Embed Size (px)
Citation preview

Inside This
Acknowledgment ................................2
CME Information and Instructions ........................................3
Methodology ......................................6
The WIN-R Trial: Early Observations on Weight-Based Dosing of Peginterferon alfa-2b/Ribavirin ................................7
Treating Interferon/RibavirinNonresponders ..................................10
References ........................................11
Dear Colleague:
This newsletter represents the first part of the expanded five-part CME compendium thatcomprises The Clinician’s Companion VI. The four newsletters, representing Parts 1 through 4,will feature timely reporting of the latest developments in the field, whereas the monograph,Part 5, will provide in-depth coverage of some of the most important issues in hepatitis Ctoday. Content for the series was developed at a meeting that featured expert presentations,panel discussions, case studies, and recommendations gathered via survey from anationwide panel of leading experts in hepatitis C. This newsletter, representing Part 1 ofthe series, covers preliminary findings from ongoing studies of peginterferon/ribavirin.
In August 2001, the Food and Drug Administration (FDA) approved combination therapywith peginterferon alfa-2b 1.5 µg/kg QW plus ribavirin 800 mg/d for treatment of chronichepatitis C. Data from Manns et al,1 published in The Lancet, showed that this regimenproduces a sustained virologic response (SVR) in 54% of patients overall, 42% of patientsinfected with hepatitis C virus (HCV) genotype 1, and 82% of those infected with HCVgenotype 2 or 3. Based on these findings, peginterferon/ribavirin has since replacedinterferon/ribavirin as the standard of care. Studies of the investigational agentpeginterferon alfa-2a, in combination with ribavirin, have been reported at nationalconferences, with SVR rates of 56% overall, 46% in genotype 1, and 76% in genotype 2/3.2
Later in this newsletter, John B. Gross, MD, looks at the extent to which the increasedefficacy of peginterferon/ribavirin over standard interferon/ribavirin provides new hopeof SVR to those who failed to respond to prior therapies.
Retrospective analyses have identified additional means of improving treatment outcomes.Analysis of the Manns et al1 data determined that the highest SVR rates were attained bypatients who received weight-based dosing of peginterferon alfa-2b (1.5 µg/kg) and thehighest doses of ribavirin per mg/kg of body weight (>10.6 mg/kg). These patients had anSVR rate of 61% compared with 50% for those who received the same dose of peginterferonalfa-2b with <10.6 mg/kg ribavirin. Patients who received >10.6 mg/kg ribavirin also hadlower relapse rates. These retrospective observations led to the initiation of a prospectiveinvestigation of weight-based dosing in the WIN-R (Weight-Based Dosing of Interferon andRibavirin) study. In the first section of this newsletter, Ira M. Jacobson, MD, discussespreliminary observations from WIN-R—the largest hepatitis C treatment trial ever conducted.
We are pleased to bring you this update on peginterferon/ribavirin, and hope that youfind it, and the rest of The Clinician’s Companion VI, informative and relevant to yourpatient care.
Sincerely,
Co-Chair Co-Chair
Willis C. Maddrey, MD Eugene R. Schiff, MDUniversity of Texas University of Miami School of MedicineSouthwestern Medical Center at Dallas Miami, Florida
The Clinician’s Companion VI: Expert Perspectives on Contemporary Clinical Issues in Hepatitis C
Release Date: September 1, 2002.This five-part newsletter andmonograph series has been plannedand produced in accordance with theACCME Essential Areas and Policies. Thisenduring activity will be reviewed within 1 year of this date and rereleased, or itsdesignation for CME credit will become invalid.
For additional
information on
hepatitis C, go to
www.projectsinknowledge.com
Part 1 of 5: Emerging Advances: Preliminary Findings FromOngoing Studies of Peginterferon/Ribavirin
Part 1: Tx Reporter: EmergingAdvances: Preliminary FindingsFrom Ongoing Studies ofPeginterferon/Ribavirin
Part 2: Tx Reporter: PredictingResponse and PromotingAdherence toPeginterferon/Ribavirin
Part 3: Tx Reporter: Mild Disease: To Treat or Not to Treat?
Part 4: Tx Reporter: What ConstitutesTreatment Response?
Part 5: Monograph: Recent InsightsInto HCV Virology andTreatment of Chronic Hepatitis C
Look forward to the NEWClinician’s Companion VI series:
2
R E P O R T E RSM : G A S T R O E N T E R O L O G Y
Nezam H. Afdhal, MDAssociate Professor of MedicineHarvard Medical SchoolChief of HepatologyBeth Israel Deaconess Medical CenterBoston, Massachusetts
Harvey J. Alter, MDChief of Infectious DiseasesAssociate Director for ResearchDepartment of Transfusion MedicineNational Institutes of Health Bethesda, Maryland
Bruce R. Bacon, MDJames F. King, MD, Endowed Chair in
GastroenterologyProfessor of Internal MedicineSaint Louis University School of MedicineDirector, Division of Gastroenterology
and HepatologySaint Louis University Liver CenterSt. Louis, Missouri
Robert S. Brown, Jr, MD, MPHMedical DirectorCenter for Liver Disease and
TransplantationColumbia College of Physicians &
SurgeonsNew York-Presbyterian HospitalNew York, New York
Robert L. Carithers, Jr, MDProfessor of MedicineUniversity of Washington School of MedicineSeattle, Washington
Massimo Colombo, MD Professor and ChairmanDivision of HepatologyIRCCS University Polyclinic HospitalMilan, Italy
Robert G. Gish, MDMedical DirectorLiver Transplantation ProgramCalifornia Pacific Medical CenterSan Francisco, California
John B. Gross, Jr, MDAssociate Professor of MedicineHead, Hepatobiliary ClinicRochester, Minnesota
Ira M. Jacobson, MDChief, Division of Gastroenterology and
Hepatology Medical Director Center for the Study of Hepatitis CWeill Medical College of
Cornell UniversityNew York, New York
Barbara H. McGovern, MDAssistant Professor of Medicine Tufts University School of MedicineBoston, Massachusetts
John G. McHutchison, MDMedical Director, Liver TransplantationDivision of Gastroenterology/HepatologyScripps Clinic and Research FoundationLa Jolla, California
David R. Nelson, MDAssociate ProfessorChief, Section of Hepatobiliary Diseases Medical Director, Liver TransplantationUniversity of Florida College of MedicineGainesville, Florida
Thierry M. Poynard, MD, PhDProfessor and Head,
Hépato-Gastro-Entérologie DepartmentGroupe Hospitalier Pitié-SalpêtriereUniversity of Paris VIParis, France
Charles L. Raison, MDAssistant ProfessorMind-Body ProgramDepartment of Psychiatry and
Behavioral SciencesEmory University School of MedicineAtlanta, GeorgiaStuart C. Ray, MDAssistant Professor of MedicineDivision of Infectious DiseasesThe Johns Hopkins University
School of MedicineBaltimore, MarylandDonald C. Rockey, MDAssociate Professor of MedicineDirector, Liver CenterDuke University Medical CenterDurham, North CarolinaAngelo Sangiovanni, MDDivision of Hepatology IRCCS Ospedale Maggiore of Milan University of MilanMilan, ItalyMark S. Sulkowski, MDAssistant Professor of MedicineThe Johns Hopkins University
School of MedicineBaltimore, MarylandMyron J. Tong, PhD, MDProfessor of MedicineUSC School of MedicineLos Angeles, CaliforniaSenior HepatologistDumont-UCLA Liver Cancer CenterLos Angeles, California
Teresa L. Wright, MDVeterans Administration Medical Center University of California–San FranciscoSan Francisco, California
ACKNOWLEDGMENTCo-chairs Willis C. Maddrey, MD, and Eugene R. Schiff, MD, and Projects In Knowledge gratefully acknowledge the contributions of the following persons in guiding the expert consensus development process and in creating the content of The Clinician’sCompanion VI: Expert Perspectives on Contemporary Clinical Issues in Hepatitis C:
George Abdelsayed, MDFrank Adams, DOAijaz Ahmed, MDClive Albert, MDShirish Amin, MDHarry Anastopoulos, MD Louis V. Antignano, MD Rex Antinozzi, MDSanjeev Arora, MDM. Samir Ayasso, MDShahid Aziz, MDMaher Azzouz, MDMichael Babich, MDWalid Baddoura, MDRobert L. Baker, MDNatarajan Bala, MDMarwan Balaa, MDChristopher N. Barrilleaux, MDR. Martin Bashir, MDIsaac Bassan, MDRichard Baum, MD
Mohammad Bawani, MDScott Becker, MDAlex Befeler, MDBrian Berk, MDMarc Bernstein, MDDavid Beswick, MDSandeep Bhargava, MDBahri Bilir, MDNuray Bilir, MDMartin Black, MDBennett L. Blitzer, MDTerry Box, MDWilliam Boyd, MDJoseph M. Bresnahan, MDNatalie Bzowej, MD, PhDWilliam Cassidy, MDMaurice Cerulli, MD Balu Chandra, MDKapil Chopra, MDAlroy Chow, MDLynn Cochran, MD
Stanley Martin Cohen, MDThomas J. Colturi, MDJeffrey Cooley, MDClayton Collins Coon, MDMichael Cox, MDDale Coy, MDRaquel Croitoru, MDDouglas Dalke, MDSamuel Daniel, MDMitchell Davis, DORobert Davis, MDRashad DeBaghi, MDLino DeGuzman, MDMichael De Micco, MDJoseph DePasquale, MDDavid Doman, MDRichard Eglow, MDStephen P. Esposito, MDW. Hunter Eubanks, MDRobert Fadden, MDFranco Felizarta, MD
Robert G. Finkel, MDAlan M. Fixelle, MDSteven L. Flamm, MD Ira L. Flax, MDJose Franco, MDBradley Freilich, MDJoseph S. Galati, MDDaniel R. Ganger, MDGabriel Garcia, MDRuel Garcia, MDAndrei Gasic, MDMichael Georgetson, MDRobert Gilbert, MDScott Gioe, MDJeffrey Goldstein, MDMichael B. Goldstein, MDStuart Gordon, MDNorman D. Grace, MDM. Bassam Haffar, MDNorman W. Haines, Jr, MDSteven-Huy Han, MD
The survey information presented in this activity reflects the consensus of the entire panel of contributors, including those listedabove, as well as:
3
TREATMENT REPORTER Emerging Advances: Preliminary Findings From Ongoing Studies of Peginterferon/Ribavirin
Tarek Hassanein, MDRonald J. Hauptman, MDJorge L. Herrera, MDRobert Herring, MDGary L. Hills, DOBrian K. Hudes, MDJoanne C. Imperial, MDMiled Jabor, MDJoseph Jackson, MDHyder Jamal, MDM. Mazen Jamal, MDRobert Jao, MDJohn Jolley, MDIsaac Kalvaria, MDSteven Katzman, MDJohn Kauffman, MDBarry Kaufman, MDRaymond Kenny, MDKelly Kensing, MDKieran Key, MDMandana Khalili, MDAlan E. Kilby, MDJohn P. Kirchner, MD, PhDRobert B. Kirkpatrick, MDMartin S. Kleinman, MDFrank Klion, MDMarcelo Kugelmas, MDShashi Kumar, MDPaul Kwo, MDGerry Lake-Bakaar, MDAnne Larson, MDEric Lawitz, MD Truong-Sinh Leduc, MDCarroll B. Leevy, MDMichael J. Levinson, MD
Robert Lewis, MDMichael Lindner, MDLawrence Lumeng, MDKip Lyche, MDMichael F. Lyons, MD Oscar Maldonado, MDSuresh Malholtra, MDKent Martin, MDDaniel Matloff, MDJonathan McCone, MDJohn D. McCracken, MDRobert McFadden, MDJeffrey Medoff, MDRobert H. Meichner, MDDaniel Meline, MDBarry Migicovsky, MDPeter Molloy, MDSamuel Moskowitz, MDSantiago J. Munoz, MDMark E. Murphy, MDMilton G. Mutchnick, MDAbdul Nadir, MDFarid Naffah, MDGuy Neff, MDFrank Nelson, MDTuan T. Nguyen, MDRod Nisi, MDFrederick Nunes, MDAnders Nyberg, MDLisa Nyberg, MDChristopher O’Brien, MDMary Pat Pauly, MDJohn Payne, MDRoger Perez, MDNeville R. Pimstone, MD
