Embed Size (px)
Citation preview

The CDC Implementation Guide on Alcohol Screening and Brief
Intervention:What PHNs Should Know
December 6, 2016
Webinar
www.phnurse.org
• All attendee telephones will be muted
• If you have a question for the presenter:
• Type it in the Question Window on the right side of your screen• Click on “send privately” button
• Questions will be answered at the end of the session in the order in which they are received
• Please refrain from sending messages to “entire audience” during the presentation
Disclosures
The presenters and planners of this educational activity have no conflict of interest and have not received any financial support for any part of the planning
of this presentation.
Phone and Webinar Etiquette

3
• In order to successfully complete the education activity and receive 1.00 nursing contact hour, webinar APHN members must attend the entire “Live” presentation and complete the online course evaluation which will be emailed to APHN members who were on the “Live” webinar.
• Continuing education credit will only be provided to those APHN members who attend the entire educational activity on 12/6/2016 and complete the evaluation form within 30 days following the “live” presentation.
• The webinar will be archived and slides will be posted on the members section of the APHN website www.phnurse.org
Accreditation Statement
Continuing education credit will be provided through the Public Health Nursing and Professional Development Unit. The Public Health Nursing and Professional Development
Unit, North Carolina Division of Public Health, is approved as a provider of continuing nursing education by the North Carolina Nurses Association, an accredited approver by the American
Nurses Credentialing Center’s Commission on Accreditation.
Disclosures

The Presenters
Ann M. Mitchell, PhD, RN, AHN-BC, FIAAN, FAANProfessor, University of Pittsburgh School of Nursing
Irene Kane, PhD, MSN, RN, CNAA, EP-CAssociate Professor, University of Pittsburgh School of Nursing
Diane King, PhDDirector and Research Assistant Professor, University of Alaska Anchorage Center for Behavior Health Research & Services; Institute of Social and Economic Research
Beth Kelsey, EdD, APRN, WHNP-BCDirector of Publications, NPWH
Susan Rawlins, MS, APRN, WHNP-BCDirector of Education, NPWH

Learner Outcomes for Webinar
• Upon completion of this webinar, PHNs will have increased knowledge regarding how to successfully plan, implement, & evaluate a successful and sustainable Alcohol SBI Program using the process outlined in the CDC Implementation Guide for Alcohol SBI.

PHN Core Competencies Addressed
Analytic and Assessment Skills
Policy Development/Program Planning Skills
Communication Skills
Leadership and Systems Thinking Skills
Implementation Process Basics
This presentation is part University of Pittsburgh School of Nursing SBI: Workforce Expansion for Nurse Leadersgrant-funded from the Centers for Disease Control & Prevention (CDC) /American Association of Colleges of Nursing(AACN) Grant WIP number: 2014-N-0004 and coordinated with IRETA and the John Hopkins School of Nursing,recipients of CDC/AACN grant. Please also see CDC http://www.cdc.gov/fasd for comprehensive FASD information.

Objectives• Educate health professionals on steps to plan, implement, and
evaluate an alcohol SBI program
• Examine step-by-step details on developing and implementing site-specific programs
• Emphasize important factors geared towards successful program outcomes
• Describe important factors that provide sustainability for site-specific program

Planning and Implementing Screening and Brief Intervention for Risky Alcohol Use
A Step-by-Step Guide for Primary Care Practices
(CDC, 2014)
Introduction to Alcohol Screen and Brief Intervention: A Critical Clinical Preventive Service
Like hypertension or tobacco screening, alcohol screening and brief intervention (alcohol SBI) is a clinical preventive service. It identifies and helps patients who may be drinking too much. It involves:
• A validated set of screening questions to identify patients’ drinking problems
• A short conversation with patients who are drinking too much, and for patients with severe risk, a referral to specialized treatment as warranted.
The entire service takes only a few minutes, is inexpensive, and may be reimbursable.
(CDC, 2014)

Risky drinking affects your patients’ health.
Risky drinking may be associated with:
• Increasing the risk of hypertension, stroke, type 2 diabetes, cancers
• Cirrhosis of the liver• Injury• Violence• Increased body weight• Can impair short – and long-term cognitive
function• Sexually transmitted diseases• Unintended pregnancy• Violent crime
(CDC, 2014)

