the start of treatment for adults
with ADHD is often a delicate time. Ralph’s history illustrates the likelihood that thesepatients have frequently experienced more than their share of frustration and disappoint-ment. Such biographies can often lead to negative perceptions of treatment, because theydo not see immediate results, particularly in complex cases, such as Ralph’s. Thus, it isimportant to “start small” and to prioritize the initial therapeutic agenda to focus on ahighly specific problem that is susceptible to incremental progress (Ramsay & Rostain,2008). “Small” problems are very often exemplars of the same patterns and issues creating“big” problems. Seeing that Ralph faced “crises” in both his marital and work domains, heand his therapist agreed that focusing on issues related to his job search was a good firststep because finding work would address a primary point of contention in his marriage andhopefully allow him to generate an income.
For Ralph, the first small steps in CBT were further complicated by his ambivalenceabout engaging in the process of change. Although Ralph genuinely wanted to find a job
480 Clinical Case Studies
by Andreea Nicoleta Nicolae on October 12, 2011ccs.sagepub.comDownloaded from
8/10/2019 the case of an adult with adhd
http://slidepdf.com/reader/full/the-case-of-an-adult-with-adhd 12/21
and improve his marriage, CBT would require him to face issues he had long avoided. Whatis more, although crucial to his overall well-being, he seemed to place too much stock inmedications as a cure-all for his problems. Thus, early interventions, during Sessions 2
through 6, also focused on enhancing his motivation for CBT by elaborating on and per-sonalizing his commitment to change, rather than solely being motivated to appease hiswife. In particular, challenging two of his core beliefs, “discomfort should be avoided” and“I’m a failure,” required that he take some risks. Therapeutic behavioral change wasreframed as a way Ralph could “avoid” cognitive, affective, and behavioral difficulties atwork and in his relationships. Thus, his compulsive avoidance was employed in the serviceof adaptive change.
With Ralph sufficiently willing to face difficult issues (or at least willing to try), theseearly sessions focused on exploring possible job options. When Ralph did not followthrough on a homework task, such as spending 30 minutes researching promising jobs, it
was viewed as a chance for him to explore and understand his avoidance. That is, wheninquiring about the cognitions associated with avoidance (“What thoughts went throughyour mind when you considered researching jobs?”), issues related to pessimism and unre-alistic notions of a “perfect” job emerged, as did problems with poor time management,procrastination, and disorganization. Each of these potential barriers lent themselves to anintervention, such as cognitive restructuring (e.g., modify task-interfering thoughts) andinstitution of specific coping strategies (e.g., break down project into manageable steps,keep track of activities in a schedule book, etc.). These interventions provided Ralph withstrategies with which to reapproach homework tasks rather than to avoid and abandon
them. He modified his search for a “dream job” to one for a job for which he was qualifiedand was “good enough.” Ralph responded well to this “win-win” approach to therapeutichomework, that is, either he would complete the task or identify the obstacles preventinghim from doing so.
By Session 8, his insight and adherence increased so that even when he did not followthrough, he was better able to describe the cognitions and behavior patterns that contributedto his avoidance. Ralph continued to work with his psychiatrist to develop an effective med-ication regimen during this time, with a focus on further reducing his impulsivity, hyper-activity, and inattention, to enhance his acquisition of new skills. His therapist wouldinquire about Ralph’s response to medications, his adherence, and the presence of side
effects. Ralph benefited from the fact that his therapist and psychiatrist consulted regularlyregarding his treatment progress.
Despite a generally positive response to medications, Ralph continued to struggle withprocrastination, feeling overwhelmed by tasks that others took for granted, often resultingin excessive self-criticism. However, each frustration was framed as another opportunity todevelop ways to manage them more effectively. For example, cognitive rehearsal via visualimagery helped Ralph to think through the steps necessary to update his resume and toidentify the task-interfering thought, “There is no job out there that I can do.” The fearedfantasy technique (Burns, 1980) was used to further elicit the meaning of this thought tohim, as illustrated in the following exchange:
Therapist (T): What are the thoughts that might prevent you from starting your job search tomorrow?Ralph (R): [sullenly] There’s no job out there for me.