James Piper, MDArthur L. Poch, MDPaul Pockros, MDGary Poleynard, MDFred Poordad, MDAnthony B. Post, MDDavid C. Pound, MDBangaru Jayapraka Prakash, MDWilliam J. Provance, DORudra Rai, MDNatarajan Ravendhran, MDGurunath Reddy, MDThomas Reed, MDFrederic Regenstein, MDTerence N. Reisman, MDAdrian Reuben, MBBS, FRCPDonato Ricci, MDRonald Rinker, MDEarl G. Robbins II, MDS. Lawrence Rothman, MDRaymond A. Rubin, MDSammy Saab, MDKia Saeian, MDGeronimo Sahagun, MDWarren Schmidt, MDFayez Seif, MDWilliam Semon, MDThomas Sepe, MDAshok Shah, MDA. Obaid Shakil, MDThomas Shaw-Stiffel, MDMuhammad Sheikh, MDAlan Sheinbaum, MDRichard Sheinbaum, MDKenneth Sherman, MD, PhD
Ann Silverman, MDBruce Silverman, MDJames A. Singer, MDMaria Sjogren, MDRobert Sjogren, MD Dirk P. Slaker, MDColeman Smith, MDRichard Sperling, MDGary Spiegelman, MDJulie Spivack, MDTimothy Spurling, MDRichard Sterling, MDRobert Strauss, MDUma Sundaram, MDJ. Thomas Swan, MDDiana Sylvestre, MDMumtaz Tabaa, MDAndrew Talal, MDHelen Te, MDHillel Tobias, MDHuy Ngoc Trinh, MDVance Van Drake, MDJoseph L. Wang, MDPeter Wayne, MDLarry Weprin, MDScott L. Wiesen, MDIan Williams, PhD, MSIra R. Willner, MDRobert Wohlman, MDDavid C. Wolf, MDHarlan I. Wright, MDRockford Yapp, MDYuen S. Yee, MDGeoffrey Zucker, MD
CME INFORMATION AND INSTRUCTIONS
A. ACCREDITATIONProjects In Knowledge is accredited by theAccreditation Council for Continuing MedicalEducation to provide continuing medicaleducation for physicians. Projects In Knowledge designates thiseducational activity for up to 2.5 hours inCategory 1 credit toward the AMAPhysician’s Recognition Award. Eachphysician should claim only those hours ofcredit that were actually spent on theeducational activity. B. TARGET AUDIENCEThis CME activity is designed forgastroenterologists and hepatologists whodiagnose and treat patients with chronichepatitis C virus (HCV) infection, and whoneed immediate and practical information toaddress real-world clinical challengesassociated with care of their patients. It isalso designed for physicians who may becalled upon to provide basic education onhepatitis C to their communities. Anintermediate to advanced level of expertisein caring for patients with HCV infection isassumed.C. LEARNING OBJECTIVESThe learning objectives for The Clinician’sCompanion VI include the following:• Discuss advances and new directions in
HCV research, including virology, naturalhistory, treatment, and prevention
• Examine new NIH consensus guidelines andhow they inform clinical decision making
• Formulate effective, individualizedtreatment strategies for patients withchronic HCV infection using pegylatedinterferon/ribavirin combination therapy
• Use diagnostic procedures, including HCVPCR and liver biopsy, in a timely fashionto determine treatment response
• Promote adherence to anti-HCV therapy bymanaging side effects and by providingappropriate psychosocial support
• Develop appropriate management strategiesfor different patient groups, includingpatients with HIV/HCV, mild disease,normal ALT levels, advanced liver disease,and hepatocellular carcinoma
D. ESTIMATED TIME FOR COMPLETIONEstimated time to complete course: 2.5 hours. E. FOR CME CREDITTo receive documentation of your participation:Read Parts 1, 2, 3, 4, and 5 of The Clinician’sCompanion VI.1. Complete the CME Posttest, Evaluation, and
Needs Assessment enclosed with Part 5.2. Send the forms to Projects In Knowledge,
One Harmon Plaza, Secaucus, NJ 07094, or fax to (201) 617-7333, beforeSeptember 1, 2003.
Projects In Knowledge will mail you acertificate of completion if you score 70% orhigher on the posttest. If you score lowerthan 70%, you will be given another chanceto take the posttest.
F. CONTENT DEVELOPMENT INFORMATIONThe Clinician’s Companion series is part ofProjects In Knowledge’s Education Initiativein Gastroenterology, which was created toadvance the knowledge base and clinical skillsof practitioners in the field; to facilitatecollaboration among thought leaders in research,academia, and clinical practice; and to providea forum for discussion among representativesfrom diverse sectors of the healthcare enterprise.Other educational activities in the EducationInitiative in Gastroenterology can be foundat www.projectsinknowledge.com.G. EDITORIAL STAFFEditor:Lauren A. CerrutoEducation Development:Dr. Deborah TeplowJo Hannah Villanueva, MDJane PerrottaProduction Editor:Kim SpinoH. DISCLOSURE INFORMATIONThe Disclosure Policy of Projects InKnowledge requires that faculty participatingin a CME activity disclose to the audienceany significant relationship they may havewith a pharmaceutical or medical equipmentcompany, product, or service that may bementioned as part of their presentation, aswell as any relationship with the commercialsupporter of this activity. This independent CME activity is supported byan unrestricted educational grant from
4
R E P O R T E RSM : G A S T R O E N T E R O L O G Y
George Abdelsayed, MD, has not specified any significantrelationships with industry. Frank Adams, DO, has not specifiedany significant relationships with industry. Nezam H. Afdhal, MD,has received grant/research support from AgouronPharmaceuticals, Inc, InterMune Inc, Isis Pharmaceuticals Inc, OrthoBiotech Products, LP, Roche Pharmaceuticals, and Schering; is aconsultant for Ortho Biotech Products, LP, and Schering; and is onthe speakers bureaus of AstraZeneca LP, Ortho Biotech Products,LP, Roche Pharmaceuticals, and Schering. Aijaz Ahmed, MD, hasreceived grant/research support from Schering; is a consultant forNovartis Pharmaceuticals Corporation, Ortho Biotech Products, LP,and Roche Pharmaceuticals; and is on the speakers bureaus ofNovartis Pharmaceuticals Corporation, Ortho Biotech Products, LP,and Schering. Clive Albert, MD, has received grant/researchsupport from Schering; and is a consultant for Schering andWyeth-Ayerst Pharmaceuticals. Harvey J. Alter, MD, is aconsultant for AcroMetrix, Ceris (France), and Roche Diagnostics.Shirish Amin, MD, has received grant/research support fromRoche Pharmaceuticals and Schering; and is on the speakersbureaus of AstraZeneca, Schering, TAP Pharmaceuticals Inc, andWyeth-Ayerst Pharmaceuticals. Harry Anastopoulos, MD, has notspecified any significant relationships with industry. Louis V.Antignano, MD, has received grant/research support fromSchering-Plough; and is on the speakers bureaus of JanssenPharmaceutica Products, LP, Prometheus Laboratories, RochePharmaceuticals, Salix Pharmaceuticals, Inc, Schering-Plough, andWyeth-Ayerst Pharmaceuticals. Rex Antinozzi, MD, is on thespeakers bureaus of AstraZeneca, Janssen Pharmaceutica Products,LP, Schering, and Wyeth-Ayerst Pharmaceuticals; and is a stockshareholder in Pfizer Inc. Sanjeev Arora, MD, has receivedgrant/research support from InterMune Inc, RochePharmaceuticals, and Schering. M. Samir Ayasso, MD, has notspecified any significant relationships with industry. Shahid Aziz,MD, has not specified any significant relationships with industry.Maher Azzouz, MD, is on the speakers bureau of Schering-Plough.Michael Babich, MD, has not specified any significantrelationships with industry. Bruce R. Bacon, MD, has receivedgrant/research support from Amgen Inc, Bristol-Myers SquibbCompany, Gilead Sciences, Inc, GlaxoSmithKline, RocheLaboratories, and Schering-Plough; is a consultant for, or memberof an advisory board of, Akros Pharma Inc, Bayer Diagnostics, ColeyPharmaceutical Group, GeneTrol Biotherapeutics, GlaxoSmithKline,Maxim Pharmaceuticals, Inc, Metaphore Pharmaceuticals,Schering-Plough, and Serono Symposia International; and is on thespeakers bureaus of Axcan Pharma Inc and Schering-Plough. WalidBaddoura, MD, is on the speakers bureaus of, and has participatedin clinical trials for, Roche Pharmaceuticals and Schering. Robert L.Baker, MD, has not specified any significant relationships withindustry. Natarajan Bala, MD, is a consultant for and is on thespeakers bureau of Schering. Marwan Balaa, MD, has receivedgrant/research support from Schering; and is on the speakersbureaus of Eisai Inc, Schering, and TAP Pharmaceuticals Inc.Christopher N. Barrilleaux, MD, has not specified any significantrelationships with industry. R. Martin Bashir, MD, is on thespeakers bureaus of Schering-Plough and Wyeth-AyerstPharmaceuticals. Isaac Bassan, MD, has not provided disclosure.Richard Baum, MD, has not provided disclosure. MohammadBawani, MD, has received grant/research support from RochePharmaceuticals and Schering-Plough; and is on the speakersbureau of AstraZeneca. Scott Becker, MD, is on the speakersbureaus of AstraZeneca, Janssen Pharmaceutica Products, LP, SalixPharmaceuticals, Inc, Schering, and TAP Pharmaceuticals Inc. AlexBefeler, MD, has not specified any significant relationships withindustry. Brian Berk, MD, has received grant/research supportfrom Bristol-Myers Squibb Company and Ortho Biotech Products,LP; and is on the speakers bureau of Schering-Plough. MarcBernstein, MD, is a stock shareholder in Amgen Inc, Bristol-MyersSquibb Company, Merck & Co, Inc, and Pfizer Inc. David Beswick,MD, is on the speakers bureaus of AstraZeneca, Schering, and TAPPharmaceuticals Inc. Sandeep Bhargava, MD, has not specifiedany significant relationships with industry. Bahri Bilir, MD, has notprovided disclosure. Nuray Bilir, MD, is on the speakers bureau ofWyeth-Ayerst Pharmaceuticals. Martin Black, MD, is on thespeakers bureaus of Amgen Inc, Axcan Schwarz LLC, GlaxoWellcome Inc, and Schering. Bennett L. Blitzer, MD, has notspecified any significant relationships with industry. Terry Box,MD, has received grant/research support from AstraZeneca,Hoffmann-La Roche Inc, Novartis Pharmaceuticals Corporation,Schering-Plough, and TAP Pharmaceuticals Inc; and is on thespeakers bureaus of Hoffmann-La Roche Inc and Schering-Plough.William Boyd, MD, is on the speakers bureaus of GlaxoSmithKline,Schering-Plough, and Wyeth-Ayerst Pharmaceuticals. Joseph M.Bresnahan, MD, has not specified any significant relationshipswith industry. Natalie Bzowej, MD, PhD, is on the speakersbureau of Axcan Scandipharm Inc. Robert S. Brown, Jr, MD,MPH, has received grant/research support from Ortho BiotechProducts, LP, Roche Pharmaceuticals, and Schering; and is on thespeakers bureaus of Ortho Biotech Products, LP and Schering.Robert L. Carithers, Jr, MD, has received grant/research supportfrom Schering and Targeted Genetics Corporation; is a consultant