Implementation Basics
I. Laying the Groundwork1. Familiarize the planning team with alcohol SBI – why it is an important medical service and
how it works2. Ensure that practice leaders are committed to implementing alcohol SBI
II. Adapting Alcohol SBI to Your Practice3. Plan Screening procedures4. Plan brief intervention procedures5. Establish procedures to refer patients with severe problems
III. Implementing Alcohol SBI in Your Practice6. Train staff for their specific roles7. Pilot test and refine your plan8. Manage initial full implementation so it succeeds
IV. Refining and Promoting9. Monitor and improve your alcohol SBI plan over time10. Publicize your efforts so that others can learn from your experience
(CDC, 2014)

I. Laying the Groundwork
Share the rationale for implementing your new program before making specific changes!
(CDC, 2014)

Step 1: Understand the Need for Alcohol SBI• It is much more than
alcohol dependence.• The main target population
for brief interventions is nondependent, risky drinkers…The goal of the brief intervention is to motivate them to cut back or stop drinking.
• What is risky drinking? How much is too much?• See Table at right.
(CDC, 2014)
A. Risky Drinking Levels for Healthy AdultsAny person drinking more than either the daily or weekly levels in the table below is drinking too much. If a person exceeds the weekly levels, a long-term risk for a wide range of chronic conditions can occur. If a person exceeds the single-day levels, he or she risks intoxication, which is associated with a variety of more immediate risks.
Healthy men ages 21-65 No more than 4 drinks on any single day (5 or more drinks consumed within 2 hours is binge drinking)ANDNo more than 14 drinks a week
All healthy women ages 21 and older
No more than 3 drinks on any single day (4 or more drinks consumed within 2 hours is binge drinking)ANDNo more than 7 drinks a week
Healthy men over age 65
B. For some people, even less is risky.The levels provided above are just one consideration in defining risky drinking. A variety of health conditions and activities may warrant limiting drinking to even lower levels or not drinking at all. Here are some examples.• Individuals taking prescription or over-the-counter medications that may interact with alcohol and cause
harmful reactions• Individuals suffering from medical conditions that may be worsened by alcohol, e.g., liver disease,
hypertriglyceridemia, pancreatitis• Individuals who are driving, planning to drive, or participating in other activities requiring skill,
coordination, and alertness
C. For some people, any drinking at all is risky.Here are some examples.• Individuals unable to control the amount they drink. This group includes people dependent on alcohol.• Women who are pregnant or might become pregnant• Individuals younger than age 21

Step 2: Get Organizational Commitment
• Implementing an effective alcohol SBI
plan requires:• A firm commitment from the leaders of
your practice.• Communication of that commitment to all
relevant staff.
• Share CDC Alcohol SBI Fact Sheet with key managers…to reach a common understanding of:• The need for alcohol SBI in your practice,• What alcohol SBI is,• Your goals, and • How you will inform staff member of your decision to implement alcohol SBI
(CDC, 2014)
II. Adapting Alcohol SBI to Your Practice
It is critical to plan fully all the elements of your alcohol SBI service before you start implementing or training staff to provide it.
Step 3: Plan for Screening
A complete alcohol SBI screening plan specifies:
• Which patients you will screen
• How often you will screen patients
• Which screening instrument you will use
• How and where you will screen
• How you will store and share screening results
(CDC, 2014)

Who Will be Screened?
Ideally, you should screen all of your patients with two possible exceptions:
• Children under 9 years of age, who are not likely to drink alcohol.
• Patients who are too ill to answer screening questions at a particular visit.
(CDC, 2014)

How Often Should Patients be Screened?
Because drinking patterns change over time, patients should be screened at least annually. If nearly all of your patients receive preventive-care physical examinations annually, the best time to provide alcohol SBI might be that visit. Alternatively, if many of your patients do not have annual physicals, you might want to screen every patient on the first visit of each year.
(CDC, 2014)

