Embed Size (px)
Citation preview
283
THE CLINICAL APPLICATION OF THEELECTROENCEPHALOGRAM IN
CEREBRAL TUMOURBy GERALD PARSONS-SMITH, M.D., M.R.C.P.
Physician, West End Hospital for Nervous Disease; Neurologist, Graylingwell Hospital;'Consultant in Electroencephalography, West London Hospital
The introduction of electroencephalographicstudy to cases of cerebral tumour has provided theneurologist, during the past I 5 years, with a newdimension in diagnostic approach which he caninter-relate with the other methods of investigationat his disposal. In I93i Berger showed that im-pairment of cortical function resulting from highintracranial pressure was associated with slowfrequency potentials. Two years later he foundsimilar waves confined to the affected hemispheresin two cases of cerebral tumour (Berger, 1933).No particular importance was attached to theseslow waves until Walter (I936) found a definitefocus of origin of these abnormal frequencies at apoint on the skull under which, at autopsy at alater date, a tumour was discovered to be involvingthe cerebral cortex. Adrian (I935) had alreadyforecast that the study of the electroencephalo-gram might be of use to the clinician, and it wasas a result of this discovery by Walter that interestin the clinical uses of the electroencephalogram(E.E.G.) was aroused.The clinician can now obtain in the E.E.G. a
permanent visual record of the distribution of theabnormal cortical waves, together with thosenormal ones which may persist, and he can use itto provide an objective physiological backgroundto the complex clinical picture which may becaused by a cerebral tumour. The usual tech-nique, which causes no discomfort to the patient,consists in placing I2 electrodes over the patient'sscalp in a standard arrangement such as is des-cribed by Cobb (1950). The recording sessiongenerally lasts for one hour, during which time thepatient lies quietly on a couch with the eyes shut.
It did, at first, seem probable that the E.E.G.would prove an exceedingly accurate diagnostic
technique, as the earlier published results onselected cases were impressive, so that it was con-sidered that if such exact localization of a tumourcould be obtained consistently by this relativelysimple and safe method, then clearly it must be themethod of choice. But in spite of great improve-ments in equipment, technique and skill in inter-pretation which have taken place during the pastdecade, the results in many large series of un-selected cases have shown that precise localizationcannot be guaranteed. The fundamental sourceof the difficulty in localization is that the abnormalbrain waves which are seen in cases of cerebraltumour arise from the altered brain tissue which isadjacent to the tumour, and that the actual sub-stance of most cerebral tumours is electricallysilent. Because of this the position of the electro-graphic abnormality may not always coincide withthe site of the tumour as exposed by the neuro-surgeon, with the result that the method may beconsidered inaccurate by the inexperienced.The claims for exact localization of accessible
cerebral tumours are varied, figures from 47.8 to88.3 per cent. being reported. Examination ofi,242 published cases of accessible cerebraltumours collected from I2 sources shows thataccurate localization was achieved in 73 per cent.af the patients (Yeager et al., 1940; Gibbs et al.,194I; Cobb, I944; Hines et al., I944; Yeagerand Luse, I945; Baudouin et al., I946; Hoeferet al., I946; Bassett and Bagchi, I947; Buchthaland Busch, 1947; Schlesinger and Strauss, I947;Parsons-Smith, I949; Kershman et al., I949).The largest number of cases in any one series wasthat published by Hoefer, Schlesinger and PennesVI946), who analyzed the results from the study of543 cases of verified brain tumours at the Neuro-
copyright. on June 1, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.28.319.283 on 1 May 1952. D
ownloaded from
POSTGRADUATE MEDICAL JOURNAL
logical Institute in New York. In 416 hemispherelesions, localization was obtained in 64 per cent.and lateralization in a further 9.6 per cent. In247 gliomata the figures were 72 per cent. and 8.Iper cent., and in 77 meningiomata 47 per cent. and17 per cent. respectively. These figures com-pare closely with the author's in a study of I50verified cases (Parsons-Smith, 1949). In thisseries ioo hemisphere tumours were localized in66 per cent. and lateralized in a further 2I percent., whilst the figures for 40 astrocytomata,grades i and 2, were 74 per cent. and 14.5 percent., for 40 astrocytomata, grades 3 and 4 (glio-bastoma multiforme), 74 per cent. and 13 per cent.,and for 20 meningomata 33 per cent. and 33 percent. Examination of the figures in the two seriesquoted above show that an abnormality will beseen in the correct hemisphere in 8o to 88 percent. of the accessible gliomata, but even so thevalue of E.E.G. study will be more apparent if itis ubed to throw light on the behaviour of thecerebral tumour rather than to place its positionanatomically.The optimum method of investigation of a
patient suspected of having a cerebral tumour is bya combination of clinical, electroencephalographicand radiological techniques, and in this way preciselocalization can be expected. Although great im-provements in the radiological localization figureshave taken place recently, the method is notsuccessful in every case. The commoner sourcesof failure are insufficient amount of air in theventricles and in not being able to determine theextent of the lesion or whether it is extra- or intra-cerebral.
Nevertheless, anatomical localization can be ex-pected by X-ray in 85 to go per cent. of all cases."The E.E.G. has proved just as accurate an indicatoras radiology in the accessible tumours, but thelocalization which it gives may not always coincidewith the site convenient for surgical approach andit should not, therefore, be used for this purpose.It is more profitable to blend-the E.E.G. data withthe anatomical evidence derived by X-ray so as tothrow light on the nature of the tumour, thedirection of its spread, and its effect on thesurrounding brain tissue.
Limitations and DiscrepanciesThe E.E.G. is a valuable diagnostic method in
cases of cerebral tumour provided that the physicianand the surgeon both appreciate that apparentfallacies may occur, though it is stressed that anaccurate physiological explanation can usually be'elicited to explain those so-called -fallacies. Thereare limitations to the E.E.G. method and the mostserious are as follows:
i. Only lesions above the tentorium directlyaffect the normal brain waves.