for Axcan Schwarz LLC, Roche Pharmaceuticals, and Schering; andis on the speakers bureaus of Roche Pharmaceuticals and Schering.William Cassidy, MD, has received grant/research support fromAventis Pharmaceuticals, GlaxoSmithKline, Merck & Co, Inc, RochePharmaceuticals, and Schering-Plough Corporation; and is on thespeakers bureaus of GlaxoSmithKline, Merck & Co, Inc, RochePharmaceuticals, and Schering-Plough Corporation. MauriceCerulli, MD, has received grant/research support fromAstraZeneca, Schering, TAP Pharmaceuticals Inc, and Wyeth-AyerstPharmaceuticals; is a consultant for, and is on the speakersbureaus of, AstraZeneca, Novartis Pharmaceuticals Corporation,Schering, TAP Pharmaceuticals Inc, and Wyeth-AyerstPharmaceuticals; and is a stock shareholder in Eli Lilly andCompany. Balu Chandra, MD, has not specified any significantrelationships with industry. Kapil Chopra, MD, is on the speakersbureau of Schering-Plough. Alroy Chow, MD, is on the speakersbureaus of AstraZeneca and Schering-Plough; and is a stockshareholder in Schering-Plough. Lynn Cochran, MD, has notspecified any significant relationships with industry. StanleyMartin Cohen, MD, is on the speakers bureaus of AstraZeneca,Roche Pharmaceuticals, Schering, and TAP Pharmaceuticals Inc.Massimo Colombo, MD, has not specified any significantrelationships with industry. Thomas J. Colturi, MD, is on thespeakers bureau of Schering-Plough. Jeffrey Cooley, MD, has notspecified any significant relationships with industry. ClaytonCollins Coon, MD, has not specified any significant relationshipswith industry. Michael Cox, MD, has received grant/researchsupport from Schering. Dale Coy, MD, has not specified anysignificant relationships with industry. Raquel Croitoru, MD, hasnot provided disclosure. Douglas Dalke, MD, has not specified anysignificant relationships with industry. Samuel Daniel, MD, hasnot provided disclosure. Mitchell Davis, DO, is on the speakersbureau of Schering Oncology/Biotech. Robert Davis, MD, has notspecified any significant relationships with industry. RashadDeBaghi, MD, has not specified any significant relationships withindustry. Lino DeGuzman, MD, is on the speakers bureaus ofSchering-Plough and Wyeth-Ayerst Pharmaceuticals. Michael De Micco, MD, has not specified any significant relationships withindustry. Joseph DePasquale, MD, has received grant/researchsupport from, and is on the speakers bureau of, Schering-Plough.David Doman, MD, is on the speakers bureaus of JanssenPharmaceutica Products, LP, Prometheus Laboratories, andSchering. Richard Eglow, MD, has received grant/research supportfrom Ortho Biotech Products, LP; and is on the speakers bureau ofSchering-Plough. Stephen P. Esposito, MD, has receivedgrant/research support from Bristol-Myers Squibb Company, GileadSciences, Inc, Roche Pharmaceuticals, Schering-Plough, and SolvayPharmaceuticals, Inc; and is on the speakers bureaus of Hoffmann-La Roche Inc and Schering-Plough. W. Hunter Eubanks, MD, hasnot specified any significant relationships with industry. RobertFadden, MD, has not provided disclosure. Franco Felizarta, MD,has received grant/research support from Abbott Laboratories,Agouron Pharmaceuticals, Inc, GlaxoSmithKline, Merck & Co, Inc,Roche Pharmaceuticals, and Schering; is a consultant for AbbottLaboratories, Boehringer Ingelheim Pharmaceuticals, Inc,GlaxoSmithKline, and Merck & Co, Inc; and is on the speakersbureaus of GlaxoSmithKline, Merck & Co, Inc; and RochePharmaceuticals. Robert G. Finkel, MD, has not provideddisclosure. Alan M. Fixelle, MD, has received grant/researchsupport from Schering; and is on the speakers bureaus ofAstraZeneca, Schering, and TAP Pharmaceuticals Inc. Steven L.Flamm, MD, has received grant/research support from, and is onthe speakers bureaus of, Roche Pharmaceuticals and Schering-Plough. Ira L. Flax, MD, has received grant/research support fromSchering. Jose Franco, MD, has received grant/research supportfrom, and is on the speakers bureau of, Schering. Bradley Freilich,MD, has received grant/research support from, is a consultant for,and is on the speakers bureau of, Schering-Plough. Joseph S.Galati, MD, has received grant/research support from RochePharmaceuticals and Schering Oncology/Biotech. Daniel R.Ganger, MD, is on the speakers bureau of Schering-Plough.Gabriel Garcia, MD, has received grant/research support from, and is on the speakers bureaus of, Roche Pharmaceuticals andSchering; and is a consultant for Aventis Pharmaceuticals andBaxter Vaccines. Ruel Garcia, MD, has not provided disclosure.Andrei Gasic, MD, is on the speakers bureaus of Wyeth-AyerstPharmaceuticals and Schering, and is a stock shareholder inSchering. Michael Georgetson, MD, has received grant/researchsupport from AstraZeneca, Glaxo Wellcome Inc, RochePharmaceuticals, and Schering; is a consultant for AstraZeneca;and is on the speakers bureaus of AstraZeneca, JanssenPharmaceutica Products, LP, and TAP Pharmaceuticals Inc. RobertGilbert, MD, has received grant/research support from Schering.Scott Gioe, MD, has not provided disclosure. Robert G. Gish, MD,has received grant/research support from, is a consultant for, andis on the speakers bureaus of GlaxoSmithKline, Gilead Sciences, Inc,Schering, and Triangle Pharmaceuticals, Inc. Jeffrey Goldstein,MD, is on the speakers bureaus of Roche Pharmaceuticals andSchering. Michael B. Goldstein, MD, has not specified anysignificant relationships with industry. Stuart Gordon, MD, has
received grant/research support from Akros Pharma Inc, Bristol-Myers Squibb Company, Gilead Sciences, Inc, GlaxoSmithKline,InterMune Inc, Isis Pharmaceuticals, Inc, Roche Pharmaceuticals,and Schering; is a consultant for Akros Pharma Inc; and is on thespeakers bureaus of Roche Pharmaceuticals and Schering. NormanD. Grace, MD, has received grant/research support fromInterMune Inc, Novartis Pharmaceuticals Corporation, RochePharmaceuticals, and Schering; is a consultant for Novo NordiskPharmaceuticals, Inc; and is on the speakers bureaus of InterMuneInc, Novartis Pharmaceuticals Corporation, and Schering. John B.Gross, Jr, MD, has received grant/research support fromInterMune Inc and Schering-Plough; and is on the speakersbureaus of InterMune Inc, Roche Pharmaceuticals, and Schering-Plough. M. Bassam Haffar, MD, is on the speakers bureaus ofAstraZeneca, GlaxoSmithKline, Novartis PharmaceuticalsCorporation, TAP Pharmaceuticals Inc, and Wyeth-AyerstPharmaceuticals. Norman W. Haines, Jr, MD, is on the speakersbureau of Schering. Steven-Huy Han, MD, has receivedgrant/research support from Bristol-Myers Squibb Company, GileadSciences, Inc, Glaxo Wellcome Inc, Idenix Pharmaceuticals, RochePharmaceuticals, and Schering-Plough. Tarek Hassanein, MD, hasreceived grant/research support from Roche Pharmaceuticals andSchering; and is on the speakers bureau of Ortho Biotech Products,LP. Ronald J. Hauptman, MD, has not specified any significantrelationships with industry. Jorge L. Herrera, MD, has receivedgrant/research support from Roche Pharmaceuticals, Schering-Plough, and SciClone Pharmaceuticals International, Ltd; and is onthe speakers bureaus of Roche Pharmaceuticals and Schering.Robert Herring, MD, has received grant/research support from, isa consultant for, and is on the speakers bureau of, Schering. Gary L. Hills, DO, is on the speakers bureaus of Schering andWyeth-Ayerst Pharmaceuticals. Brian K. Hudes, MD, has notspecified any significant relationships with industry. Joanne C.Imperial, MD, has received grant/research support from, and is onthe speakers bureaus of, Gilead Sciences, Inc, Glaxo Wellcome Inc,Ortho Biotech Products, LP, Roche Pharmaceuticals, and Schering.Miled Jabor, MD, has not specified any significant relationshipswith industry. Ira M. Jacobson, MD, has received grant/researchsupport from Gilead Sciences, Inc, Glaxo Wellcome Inc, InterMuneInc, Isis Pharmaceuticals Inc, Ribozyme Pharmaceuticals, Inc, andSchering; is a consultant for Akros Pharma Inc and Schering; and ison the speakers bureaus of Roche Pharmaceuticals and Schering.Joseph Jackson, MD, has not provided disclosure. Hyder Jamal,MD, is on the speakers bureau of TAP Pharmaceuticals Inc. M. Mazen Jamal, MD, has received grant/research support fromFeRx Inc, and is on the speakers bureaus of AstraZeneca, JanssenPharmaceutica Products, LP, and Schering-Plough. Robert Jao,MD, has received grant/research support from Schering; is aconsultant for AstraZeneca and Schering; is on the speakersbureau of AstraZeneca; and is a stock shareholder in AmericanHome Products Corporation and Pfizer Inc. John Jolley, MD, hasreceived grant/research support from Roche Pharmaceuticals andSchering; and is a consultant for Roche Pharmaceuticals. IsaacKalvaria, MD, is a consultant for, and on the speakers bureau of,Schering. Steven Katzman, MD, is a stock shareholder inSchering-Plough. John Kauffman, MD, has not specified anysignificant relationships with industry. Barry P. Kaufman, MD,FACG, CNSP, has received grant/research support from RochePharmaceuticals and Schering; and is a consultant for Wyeth-Ayerst Pharmaceuticals. Raymond Kenny, MD, has receivedgrant/research support from Roche Pharmaceuticals and Schering-Plough; is on the speakers bureau of Schering-Plough; and is astock shareholder in Enzon Inc. Kelly Kensing, MD, has notspecified any significant relationships with industry. Kieran Key,MD, has not specified any significant relationships with industry.Mandana Khalili, MD, has received grant/research support fromRoche Pharmaceuticals and Schering-Plough. Alan E. Kilby, MD,has received grant/research support from Schering. John P.Kirchner, MD, PhD, has received grant/research support from, and is on the speakers bureau of, Schering-Plough. Robert B.Kirkpatrick, MD, is on the speakers bureaus of RochePharmaceuticals and Schering. Martin S. Kleinman, MD, is on the speakers bureau of Schering-Plough. Frank Klion, MD, hasreceived grant/research support from Roche Pharmaceuticals andSchering-Plough; and is on the speakers bureau of Schering-Plough. Marcelo Kugelmas, MD, has received grant/researchsupport from InterMune Inc and Schering-Plough; and is on thespeakers bureau of Schering. Shashi Kumar, MD, is on thespeakers bureau of Schering-Plough. Paul Kwo, MD, has receivedgrant/research support from InterMune Inc and Schering-Plough.Gerry Lake-Bakaar, MD, has received grant/research supportfrom, and is on the speakers bureaus of, Roche Pharmaceuticalsand Schering. Anne Larson, MD, has received grant/researchsupport from InterMune Inc, Roche Pharmaceuticals, and Schering;and is on the speakers bureaus of Astra Merck Inc, InterMune Inc,Roche Pharmaceuticals, and Schering. Eric Lawitz, MD, hasreceived grant/research support from InterMune Inc, Schering-Plough, TAP Pharmaceuticals Inc, and Wyeth-AyerstPharmaceuticals. Truong-Sinh Leduc, MD, is on the speakersbureau of Schering. Carroll B. Leevy, MD, has received
This activity may include a discussion of therapies that are unapproved for use or investigational, ongoing research, or preliminary data.The opinions expressed during this activity are those of the faculty and do not necessarily reflect those of the sponsor or the commercial supporter.