Which Screening Instrument Will You Use?
Recommended Screening Tools:
The Single Question Alcohol Screen
• Single Question
• Can be included on intake questionnaire
• Simple, quick, and easy method of screening
AUDIT-1-3 (US)
• Questions 1-3 identify patients who are drinking too much
• Can be administered in a minute (2-3 minutes for the full AUDIT)
(CDC, 2014)

How Will the Screening be Performed and Where?Some suggestions are:
• Via computer before the patients arrives
• Via questionnaire in the reception room
(CDC, 2014)
How Will Screening Forms be Scored and the Results be Shared and Stored?1. Who will score the screening instruments?
2. How will screening results be shared with staff who will provide brief interventions?
3. How will screening results be recorded in the patient’s chart?
4. Where will screening forms (if used) be stored and managed?
5. How will patients who screen positive be followed during future visits? If a patient screens positive, you will need to follow up appropriately as you would with any other risk factor.
(CDC, 2014)

Step 4: Plan for Brief Intervention
• Two main issues:• Who will deliver the interventions?
• Time Availability• Knowledge and Experience• Interpersonal Skills• Willingness
• What will the basic elements of your intervention system be?• When will interventions be delivered?• How will you introduce the intervention for patients who screen positive?• What elements will you include in the intervention?• How long will interventions typically take?• How will you intervene with patients who are likely to be dependent on alcohol?• How will you follow patients who receive an intervention?• How will the intervention be documented?
(CDC, 2014)

Who Will Deliver the Interventions?
Factors to Consider:
• Time Availability
• Knowledge and Experience
• Interpersonal Skills
• Willingness
(CDC, 2014)

What Will the Basic Elements of Your Intervention System Be?Questions to Consider:
• When will interventions be delivered?
• How will you introduce the intervention for patients who screen positive?
• What elements will you include in the intervention?
• How long will interventions typically take?
• How will you intervene with patients who are likely to be dependent on alcohol?
• How will you follow patients who receive an intervention?
• How will the intervention be documented?
(CDC, 2014)

Step 5: Establish Referral Procedures
Three Available Resources:
1. The Substance Abuse and Mental Health Services Administration (SAMHSA.gov)
2. Your practice’s contacts
3. Alcoholics Anonymous (AA)
(CDC, 2014)

III. Implementing Alcohol SBI in Your Practice
The steps for implementation include:
• Orienting and training all staff• Planning and evaluating a pilot test• Managing start up of full
implementation
(CDC, 2014)
Picture via: http://www.kinshipenterprise.com/_blog/Blog/post/how-social-australian-business-adapt-to-survive/#.VV86jE9VhBc

Step 6: Orientation and Training
Steps to orientation and training include:
1. Determine who needs training
2. Orient all staff about risky alcohol use and alcohol SBI
3. Help staff become more comfortable discussing alcohol use
4. Train for alcohol SBI specialized functions
(CDC, 2014)Picture via: http://www.solutions4schools.org.uk/site/index.php/newgalleries/galleries/staff-training
Step 7: Plan a Pilot Test
Pilot Testing Evaluation Points:
1. Number of patients in target population2. Percentage screened3. Number and percentage who screen
positive4. Percentage of positives receiving an
intervention5. Percentage referred to treatment
(CDC, 2014)
Picture via: http://www.samprasoft.com/mobile_app_testing

Step 8: Support a Strong Start-Up
When starting up your official and permanent program, consider the following:
1. Communicate
2. Provide hands-on help
3. Address unforeseen issues quickly
4. Offer feedback, encouragement,and thanks
(CDC, 2014)
Picture via: http://www.loyaltyandretention.com/wp-content/uploads/2012/10/Communicating.jpg

• Monitor your quality improvement
• Stay current with developments in other programs
• Publicize your achievements.
(CDC, 2014)
IV. Refining and Promoting
Picture via: http://primarycaredigest.org/2014/09/19/new-program-supports-quality-improvement-through-practice-facilitation/
Step 9: Monitor and Update Your Plan
• Seek front-line feedback
• Set specific time intervals to evaluate your program
• Keep up on research
• Learn from others
(CDC, 2014)Picture via: http://elicitator.uncertweb.org/

