Embed Size (px)
Citation preview
The Comprehensive Breast Care Center of Tampa BayPeter W. Blumencranz, M.D., FACS
Medical DirectorSurgical Oncology
Diseases of the Breast/Melanoma
Kathleen G. Allen, M.D., FACS Surgical Oncology
Diseases of the Breast
MBA,
Thank you for choosing The Comprehensive Breast Care Center of Tampa Bay.
Appointment Location
___ Axelrod Pavilion 400 Pinellas Street Appointment Date: __________________ Suite 200 Clearwater, Florida 33756 Please arrive at: _________:________am/pm (727) 462-2131
___ Morton Plant Mease Outpatient Center 2102 Trinity Oaks Boulevard Suite 202 Trinity, FL 34655 (727) 462-2131
Please bring the following information to the appointment with you:
Photo ID
Insurance Card(s)
Completed paperwork
and reports from imaging center outside of Morton Plant (example: SDI, Rose Radiology, Gateway Radiology, Palm Harbor MRI, Westcoast Radiology)
Failure to bring completed paperwork and imaging reports/disks may result in your appointment being
rescheduled.
Thank You!
The Comprehensive Breast Care Center of Tampa Bay
Rev. 3/2017
mron Fiotraattsiegt RientaatPormation nfatient IP
:emNa ___________________________________________________________________ e:mat nsd �rererefferrP _______________________________________
:OBD __________________________________________________ le aem F N:le SSa M __________________________________________________
e:nohy praimrP ________________________________ e: ypTTyp emHo lelC s:utatl satirak MroWWo ___________________________________
ce: enerefferrn piotai�ctot nientay praimrP e nohy praimrP neho pyy randoceS liMa
: ythnicitE o intar Lnic oapsiH ace: o Rintar Lnic oapsit HoN e vitaka Nsalr An oadinn IaicermA n asiAn aicermn Aaicrffrr Ak oaclB
der nalsaci�c Ier Phtr On oaiiwaaawae HvitaN eitWh er htOe:gagunay lraimrP ______________________________________________
s: esy addrraimrP _____________________________________________________________________________________________________________________
:yitC ________________________________________________________________________ :eatt S _______________________ :ip Z _______________________
s:esy addrraimrf py ortunoC ______________________________________
:neho pyy randoceS __________________________________________________________________________________ e: yp T Typ emHo lelC krWo
l*:ial emanoserP ________________________________________________________________ n: iotai�ctof nd oohetd mererefferrP nehoP laimElatrot penitae pho ts tseccr aod f foeriuqes rl iial emanoser*P
s:esy addrradncoeS ___________________________________________________________________________________________________________________
:yitC ________________________________________________________________________ :eatt S _______________________ :ip Z _______________________
ormation nfformationatient Idditional PA
n:aysicihhysicie pray craimrP _______________________________________________________________________________________________________________