Rosenfield et al. / Young Man With Severe ADHD 481
by Andreea Nicoleta Nicolae on October 12, 2011ccs.sagepub.comDownloaded from
8/10/2019 the case of an adult with adhd
http://slidepdf.com/reader/full/the-case-of-an-adult-with-adhd 13/21
T: And if you couldn’t find a job, what is the worst thing that you can imagine happening to you?R: My wife will divorce me.T: And, for the sake of argument, if your wife divorced you, what would be the worst thing that you can
imagine happening to you?
R: I would be homeless.T: And if you were homeless, what is the worst thing that might happen?R: I would be dead on the street.T: How does that thought make you feel?R: Terrible . . . depressed.T: The depression is understandable, given your thoughts. Can I ask you a question?R: Yes.T: How likely is it that starting your job search tomorrow will result in your being divorced, homeless, and
dead in the street?R: [laughter and visible relief] I guess that’s a little extreme.T: Do you see how sometimes our thoughts and expectations can be distorted and how that influences how
we feel and how we behave? In this case, the job search understandably makes you feel bad. Why?Because it is associated with these very negative thoughts and emotions. However, the short-term gainof avoiding these negative thoughts and feelings by avoiding the job search ensures that you will not finda job and increases the likelihood that your wife will divorce you.
R: You’re right. It really is a vicious cycle.
During his early sessions, Ralph had found it helpful to use Daily Thought Records(DTR; Beck, Rush, Shaw, & Emery, 1979) to systematically develop alternative thoughtsto his pessimistic reactions. These forms helped him produce the following adaptivethoughts: “I’m resourceful. I’ve gotten married, found other jobs, I have a family. I amcapable of finding another job. I did well in college when I had support.” Ralph also usedthe forms to temper his tendency to engage in excessively positive “magical thinking,” suchas, “I don’t need to practice for the job interview. I think on my feet pretty well,” insteaddeveloping the view, “Let me spend 15 minutes practicing my answers to some basic ques-tions so I feel prepared.”
However, after the progress achieved during the first 10 sessions of individual CBT,there was one problem that could no longer be deferred. Ralph’s wife had stopped wearingher wedding ring and had informed him she was making plans to leave him and live withher parents. By reviewing his options in CBT sessions, Ralph saw three potential ways torespond to the situation. First, he would demonstrate his “stability” by finding and holding
a job. Second, he would practice relationship enhancement skills (e.g., listening, construc-tive communication) to reduce his admitted lack of social graces. Finally, Ralph wouldinvite his wife to couple’s therapy attempt to improve their increasingly toxic relationship.
In the subsequent individual CBT session, the therapy agenda included the discussion of principles of effective communication (e.g., Burns, 1980). More specifically, Ralph shareda recent example of a “she said–I said” argument with his wife. He and his therapist thenperformed a reverse role-play of the same interaction with Ralph playing his wife’s role andthe therapist playing a rather impulsive Ralph, so that he experience the argument from herstandpoint. He acknowledged that he did not like what he heard, thus the exercise accom-plished its goal of creating empathy and cognitive dissonance, thereby increasing motiva-tion to change. The role-play was then repeated with the therapist, playing a new, adaptiveRalph, demonstrating communication strategies such as disarming, reflecting, gentle
482 Clinical Case Studies
by Andreea Nicoleta Nicolae on October 12, 2011ccs.sagepub.comDownloaded from
8/10/2019 the case of an adult with adhd
http://slidepdf.com/reader/full/the-case-of-an-adult-with-adhd 14/21
inquiry, and empathy, while avoiding defensiveness, name-calling, and interruptions. Ralphquickly acknowledged that the experience demonstrated how “my impulsive interruptingmust drive my wife crazy” and that the new method could actually increase the couple’s
intimacy. Ralph practiced the new strategies in a final role-play as himself, whereas thetherapist carefully shaped his behavior. The rationale for this intervention was to boostRalph’s confidence and competence, with an eye toward eventually generalizing theseskills to other life domains.