5
TREATMENT REPORTER Emerging Advances: Preliminary Findings From Ongoing Studies of Peginterferon/Ribavirin
grant/research support from InterMune Inc, Roche Laboratories,and Schering Corporation; is a consultant for Gilead Sciences Inc,InterMune Inc, Roche Laboratories, and Schering Corporation; andis on the speakers bureaus of Axcan Scandipharm Inc, InterMuneInc, Janssen Pharmaceutica Products, LP, Ortho Biotech Products,LP, Roche Laboratories, and Schering Corporation. Michael J.Levinson, MD, has not specified any significant relationships withindustry. Robert Lewis, MD, is on the speakers bureau of ScheringHepatitis Innovations. Michael Lindner, MD, has receivedgrant/research support from, is a consultant for, and is on thespeakers bureau of, Schering. Lawrence Lumeng, MD, has notspecified any significant relationships with industry. Kip Lyche,MD, has received grant/research support from, and is on thespeakers bureaus of, Roche Pharmaceuticals and Schering. MichaelF. Lyons, MD, has received grant/research support from InterMuneInc and Schering; and is on the speakers bureaus of AstraZeneca,InterMune Inc, Roche Pharmaceuticals, Schering, and TAPPharmaceuticals Inc. Willis C. Maddrey, MD, is a consultant for Eli Lilly and Company, Isis Pharmaceuticals Inc, RibozymePharmaceuticals Inc, and Schering. Oscar Maldonado, MD, hasnot provided disclosure. Suresh Malholtra, MD, has not specifiedany significant relationships with industry. Kent Martin, MD, is onthe speakers bureau of Schering. Daniel Matloff, MD, has notspecified any significant relationships with industry. JonathanMcCone, MD, has received grant/research support from Schering;and is on the speakers bureau of TAP Pharmaceuticals Inc. John D.McCracken, MD, is a consultant for, and a stock shareholder in,Encore Pharmaceuticals, Inc; and is on the speakers bureaus ofGlaxoSmithKline and Schering. Robert McFadden, MD, hasreceived grant/research support from, and is on the speakersbureau of, Schering. Barbara H. McGovern, MD, is a consultantfor Roche Pharmaceuticals and is on the speakers bureau ofSchering-Plough. John G. McHutchison, MD, has receivedgrant/research support from BioMedicines, Inc, Bristol-MyersSquibb Company, Gilead Sciences, Inc, Isis Pharmaceuticals Inc,Ribozyme Pharmaceuticals, Inc, Roche Pharmaceuticals, andSchering-Plough; is a consultant for Isis Pharmaceuticals Inc andSchering-Plough; and is on the speakers bureaus of RochePharmaceuticals and Schering-Plough. Jeffrey Medoff, MD, hasreceived grant/research support from Roche Pharmaceuticals andSchering. Robert H. Meichner, MD, is a consultant for Scheringand is on the speakers bureaus of AstraZeneca LP, JanssenPharmaceutica Products, LP, Schering, TAP Pharmaceuticals Inc, andWyeth-Ayerst Pharmaceuticals. Daniel Meline, MD, has receivedgrant/research support from Roche Pharmaceuticals and Schering;and is on the speakers bureau of, and is a stock shareholder in,Schering. Barry Migicovsky, MD, has not specified any significantrelationships with industry. Peter Molloy, MD, has receivedgrant/research support from Roche Pharmaceuticals, Schering, andWyeth-Ayerst Pharmaceuticals; and is on the speakers bureau ofJanssen Pharmaceutica Products, LP. Samuel Moskowitz, MD, hasreceived grant/research support from Roche Pharmaceuticals andSchering; is on the speakers bureau of Schering; and is a stockshareholder in Enzon Inc. Santiago J. Munoz, MD, has receivedgrant/research support from, and is on the speakers bureaus of,InterMune Inc, Roche Pharmaceuticals, and Schering. Mark E.Murphy, MD, has received grant/research support from Schering-Plough; is on the speakers bureaus of AstraZeneca,GlaxoSmithKline, Roche Pharmaceuticals, and Schering-Plough;and is a stock shareholder in Pfizer Inc. Milton G. Mutchnick,MD, has received grant/research support from Schering; and is onthe speakers bureaus of GlaxoSmithKline and Schering. AbdulNadir, MD, has not specified any significant relationships withindustry. Farid Naffah, MD, is on the speakers bureaus of AstraMerck Inc, Janssen Pharmaceutica Products, LP, and TAPPharmaceuticals Inc. Guy Neff, MD, has not provided disclosure.David R. Nelson, MD, has received grant/research support fromInterMune Inc, Roche Pharmaceuticals, Schering, and SciClonePharmaceuticals International, Ltd; and is a consultant for, and onthe speakers bureau of, Schering. Frank Nelson, MD, is on thespeakers bureaus of Schering-Plough and TAP Pharmaceuticals Inc.Tuan T. Nguyen, MD, has received grant/research support fromBristol-Myers Squibb Company, Schering-Plough, and TrianglePharmaceuticals Inc; and is on the speakers bureaus of Schering-Plough and TAP Pharmaceuticals Inc. Rod Nisi, MD, has notprovided disclosure. Frederick Nunes, MD, has not specified anysignificant relationships with industry. Anders Nyberg, MD, hasnot specified any significant relationships with industry. LisaNyberg, MD, has received grant/research support from RochePharmaceuticals and Schering-Plough; and is on the speakersbureau of Schering-Plough. Christopher O’Brien, MD, has receivedgrant/research support from Achillion Pharmaceuticals, Inc, IdenixPharmaceuticals, Roche Pharmaceuticals, and Virapharm; is aconsultant for Ribapharm; and is on the speakers bureaus of RochePharmaceuticals and Schering. Mary Pat Pauly, MD, has receivedgrant/research support from Roche Pharmaceuticals and Schering-Plough. John Payne, MD, has not provided disclosure. RogerPerez, MD, is on the speakers bureau of Schering-Plough. NevilleR. Pimstone, MD, has received grant/research support fromAmgen Inc, Roche Pharmaceuticals, and Schering; and is on thespeakers bureaus of Roche Pharmaceuticals and Schering. JamesPiper, MD, is on the speakers bureau of Schering. Arthur L. Poch,MD, has not specified any significant relationships with industry.
Paul Pockros, MD, has received grant/research support fromSchering-Plough. Gary Poleynard, MD, has received grant/researchsupport from Roche Pharmaceuticals and Schering; and is on thespeakers bureau of Schering. Fred Poordad, MD, has receivedgrant/research support from Glaxo Wellcome, RochePharmaceuticals, and Schering-Plough; and is on the speakersbureaus of Ortho Biotech Products, LP, Roche Pharmaceuticals, andSchering-Plough. Anthony B. Post, MD, has not specified anysignificant relationships with industry. David C. Pound, MD, hasnot specified any significant relationships with industry. BangaruJayapraka Prakash, MD, has not provided disclosure. William J.Provance, DO, has received grant/research support from, and is onthe speakers bureau of, Schering-Plough. Thierry M. Poynard, MD,PhD, has received grant/research support from BoehringerIngelheim Pharmaceuticals, Inc, Bristol-Myers Squibb Company,Gilead Sciences, Inc, GlaxoSmithKline, Maxim Pharmaceuticals,Novirio Pharmaceuticals, Roche Pharmaceuticals, and Schering.Rudra Rai, MD, has received grant/research support fromGlaxoSmithKline, Roche Pharmaceuticals, Schering, and SmithKlineBeecham Pharmaceuticals; and is on the speakers bureaus ofRoche Pharmaceuticals and Schering. Charles L. Raison, MD, is onthe speakers bureaus of Roche Pharmaceuticals and Wyeth-AyerstPharmaceuticals. Natarajan Ravendhran, MD, has receivedgrant/research support from GlaxoSmithKline, RochePharmaceuticals, and Schering-Plough; is a consultant for, andstock shareholder in, Schering-Plough; and is on the speakersbureaus of Ortho Biotech Products, LP and Schering-Plough. Stuart C. Ray, MD, has received unrestricted grants for speakingfrom Agouron Pharmaceuticals, Inc, Roche Pharmaceuticals, andSchering-Plough, and his division has received unrestricted grantsupport from Ortho Biotech Products, LP, Roche Pharmaceuticals,and Schering-Plough. Gurunath Reddy, MD, has not provideddisclosure. Thomas Reed, MD, is on the speakers bureau of, and isa stock shareholder in, Schering-Plough. Frederic Regenstein, MD,has received grants/research support from Schering-Plough; is aconsultant for Roche Pharmaceuticals; and is on the speakersbureaus of InterMune Inc and Roche Pharmaceuticals. Terence N.Reisman, MD, has not specified any significant relationships with industry. Adrian Reuben, MBBS, FRCP, has receivedgrants/research support from Glaxo Wellcome Inc and Schering;and is on the speakers bureaus of Axcan Scandipharm Inc andSchering. Donato Ricci, MD, is on the speakers bureaus ofSchering and Wyeth-Ayerst Pharmaceuticals. Ronald Rinker, MD,has received grant/research support from Schering. Earl G.Robbins II, MD, has not specified any significant relationshipswith industry. Donald C. Rockey, MD, has not specified anysignificant relationships with industry. S. Lawrence Rothman, MD,has