Embed Size (px)
Citation preview
VOLUME 18 l ISSUE 4 l APRIL 2019
CSJTHE CLINICAL SERVICES JOURNAL
W W W . T E S T M E D I C A L . C O . U K
Alternative test methods for washer disinfectors

Most of the time these advances arepositive and can save vital time and moneyfor the Trust, but how would a user knowthey are getting the same quality of test? Thisis a key consideration as any contamination,be it protein or microbial, needs be flaggedup accurately and in a way that is compliantwith the guidance. Historically there havebeen several examples where a method oftesting has become popular ‘in the field’ dueto ease or cost only to found ineffective whenguidance changes.
The ideal testing method would beperformed in situ, low cost and provide
Alternative test methodsfor washer disinfectors
instant and reliable results. Discussed beloware some examples of the alternative testingmethods that have been employed in the lastdecade or so. These fulfil many of the abovecriteria however the user should be awarethat no test method is perfect and they maybe sacrificing vital elements of the detectionmethod to save time or money.Understanding the science behind the testsis key to making the right decision for thedepartment or process.
A quicker way to detect bacteria: PCRTraditional microbiology has always beenlimited by the speed that bacteria, yeasts orfungi grow as the way that they are detectedis visual; individual bacteria in a watersample need to grow into a colony of millions that can be seen unaided by themicrobiologist’s eye. These microorganismscan have different growth rates dependant onthe species and can take anywhere between24 hours and 28 days to grow in anincubator.
Therefore, if you are looking for species ofPseudomonas this may be as quick as 24hours but Legionellae are slower and take upto 10 days to grow into colonies. Species ofthe Mycobacteria genus are slower still and a28-day incubation is needed to ensure eachhas had enough time to grow. These agarplate-based methods are considered the goldstandard of microbiology, they are trustedand well understood.
A faster and more direct method would be infinitely more useful for the modernendoscopy or CSSD department. However,the trouble with detecting bacteria is that in trying to directly detect small numbers of bacteria any ‘signal’ generated is going to be too weak to be picked up by aninstrument or detector.
Waiting for them to multiply into biggernumbers by themselves is slow and requires the exact right growth conditions. A way to speed this up is to specifically
Tests can be critical in detecting failures ofthe process and help the user detect thingsthat can’t be seen by eye; proteins, bacteriaand residual process chemicals. For anygiven test requirement there may be severalmethods for the user to choose between andwithout having knowledge of the scienceinvolved or consulting an AE(D) it can beeasy to make the wrong choice. Off-the-shelftest kits are promising faster and easierresults and it can be tempting to move awayfrom the more traditional testing methodsthat can be carried out in-house, especiallywhen cost is a determining factor.
Managing a testing schedule for a busy endoscopy or sterile-services department can be a challenging task for hospital staff. As David Woods,operations manager for T.E.S.T. asserts, each type of machine will require different quarterly, annual and weekly tests - and it can be difficult to keep up with guidance which is being constantly updated.
The current method of testing Mycobacteria is membrane filtration and 28-day incubation.
2 I WWW.CLINICALSERVICESJOURNAL.COM REPRINTED FROM APRIL 2019
DECONTAMINATION & STERILISATION
REPRINTED FROM APRIL 2019 WWW.CLINICALSERVICESJOURNAL.COM I 3
DECONTAMINATION & STERILISATION
Weekly tests for endoscope washers
grow or ‘amplify’ small parts of the bacteriathat can be more easily and quickly detected.This is the realm of molecular biology, whichis a branch of biology established after thediscovery of DNA and how it can bereplicated and controlled using enzymes.This process of replication is called PCR orPolymerase Chain Reaction.