At the start of a Session 12, Ralph announced that he had been offered a job. Hisresponse to the congratulations he received from his therapist, however, was subdued.Ralph admitted he was considering rejecting the offer. Review of a DTR in session revealedthe following negative automatic thoughts regarding the job: “It’s a dead-end job. I’ll bestuck there for life.” These negative cognitions understandably engendered “fright, frustra-tion, and hopelessness.” After exploration, Ralph pronounced these thoughts to be distor-
tions and generated the following rational response to them: “My fears aren’t rational—Iwon’t be stuck. I can still look for a better job after I give this one a fair chance. This is sta-ble pay. Holding a job will show my wife I’m serious about making changes.”
During the next several weeks, Ralph and his therapist collaboratively targeted his prob-lems at work, including reported personality clashes between a “controlling” boss and anadmittedly “rigid” Ralph. From his perspective, disagreements focused on specific detailsof how he completed tasks rather than the quality of Ralph’s work. Ralph was left feelinganxious and “incompetent” and, thus, prone to respond impulsively to his boss. Eventhough Ralph could clearly see that this was a risky pattern and he has received excellent
pharmacotherapy, he lacked the ability to manage his frustration, reflecting the cognitiveinflexibility and poor problem-solving often seen in ADHD. Ralph agreed to experimentwith the following procedures at work, which he recorded on a written flowchart that hecould keep with him while on the job:
1. When “anxious,” take a moment to actively think before responding.2. Use the DTR to identify automatic thoughts and distortions, and to formulate a rational
response.3. Communicate to my boss in an assertive but nonaggressive manner, as we role-played in
session, repeatedly.4. Employ the Three Sentence Rule; that is, limit responses in conversations to two or three sen-
tences to avert lapsing into frustrating tangents and to decrease the probability of inadver-tently saying something offensive (J. R. Ramsay, personal communication, January 5, 2007).
5. Listen to my boss’s feedback and voice agreement with some aspect of it. Remember,the primary goal: to communicate to my boss that I hope to do the best job as efficientlypossible.
After a number of successes resulting from this procedure, Ralph and his therapist rela-beled Ralph as “assertive” and collaborative. However, despite these improvements at work and the fact he was working hard to maintain gainful employment, the deteriorating rela-tionship with his wife was a complicating factor that required a modification to the multi-modal treatment plan to include marital therapy. Thus, after about 4 months of concurrentpharmacotherapy and CBT, June and Ralph agreed to attend marital sessions.
Rosenfield et al. / Young Man With Severe ADHD 483
by Andreea Nicoleta Nicolae on October 12, 2011ccs.sagepub.comDownloaded from
8/10/2019 the case of an adult with adhd
http://slidepdf.com/reader/full/the-case-of-an-adult-with-adhd 15/21
8 Complicating Factors
Despite decreased conflict in their interactions during the course of his individual CBT,
Ralph’s wife reportedly remained skeptical of his ability to sustain his current improve-ments and new job. Although she remained steadfast in her intention to pursue a divorce,June reluctantly accepted Ralph’s invitation to attend marital therapy sessions. In manycases, individual CBT for adult ADHD may include periodic sessions with a significantother to address relationship issues and gather corroborative information about progresstoward treatment goals (e.g., Safren, Perlman, Sprich, & Otto, 2005). However, many cou-ples affected by ADHD seek marital therapy focused on managing the effects of ADHD ontheir relationship (e.g., Kilcarr, 2002). Considering the degree of conflict within their mar-riage, it was recommended that Ralph and his wife meet with another clinician at theauthors’ program specifically to address marital issues, thus allowing Ralph to continueindividual sessions to focus on his efforts at personal change.