Step 10: Share Your Success
Who to share your success with:
• Your organization’s leaders• Local community leaders,
organizations, and citizens• Members of regional and national
organizations committed to quality medical services and advancing alcohol SBI
(CDC, 2014)Picture Via: http://www.rimt.ac.in/sharestory.html

References
Centers for Disease Control and Prevention. Planning andImplementing Screening and Brief Intervention for Risky Alcohol Use: A Step-by-Step Guide for Primary Care Practices. Atlanta, Georgia: Centers for Disease Control and Prevention, National Center on Birth Defects and Developmental Disabilities, 2014.
Implementing Alcohol Screening and Brief Intervention (SBI) with Alaska Section of
Public Health Nursing
Supported by: CDC Cooperative Agreement #U84DD000886-01

Why Should Public Health Nurses Implement Alcohol SBI?• Public Health Nurses are in an ideal position to
reach/identify patients who drink at risky levels and provide brief education or intervention.
• Alcohol SBI Fits with public health objectives to reduce health risk through population-based approaches.
• Alcohol use contributes to increased STD rates, domestic violence, unplanned pregnancies, and FASDs, as well as higher risk for chronic conditions (hypertension, cancer).
• Risky use can be identified in 1-3 screening questions.
• 5 minutes of provider-focused counseling has been proven to reduce patients’ alcohol use over sustained periods.

Adoption of evidence based interventions requires systems-level changes, which in turn require planning and commitment of resources
Healthcare systems/providers willing to adapt their processes
Researcherswilling to adapt EBIs so they are feasible yet still effective
The literature has identified two essential ingredients to implementing practice change:

CDC-funded Opportunity: Project Goals
• Partner with a multi-clinic healthcare system that provides primary care services, to implement and evaluate alcohol SBI
1. Incorporate SBI into day-to-day clinical care
2. Identify barriers and facilitators
3. Create solutions to identified barriers
4. Evaluate the uptake of SBI in pilot sites
• Utilize CDC Draft SBI Implementation Guide

Participating partners
• Arctic FASD Regional Training Center (CBHRS, UAA) received a two-year award from CDC.
• Alaska Section of PHN: 24 public health centers plus itinerant nurses who support over 280 Alaska Native villages across the state.
• 3 PHN health centers (two urban and 1 rural)participated in the pilot.

What we did (Timeline of steps)
• Obtained organizational commitment from PHN Section Chief and Leadership team (March 2013)
• Formed a Planning team (April 2013)• PHN quality improvement, informatics, training, nurse providers and
managers, and UAA research team
• Decided on screening, brief intervention, referral and documentation processes (May 2013)• Selected Screeners: T-ACE plus two NIAAA questions (CRAFFT for
adolescents)• Designated Eligible Visits: Gyn, Family Planning, Prenatal, Postpartum, STI,
TB• Designated staff roles:
• Who screens, who scores; where and when? • Who delivers intervention; and when?
• Designed patient education materials/provider pocket guides and resources
• Drafted SBI policy and procedure and distributed it to 3 pilot sites

What we did (Timeline, continued)
• Trained health center staff at 3 pilot sites (June 2013)
• Conducted a pilot/collected data (July 2013-September 2014)• Providers entered screening outcomes and contact notes in health records.• Research team provided TA during regularly scheduled calls with pilot sites.• Research team documented implementation process, provider feedback,
and conducted key informant interviews with diverse PHN staff.
• Refined P&P throughout, shared data, implemented ideas
• Finalized P&P and Trained all PHNs to conduct alcohol SBI

