Embed Size (px)
Citation preview

THE DELIVERY OF HEALTH SERVICES IN KINONDONI
MUNICIPAL: CIVIL SERVANTS’ PERCEPTIONS
By
Felician Zephrine Mufumu
Dissertation Submitted to Mzumbe University – Dar es Salaam Campus College
for the Requirements of the award of a Master Degree in Public Administration
of Mzumbe University
2013
i
CERTIFICATION
We, the undersigned, certify that we have read and hereby recommend for acceptance
by the Mzumbe University, a dissertation entitled The Delivery of Health Services in
Kinondoni Municipal: Civil Servants’ Perceptions, in partial fulfillment of the
requirements of award of the Degree of Master of Public Administration (MPA) of
Mzumbe University.
____________________________
Major Supervisor
____________________________
Internal Examiner
Accepted for the Board of
_________________________________________________________________
DEAN/DIRECTOR, FACULTY/DIRECTORATE, SCHOOL BOARD
ii
DECLARATION AND COPYRIGHT
I Felician Zephrine Mufumu, do hereby declare to the Faculty of Public
Administration of Mzumbe University – Dar es Salaam Campus College, Tanzania,
that this research is my own work and has not been submitted for Master Degree Award
at any other university or institution of higher learning.
Signature____________________________
Date ________________________________
©
All rights reserved. No part of this research may be reproduced in any form or by any
means, electronic or mechanical, including photocopying, recording or any
information storage or retrieval system without prior permission from the author or
Mzumbe University.
iii
ACKNOWLEGMENT
I would like to thank the Municipal Medical Officer of Kinondoni municipal for
granting me permission to conduct my study in the municipal health facilities. Special
thanks should also go to Medical Officers in-charge and staff of Lugalo hospital,
Mwananyamala hospital, Sinza hospital, Magomeni health centre and Tandale
dispensary for their great contributions.
iv
DEDICATION
I dedicate this work to my lovely wife Captain Jamila Nyanza and my daughter Stella
who really missed my love during the busy times of my studies.
I also dedicate this work to my beloved parents the late DR. Mufumu and Mrs.
Mufumu for their good parental care, for giving me good foundation in my education
also for giving me an opportunity to make a difference in their lives.
v
ABBREVIATIONS
ADDO - Accredited Drug Distribution Outlet
AIDS - Acquired Immuno – Deficiency Syndrome
CCM - Chama Cha Mapinduzi
CHF - Community Health Fund
FBO - Faith Based Organization
HIV - Human Immuno Deficiency Virus
HSR - Health Sector Reform
ILO - International Labour Organization
IMF - International Monetary Fund
MCHA - Maternal and Child Health Aides
MDG - Millennium Development Goal
MOH - Ministry of Health
MOHSW - Ministry of Health and Social Welfare
NGO - Non Governmental Organization
NHI - National Health Insurance
NHIC - National Health Insurance Corporation
NHIF - National Health Insurance Fund
NIC - National Insurance Corporation
NIMR - National Institute of Medical Research
PMO-LAG - Prime Minister Office, Regional Administration and Local
Government
RHMT - Regional Health Management Team
SAP - Structural Adjustment Program
SSA - Sub-Saharan Africa
TDV - Tanzania Development Vision
WB - World Bank
WHO - World Health Organization
vi
ABSTRACT
The study was set out to assess health services delivery as perceived by civil servants
in Kinondoni municipal health facilities using Lugalo, Mwananyamala, sinza,
Magomeni and Tandale with a particular interest to clients who are member of NHIF.
The specific objectives were to assess the perception of civil servants on health care
services provided in Kinondoni municipal health facilities, to assess the contribution
of health insurance towards the improvement of health care services and to elicit civil
servants opinions on how to improve health care services provided in Kinondoni
municipal health facilities.
The findings of the study revealed that respondents were satisfied with health care
services they had received in Kinondoni municipal health facilities, particularly on
consultation time, information sharing and client – provider interaction, the cleanliness
of the facilities surroundings and physical state of the facilities buildings.
Also the findings of the study revealed that respondents perceived shortage of
medicines, medical supplies and equipments as a problem in all the municipal health
facilities under the study. The findings also revealed lack of privacy, but generally it
was concluded that the health care services delivered in Kinondoni municipal health
facilities was satisfactory.
In order to improve the delivery of health care services in Kinondoni municipal health
facilities, respondents suggested that, availability of medicines, medical supplies and
equipments should be improved. Also, health care providers should be well trained
and adequate.
TABLE OF CONTENTS

vii
Pages
CERTIFICATION ...................................................................................................... i DECLARATION ........................................................................................................ ii COPYRIGHT ................................................................ Error! Bookmark not defined.
ACKNOWLEGMENT ............................................................................................. iii DEDICATION ........................................................................................................... iv ABBREVIATIONS .................................................................................................... v ABSTRACT ............................................................................................................... vi
TABLE OF CONTENTS .......................................................................................... vi LIST OF TABLES .................................................................................................... ix
LIST OF FIGURES ................................................................................................ viii
LIST OF APPENDICES .......................................................................................... ix
CHAPTER ONE ........................................................................................................ 1 INTRODUCTION ...................................................................................................... 1
1.1 Background to the Problem ....................................................................... 3
1.2 Statement of the Problem .......................................................................... 7 1.3 Research Questions ................................................................................... 9
1.4 Objective of the Study ............................................................................... 9 1.4.1 General Objective ...................................................................................... 9
1.5 Specific Objectives .................................................................................. 10 1.6 Significance of the Study ........................................................................ 10
1.7 Area and Scope of the Study ................................................................... 10 1.8 Limitations of the Study .......................................................................... 10 1.9 De – limitations ....................................................................................... 11
CHAPTER TWO ..................................................................................................... 11
LITERATURE REVIEW ........................................................................................ 11 2.1 Introduction ............................................................................................. 12 2.2 Theoretical Perspectives .......................................................................... 14
2.2.1 Market Failure ......................................................................................... 14
2.2.2 Government Failure................................................................................. 15
2.3 Quality of Health Care Services .............................................................. 15 2.4 National Health Policy ............................................................................ 21 2.5 Health Delivery System in Tanzania ....................................................... 22
2.6 Health Sector Reforms ............................................................................ 26 2.7 Health for All (Universal Coverage) ....................................................... 29
2.8 Health Expenditure and Financing in Developing Countries.................. 30 2.9 Health Insurance Schemes ...................................................................... 31 2.10 Health Financing in Tanzania ................................................................. 32
2.11 Effects of Costs on Health Seeking Behavior ......................................... 34
CHAPTER THREE ................................................................................................. 34 RESEARCH METHODOLOGY ........................................................................... 34
3.1 Introduction ............................................................................................. 34
viii
3.2 Study Area ............................................................................................... 35 3.3 Study Design ........................................................................................... 35
3.4 Study Population ..................................................................................... 35 3.5 Sample and Sampling Technique ............................................................ 36 3.6 Data Collection Instruments .................................................................... 37 3.6.1 Questionnaire .......................................................................................... 37 3.6.2 Interview.................................................................................................. 37
3.6.3 Observation ............................................................................................. 38 3.7 Data Analysis .......................................................................................... 38
CHAPTER FOUR .................................................................................................... 39 PRESENTATION OF FINDINGS .............................. Error! Bookmark not defined.
4.1 Introduction ............................................................................................. 40
4.2 Respondent Interview .............................................................................. 40
4.3 Facility Checklist..................................................................................... 48
4.3.1 Services Offered ...................................................................................... 48
4.3.2 State of Physical Structures ..................................................................... 49
4.3.3 Environmental Cleanliness ...................................................................... 49
CHAPTER FIVE ...................................................................................................... 50
DISCUSSION OF THE FINDINGS ....................................................................... 50 5.1 Introduction ............................................................................................. 50 5.2 Provider – Client Interaction ................................................................... 51
5.3 Availability of Medicines and Medical Supplies .................................... 52 5.4 Waiting Time........................................................................................... 53
5.5 Physical State of Buildings ..................................................................... 54 5.6 Patients’ Satisfaction or Dissatisfaction with Health Services Delivery . 54 5.7 Market Failure ......................................................................................... 57
5.8 Government Failure................................................................................. 58
CHAPTER SIX ........................................................................................................ 59 SUMMARY, CONCLUSIONS AND RECOMMENDATIONS ......................... 59
6.1 Introduction ............................................................................................. 59 6.2 Summary ................................................................................................. 59
6.3 Conclusion ............................................................................................... 60 6.4 Recommendations ................................................................................... 61 6.4.1 Specific Recommendations ..................................................................... 61 6.4.2 General Recommendations ..................................................................... 62 6.4.3 Areas for Further Researches .................................................................. 62
REFERENCES ......................................................................................................... 62
APPENDICES .......................................................................................................... 68
LIST OF TABLES
Pages
ix
Table 1.1: Health Facilities Registered by the Fund Up to March 2012 ............... 7
Table 2.1: Dimensions of Quality Health Service…………………………..….17
Table 2.2: Conceptual Framework for Assessing Health Service Quality……..19
Table 2.3: Countries that have Achieved Universal Coverage in the World 30
Table 2.4: Implementation of Universal Coverage in African countries ............ 30
Table 4.1: Socio-Demographic Characteristics of Respondents Interviewed ..... 40
Table 4.2: Reasons for Choice of Health Facility ............................................... 41
Table 4.3: Mode of Transport Used By Respondents to Attend at the Health
Facilities ............................................................................................. 42
Table 4.4: Respondents’ Perception on Drug Availability at the Health Facility 42
Table 4.5: Respondents’ Perception on Health Care Providers’ Attitude ........... 43
Table 4.6: Respondents’ Opinions on Adequacy of Consultation Time ............. 43
Table 4.7: Respondents Given Adequate Explanations of their Health Problems
............................................................................................................ 44
Table 4.8: Respondents Reported to have Been Counseled ................................ 44
Table 4.9: Respondents Given Instructions on How to Use Prescribed Medicines
............................................................................................................ 45
Table 4.10: Respondents Examined Physically and Privacy Maintained ............. 45
Table 4.11: Respondents’ Perception on Physical State of the Buildings ............. 46
Table 4.12: Respondents’ Perception on Total Time to Get Health Care Services
............................................................................................................ 46
Table 4.13: Respondents’ Satisfaction with the Quality of Health Care Services 46
Table 4.14: Respondents’ Reasons for Satisfaction with Quality of Health Services
............................................................................................................ 47
Table 4.15: Respondents’ Reasons for Dissatisfaction with the Quality of Services
............................................................................................................ 47
Table 4.16: Respondents’ Recommendations on Improving the Health Services 48
Table 4.17: Various Services Provided in Municipal Health Facilities ................ 49
LIST OF FIGURES
Figure 2: 1 Figure 2.1: Health Quality Dimensions Relationship......................... 18

x
Figure 2.2: The Health System in Tanzania ............................................................... 24
Figure 2.3: Ministries, Departments and Agencies Most Involved in Health
Sector and their Responsibilities …………………………………………………..26
LIST OF APPENDICES
Pages

xi
Appendix 1: The Informed Concert ........................................................................ 68
Appendix 2: Client Questionnaire (English Version) ............................................. 70
Appendix 3: Clients Questionnaire (Swahili Version) ............................................ 81
Appendix 4: Facility Check List to Assess Health Services Delivered .................. 91
1
CHAPTER ONE
INTRODUCTION
Since independence in 1961, the Government of Tanzania has consistently focused her
development strategies on combating ignorance, diseases and poverty. The investment
in health services is recognized as a potential tool in fighting diseases and at the same
time improving the quality of lives of the majority of the people.