le: bsinopesy rllacinan �noserP p:hisniotaleR
le: bsinopesy rllacinan �noserP _____________________________________________ p:hisniotaleR ____________________________________
e):ray craimrm port f frenern (if di��eraysicihg pinrerefferR ___________________________________________________________________________________
s?t uuobr aaeu how did yoH ___________________________________________________________________________________________________________
:erylopEm ___________________________________________________________________________________________________
s:eser addrylopEm ____________________________________________________________________________________________________________________
:yitC ________________________________________________________________________ :eattS _______________________ :ip Z _______________________
:nehoP _________________________________________________________________________ xt:E _________________________
t:actny cocengerEm _________________________________________________ t:actncoy cenger Em _____________________________________________
t:actno cop thisniotaleR _________________________________________ t:actno cop thisniotaleR _____________________________________________
e: noht pactnoC _________________________________________________________ e: noht pactnoC _____________________________________________
s: utatt senmylopEm __________________________________________________________________________________________________________________
m
:yarmiPr
ormationnfnsurance II
ron Fiotraattsiegt RientaatP
______________________________________________________ :yradonce S __________________________________________________________
lder ID:oy hlicoP _____________________________________________ lder ID:oy hlico P ____________________________________________________
e:malder noy hlicoP ___________________________________________ e:malder noy hlico P _________________________________________________
B:Older Doy hlicoP ___________________________________________ B:Older Doy hlico P _________________________________________________
: erylops em’lderoy hlicoP _____________________________________ : erylops em’lderoy hlico P ____________________________________________
:lderoy hlicoo pp thisniotalet rientaP __________________________ :lderoy hlicoo pp thisniotalet rienta P ________________________________
le aemFex: lder soy hlicoP leaM ex: lder soy hlico P
t:unomy aapoC
elMale aemF
_______________________________________________
:ycmarhaP ______________________________________________________ n:iotacoL _____________________________________________
e:nohy pacmrahP _____________________________________________________________________________________________________________________
:idervorP
. ww. loeider(s) bvore phf te omae nhe ttadice insalees, pf y yes, pI
Noes YYes r? otce doray craimrur poh ytit wsiit vsaur loce y yot sinsliaciepen a seu soe yvaH
Noes YYes r? otcur dooh ytin wiotaunicmmen cokken coope stalicpml colit waht tenmirapg iminraee a hvau hoo yD