2. The actual substance of a cerebral tumourhas been shown to be electrically inactive, and itis now known that the electrical abnormalitiesarise in the abnormal cerebral tissues around thetumours.
3. The diagnosis of cerebral tumour cannot bemade from the E.E.G. alone, as no one E.E.G.appearance is per se specific for a neoplasm.
4. It is not possible to differentiate the varioustumour types on E.E.G. appearances. This is notunexpected. Scherer (1938) showed that when allareas of any one glioma are sectioned it is oftenimpossible to classify it, as one point may showrelatively benign features whilst another may behighly malignant. Even so, diagnostic E.E.G.dlaims of this sort continue to appear in theliterature.
5. Parasagittal frontal lesions, even when verymalignant, may not necessarily disturb the normalcortical rhythms.
6. Mirror foci, and so-called false localizingsigns, are potential sources of the quite gross dis-crepancies which occur with greater frequencythan many observers admit. Thus in about 20per cent. of tumours involving the cerebello-pontine angle a severe focal abnormality may beseen in the contralateral temporal lobe. The falselocalizing signs and mirror foci seen with posteriorfossa lesions present an interesting physiologicalproblem which is not fully understood. It ispossible that the action potentials of brain cellsand axons are conducted along such connectionsas the corpus callosum and fronto-pontine tracts.In other cases the false foci may be caused byoedema resulting upon brain shift or interferencewith the blood supply. In the following case thefocus must have been significant from the first butwas ignored:A boy of nine developed a staggering gait and
signs of raised intracranial pressure. An E.E.G.showed a one- to two-a-second focus in the leftparietal area. Moderate hydrocephalus was seenin the ventriculogram with signs of a left cere-bellar tumour. This was confirmed at operationwhen a malignant medulloblastoma was exposed.The child was treated with radiotherapy. Tenmonths later the child developed epilepsy involv-ing the right arm and leg, the fits clearly arising inthat area of the cortex which had earlier beeninvolved in the E.E.G. abnormality.
7. It is not possible to localize, or even tolateralize, by electroencephalography, tumours ofthe posterior fossa (see Fig. i).'
8. Either very high intracranial pressure, orsevere changes in consciousness, or both, will pro-
284 MOY 1 952
copyright. on June 1, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.28.319.283 on 1 May 1952. D
ownloaded from
PARSONS-SMITH: Electroencephalogram in Cerebral Tumour
\ 'v,
.r'W
X,,kI
AI\r\
./..Av4f.)
^yrv~-
..YAAf<\J\A
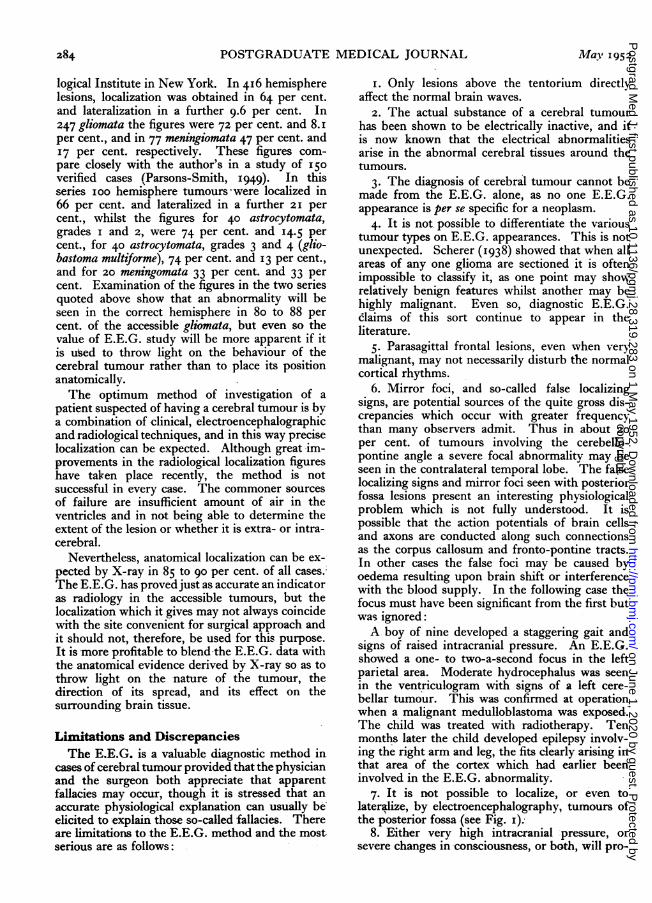
A-FIG. T.-Right cerebellar cystic astrocytoma. High voltage three-a-second pressure waves arising
from both cerebral hemispheres. First a phase reversal is seen from the left frontal lobe, andlater in the record from the right.
FIG. Z.-Rght anterior temporal fibrillary astrocytoma. High 'voltage one- to two-a-second wavesappear in. the right anterior temporal lead, with a phase reversal. The posterior temporal leadon the right side contains two- to five-a-second activity. In all the figures the horizontal linerepresents I second and the vertical signal 50 microvolts.
I
I
M-aY 1952 285
I
I,,\
.1
copyright. on June 1, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.28.319.283 on 1 May 1952. D
ownloaded from
286 POSTGRADUATE MEDICAL JOURNAL May 1952
duce abnormal waves which may completely maska severe focal abnormality.
E.E.G. Appearances Produced by CerebralTumours
Various degrees of severitv of the E.F.G.abnormality are met with in most cases of cerebraltumour, but in some patients the record may bequite normal. The abnormality is usually a slowwave focus, a delta focus, and its rate may varyfrom one to seven cycles a second. There is noconstant relationship between the rate of the deltafocus and the underlying cerebral pathology,though the slower frequencies are more frequentlyassociated with a raised intracranial pressure.Although a half- or one-a-second focus is generallythought to be associated with a severe infiltratingtumour, it can just as readily be produced by abenign tumour, or even with localized lesions dueto active cortical atrophy, encephalitis or cerebralthrombosis, whereas conversely a three- to four-a-second focal abnormality may be associated with avery malignant tumour. Very frequently five- toseven-a-second waves appear, so-called thetawaves, and these generally indicate the edge of adeeply placed tumour. They have no furtherreliable significance.