received grant/research support from Schering-Plough; and ison the speakers bureaus of InterMune Inc and Schering-Plough.Raymond A. Rubin, MD, has received grants/research supportfrom Bristol-Myers Squibb Company, Gilead Sciences, Inc, RochePharmaceuticals, and Schering; and is on the speakers bureaus ofRoche Pharmaceuticals and Schering. Sammy Saab, MD, hasreceived grant/research support from Schering. Kia Saeian, MD,has received grant/research support from Schering Corporation.Geronimo Sahagun, MD, is a stock shareholder in Schering-Plough. Angelo Sangiovanni, MD, has not specified anysignificant relationships with industry. Eugene R. Schiff, MD,has received grant/research support from, is a consultant for, andis on the speakers bureaus of Abbott Laboratories, BayerCorporation, Bristol-Myers Squibb Company, Gilead Sciences, Inc,GlaxoSmithKline, Ortho Biotech Products, LP, Ortho Diagnostics,Ribapharma, Roche Diagnostics, Schering, and SciClonePharmaceuticals; is a consultant for Achillion Pharmaceuticals, Inc,Fujisawa Healthcare Inc, Novartis Pharmaceutical Corporation, andPfizer Inc; and is on the speakers bureaus of AstraZeneca, LP, AxcanPharma, Inc, and InterMune Inc. Warren Schmidt, MD, is a stockshareholder in Schering-Plough. Fayez Seif, MD, has receivedgrant/research support from Schering; and is on the speakersbureaus of AstraZeneca, GlaxoSmithKline, Janssen PharmaceuticaProducts, LP, Schering, TAP Pharmaceuticals Inc, and Wyeth-AyerstPharmaceuticals. William Semon, MD, has receivedgrants/research support from, and is on the speakers bureau of,Schering. Thomas Sepe, MD, has received grants/research supportfrom Roche Pharmaceuticals and Schering; is a consultant forAstraZeneca; and is on the speakers bureaus of AstraZeneca andSchering. Ashok Shah, MD, is on the speakers bureaus ofCentocor, Inc, Merck & Co, Inc, Novartis PharmaceuticalsCorporation, and Schering. A. Obaid Shakil, MD, has receivedgrant/research support from Akros Pharma Inc, InterMune Inc, andSchering-Plough; and is on the speakers bureaus of RochePharmaceuticals and Schering-Plough. Thomas Shaw-Stiffel, MD,has received grant/research support from Roche Pharmaceuticalsand Schering-Plough; and is on the speakers bureaus of RochePharmaceuticals, Schering-Plough, and Wyeth-AyerstPharmaceuticals. Muhammad Sheikh, MD, has receivedgrant/research support from Achillion Pharmaceuticals, Inc, andInterMune Inc; and is on the speakers bureaus of GlaxoSmithKlineand InterMune Inc. Alan Sheinbaum, MD, has receivedgrants/research support from, and is on the speakers bureau of,Schering-Plough; is a consultant for Axcan Scandipharm Inc andSchering-Plough; and is a stock shareholder in Merck & Co, Inc,and Schering-Plough. Richard Sheinbaum, MD, has received
grant/research support from Schering-Plough; is a consultant forAstraZeneca, GlaxoSmithKline, Novartis PharmaceuticalsCorporation, Schering-Plough, and TAP Pharmaceuticals Inc; and ison the speakers bureaus of AstraZeneca, Axcan Scandipharm Inc,GlaxoSmithKline, Novartis Pharmaceuticals Corporation, Schering-Plough, and TAP Pharmaceuticals Inc. Kenneth Sherman, MD,PhD, has received grant/research support from, and is on thespeakers bureau of, Schering. Ann Silverman, MD, has receivedgrant/research support from Akros Pharma Inc, Gilead Sciences,Inc, InterMune Inc, Isis Pharmaceuticals Inc, NovartisPharmaceuticals Corporation, Roche Pharmaceuticals, Schering,SciClone Pharmaceuticals International, Ltd, and Wyeth-AyerstPharmaceuticals; and is on the speakers bureau of AstraZeneca.Bruce Silverman, MD, has received grant/research support formSchering. James A. Singer, MD, has not specified any significantrelationships with industry. Maria Sjogren, MD, has not provideddisclosure. Robert Sjogren, MD, has received grant/researchsupport from InterMune Inc, Roche Pharmaceuticals, and Schering;and is on the speakers bureaus of AstraZeneca, InterMune Inc, andWyeth-Ayerst Pharmaceuticals. Dirk P. Slaker, MD, has notprovided disclosure. Coleman Smith, MD, has receivedgrant/research support from GlaxoSmithKline, Ortho BiotechProducts, LP, and Schering; and is on the speakers bureaus ofRoche Pharmaceuticals and Schering. Richard Sperling, MD, is astock shareholder in Schering-Plough. Gary Spiegelman, MD, ison the speakers bureaus of Schering and TAP Pharmaceuticals Inc.Julie Spivack, MD, is a consultant for Roche Pharmaceuticals; andis on the speakers bureau of GlaxoSmithKline. Timothy Spurling,MD, has received grant/research support from GlaxoSmithKline;and is a consultant for, and on the speakers bureaus of, Astra,GlaxoSmithKline, Johnson & Johnson • MERCK ConsumerPharmaceuticals Co, and TAP Pharmaceuticals Inc. RichardSterling, MD, has received grant/research support from OrthoBiotech Products, LP, PharmaResearch Corporation, and RochePharmaceuticals; is a consultant for Pharmacy Times; and is on thespeakers bureau of Schering-Plough. Robert Strauss, MD, has notspecified any significant relationships with industry. Mark S.Sulkowski, MD, has received grant/research support from, and ison the speakers bureaus of, Ortho Biotech Products, LP, RochePharmaceuticals, and Schering. Uma Sundaram, MD, has receivedgrant/research support from Schering Oncology/Biotech. J. ThomasSwan, MD, has not specified any significant relationships withindustry. Diana Sylvestre, MD, has received grant/research supportfrom Roche Pharmaceuticals and Schering Oncology/Biotech.Mumtaz Tabaa, MD, has not provided disclosure. Andrew Talal,MD, has received grant/research support from Gilead Sciences, Inc,Roche Pharmaceuticals, and Schering; and is a consultant forOrtho Biotech Products, LP. Helen Te, MD, has receivedgrant/research support from Gilead Sciences, Inc, RochePharmaceuticals, and Schering-Plough. Hillel Tobias, MD, hasreceived grant/research support from Schering. Myron J. Tong,PhD, MD, has received grant/research support from RibozymePharmaceuticals, Inc; is a consultant for National GeneticsInstitute; and is on the speakers bureau of Schering. Huy NgocTrinh, MD, has not provided disclosure. Vance Van Drake, MD, ison the speakers bureau of Wyeth-Ayerst Pharmaceuticals and is astock shareholder in Elan Pharmaceuticals. Joseph L. Wang, MD,has received grant/research support from AstaZeneca and SolvayPharmaceuticals, Inc; and is on the speakers bureaus ofAstraZeneca, Janssen Pharmaceutica Products, LP, Schering-Plough,and TAP Pharmaceuticals Inc. Peter Wayne, MD, has receivedgrant/research support from Schering-Plough; and is on thespeakers bureaus of Roche Pharmaceuticals and Schering-Plough.Larry Weprin, MD, has not provided disclosure. Scott L. Wiesen,MD, has not provided disclosure. Ian Williams, PhD, MS, has notspecified any significant relationships with industry. Ira R. Willner,MD, is on the speakers bureau of Schering. Robert Wohlman, MD,has not specified any significant relationships with industry. DavidC. Wolf, MD, has received grant/research support from Schering.Harlan I. Wright, MD, has not provided disclosure. Teresa L.Wright, MD, has received grant/research support from GileadSciences, Inc, GlaxoSmithKline, Hoffmann-La Roche Inc, andSchering-Plough; is a consultant for GlaxoSmithKline; is on thespeakers bureaus of Roche Pharmaceuticals and Schering-Plough;and is on the advisory boards of Eli Lilly and Company, GileadSciences, Inc, GlaxoSmithKline, Hoffmann-La Roche Inc, InterMuneInc, and Ortho Biotech Products, LP. Rockford Yapp, MD, hasreceived grant/research support from Schering and Wyeth-AyerstPharmaceuticals; is a consultant for Boston Scientific, JanssenPharmaceutica Products, LP, Roche Pharmaceuticals, Schering, andTAP Pharmaceuticals Inc; and is on the speakers bureaus of BostonScientific, Janssen Pharmaceutica Products, LP, RochePharmaceuticals, and Schering. Yuen S. Yee, MD, is a consultantfor AstraZeneca, GlaxoSmithKline, InterMune Inc, and RochePharmaceuticals; is on the speakers bureaus of AstraZeneca,Janssen Pharmaceutica Products, LP, and Schering-Plough; and is astock shareholder in Bristol-Myers Squibb Company, Pfizer Inc, andSchering-Plough. Geoffrey Zucker, MD, has receivedgrant/research support from Schering-Plough Pharmaceuticals.
6
R E P O R T E RSM : G A S T R O E N T E R O L O G Y
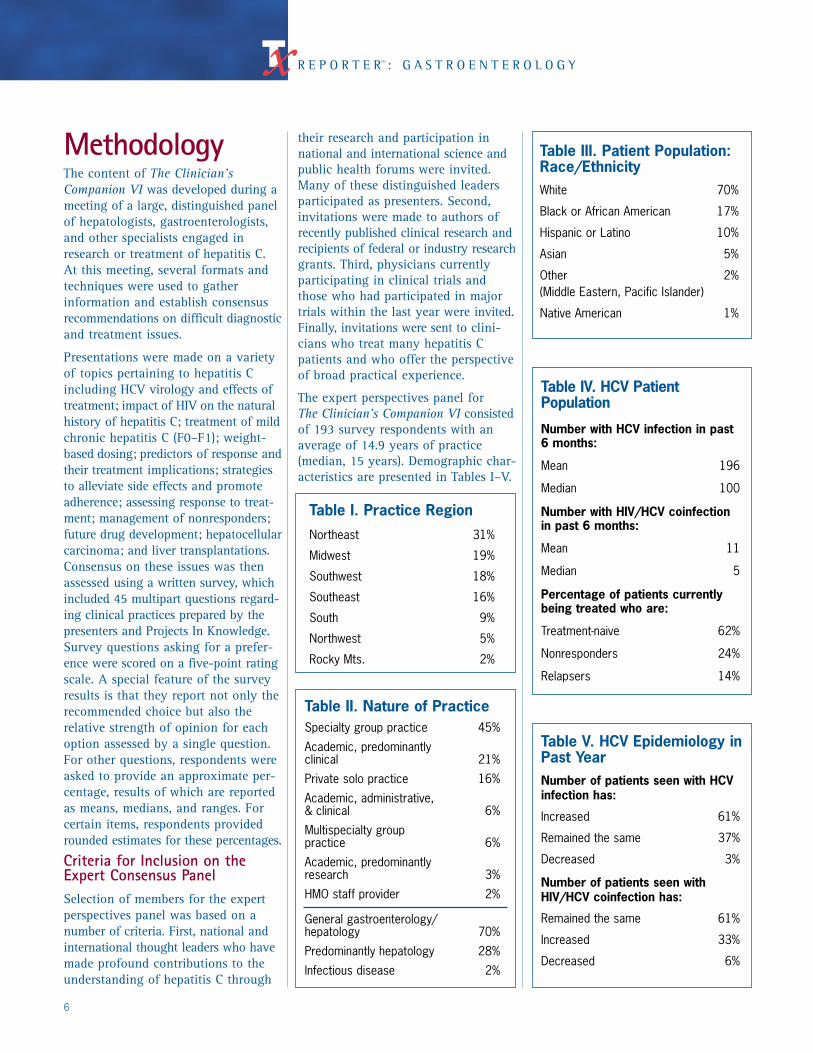
MethodologyThe content of The Clinician’sCompanion VI was developed during ameeting of a large, distinguished panelof hepatologists, gastroenterologists,and other specialists engaged inresearch or treatment of hepatitis C.At this meeting, several formats andtechniques were used to gather information and establish consensus recommendations on difficult diagnosticand treatment issues.