The marital therapist (J.R.R.) had been involved in Ralph’s assessment, thus he wasfamiliar with the case. During their first marital therapy session, the therapist invited Ralphand June to take turns expressing their goals for what marital sessions could accomplish.Ralph said that he realized his ADHD symptoms had negatively affected the relationship interms of his unemployment and inability to pay attention to his wife. He was optimistic thatCBT would help him improve in those areas but he easily lapsed into anger when he per-ceived that June did not appreciate his struggles with ADHD or his progress. Juneexpressed her frustration at being the sole wage earner, compounded by the fact she felt she
was also expected to complete household responsibilities left uncompleted by Ralph. Ralphfidgeted in his seat while listening to his wife, periodically interrupting with pressuredspeech to argue individual points. The therapist reminded Ralph to give his wife an oppor-tunity to speak freely and encouraged him to write down his thoughts on an available tabletof paper to discuss them later.
The therapist asked the couple each to rate the likelihood they would divorce on a 0 to100 scale. Ralph replied “zero,” and his wife shot back “85 to 90.” Shocked, Ralphdemanded, “How can you say that when I’ve made so much progress already in treatment?”The therapist interrupted again to summarize and empathize with each of their frustrationsabout the relationship. The therapist pointed out that the purpose of marital therapy wouldbe to improve their relationship, whether or not they decided to divorce. However, becausethe specter of divorce was contributing to the daily stress they experienced, the therapistasked if they would be willing to put a 3-month moratorium on making a final decisionabout divorce. The rationale for this request was to give them time to focus on the issuesthat contributed to thoughts of divorce and to implement changes without being in “crisismode” (and there was no evidence of physical or emotional abuse that might have necessi-tated a separation for safety’s sake). Thus, the therapist clarified that this approach wouldask June to temporarily suspend the threat of divorce. This approach also would ask Ralphto refrain from asking his wife for assurances that she would not eventually proceed with a
divorce to allow them both to focus on making personal changes that would improve theirrelationship. June and Ralph both agreed to this plan.The remainder of the first marital session dealt with “starting small” and identifying discrete
examples of problems they faced in the context of daily life. For example, a recent argument
484 Clinical Case Studies
by Andreea Nicoleta Nicolae on October 12, 2011ccs.sagepub.comDownloaded from
8/10/2019 the case of an adult with adhd
http://slidepdf.com/reader/full/the-case-of-an-adult-with-adhd 16/21
8/10/2019 the case of an adult with adhd
http://slidepdf.com/reader/full/the-case-of-an-adult-with-adhd 17/21
medications. The two therapists discussed the various individual and marital issuesaddressed in session to ensure that they were providing consistent messages to Ralph andreinforcing the use of various coping strategies. Although he faced a number of ongoing
difficulties, it was agreed that Ralph seemed to be making slow, steady progress.Unfortunately, June suddenly dropped out of marital therapy near the end of the 3-monthmoratorium (after six sessions of marital therapy) after Ralph demanded that she make adecision about whether or not she planned to pursue divorce. He said that he had beengrowing increasingly anxious about the prospect of divorce despite the fact they had beengetting along much better. Ralph reportedly confronted June one evening, catching her off guard, and demanded that “she owed [him]” reassurance that she would not leave him.Presented with his impulsive, pressured, and rigid ultimatum, and after a lengthy argument,June said that she “had had enough” and reverted to her plan to leave him.
The marital therapist made himself available to the couple if they wanted to continue to
work on reconciliation or even to work through a possible divorce. However, June declinedand Ralph was encouraged to deal with resulting coping issues with his individual thera-pist, whom the marital therapist apprised of the situation. Consequently, 6 months aftercompleting his ADHD evaluation and starting treatment ostensibly to save his marriage,Ralph was left to face the crisis of impending divorce and the financial crisis of deciding if he could afford to continue to live alone in his house.