If in the more difficult cases serial E.E.G.s areperformed, light will be thrown on the nature ofthe tumour. Thus a mild abnormality, rapidly
worsening, would suggest a malignant tumour,whereas a mild abnormality which did not alterappreciably over months of observation wouldpoint to the lesion being relatively benign. lt isfound that different types of cortical tumour aremore likely to produce a slow wave focus thanothers, so that different results in E.E.G. diagnosismay be expected. The commoner groups withany features which may be expected are as follow:
i. Astrocytoma, types i and 2By exhibiting a slow wave focus in the E.E.G.,
this type of tumour should be localized or lateral-ized to the correct hemisphere in 88 per cent. ofcases (Figs. 2 and 3). The slow wave abnormalityis usually seen constantly, but in about 20 percent. of the cases it may only be seen occasionally.If an history of epilepsy is combined with radio-logical evidence of brain displacement, as seen by alateral shift of the septum pellucidum, then afocal E.E.G. abnormality will invariably occur.This may be of value in differential diagnosis. Insome cases there may be no slow waves indicativeof brain damage over the area involved by thetumour, but epileptic outbursts may be recordedon the affected hemisphere'and arise from that partof the cortex directly overlying the astrocytoma.A man of 37 gave an eight-month history of
epileptic fits. Except that his memory had beenpoor for three months there were, otherwise, no
2 Q
46CJ3
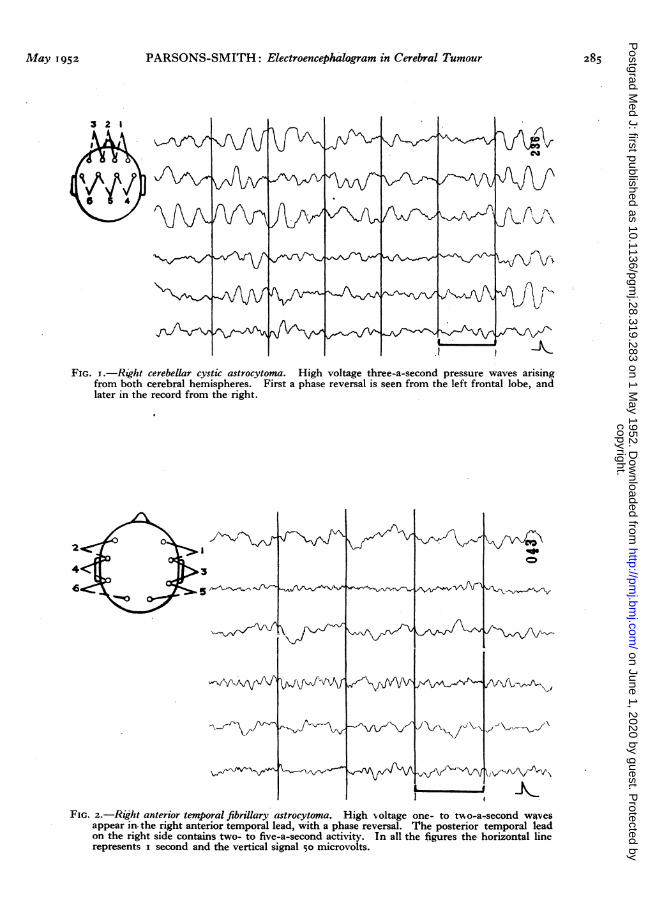
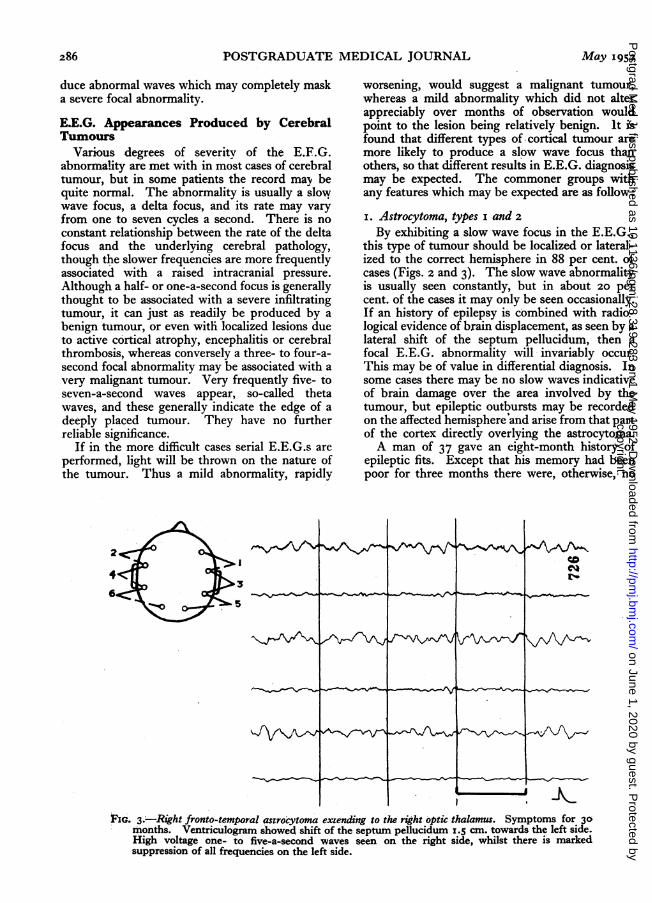
FIG. 3.-Right fronto-temporal asrrocytoma extending to the right optic thalamus. Symptoms for 30months. Ventriculogram showed shift of the septum pellucidum I.5 cm. towards the left side.High voltage one- to five-a-second waves seen on the right side, whilst there is markedsuppression of all frequencies on the left side.
copyright. on June 1, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.28.319.283 on 1 May 1952. D
ownloaded from
PARSONS-SMITH: Electroencephalogram in Cerebral Tumour
abnormal signs or symptoms. An E.E.G. showedno slow wave focal abnormality but outbursts ofthree- to four-a-second waves arose in the rightfrontal region and spread over* the right hemi-sphere. A ventriculog'ram showed a right anteriorfrontal expanding process, and at operation a verycellular astrocytoma measuring 6 by 5 cm. wasremoved from the right frontal lobe. Two monthslater the E.E.G. was quite normal and the patientfree from symptoms.