Noes YYes r? otcur doom y yoorl f fraiertaen mttirg wadinem roru f frot yenverl plit waht tenmirapl imausie a vvau hoo yD
ormationnfformationd IendextE
____________________________________________________________________________________________________________________________
:idervorP ____________________________________________________________________________________________________________________________
eurtnaatigt snetiatP :_________________________________________________________________________
e:mad netinrP
____/____/____:eta D
____________________________________________________________________________
C1700186-0217B
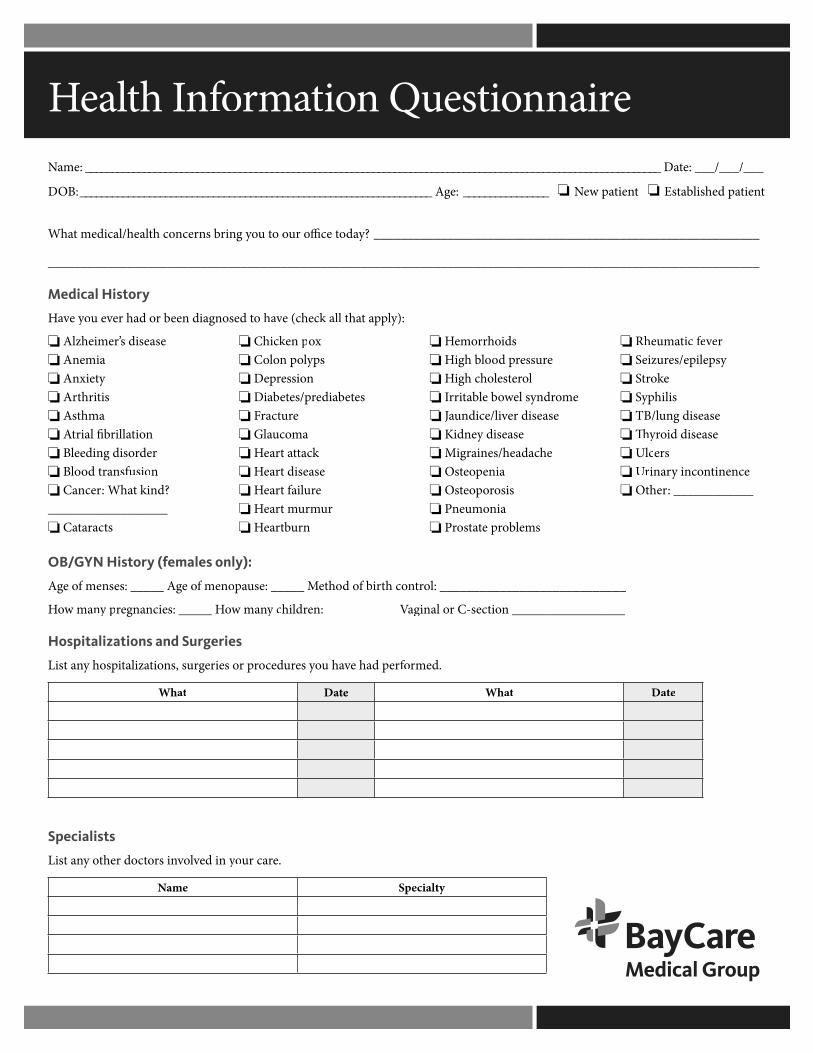
eirnann Questioiotamroffon IhtaleH
___________________________________________________________________________________________________________
__________________________________________________________y? daay? o�ce tur o oou tog yinr bsnncerh cotla medical/hetahW
t tienw paeN________________:eg A__________________________________________________________________:BOD
___________________________________________________________________________________________________________:emaN
yistordical HeM
y):lpp atah all tkk hec (cev ha avod teen diagnose brer had ovu eo y yoevaavH
emales only):y (f females only):istorYN HG/OB
_________________ntioec C-sraginal oen: ___________V Vaginal oildrh cyy nw maoncies: _____ Hegnar pyy nnyw maoH
l: ____________________________ortnh cotri bff odohtee: _____ Muspa menoff menoe oges: _____ As menff mene ogA
eriesrguHospitalizations and S
h Otinr U Ur
lc Uy � �y
TB/p Syro St
eiz Seh R Rh
slemobr petaostr Pianeumon Posisropoets O
eniapoets Oehdacanes/heigrai M
ease disyidne Keaseer disvundice/lia J
meol syndrewole bbatirr Ilorelestoh chgi H
eessurrd pool bhgi Hidsrhormoe H
nurtbrae Hurmrut mrae H
eurilt farae Heaset disrae H
kcattt arae Hmauco Glaerutrac F
esetbdiaeres/petb Dianessiorpe Dypslon ploo C
xoen pkken p Chic
tsracata C__________________
kind? tah: Wncera Cnusiosffusion tradool B
derrog diseedinl Bniotrillabrial �t A
amht Asstirithr A
Anxiety Anemia
ease diss’ Alzheimer
________________
________________
ttienished palbaEst
___/___/___:etaD __
te
____________:herinencetny incorna
sereaseid disoryeaseg disun /l
silihpkeo
ilepsyes/epzurrevveeic f feteuma
aa D
.medroffore had pevu haoes yuredcor pries oergs, surntioalizatiy hospnst aiL
D te taatWhaDtaaWh
pecialistsS
. erur caoed in y yovlovs inrotcher doty onst aiL
ialtycepSmeaN
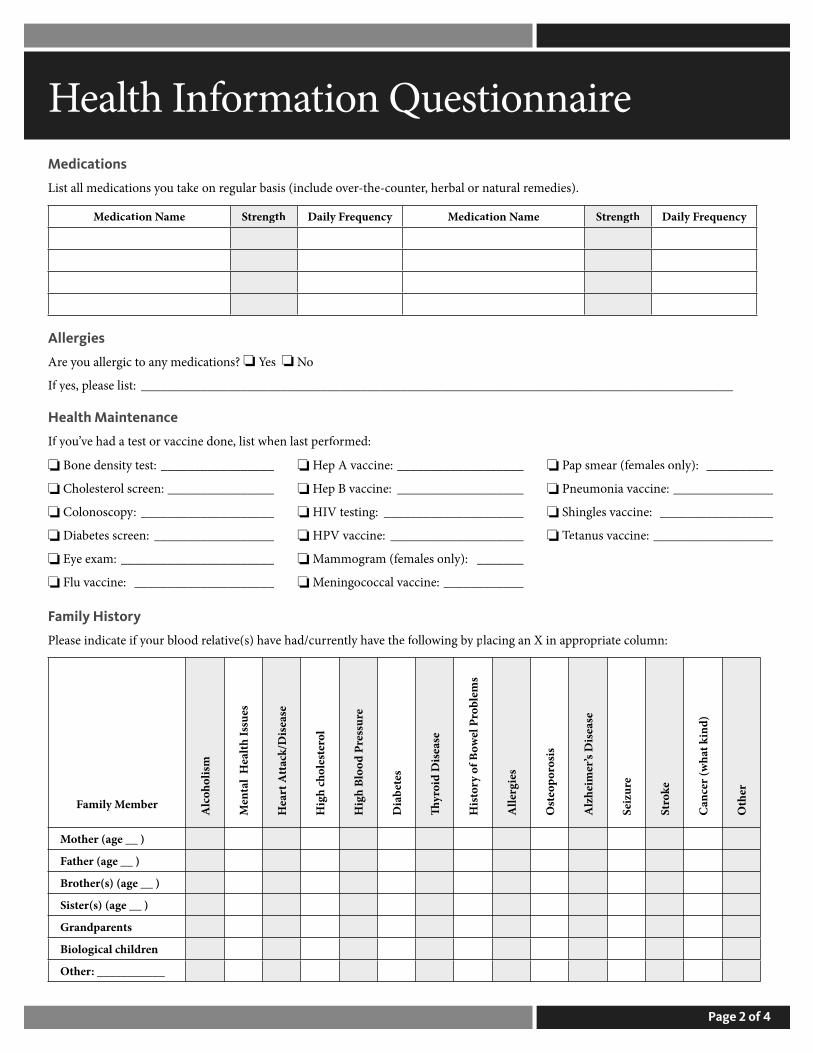
edicationseM
irnann Questioiotamroffon IhtaleH
medies). eural rt nar herbal o,retunhe-co-tervude olcr basis (inegula rn oekkeau to ysniotst all medicaiL
th ynceuqerly FDaiggthnertSth mean NoitaacideMynceuqerly FDaiggnertSmea NnotiaacdieM
lergieslA
_________________________________________________________________________________________ list: esaeles, p yff I
Noes Y Yes s? nioty medican aogic tu alleroe yAr
enanceHealth Maint
