Embed Size (px)
DESCRIPTION
The Changing Healthcare Environment: 1115 Waiver Implementation in Texas. Alliance for Healthcare Excellence Dr. Ron Anderson, M.D Sue Pickens, M.Ed. Waiver Goals Expand risk-based managed care statewide. Support the development and maintenance of a coordinated care delivery system. - PowerPoint PPT Presentation
Citation preview

The Changing Healthcare Environment:
1115 Waiver Implementation in Texas
Alliance for Healthcare ExcellenceDr. Ron Anderson, M.D
Sue Pickens, M.Ed.

1115 Waiver
• Waiver Goals • Expand risk-based managed care statewide. • Support the development and maintenance of a coordinated care delivery system. • Improve outcomes while containing cost growth. • Protect and leverage financing to improve and prepare the health care infrastructure
to increase access to services. • Transition to quality based payment systems in managed care and in hospital
payments. • Provide a mechanism for investments in delivery system reform including improved
coordination in the current indigent care system in advance of health care reform.
2

1115 Waiver
• Waiver’s impact is state and local, rather than federal • Works whether the healthcare reform law remains
intact or not• Milestones
• Expansion of primary care
• Behavioral health goals
• Specialty care access goals
• DSRIP and UC more than doubles the former UPL annual payment
3

1115 Waiver
• Under the waiver, additional new funds are distributed to hospitals through two pools:• Uncompensated Care (UC) Pool : Costs of care provided to
individuals who have no third party coverage for the services provided by hospitals or other providers (beginning in first year).
• Delivery System Reform Incentive Payments (DSRIP): Support coordinated care and quality improvements through Regional Healthcare Partnerships (RHPs) to transform care delivery systems (beginning in later waiver years).
4

Proposed RHP Map
5

1115 Waiver – CMS Expectations
CMS Expectations• Planning process that demonstrates regional collaboration.
• Projects selected address community needs identified through a Community Needs Assessment (DFWCH)
• Projects selected are the most transformative for the region.
• RHP Plan includes projects that tie into four categories established y HHSC to demonstrate outcomes• Infrastructure• Innovation• Quality• Reporting
6

Uncompensated Care Pool
• Anchor Hospital (IGT Entity) – Provides funds to HHSC for match
• Hospitals apply directly using a state designed tool to receive UC payments to include:
• Physician costs related to direct patient care services
• Mid-level professional costs related to direct patient care services
• Pharmacy costs related to he “Texas Vendor Drug” program
• Excess “Medicaid DSH” costs not reimbursed via the Medicaid DHS program
• Specific tool for submitting reimbursement provided by HHSC through TexNet (not yet available)
7

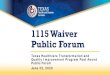
DSRIP Pool – Funding Flow
8
• Public Hospital• In areas with no public hospital:
• Hospital District• Hospital Authority’• County• State University with HSC or medical school
AnchorRHP
Administrative Functions
HHSCApproves
performance
IGT Entity Reviews
performance
Performing Provider Reports
Performance
Performing Subcontractor Reports performance to
performing provider
Examples: Examples:Public Hospital Public HospitalPublic Hospital Private HospitalPublic Hospital Private Hospital Clinic LMHA LMHA
HHSC
Requests IGT from IGT Entities
IGT Entity Provides IGT to
the State
HHSCRequests federal match from CMS
HHSCProvides payments to performing provider
CMSApproves Federal
match and sends to HHSC
Performing ProviderReceives payments
Performing Subcontractor
Receives payments from performing
provider.

Texas Healthcare Transformation and Quality Improvement Program
Section 1115 Waiver ProgramRegion 9 RHP Organization Ensuring Regional
Collaboration
Centers for Medicare and Medicaid Services (CMS)
Delivery System Redesign Incentive Pool Task Force
Co-ChairsRon Anderson MD and David
Ballard MD
Oversight Work GroupCo-Chairs
Tom Royer MD and Joel Allison (Dr. Royer was replaced by Ted Shaw)
Dallas Medical Resource
Regional Healthcare Partnership (RHP)
Dallas County Hospital District
Board of Managers (DCHD – Dallas Anchor)
Texas Health and Human Services Commission
(HHSC)
Uncompensated Care Pool Task ForceCo-Chairs
John Dragovits and Fred Salvelsbergh (John Dragovits
replaced by Jody Springer)
1115 Waiver Steering Committee
Tom Royer MD (Dr. Royer replaced by Ted Shaw)
Committee replaced with the Plan Writing
Committee
Anchors development of the Dallas RHP and the RHP Plan:Develops the Dallas RHP Plan Designates Dallas Regional
Healthcare Partners (Dallas RHPs) Performs a community needs
assessment that serves as basis for the RHP plan
Approves Dallas Intergovernmental Transfer (IGT) contributions
Approves selected Dallas regional DSRIP projects from the State approved menu of projects
Allocation of funds to UC and DSRIP projects
Provides an opportunity for public input and review of the RHP Plan
Provides ongoing Dallas RHP plan administration and reporting.
Develop Dallas Regional Health Partnerships Plan: •Designating Dallas Regional Healthcare Partners•Community Needs assessment•Identify and approve IGT contributions •Approve selected Dallas regional DSRIP projects•Approve allocation of funds to UC and DSRIP projects•Provide opportunity for public Input and review of the RHP Plan•Ongoing Dallas RHP Plan administration and reporting
Partner with DCHD to develop the Dallas RHP and RHP Plan:•Serve as a forum for the work group and task forces to develop required elements for the RHP/RHP plan.•Assure range of Dallas stakeholders are involved •Assist in project management and ensure project transparency•Assist in coordinating Dallas’ input to DHHS on statewide elements of waiver program
A work group designated by DMR and DCHD will serve as the project steering committee responsible for:• Developing recommendations to the DCHD Board of Managers on the Dallas Regional Healthcare Partners Plan

