Embed Size (px)
Citation preview

The challenge of developing new TB vaccines
Paul-Henri LAMBERTCentre of VaccinologyUniversity of Geneva
ADVAC 2009

Tuberculosis: the global figure
WHO 2007
about 2 billion individuals infected with M.tb9.273 million new tuberculosis cases/year (20%MDR, 2%XDR)1.772 million deaths / year (2/3 Afr. + S-E Asia)

Tuberculosis: the global MDG goals
1990 2015 1990 2015 1990 2015
WHO 2007
by 2015: reduce death rates by 50% vs 1990

Time
persistence
Bact
erial
load
TB- Infection profile
Naive host

Time
persistence
Bact
erial
load
Naive host
Early protection in children (used in >2 billion infants)
BCG

Time
persistence
Bact
erial
load
Naive host
Early protectionIn children
BCG•Variable efficacy in adolescents and adults; •little impact on TB epidemiol.

-20 0 20 40 60 80 100
UK, BIRMINGHAM
CANADA Indians
NORWAY, gen popn
HAITI
SWEDEN, gen popn
USA, Indians
USA, NEW YORK infants
UK, schoolchildren
UK, gen popn 1983
SOUTH AFRICA, miners
SWEDEN, military
ISRAEL, children
INDONESIA JAKARTA
PUERTO RICO
INDIA MADANAPALLE
MALAWI KARONGA
INDIA CHINGLEPUT
CohortC. Trial
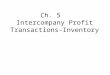
Published estimates of efficacy of BCG against pulmonary tuberculosisP. FineLancet 1995; 346: 1339-45

Time
persistence
Bact
erial
load
Naive host
Early protectionIn children
BCG
•Poor efficacy in adolescents and adults; little impact on TB epid.
•Reduced efficacy if previous exposure to environmental-mycob.

Time
persistence
Bact
erial
load
Naive host
Early protectionIn children
BCG
•Poor efficacy in adolescents and adults; little impact on TB epid.
•Reduced efficacy if previous exposure to environmental-mycob.
•Risk of disseminated BCG disease in HIV infected children


Data for Cape Town children less than 2 years of ageTB incidence: 860/100’000 person-yearsTBM & MTB incidence: 61 / 100’000 person-yearsMahomed et al. Ped Infect Dis J. Dec 2006
417 / 100’000
Risk scenarios of disseminated BCG disease

BCGPros
• most used vaccine at global level
• very low cost
• recognized protective efficacy against infanttuberculosis(e.g. TB-meningitis, MTB)
Cons
•Poor efficacy in adolescents and adults;
•Reduced efficacy if previous exposure to environmental mycob.
•Risk of disseminated BCG disease in HIV inf. children

M tb
Mycobacterium tuberculosis (M tb)
Strategies towards new TB vaccines

Candidate vaccinesLive mycobacteriaLive vectorsProteins + Th1 AdjGlycolipids
From Kaufmann SH & McMichael AJ. (2005) Nature Medicine 11, S33 - S44
New TB vaccines desirable immunological target


persistence
Bact
erial
load
Time
1 2
New TB vaccinesA- Pre-exposure vaccines
(1) more rapidly effective than BCG (2) more efficient bacterial clearance(3) less susceptible to previous mycobacterial exposure

persistence
Bact
erial
load
Time
1 23 4
(3) to reduce the persistent bacterial load (4) To prevent re-activation of latent Mtb
New TB vaccinesB- Post-exposure vaccines
C- Multi-stage vaccines?

1- Genetically engineered live TB vaccines
BCG
Improved rBCG
Increase expression of protective gene(s)
Add genes to improve immunogenicity (CD8) & safety
a- Modified BCG

1- Genetically engineered live TB vaccines
BCG
Improved rBCG
Increase expression of protective gene(s)
Add genes to improve immunogenicity (CD8) & safety
rBCG30 Increased expressionof 30-kDa
Horwitz
BCG::RD1 Expression of Mtb ag Cole
rBCG-ΔUreC:Hly+
Expression of Listeria cytolysin
KaufmannGrode
rBCG-AERAS403
Expression of Perfringolysin + Ag85&TB10.4
AERAS
a- Modified BCG
To be used as BCG-replacement vaccines

Candidate -vaccines Developer
Initial cGMP
Production
Regulatory Assessm.
Phase IClinical Trials
Estimated Phase 3 initiation
rBCG-Hly
VPM2005-06 2007-08 2008-09 2013
rBCG(rBCG-ΔUreC:Hly+)
BCG antigens escape from endosome to cytoplasm: increased immunogenicity & safety
rBCG-ΔUreC:Hly+