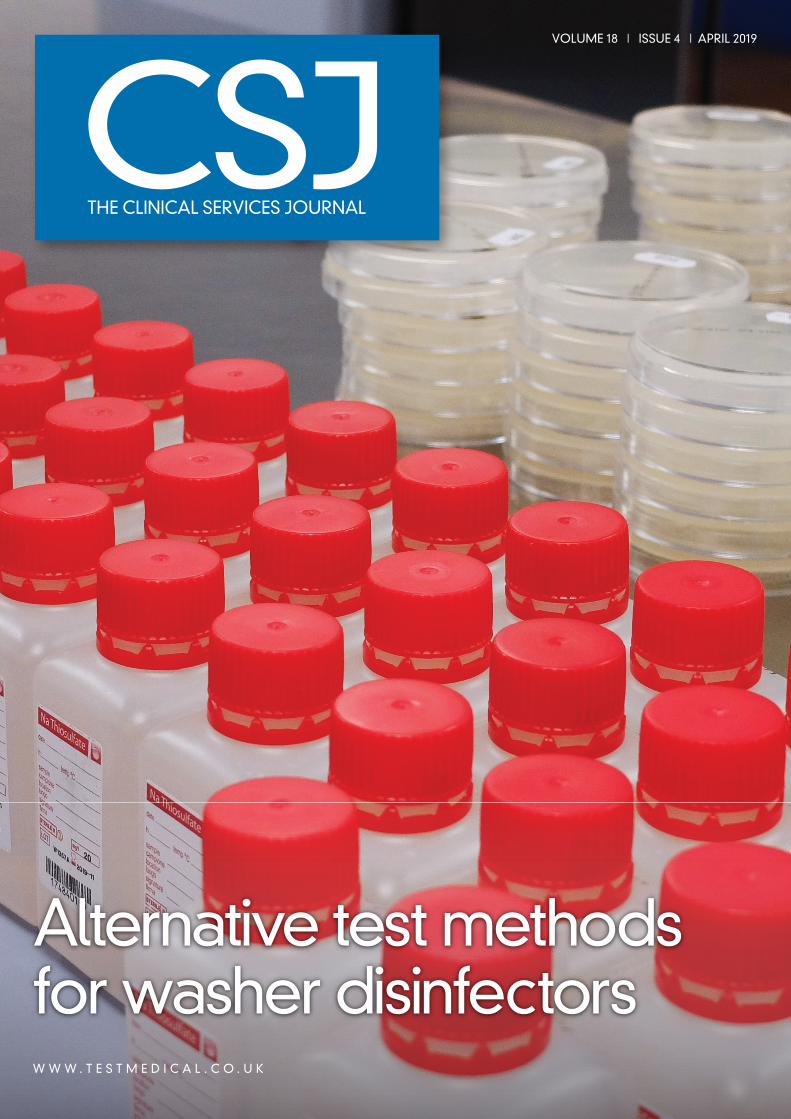
The principle of PCR is as follows: Thebacteria in a sample are broken open torelease their DNA from inside the cell. Shortpieces of DNA (primers) are used to ‘find’ theregion to be amplified and new copies ofDNA are created using a type of DNA-building enzyme (polymerases). The processis carried out by varying the temperature overa thermal cycle which takes just minutes. Asthis thermal cycle is continuously repeatedthe DNA will replicate exponentially over thecourse of a few hours. This large amount ofDNA produced can be easily detected byeither fluorescence or separating on a gelthrough its electrical charge (electrophoresis)
Advantages: PCR can be extremely rapid andvery specific. In just a few hours thepresence or absence of a single species canbe confirmed along with a quantitativemeasure of the amount of original DNA (inGenomic Units as opposed to ColonyForming Units).
Disadvantages: The technique must becarried out in the laboratory environment asDNA contamination is a risk. PCR will alsodetect dead bacteria that don’t necessarilypresent any infection control risk, althoughtechniques have been developed which gosome way to address this issue. Because ofthe various techniques employed by eachlaboratory it is very difficult to compareresults and there is no ‘standard’ method tojudge compliance. Sensitivity is a majorproblem, although PCR can theoreticallydetect single bacteria, because of the smallvolumes used in the method bacteria mayneed to be in the tens or hundreds in a watersample to be detected reliably.
In the healthcare setting the approachneeds to be flexible and the impact on thedecontamination process should beconsidered, as shutdown due to failed resultsand/or major refurbishment could have“serious consequences for patient care”(HTM 01-06 Part E, 2016). Unless cost isprohibitive, these methods can be run sideby side with the approved methods to give a complete picture and provide additional
assurance. The user needs to make adecision based on the urgency of the resultsand take a risk-based approach before usingPCR to replace well established plate-basedmicrobiology to detect bacterial pathogens.PCR is not the only rapid molecular biologymethod, but it is the most common; othertechniques involving enzymes and antibodiesare emerging but none that have theflexibility of the PCR technique. The assaycan be adapted to not only quantify theamount of DNA but specific species andgroups of organisms can be isolated basedon their unique genetic material.
