Embed Size (px)
Citation preview
The Continuum of Products
and Solutions for the
COPD Patient
1 AARC CEU credit
Objectives
• Review COPD
• Discuss current practices for treatment – components
of care
• Review COPD staging
• Identify the Philips Respironics Incorporated (PRI)
products and solutions as they relate to the
progression of COPD
• Present tools which will help your DME to grow and
thrive in today’s market
2
Objectives
• Understand how home NIV may contribute to
reduction of readmissions for patients may have
chronic respiratory failure.
• Review patient identification for home NIV Tx
• Understand new options for home NIV
– AVAPS-AE mode of ventilation
– Mouthpiece Ventilation
3

COPD and Home NIV
COPD: An overview
4
5
COPD and Respiratory Insufficiency
• Often (but not always) caused by smoking or long term exposure to
irritants. Over time this irritation creates obstruction of the lower airway
that interferes with gas exchange, can’t get air in or out.
• Patients with OSA have obstruction issues in the upper airway, COPD
creates obstruction in the lower airways.
• Lungs lose normal elasticity like an overstretched rubber band. Patients
with advanced/very severe COPD often experience respiratory fatigue
leading to respiratory failure. Respiratory Failure in COPD is
sometimes referred to as hypercapnia meaning elevated levels of CO2.

COPD – fast facts
• leading cause of death
• Million afflicted
• Million diagnosed
• Million moderate to severe
COPD worldwide
• 3rd
• 24
• 12
• 65
6
COPD Characteristics
• Chronic Bronchitis & Emphysema
• Persistent, Non-Reversible Airflow Limitation
• Loss of Tissue Elasticity
• Paranchymal Destruction
• Airway Inflammation

8
Long-Term NIV for COPD with Chronic
Respiratory Failure Nava EMJ Oct 2013;1;54-62
1.) COPD During Sleep: Nocturnal Hypoventilation noted in REM sleep*
• 42% COPD Pts.= PaCO2 ↑ >10mmhg at night – ↑ tolerance for ↑ PaCO2
• Low Central Respiratory Drive
*REM sleep = Impaired upper airway tone and accessory muscle
activity. 1

Quality of Life Impact of Severe COPD
Long-Term NIV for COPD with Chronic Respiratory Failure
– Nava, Ergan EMJ 2013; 1:54-62
“Symptom burden comparable
to that of cancer”
“Greater negative impact
on health status than
cardiovascular disease
or diabetes”
9

Change in COPD Mortality compared with
other major causes from 1970-2002
COPD Heart disease Cancer Stroke Accidents Diabetes
Death rate (% change) 102.8% -52.1% -2.7% -63.1% -41.0% 3.2%
-80.0%
-60.0%
-40.0%
-20.0%
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
120.0%
Death rate (% change)
U.S. Leading Causes of Death; JAMA, September 14, 2005 – Vol. 294, No. 10 10

Published guidelines
GOLD
• Global initiative for Chronic Obstructive Lung Disease
NICE
• The National clinical guidelines on management of COPD in adults in primary and secondary care
ATS – ERS
• American Thoracic Society – European Respiratory Society
SEPAR – ALAT
• Spanish Society of Pulmonary and Thoracic Surgery – The Latin American Thoracic Association
HOT TOPICS IN RESPIRATORY MEDICINE: Issue 5, 2007 ... Guidelines for the treatment of COPD. Javier de Miguel Díez, Myriam Calle Rubio, ..... Aalbers R, Ayres J, Backer V, et al. 11
COPD stages
Severity classified by spirometry (PFT’s)
Stage 1 Stage 2
Stage 3 Stage 4
12