For more than two decades Tanzania has been one party state. One of the major
directives of the ruling party was that the health services should be available to all
Tanzanians. To implement these directives the government made health provision free
of charge. It further expanded health services delivery units by building dispensaries
and health centers in rural areas where the majority of the population lived. The
government remained the main provider of health services in the country and the sole
source of health financing. Her effort in health services provision were supplemented
to the not for profit NGO’s. Development for the private-for-profit sector was
discouraged (MOH, 2001).
However, the problems of implementation of vertical programs, inappropriate
utilization of manpower, improperly functioning referral system, shortage of staff,
inadequate medical equipments and other medical supplies made the government to
change its role from that of main provider to facilitator of health services and adopt
use fee as an alternative health financing mechanism (MOH, 2000).
User fee (health insurance) is not a new phenomenon in most of the third world
countries. It has been practiced by private health facilities and Non Governmental
Organizations for many years ago (Shaw, 1995).
Health care services were previously provided free of charge in most of developing
countries especially in Africa and other third world countries. The need to provide for,
accessible, equitable, effective and sustainable health services was a political decision
2
made by most of African leaders soon after independence of their countries in early
1960s. However, due to economic crisis which was facing the world in early 1980s the
WB and IMF introduced Structural Adjustment Programs. SAP’s were accompanied
with a number of reforms, HSR was one of them. Health insurance was an important
aspect of HSR. It is a part of wide perspective of financial reforms. Together with other
reforms in the health sector, it is intended to create a sustainable, purposeful and
fundamental change to address significant strategic dimension in health system
(Berman, 1995).
The primary purpose of health insurance is to generate revenue. In public sectors fees
are usually introduced to supplement public funds when those sectors fails to keep up
with the cost of providing services and expanding services to meet increasing demand.
Although the primary purpose is to generate revenue but the total amount of revenue
generated is unlikely to be sufficient to meet the growing need and demand for high
quality health care services (Newbrander and Sacca, 1996).
In Tanzania, the concept of NHI for employees in the formal sector evolved from a
number of concerns that have risen regarding the financial sustainability of the health
sector. The concerns were based on observed decline in the amount of resources
flowing into the sector, of which has resulted in decrease in the availability and quality
of health services provided. Between 1990 and 1992 the MOH carried out a health
financing study which recommended user fee in the government health facilities and
development of NHI for employees in the formal sector.
The introduction of alternative health financing mechanisms such as user fees,
Community Health Fund and National Health Insurance Fund was viewed as a means
of generating additional revenue for the health sector, improving quality of health
services, as well as promoting equity, accessibility, and efficiency in the use of health
services in Tanzania (MOH, 1997).
3
The government in July 1993 adopted the policy of cost sharing in government health
facilities. This policy was preceded by pilot studies which indicated that the
communities were willing to pay by anticipating that drugs will be available with well
maintained health facility infrastructures and improved doctor – patient relationship
and availability of other medical supplies (Mujinja and Mabara, 1992). That decision
was a major departure to the previous policy of providing free health care services at
the point of health delivery.
In Kinondoni municipal, the introduction of health insurance for civil servants started
in October 2001. Before the introduction of health insurance, health services were
provided by cost sharing and in some places were given free of charge. However, the
health care services provided were of poor quality due to lack of medicine and other
medical supplies, inadequate staff and poor health facility infrastructures.
This study aimed at determining how can health services delivered in Kinondoni
municipal health facilities (as perceived by civil servants) were improved.
1.1 Background to the Problem
The delivery of health services in Tanganyika then Tanzania began during the German
colonialism (1888 - 1891) along the coast areas of Tanga, Pangani, Bagamoyo, Dar es
Salaam and Kilwa (Clyde 1962). Further expansion of the services was limited during
this time because much of the country had not been explored. In developing health
services in these areas, the Germans were mainly guided by economic and
administrative factors.
When the British colonialists came in the period between 1916 – 1920 they devoted to
the reconstruction and re-establishment of civil medical services upon which the
country current medical services are based. Since then, there have been minimal
reforms to Tanzania Mainland health services. Save for the Titmus Report (1966), the
Arusha Declaration (1967) which emphasized on health services delivery in rural areas
and the Acts on Decentralization (1972 and 1982) that gave decision making autonomy
to the districts.
4
The primary health care service forms the basement of pyramidal structure of health
care services. It is made up of a number dispensaries, health centers and district
hospitals. Currently, the health facilities for both public and private include 4679
dispensaries, 481 health centers and 219 hospitals distributed throughout the country.
The dispensaries and health centers are planned to service an average population of
10,000 and 50,000 respectively (MOH, 2007).
However, with increasing population and slow pace of construction of primary health
care facilities, the average population served by these facilities is more than the
planned population. The problem as stated earlier is compounded with shortage of
staff, inadequate medical equipments and other supplies. To meet all these challenges,
the government has decided to adopt user fee in its health facilities as an alternative
health financing mechanism (MOH, 1996).
Human beings irrespective of their income, races, nationality or level of social
economic developments, they all need protection against ill-health, related health
shocks and costs of illness. Tanzania realized this and it concurred with the idea:
“Nothing in the history of a social policy that has transformed the life of an ordinary
man than an assurance that in the event of ill-health, he will not turn into destitute”
(Jenks, 1971), thus it established NHI.
Since 1883, when the first Social Health Insurance Scheme in the world (the Bismarck
model) was introduced in Germany, the world witnessed a notable developments and
reforms aimed at achieving the goal of health for all. Globalization, the MDGs and the
need by the International Community to reduce poverty are therefore international
intervention strategies geared towards establishing systems which ensure every citizen
of the community is protected against shocks and causes of ill-health.
Some of the international declarations, Regional initiatives or National policies that
have been adopted or implemented are:

5
(i) ILO (1952) that minimum standards on coverage required to be extended to the
society that includes medical care.
(ii) The Arusha Declaration (1967) that provides for the right of social protection.
(iii) WHO (1978) health for all initiative, the Alma-Ata Declaration.
(iv) The Health Policy (1990) aimed at equitable and accessible health care services
by all.
(v) The Social Security Policy (2003) aimed at social protection and harmonization
mainly of the pension sector.
(vi) WB (2005) Integrating Health Insurance in social protection.
Immediately after independence the government of Tanzania started to provide free
health care services to its citizens aimed at attaining equity in health care provision
(MOH, 1994). However, the economic crisis in the mid 1970s, increased population
growth, change in disease pattern and increased cost of disease management, reduced
the government ability to continue to provide free health services resulting into
inadequate funding of public health facilities at all levels (MOH, 1996). Inadequate
funding of public health sector led to poor morale of health staffs due to low wages,
shortage of medicines and other medical supplies and deterioration of the health
infrastructure (MOH, 1994).
User fees were the first alternative health financing mechanism adopted in Tanzania
and it was introduced in 1993. Its implementation was done in phases, starting with
referral hospitals and regional hospitals followed by district hospitals, then health
centers and finally dispensaries (MOH, 1999). Introduction of user fees in the public
health facilities provided a big challenge to the majority of Tanzanians because there
were no longer free medical services offered except for pregnant women and under
five years children. This created the demand for introduction of health insurance
schemes for civil servants in the public sectors (MOH, 1997).
In Tanzania, the insurance industry has existed under the monopoly of the NIC. There
has been no formal system of health insurance except for some form of pre-paid plans
6
or self insurance. Through these arrangements, the employers entered into contracts
with private health facilities to provide services for their employees. In certain cases,
organizations ran their own health facilities or clinics.
The NHIF which is a contributory Social Health Insurance Scheme was established
under NHI Act No 8 of 1999. Initially, it was established in order to oversee the system
of service provisional for central government employees only. But in the year 2002,
the law was amended to include other employees in the entire public service. While
the law to establish the fund was enacted in 1999, the fund commenced its operations
on the 1st July 2001 and beneficiaries started to access medical services in October
2001.
The health scheme covers public service employees in the central government, local
government and executive government agencies. The scheme is compulsory in nature
and the contribution rate is 6% of which the employee contributes 3% and the
employer contributes 3%. It covers six people in the family. The beneficiaries include
the principal member, the spouse, four children or legal dependants.
The fund has opened offices in 22 regions of the mainland Tanzania (Kinondoni
municipal, Ilala municipal, Temeke municipal, Mwanza, Mara, Tabora, Kigoma,
Dodoma, Kilimanjaro, Arusha, Tanga, Morogoro, Iringa, Ruvuma, Mbeya, Rukwa,
Mtwara, Kagera, Manyara, Singida, Lindi, Pwani, Shinyanga) and 1 office in Zanzibar.
Up to 31st March, 2012 the fund has been able to offer health care services to 18.2%
of the whole population. This is equal to 6,269,163 members of NHIF and CHF. Also
the fund has registered 5,381 health facilities in the whole country. This is equal to
68% of 7,966 health facilities present in the country. Among them, 4,319 (80%) are
owned by the government, 625 (12%) are owned by religious organizations and 437
(8%) are owned by private sectors (NHIF, 2012).
The government through its party manifesto (CCM, 2010) ordered the fund to increase
the number of members up to 30% of the whole population by the year 2015 in order
to provide health services for all (table 1).
7
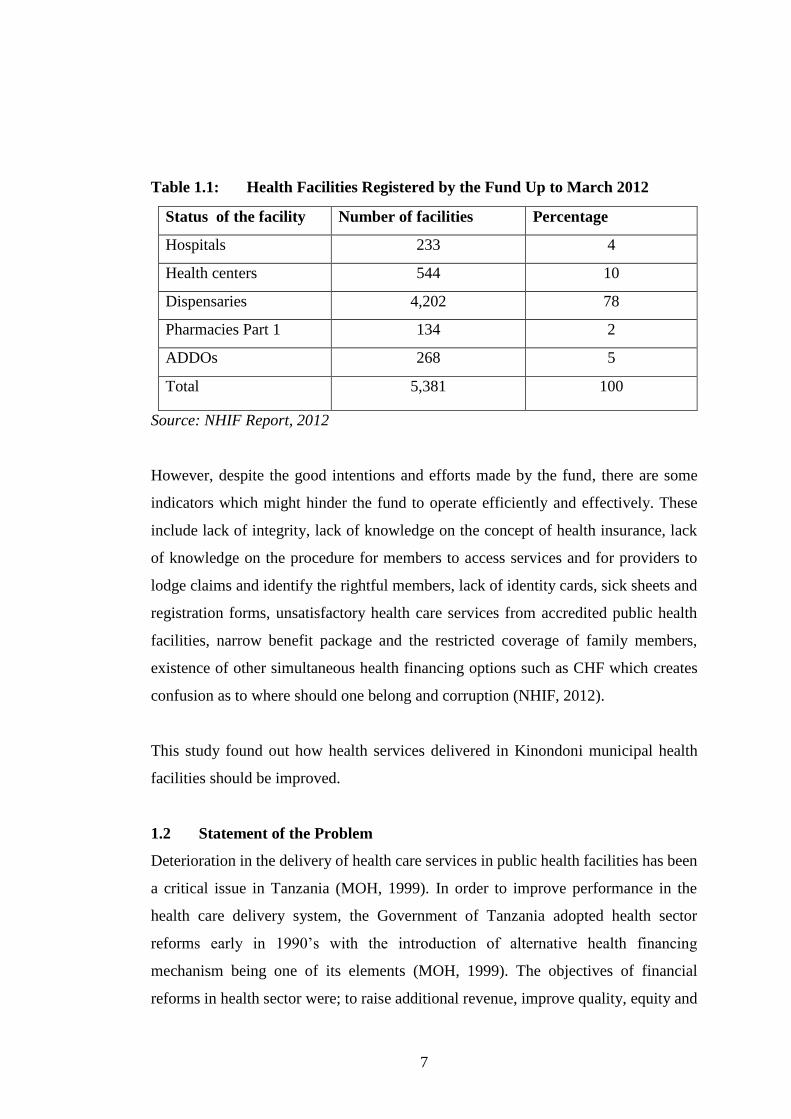
Table 1.1: Health Facilities Registered by the Fund Up to March 2012
Source: NHIF Report, 2012
However, despite the good intentions and efforts made by the fund, there are some
indicators which might hinder the fund to operate efficiently and effectively. These
include lack of integrity, lack of knowledge on the concept of health insurance, lack
of knowledge on the procedure for members to access services and for providers to
lodge claims and identify the rightful members, lack of identity cards, sick sheets and
registration forms, unsatisfactory health care services from accredited public health
facilities, narrow benefit package and the restricted coverage of family members,
existence of other simultaneous health financing options such as CHF which creates
confusion as to where should one belong and corruption (NHIF, 2012).