ProteinTesting for protein is crucial on reusablemedical devices as it provides a valuableindicator of the cleaning efficacy. Proteinswill be introduced to the external and internalsurfaces during patient procedures and willmainly be comprised of blood components;albumins, globulins and fibrinogen andcomponents from mucosa; mucins,glycoproteins and various enzymes. Allproteins are composed of amino acids, thereare 21 types of amino acid and detection ofthese (and the bonds between them) formsthe basis of most instant protein tests. Thereare two categories of colour-change typetests, those which use copper ions and thosewhich use dyes to detect proteins.
Copper based protein testsThe reduction of copper to form a colouredcomplex forms the basis of the biuret andLowry methods. These require a peptiderather than free amino acids as it relies on thestructure of the amino acids when in thepeptide chain. A modified version of thebiuret reaction is the BCA (bicinchoninic acid)test and responds more uniformly to differentproteins at higher levels of sensitivity. TheBCA method is one of the most commonlaboratory-based tests for quantifying protein.
Other protein testsThere are an abundance of different dye-based assays but the most common visuallyassessed test is the Coomasie blue/Bradfordmethod which is simple to carry out in a test-kit form at room temperature withoutincubation. This dye was originallydeveloped for textiles but now forms thebasis of most protein test kits. This hasreplaced the ninhydrin test which was foundto be not sensitive enough to demonstratethe <5μg sensitivity required by the latestguidance.
In the quest for more instant andenumerable methods some alternative testshave been employed. The Coomassie blueand ninhydrin test kits are often limited asthey are not quantitative (some are semi-quantitative by visual colour comparison).This has led to the popularity of ATP basedmethods as a measure of cleaning efficacy.1
Although ATP does provide some measure ofcontamination, as it will indicate current andpast contamination from living organisms,ATP (adenosine triphosphate) is a universalenergy molecule and is derived from a DNAnucleotide and in no way can be considereda protein. It is important that this is not usedin place of a test where a protein isspecifically required to be measured, likesurgical instruments.
n Weekly safety checksn Daily tests (including ACT)n Process challenge device cleaning efficacyn Water hardnessn Water conductivityn Final rinse TVC
The PCR process: The denaturation, annealing and extension is repeated multiple timesto create large amounts of the specific DNA section of interest.
n Weekly safety checksn Daily testsn Water hardnessn Water conductivityn Automatic Control Test (ACT)
Weekly tests for instrument washers
Protein testing

Some methods must be read using UVexcitation and detection of fluorescence. OPA(ortho-phthalaldehyde) based reagents havebeen used to detect proteins, peptides andamino acids for over 30 years in thelaboratory.2 Recently this has been applied to surgical instruments for a more directmeasure: When the reagent is applied as a spray, it is possible to detect the protein in situ without needing to swab theinstrument, this method of imaging isquantifiable, based on the intensity offluorescence.
Choosing a protein testWhen purchasing a protein test kit, inaddition to cost and ease of use, it isimportant for the user to consider:n Sensitivity ie: the lowest detection
level of protein in micrograms (μg). For surgical instruments this should be under 5μg for each instrument side
n Variability of sensitivity between differenttypes of proteins (size and amino acidcomposition)
n Calibration and traceability are vital toassuring the test results: ensure there is a means to calibrate the equipment to certified standards
n If it is being bought off-the-shelf, check the test kit is CE marked.
Limitations of protein testsAt the time of publication of HTM 2030 in1997 the focus of protein removal was toreduce the risk of prion transmission. Overtime there has been a gradual shift awayfrom the qualitative Ninhydrin tests to othertypes of assay. Each method of determiningprotein content has limitations of either itssensitivity or practicality in a given situation.Because of the nature of the chemistry andequipment involved some test methods maystruggle to achieve the required sensitivity.3
All tests have a certain degree of variability,so they may be less sensitive to certain typesof protein from different sources. Also,without complex laboratory techniques suchas mass-spectrometry it is not possible toidentify exact types of protein.