COPD stages
Severity classified by spirometry
Stage 1
GOLD Pocket Guide to COPD Diagnosis, Management, and Prevention. A guide for Health Care Professionals Updated 2010. See also www.goldcopd.org 13
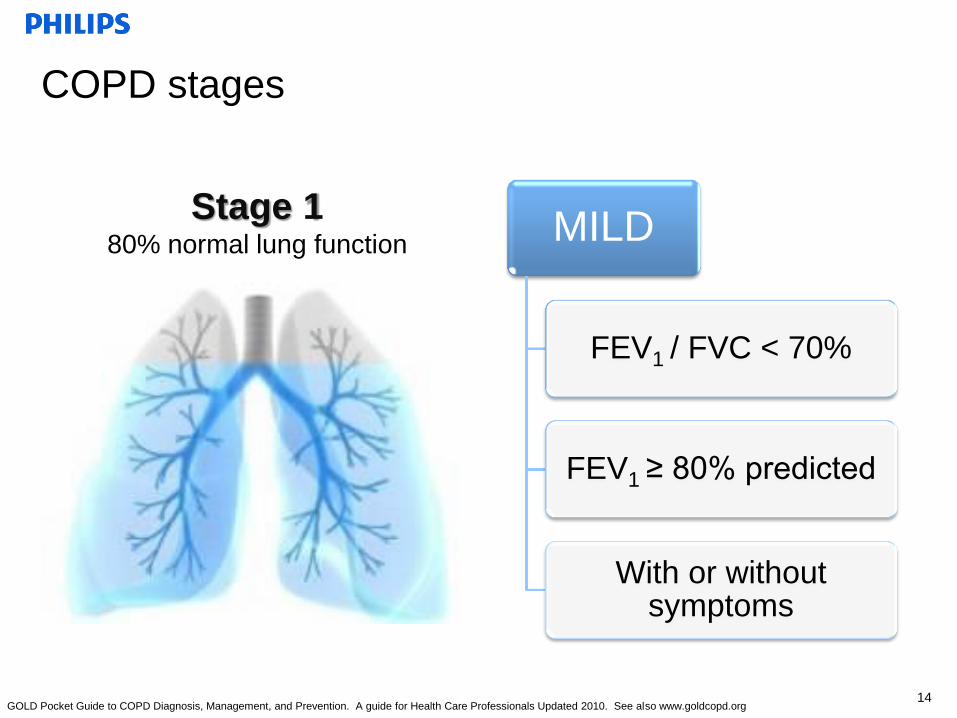
COPD stages
MILD
FEV1 / FVC < 70%
FEV1 ≥ 80% predicted
With or without symptoms
Stage 1 80% normal lung function
GOLD Pocket Guide to COPD Diagnosis, Management, and Prevention. A guide for Health Care Professionals Updated 2010. See also www.goldcopd.org 14

COPD treatment considerations
Stage 1
Mild
• Avoid risk factors
• Influenza vaccination
GOLD Pocket Guide to COPD Diagnosis, Management, and Prevention. A guide for Health Care Professionals Updated 2010. See also www.goldcopd.org 15
COPD treatment considerations
Stage 1
Mild
• Avoid risk factors
• Add SABA
OptiChamber Diamond, valved holding chamber
GOLD Pocket Guide to COPD Diagnosis, Management, and Prevention. A guide for Health Care Professionals Updated 2010. See also www.goldcopd.org 16
COPD treatment considerations
Stage 1
Mild
• Avoid risk factors
• Add SABA
Holding chamber
SVN - MicroElite
GOLD Pocket Guide to COPD Diagnosis, Management, and Prevention. A guide for Health Care Professionals Updated 2010. See also www.goldcopd.org 17
COPD treatment considerations
Stage 1
Mild
• Avoid risk factors
• Add SABA
• Spirometry
GOLD Pocket Guide to COPD Diagnosis, Management, and Prevention. A guide for Health Care Professionals Updated 2010. See also www.goldcopd.org 18
COPD treatment considerations
Stage 1
Mild
• Avoid risk factors
• Add SABA
• Spirometry
Oximetry screening – WristOx
GOLD Pocket Guide to COPD Diagnosis, Management, and Prevention. A guide for Health Care Professionals Updated 2010. See also www.goldcopd.org 19