Regional Healthcare Partnership Committees
Elected LeadersCounty Judges other elected officials responsible for IGT entities
SteeringCEOs of Local & Regional participant Hospitals, MHMR and School of Medicine
PlanningPlanning officers of participant Hospitals, MHMR, Public Health and School of Medicine
Finance (IGT and UC)Finance officers of participant Hospitals, MHMR and School of Medicine
Quality/ClinicalQuality/Medical officers of participant Hospitals, MHMR, Public Health, School of Medicine, Medical Associations
Region 10DRAFT Regional Healthcare Partnership Planning Approach
April May June July August September October
• Stakeholder engagement
• RHP Committee formation
• Centralized community Needs Assessment workshops• Provide Community Needs Assessment templates, baseline
data, guidance and technical assistance• Provide DSRIP parameters, metrics and guidance per THHSC &
RHP (if allowed)
• Develop individual County Community Needs Assessments
• Conduct individual County Visioning Sessions• DSRIP coordination, development & evaluation
process
• Develop RHP-wide Community Needs Assessment
• Begin RHP Plan Development• Community forums for plan review• Finalize DSRIP plans
• Draft plans to THHSC 8/1
• Draft plans to CMS 8/31
• Review/ update plans based on feedback
• Final plans to CMS
Regional Healthcare Partnership Planning
Today (April 20 2012) 6 Month Year 1 Year 2 Year 3 Year 4 Year 5+
Regional Healthcare Partnership Collaborative “Governance” Guiding Principles
Transparency Patient-Centered Collaborative Value-Driven Accountability
Ensure that decision making process takes place in the public eye and that processes are clear to participants
RHP and criteria should focus on improving patient care & experience through more efficient, patient-centered and coordinated system
RHP informed by collaborative process that reflects the needs of the community(s) in inputs of stakeholders
RHP should focus on increasing value to patients, community, payers and other stakeholders. Better Care, Less Cost
Stakeholders are held to common performance standards, deliverables and timelines
Texas Healthcare Transformation and Quality Improvement Program
Section 1115 Waiver ProgramRegion 10 RHP Organization Ensuring Regional
Collaboration

Page 11
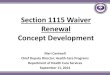
Pool Funding Distribution
Transformation is the Goal
Pool Funding Distribution in Billions
Pool Type DY* 1
(2011-2012) DY 2
(2012- 2013) DY 3
(2013- 2014) DY 4
(2014-2015) DY 5
(2015-2016) Totals
UC $3.7 $3.9 $3.534 $3.348 $3.1 $17.582
DSRIP $0.5 $2.3 $2.666 $2.852 $3.1 $11.418
Total/DY $4.2 $6.2 $6.2 $6.2 $6.2 $29
% UC 88% 63% 57% 54% 50% 60%
% DSRIP 12% 37% 43% 46% 50% 40%

RHP Category 1 and 2 Minimum Number of
Projects
Share of population under 200% FPL
Min number of Cat 1 and 2
projects
Min number of Cat. 2 projects
Tier 1 >15% 20 10
Tier 2 (Regions 9 and 10)
7-15% 12 6
Tier 3 3-7% 8 4
Tier 4 (Region 18) <3%, no public hospital, or public hospitals serve
<15% UC
4 1
12
• Four Tiers based on share of the statewide population under 200 percent of the federal poverty level (FPL)

RHPs and DSRIP
• RHP Plans include: • Regional health assessments
• Participating local public entities
• Public engagement
• Identification of hospitals receiving incentives and of yearly performance measures
• Incentive projects by DSRIP categories
• RHPs and RHP plans do not: • Require four-year local funding commitments
• Determine health policy, Medicaid program policy, regional reimbursement, or managed care requirements