This study found out how health services delivered in Kinondoni municipal health
facilities should be improved.
1.2 Statement of the Problem
Deterioration in the delivery of health care services in public health facilities has been
a critical issue in Tanzania (MOH, 1999). In order to improve performance in the
health care delivery system, the Government of Tanzania adopted health sector
reforms early in 1990’s with the introduction of alternative health financing
mechanism being one of its elements (MOH, 1999). The objectives of financial
reforms in health sector were; to raise additional revenue, improve quality, equity and
Status of the facility Number of facilities Percentage
Hospitals 233 4
Health centers 544 10
Dispensaries 4,202 78
Pharmacies Part 1 134 2
ADDOs 268 5
Total 5,381 100

8
accessibility to health care services and to promote the efficient use of public health
care facilities (MOH, 1994).
Health care services were previously provided free of charge in Tanzania. The
Government was the main provider of health services in the country and the sole source
of health financing. The government expanded health services delivery units by
building dispensaries and health centers in rural areas where the majority of the
population live. However, the problems of implementation of vertical programs,
inappropriate utilization of manpower, improperly functioning referral system,
shortage of staff and inadequate medicines and other medical supplies made the
government to change its role from that of main provider to facilitator of health
services and adopt user fee as alternative health financing mechanism (MOH, 1997).
The introduction of user fee (health insurance) was adopted to overcome the problems
associated with the previous free of charge health care services. The free of charge
health care system made the provision of health services poor because it did not
facilitate effectively and efficiently the flow of resources in the sector, which resulted
in decrease in the availability and quality of health services provided (MOH, 1994).
Literature from Tanzania and other developing countries which were providing free of
charge health care services showed that those services were of poor quality (Mwabu
and Wang’ombe, 1995).
As Norm and Weber (1994) noted, in most of developing countries like Tanzania, the
physical resources are inadequate, inequitably distributed and are of poor quality, staff
in health infrastructures are poorly trained with inadequate resources. In the right
condition, however, insurance may provide equitable method of financing health
delivery system than out of pocket payments. Similarly, MOH (1994) emphasizes that
the introduction of health insurance in the formal sector in Tanzania will improve the
quality, equity, efficiency, effectiveness and accessibility of medical services.
The health services delivery system in Tanzania consists of a network of facilities
starting from dispensary to health center through district and regional hospitals to the
9
referral hospitals. Unfortunately, this system is not functioning as intended due to a
number of factors such as underfunding, weak management arrangements, inadequate
staffing and difficulty in transport and communication (MOH, 2007).
The 2007 health policy recognized the importance of accessible and sustainable
Primary Health Care services for all Tanzanians through provision of a dispensary in
every village, a health center in every ward and a hospital in every district. However,
with the given country size, population and the geographical barriers, the health
services are not accessible to all Tanzanians (MOH, 2008). Furthermore, most
positions in those facilities are not filled with qualified health workers leaving
Tanzania with a severe human resource crisis (MOH, 2008).
Despite the health sector reforms which were deliberately designed to improve health
sector performance, the deterioration in health care service delivery is still going on in
most of the public owned health facilities in Tanzania (MOH, 2008). The researcher
did not come across any previous studies that investigate the delivery of health care
services in Kinondoni municipal health facilities. Therefore, there is a critical need to
fill this gap.
1.3 Research Questions
(i) What are the perceptions of civil servants on health care services
provided in Kinondoni municipal health facilities?
(ii) To what extent has health insurance contributed towards the
improvement of the health care services?
(iii) How can health care services provided in Kinondoni municipal health
facilities (as perceived by civil servants) be improved?
1.4 Objective of the Study
1.4.1 General Objective
To assess the delivery of health care services in Kinondoni municipal.
10
1.5 Specific Objectives
(i) To assess the perception of civil servants on health care services
provided in Kinondoni municipal health facilities.
(ii) To assess the contribution of health insurance towards the improvement
of health care services.
(iii) To elicit civil servants opinions on how to improve health care services
provided in Kinondoni municipal health facilities.
1.6 Significance of the Study
Clients are not only consumers of health services but they also play a great role in
contributing to financial resources which are used in running the health care facilities.
Assessing clients perceptions on health care services will give them an opportunity to
give their opinions on health care services they are provided and what is to be done.
Also, the information obtained from this study will help to inform the policy makers
and health care providers about the health care services as perceived by consumers.
This will enable them to develop and implement appropriate strategies for improving
the health care services provided in Kinondoni municipal health facilities.
Furthermore, the study enabled the researcher to fulfill the requirement for the Degree
of Masters of Public Administration of Mzumbe University.
1.7 Area and Scope of the Study
The study was conducted in Kinondoni municipal. The familiarity of the place was
one of the major reasons, which impressed the researcher to carry out the study.
1.8 Limitations of the Study
There were some challenges in this research which included among others:
(i) Time: the time allocated was short for this research.
(ii) Finance: the researcher was faced with financial constraints due to the fact that
he was self sponsored.
11
Despite that, the researcher put all efforts to accomplish the data collection and
analysis as it was required by the supervisor.
1.9 De – limitations
In order to carry out the research effectively, the research was carried out in Kinondoni
municipal only due to limited time. Furthermore, the area was cost effective to the
researcher.
CHAPTER TWO
LITERATURE REVIEW
12
2.1 Introduction
The increased deterioration in the quality and quantity of health services in the late
1970s and early 1980s sparked out the WB recommendation of increased cost recovery
as part of publicly provided health services in developing countries (World Bank,
1987). In most countries in Sub – Saharan Africa, health care services were provided
free of charge and often with high subsidies from their governments.
Severe shortage in resources such as medicines and other medical supplies finance and
staffs affected the effectiveness and quality of health services leading to the WB
proposition for cost recovery. User fee was taken as a way to improve efficiency and
equity of the health system. Through user fees, clients are provided with the available
health care services at the lower cost and at the same time discouraging excessive use
of resources.
The introduction of user fees (health insurance) in the government health facilities has
been one of the most visible policy changes associated with changes from government
dominated health services to market oriented health services financing provision.
Since government resources were decreased while demand have been increased in
many countries, more private resources have been needed to increase the quality and
quantity of health services (Newbrander and Sacca, 1996).
In order to get loans from the WB and IMF, governments in developing countries were
forced to devalue their currencies and cut back their public expenditure. Throughout
that period of economic crisis, national health expenditure in SSA has been decreased
not only in terms of absolute allocation but also in relation to total budget (Korte,
1992). This has resulted in poor quality of health care, lack of drugs, low resources
allocation and low morale to some of health providers in health facilities. In some
areas, the essential health services ceased to function.
The tangible benefits of cost recovery in government health services must include the
change of previous poor condition to what the community is able to discern as an
improvement in the service. Revenues can be used to expand the available services by
freeing resources or financing services that are under financed, for example medicines,
13
medical supplies, rehabilitation and increasing morale of service providers. Efficiency
is increased through reduction of excessive use of services, but increasing capacity
according to the need of the clients.
The social health insurance is based on mutual support and involves a transfer of
resources from relatively richer and healthier people to relatively poorer and sicker
people. It works best when there is a consensus among the population that mutual
support is a good thing (Norm and Weber, 1994).
Countries that have started user fees differ in the emphasis they put on the mobilization
and use of such fees. User fee survey by the WB in various countries in SSA revealed
a number of countries participating in the user fee scheme. Out of 27 countries, 30%
saw the revenue collection as a primary objective. The rest apart from collection of
revenue put emphasis on improving primary health care services including staff
incentives and drugs procurement (Shaw, 1995). Moreover, mobilization of user fee
without targeting improvement of health services quality cannot convince the client on
the need of user fees.
According to Nolan and Turbat (1993), health insurance should encourage clients to
move across the various levels of referral system without bypassing other levels.
Clients feel secured when they are referred officially to the next level. Only the right
signals are able to enhance improvement in quality using the user fees. When there is
an escalating user fee charges coupled with improved quality, then individuals are
given incentive to enter the health system. At the higher level, they pay more but they
also expect more in terms of expertise and efficiency.
The effectiveness of health insurance as a method of improving quality depends on its
ability to purchase the services that are being offered. Health insurance that had been
eroded by inflation is unlikely to contribute toward the goal in improving the quality
of health services. For health insurance to be effective, it must be adjusted to keep pace
with inflation as observed in Ghana, Zambia and Zaire (Shepard et al, 1995).
14
Poorly structured health insurance for services has been criticized due to failure to
portray the right picture in terms of value for money and thus negatively affecting the
amount of revenue generated from user fees. Each client would like to perceive the
exact value of service one is paying for. Flat user fees, although are simple in
administration, are unpopular and do not help clients to appreciate the value of the
services provided. A flat user fees in Uganda was also associated with frequent
shortage of drugs and staffing as it elicited a negative response by the community
(McPake et al, 1992).
2.2 Theoretical Perspectives
2.2.1 Market Failure
Market fail when it is possible to make one person better off without making someone
else worse off, thus indicating inefficiency (Winston, 2006). Market failure is a
concept within economic theory where the allocation of goods and services by a free
market is not efficient. There is the problem which prevents the market from operating
efficiently. Market failure refers to a situation where the market in theory is supposed
to function but may fail to do so in practice. Market fails to allocate resources
efficiently and produce socially optimum amounts of goods and services over time
when at least one of its components does not function well. The prevalence of market
failure is due to lack of conviction in favor of markets, the inflexibility of intervening
government agencies and political forces that enable certain interest groups to benefit
at the expense of society as a whole (Winston, 2006).
In health care market, the illnesses and the diseases of the patients, and their treatments
and investigations are the commodities that are traded. Thus, illness and diseases and
their investigations and treatments have a market value. Kenneth (1963) identified that
health care is inherently subject to market failure. While the government might be able
to improve some of the institutional and organization deficiencies, it will not be able
to improve all market deficiencies since some of the problems facing the government
are similar to those facing the market (Stiglitz, 1989).
15
2.2.2 Government Failure
Government fails when an intervention is unwarranted because markets are performing
well or when the intervention fails to correct a market problem efficiently (Winston,
2006). Government failure is the public sector analogy to market failure and occurs
when a government intervention causes a more inefficient allocation of goods and
resources than would occur without that intervention. Some types of government
interventions such as taxes, subsidies, price control and regulations including attempts
to collect market failure may also lead to an inefficient allocation of resources which
may make the matter worse rather than better.
Just as market failure, government failure is not a failure of the government to bring
about a particular solution, but is rather a systemic problem which prevents an efficient
government to provide a solution to the problem. The existence of market failure is
sometimes used as a justification for government intervention in a particular market.
Wolf (1979) emphasized that the possible existence of market failure is not sufficient
to prove the certainty of government success. According to Wolf, government may
also fail due to externalities and private goals, redundant and rising costs and
distributional inequity due to influence and power of interest group. The government
policy can be improved by making greater use of market oriented situations that have
already produced benefits in certain situations. ‘If the markets don’t like your policies,
they will punish you’ (Blair, 2004).