COPD stages
Severity classified by spirometry
Stage 1 Stage 2
20
COPD stages
MODERATE
FEV1 / FVC < 70%
50% ≤ FEV1 < 80%
predicted
Stage 2 50 – 80% normal lung function
GOLD Pocket Guide to COPD Diagnosis, Management, and Prevention. A guide for Health Care Professionals Updated 2010. See also www.goldcopd.org 21
COPD treatment considerations
Stage 2
Moderate
• Stage 1 plus
LABA
SVN – SideStream Plus
GOLD Pocket Guide to COPD Diagnosis, Management, and Prevention. A guide for Health Care Professionals Updated 2010. See also www.goldcopd.org 22
COPD treatment considerations
Stage 2
Moderate
• Stage 1 plus
LABA
• Pulmonary rehab
GOLD Pocket Guide to COPD Diagnosis, Management, and Prevention. A guide for Health Care Professionals Updated 2010. See also www.goldcopd.org 23
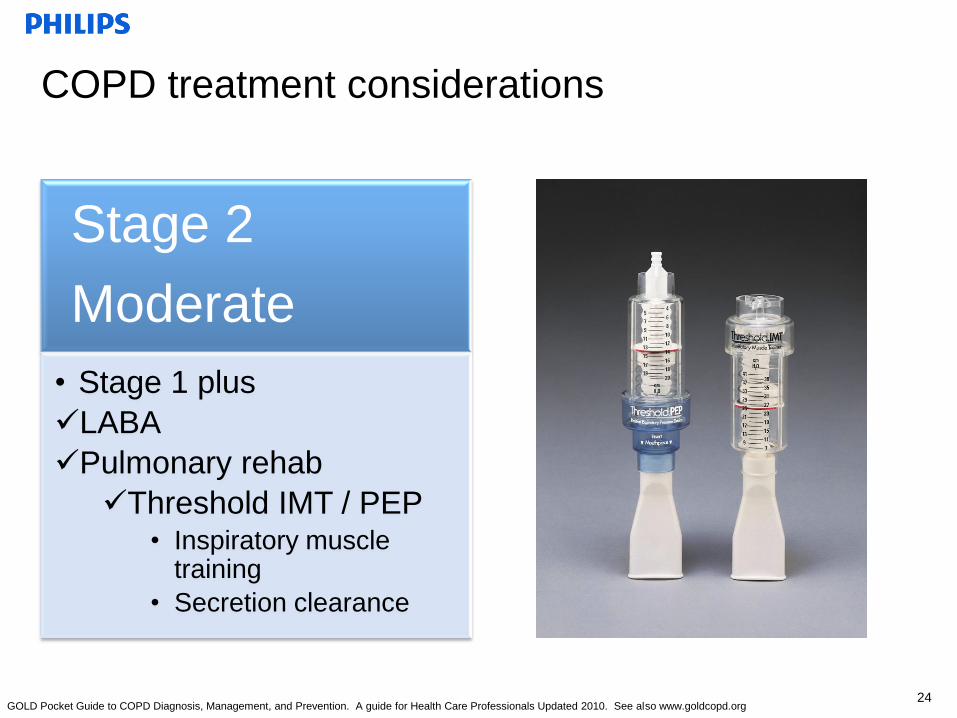
COPD treatment considerations
Stage 2
Moderate
• Stage 1 plus
LABA
Pulmonary rehab
Threshold IMT / PEP • Inspiratory muscle
training
• Secretion clearance
GOLD Pocket Guide to COPD Diagnosis, Management, and Prevention. A guide for Health Care Professionals Updated 2010. See also www.goldcopd.org 24
COPD treatment considerations
Stage 2
Moderate
• Stage 1 plus
LABA
Pulmonary rehab
Supplemental O2
HomeLox / GoLox
GOLD Pocket Guide to COPD Diagnosis, Management, and Prevention. A guide for Health Care Professionals Updated 2010. See also www.goldcopd.org 25
COPD treatment considerations
Stage 2
Moderate
• Stage 1 plus
LABA
Pulmonary rehab
Supplemental O2
UltraFill
GOLD Pocket Guide to COPD Diagnosis, Management, and Prevention. A guide for Health Care Professionals Updated 2010. See also www.goldcopd.org 26

COPD treatment considerations
Stage 2
Moderate
• Stage 1 plus
LABA
Pulmonary rehab
Supplemental O2
EverGo
GOLD Pocket Guide to COPD Diagnosis, Management, and Prevention. A guide for Health Care Professionals Updated 2010. See also www.goldcopd.org 27

COPD treatment considerations
Stage 2
Moderate
• Stage 1 plus
LABA
Pulmonary rehab
Supplemental O2
PAP consideration for overlap – BiPAP S/T
GOLD Pocket Guide to COPD Diagnosis, Management, and Prevention. A guide for Health Care Professionals Updated 2010. See also www.goldcopd.org 28