Data Collected
• Reach (# of eligible patient visits receiving screening)• Effectiveness (# of positive patients receiving a brief
intervention or referral)• Implementation process (used to monitor fidelity and
refine protocols)• Screening rates monitored throughout the study• Chart reviews • Field Notes from ongoing practice facilitation calls• Key Informant Interviews
• Sustainability• Provider satisfaction, perceived feasibility/effectiveness• Formal policy and procedure for SBI• Ongoing quality metrics and opportunities for staff training
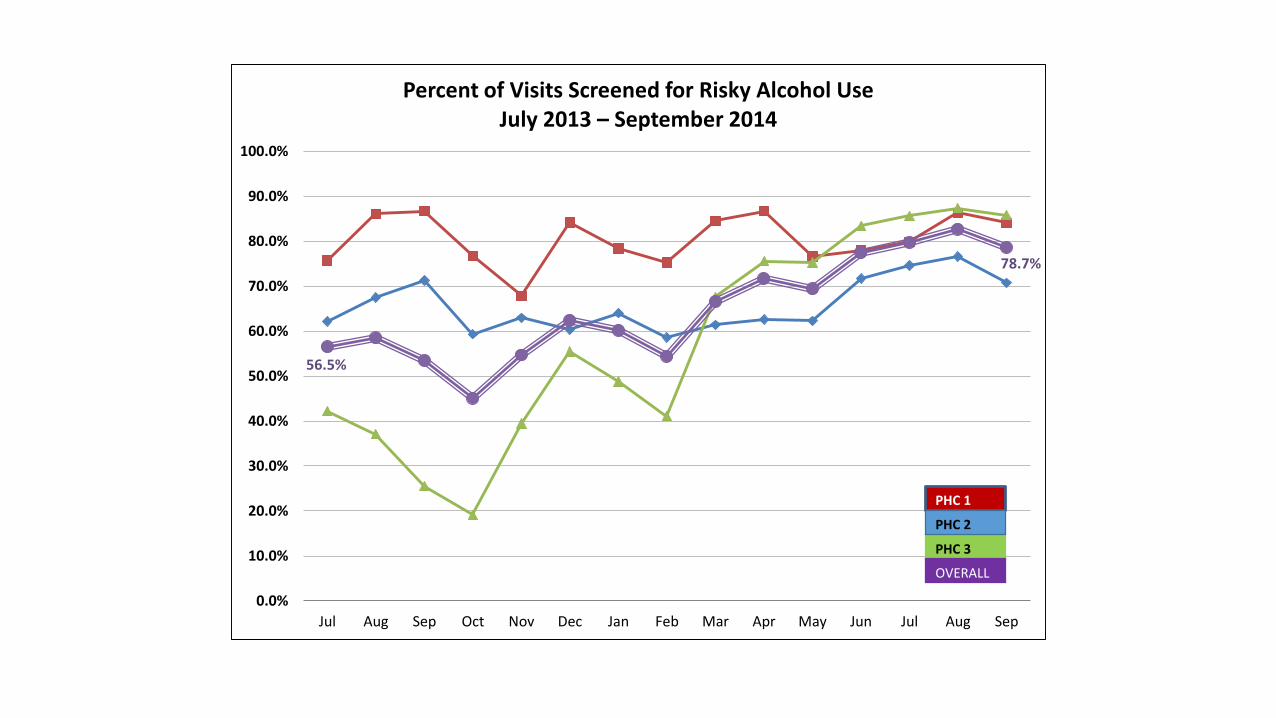
56.5%
78.7%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep
Percent of Visits Screened for Risky Alcohol UseJuly 2013 – September 2014
PHC 1
PHC 3
OVERALL
PHC 2

23.6%
32.4%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep
Percent of Screenings that Scored Positive for Risky Alcohol UseJuly 2013 – September 2014
PHC 1
PHC 3
OVERALL
PHC 2
Implementation Process - get started
• Skills competence and confidence with SBI varied following training
“…I think that [onsite training] made a difference in how easy it was for folks to incorporate it.” [nurse interview]
“It’s all about approach. Incorporate it as a part of the conversation.” [training observation]
“…trying to figure out a good way to talk about problem drinking or to talk about why we're asking all these questions. That can kind of take a little bit of thinking and just trying to figure out the best way to approach it for each person.” [nurse interview]
“We should be asking these questions. I think it's right in there with our usual screenings or questions that we ask people regarding their well being and health habits.” [nurse interview]