Direct measurement with UV detectioncan have excellent sensitivity but complexinstruments and endoscopes will be difficult,if not impossible, to image using thismethod. Each method should also haveavailable a calibration standard, so that theinstrument can be periodically verified andthe results are traceable. Although issues do
exist with these methods, cleaning processeshave come under great scrutiny in recentyears and have been greatly improved as aresult. Protein testing should now be carriedout weekly as part of the cleaning efficacywith a process challenge device.
Methods to detect bacterialendotoxinsBacterial Endotoxins (Pyrogens) arefragments of bacterial cells that canpotentially generate an immune response inpatients when present on instruments.Endotoxin is a broad term referring to manydifferent types of immunostimulatorymolecules but mainly lipopolysaccharidesfrom the membranes of gram-negativebacteria are referred to. As these substancescan be present, or even are generated, afterdeath of the bacterial cell they present apatient risk even on sterile instruments.
Testing methods for these are mainlybased on biochemical assays involvingimmune components extracted from otherorganisms. The first testing methods used forendotoxins involved injecting the sample intolaboratory-bred rabbits and measuring therise in temperature from the fever thatresulted, hence the term ‘pyrogen’ (heat-producing). This method has now beenreplaced by more modern techniques whichuse immune components in vitro often in anautomated optical reader. The extract, fromhorseshoe crab blood is referred to as ‘lysate’.
Because of the complexity of the testmethods the analysis must be carried out inthe laboratory. The test is very sensitive tointerference and must be carried out withpositive (spiked) samples as well as astandard curve with each test so that thecolour change can be directly correlated to a certified reference standard endotoxin.
4 I WWW.CLINICALSERVICESJOURNAL.COM REPRINTED FROM APRIL 2019
Cross sectional view of how the ‘t-store’ surrogate device mimics the internal air-water channel of an endoscope.
In the healthcare setting the approach needs to be flexible and the impact on thedecontamination process should be considered, as shutdown due to failed resultsand/or major refurbishment could have “serious consequences for patient care”
DECONTAMINATION & STERILISATION

REPRINTED FROM APRIL 2019 WWW.CLINICALSERVICESJOURNAL.COM I 5
DECONTAMINATION & STERILISATION
The user should be aware of the differentmethods to assess the suitability
Gel clot tests: These are normally carried outin a test tube and can be limit tests (notquantitative) or semi quantitative methods.The test relies on the operator observing thelysate clotting into a firm gel and so may besubject to inter operator variability. If the testfails the specification, it may be expressedsimply as ‘greater than’ the sensitivity of thetest and these results may not always bemeaningful, dependent on the specificationbeing applied.
Photometric and chromogenic techniques:The reaction of the lysate in these tests canbe more quantitively measured by thedevelopment of a turbidity or colorimetrically.These are often in conjunction with amicroplate reader so that the correlation ofthe reaction onset time can be automaticallycorrelated to traceable endotoxin value.
Most of these methods are based on theBritish/European Pharmacopoeia standardmethods which is considered the goldstandard for this test. As with allsubcontracted laboratory analysis the usershould seek reassurances that the laboratoryhas UKAS accreditation for the testingmethod. This ensures that the qualitymanagement system is in place to controland monitor operator training, proficiencytesting schemes and method validation.
Residual chemicalsWasher disinfectors use several chemicals aspart of the cycle, namely detergents,disinfectants and rinse aids. These must beremoved by rinsing with water during severalpoints during the process to ensurechemicals do not carry-over into the nextstage and potentially reduce the activity ofdisinfectants and other chemicals.Furthermore, instruments must be free fromunintended chemical contamination after the process. Testing the rinse water will givea measure of the level of residues comparedto the ‘control’ source water sample. The twomain methods for assessing residualchemicals are:n Total Organic Carbon (TOC) – Almost all
detergents and disinfectants will containorganic carbon, this can be determined by laboratory analysis
n Electrical Conductivity – Dissolved ionsfrom process chemicals remaining in therinse water will decrease the electricalresistance of the water and increase theconductivity reading. Comparison of thetwo readings can determine the relativelevel of residues.