COPD stages
Severity classified by spirometry
Stage 1 Stage 2
Stage 3
29
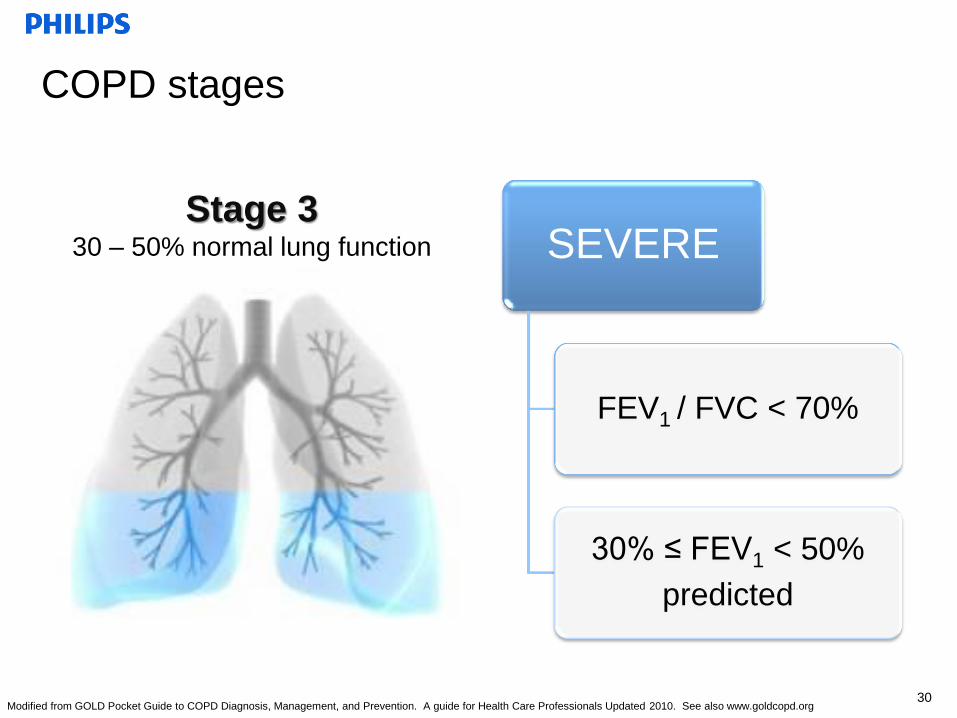
COPD stages
SEVERE
FEV1 / FVC < 70%
30% ≤ FEV1 < 50%
predicted
Stage 3 30 – 50% normal lung function
Modified from GOLD Pocket Guide to COPD Diagnosis, Management, and Prevention. A guide for Health Care Professionals Updated 2010. See also www.goldcopd.org 30
COPD treatment considerations
Stage 3
Severe
• Stage 1 & 2 plus
ICS
GOLD Pocket Guide to COPD Diagnosis, Management, and Prevention. A guide for Health Care Professionals Updated 2010. See also www.goldcopd.org 31

COPD treatment considerations
Stage 3
Severe
• Stage 1 & 2 plus
ICS
NIV – BiPAP AVAPS
GOLD Pocket Guide to COPD Diagnosis, Management, and Prevention. A guide for Health Care Professionals Updated 2010. See also www.goldcopd.org 32

COPD treatment considerations
Stage 3
Severe
• Stage 1 & 2 plus
ICS
NIV
Patient interface
GOLD Pocket Guide to COPD Diagnosis, Management, and Prevention. A guide for Health Care Professionals Updated 2010. See also www.goldcopd.org 33

COPD stages
Severity classified by spirometry
Stage 1 Stage 2
Stage 3 Stage 4
34

COPD stages Severity classified by spirometry
VERY SEVERE
FEV1 / FVC <70%
FEV1 <30% predicted
Stage 4 Less than 30% normal lung function
Modified from GOLD Pocket Guide to COPD Diagnosis, Management, and Prevention. A guide for Health Care Professionals Updated 2010. See also www.goldcopd.org 35
COPD treatment considerations
Stage 4
Very severe
• Stages 1-3 plus
• Surgical options
• LVRS
GOLD Pocket Guide to COPD Diagnosis, Management, and Prevention. A guide for Health Care Professionals Updated 2010. See also www.goldcopd.org 36
COPD treatment considerations
Stage 4
Very severe
• Stages 1-3 plus
• Surgical options
Mechanical Ventilation – Trilogy PIV
http://piv.respironics.com
GOLD Pocket Guide to COPD Diagnosis, Management, and Prevention. A guide for Health Care Professionals Updated 2010. See also www.goldcopd.org 37
COPD treatment considerations
Stage 4
Very severe
• Stages 1-3 plus
• Surgical options
Mechanical Ventilation
Lifeline
24/7
Auto-alert
GOLD Pocket Guide to COPD Diagnosis, Management, and Prevention. A guide for Health Care Professionals Updated 2010. See also www.goldcopd.org 38