Implementation Process – identify and address unforeseen issues quickly• Documenting positive screens in patient charts met
with some initial concern and resistance.
“Uncomfortable with the terminology- sounds too incriminating if records were released.” [nurse, during a facilitation call]
“Let the people who actually work with clients decide what the wording should be.” [nurse, during a facilitation call]
• Identified needs for continuous process improvement and skills practice/booster training
“I think it was the intervention piece that was, that's still the hardest part of it all.” [nurse interview]
“…my comfort level is getting stronger with more practice.” [training observation]
Implementation Process – monitor fidelity, provide support

Implementation Process – update plans, integrate recommendations
• Competence and confidence improved over time
“I think initially it was challenging just because it was a change and it was a new form and a new way to question people. It’s gotten a lot easier as we’ve used it.” [nurse interview]
“I have more tools to use.” [nurse, during a facilitation call]
• Adapting and refining a draft P&P encouraged acceptance.
“I think it was helpful to see the process adapt as it went on, and that really empowered people for realizing that their experience and their voice did matter. And the process didn’t change significantly as we went along, but there were improvements made. I think people felt that by the time it rolled out system-wide, it was a better process than it was when we started it as a pilot.” [nurse manager interview]
Implementation Process – Success stories
• Regarding a client in STD clinic…“…we did the ETOH screen and talked briefly about family history. Apparently it hit a nerve because she returned to clinic 2 months later and saw a different nurse. She told him she had really taken the counseling to heart and was at that time 29 days sober. It was definitely a ‘brief’ intervention, but for her it had an impact!”
• Adolescent female client reported, “I don’t drink, I don’t do drugs.” Through screening the nurse found the client had a history of heavy alcohol use and was currently sober. The nurse mentioned she would not have learned about this information if SBI had not occurred.
“It really IS in HOW you ask the questions.”
Alaska PHN Today– alcohol SBI still going strong!• As of October, 2016, policy still in place, actively monitoring quality:
• 73-78% eligible visits screened • 7% of eligible visits deferred (goal is <5%)• 27-32% of eligible visits screened positive• However, 15-20% of eligible visits incomplete (i.e., no documentation of screening or
deferment; investigating this)
• What contributed to sustaining alcohol SBI?• Planning incorporated knowledge of what worked for other screenings (e.g., Domestic
Violence; meaningful reporting)• Piloting in a few PHC’s to figure out the glitches• Pilot led to development of supportive tools, refinement of policy• PHNs knew about pilot and that alcohol SBI was coming• Education and videos were put in place, so all new nurses get the same training

Final Points
• Alcohol SBI is a feasible, effective public health approach • provides a low-intensity, low-cost clinical prevention service • used to identify and intervene with people who drink too much• Many who receive alcohol SBI respond positively and will reduce risks over time
• Clients not only asked about alcohol, but nurses have to talk to them about it, document, and follow-up
• Focus of BI on harm reduction, empowered nurses to intervene, reduce need to refer to treatment
• Implementing alcohol SBI requires planning and input from all levels of staff
• Drafting a written policy and procedure, that is piloted and refined prior to roll-out, enhances likelihood of success and sustainability
• Ongoing monitoring of adherence to screening protocols and improvement of brief intervention skills is key to assuring maximum reach and impact.

Acknowledgements
• Centers for Disease Control (project funder);
• Rhonda Richtsmeier, MN, RN (retired section chief), State of Alaska Public Health Nursing
• Linda Worman, DM, RN (current section chief), State of Alaska Public Health Nursing
• Arctic FASD-RTC project team, Becky Porter, project manager
• Marilyn Pierce-Bulger, ANP, CNM, project consultant and trainer