These methods will help to ensure theinstruments remain free from chemical residues,however other methods can be recommendedby the manufacturer that may be more specificto the chemical used in the process. Someprocess chemicals are permitted in the finalrinse water as they are intentionally added to
discourage microbial proliferation in the rinsewater. These may include low-leveldisinfectants such as chlorine-basedcompounds that have been demonstrated tobe non-toxic or at a low enough concentration.Off-the-shelf test kits or monitoring strips maybe used to routinely check the levels present inthe final rinse water.
Air monitoringChemicals used in the process may producehazardous gases and become a risk to theoperator. Monitoring can be performedperiodically or with fixed equipment to ensurework exposure limits are not being exceededduring the process. It is a requirement of theHTM to ensure yearly and on revalidation thatchemical vapours are measured using gasmonitoring equipment. This is usually withsensors that measure the infra-red absorptionby the gas or with an electrochemical sensordependent on the type of gas. This testingmay not be part of the main EWD service andvalidation schedule so the user should seekout an independent testing provider.
Disinfection efficacy and surrogate devicesIn thermal washer disinfectors disinfectionefficacy is a relatively straightforwardmeasurement of the temperature, endoscopewasher disinfections however can have manymore factors which affect the chemicaldisinfection. Routine microbiological testing ofthe disinfection efficacy has been removedfrom the latest guidance which means thatpotential disinfection problems may gounnoticed. The current alternative test methodis to sample endoscopes for naturalcontamination that remains after the process,as opposed to inoculating a surrogate devicewith live organisms. This is currentlyrecommended only if a problem is suspected.The AE(D) or user may request the disinfectionefficacy is proven using the method describedin ISO 15883 Part 4 to demonstrate thewasher disinfector is still performing inaccordance with its original type testing.
The user should be aware that there are alarge variety of surrogate devices being usedon EWDs and not all of them accurately mimican endoscope. According to the internationalstandard the surrogate device should containtrumpet valves and connection ports so thatthe fluid pathway reflects the actualinstrument and connection method.
Drying cabinets and storage systems: Thesepieces of equipment are often less complex indesign than an endoscope washer disinfector
but still have a significant risk associated withthem if not properly used and maintained.Surrogate devices used in these systems needto reflect the complexity of the internalchannels, which can make drying significantlymore difficult than a unbifurcated length oftubing. Testing conditions should control forfactors that present a risk such as connectionmethods and the initial state of the endoscope,which will have an unknown residual volumeof water present from the EWD process.Furthermore, this residual water is notguaranteed to be free of bacteria. A sterile, drylength of tube will not adequately control forthis initial state: if surrogates are to be used inplace of endoscopes during routine testing thenthe requirement Annex E2 of EN 16442:2015to clean and disinfect beforehand according tothe ‘procedure in force in the unit’ would betterreflect actual conditions.
In conclusion, users should be cautious inreplacing test methods purely because it morecost effective or a new technology. If possible,carry them out side by side and seek theadvice of the AE(D) until the method isincorporated into the official guidance.Current testing methods should be constantlyreviewed as the fast pace of development inthese areas means they may quickly becomeobsolete or non-compliant. CSJ
References1. Parohl et al. (2017) Monitoring of endoscope
reprocessing with an adenosine triphosphate (ATP) bioluminescence method. GMS Hygiene andInfection Control
2. Friter et al. (1988). OPA method modified by use of N, N-dimethyl-2-mercaptoethylammoniumchloride as thiol component. Fresenius Journal of Analytical Chemistry
3. Lipscomb et al. (2006) The sensitivity of approvedNinhydrin and Biuret tests in the assessment ofprotein contamination on surgical steel as an aid to prevent iatrogenic prion transmission. Journal of Hospital Infection
About the authorDavid Woods BSc (Hons) has been theOperations Manager for T.E.S.T. since2014 and is an Authorised Person(Decontamination). Since universityDavid has worked as a microbiologist and managed sterilisation and washer-disinfector validation processesas part of the range of independentservices offered by T.E.S.T.
The AE(D) or user may request the disinfectionefficacy is proven using the method describedin ISO 15883 Part 4 to demonstrate the washerdisinfector is still performing in accordance with its original type testing.