__________________s vaccine: unate T Te
_________________les vaccine: ghin S
_______________ia vaccine: neumon P
__________y): lnemales or (f females oap smea P
____________ccal vaccine: coogenin M
_______y): lnemales om (f females ommograa M
____________________ HPV vaccine:
_____________________g: stine HIV t
___________________ep B vaccine: H
___________________ep A vaccine: H
_____________________u vaccine: Fl
_______________________m: e exay E Ey
__________________en: erces setb Dia
____________________:ypocnosloo C
________________en: ercl sorelest Cho
_________________st: ety tsine deno B
med:rofforeen last ph, list w whne vaccine dorst oe had a tev’uo yff I
yistoramily HF
umn:le cotairporpp X in ang aacinl pyy g binwllooe f foh tev hayltnerur had/ceve(s) ha avvtilae rdoolur boe if y yot indicaesaPle
Oth
ere
ind)
t kha
ncer
(wa
C
kSt
ro
e
eiz
ureS
saes D
is’
Alz
heim
ers osis
ropoetsO
eirgel
Al
e
ms
eob
lr
owel
P Bff
y o
rosti
H
sae D
isdiory
��y
e
esetb
Diaa
b
essu
rr
Pdool Bhgi
H
e
oler
ste c
hol
hgiH
saeta
ck/D
isttt
t Aare
H
coho
lism
essus
alth
Ie
al H
tneMA
lerembly MmiaF
4f 2 oegaP
___________:Other
nerdlal chiciogoliB
arentsandpGr
er(s) (age __ )stiS
ther(s) (age __ )orB
ther (age __ )aF
ther (age __ )oM
eirnan Questiohtalet Htienaatienw PeN
s:nuestioal qntioe addiesher tswnes, aed yerswnu ao yff I Noes Y Yes l? hoink alcou dro y yooD
ld: ehouss in honosre pff er obmu Nen: ildrh cff er obmbuN
__en? �w ooH_______________________c.)? g, etg, swimminunning, r, walkingkini.g. b (eeciser exff oe typtahWo Nes Y Yes e? cisery exrlegulau ro y yooD
____________________________________________________________h grade: uggh grade: orhn tiotucaEd
_________________________________________:herOtd ewidoWed crovDiedrriaMle gniSus: tatl satiraM
__________________________________________________________________n: tiopauccer omrour f foo was y yotah w,detire rff Iull-time Fn: _______________________________________________________________________tiopauccO
___________________________l? ho alcoff oe typtah W_______________________________y? ltueneqrw f fro H
_______h? u higoet y go tekkea ttes iinks do dryy nw mao H
Noes Y Yes g? inkindrur og yicizinti cryy u bod yeynonle apoe pevaH
Noes Y Yes g? inkinur droynwn ot douuld cu shoo ytleer f fevu eo yevaH
Noes Y Yes es? vur nero yyy dae stog tninrmoe hg in thinst tink �rer had a drvu eo yevaH
ual qntioe addiesher tswnes, aed y yes, aerswnu ao y off Ilem obre pusbnce aaer had a substvu eo yevaH
__________e? u usougs do y drff oe typtah W
ual qntioe addiesher tswnes, aed y yes, aerswnu ao y off I Noes Y Yes ed? kked? er smovu eo yevaH
_______________________________y? ltueneqrw f fro H
o Nes Y Yes e? ku still smoo yo D_______________________y? es/daay? tter cigayy nw mao H
_______ed? ku smoo yevs harae yyy nw mao H
____________________________t? iuu qoyen did hg, winked smoppoy stltceneu ro yff I
yistorSocial H
4ff 3 oegaP
____________
________________________
____________
____________
____________t-timera P
s:nuestio Noes Y Yes m?