Position Statement on the Prevention of Alcohol Exposed
Pregnancies

Why do organizations develop position statements ?
• Address an identified issue relevant to mission statement and vision/goals
• Educate stakeholders about an issue
• Increase visibility as a leader concerning the issue
• Provide documentation of recommended actions to assist in obtaining support for related project/projects
• Provide documentation of recommended actions to assist in ongoing evaluation of achievements
NPWH’s Mission is to ensure the provision of quality primary and specialty health care to women of all ages by women’s health nurse practitioners and other women’s health focused advanced practice registered nurses. Our mission includes protecting and promoting a woman's right to make her own choices regarding her health within the context of her personal belief system.
NPWH’s Vision is to strive to continuously improve access and quality of health care for women. This will be accomplished through excellence and innovation in continuing education and professional development; leadership in policy, practice and research; and through support and services for our members.
Writing Position Statements –Initial Challenges
• Our BOD, CEO, and staff are dedicated to NPWH’s mission and vision
• Our BOD, CEO, and staff are very, very busy
• We needed to agree on issues that should take highest priority
• We needed a plan for coordinating the process
Why Prevention of Alcohol Exposed Pregnancies?
WHNPs see reproductive age women who are –
• sexually active and not planning a pregnancy
• planning to become pregnant
• pregnant
CDC Planning and Implementing Screening and Brief Intervention for Risky Alcohol Use: A Step-by-Step Guide for Primary Care Practices published in 2014
Opportunity to build partnerships with others with similar interests/goals

Developing Position Statements - Membership Engagement
Position Statement
Writing Group
Reviewers
Public Comment
Board of Directors
Our Position Statement Format • Statement of position
• Background information
• Implications for members and those they serve
• Recommendations for practice and advocacy
• Action organization will take to provide leadership and resources
• References
• Another challenge - Keeping it brief!

Step 1: The Writing Group
• Writing group recruitment
• Preparation of ‘working’ draft for the writing group
• Additional resources/references obtained from writing group members
• Back and forth review and revision process

Step 2: Reviewers
• Recruitment of experts on the issue outside the organization
• Clinical specialists – interdisciplinary
• Relevant national agency representatives
• Healthcare professionals involved in national level projects on the issue

Step 3: Public Comment
NPWH Members and Affiliates

Step 4: NPWH Board of Directors Approval
Does the position statement support the mission and vision of NPWH?

Getting Our Position Statement Out There
• Website
• Organization publications
• Conference and other meeting presentations
• Distribution to relevant policy makers and other organizations
• Virginia Henderson E-repository
Does a position statement make a difference?Done
Survey of members prior to release of position statement regarding knowledge, skills, attitudes, behaviors related to the issue
To Do
• Survey of members after release of position statement
• Collect data on types and number of stakeholders reached through dissemination venues
• Collect data on achievement of recommendations

Our Survey
• N = 216
• What We Learned
•

% who responded frequently or always –
How often do you ask about alcohol use in your patients who are:
• sexually active and do not want to get pregnant in the next year, but are at risk for pregnancy? 72%
• planning a pregnancy within the next year? 84%
• are pregnant? 90%
64% have a protocol in place in their practice to screen all patients for their alcohol use.

% who answered very / completely confident in their skills to -
• ask women, including pregnant women, about their alcohol use. 87%
• identify levels of alcohol use considered risky in women. 69%
• conduct brief interventions for reducing alcohol use. 41%
• educate pregnant and non-pregnant women of reproductive age about the effects of alcohol on a developing fetus. 76%

% who agreed / strongly agreed with these statements
• Risky levels of drinking alcohol in women are considered to be > 4 drinks per occasion or > 7 drinks per week. 85%
• It is important to screen all pregnant women for alcohol use. 96%
• It is important to screen all women of reproductive age for alcohol use. 95%
• It is important to educate pregnant and non-pregnant women of reproductive age about the effects of alcohol on a developing fetus. 95%
• Alcohol is a teratogen. 95%

Next Steps • Webinars to address identified gaps in knowledge
and skills
• Continue to develop partnerships
• Development of other education and practice strategies to facilitate clinicians in their efforts to prevent of alcohol exposed pregnancies
• Evaluate outcomes

“If we did all of the things we are capable of doing, we would literally astonish ourselves.”
Thomas Edison

Questions & Comment

Celebrating 80 Years of Public Health Nursing
THANK YOU!
For further information on this Webinar and other programs offered by the
Association of Public Health Nurses, please go to:
www.phnurse.org
or call us at 614-846-1777
You can also reach us by email at:
or





