Although it was not an easy period for him, it is interesting that Ralph was able to main-tain perspective and to focus on managing problems as they presented themselves whilekeeping up with the demands of his job. He recognized the many improvements he had
made and came to the realization that, “This is hard right now, but I have to break it downto face one issue at a time. I might even be better off without the marital stress.”In the subsequent 3 months, Ralph continued pharmacotherapy and individual CBT. He
took steps to reconnect with his parents and to let them know about his situation with June.His parents provided him with some financial support that helped him weather the short-term financial crisis of the separation from June. Ralph used CBT sessions to sort throughand prioritize his personal affairs to clarify his plans. He and June had sporadic contact dur-ing the first month or two of their separation to take steps to disentangle their affairs. Ralphwas also encouraged by his individual therapist’s prediction (based on Junes personalityfeatures, including some moderate abandonment issues) that his absence may, in fact, make
his wife’s “heart grow fonder.”About 3 months after leaving him (i.e., after 9 months of treatment), June began to invite
Ralph out on casual “dates.” June did not say that she would reconcile with him but saidthat she was not ready to file for divorce. Ralph was ambivalent about this arrangement,until his therapist asked Ralph if he was willing to tolerate the uncertain situation with Junefor another 6 months. Ralph stated that it was not a healthy situation for him and he rec-ognized that he could not afford to continue to pay the mortgage for the house by himself.He soon thereafter told June that it was “unfair to be left in limbo” and that he would needa decision from her either to reunite and resume martial therapy or he would plan to “moveon with his own life,” including selling their house and splitting the proceeds with her.Rather than a pressured demand driven by a need to assuage his anxiety or to be vindictive,he delivered his well-reasoned decision in an appropriately assertive, even-tempered man-ner. Paradoxically Ralph’s assertion that he was ready to leave her finally demonstrated the
486 Clinical Case Studies
by Andreea Nicoleta Nicolae on October 12, 2011ccs.sagepub.comDownloaded from
8/10/2019 the case of an adult with adhd
http://slidepdf.com/reader/full/the-case-of-an-adult-with-adhd 18/21
8/10/2019 the case of an adult with adhd
http://slidepdf.com/reader/full/the-case-of-an-adult-with-adhd 19/21
recognize how ADHD complicated their relationship issues and to use this information tostart to change their relationship coping and interaction patterns. The combination of dif-ferent modes of treatment was necessary to target the wide ranging negative effects of ADHD on Ralph’s functioning.
It is also clear that Ralph will likely require ongoing coping support, at least for the near