__________
s:nuestio
__________
____________________
__________
______________________________:her Otl ortnh cotri Bs mndoo Cn: tioraceptn coff e osUUs__________________n: tioatienred oibcrlf-deseS
_____s: nertre pa lif fe paff er obmuN_________________s: nertr paff t # oenrru C_____________e: agt aevtist acFir Noes Y Yes e? vtiy acexuallu soe yAr
Noes Y Yes do? oed tu usogs y ohing tin in doesurael prst oeret inkk u laco y yooD Noes Y Yes e? ur lif fe? oss in ye strff strl oevh le a higeveu hao y yooD
Noes Y Yes s? lemobr pgniy sleepnny sleep aevu ha avo y yooD Noes Y Yes r basis? egula rneine o��eine oe cau uso y yooD
Noes Y Yes ecial diet? p a snu ooe yAr Noes Y Yes y diet? hhy diet? talt a heau eo y yooD
Noes Y Yes t? nmenovirme enur hoo in yeffeael seu f feo y yooD______________________________:her Otrm Dondo o Ct tmenrap Aesu Hot: menegnrar agg vin liff oe typtahW
__________________________ p______________________________
eormationfformationnGeneral I
irnan Questiohtalet Htienaatienw PeN
m.otpe symh tork next tk maechace a clys, pe last 10 da ays, phe issues in tesh tff y onienced aeru expo yff I
______________________________________________________________________________e? typtahes, w yff I Noes Y Yes e? vtiecnce dirva adn ar will ogg will ovin a lievu hao y yooD
__________________________________________________________________ty? liibaur diso yff oerute nah is ttahes, w yff I Noes Y Yes ed? lbau disoe yAr
___________________________________:her Otl i Emae n Phou? ot y yoactn coo�ce te ohr toy f fost waee bh is ttahW___________________________________________________n? tiomaro inf foer cahtalr heo f foeuaggnd laererefferrur po is y yotahW
________________________________________________________________m? ro f fohtalis hehed tletpmo cohW
General
inloss/gatheigghined wlaexpnU
tigue faevcessiExrevet f fe Recen
sEye
gniret warg ohinct Ith sigff sigss oo L
nd visioerurl Bgninru brin oa P
egrhac Dis
eastBr
egrhacle disppi Nsmp Lu
ina P
yespiratorRhugoC
ental Health M
rsehotg minr haff ts ohuggh�o
Anxiety skcattnic aa P
gnile sleepbuor T Trslemobrl patira M
suicideff suicidets ohuggh �o
Skinils in naegn Cha
t rashesenrru RecsmpLu
gginnahe cr atahles to Meedl btah tro
al t he will notahes troS
arsEsg losinrae H
ndocrineE
regnu hevcessiExsthir tevcessiEx
ld coff once leraotusual innU
tae hoff nce leraotusual innU
yrinarU
maert in segn Chaine urff e oakage L
etina uro tp ugkina W Waetina uro tgg tinrale stbuor T Tr
ine in urdool Bniotinat urueneqr F
niotina urhtg wininurin/ba P
stemyous SvreNhesadace H
vCardio
eg p Leg p L
elliw St roh S
ssina Phtaerb
akwAAw Chest
t arhenobAAb
oinGastr
dtrae Hu infful swalloa P
doo Fss oo L
l ban U
4f 4 oegaP
_________
_________
___________________________
ascularv
gin/walkin agestinin/r aleskklesn aff g oin
htaer bff bness otug on
slemobrg phinht with nig ghten akken a
in t patae b
r egularal/irmr
ntestinal
lsook stlsoot in sd
sl ewo in begnaht cn
notipatiahe
inh paacmo strminal odool bgg tin
aenestio
nurtbginwul swallo
taorhks in tict stheigghe/wttiepp aff o
sdooin f foatt cera eole t
eletalosk
nesserole sness sti� �ness
in pa
sordersi D
geedinl bevsisguisinr b
ginron Sgeezinh W
htaer bff btness oroh Sdool bpg uhinugghino C
hugoC
omene - WoductiveprR
esruocretingnirule duboin/traP
sdoireul pinfful py pausualln Ughinctg/ininrub
/ egrhacginal disaVVasdoireeen ptwe bgtintop S
sdoirer pegularr I
nee - MoductiveprR
ntioec erhts wilemobr Pesruocretin
gnirule duboin/traPlesstice tff g oellin swrin oa P
enis pmor f fregrhac Dis
g
llnessur f fua eff g oeline Fheraca E
gingRin
oatThrouth and M
al issuestne Dssenesra Ho
sh ulcertuo Mtaroh treo S
aerh atuin mog eedinl brness oeroS
htuy mo Dr
tyul di�cheecp Sbg in limling tinff g oeline Fess nbumbn/niotasne sff ss oo L
remo trrs oakinesh Sssenka We
s losyy rt memoueneqr Fellsp sgg tinina F
snulsiovnes/coeizur S
inusesse and SoN
smellff smelle osne sff ss oo Lgeezinn S
nestiognl coasa Ngeedinl B
eckNina P
smpLu
k acl Bdool Bsbitah
Recentsno C
rhr Diadob A Abmio V Vo
esu Naedign I
usculoM
l csu Mt sino Jt pino J
Blood D
ces Exsy ba E
uey Qrotsiy HlmiaF
eiranniotes
iskrrecant c
amon idroyhT reOth