Putting it all together
39
I Mild
II Moderate
III Severe
IV Very severe

The Right Fit Oxygen Advisor
39
40

• COPD is preventable and treatable
• Current practices for COPD treatment continue to
evolve
• COPD staging – GOLD revisions were changed in
2013
Conclusion – wrap up
41
CEU certificate
• To obtain your CEU certificate log on to the Philips Respironics’
Partners in Training website at: http://pit.respironics.com
• Log in to the website
• Click on “CEU Online Management System” on the left side
COPD stages Severity classified by spirometry
VERY SEVERE
FEV1 / FVC <70%
FEV1 <30% predicted
or FEV1 <50% predicted plus
chronic respiratory failure
Stage 4 Less than 30% normal lung function
Modified from GOLD Pocket Guide to COPD Diagnosis, Management, and Prevention. A guide for Health Care Professionals Updated 2010. See also www.goldcopd.org 43
COPD treatment considerations
Stage 4
Very severe
• Stages 1-3 plus
• Surgical options
• LVRS (remove 20 to 35% of the poorly functioning lung tissue)
• Airway stents?
GOLD Pocket Guide to COPD Diagnosis, Management, and Prevention. A guide for Health Care Professionals Updated 2010. See also www.goldcopd.org 44

COPD treatment considerations
Stage 4
Very severe
• Tx for Stages 1-3 plus
• Surgical options
Mechanical Ventilation – Trilogy Nocturnal NIV
Secondary mode: MPV
GOLD Pocket Guide to COPD Diagnosis, Management, and Prevention. A guide for Health Care Professionals Updated 2010. See also www.goldcopd.org 45
COPD and Home NIV
Healthcare costs related to COPD
readmissions
46

The costs of readmissions
• In the US, hospital
readmissions for COPD
within 30 days occur in 15-
25% of cases. ¹
• The estimated costs of
these admissions to US
Health Care is over $49
billion dollars. ³
² Plant P, Owen J, Parrott S, Elliott M. Cost effectiveness of ward based non-invasive ventilation for acute exacerbations of COPD; economic analysis of randomized
controlled trial. BMJ 2003; 326 1-5. 3Keenan S. Gregor, Sibbald W. Cook D, Gafni A. Noninvasive positive pressure ventilation in the setting of severe, acute exacerbations of COPD: More effective and
less expensive. Crit Care Med 2000; Vol. 28, No. 6 (2094-2102)
¹ Jencks Sl, Williams M, Coleman E.. Rehospitalizations among Patients in the Medicare Fee –for –Service Program. NE Journal of Med 2009; 360: 1418-28³
47
48
New Medicare focus on readmissions
Pt. Protection and Affordable Care Act
– The Hospital Readmissions Reduction Program (HRRP), part of the
Affordable Care Act, took effect on October 1, 2012
– Medicare targeting the diagnoses accounting for highest numbers of
readmissions
-
RT for Decision Makers March 2013
49
Pt. Protection and Affordable Care Act
•Hospital is accountable for
readmission within 30 days.
- RT for Decision Makers March 2013
50
Medicare is targeting 7 Diagnoses that are
responsible for 30% of all readmissions
2012
• CHF
• Acute MI
• Pneumonia
2015
• COPD
• Angioplasty
• Coronary Artery
Bypass Graft
• Vascular Disease
51
Pt. Protection and Affordable Care Act
•COPD and the other new Dx’s
kicked in Oct. 1 of 2014.
- RT for Decision Makers March 2013

52
Pt. Protection and Affordable Care Act
Hospital payment penalties:
Medicare payment penalties
1% in 2013
2 % in 2014
3% in 2015
- RT for Decision Makers March 2013

Hospital Compare
• CMS website/database:
– Quality of care
– Hospital 30 day readmission rates
– Data for 4000 Medicare certified hospitals across the country
– http://www.medicare.gov/hospitalcompare/search.html
– Number of COPD discharges reported
– How compares with national average
Home Non-Invasive Ventilation
Where we came from and
where we are today

Perceptions of home ventilation
• Past: 24/7 vent dependency, trach/INV only,
complex devices, high risk/cost service.
• Present: Option for patients needing INV or NIV
treatment of neuromuscular, thoracic restrictive
and chronic respiratory failure associated with
chronic obstructive pulmonary disease*.
(*Medicare NCD)
55