future. He remains employed in the same job for more than a year and is facing theuncharted issues related to maintaining adequate performance over the long term. Likewise,the prospect of raising a family will surely introduce new individual, marital, and familystressors associated with becoming a parent. The need for ongoing treatment support is notmeant to imply that Ralph’s multimodal treatment was ineffective. On the contrary, his cop-ing challenges illustrate that ADHD, particularly in severe cases such as Ralph’s, is a life-long, developmental disorder with pervasive effects that can severely impair functioning atvarious life junctures.
11 Recommendations to Clinicians and Students
Many individuals with ADHD who seek help receive inadequate or incomplete treatmentthat runs the risk of being only minimally successful at best. Lack of positive outcome mostoften occurs in one of two ways. In the first scenario, well-meaning clinicians make capableefforts to treat presenting problems, such as anxiety or depression without awareness of under-lying ADHD. Also, lack of diagnostic accuracy results in treatment that misses the mark
In the second scenario, patients receive an accurate diagnosis of ADHD and treating psy-chiatrists or primary care physicians provide pharmacotherapy targeting symptom relief. Adult
patients with uncomplicated symptoms may benefit greatly from medications alone. However,many patients with ADHD may continue to founder because, although the medication hasameliorated some of the core symptoms, there is not adequate attention paid to behavioralfunctioning, including improving organization, problem solving, time management, and social
488 Clinical Case Studies
0
10
20
30
40
50
60
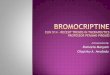
Pre 1 2 7 10 11 12 Post
BDI
BADS
120
100
80
60
40
20
0 B e c
k D e p r e s s
i o n
I n v e n
t o r y
( B D I )
B e
h a v
i o r a
l A c
t i v a
t i o n
f o r
D e p r e s s
i o n
S c a
l e ( B A D S )
Session3 4 5 6 8 9
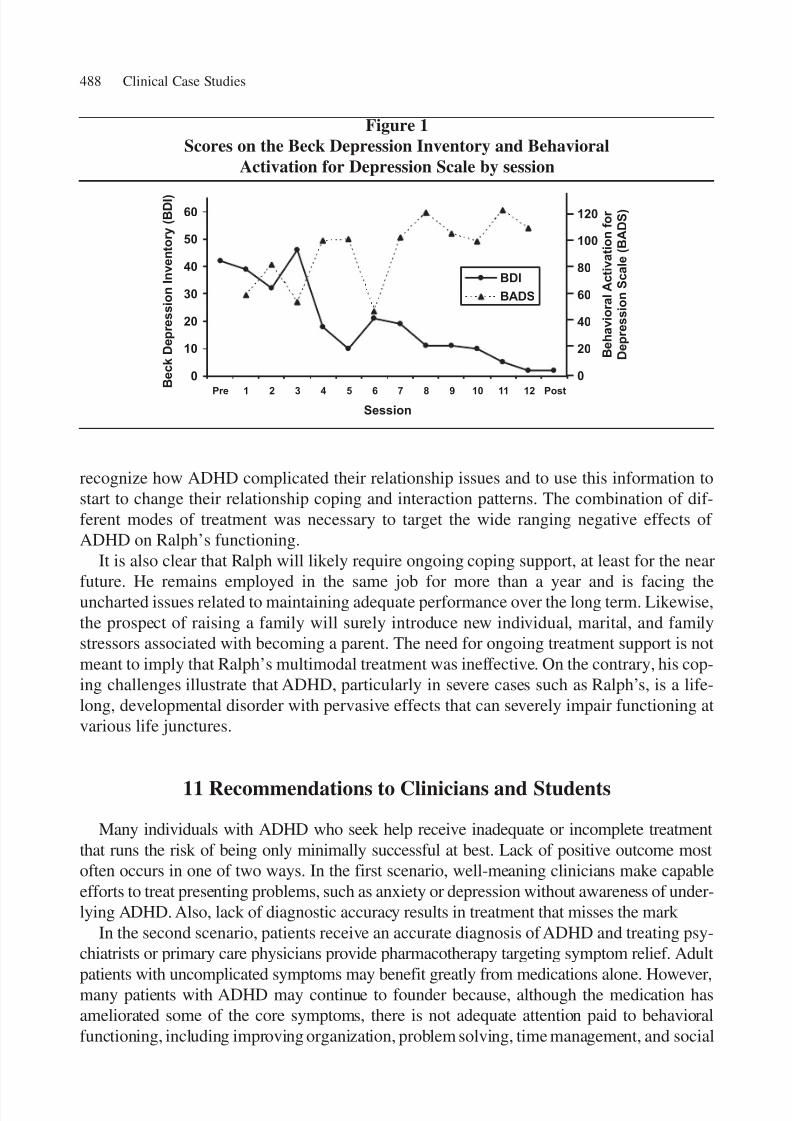
Figure 1Scores on the Beck Depression Inventory and Behavioral
Activation for Depression Scale by session
by Andreea Nicoleta Nicolae on October 12, 2011ccs.sagepub.comDownloaded from

8/10/2019 the case of an adult with adhd
http://slidepdf.com/reader/full/the-case-of-an-adult-with-adhd 20/21
skills, and the corrosive effects of negative beliefs that have developed from a lifetimeof frustrations.
Not every patient with ADHD will require the same level of clinical services as Ralph
did. However, Ralph’s case illustrates the pervasive impairment that can be associated withADHD and the corresponding need for individualized multimodal treatment approaches foradults with ADHD to address their diverse clinical needs and improve overall well-being.
References
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4th ed., textrev.). Washington, DC: Author.
Barkley, R. A., Fischer, M., Smallish, L., & Fletcher, K. (2006). Young adult outcome of hyperactive children:
Adaptive functioning in major life areas. Journal of the American Academy of Child and Adolescent Psychiatry, 45 , 192-202.Barkley, R. A., & Murphy, K. R. (2006). Attention-deficit hyperactivity disorder: A clinical workbook (3rd ed.).