Candidate -vaccines Developer
Initial cGMP
Production
Regulatory Assessm.
Phase IClinical Trials
Estimated Phase 3 initiation
rBCG-Hly
VPM2005-06 2007-08 2008-09 2013
rBCG-ΔUreC:Hly+
Protection against M. tb Beijing/W (mice)
ΔureC hly+ rBCG
parental BCG
Challenge 200 CFU “Beijing“ 120 d post vaccination)
Grode L. & al. , J Clin Invest 2005

1- Genetically engineered live TB vaccines
M tb
Attenuated rMtb
Delete virulence genesfrom Mtb
Identify virulence genes
b- Attenuated Mtb

1- Genetically engineered live TB vaccines
M tb
Attenuated rMtb
Delete virulence genesfrom Mtb
Identify virulence genes
M. tb PhoPmutant
Deletion PhoP virulence genes
Martin
M. Tb mc2
6020/30 mutant
Deletion LysA+panCD or panCD+RD1 virulence genes
Jacob
b- Attenuated Mtb
Appears efficient and safe in pre-clinical studies

The live Mycobacterium tuberculosis phoP mutant strain is more attenuated than BCG and confers protective immunity against tuberculosis
in mice and guinea pigs. Martin C, et al. Vaccine 2006 Protective efficacy in guinea pigs
Mtb phoP mutant
phoP mutant
BCG
High safety profile in SCID micephoP mutant
Lung
Spleen
phoP mutant
High dose Mtb H37Rv challenge @ 10wks

POTENTIAL ADVANTAGES MAIN ISSUES
Relatively easy to produce Mutant strain stability, QC?
Will benefit from BCG experience Must be at least as safe as BCG (including HIV infected people)
For initial protection & for priming
Have to appear significantly betterthan BCG
May exert adjuvant effect for concomitant vaccines
Ethical issues re: clinical assessment
Live mycobacterial vaccines

POTENTIAL ADVANTAGES MAIN ISSUES
Relatively easy to produce Mutant strain stability, QC?
Should benefit from BCG experience Must be safer than BCG in HIV infectedand immunocompromised
For initial protection & for priming Should be at least as good as BCG
May exert adjuvant effect for concomitant vaccines
Some ethical issues re: clinical trials
Live mycobacterial vaccines

2- New Sub-unit TB vaccines
Clone relevant genesM tb
Mycobacterium tuberculosis (M tb)
Identify « protective » antigens
To prime or boost BCG-induced
immunity
Sub-unit vaccinesProtein(s) + adjuvant
Live vectors

Candidate -vaccines Vaccine antigens
Ag85B-ESAT6 (H1)+ IC-31
SSI
MVA-Ag85A, live vector
U-Oxford
Mtb72recAg + AS-02
GSKBE
Leading sub-unit TB vaccine candidates
Mtb orBCG
Protein(s) + adjuvant
Live vector + Mb-ag
Clone relevant genes(« protective » antigens)
Ra35TbH9 39 kDaRa12
34 kDa -Serine protease
Mycolyl transferase
MVA expressing Ag85A
ESAT-6Ag85BMycolyl transferase Mtb- spec ag

Candidate -vaccines Vaccine antigens CT
Ag85B-ESAT6 (H1)+ IC-31
SSI - IC 1
Ag85B-TB10.4 (H4)recAg + IC-31
SSI-Sanofi-P 1
MVA-Ag85A, live vector
U-Oxford 2
Adeno35-Ag85A-B-TB10.4
Crucell 1
Mtb72recAg + AS-02/01
GSK1-2
Leading sub-unit TB vaccine candidates
Mtb orBCG
Protein(s) + adjuvant
Live vector + Mb-ag
Clone relevant genes(« protective » antigens)
Ra35TbH9 39 kDaRa12
34 kDa -Serine protease
Mycolyl transferase
MVA expressing Ag85A
ESAT-6Ag85BMycolyl transferase Mtb- spec ag
TB10.4Ag85BBCG- spec ag
Ad 35 vector + Ag85 + TB10.4

Discovery
Pre-clinicalefficacy
GMP-Production
Non-clinicalsafety
INDfile
Effective protection (mice , g-pigs, N-hu Prim)
Lot consistency-- Formulation
Incl. neonatal. TOXstudies
As RQ by RA
Ph1 Trials Safety / immunogenicityadults (in area of production)
PPD neg BCG primed LTBI or treated TB