Hospital NIV Ventilator
Home NIV Ventilator
• Present: Nocturnal NIV
57

Home NIV Advantages
• Ease of use
• Reduced need for skilled caregivers
• Elimination of tracheostomy-related
complications
• Improved patient comfort
• Allows speech, improved communication
• Lower overall cost of care
58
Goals of Home NIV
• Relieve symptoms
• Reduce work of breathing
• Improve or stabilize gas exchange
• Improve duration and quality of sleep
• Maximize quality of life
• Prolong survival
• Nicholas Hill, Noninvasive Positive Pressure Ventilation: Principles and
Applications
59
60
Diagnoses that may be appropriate for Home NIV?
• Muscular Dystrophies
• ALS
• Higher Spinal Cord Injuries
• Other myopathies: Acid maltase deficiency, polymyositis,
mitochondrial disorders.
• Neurological disorders: Spinal muscular atrophies (SMA l,ll,lll)
Neuropathies: Guillain-Barre syndrome, Multiple Sclerosis
• Skeletal pathologies such as kyphoscoliosis
• COPD with respiratory insufficiency/chronic respiratory failure
COPD and Home NIV
Clinical References
(pubmed.gov)
61
Barnes Healthcare Non-Invasive Management Program
• The Barnes Healthcare Services (AL, FL, GA) Non-Invasive Ventilation
Management Program.
• Published June 2015 in Journal of Clinical Sleep Medicine.
”Retrospective Assessment of Home Ventilation to Reduce
Rehospitalization in Chronic Obstructive Pulmonary Disease. 663-670. “
Steven Coughlin, PhD1; Wei E. Liang, PhD2; Sairam Parthasarathy, MD3
• Retrospective study of a QI program preformed at a single center.
Intervention included nocturnal NIV with AVAPS-AE. Medication
reconciliation by a pharmacist, adequate provision of O2 and ongoing
RT follow-up.
Barnes COPD Home Management data presented at the
AARC (Published in Journal of Clinical Sleep)
• 397 COPD Chronic Respiratory Failure patients 1 year pre home NIV
and 1 year post
• Inclusion criteria included 2 (or more) admissions within the previous
year due to acute COPD exacerbations . Trilogy with AVAPS-AE mode
used on all patients in 1 yr post
• Tidal Volume based on Ideal Body Weight with Min and Max pressures
to meet patients demands/needs
• Only 9 of 397 required readmission for COPD exacerbation the year
following initiating Trilogy/AVAPS-AE vs 100% the year prior.
• One year survival rate increased to 82%

64
High-Intensity non-invasive positive pressure ventilation
for stable hypercapnic COPD
Wolfram Windisch et al. International Journal of Med Sciences, 2009; 6 (2)
72-76
• Describe outcome of high-intensity NIV aimed at decreasing
PaCO2 as an alternative to conventional NIV with lower
settings in stable hypercapnic COPD patients.
• High Intensity = Ave I Pressure is 28 cm H20
• Low Intensity = IPAP 12 to 18cm H20

High-Intensity non-invasive positive pressure ventilation
for stable hypercapnic COPD
Wolfram Windisch et al. International Journal of Med Sciences, 2009; 6 (2)
72-76
• Physiological parameters, exacerbation rates and long-term
survival were assessed in 73 COPD patients (mean FEV1
30 % predicted) who were placed on high-intensity NIV due
to chronic hypercapnic respiratory failure between March
1997 and May 2006.
• Results: Controlled NIV with RR of 21 breaths/min and
positive airway pressures of 28 (+5/-5) cm H20 led to
significant improvements in ABG’s and lung function
65

High-Intensity non-invasive positive pressure ventilation
for stable hypercapnic COPD
After two months of NIV:
• TLC remained unchanged
• FVC on average went from 49% to 55% of predicted
• FEV1 30 to 35%
PC02 51 to 47
Wolfram Windisch et al. International Journal of Med
Sciences, 2009; 6 (2) 72-76
66
High-Intensity non-invasive positive pressure ventilation
for stable hypercapnic COPD
Wolfram Windisch et al. International Journal of Med Sciences, 2009; 6 (2)
72-76
• Readmissions:
67
Only 16 of the 73 patients (22%)
required hospitalization due to a
COPD exacerbation during the first
year.
Decrease in EMG activity with Long Term Ventilation in
COPD
• Respiratory Muscle strength
– Electrical activity of Respiratory Muscles. Three Respiratory
Muscles,
– Intercostal
– Diaghram
– Scalenes
– Chronic NIV may be beneficial for the electrical activity of the
respiratory muscles
Deiverman et al. ERS Abstract in 2009.
68
Rationale for NIV in COPD Treatment
Improved Sleep
• Improved Sleep (Total time of sleep, efficiency of sleep
– Patients had COPD and were hypercapnic. Patients were using
either O2 or O2 and NIV during the night.
– TST % 202 – 260 min w O2, 339 min with O2 and NIV
,
Efficiency % Total number of hours asleep as opposed to total
number of hours in bed. Average 50%, up to 70% with O2 and
80% with O2 and NIV
– Awake % 40, 30 with O2 20% with O2 and NIV
Meecham Jones. Et al 1995 AJRCCM
69