lpmo celeasP
yilmFa
uroY
uYo
sonrepg inowoll the foelet
deseaecDY/N
f oegAsisongDia
staBre
N/A
y to istory hilmafadal ann
yrvaO eascranP sruUte
ast er brss youse asrett be
nloComuectR
r oachmotSlwe BollamS
laneM
terhtgDau
erthMouroY
s)(terSisuroY
n SoruYo
erFatheuroY
alrnteaMerhtomodandGr
alrnteaM)st(ntAu
uroYs)(ertheorB
alrnteaMerhatffatdandGr
alrnteaM
alrnteaPerhtomodandGr
alrnteaP)st(ntAu
)scle(Un
alrnteaPerhatffatdandGr
alrnteaP)scle(Un
etene: GemtcoOunlyUse Oice fi ffO
khksAfouoye rA_______________
y anyr ouoye Hav
erOth)(
ederfeffOgnelisnuo/CgnestiTic t:y
sYe?ytrysceni aazenak______________________________
een gad haer everbmemyilmafay
______slaitinIedsufue/R
wnonknkUNo_______________________________
o NYes ?gnitestic et
_____ _____etaD_ ___
____________________________
rdnae pyt tslilease p,s yefI
____________
: ltsuesr
. 10/16v. eR
iotuese Qrat CsaerB
eiranno
_________
___NoYes
dioer pruoye rAt sirfiruoyfoe Ag
LARUTNSEM
etfesear buoyDidniv lif oerbmNue vt lisirfifoe Ag
CYNANGREP
NoYes ?laruegu rs________: _diorepal utrsnemt
: DSRIOE P
NoYes : dee_ ______ _: nerild chg
_________: _thirb:
P(
ug:r dthatW evuoye HavNEORMHO
fod n anehW evuoye Hav
H COBIRT
)ti lidi/B/Pi
_____________________________?seneomrohenk taer v
:YPARHE TE
_____________ __?ngolwo hoorfo?illspl otrnt cothir benk taer v
:LRONT O
est Whe CsuioevrPyspiot BsearB
evomeies RarOvymytoectersyHy HILAICURGS
uopanoemtaegAd ori petsa letatD
py
NosYeniatioadRall WNoYes NoYesedNoYes
:RYOT S
_______________ ___?esu_________________ __?nag be
g
?reehewd n anehwo, sfI__: _Datet ft eLt / ht igRaDh tot/ Bft eLt / ht igR______________ _:
fd nd anehW
aremar P.ge.(
______________________ _____? ____:egA________________
__e: _Ag____________ _:etat____ ________:egA______
______________ __?ngolwo hoorfo
)sticalentidio/Borpempr/Pin/r
______________ __________
_
__________
l UltbAb
mal Mama ronobAb
mauarTt searB
garchale DispNip
ainP
n feacu o ypmpuLR PNTECURR
NY d
NoYes margom
NoYes
NoYes eg
NoYes
NoYesleeW :MEBLRO
_____________________
_____________________
_____________________
_____________________
____________________ice?tnoirst u fod ydiWhen
_____________________________
_____________________________
_____________________________
____________________________
____________________________
___________
__________
___________
___________
___________
AN NCIYSIHP
rehewd nd anehW
rehewd nd anehW:INGGAIM
erOth
asal Ultrma ronobA
S: ET NO
ounsartlutsaerbtsa lruoysawe
?margommamatsa lruoysawe
NoYes
NoYes dnduso
______________________ ___d?nd
________________________ ____
____________________
_____________________
______________________________
______________________________
_______________________________
_____________________________
___________________
____________________
____________________
____________________
____________________
_____
___
__________
__________
________________
________________
________________
________________
________________
___________________________________
___________________________________
__________________________________
___________________________________
___________________________________
__________________________________
__________________________________
__________________________________
__________________________________
__________________________________
_________________________________
_________________________________
_________________________________
_________________________________
_________________________________
. 10/16v. eR
__________________________________________________
__________________________________________________________________
__________________
Uses and Disclosures of Your Protected Health Information (PHI)I understand that as part of my health care, the practice originates and maintains paper and/or electronic records describing my health history, symptoms, examination, test results, diagnoses, treatment and any plans for future care or treatment. I understand that this information serves as:
A basis for planning my care and treatment
A means of communication among the health professionals who contribute to my care, such as referrals