Presentations were made on a varietyof topics pertaining to hepatitis Cincluding HCV virology and effects oftreatment; impact of HIV on the naturalhistory of hepatitis C; treatment of mildchronic hepatitis C (F0–F1); weight-based dosing; predictors of response andtheir treatment implications; strategiesto alleviate side effects and promoteadherence; assessing response to treat-ment; management of nonresponders;future drug development; hepatocellularcarcinoma; and liver transplantations.Consensus on these issues was thenassessed using a written survey, whichincluded 45 multipart questions regard-ing clinical practices prepared by thepresenters and Projects In Knowledge.Survey questions asking for a prefer-ence were scored on a five-point ratingscale. A special feature of the surveyresults is that they report not only therecommended choice but also the relative strength of opinion for eachoption assessed by a single question.For other questions, respondents wereasked to provide an approximate per-centage, results of which are reportedas means, medians, and ranges. Forcertain items, respondents providedrounded estimates for these percentages.
Criteria for Inclusion on theExpert Consensus PanelSelection of members for the expertperspectives panel was based on anumber of criteria. First, national andinternational thought leaders who havemade profound contributions to theunderstanding of hepatitis C through
their research and participation innational and international science andpublic health forums were invited.Many of these distinguished leadersparticipated as presenters. Second,invitations were made to authors ofrecently published clinical research andrecipients of federal or industry researchgrants. Third, physicians currentlyparticipating in clinical trials andthose who had participated in majortrials within the last year were invited.Finally, invitations were sent to clini-cians who treat many hepatitis Cpatients and who offer the perspectiveof broad practical experience.
The expert perspectives panel for The Clinician’s Companion VI consistedof 193 survey respondents with anaverage of 14.9 years of practice(median, 15 years). Demographic char-acteristics are presented in Tables I–V.
Table I. Practice Region
Northeast 31%
Midwest 19%
Southwest 18%
Southeast 16%
South 9%
Northwest 5%
Rocky Mts. 2%
Table II. Nature of PracticeSpecialty group practice 45%
Academic, predominantly clinical 21%
Private solo practice 16%
Academic, administrative, & clinical 6%
Multispecialty group practice 6%
Academic, predominantly research 3%
HMO staff provider 2%
General gastroenterology/hepatology 70%
Predominantly hepatology 28%
Infectious disease 2%
Table III. Patient Population:Race/EthnicityWhite 70%
Black or African American 17%
Hispanic or Latino 10%
Asian 5%
Other 2%(Middle Eastern, Pacific Islander)
Native American 1%
Table IV. HCV PatientPopulation
Number with HCV infection in past 6 months:
Mean 196
Median 100
Number with HIV/HCV coinfection in past 6 months:
Mean 11
Median 5
Percentage of patients currently being treated who are:
Treatment-naive 62%
Nonresponders 24%
Relapsers 14%
Table V. HCV Epidemiology inPast YearNumber of patients seen with HCVinfection has:
Increased 61%
Remained the same 37%
Decreased 3%
Number of patients seen withHIV/HCV coinfection has:
Remained the same 61%
Increased 33%
Decreased 6%
7
TREATMENT REPORTER Emerging Advances: Preliminary Findings From Ongoing Studies of Peginterferon/Ribavirin
Ira M. Jacobson, MDIn the registration trial ofpeginterferon/ribavirin for treatingchronic HCV infection, Manns et al1 reported a strikingly linearrelationship between the dose ofribavirin in mg/kg and the rate of SVR on retrospective logisticregression analysis, suggesting thatweight-based dosing of ribavirin is likely to enhance its efficacy. As a result, weight-based peginterferonalfa-2b and ribavirin combinationtherapy was approved in Europe in March 2001. However, in theabsence of prospective data onweight-based ribavirin dosing, theFDA approved only a fixed ribavirindose of 800 mg/d in combinationwith peginterferon alfa-2b 1.5 µg/kgQW in August 2001. The prospectiveWIN-R Trial was subsequentlyinitiated by investigators to addressthis issue in the United States.
Design of the WIN-R TrialThe WIN-R Trial is being conductedin 23 regions of the United States,each containing an average of 10subsites. Participants with chronicHCV infection and elevated alanineaminotransferase levels are assignedby central randomization andstratified by genotype and degree offibrosis, to either:
• Standard dosing (STD):peginterferon alfa-2b 1.5 µg/kg QW+ ribavirin 800 mg/d, or
• Weight-based dosing (WBD):peginterferon alfa-2b 1.5 µg/kg QW
+ ribavirin dosed according tobody weight: 800 mg/d for <65 kg,1000 mg/d for 65 to 85 kg, 1200 mg/d for 86 to 105 kg, and1400 mg/d (a dose not previouslystudied) for >105 kg.
Patients infected with genotype 2/3are also randomized to either 24 or 48 weeks of therapy; patientswith genotype 1 are all treated for48 weeks. WIN-R enrollment ofpatients with HCV genotype 1 endedin January, while enrollment ofpatients with genotype 2/3 isongoing. Thus far, approximately4900 patients have been enrolled,including 400 African Americans.
The principal investigator andSteering Committee are currentlyblinded to data on antiviral efficacy;thus, no data regarding virologicresponse are available yet. However,a large body of demographic,clinical, and hematologic data hasbegun to accumulate.
Demographic DataThe age distribution of the WIN-Rpopulation is typical of the HCV-infected population nationwide, with 63.4% being 45 to 64 years ofage and 29% aged 35 to 44 years.Eighty-two percent are Caucasian,10% African American, 5% Latino,2% Asian, and 1% other. The majority(68%) are infected with genotype 1.As in other investigations, theprevalence of genotype 1 infection
is disproportionately higher amongAfrican Americans at 91%, versus72% among Latinos, 66% amongCaucasians, and 55% among Asians.The prevalence of genotype 3 islower in older age groups thanamong younger patients, furthersupporting previous hypotheses thatthis genotype is the most recentlyintroduced into the United States.Seventy percent of the populationhas stage F0 to F2 fibrosis, and therest have more advanced disease.(Jacobson IM, et al, unpublisheddata, 2002.)
Analysis of the demographic datafrom the WIN-R populationindicates that genotype 1 isassociated with about a twofoldhigher viral level than genotype 2/3.However, neither genotype nor virallevel is correlated with the degree ofprogression of fibrosis. AfricanAmericans, who have a higherprevalence of genotype 1, are notmore likely than Caucasians to havesevere fibrosis. Persons infected withgenotype 3 are more likely to havesteatosis. In the overall studypopulation, steatosis is associatedwith a higher prevalence of severefibrosis. (Jacobson IM, et al,unpublished data, 2002.)
Hematologic Safety DataIn the study by Manns et al,1
patients receiving the higher dose of peginterferon (1.5 µg/kg QW)were given ribavirin 800 mg/dbecause of concerns that excess
The WIN-R Trial: Early Observations on Weight-BasedDosing of Peginterferon alfa-2b/Ribavirin
hematologic toxicity might occur ifthe then-standard dose of ribavirin(1000–1200 mg/d) were used. Thus, the WIN-R study is carefullyassessing hematologic toxicity,particularly among patientsreceiving higher doses of ribavirin.
The WIN-R trial allows the use oferythropoietin for hemoglobin <10 g/dL and granulocyte colony-stimulating factor for absoluteneutrophil count (ANC) <750/mm3.Use of these growth factors is not permitted to substitute for thedosage reductions mandated by the protocol, but concurrent dosereductions and use of growth factorsare permitted. According to thestudy protocol, a neutrophil countof <750/mm3 mandates a reductionto peginterferon alfa-2b 1.0 mg/kg,and a hemoglobin level <10 g/dLmandates a decrease of between 200and 400 mg in ribavirin dose.However, doses of peginterferon orribavirin can be increased to theiroriginal levels if the ANC exceeds1250/mm3 or the hemoglobinexceeds 11.5 g/dL after growthfactors have been started.