2.3 Quality of Health Care Services
According to the 2009 – 2015 Health Sector Strategic Plans III, quality in health
services is working according to specific standards which aim at improving the health
status of individuals and communities, reducing suffering due to diseases and illnesses
and increasing client’s satisfaction. At the same time efficiency and effectiveness is
increased (URT, 2008). Edvardsson (1998) emphasized that the concept of service
quality should be approached from the customer’s perception. It is the customer’s
perception which determines the level of service quality and satisfaction. Therefore,
the customer is the best judge of the quality of service and not the service provider.

16
Parasurman et al (1988) proposed five dimensions of factors affecting service quality,
those were: tangibles that include the physical appearance of the service facility,
equipments, service personnel and communication materials; reliability to deliver the
promised service dependently and accurately; responsiveness which refers to
willingness of the service provider to be helpful and prompt in providing service;
assurance that refers to the knowledge and courtesy of employees and their ability to
inspire trust and confidence; and empathy which is the customer longs for compassion,
caring and individualized attention from the service provider. Similarly, Brown et al
(1991) drew insight from Parasurman et al (1988) and developed six dimensions to
explain service quality. These dimensions are: technical competence which refers to
the degree to which health workers are trained and communicate with client’s; access
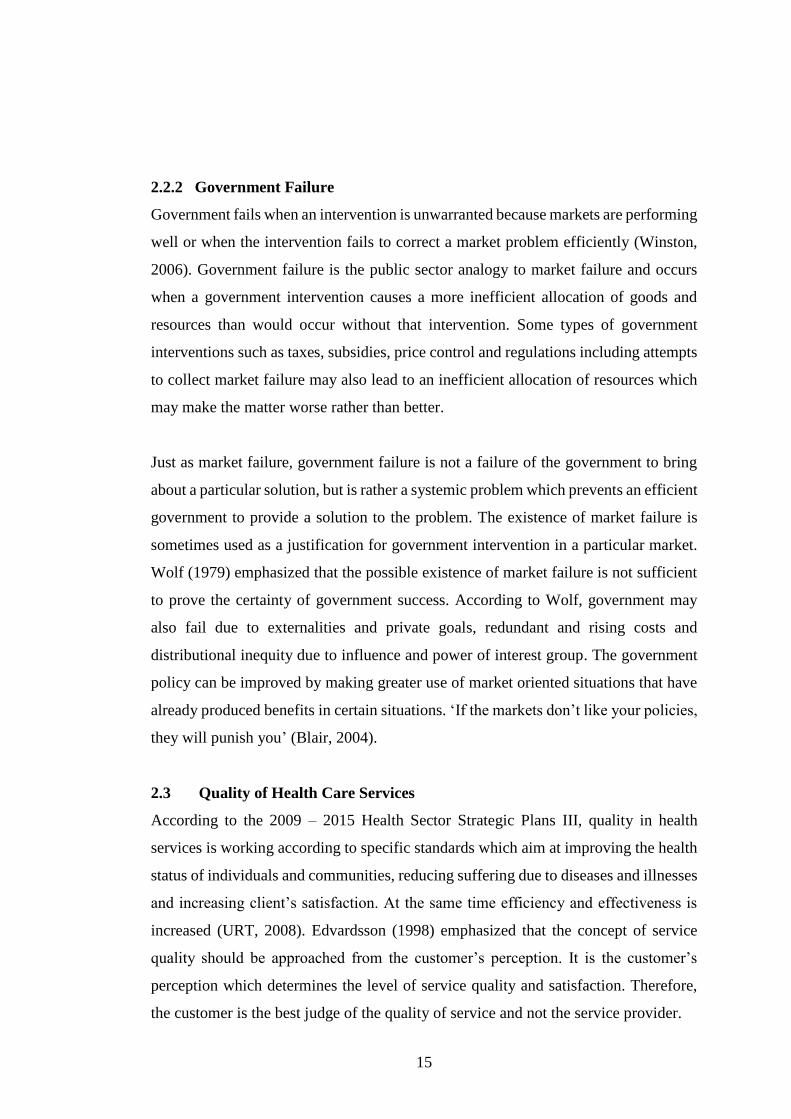
to service; affordability; interpersonal relation; reliability and tangibility (table 2.1).
Table 2.1: Dimensions of Quality Health Service
Dimension Details
TECHNICAL COMPETENCE The degree to which health care personnel have
the training and ability to assess, treat and
communicate with clients.
ACCESS TO SERVICE Being accessible and easy to contact in term of
distance from place of residence and availability
of service.
17
AFFORDABILITY Service affordable in term of client’s ability to
pay for service. Affordable service provides the
greatest benefit within the resources available.
INTERPESONAL RELATION Good interpersonal relation establishes trust and
credibility through demonstration of respect,
politeness, confidentiality, courtesy,
responsiveness and empathy.
RELIABILITY Client receives the complete range of health of
that he/she needs without interruption, cessation
or unnecessary repetition of diagnosis and
treatment. Services must be offered on an
ongoing basis and near the place of residence.
TANGIBILITY Relates to the physical appearance of facilities,
availability of personnel, and materials as well as
to comfort, cleanliness and privacy.
Source: Adopted from Brown et al, 1991
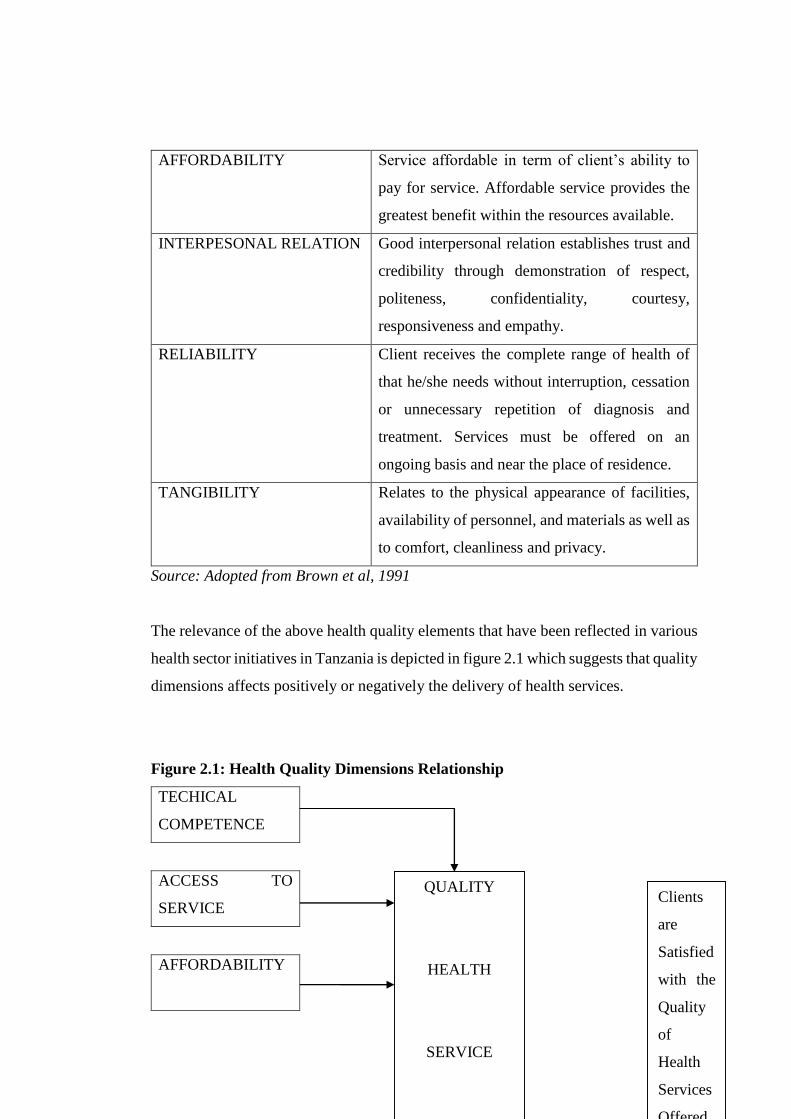
The relevance of the above health quality elements that have been reflected in various
health sector initiatives in Tanzania is depicted in figure 2.1 which suggests that quality
dimensions affects positively or negatively the delivery of health services.
Figure 2.1: Health Quality Dimensions Relationship
TECHICAL
COMPETENCE
ACCESS TO
SERVICE
AFFORDABILITY
QUALITY
HEALTH
SERVICE
Clients
are
Satisfied
with the
Quality
of
Health
Services
Offered
18
INTERPERSONAL
RELATION
RELIABILITY OF
SERVICES
TANGIBILITY
Source: Adopted from Shillingi and Mutalemwa, 2012
Following the introduction of alternative health financing mechanisms, measurement
of quality in government health facilities has received a great attention in SSA. This is
based on assumption that introduction of user fees in the previously free health care
services can only be successful and acceptable if quality of health care is also improved
at the same time (Litvack and Bordat, 1993).
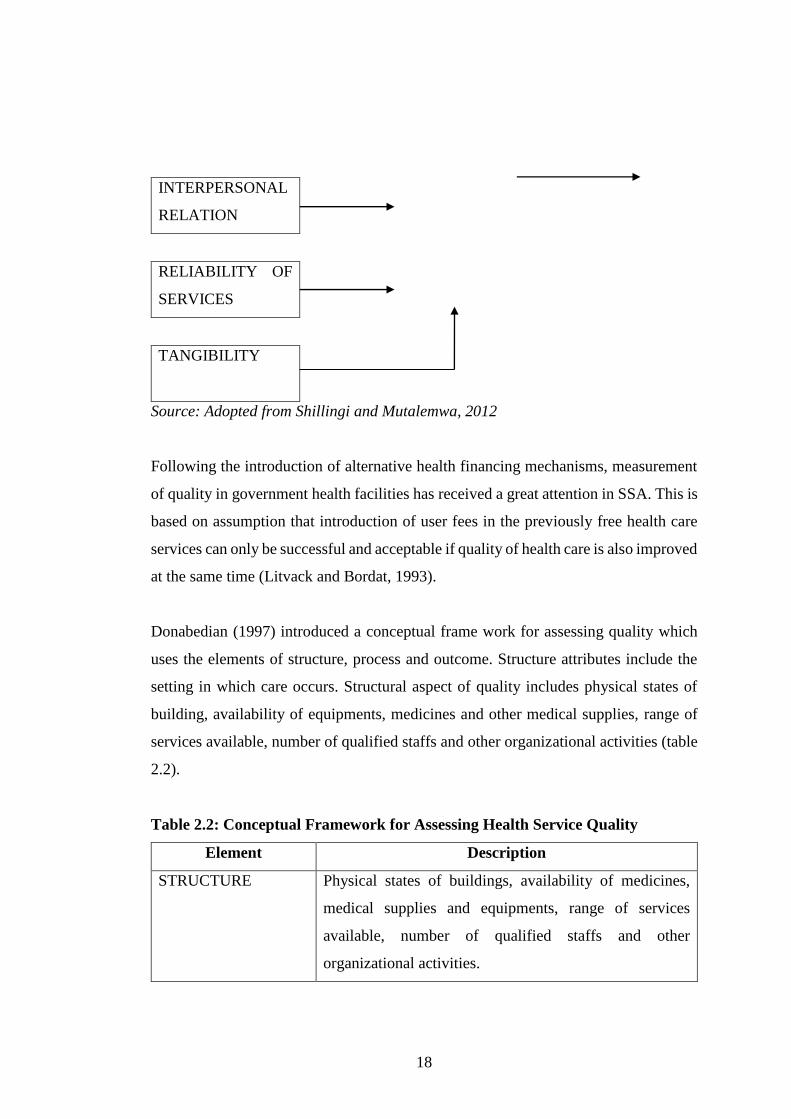
Donabedian (1997) introduced a conceptual frame work for assessing quality which
uses the elements of structure, process and outcome. Structure attributes include the
setting in which care occurs. Structural aspect of quality includes physical states of
building, availability of equipments, medicines and other medical supplies, range of
services available, number of qualified staffs and other organizational activities (table
2.2).