Dallas Fort Worth Hospital Council Community Needs
Assessment Report.: RHP 9 – Findings (DRAFT)
The following regional priorities were identified as primary community health needs and are recommended for consideration as context for identification of strategies and recommended actions of the regional plan:
Capacity - Primary and Specialty Care•The demand for primary and specialty care services exceeds that of available medical physicians in these areas, thus limiting healthcare access for many low level management or specialized treatment for prevalent health conditions.
Behavioral Health - Adult, Pediatric and Jail Populations•Behavioral health, either as a primary or secondary condition, accounts for substantial volume and costs for existing healthcare providers, and is often utilized at capacity, despite a substantial unmet need in the population.
Chronic Disease - Adult and Pediatric•Many individuals in North Texas suffer from chronic diseases that present earlier in life, are becoming more prevalent, and exhibit more severe complications.
Patient Safety and Hospital Acquired Conditions•Continued coordinated effort is needed to improve regional patient safety and quality.
Emergency Department Usage and Readmissions•Emergency departments are treating high volumes of patients with preventable conditions, or conditions that are suitable to be addressed in a primary care setting. Additionally, readmissions are higher than desired, particularly for those with severe chronic disease or behavioral health.
14

Stakeholder Engagement
Stakeholder Engagement• RHP Participant Engagement
• Information for Performing Providers including hospitals, Community Mental Health Centers, Academic Health Science Centers and Local Health Departments.
• Public Engagement• Processes used to solicit public input into RHP Plan and public review prior
to plan submission, including county medical societies.• Must include a description of public meetings and posting of RHP Plans for
input.• Plan for ongoing engagement with public stakeholders.
15

RHP Plans and CMS Expectations – Regional
Transformation
• Transparent planning process that demonstrates regional collaboration and public input.
• Projects selected address community needs and regional goals.
• Projects selected are the most transformative for the region• RHP Plan includes projects that tie to the four DSRIP
categories together to demonstrate outcomes• RHP Plan includes broad UC and DSRIP participation.
16

Funds Flow Mechanics DSRIP Pool
17
The allocation of the DSRIP Pool is quite complex with respect to both the allocation to regions and the allocations within each region
Percent of population < 200% FPL
Percent of Medicaid acute care payments
Percent of UPL program payments
HospitalsTargeted to receive 75% of fundsMust have participated in DSH or UPL programsAllocated on basis of: Percent of Medicaid payments, Percent of UPL, Percent of UCNon HospitalsCommunity mental Health Centers – 10%Academic Physicians Practices - 10%Local Health Departments- 5%
ConditionsMeet minimum number of projects; each project capped generally at $20m for 4 yearsRequire participation for major safety net hospitals (at least 4) Broad hospital participation – at least 30% of the pool allocated to private hospitals
ConditionsTo be eligible to have a Pass 2, the conditions of Pass 1 must be metHospitals Non DSH/UPL providers – 15%Additional projects for pass 1 participantsNon HospitalsNon academic physician practices – 10%Additional projects of Pass 1 participants

Eligibility for “Pass 2” Major Safety Net Hospital
Participation
• A minimum number of major safety net hospitals must participate in DSRIP as Performing Providers based on Tier level.
Tier 1 At least 5
Tier 2 At least 4
Teir 3 At least 2
Tier 4 At least 1
TotalAt least 38 Major Safety Net Hospitals In Texas
18
For RHP 9, Major Safety Net hospitals include: Parkland, Baylor University Medical Center, Methodist Medical Center, Medical City and Children’s Medical Center

Page 19
DSRIP Category 1:Infrastructure Development

DSRIP Category 2:Program Innovation and
Redesign
Page 20

Page 21
DSRIP Category 3:Quality Improvements
CMS Outcomes Definition:“…..Measures that assess the results of care experienced by patients,
including patients’ clinic events, patient’s recovery and heath status, patient’ experiences in the health system, and efficiency/cost.”
• All Category 1 & 2 projects must have one or more associated Category 3 outcomes.
• Outcomes measured are based on specific patient population served by the project.
• Encouraged by CMS to pursue a common, regionally-based Category 3 outcome
• A list of Category 3 outcomes is still under development

Page 22
DSRIP Category 4:Population-focused
Improvement
• Potentially preventable admissions
• 30-day readmissions
• Potentially preventable complications
• Patient-centered healthcare, including patient satisfaction and medication management
• ED admissions time

UC an DSRIP Participation
• Hospitals receiving uncompensated care (UC) payments must report on a subset of Delivery System Reform Incentive Payment (DSRIP) Category 4 measures.
• Potentially Preventable Admissions (PPAs)• Potentially Preventable Readmissions (PPRs)• Potentially Preventable Complications (PPCs)
• Failure to report on the requirement measures by the last quarter of the year (with a six-month extension) will result in forfeiture of UC payments in that quarter.
23