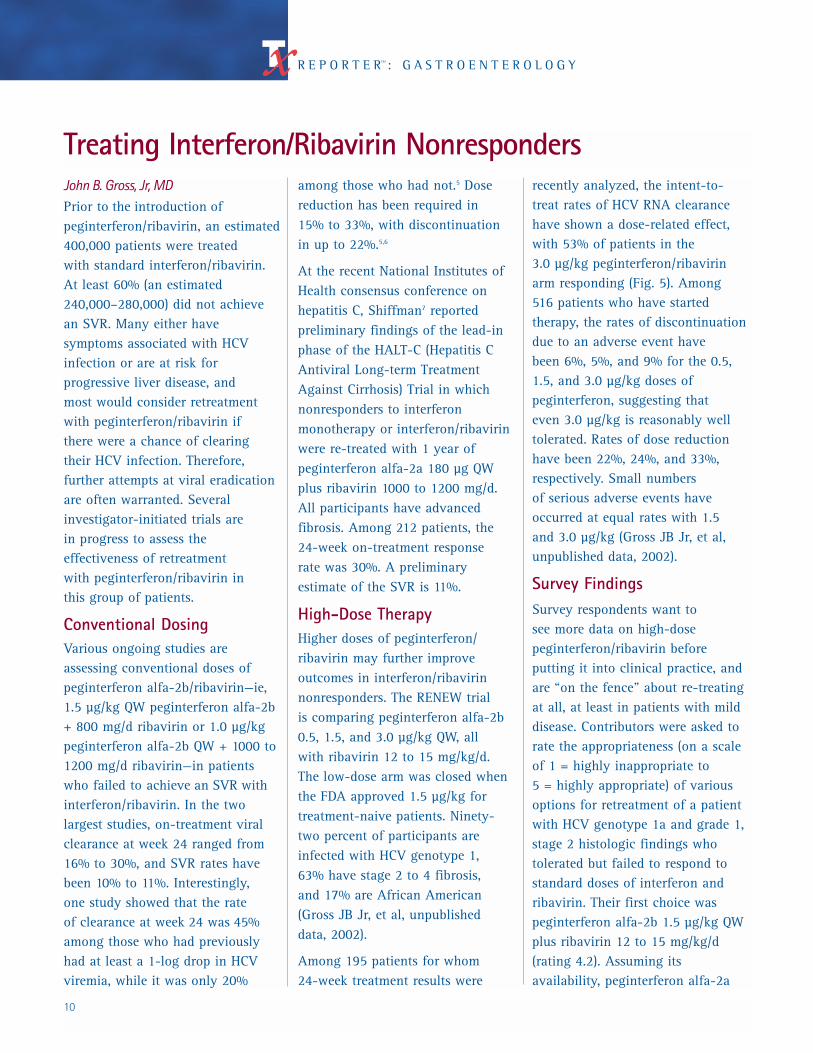
At all points evaluated thus far (upto 24 weeks), mean hemoglobin
level has beenslightly lower (byabout 0.5 g/dL) inpatients treatedwith WBD versuspatients treatedwith STD. At week 12, meanhemoglobin levelwas 11.9 g/dLversus 12.4 g/dL,respectively, andat week 24 was11.8 g/dL versus 12.3 g/dL,respectively. Within the WBD group,however, there are no significantdifferences in hemoglobin level by
ribavirin dose (Fig. 1). Particularlyof note, the degree of anemia is notany greater in patients who received
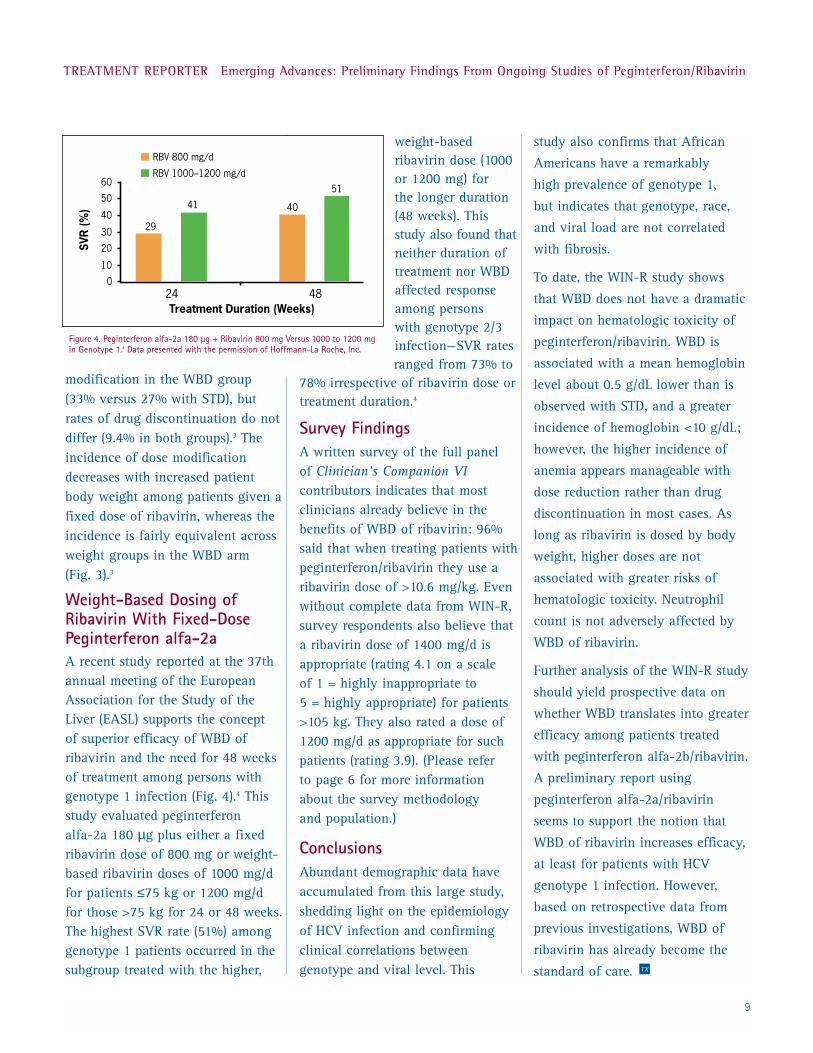
1400 mg/d thanamong patients whoare receiving lowerdoses of ribavirin.The incidenceof hemoglobin level <10 g/dL isapproximately 45% greater in the WBD group than in the STDgroup, although
the discrepancy lessens by week 24,presumably as a result of acombination of dose reduction, useof growth factors, and patient
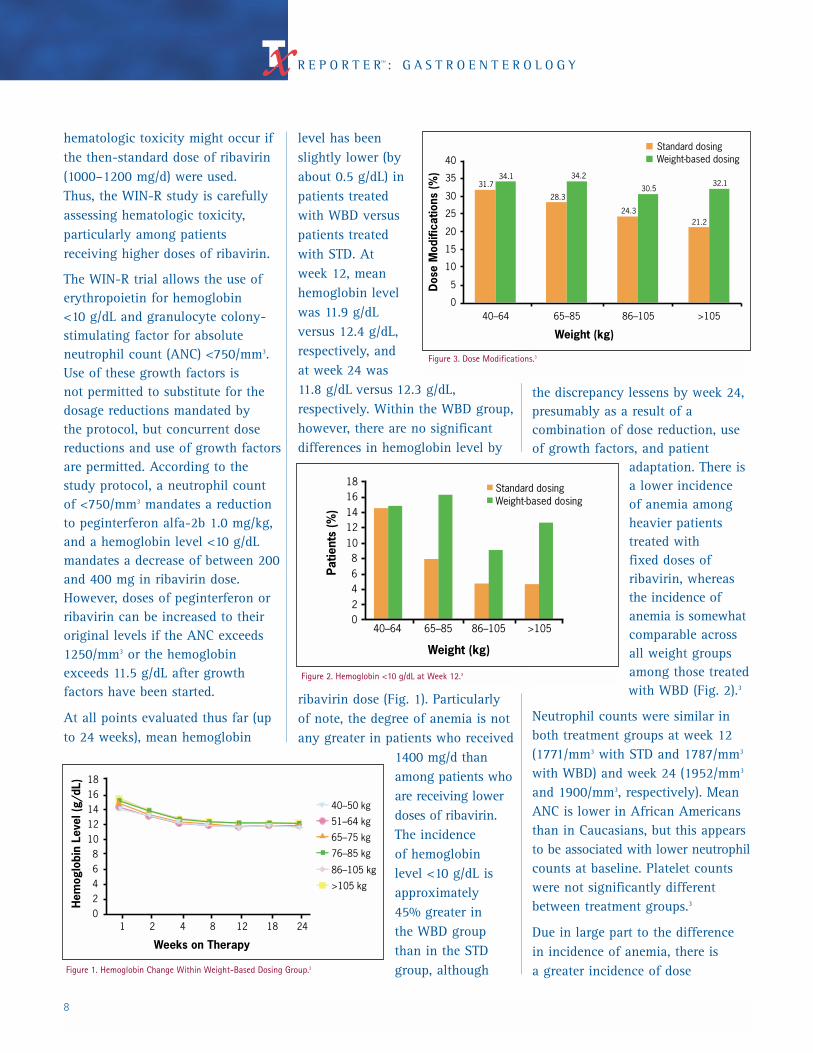
adaptation. There isa lower incidence of anemia amongheavier patientstreated with fixed doses ofribavirin, whereasthe incidence ofanemia is somewhatcomparable acrossall weight groupsamong those treatedwith WBD (Fig. 2).3
Neutrophil counts were similar in both treatment groups at week 12(1771/mm3 with STD and 1787/mm3
with WBD) and week 24 (1952/mm3
and 1900/mm3, respectively). MeanANC is lower in African Americansthan in Caucasians, but this appearsto be associated with lower neutrophilcounts at baseline. Platelet countswere not significantly differentbetween treatment groups.3
Due in large part to the difference in incidence of anemia, there is a greater incidence of dose
8
R E P O R T E RSM : G A S T R O E N T E R O L O G Y
Weeks on Therapy
02468
1012141618
1 2 4 8 12 18 24
40–50 kg
51–64 kg
65–75 kg
76–85 kg
86–105 kg
>105 kg
Hem
oglo
bin
Leve
l (g/
dL)
Figure 1. Hemoglobin Change Within Weight-Based Dosing Group.3
02468
1012141618
40–64 65–85 86–105 >105
Patie
nts
(%)
Standard dosingWeight-based dosing
Weight (kg)
Figure 2. Hemoglobin <10 g/dL at Week 12.3
0
5
10
15
20
25
30
35
40
40–64 65–85 86–105 >105
Standard dosingWeight-based dosing
31.734.1
28.3
34.2
24.3
30.5
21.2
32.1
Dos
e M
odifi
catio
ns (%
)
Weight (kg)
Figure 3. Dose Modifications.3
9
TREATMENT REPORTER Emerging Advances: Preliminary Findings From Ongoing Studies of Peginterferon/Ribavirin
modification in the WBD group(33% versus 27% with STD), butrates of drug discontinuation do notdiffer (9.4% in both groups).3 Theincidence of dose modificationdecreases with increased patientbody weight among patients given afixed dose of ribavirin, whereas theincidence is fairly equivalent acrossweight groups in the WBD arm (Fig. 3).3
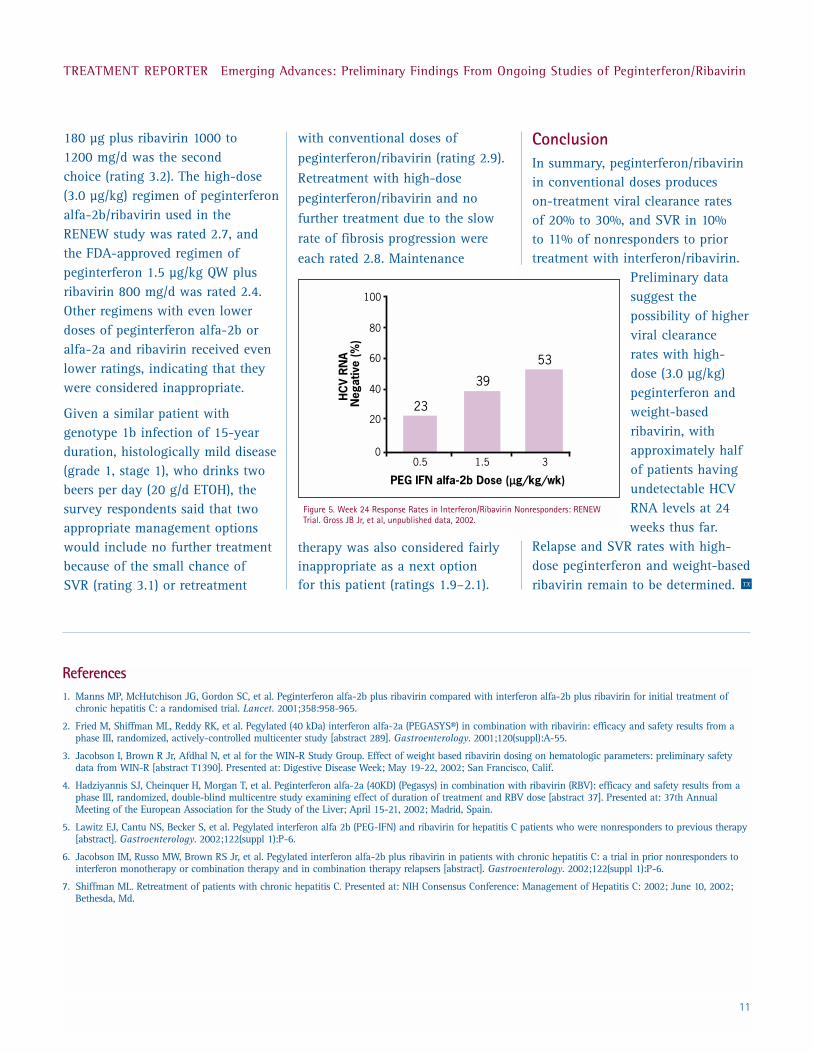
Weight-Based Dosing ofRibavirin With Fixed-DosePeginterferon alfa-2aA recent study reported at the 37thannual meeting of the EuropeanAssociation for the Study of theLiver (EASL) supports the concept of superior efficacy of WBD ofribavirin and the need for 48 weeksof treatment among persons withgenotype 1 infection (Fig. 4).4 Thisstudy evaluated peginterferon alfa-2a 180 µg plus either a fixedribavirin dose of 800 mg or weight-based ribavirin doses of 1000 mg/dfor patients ≤75 kg or 1200 mg/dfor those >75 kg for 24 or 48 weeks.The highest SVR rate (51%) amonggenotype 1 patients occurred in thesubgroup treated with the higher,
weight-basedribavirin dose (1000or 1200 mg) for the longer duration(48 weeks). Thisstudy also found thatneither duration oftreatment nor WBDaffected responseamong persons with genotype 2/3infection—SVR ratesranged from 73% to
78% irrespective of ribavirin dose ortreatment duration.4
Survey FindingsA written survey of the full panel of Clinician’s Companion VIcontributors indicates that mostclinicians already believe in thebenefits of WBD of ribavirin: 96%said that when treating patients withpeginterferon/ribavirin they use aribavirin dose of >10.6 mg/kg. Evenwithout complete data from WIN-R,survey respondents also believe thata ribavirin dose of 1400 mg/d isappropriate (rating 4.1 on a scale of 1 = highly inappropriate to 5 = highly appropriate) for patients>105 kg. They also rated a dose of1200 mg/d as appropriate for suchpatients (rating 3.9). (Please refer to page 6 for more informationabout the survey methodology and population.)