Table 2.2: Conceptual Framework for Assessing Health Service Quality
Element Description
STRUCTURE Physical states of buildings, availability of medicines,
medical supplies and equipments, range of services
available, number of qualified staffs and other
organizational activities.
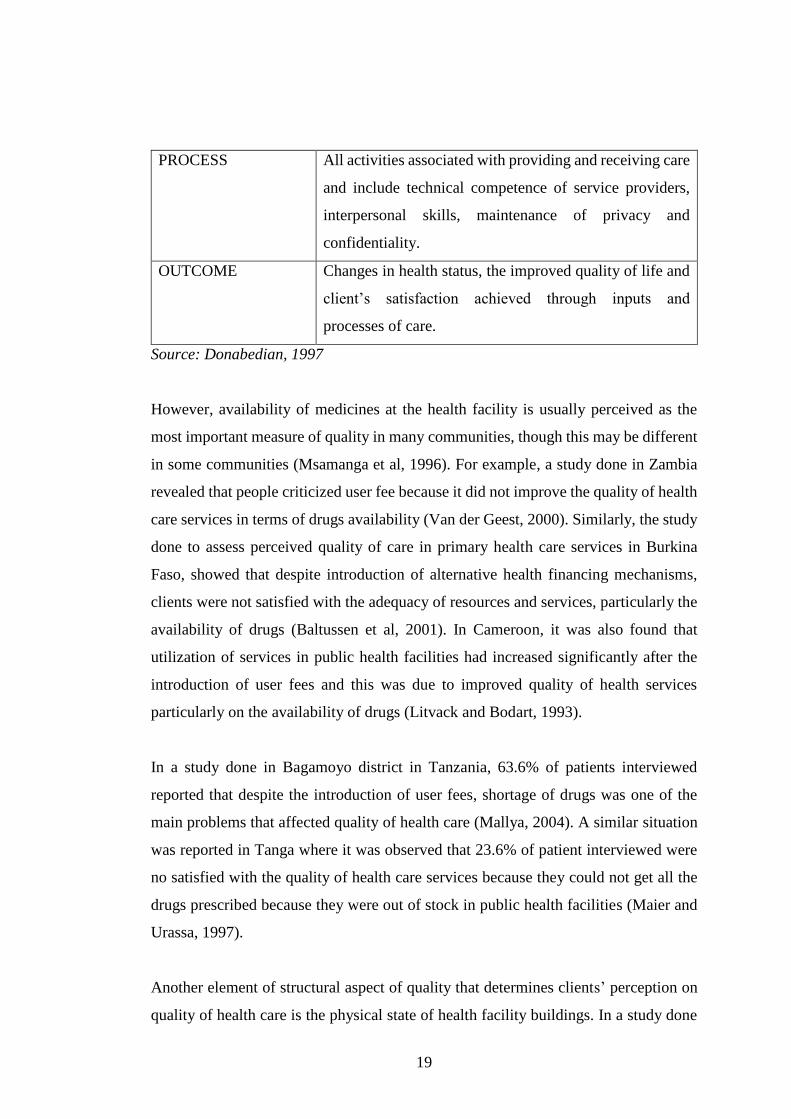
19
PROCESS All activities associated with providing and receiving care
and include technical competence of service providers,
interpersonal skills, maintenance of privacy and
confidentiality.
OUTCOME Changes in health status, the improved quality of life and
client’s satisfaction achieved through inputs and
processes of care.
Source: Donabedian, 1997
However, availability of medicines at the health facility is usually perceived as the
most important measure of quality in many communities, though this may be different
in some communities (Msamanga et al, 1996). For example, a study done in Zambia
revealed that people criticized user fee because it did not improve the quality of health
care services in terms of drugs availability (Van der Geest, 2000). Similarly, the study
done to assess perceived quality of care in primary health care services in Burkina
Faso, showed that despite introduction of alternative health financing mechanisms,
clients were not satisfied with the adequacy of resources and services, particularly the
availability of drugs (Baltussen et al, 2001). In Cameroon, it was also found that
utilization of services in public health facilities had increased significantly after the
introduction of user fees and this was due to improved quality of health services
particularly on the availability of drugs (Litvack and Bodart, 1993).
In a study done in Bagamoyo district in Tanzania, 63.6% of patients interviewed
reported that despite the introduction of user fees, shortage of drugs was one of the
main problems that affected quality of health care (Mallya, 2004). A similar situation
was reported in Tanga where it was observed that 23.6% of patient interviewed were
no satisfied with the quality of health care services because they could not get all the
drugs prescribed because they were out of stock in public health facilities (Maier and
Urassa, 1997).
Another element of structural aspect of quality that determines clients’ perception on
quality of health care is the physical state of health facility buildings. In a study done
20
in Bagamoyo district, 65.4% of the clients interviewed reported that the introduction
of user fees has little positive impact on the state of hospital buildings in terms of
cleanliness and maintenance (Mallya, 2004). Similarly, in the study done in Tanga it
was observed that some of the buildings had collapsed due to lack of regular
maintenance (Maier and Urassa, 1997). In most instances, structural aspect of quality
care had been evaluated in terms of physical condition of facility buildings and
availability of adequate equipment and drugs. However, the organizational aspects
such as number of staffs, qualification of staffs, administrative and managerial
procedures are also important. This is due to the fact that poor quality of health care
services can also be contributed by poor performance of health workers due to lack of
knowledge, inability to translate sufficient knowledge acquired through training into
appropriate attitude and performance, and low staff morale and motivation caused by
meager wages and poor working environment.
Process is another aspect of quality. It refers to all the activities associated with
providing and receiving care and include technical competence of service providers,
interpersonal skills, maintenance of privacy and confidentiality (Donabedian, 1980).
The technical aspect of quality refers to how well medical science and knowledge are
applied to the diagnosis and treatment of medical problems. Beyond technical aspect,
interpersonal aspect of quality of health care service is an essential part of the process
of health care provision. It refers to interactions between client and provider, in which
friendliness, attentiveness of health care providers and effective communication skills
has critical impact on client satisfaction with quality of health care services
(Donabedian, 1980).
Studies has shown that, in some countries, lack of respect for patients, stigmatism and
abusive language of health providers towards patients is still a big problem even after
the introduction of alternative financing mechanisms (Van der Geest, 2002). However,
provider – client interaction does not only involve attitude of health providers but also
the process of interaction such sharing of information and privacy. In most of primary
health care facilities, privacy has been reported to be poor due to inadequate space for
counseling and examination (MOH, 2001).
21
Outcome is another measure of quality of health care services. It includes the changes
in health status, the improved quality of life and clients’ satisfaction achieved through
inputs and processes of care. However, changes in health outcome have proven to be
difficult to measure instead many studies have been used clients’ satisfaction as an
important measure of outcome aspect of quality care. Clients’ satisfaction occurs when
services experienced meet clients’ expectations. To the great extent it is related to
aspects that are not strictly medical or technical but mainly on interpersonal aspects.
Many studies have been done to assess the impact of user fees on the quality of health
care services. However, there is still mixed evidence from African countries that user
fees contribute to the improvement of quality health care. In some countries, evidence
indicates that fees improved quality of care and patients attendance in public health
facilities, while in some areas user fees are reported to have caused utilization of health
care services. Assessment of equity implication of health sector user in Tanzania found
that there is limited positive evidence that user fees have in general achieved their
objectives of sustainability, drug availability, quality care, equity and access to the
poor. Members of NHIF have also shown concerns on poor patient – providers
interactions, long waiting time and shortage of drugs as the main problems which have
led dissatisfaction with quality of health care services (NHIF, 2012).
2.4 National Health Policy
The national health policy aims at implementing national and international
commitments. The overall objective of national health policy in Tanzania is to improve
the health care well being of all Tanzanians with the focus on those most at risk to
reduce morbidity, to raise the life expectancy and to encourage the health system to be
more responsive to the need of the people. The vision of the Government is to have a
healthy society, with improved social well being that will contribute effectively to
personal and national development. The mission is to provide basic health services in
accordance to geographical conditions which are of acceptable standards, equitable,
quality, affordable, sustainable and gender sensitive (MOH, 2009).
22
Specifically, the government aims to; reduce morbidity and mortality in order to
increase the life span of all Tanzanians by providing quality health care; ensure that
basic health services are available and accessible; prevent and control communicable
and non communicable diseases; sensitize the citizens about preventable diseases;
create awareness to individual citizens on their responsibility on health; improve
partnership between public sector, private sector, religious institutions, civil society
and community in provision of health services; plan, train and increase the number of
competent health staff; identify and maintain the infrastructures and medical
equipments and review and evaluate health policy, guidelines, laws and standards for
provisional of health services (MOH, 2009).
The government has developed a number of enabling policies and environment as an
effort to strengthen the health services in the country. These enabling policies are both
national and international commitments like Tanzania Development Vision 2025,
National Strategy for Growth and Reduction of Poverty, and Millennium Development
Goals. In TDV 2025, the main objective is achievement of high quality live hood for
all Tanzanians. The MOHSW contribute towards the improvement of health status life
expectancy of the people of Tanzania. This is partly achieved through public health
interventions and primary health services. Under MDG, the government is required to
reduce child mortality by two-thirds and improve maternal health by reducing maternal
mortality rate by three-quarters from 1990 to 2025, also to combat HIV/AIDS, malaria
and other diseases. NSGRP places MDG’s within cluster II which addresses
improvement of the quality of life and social wellbeing (MOH, 2009).
2.5 Health Delivery System in Tanzania
The health service delivery system in Tanzania consists of a network of facilities which
assumes a pyramidal structure starting from a dispensary, health center through the
district and regional hospitals to referral hospitals. In principle, the referral system is
designed for the dispensary to refer patients to health centers and for the health centers
in turn to refer into hospitals (figure 2.2). Unfortunately, this system is not functioning
as intended due to a number of factors such as underfunding, weak management
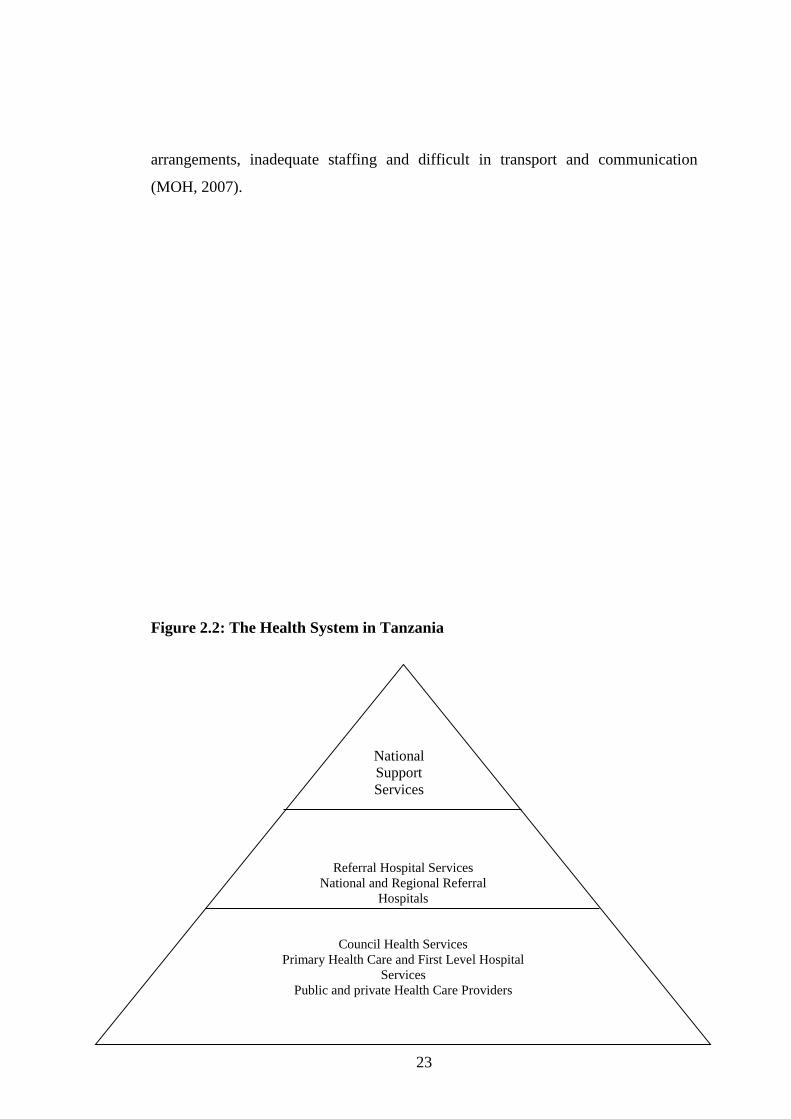
23
arrangements, inadequate staffing and difficult in transport and communication
(MOH, 2007).