2. Astrocytoma, types 3 and 4 (malignant glioma)A similar E.E.G. diagnosis rate is expected with
the malignant gliomata as with the benign astro-cytomata, but the radiological diagnosis may notso readily be achieved because in manv of thecases the tumour is infiltrating rather than dis-placing the substance of the brain. In about one-fifth of the cases X-ray findings may not becontributory in diagnosis, but in these very casesa severe E.E.G. focus will be seen as in the follow-ing case, where ventriculography, arteriographyand 'even direct inspection refuted the correctdiagnosis:
This was a woman of 67 who had been in goodhealth until four months previously, when shehad noted a sensation of numbness in her lefthand. Two months later she had a focal fit in-volving the left hand and the left side of her face.On examination she had a left facial weakness anda left hemiplegia, involving both motor andsensory modalities, which affected the arm morethan the leg and was mainly sensory. A per-sistent right parietal E.E.G. focal abnormality wasrecorded and because of it, and in spite of both anegative ventriculogram and arteriogram, a crani--otomy was performed. No tumour was found.During the next few weeks her clinical conditionworsened and the E.E.G. appearances were seento deteriorate. When she died, six months afterher first symptom, a large infiltrating malignantglioma was exposed at the site where the originalE.E.G. record had placed it.
It happens, not infrequently, that a severe focalabnormality is exposed in the routine E.E.G. ofthe out-patient who presents with symptoms ofepilepsy of late onset. The electroencephalogramshould not be used as an out-patient filter in theway that mass radiography is used in the controlof pulmonary tuberculosis, but when, as the re-sult of study of the record, severe focal braindamage is reported in an out-patient, the caseshould be admitted to a neurological departmentfor further investigation.A man of 52 was referred as an out-patient for
an E.E.G. He had had an epileptic fit two monthspreviously after which mild right hemiplegic signswere noted but which later improved. An E.E.G.
showed a severe clear-cut left temporal lobeabnormality where high voltage two-a-secondwaves arose. As a result of the E.'E.G. report aventriculogram and exploratory operation 'wereperformed to disclose an inoperable malignantglioma. This had arisen from the left caudatenucleus.
3. OligodendrogliomaThis type of slow growing neoplasm'gives rise
to focal slow wave abnormalities-, and- accurateE.E.G. localization can usually be expected.
4. MedulloblastomaNo direct diagnostic help can be expected'from
E.E.G. stu'dy in cases of cerebelIar medullo-blastoma. Following successful surgical and deepX-ray treatment the generalized high pressurewaves are seen to make way for the more normalfrequencies. When the inevitable and terminalwvorsening of the condition sets in the deteriorationin the E.E.G. records will be apparent at a veryearly stage. Deep X-ray therapy to the tumour'inthe posterior fossa may later cause suppression" ofthe alpha rhythm on the side which has beenirradiated.
5. Pituary AdenomaThe extrasellar extensions may rise as much as
2 or 3 cm. above the diaphragm and even, insevere cases, obliterate the foramina of Munro,when symptoms due to raised intraventricularpressure will ensue. If, however, there is nochange in pressure the largest tumours will butrarely cause alterations in the E.E.G. Five- toseven-a-second waves, occurring in runs, weredescribed in the literature with these tumours, butthey seem now to occur in less than 2o per cent.of the cases and they are certainly not diagnostic.Bilateral synchrony of five- to six-a-second wavesis more suggestive of a deep mid-line lesion thanwhen runs are recorded, but even so a large pro-portion of the very gross adenomata may havenormal E.E.G. records.
6. MeningiomaAs a result of clinical, electroencephalographic
and pathological findings, it is possible to sub-divide the meningiomata into three groups. Inthe first group, which is associated with a normalE.E.G., the tumour is slow growing, hard, rela-tively easy to remove and derives its main bloodsupply from the dura mater. There may be somesuppression of the cortical potentials if the tumouris superficial.A man of 4I was admitted for investigation with
and eight-month history of epilepsy. The initialsymptom had been a focal fit commencing in the
May I952 287copyright.