ConclusionsAbundant demographic data haveaccumulated from this large study,shedding light on the epidemiologyof HCV infection and confirmingclinical correlations betweengenotype and viral level. This
study also confirms that African
Americans have a remarkably
high prevalence of genotype 1,
but indicates that genotype, race,
and viral load are not correlated
with fibrosis.
To date, the WIN-R study shows
that WBD does not have a dramatic
impact on hematologic toxicity of
peginterferon/ribavirin. WBD is
associated with a mean hemoglobin
level about 0.5 g/dL lower than is
observed with STD, and a greater
incidence of hemoglobin <10 g/dL;
however, the higher incidence of
anemia appears manageable with
dose reduction rather than drug
discontinuation in most cases. As
long as ribavirin is dosed by body
weight, higher doses are not
associated with greater risks of
hematologic toxicity. Neutrophil
count is not adversely affected by
WBD of ribavirin.
Further analysis of the WIN-R study
should yield prospective data on
whether WBD translates into greater
efficacy among patients treated
with peginterferon alfa-2b/ribavirin.
A preliminary report using
peginterferon alfa-2a/ribavirin
seems to support the notion that
WBD of ribavirin increases efficacy,
at least for patients with HCV
genotype 1 infection. However,
based on retrospective data from
previous investigations, WBD of
ribavirin has already become the
standard of care. TX
SVR
(%)
24 480
10
20
30
40
50
60
29
41 40
51
RBV 800 mg/d
RBV 1000–1200 mg/d
Treatment Duration (Weeks)
Figure 4. Peginterferon alfa-2a 180 µg + Ribavirin 800 mg Versus 1000 to 1200 mgin Genotype 1.4 Data presented with the permission of Hoffmann-La Roche, Inc.
John B. Gross, Jr, MDPrior to the introduction ofpeginterferon/ribavirin, an estimated400,000 patients were treated with standard interferon/ribavirin.At least 60% (an estimated240,000–280,000) did not achievean SVR. Many either havesymptoms associated with HCVinfection or are at risk forprogressive liver disease, and most would consider retreatmentwith peginterferon/ribavirin if there were a chance of clearing their HCV infection. Therefore,further attempts at viral eradicationare often warranted. Severalinvestigator-initiated trials are in progress to assess theeffectiveness of retreatment with peginterferon/ribavirin in this group of patients.
Conventional DosingVarious ongoing studies areassessing conventional doses ofpeginterferon alfa-2b/ribavirin—ie,1.5 µg/kg QW peginterferon alfa-2b+ 800 mg/d ribavirin or 1.0 µg/kgpeginterferon alfa-2b QW + 1000 to1200 mg/d ribavirin—in patientswho failed to achieve an SVR withinterferon/ribavirin. In the twolargest studies, on-treatment viralclearance at week 24 ranged from16% to 30%, and SVR rates havebeen 10% to 11%. Interestingly, one study showed that the rate of clearance at week 24 was 45%among those who had previouslyhad at least a 1-log drop in HCVviremia, while it was only 20%
among those who had not.5 Dosereduction has been required in 15% to 33%, with discontinuationin up to 22%.5,6
At the recent National Institutes ofHealth consensus conference onhepatitis C, Shiffman7 reportedpreliminary findings of the lead-inphase of the HALT-C (Hepatitis CAntiviral Long-term TreatmentAgainst Cirrhosis) Trial in whichnonresponders to interferonmonotherapy or interferon/ribavirinwere re-treated with 1 year ofpeginterferon alfa-2a 180 µg QWplus ribavirin 1000 to 1200 mg/d.All participants have advancedfibrosis. Among 212 patients, the 24-week on-treatment response rate was 30%. A preliminaryestimate of the SVR is 11%.
High-Dose TherapyHigher doses of peginterferon/ribavirin may further improveoutcomes in interferon/ribavirinnonresponders. The RENEW trial is comparing peginterferon alfa-2b0.5, 1.5, and 3.0 µg/kg QW, all with ribavirin 12 to 15 mg/kg/d. The low-dose arm was closed whenthe FDA approved 1.5 µg/kg fortreatment-naive patients. Ninety-two percent of participants areinfected with HCV genotype 1, 63% have stage 2 to 4 fibrosis, and 17% are African American(Gross JB Jr, et al, unpublished data, 2002).
Among 195 patients for whom 24-week treatment results were
recently analyzed, the intent-to-treat rates of HCV RNA clearance have shown a dose-related effect,with 53% of patients in the 3.0 µg/kg peginterferon/ribavirinarm responding (Fig. 5). Among 516 patients who have startedtherapy, the rates of discontinuationdue to an adverse event have been 6%, 5%, and 9% for the 0.5,1.5, and 3.0 µg/kg doses ofpeginterferon, suggesting that even 3.0 µg/kg is reasonably welltolerated. Rates of dose reductionhave been 22%, 24%, and 33%,respectively. Small numbers of serious adverse events haveoccurred at equal rates with 1.5 and 3.0 µg/kg (Gross JB Jr, et al,unpublished data, 2002).
Survey FindingsSurvey respondents want to see more data on high-dosepeginterferon/ribavirin beforeputting it into clinical practice, andare “on the fence” about re-treatingat all, at least in patients with milddisease. Contributors were asked torate the appropriateness (on a scaleof 1 = highly inappropriate to 5 = highly appropriate) of variousoptions for retreatment of a patientwith HCV genotype 1a and grade 1,stage 2 histologic findings whotolerated but failed to respond tostandard doses of interferon andribavirin. Their first choice waspeginterferon alfa-2b 1.5 µg/kg QWplus ribavirin 12 to 15 mg/kg/d(rating 4.2). Assuming itsavailability, peginterferon alfa-2a
10
R E P O R T E RSM : G A S T R O E N T E R O L O G Y
Treating Interferon/Ribavirin Nonresponders
11
TREATMENT REPORTER Emerging Advances: Preliminary Findings From Ongoing Studies of Peginterferon/Ribavirin
180 µg plus ribavirin 1000 to 1200 mg/d was the second choice (rating 3.2). The high-dose(3.0 µg/kg) regimen of peginterferonalfa-2b/ribavirin used in the RENEW study was rated 2.7, and the FDA-approved regimen ofpeginterferon 1.5 µg/kg QW plusribavirin 800 mg/d was rated 2.4.Other regimens with even lowerdoses of peginterferon alfa-2b oralfa-2a and ribavirin received evenlower ratings, indicating that theywere considered inappropriate.
Given a similar patient withgenotype 1b infection of 15-yearduration, histologically mild disease(grade 1, stage 1), who drinks twobeers per day (20 g/d ETOH), thesurvey respondents said that twoappropriate management optionswould include no further treatmentbecause of the small chance of SVR (rating 3.1) or retreatment
with conventional doses ofpeginterferon/ribavirin (rating 2.9).Retreatment with high-dosepeginterferon/ribavirin and nofurther treatment due to the slowrate of fibrosis progression wereeach rated 2.8. Maintenance
therapy was also considered fairlyinappropriate as a next option for this patient (ratings 1.9–2.1).
ConclusionIn summary, peginterferon/ribavirin in conventional doses produces on-treatment viral clearance rates of 20% to 30%, and SVR in 10% to 11% of nonresponders to priortreatment with interferon/ribavirin.
Preliminary datasuggest thepossibility of higherviral clearance rates with high-dose (3.0 µg/kg)peginterferon andweight-basedribavirin, withapproximately halfof patients havingundetectable HCVRNA levels at 24weeks thus far.
Relapse and SVR rates with high-dose peginterferon and weight-basedribavirin remain to be determined.
References1. Manns MP, McHutchison JG, Gordon SC, et al. Peginterferon alfa-2b plus ribavirin compared with interferon alfa-2b plus ribavirin for initial treatment of
chronic hepatitis C: a randomised trial. Lancet. 2001;358:958-965.
2. Fried M, Shiffman ML, Reddy RK, et al. Pegylated (40 kDa) interferon alfa-2a (PEGASYS®) in combination with ribavirin: efficacy and safety results from aphase III, randomized, actively-controlled multicenter study [abstract 289]. Gastroenterology. 2001;120(suppl):A-55.
3. Jacobson I, Brown R Jr, Afdhal N, et al for the WIN-R Study Group. Effect of weight based ribavirin dosing on hematologic parameters: preliminary safetydata from WIN-R [abstract T1390]. Presented at: Digestive Disease Week; May 19-22, 2002; San Francisco, Calif.
4. Hadziyannis SJ, Cheinquer H, Morgan T, et al. Peginterferon alfa-2a (40KD) (Pegasys) in combination with ribavirin (RBV): efficacy and safety results from aphase III, randomized, double-blind multicentre study examining effect of duration of treatment and RBV dose [abstract 37]. Presented at: 37th AnnualMeeting of the European Association for the Study of the Liver; April 15-21, 2002; Madrid, Spain.
5. Lawitz EJ, Cantu NS, Becker S, et al. Pegylated interferon alfa 2b (PEG-IFN) and ribavirin for hepatitis C patients who were nonresponders to previous therapy[abstract]. Gastroenterology. 2002;122(suppl 1):P-6.
6. Jacobson IM, Russo MW, Brown RS Jr, et al. Pegylated interferon alfa-2b plus ribavirin in patients with chronic hepatitis C: a trial in prior nonresponders tointerferon monotherapy or combination therapy and in combination therapy relapsers [abstract]. Gastroenterology. 2002;122(suppl 1):P-6.
7. Shiffman ML. Retreatment of patients with chronic hepatitis C. Presented at: NIH Consensus Conference: Management of Hepatitis C: 2002; June 10, 2002;Bethesda, Md.
TX
0
20
40
60
80
100
0.5 1.5 3
PEG IFN alfa-2b Dose (µg/kg/wk)
HC
V R
NA
Neg
ativ
e (%
)
23
39
53
Figure 5. Week 24 Response Rates in Interferon/Ribavirin Nonresponders: RENEWTrial. Gross JB Jr, et al, unpublished data, 2002.
PROJECTS IN KNOWLEDGE
One Harmon Plaza
Secaucus, NJ 07094-9709
EducationInitiative inGastroenterology
Copyright © 2002, Projects In Knowledge, Inc. All rights reserved.1571A
THE CLINICIAN’S COMPANION VI:
Expert Perspectives onContemporary ClinicalIssues in Hepatitis C