Figure 2.2: The Health System in Tanzania
Referral Hospital Services
National and Regional Referral
Hospitals
Council Health Services
Primary Health Care and First Level Hospital
Services
Public and private Health Care Providers
National
Support
Services
24
Source: Ministry o f Health and Social Welfare, 2008
Tanzania Mainland is divided into 24 administrative regions and 115 districts with
133 councils. There 10342 villages. Primary health care forms the basis of the
pyramidal structure of health care services. There are 4679 dispensaries and 481 health
centers. About 90% of the population lives within 5km of a primary health facility.
There are 55 district hospitals owned by the government and 13 designated district
hospitals owned by FBO’s. Furthermore, there are 86 other hospitals at first referral
level owned by the government, parastatals and private sectors. There are 18 regional
hospitals functioning as referral hospitals for district hospitals and 8 consultancy and
specialized hospitals in the country (MOH, 2007).
Government staffing norms for health facilities exist but only 35% of the positions are
filled with qualified health workers leaving Tanzania with a severe human resources
crisis (MOH, 2009). The 2007 Health Policy recognize the importance of accessible
and sustainable Primary Health Care services for all Tanzanians through provision of
dispensary in every village, a health center in every ward and a hospital in every
district. However, with the given country size, population and the geographical
barriers, the health services are not accessible to all.
In order to achieve its goals, Tanzania has decentralized many government functions
through Decentralization by Devolution. Local Government Authorities are
responsible for delivering public services in local health, education, water and
agriculture. The MOHSW and PMO-LAG in collaboration with Public Service
Management Office are responsible for recruitment and distribution of staff throughout
the country (figure 2.3).

25
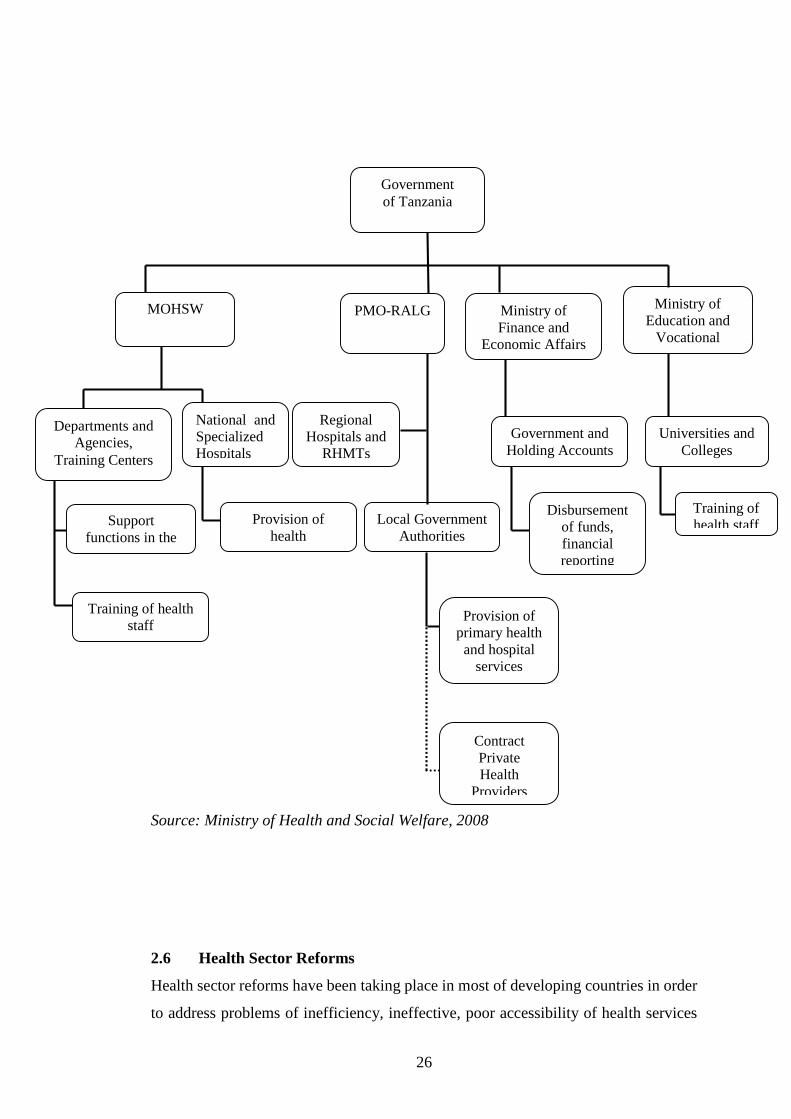
Figure 2.3: Ministries, Departments and Agencies Most Involved in Health Sector
and their Responsibilities
26
Source: Ministry of Health and Social Welfare, 2008
2.6 Health Sector Reforms
Health sector reforms have been taking place in most of developing countries in order
to address problems of inefficiency, ineffective, poor accessibility of health services
Government
of Tanzania
PMO-RALG Ministry of
Finance and
Economic Affairs
Government and
Holding Accounts
Universities and
Colleges
Disbursement
of funds,
financial
reporting
Reporting
Training of
health staff
staff
Ministry of
Education and
Vocational
Regional
Hospitals and
RHMTs
Local Government
Authorities
Provision of
primary health
and hospital
services
Contract
Private
Health
Providers
Provision of
health
Services
Support
functions in the
health sector
National and
Specialized
Hospitals
Departments and
Agencies,
Training Centers
MOHSW
Training of health
staff
27
and growing concern of financial sustainability. The driving forces behind health
sector reforms were the economic crisis which occurred in the late 1970s and early
1980s due to tremendous increase in oil prices, rising interest rates of external debts
and falling of other commodities which made African countries and other developing
countries unable to repay their foreign debts. In order to solve these problems, African
countries and other developing countries signed an agreement with the WB and IMF
to adopt SAP, which recommended cutbacks in government expenditure on health
sector and other social services (World Bank, 1993).
The dramatic drop in health expenditure in 1980s and 1990s in developing countries
led to fall in the economic and social developments attained in the past two decades,
which were characterized by increased number of health professionals employed in
public sector, improved infrastructure and extension of health care. For instance,
before the implementation of SAP in Tanzania, the government had succeeded in
expanding access to health care national wide. By 1977, more than three quarters of
Tanzanians population lived within 5km of a health facility, but after implementation
of SAP under funding occurred in the health sector leading to poor performance.
In order to generate resources for health sector and attain better quality and more
efficient and effective health care system, the WB agenda for reforms was launched as
well as the promotion of Bamako initiative of 1987 by UNICEF and WHO. In its
agenda for reform, the WB emphasized the need for introduction of cost recovery
strategies (World Bank, 1993). This included introduction of user fee for health
services that were previously provided free of charge and promotion of Health
Insurance Schemes or Prepayment Schemes (Green, 1992, World Bank, 1993). The
objectives of Bamako initiative were to improve quality of services and ensure equity
in access of care through community participation in form of payments for drugs and
development of community management capacity (Russell and Gilson, 1997).
In response to WB recommendations to adopt cost recovery and the Bamako initiative,
various countries in SSA and the rest of developing countries introduced user fees into
their health sector by the mid 1990s. A survey done by the WB in 1993 reported that
28
out of 37 African countries, 33 of them had cost recovery policies for the public sector
(Nolan and Turbat, 1995). Although in public health facilities user fees were
introduced in the last decade, they had been used in private and voluntary owned
organizations in most of developing countries for a long time ago even before the WB
recommendation to adopt cost recovery in health services (Shaw, 1995).
Experience shows that alternative health care financing schemes can succeed in
achieving their goals only if government takes complementary measure to ensure that
the services are accessible to all people and are of reasonable quality and that the
generated revenue is properly managed and reinvested to improve the quality of health
care services. However, studies show that these conditions are rarely met in practice.
It has been revealed that in some cases user fees revenues have not been retained within
the health sector, but goes to other local uses.
In Tanzania, the health sector has undergone continuous reforms since independence.
The Arusha Declaration of 1967 advocated for the development of a health service that
limited the role of the private sector, advocating for free medical services and placed
emphasis on rural development (MOH, 1997). During the period of the 70’s the
Government developed and extensive health services delivery infrastructure that
extended into the rural areas delivering curative, preventive and promotive services
through a network of hospitals, health centers and dispensaries. The health services
delivery was supported by health manpower training institutions.
Despite this extensive health services delivery infrastructure, health indicators did not
improve sufficiently. The cost of running this extensive health service in light of the
increasing cost for medicines, medical supplies and equipment and the deteriorating
economy was impossible for the government to meet. In additional the system faced
managerial and organization problems that decreases its efficiency (MOH, 1997).
In 1994 the MOH embarked on a more systematically planned HSR and aims at
improvement of access, quality and efficiency health services delivery. Primary Health
Care was adopted as the most cost- effective strategy to improve the health of the
29
people. The major focus of HSR is therefore on strengthening the District Health
Services as well as strengthening and reorientation of secondary and tertiary services
delivery in hospitals in support of primary health care (MOHSW, 2007).
The health sector reforms are in the following dimensions: decentralization of health
services; financial reforms, such as enhancement of user-charges in government
hospitals, introduction of health insurance and community health funds and
Public/Private Partnership reforms such as encouragement of private sector to
complement public health services. They also include organizational reforms such as
integration of vertical health programs into the general health services and propagation
of demand oriented researches in the health sector (MOHSW, 2007).
2.7 Health for All (Universal Coverage)
Universal coverage is a situation whereby society is covered with needed health
services for all people and at an affordable cost (Bayarsaikhan, 2006). This is known
as equity in accessing health care services. Accessing health care services is often
interpreted as securing services to everyone when they need irrespective of income,
sex, age or social status. Universal coverage is also associated with equity in finance
implying that households contribute on the basis of ability to pay.
In order to achieve universal coverage, organizational mechanisms are needed to
collect financial contributions equitably and efficiently to pool those contributions so
that financial risk associated with the need to pay for care are shared by all and to
purchase or provide effective and cost effective interventions with those contributions
(Preaker, 2005).