New York: Guilford.Barkley, R. A., Murphy, K. R., & Fischer, M. (2008). ADHD in adults: What the science says . New York:
Guilford.Beck, A. T. (1976). Cognitive therapy and the emotional disorders . New York: Meridian.Beck, A. T., Rush, A. J., Shaw, B. F., & Emery, G. (1979). Cognitive therapy of depression . New York: Guilford.Beck, A. T., & Steer, R. A. (1989). Manual for the Beck Hopelessness Scale . San Antonio, TX: Psychological
Corporation.Beck, A. T., & Steer, R. A. (1990). Beck Anxiety Inventory manual . San Antonio, TX: Psychological
Corporation.Beck, A. T., Steer, R. A., & Brown, G. K. (1996). Beck Depression Inventory—Second edition manual . San
Antonio, TX: Psychological Corporation.Biederman, J., & Faraone, S. V. (2005, October). Economic impact of adult ADHD . Poster session presented at
the 17th CHADD annual international conference, Dallas, TX.Biederman, J., Faraone, S. V., Spencer, T. J., Mick, E., Monuteaux, M. C., & Aleardi, M. (2006). Functional
impairments in adults with self-reports of diagnosed ADHD: A controlled study of 1001 adults in the com-munity. Journal of Clinical Psychiatry, 67 , 524-540.
Biederman, J., Mick, E., & Faraone, S. V. (2000). Age-dependent decline of symptoms of attention deficithyperactivity disorder: Impact of remission definition and symptom type. American Journal of Psychiatry,157 , 816-818.
Brown, T. E. (1996). Brown Attention Deficit Disorder Scales . San Antonio, TX: Psychological Corporation.Burns, D. D. (1980). Feeling good . New York: Signet.Casey, B. J., & Durston, S. (2006). From behavior to cognition to the brain and back: What have we learned
from functional imaging studies of attention deficit hyperactivity disorder? American Journal of Psychiatry ,163 , 957-961.
Conners, C. K., Erhardt, D., & Sparrow, E. (1999). Conners’ Adult ADHD Rating Scales . North Tonawanda,NY: Multi-Health Systems.
Dodson, W. W. (2005). Pharmacotherapy of adult ADHD. Journal of Clinical Psychology, 61 , 589-606.Fayyad, J., DeGraaf, R., Kessler, R., Alonso, J., Angeermeyer, M., Demyttenaere, K., et al. (2007). Cross-
national prevalence and correlates of adult attention-deficit hyperactivity disorder. British Journal of Psychiatry, 190 , 402-409.
First, M. B., Spitzer, R. L., Gibbon, M., & Williams, J. B. W. (1997). User’s guide for the Structured Clinical
Interview for DSM-IV Axis I disorders . Washington, DC: American Psychiatric Press.Hudziak, J. J., Derks, E. M., Althoff, R. A., Rettew, D. C., & Boomsma, D. I. (2005). The genetic and environ-
mental contributions to attention deficit hyperactivity disorder as measured by the Conners’ RatingScales–Revised. American Journal of Psychiatry, 162 , 1614-1621.
Rosenfield et al. / Young Man With Severe ADHD 489
by Andreea Nicoleta Nicolae on October 12, 2011ccs.sagepub.comDownloaded from

8/10/2019 the case of an adult with adhd
http://slidepdf.com/reader/full/the-case-of-an-adult-with-adhd 21/21
Kessler, R. C., Adler, L. A., Ames, M., Barkley, R. A., Birnbaum, H., Greenberg, P., et al. (2005). The preva-lence and effects of adult attention deficit/hyperactivity disorder on work performance in a nationally rep-resentative sample of workers. Journal of Occupational and Environmental Medicine, 47 , 565-572.