Rationale – Improved Ventilation
• Improved Ventilation
• Nocturnal NIV in addition to Rehab in hypercapnic pateints with
COPD (2008)
– Author looked at tidal volume, minute volume and RR
– Found significant Increases in ventilation during the
daytime when patients are using NIV at night.
Deiverman et al.2008
70

Long-term home noninvasive mechanical ventilation
increases systemic inflammatory response in chronic
obstructive pulmonary disease:
RESULTS:
• Ninety-three patients were included (48 NIV, 45 oxygen), with analogous
baseline features. Sputum analysis showed similar HNP, IL-6, IL-10, and TNF-
alpha levels (P > 0.5). Conversely, NIV group exhibited higher HNP and IL-6
systemic levels (P < 0.001) and lower IL-10 concentrations (P < 0.001).
Subjects undergoing NIV had a significant reduction of rehospitalizations
during follow-up compared to oxygen group (P = 0.005). These findings were
confirmed after propensity matching and pH stratification.
Paone G, et al Abstract 2014 71
Long-term home NIV increases systemic inflammatory
response in chronic obstructive pulmonary disease
RESULTS:
These findings challenge prior paradigms based on the assumption that
pulmonary inflammation is per se detrimental.
NIV beneficial impact on lung mechanics may overcome the potential
unfavorable effects of an increased inflammatory state.
Paone G, et al Abstract 2014
72

Rational for NIV
• Respiratory Muscle strength
– . Decrease in EMG activity with Long Term Ventilation in COPD
– Electrical activity of Respiratory Muscles. Three Respiratory
Muscles,
– Intercostal
– Diaghram
– Scalenes
– Chronic NIV may be beneficial for the electrical activity of the
respiratory muscles
Deiverman et al. ERS Abstract in 2009
73
How may home NIV help the COPD patient?
• Rest and unload the respiratory muscles
• Improved sleep efficiency
• Improvements in PFTs and ventilation,
• Improvements in inflammation response
• Reduction in readmissions for chronic
respiratory failure

75
• AVAPS-AE Mode
– Auto backup rate
– Adjustable AVAPS rate
Mouthpiece Ventilation
Pressure Support up to 50 cmH2O
New NIV updates and expanded versatility
AVAPS Review
• AVAPS acts primarily as a bi-level pressure support device but is able
to provide a constant tidal volume with the AVAPS feature enabled
– Can be used with S, S/T, PC or T modes
• Automatically adjusts the pressure support level to maintain a
consistent tidal volume
– IPAP will automatically increase or decrease to maintain set tidal
volume
76
• Automatically titrates pressure support
– Changes in body position
– Sleep stage
– Changes in respiratory mechanics
• Delivers average tidal volume
– Within the night
– Long-term progression
• AVAPS produces results comparable to sleep lab titration of PS1
– CO2 reduction
– Health-related quality of life
– Sleep quality
1Murphy, PBThorax thoraxjnl-2011-201081: Published Online First: 1 March 2012 doi:10.1136/thoraxjnl-2011-201081
AVAPS: proven effective
77

Performance Capabilities
AVAPS
With AVAPS
78
AVAPS- AE
AVAPS-AE is a auto-titration mode of noninvasive ventilation designed to
better treat respiratory insufficiency patients (OHS, COPD and NMD) in
the hospital and homecare environments
Achieving a targeted volume is now completely automatic
• Proven performance of AVAPS
• Auto EPAP
• Auto backup rate
• Can be used together or in various combinations
79

AVAPS-AE
Auto EPAP maintains patent upper airway
at a comfortable pressure
• Auto adjusting EPAP to meet changing patient needs
• Maintains a patent airway
80

Current PRI Auto EPAP/CPAP
Flatness Roundness Peak Shape
AVAPS-AE
Flo
w
Pre
ssu
re
Forced oscillation technique (FOT) at 5 Hz, 1
cm amplitude during EPAP
Comparison of Auto EPAP methods
81