A source of information for applying my diagnosis and treatment information to my bill
A means by which a third-party payer can verify that services billed were actually rendered
A tool for routine health care operation, such as assessing quality and reviewing the competence of sta�
I have been provided with a “Notice of Patient Privacy Practices” that provides a more complete description of information uses and disclosures.
Tell us with whom we may discuss your protected health information: (Name and relation - Example: Jane Doe, Wife; Jan Doe, Daughter) ____________________________________________________________________________________________________________
Messages or Appointment RemindersMessages will be of a non-sensitive nature, such as, appointment reminders.May we leave a message on your voice mail using doctor’s/practice name? Yes NoMay we leave a message with another individual using doctor’s/practice name? Yes NoMay we leave a message at your work using doctor’s/practice name? Yes No
I understand that as part of treatment, payment or health care operations, it may become necessary to disclose health information to another entity, e.g. referrals to other health care providers. I understand that my information may be used or disclosed, without an authorization, as permitted or required by law.
_________________________________________________________________ _________________________________Patient/guardian signature Date
_________________________________________________________________Print name of person signing
If other than the patient (patient name) _______________________________________________________________________is signing, are you the legal guardian, custodian, or have Power of Attorney for this patient, for treatment, payment or health care operations? Yes No
Patient ConsentRequest for Care and Consent for Treatment�e undersigned consents to the medical care and treatment, as may be deemed necessary or advisable in the judgment of my physician or other provider, which may include but are not limited to laboratory procedures, X-ray examination, medical or surgical treatment or procedures, anesthesia or other services rendered to the patient under the general and special instructions of the patient’s physician. BayCare Medical Group has the right to refuse to treat you if you refuse to sign this consent or if, at any time, you choose to revoke this consent.
Assignment of Insurance BenefitsI authorize payment directly to BayCare Medical Group of any insurance bene�ts otherwise payable to me for services, at a rate not to exceed BayCare Medical Group regular charges for such services.
Releasing Medical InformationI understand that BayCare Medical Group, its business associates, any treating physician/surgeon and/or my insurance company may obtain, use and/or disclose information for the purposes of treatment, payment and normal health care operations. �is use and disclosure may include collection agencies and credit bureaus. Information may include psychiatric, drug abuse, alcohol and/or HIV status. I understand that if I do not consent to release of information for payment purposes, the Facility and other health care providers will be unable to bill my insurance company or other party which is or may be responsible for payment for the services documented by the withheld information, and I will be billed directly for these services. Patients with implantable devices consent to the release of their Social Security numbers to the device manufacturer to comply with the Safe Medical Devices Act. For a more detailed description of uses and disclosures for treatment, payment or normal health care operations, review BayCare Medical Group’s Notice of Privacy Practices.
Permission for TreatmentPermission is hereby granted for physicians, employees or agents of the Practice to render the patient named below such medical and surgical treatment as is deemed necessary.
�e undersigned certi�es that he/she has read the forgoing, received a copy therof and is the patient or is duly authorized by the patient as patient’s general agent to execute the above and accepts its terms.