Category Allocations
DY 2 DY 3 DY 4 DY 5
Category 1 & 2 No more than 85%
No more than 80%
No more than 75%
No more than 57%
Category3 At least 10% At least 10% At least 15% At least 33%
Category 4 5% 10-15% 10-15% 10-15%
24
Hospital Performing Providers
DY 2 DY 3 DY 4 DY 5
Category 1 & 295-100%
No more than 90%
No more than 90%
No more than 80%
Category3 0-5% At least 10% At least 10% At least 20%
Non- Hospital Performing Providers

1115 Waiver as a Foundation for Reform
25
• Supreme Court decision allowing states to opt out of Medicaid Expansion
• $155 Billion being eliminated from Hospitals as Health Care Reform is Implemented
• Lessons learned from Massachusetts Newly covered individuals not able to find care (infrastructure not
developed to handle increase in covered individuals)
• Without expansion of Medicaid, many Texas Hospitals will have a difficult challenge ahead
1115 Waiver offers the opportunity to transform the delivery system to provide more than cover – the opportunity to reach the Triple Aim Goals

Triple Aim
Institute for Healthcare Improvement, 2007• 3 critical objectives:
• Improve the health of the population
• Enhance the patient experience of care (including quality, access, and reliability)
• Reduce, or at least control, the per capita cost of care
Ultimately we must move beyond Coverage and Care to the Prevention and the Social Determinants of Health
26

Fence or Ambulance?
Malins J. Fence or ambulance? Bulletin of the North Carolina State Board of Health 1913;27(10):16Available at: http://www.archive.org/stream/bulletinofnorthc27nort#page/16/mode/1up.
“Twas a dangerous cliff, as they freely confessed,
Though to walk near its crest was so pleasant;
But over its terrible edge there had slipped
A duke, and full many a peasant;
So the people said something would have to be done,
But their projects did not at all tally.
Some said, “Put a fence around the edge of the cliff”;
Some, “An ambulance down in the valley.”
“Better guide well the young than reclaim them when old,
For the voice of true wisdom is calling;
To rescue the fallen is good, but ‘tis best
To prevent other people from falling;
Better close up the source of temptation and crime
Than deliver from dungeon or galley;
Better put a strong fence ‘round the top of the cliff,
Than an ambulance down in the valley”.
The poem “Fence or Ambulance?” by Joseph Malins that was published in the 1913 Bulletin of the North Carolina State Board of Health opens this way:
Prevention is better than cure. Desiderius Erasmus1466-1536

Elements Needed in the
Changing Environment
• New delivery models are as important as insurance reform• Rationalizing delivery models
- Primary medical care homes
- Care management
- Addressing socioeconomic determinants of health
- Addressing disparities adequately
• Shift from volume-driven to value-driven (outcomes vs. thru-put)
• Access is as fundamentally important as coverage
• Evidence-based practice and policy are critical• Must deal with variations in practice that are not bringing value• Must promote comparative effectiveness research and its applications• Must balance “sticks and carrots”
28

Safety Net in the Changing
Environment
• Needs to expand upstream and deal with the determinants of health at the community level: • Prevention• Health promotion• Care management• Population-driven medicine
• The Safety Net may need to be redefined:• More adaptable and flexible• More accountable• More upstream interventions
29

Safety Net in a Changing
Environment• Investment in public infrastructure may be the best way for many
urban areas to provide the elements necessary for reform to succeed, especially in these areas:
• Physician, nurse and other provider training
• Outcomes studies for comparative effectiveness and disparities
• Population medicine
• Provision of regional tertiary/quaternary services
• Rethinking the health delivery model, moving from individual medicine to population health
• Need incentives to improve collaboration among hospitals, public health and community-based services
• Meet as a community to determine how to harvest the synergy of education, housing, police, fire, etc.

Recreate “the Commons”
• Restore our sense of community
• Re-tap our energy to solve our own problems
• Rediscover the strengths of ad hocracies
• De Tocqueville — early 1800s
• Effects will be seen in areas other than health care

• We must manage the In-Between, or the Common Ground that benefits the whole infra-structure but is not managed by any one part
• Important for accountability, stewardship and outcomes
• Promotes synergism with one success building upon another
Managing the In-Betweens
Health in All
Policies

Call to Action
To improve quality, safety & access:
• Goals for Dallas to bring us together – Healthy Dallas Goals for United Way Strategic Plan
• Collaborative Dialogue
• Community Driven Process • (Managing the In-Betweens)
• Regional Health Partnerships – • Planning for Health Among Competitors • (1115 Medicaid Waiver)