Discovery
Pre-clinicalefficacy
GMP-Production
Non-clinicalsafety
INDfile
Effective protection (mice , g-pigs, N-hu Prim)
Lot consistency-- Formulation
Incl. neonatal. TOXstudies
As RQ by RA
Ph1 Trials Safety / immunogenicity adults (in area of production)
PPD neg BCG primed LTBI or treated TB
Ph2a- Safety / immunogenicity ados. + infants
Adults/Ados Infants [Formulation. Bridg.]
Interference studies
HIV pos ados/infants
Ph1-Safety / immunogenicity adults (high endemicity area)
PPD neg & BCG primed LTBI
Phase IIb Phase III
Adults/ados infant Adults/ados infants

Discovery
Pre-clinicalefficacy
Effective protection (mice , g-p, N-hu P)
Ag85B-ESAT6 + IC31 (H1)SSI + IntercellDK-AT
ESAT-6Ag85B

Ag85B-ESAT6Non-vaccinated
Lymph node destruction
Lung granuloma
Reduced TB pathology in vaccinated cynomolgus monkeys
Langermans J, Vaccine. 2005 ;23(21):2740-50

Discovery
Pre-clinicalefficacy
GMP-Production
Non-clinicalsafety
INDfile
Effective protection (mice , g-p, N-hu P)
Lot consistency-- Formulation
neonatal & immunocomp.
TOXstudies
As RQ by RA
Safety / immunogenicity(EU- adults)
PPD neg PPD pos LTBI
Ag85B-ESAT6 + IC31 (H1)SSI + IntercellDK-AT
ESAT-6Ag85B

Phase 1 –trial in PPD-neg 2006-07 Leiden- NL
Immunogenicity:excellent primary response
Safety: very low reactogenicity
0
1000
2000
30003000
15000
pg/m
l
-2 0 6 12 32
Ag85B ESAT6 H1
-2 0 6 12 32-2 0 6 12 32weeks
IFNγ ELISA
-2 0 6 12 320
250
500
750
Ag85B ESAT6 H1
IFNγ
SFU
/ 106
PBMC
-2 0 6 12 32-2 0 6 12 32weeks
IFNγ ELISPOT
Resp. to:
Ag85B-ESAT6 + IC31 (H1)SSI + IntercellDK-AT
ESAT-6Ag85B
It is unlikely that H1 vaccination would interfere with ESAT6-based diagnostic (QFT)

Discovery
Pre-clinicalefficacy
GMP-Production
Non-clinicalsafety
INDfile
Effective protection (mice , g-p, N-hu P)
Lot consistency-- Formulation
neonatal & immunocomp.
TOXstudies
As RQ by RA
Safety / immunogenicity(EU- adults)
PPD neg BCG primed
LTBI or treated TB
Ph1-Safety / immunogenicity(AFR- adults)
PPD neg & BCG primed LTBI
Ag85B-ESAT6 + IC31 (H1)SSI + IntercellDK-AT
ESAT-6Ag85B

Discovery
Pre-clinicalefficacy
GMP-Production
Non-clinicalsafety
INDfile
Effective protection (mice , g-p, N-hu P)
Lot consistency-- Formulation
immunocompr. TOXstudies
As RQ by RA
Safety / immunogenicity(EU- adults)
PPD neg BCG primed LTBI
MVA-Ag85A U-OXF + IDTUK + DE
MVA live vectorexpressing Ag85A
from H McShane & al., Nature Medicine 10, 1240 (2004)
0 4 12 24
BCG + MVA85A
MVA85A
0
250
500
750
SFC/
1x10
6PB
MC
Response to: Ag85Aweeks
IFNγ-ELISPOT
Phase 1 trial in PPD negMVA85A alone or BCG + MVA85A
Immunogenicity:excellent primary responseVery good boosting effect (12 yrs!)
Safety: low reactogenicity

Discovery
Pre-clinicalefficacy
GMP-Production
Non-clinicalsafety
INDfile
Effective protection (mice , g-p, N-hu P)
Lot consistency-- Formulation
neonatal & immunocomp.
TOXstudies
As RQ by RA
Safety / immunogenicity (EU- adults)
PPD neg BCG primed
LTBI or treated TB
HIV infected
Ph2a-Safety / immunogenicity ados. + infants (AFR)
Ados/ Infants Age de-escalation
Dose escalation
Interferencestudies
HIV infected ados/infants
Ph1- Safety / immunogenicity(AFR- adults)
PPD neg & BCG primed LTBI HIV infected
MVA-Ag85A U-OXF + IDTUK + DE
MVA live vectorexpressing Ag85A