Patient (print name): __________________________________________________________________________________Signature of patient or authorized person: __________________________________________________________________Relationship: _______________________________________________________________ Date: ____________________Witness signature: __________________________________________________________ Date: ____________________If the patient did not sign, please state reason: _______________________________________________________________
BC1505258_0815 BC 1873
Financial ResponsibilityImportant Information Regarding Your Account
Statement of Financial ResponsibilityI understand that I am responsible for the payment of this account, and hereby assume and guarantee prompt payment of all expenses incurred.
Notice of “Non-Covered” ServicesI am aware that some services performed by the Practice may be considered “non-covered” by my insurance carrier or Medicare, therefore I will become fully responsible for payment of these services.
Waiver of “Usual, Customary and Reasonable” Clauses (For patients with “Out-of-Network” coverage)I acknowledge that the fee charged by the Practice for services rendered to me, or to the person for whom I assume �nancial responsibility, may exceed the fees considered “usual, customary and reasonable,” due to specialized services and sta�. However, I agree to pay the Practice fees in full, even if the amount is greater than what I am reimbursed from my insurance company.
Bill To/Payment Instructions_____ Commercial Insurance/�ird Party Payor _____ Medicare _____ Medigap*Initial Initial Initial
I hereby authorize the Practice to bill my insurance company and/or Medicare (indicated or initialed above) for services provided to me and request that payments for such services to be made to the Practice on my behalf.
*If Medigap _______________________________ ___________________________ __________________________ Name of Bene�ciary Medigap Policy Number Health Insurance Claim Number
List Names of Those with Whom You Want Us to Share Your Financial Responsibility Information: Name: Relationship:_______________________________________________________________ ____________________________________________________________ _______________________________________________________________ ____________________________________________________________ _______________________________________________________________ ____________________________________________________________
Financial Agreement�e undersigned agrees, whether he/she signs as agent or as patient, that in consideration of the services to be rendered to the patient, he/she obligates himself/herself to pay the account of the clinic in accordance with the regular rates and terms of the clinic. Should the account be referred to an outside agency or an attorney for collections, the undersigned agrees to pay reasonable collection and attorney fees for collection expenses.
Patient’s name: ____________________________________________________________________________________________________________________________ (please print)
Patient (or legal guardian’s) signature: ____________________________________________________________
Date: ____________________________________________________________________________________________
If legal guardian, relationship to the patient: _____________________________________________________
Authorization to Use or Disclose Protected Health Information
Physician___________________________________________________________________________________
I hereby authorize the above physician(s) to use or disclose the following information from the health records of the individual whose name is described below.
Patient Name:_________________________________________ Date of Birth:___________________ (Please Print) Address:__________________________________________________________________________________ (City) (State) (Zip) Phone Number:_______________________________ Social Security #______________________________
I authorize the above physician(s) to release medical, mental, alcohol and/or drug abuse, HIV (human immunodeficiency virus) testing, AIDS, eating disorders or any other medical information of a sensitive nature to the following individuals or organization(s):
Name:____________________________________________________________________________________
Address:__________________________________________________________________________________ (City) (State) (Zip)
This information for which I’m authorizing disclosure will be used for the following purpose: Description:_______________________________________________________________________________
Dates of service to be released:________________________________________________________________
The type of information to be used or disclosed is as follows (check the appropriate boxes and include other information where indicated). Copy medical records to Electronic medium or Paper
Office Notes Radiology Results Immunization Record Lab Results EKG Medications Other: (please describe)_______________________________________________________________
I understand that if the organization authorized to receive the information is not a health plan or healthcare provider, the release information may no longer be protected by Federal privacy regulations. I understand that I need not sign this authorization to ensure treatment. This authorization shall remain valid for six months from the date signed below.
I understand that I have a right to revoke this authorization at any time. I understand that if I revoke this authorization, I must do so in writing and present my written revocation to the department or facility listed on the authorization. I understand that the revocation will not apply to information that has already been released in response to this authorization. I understand that the revocation will not apply to my insurance company when the law provides my insurer with the right to contest a claim under my policy.
Signed_______________________________________________ Date________________________ Patient or Authorized Person, Parent Legal Guardian Executor Power of Attorney Photo ID checked
Witness:______________________________________________ Date:________________________
Copied by:____________________________ Date:____________________ Pages copied:_____________
AUTHORIZATION TO USE OR DISCLOSE PROTECTED HEALTH INFORMATION BC 2958 4/16
P A T I E N T