AVAPS-AE
Auto backup rate provides
comfortable assistance when needed
• Auto backup rate is near resting rate
• No manual adjustments
(auto-default setting)
82
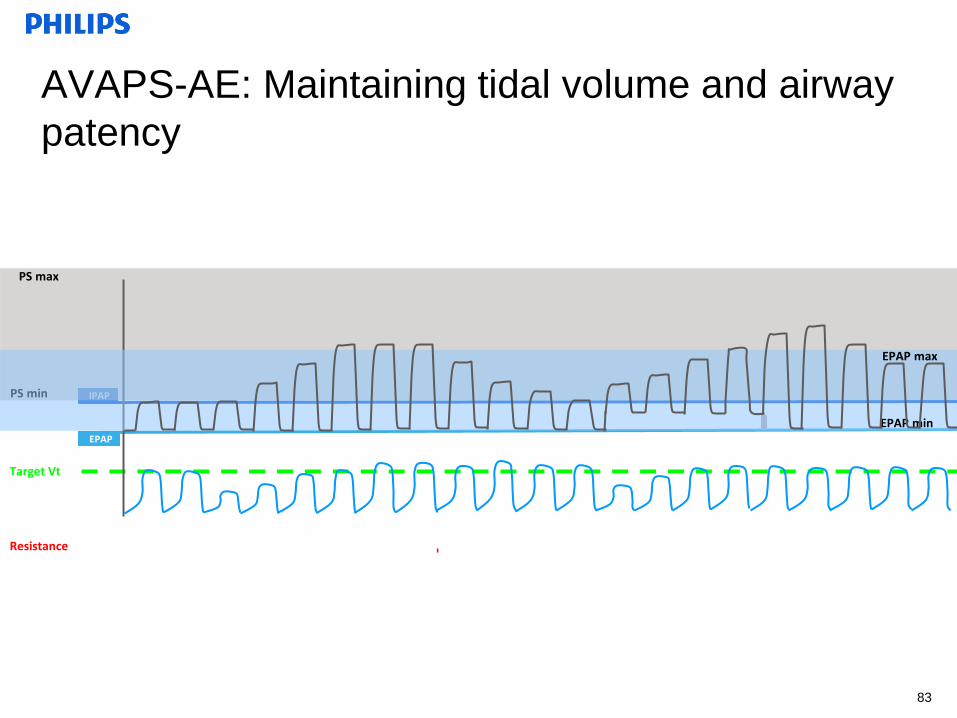
EPAP
Target Vt
IPAP PS min
PS max
AVAPS-AE: Maintaining tidal volume and airway
patency
EPAP min
EPAP max
Resistance
83
AVAPS-AE: Auto EPAP
• Auto EPAP provides airway patency
– Designed for NIV use only
– Patient benefit: lower, more comfortable
EPAP pressure
• AVAPS-AE and patient overlap
– 29% to 40% of COPD patients have OSA1
– 90% of OHS patients have OSA2
• AVAPS-AE: 1st NIV therapy with Auto EPAP
designed for respiratory insufficiency and
respiratory failure patients
1Jelic International Journal of COPD 2008:3(2)269-275 2Mokhlesi. Chest 2007:131;1624-1626
84

Expanding Ventilatory Support
Mouthpiece ventilation (MPV)
MPV is a form of volume ventilation whereby the patient’s normal state is
disconnected from the ventilator and the patient initiates a breath, as
needed, through an oral interface.
85

Kiss Trigger and MPV Support System
• A new ‘kiss’ trigger with signal flow technology detects when the patient
engages and disengages from the mouthpiece to deliver on-demand
ventilation
• This feature combines with a mouthpiece ventilation (MPV) support
system to enhance ease of use
86

BiPAP vs Trilogy NIV Vent for Respiratory Failure/COPD
(General Overview – See CMS NCD/LCD’s)
Trilogy NIV Vent (E0464)
• Chronic Respiratory Failure
• NCD currently (no LCD)
• Physician documentation of Chronic
Respiratory Failure and why an NIV
Vent is being ordered for patient.
• Documentation considerations:
May include PCO2 and/or PFT’s (Stage
4 COPD)
Readmissions for Resp Failure
Higher pressures (up to 40cmH20)
Auto Pressure Support and EPAP
Mouthpiece Ventilation available
AVAPS-AE Mode
Protection from breath-stacking
Auto Rate
More time to exhale
BiPAP (E0470/E0471)
May be adequate if device meets
patients needs
• Lower pressures are adequate
• Patient meets RAD Guidelines:
1, ABG PaCO2, done while awake and breathing the
patient’s usual prescribed Fi02 ≥ 52mmhg
and
2. Sleep oximetry SaO2 less than or equal to 88% for at
least five continuous minutes, done while breathing oxygen
at 2 LPM or the patient’s usual FIO2 (whichever is higher)
and
3. Prior to initiating therapy, Obstructive Sleep Apnea (OSA)
and treatment with a continuous positive airway pressure
device (CPAP) has been considered and ruled out

88
Questions???