Discovery
Pre-clinicalefficacy
GMP-Production
Non-clinicalsafety
INDfile
Effective protection (mice , g-p, N-hu P)
Lot consistency-- Formulation
neonatal & immunocomp.
TOXstudies
As RQ by RA
Ph1- Safety / immunogenicity(EU- adults)
PPD neg BCG primed
LTBI or treated TB HIV
Mtb72 + AS-01/2GSKBE
Ra35TbH9 39 kDaRa12

BCG+VAC BCG only
0 60 90 240 0 60 90 240
0
200
400
600
800
1000
1200
1400
1600
1800
Median
Vaccination with Mtb72F in BCG-primed and Mtb-exposed individuals (Lausanne/ TBVAC)
• Highly immunogenic (boosting)
• Safe with acceptable local reactogenicity in BCG-primed individuals
Mtb72F-specific cellular responses (IFN-γ ELISPOT)Mtb72F + AS-02
GSKBE
Ra35TbH9 39 kDaRa12

Discovery
Pre-clinicalefficacy
GMP-Production
Non-clinicalsafety
INDfile
Effective protection (mice , g-p, N-hu P)
Lot consistency-- Formulation
neonatal & immunocomp.
TOXstudies
As RQ by RA
Ph1- Safety / immunogenicity (EU- adults)
PPD neg BCG primed
LTBI or treated TB
HIV infected
Ph1-Safety / immunogenicity(AFR- adults)
PPD neg & BCG primed
LTBI HIV infected
Mtb72 + AS-01GSKBE
Ra35TbH9 39 kDaRa12

POTENTIAL ADVANTAGES MAIN ISSUES
-Good for boosting - would benefit from neonatal exposure to BCG
Subunit mycobacterial vaccines

Prior exposure to environmental mycobacteria interferes with the protective effect of BCG
but not of a subunit vaccine
0
0.2
0.4
0.6
0.8
1
1.2
1.4
NoneBCGAG85-ESAT6
PROT
ECTI
VE E
FFEC
TLo
g 10
resis
tanc
e
no pre-exposure
env-mycpre-exposure
From Peter Andersen, SSI, Copenhagen ADVAC 9

POTENTIAL ADVANTAGES MAIN ISSUES
-Good for boosting - would benefit from neonatal exposure to BCG
- Safe in immunocompromised- May be combined with othervaccines
Subunit mycobacterial vaccines
- Single dose (live vectored vaccines)

POTENTIAL ADVANTAGES MAIN ISSUES
-Good for boosting - would benefitfrom neonatal exposure to BCG
- Cost? Not really …- Need for adjuvant (protein vacc.)
- Safe in immunocompromised- May be combined with othervaccines
- Risk of pathology enhancement? Koch phenomenon in previouslyinfected individuals?
Subunit mycobacterial vaccines
- Single dose (live vectored vaccines)
- Single use of live vectoredvaccines

DISCOVERY
DOWNSTREAMDEVELOPMENT
New Antigens
HBHAHeparin-binding Hemagglutinin ( IP-Lille)
e.g. Diacylated Sulfoglycolipids(CD1-restricted)(G Puzzo)
Latency TB antigens
e.g. Rv2660 -SSI

Combined strategies?
rBCG or att-Mtb priming

Combined strategies?
Ag85A or Ag85B or M72 boosting
(+/- TB10.4 / ESAT6)
rBCG or att-Mtb priming

Combined strategies?
Latency ag
Ag85A or Ag85B or M72 boosting
(+/- TB10.4 / ESAT6)
rBCG or att-Mtb priming

Combined strategies?
Lipid?
Latency Ag
Ag85A or Ag85B or/& M72 boosting
(+/- TB10.4 / ESAT6)
rBCG or att-Mtb priming

New TB vaccination Strategies1- adding on BCG
Pre-exposure vaccines
Leve
l of I
mm
unity
(T-c
ells)
Boostimmunity
(infant or ado)BCG
priming(infant)

New TB vaccination Strategies2- improving priming?
Pre-exposure vaccines
Leve
l of I
mm
unity
(T-c
ells)
rBCGpriming(infant)
Boost with sub-unit latency
vaccine?
Post-exposure vaccines
Boost(infant or ado)
e.g.M72
MVA85AH1/4-IC31