on June 1, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.28.319.283 on 1 M
ay 1952. Dow
nloaded from
288 POSTGRADUATE MEDICAL JOURNAL May 1952
right arm. There were no abnormal physicalsigns. An E.E.G. showed a dominant frequencyat nine-a-second, with generalized underlying fastactivity at 22-a-second. There was no evidenceof any focal abnormality. A ventriculogram thefollowing day showed poor filling of the ventricularsystem and a shift of the septum pellucidum ofo.s cm. to the right of the mid-line. The leftforamen spinosum was enlarged. An arteriogramshowed displacement of the left anterior cerebralartery o.s cm. to the right of the mid-line, and aphlebogram showed evidence of abnormal veins inthe left frontal region. At operation a typicalmeningioma, 7 by 6 cm., was removed from theleft fronto-paretal region. It was not undulyvascular and very little trauma was caused atoperation to the surrounding tissues. Microscopyshowed it to be a rather cellular meningioma. Thiswas a very slow growing parietal meningiomawhich had not involved the surrounding brainsubstance and which was associated with analmost normal E.E.G.The second group in which there is a focal
E.E.G. abnormality consist of tumours which maybe of the same size as those seen in the first groupand have a similar microscopic appearance, butwhich at operation are found to be extremelyvascular and to derive their blood supply fromboth the meningeal and cerebral vessels. The site
of the tumour does not necessarily coincide withthe E.E.G. focus.A woman of 50 had a focal epileptic attack in
her left hand seven years previously, following amild head injury. For the next three years s'hewas treated for a menopausal ' nervous break-down,' even though she was suffering from re-current fits in her left hand. During the yearbefore admission she had developed recurrentheadaches, deterioration of her eyesight andalteration of personality. On examination she wasmildly demented, had a left facial weakness, andthe tendon jerks were increased in the left arm.An E.E.G. showed a diffuse abnormality in theright temporal region where medium voltagetwo-a-second waves occurred in short runs. Aventriculogram showed a shift of the septumpe1lucidum of 2 cm. due to an anterior parietallesion. At operation an extremely vascular super-ficial meningioma, 5 by 5 cm., lying just above andbehind the Sylvian point was removed. It was icm. thick. Microscopically it was a meningiomawith widely dilated lymph and blood spaces. Thiswas a very vascular parietal meningioma withi aslow wave focus adjacent to the superficial site ofthe tumour.The meningiomata-en-plaque make up the
third group, in which a slow wave focus is foundinstead of the general suppression which at first
2 B
43
0-' 9>rMiv~WIAfrV
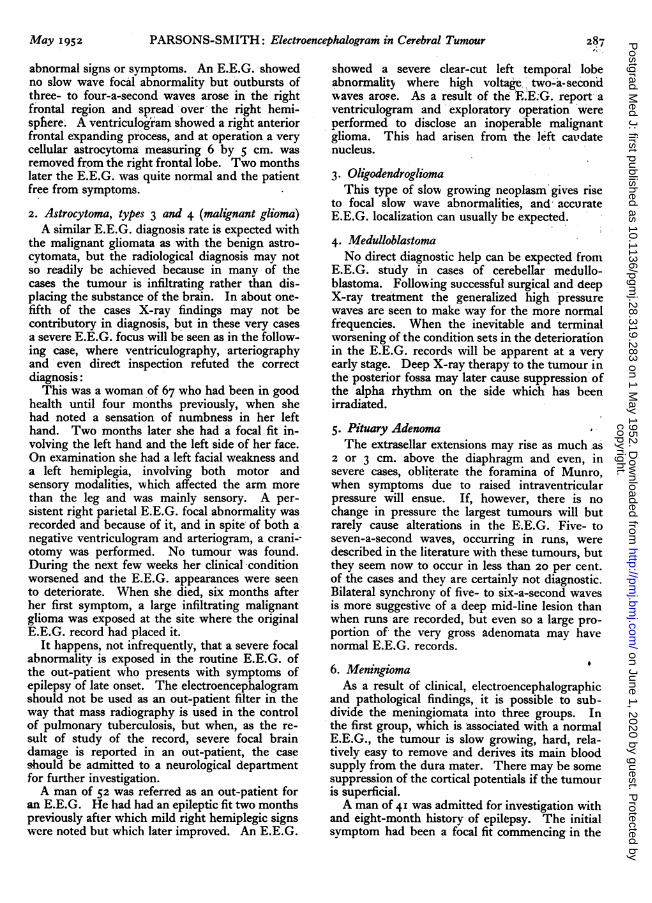
FIG. 5.-Recurrent haemangioblastoma. Symptoms of postural headache and unsteadiness whenwalking. A ventriculogram was ,considered to rule out a recurrence of a cerebellarhaemangioblastoma, and the ventricular pressure was normal. The E.E.G., however, showed ageneral abnormality; the alpharhythm of io-a-second is disturbed in all leads by runs of 5-a-second waves.
copyright. on June 1, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.28.319.283 on 1 May 1952. D
ownloaded from
M11ay 1952 PARSONS-SMITH: Electroencephalogram in Cerebral Tumour 289
2 o
4<>
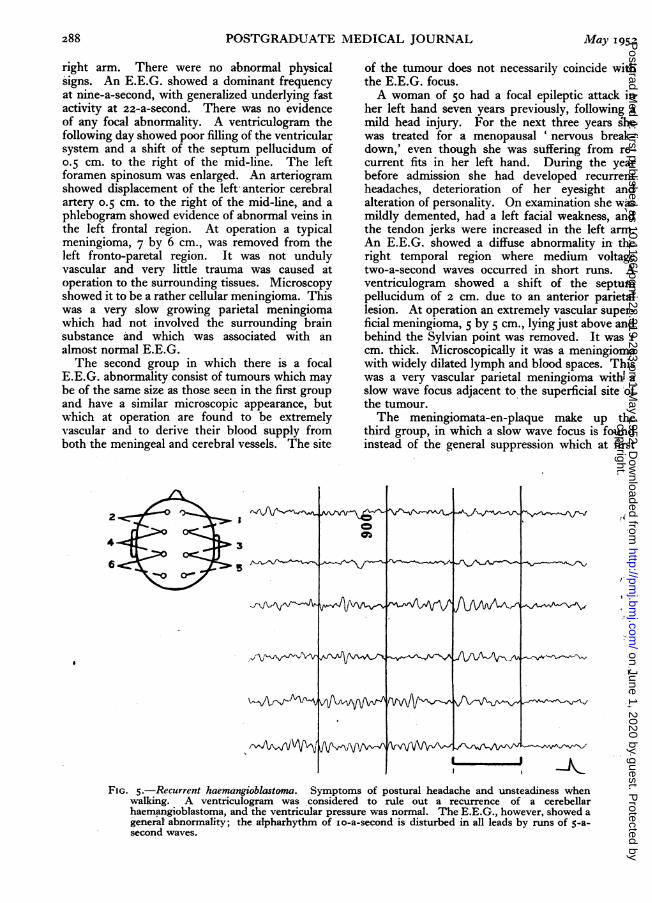
FIG. 6.-Five weeks later he had developed symptoms of raised. intracranial pressure withpapilloedema. Note the change in the character of the records, high voltage 5-a-second wavesnow occurring in all leads. A week later an haemangioblastoma 3 cm in diameter was removed.Ten days later the E.E.G. was quite normal.