Kessler, R. C., Adler, L. A., Barkley, R. A., Biederman, J., Conners, C. K., Demler, O., et al. (2006). The preva-
lence and correlates of adult ADHD in the United States: Results from the National Comorbidity SurveyReplication. American Journal of Psychiatry, 163 , 716-723.
Kilcarr, P. (2002). Making marriages work for individuals with ADHD. In S. Goldstein & A. T. Ellison (Eds.),Clinician’s guide to adult ADHD: Assessment and intervention (pp. 219-240). San Diego, CA: AcademicPress.
McGough, J. J., & Barkley, R. A. (2004). Diagnostic controversies in adult attention deficit hyperactivity dis-order. American Journal of Psychiatry, 161 , 1948-1956.
Murphy, K. R., & Barkley, R. A. (1996a). Attention deficit hyperactivity disorder adults: Comorbidities andadaptive impairments. Comprehensive Psychiatry, 37 , 393-401.
Murphy, K. R., & Barkley, R. A. (1996b). Prevalence of DSM-IV symptoms of ADHD in adult licensed dri-vers: Implications for clinical diagnosis. Journal of Attention Disorders, 1 , 147-161.
Nigg, J. T. (2006). What causes ADHD? Understanding what goes wrong and why . New York: Guilford.Ramsay, J. R., & Rostain, A. L. (2007). Psychosocial treatments for attention-deficit/hyperactivity disorder inadults: Current evidence and future directions. Professional Psychology: Research and Practice, 38, 338-346.
Ramsay, J. R., & Rostain, A. L. (2008). Cognitive-behavioral therapy for adult ADHD: An integrative psy-chosocial and medical approach . New York: Routledge.
Safren, S. A., Perlman, C. A., Sprich, S., & Otto, M. W. (2005). Mastering your adult ADHD: A cognitive-behavioral treatment program—Therapist guide . Oxford, UK: Oxford University Press.
Seidman, L. J., Valera, E. M., & Makris, N. (2005). Structural brain imaging of attention-deficit/hyperactivitydisorder. Biological Psychiatry, 57 , 1263-1272.
Wilens, T. E., Biederman, J., & Spencer, T. J. (2002). Attention deficit/hyperactivity disorder across the lifes-pan. Annual Review of Medicine, 53 , 113-131.
Young, J. E. (1999). Cognitive therapy for personality disorders: A schema-focused approach (3rd ed.).Sarasota, FL: Professional Resource Press.
Bradley M. Rosenfield a clinical associate at the University of Pennsylvania School of Medicine, Adult ADHDTreatment and Research Program, Center for Cognitive Therapy. He is also a clinical assistant professor atPhiladelphia College of Osteopathic Medicine, teaching a doctoral-level class surveying research and treatment forADHD. He has lectured internationally to clinicians and academicians on the clinical applications of cognitive ther-apy, multicultural competence, applied behavior analysis, and persuasion and social influence in the clinical context.
J. Russell Ramsay , PhD, is a licensed psychologist and is assistant professor of psychology in psychiatry at theUniversity of Pennsylvania School of Medicine. In addition to cofounding and serving as associate director of
the University of Pennsylvania Adult ADHD Treatment and Research Program, he is a senior staff psychologistat the Center for Cognitive Therapy. He has lectured internationally to mental health professionals on the princi-ples and clinical applications of cognitive therapy and on the assessment and treatment of adult ADHD. Hisresearch interests are focused on developing effective assessment and treatment strategies for adults with ADHD.
Anthony L. Rostain , MD, is professor of psychiatry and pediatrics at the University of Pennsylvania, wherehe serves as Director of Education for the Department of Psychiatry. He is codirector of The Children’s Hospitalof Philadelphia’s Pediatric Neuropsychiatry Program and cofounder and director of the University of Pennsylvania Adult ADHD Treatment and Research Program. His research interests have focused on improv-ing clinical outcomes for patients with neuropsychiatric disorders, including ADHD, Tourette’s syndrome,Asperger’s syndrome, and complex learning disorders. He is triple boarded in pediatrics, adult psychiatry, and
child and adolescent psychiatry.
490 Clinical Case Studies