Historical perspective and social choices have been used by different countries to
determine which type of system forms the basis, but the important characteristics of
social protection. One indicative factor that needs to be considered by policy makers
is the degree of prepayment and pooled plans vis-à-vis the out of pocket spending. If
out of pocket is still the dominant method of financing health care, then a particular
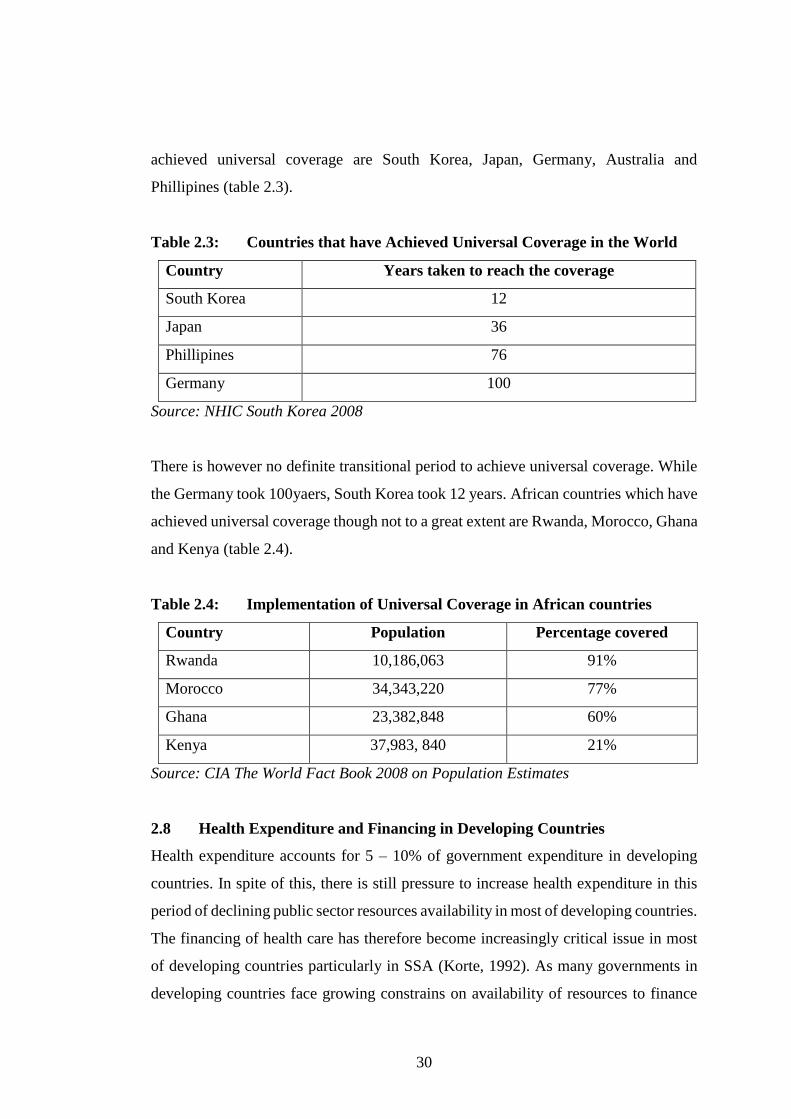
society is still at a beginning of its universal coverage route. Countries that have
30
achieved universal coverage are South Korea, Japan, Germany, Australia and
Phillipines (table 2.3).
Table 2.3: Countries that have Achieved Universal Coverage in the World
Country Years taken to reach the coverage
South Korea 12
Japan 36
Phillipines 76
Germany 100
Source: NHIC South Korea 2008
There is however no definite transitional period to achieve universal coverage. While
the Germany took 100yaers, South Korea took 12 years. African countries which have
achieved universal coverage though not to a great extent are Rwanda, Morocco, Ghana
and Kenya (table 2.4).
Table 2.4: Implementation of Universal Coverage in African countries
Country Population Percentage covered
Rwanda 10,186,063 91%
Morocco 34,343,220 77%
Ghana 23,382,848 60%
Kenya 37,983, 840 21%
Source: CIA The World Fact Book 2008 on Population Estimates
2.8 Health Expenditure and Financing in Developing Countries
Health expenditure accounts for 5 – 10% of government expenditure in developing
countries. In spite of this, there is still pressure to increase health expenditure in this
period of declining public sector resources availability in most of developing countries.
The financing of health care has therefore become increasingly critical issue in most
of developing countries particularly in SSA (Korte, 1992). As many governments in
developing countries face growing constrains on availability of resources to finance
31
health care, efforts to seek alternative forms of financing have intensified. Typically,
alternative methods of financing health services include providing insurance or other
coverage, charging users of health facilities, greater cooperation with private and the
effective use of non-governmental resources.
The main options are compulsory health insurance, community fund and user charge
(Smith and Rawal, 1992). Governments should supplement tax revenue by increasing
direct households contribution to the health sector through a variety of policy reforms;
user fees at government facilities, the adoption or encouragement of community based
financing schemes and the encouragement of not for profit making but fee charging
non-governmental organizations.
2.9 Health Insurance Schemes
Currently, the focus of international community is on the need to move away from out
of pocket payment as a source of health financing towards health insurance schemes.
The types of health insurance schemes include; Social Health Insurance Schemes in
which contributions are based on payroll deductions, with employee and employer
contributing to the premium set. The second type is Community Based Health
Insurance Scheme. This is not linked to the employment status but premiums are
commonly set according to risk faced by average number of the community.
Enrollment in these schemes is voluntary in nature. The third type is Private Insurance
Schemes where people pay premiums related to expected cost of providing services to
beneficiaries. In this type, people at high risk pay more than those at low risk (Bennet
and Gilson, 2001).
However, in developing countries, health insurance schemes are still confined to a
minority of population and only few countries have considerable experience in setting
up micro-health insurance. These countries include Burkina Faso, Mali, Ghana and
Senegal. In Tanzania as stated earlier, the first health financing option was User Fees
adopted in 1993, followed by Community Health Fund which was introduced in 1996
and finally National Health Insurance Fund which started to operate in 2001.

32
2.10 Health Financing in Tanzania
Health services financing mechanisms in Tanzania includes Central and Local
government funds, religion organizations, voluntary agents and donors. Other
financial sources are community contribution, community health funds, user fees and
national health insurance fund (MOH, 2002).
(a) Central Government Funds
The central government finances health sector in two ways:
(i) The ministry of health provides funds to referral hospitals and various medical
schools. It also provides funds to its parastatals such as NIMR. The ministry
also gives subventions to Kilimanjaro Christian Medical Center, Bugando
Medical Center and Designated DistrictHospitals.
(ii) The Prime Minister’s Office provides funds to run regional and district
hospitals including salaries for employees. At the same time, the office gives
subventions to the local council for running the health centers and dispensaries.
(b) Local Government Funds
The local governments are responsible for running health centers and dispensaries in
rural areas. They provide funds for purchasing of medicines and other medical
supplies, salaries, training and development of employees, constructions and
maintenance of health centers and dispensaries. They get their funds from government
subventions and local taxes.
(c) Religious Organizations and Voluntary Agencies
Religious organizations and voluntary agencies run their health facilities through their
own funds and service charges. The government provides subsides to these
organizations.
33
(d) Donors Funds
Some countries and International Organizations help Tanzania in provision of health
services in different forms. Most donors provide their funds to the MOHSW for
running national, regional or district health projects. Other donors help by bringing
their experts and offering medical supplies. Such assistances are through international
organizations like WHO etc.
(e) Community Contributions
Community contributions are mainly in cash. These are:
(i) User Fees
Communities contribute through user fees or cost sharing in health facilities
complements the government financing. Exemption is granted for old ages of more
than 60 years old, pregnant women and children under five years old.
(ii) Community Health Fund
Community health fund is recognized as an effective tool for mobilizing voluntary
community involvement and participation in supporting health care. It provides an
opportunity for seasonal income earners in the informal sector to pay for their services
before they fall sick.
(iii) National Health Insurance Fund
This is a mechanism to ensure medical protection in the formal sector.
According to section 4(2) of the Act, the main objectives of establishing the fund are;
to establish a reliable system that will enable the public sector employees to contribute
towards their health care services and that of their families, to promote public private
partnership that would instill competition which would in turn lead to improvement of
both accessibility to and quality of health services which is the essence of instituting
health reforms in Tanzania, and finally to expedite improvement of the health sector
by putting in place an alternative health financing option that would complement the
government health budget and hence reducing the financing gap.

34
2.11 Effects of Costs on Health Seeking Behavior
People perceive illness differently. The perception is an important determining factor
in seeking health care. An individual or households has to undergo several decision
making process before conclusion. These decision making processes are divided in
three stages. First, awareness of the presence of illness in the family will make them
to decide or not to seek health care services. Secondly, the type of health care provider
has to be decided upon and their various provider alternatives including self care and
decision on which one to go has also to be made. Lastly, the patient has to decide
whether or not there is a need to seek further treatment if cure is not affected after a
period of time.
Apart from making decision to where to seek care, there are factors that can determine
demand for health care. Researchers have shown that these factors include age, gender,
income, education and employment status, type and severity of illness, cultural factors,
distance and cost in time in reaching medical facility, time spent in waiting to get
medical care at the facility and quality of care offered. The availability of drugs,
medical supplies and competent staffs are supply side factors (Ellis and Stephenson,
1992).
CHAPTER THREE
RESEARCH METHODOLOGY
3.1 Introduction
This chapter focuses on the methods and instruments that were used to collect and
analyze data. It starts by describing the study area, research design and population of
the study. Sample size and data collection instruments are also discussed. The chapter
concludes by discussing the approaches to data collection and analysis.
35
3.2 Study Area
The study was conducted in Kinondoni municipal. The municipality has a total area of
531 square kilometers. According to the 2012 census, the municipality has a
population of 1,775,049 with a population growth rate of 5.0% per annum and
population density 3,343 people per square kilometer. Administratively Kinondoni is
broken into 4 divisions, 27 wards and 113 sub-wards.
Kinondoni municipal was selected for the study mainly due to its conveniences to the
easiness of communication, cost effective and limited time. Furthermore, Kinondoni
is divided into urban, sub – urban and villages which are inhibited by all classes of
people, from the richest to the poorest.
3.3 Study Design
A research design is a conceptual structure within which research is conducted; it
constitutes a blueprint for the data collection measurement and analysis (Cooper and
Schindler, 2003). It also refers to the way a study is planned and conducted, the
procedures and techniques employed to answer the research problem or questions
(Kothari, 2004).
A cross sectional study was employed in this research which was conducted in
Kinondoni municipal health facilities in April 2013. A cross sectional study is one that
studies a cross – section of the population at a single point in time, and data collection
is done once (Adam and Kamuzora, 2008). These are studies which are not repetitive
in nature and are carried out once at a particular point in time. Cross sectional study
was preferred by the researcher due to time constraint. Qualitative approach was used.
3.4 Study Population
A population is a collection of all elements to be studied and about which one want to
draw conclusion (Levin and Rubin, 2002). It also refers to the totality of objects under
investigations. The term population is not only applicable to human beings but to any
case of interest in the study (Adam and Kamuzora, 2008). The study population

36
consisted of civil servants attending health facilities in Kinondoni municipal who paid
health care services through NHIF.
This population was selected because other studies have indicated the need for
assessing the contribution of user fees in delivery of health services in public health
facilities. For example, Mallya (2004), in a study done in Bagamoyo district revealed
that, despite the introduction of user fees, shortage of drugs was one of the main
problems that affected quality of the health care services.
3.5 Sample and Sampling Technique
A sample is a group, hopefully representative of the population that is studied and from
which one derives generalizations about the population (Adam and Kamuzora, 2008).
The exact number of items selected from a population to constitute a sample is called
sample size. Sample size is the number of representative selected for interview from a
research population. In this study, stratified random sampling technique was used to
select the sample from the targeted population.
Stratified random sampling technique is a modification of simple random sampling
and systematic sampling that is designed to produce more representative and accurate
samples where a population comprises distinct groups (Adam and Kamuzora, 2008).
In stratified random sampling, the population is stratified into a number of non-
overlapping sub-populations or strata and sample items are selected from each stratum
based on simple random sampling (Kothari, 2004).