sight would have appeared probable. The reasonfor this unexpected finding is that this type ofmeningioma is not, in fact, a flat innocent plaquebut is a vascular and infiltrating mass firmlyjoined with the brain substance.The slow distortion of the brain by a meningioma
frequently results in the appearance of pathologicalfast activity over both hemispheres. These fast,beta waves, are generally at 22-a-second and areseen more commonly with the meningiomata thanwith any other type of cerebral tumour. Incommon with the other cerebral tumours theparasaggital lesions are exceedingly difficult tolocalize, and indeed a normal record may beobtained with veryr vascular meningiomata occurr-ing at this site.
7. HaemangioblastomaThese tumours cannot be localized, nor even
lateralized, by E.E.G. methods owing to theirsituation in the posterior fossa. Slowing of thealpha rhythm may occur as the earliest physicalsign of altered cortical metabolism in the earlieststages of the development of raised intracranialpressure and may be present at a time when theintraventricular pressure, as measured at ven-triculography, may be considered normal (Figs.5 and 6). After successful removal of anhaemangioblastoma the alpha rhythm should re-turn to its normal frequency and become stable.
8. CholesteatomaAlthough these large avascular mid-line frontal
tumours are usually associated with symptoms ofepilepsy and may slowly displace the frontal lobes,the electroencephalogram is generally found to bequite normal.
9. CraniopzharyngiomaUnlike the chromophobe adenomata these mid-
line suprasellar tumours give rise to well-markedslow wave abnormalities, probably because oflateral extensions of the cyst. The E.E.G. willshow which frontal lobe is the more affected andwill assist the surgeon to determine through whichside he should approach the tumour at operation.
IO. Metastatic TumoursGenerally the appearances are similar to those
encountered with the gliomata, but the recordsmay contain more than one focal abnormality,these indicating the presence of multiple lesions.
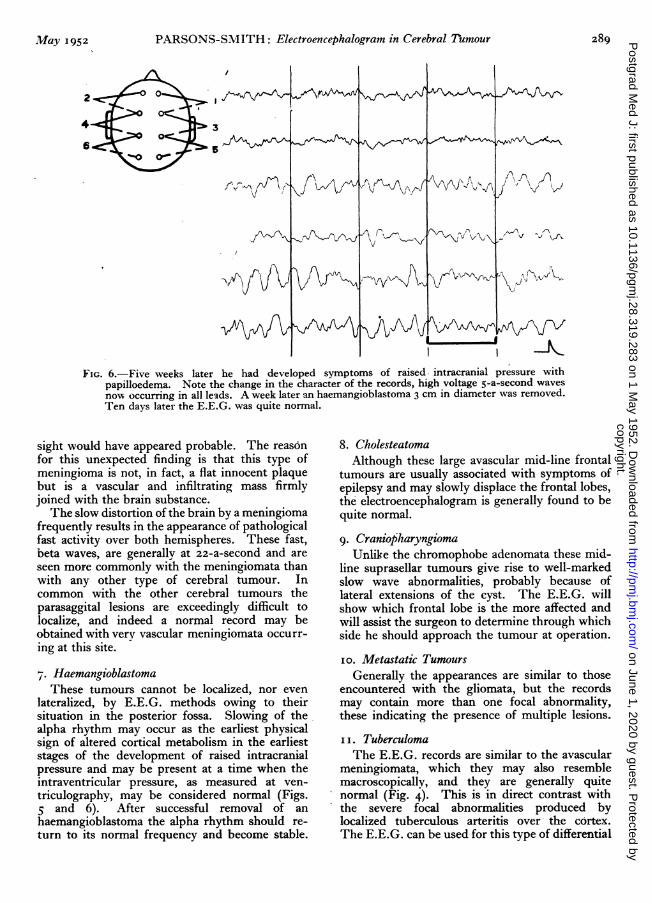
i i. TuberculomaThe E.E.G. records are similar to the avascular
meningiomata, which they may also resemblemacroscopically, and they are generally quitenormal (Fig. 4). This is in direct contrast withthe severe focal abnormalities produced bylocalized tuberculous arteritis over the cortex.The E.E.G. can be used for this type of differential
copyright. on June 1, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.28.319.283 on 1 May 1952. D
ownloaded from
290 POSTGRADUATE MEDICAL JOURNAL May 1952
J
4
FIG 4.-Right parietal parasaggital tuberculoma. A fairly stable alpha rhythm of io-a-second is seenover both hemispheres. The increase of the voltage on the right side is due to the presenceof a burr-hole in the right parietal area.
diagnosis in those tuberculous patients who de-velop signs of cerebral disease.
I2. Subdural HaematomaAlthough close clinical resemblance exists be-
tween an intracerebral tumour and a chronicsubdural haematoma, the E.E.G. is a guide indifferentiating between the two conditions. Evenwith distortion of the brain, as seen by grossdisplacement of-the septum pellucidum, recordsfrom an anterior subdural haematoma will bequite normal, w4hereas in' the posteriorly placedlesion there will be suppression of the dominantfrequency on the affected side.A woman of 58 had an i8-months' history of
mental changes. For a year she had been in-creasingly irritable, and for six months had haddifficulty with her speech. There was no historyof head injury. On examination she was retardedbut there was no evidence of abnormality in hernervous system. An E.E.G. was quite normal.A ventriculogram showed a large left posteriorfrontal expanding lesion with a shift of the septumpellucidum of I.5 cm. to the right. At operationa tense bluish dura was incised to reveal a long-standing subdural haematoma containing thick,bright yellow fluid. The membranes were re-moved 'to reveal convolutions which thoughflattened were otherwise normal. She made arapid and complete recovery followingoperation.
The presence of a slow wave focus in a provencase indicates that there has been recent damageto the underlying cerebral cortex which has not,as yet, resolved.A district nurse of 5I had a short history of
mental deterioration and a right hemiparesis. AnE.E.G. showed suppression of the alpha rhythmin the left occipital region but there was also amild diffuse abnormality in the left temporal lobeconsisting of low voltage one- to three-a-secondwaves. At operation 0OO cc. of dirty brown fluidescaped from a left posterior parietal burrhole.It was considered that the haematoma was aboutfour weeks old. She made a rapid recovery andtwo weeks later the E.E.G. was quite normal,showing that resolution of the damaged brain wascomplete.
13. Cerebral AbscessAn acute untreated cerebral abscess gives rise
to an unusually severe and very localized slowwave focus consisting of high voltage half- to one-a-second waves which completely exclude allother activity. Recordings from other parts ofthe hemispheres may be only slightly abnormal.If treatment has been commenced with antibioticsthe changes are less specific.
Clinical ApplicationElectroencephalography can be used in several
ways in cases suffering from cerebral tumour and,
copyright. on June 1, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.28.319.283 on 1 May 1952. D
ownloaded from
PARSONS-SMITH: Electroencephalogram in Cerebral Tumour
broadly, these can be divided into three groups.First in the selection of cerebral tumours; thisparticularly applies to out-patient cases in whomdiagnosis of cerebral tumour is suspected;secondly in the differentiation of the cases whoseinvestigation for cerebral tumour have alreadycommenced; and thirdly in the control of theproven cases of cerebral tumour.SelectionThe occurrence of epileptic fits in an out-patient
is the most frequent cause for reference for electro-encephalographic examination. If the E.E.G.shows a very severe slow wave focus with super-added paroxysms of epileptic activity, then thatpatient must be suffering from symptomaticepilepsy. Conversely, if short paroxysms of truespike and wave activity, or bursts of generalizedfast activity, disturb and otherwise normal recordit is more probable that the patient is sufferingfrom idiopathic epilepsy. There will, of course,be many intermediate types in which the E.E.G.appearances are not specific and on which nofirm differential diagnosis can be made. Theidiopathic epileptic patient will be treatedmedically, but the patient suffering from sympto-matic epilepsy will require further study and in-vestigation. In many cases the optimum time forcommencing these further investigations can befound from a study of the E.E.G. records. Theappearance of a severe focal abnormality in theE.E.G. of a patient with symptomatic epilepsymay precede by months, or even years, the onset-of physical signs, or localizing symptoms, andduring this time, if the clinical picture permits, itwill be safe to keep the patient under carefulmedical observation, at first repeating the recordsevery two weeks and later, if there has been noclinical deterioration, every two months.
If the severe focal abnormality lessens and theimprovement continues over several weeks, it isunlikely that the patient is suffering from an in-filtrating tumour but more probable that he has anarea of active cortical disease such as results upon-localized vascular insult, with cortical atrophy, orfollowing trauma or infection. On the other hand,steady worsening of the records is produced by aprogressive lesion and is almost certainly due to acerebral tumour. If- steady deterioration is seenthe patient should be referred for a neurosurgicalopinion. The occurrence of generalized highpressure waves in the record, which may bepresent without there being any papilloedema,kdemands that air study be carried out by ven-triculography rather than by encephalography,w'hich would be unsafe.Differentiation
Examination of' the features of the various.
cerebral tumours which can be expected in any casehas already been described and in this way theE.E.G. may be used in many cases as a differentialdiagnostic aid. It is essential, however, always toadd the E.E.G. results to the clinical and radio-logical findings, thus, in a case which by ven-triculography is shown to have a large hemispherelesion and which has a normal record, the likeli-hood of the tumour being a glioma is remote and itwill almost certainly be an avascular type ofcondition. Similarly, the patient who shows butindefinite radiological signs and yet has a rapidlyworsening E.E.G. most probably has an infiltratingand highly malignant tumour.
It is generally valueless, in differential diagnosis,to depend on only one record and serial recordingswill be found to throw considerable light on thenature of the lesion. It is, of course, quite easy tocarry out serial recordings in special neurologicalcentres, the method not distressing the patient,being quite painless and devoid of risk. By studyof the various appearances which have been de-tailed above, it will be seen that if a normal E.E.G.is obtained in a case of cerebral tumour, themethod cannot be considered to have failed, butit has in fact thrown light on the nature of thetumour. This particularly applies in the meningio-mata. The presence of more than one focalabnormality suggests that the lesions are meta-static; though if these are observed in both frontalareas it is more likely that there has been a spreadof a primary frontal tumour into the corpuscallosum. The practice of so-called blind analysisis quite worthless and in every case as many de-tails as possible should be given to the physicianwho is interpreting the record so that the maximumvalue of the method can be obtained.
ControlAfter surgical or radiological treatment has been
given to any case of cerebral tumour, the recordswill be seen to improve in a dramatic way in asuccessful case; persistence of a severe focalabnormality, however, is of poor prognosis andheralds the return of the patient's symptoms. Theoccurrence of post-operative epilepsy may beanticipated by the appearance in the records of anincreasing amount of paroxysmal epileptic activityand the appearance of these larval attacks mayprecede by years the development of clinical fits.The first sign of return of symptoms due to a re-currence of the tumour will either be focal or, inthe case of posterior fossa tumours, will begeneralized when slowing of the alpha rhythm isthe earliest abnormality to be seen. Completeabsence of the cortical potentials in any one par-ticular area following treatment indicates thatabsolute cell aestruction has taken place there, and
May 1952 2grlcopyright.
on June 1, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.28.319.283 on 1 M
ay 1952. Dow
nloaded from
292 POSTGRADUATE MEDICAL JOURNAL May 195Z
that no resolution is possible. Any persistentsymptoms connected with the affected area can beexpected to be permanent.
ConclusionsThe electroencephalogram must be regarded
merely as an ancillary method of diagnosis whenit is used in cases of cerebral tumour and, just asthe results obtained from other forms of laboratorystudy are supplementary to the clinical findings, sothe electroencephalographic reports in each patientmust be blended by the neurologist with thepathological and radiological findings to form abroad background to the clinical scene.
The electroencephalogram should not be em-ployed to demarcate the anatomical limits of acerebral tumour, since this can be achieved soaccurately in the majority of cases by the variousradiological methods, but rather should it be usedas a sensitive indicator of the changes in corticalphysiology which may be brought about in statesof cerebral pathology. In this way the electro-encephalogram will be found to represent a newdimension in the widening scheme of intracranialdiagnosis.The electroencephalogram can play an important
part in the observation and control of proven casesof cerebral tumour.
BIBLIOGRAPHY
ADRIAN, E. D. (I935), Proc. Roy. Soc. Mfed., 29, 197.BASSETT, R. C., and BAGCHI, B. K. (I947), Univ. Hosp. Bull.
Ann. Arbor., 13, I I.BAUDOUIN, A., PUECH, P., FISCHGOLD, H., and LERIQUE-
KOECHLIN, A. (1946), Sem. H p., Paris, 26, I226.BERGER, H. (I931), Arch. f. Psychiat., 94, I6.BERGER, H. (1933), Ibid., I00, 301.BUCHTHAL, F., and BUSCH, E. (I947), Acta. Psych. Neurol.,
22, 9.COBB, W. A. (I944), .7. Neurol. Neurosurg. Psychiat., 7 .96.COBB, W. A. (I950), Chap. 9, ' Electroencephalography,' edited by
Hill, J. D. M., and Parr, G.; Macdonald and Co.GIBBS, F. A., MONRO, D., and WEGNER, W. R. (I94I), New
Eng. Y. Med., 225, 279.
HINES, C. G., TENNY, L. H., and HUGHES, J. (I944), NavMed. Bull. Wash., 42, 10.
HOEFER, P. F. A., SCHLESINGER, E. B., and PENNES, H. H.(1946), Trans. Amer. Neurol. Ass., 52.
KERSHMAN, J., CONDE, A., and GIBSON, W. C. (I949),Arch. Neurol. Psychiat., 62, 255.
PARSONS-SMITH, B. G. (1949), 'M.D. Thesis,' CambridgeUniversity.
SCHLESINGER, B., and STRAUSS, H. (I947), J. Mt. SindiHosp., I4, 47.
WALTER, W. G. (1936), Lancet, ii, 305.YEAGER, C. L., BALDES, E. J., CRAIG, W. McK., and WOLT-
MAN, H. W. (I940), Proc. Mayo Clin., 15, I47.YEAGER, C. L., and LUSE, S. S. (1945), Arch. Neurol. Psychiat.,
54, 197.
'CONCERNING ANAESTHESIA'A series of Papers reprinted fromthe Postgraduate Medical Journal50 pages 2/- per copy
SPINAL ANALGESIABy William W. Mushin, M.A., M.B., B.A., F.F.A., R.C.S.
INHALATION ANAESTHESIABy John Gillies, C.V.O., M.C., M.B., Ch.B., F.R.C.S.E., D.A.
A SYSTEM OF ANAESTHESIA USINGD-TUBOCURARINE CHLORIDE FOR
CHEST SURGERYBy T. Cecil Gray, M.D., D.A., F.F.A., R.C.S.
ANALGESIA IN OBSTETRICSBy P. J. Helliwell, M.B., Ch.B., D.A., and A. Michael Hutton,
M.R.C.S., L.R.C.P., D.A.
GENERAL ANAESTHESIA FOR DENTAL SURGERYBy W. S. McConnell, M.B., B.S., D.A.
REGIONAL ANAESTHESIABy Alan Hunt, D.M., M.Ch., F.R.C.S.
POST-OPERATIVE CAREBy John Beard, M.D., D.A.
Published byTHE
FELLOWSHIP OF POSTGRADUATE MEDICINE60 Portland Place, W.I
CEREBRAL TUMOURSReprinted from the Postgraduate Medical Journal
PRICE:2/9
POST FREE
EDITORIAL: SIR VICTOR HORSLEY
THE PATHOLOGY OF INTRACRANIAL TUMOURSDorothy S. Russell, M.D. (Lond.), Sc.D. (Camb.).
F.R.C.P. (Lond.)VIRAL INFECTIONS OF THE HUMAN NERVOUS
SYSTEMAlbert B. Sabin, M.D.
TUMOURS OF THE FRONTAL LOBEGeoffrey Jefferson, M.S.. F.R.C.S., F.R.C.P., F.R.S.
PITUITARY, PINEAL AND THIRD VENTRICLE TUMOURSJoe Pennybacker, M.D., F.R.C.S.CEREBRAL ANGIOGRAPHY
J. W. D. Bull, M.A.. M.D., M.R.C.P., D.M.R.
THE ORTHOPAEDIC REHABILITATION OF A PATIENTAFTER EXaSION OF A CEREBRAL TUMOUR
Wylie McKisock, O.B.E., M.S., and K. I. Nissen, F.R.C.S.
SPASTIC PARAPLEGIA IN MIDDLE AGEColin Edwards, M.R.C.P.
Published byTHE FELLOWSHIP OF
POSTGRADUATE MEDICINE
60, Portland Place, London, W.1
copyright. on June 1, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.28.319.283 on 1 May 1952. D
ownloaded from





