In this study, the targeted population was divided into different groups or layers before
selection of the representative in order to ensure representation of all members in the
population with similar characteristics such as gender, age group, marital status and
education level were stratified in the same stratum and then randomly selected. A total
number of 100 respondents attending the health facilities to receive health care services
were selected to form the sample; 20 respondents from Lugalo, 20 from
Mwananyamala, 20 from Sinza, 20 from Magomeni and 20 from Tandale.

37
3.6 Data Collection Instruments
Data were collected daily from 8.00 am to 4.00 p.m except for weekends and holidays
for the period of four weeks. The data collection instruments were questionnaires with
both open and closed ended questions, interview using hospital checklists and personal
observation in health facilities. Secondary data were obtained through library study,
journals and internet.
3.6.1 Questionnaire
Questionnaire is a series of questions each one providing a number of alternative
answers from which the respondents can choose (White, 2002). Quite often,
questionnaire is considered to be the heart of cross- sectional studies. This is because
apart from being cheaper to administer, questionnaire facilitate conveniences of
reaching respondents who are not easily reachable and provide respondents with time
to give well thought out and objective answers (Kothari, 2004). To be successful, the
questionnaire should be comparatively short and simple. Questions should proceed in
logical sequence moving from simple to more difficult questions (Kothari, 2004).
Based on that, simple and understandable questionnaires with both open and closed
ended questions were constructed. Copies were made and given to respondents who
were attending the health facilities to get treatment. They were provided with adequate
time to give answers. Finally filled questionnaires were collected.
3.6.2 Interview
The method of collecting information through personal interview is usually carried out
in a structured way. Such structure interview involves the use of set of pre-determined
questions and of highly standardized techniques of recording. A structured interview
guide is prepared to capture more information in great depth from key informants
(Kothari, 2004). This study used facility checklist because the idea was to capture more
detailed information on health services delivery. The scheduled visits to heads of
departments in the five municipal health facilities under the study were prepared and
prior appointment for interview was made.
38
3.6.3 Observation
When observation is used as data collection tool, the information is sought by way
investigators’ own direct observation without asking from respondent hence subjective
bias is eliminated and information relate to what is currently happening (Kothari,
2004). Another equally important reason for using observation in the study was that,
it gives an opportunity to gather live data from live situation (Cohen, 2000). In this
study, observation aimed at collecting data on physical state of buildings, general
cleanliness of the buildings, consultation, rooms and environmental cleanliness of the
facility surroundings.
3.7 Data Analysis
After collecting data from the field, raw data were edited and correction made on
obvious errors such as entry in a wrong place. In case of inappropriate or missing
replies, proper answers were determined by reviewing other information in the
questionnaire as proposed by Kothari (2004). Editing involved step by step, sorting
and checking of collected data to determine the relevant and irrelevant data and to
arrange them in a proper way to make easy presentation. After these validity and
reliability checks have performed, data were coded in different categories so as to
simplify the analysis and eventually were entered into computer spreadsheets.
Thereafter, data entered into Microsoft Excel software for summarization and
interpretation. The analysis was conducted based on the data from and information
collected from primary and secondary sources. The analyzed data were presented in
tables for easy interpretation and conclusion drew.

39
CHAPTER FOUR
PRESENTATION OF FINDINGS
40
4.1 Introduction
The purpose of this chapter is to present and analyze data obtained in the field in
simpler measures of statistics so that the data can be interpreted and understood by the
majority of people. The data presented in this chapter answers the research questions.
4.2 Respondent Interview
A total number of 100 civil servants attending municipal health facilities in Kinondoni
municipal were interviewed, 20 respondents were from Mwananyamala hospital, 20
from Sinza hospital, 20 from Lugalo hospital, 20 from Magomeni health center and 20
from Tandale dispensary. All were members of NHIF.
Table 4.1 shows that, a higher proportion of the sample study was males (55%). Most
of the respondents were either married (70%) or single (28%). About 44% of
respondents interviewed were in the age group of 40 to 49 years, those aged above 50
years contributed only 5 % of the total respondents. Respondent in the secondary
education (49) category formed the majority (49%) of the study sample.
Table 4.1: Socio-Demographic Characteristics of Respondents Interviewed
Characteristics n (%)
Sex
Male 55 55
Female 45 45
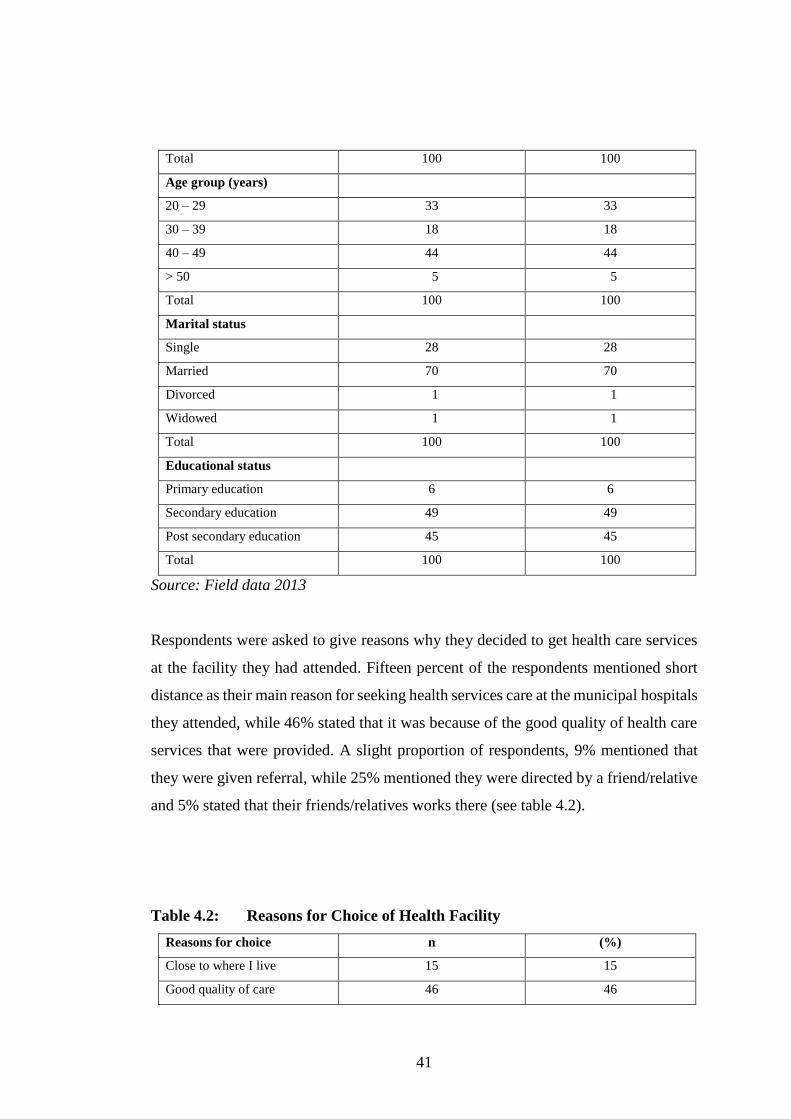
41
Total 100 100
Age group (years)
20 – 29 33 33
30 – 39 18 18
40 – 49 44 44
> 50 5 5
Total 100 100
Marital status
Single 28 28
Married 70 70
Divorced 1 1
Widowed 1 1
Total 100 100
Educational status
Primary education 6 6
Secondary education 49 49
Post secondary education 45 45
Total 100 100
Source: Field data 2013
Respondents were asked to give reasons why they decided to get health care services
at the facility they had attended. Fifteen percent of the respondents mentioned short
distance as their main reason for seeking health services care at the municipal hospitals
they attended, while 46% stated that it was because of the good quality of health care
services that were provided. A slight proportion of respondents, 9% mentioned that
they were given referral, while 25% mentioned they were directed by a friend/relative
and 5% stated that their friends/relatives works there (see table 4.2).
Table 4.2: Reasons for Choice of Health Facility
Reasons for choice n (%)
Close to where I live 15 15
Good quality of care 46 46
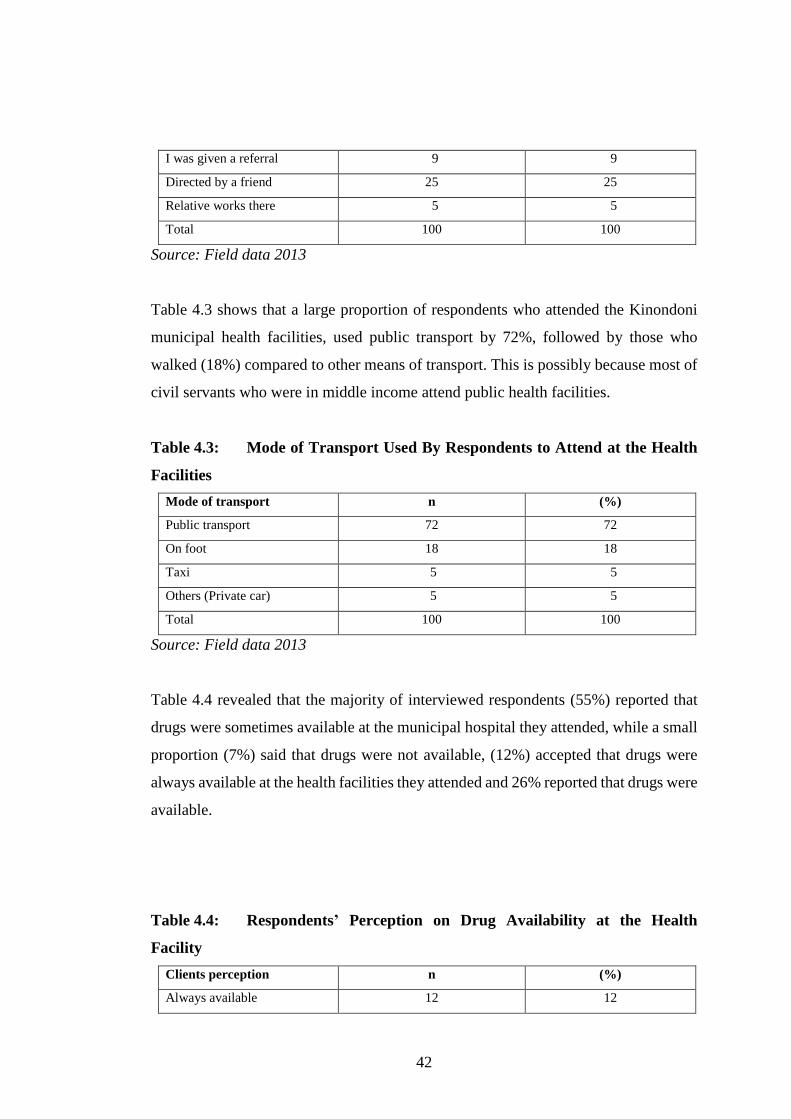
42
I was given a referral 9 9
Directed by a friend 25 25
Relative works there 5 5
Total 100 100
Source: Field data 2013
Table 4.3 shows that a large proportion of respondents who attended the Kinondoni
municipal health facilities, used public transport by 72%, followed by those who
walked (18%) compared to other means of transport. This is possibly because most of
civil servants who were in middle income attend public health facilities.
Table 4.3: Mode of Transport Used By Respondents to Attend at the Health
Facilities
Mode of transport n (%)
Public transport 72 72
On foot 18 18
Taxi 5 5
Others (Private car) 5 5
Total 100 100
Source: Field data 2013
Table 4.4 revealed that the majority of interviewed respondents (55%) reported that
drugs were sometimes available at the municipal hospital they attended, while a small
proportion (7%) said that drugs were not available, (12%) accepted that drugs were
always available at the health facilities they attended and 26% reported that drugs were
available.
Table 4.4: Respondents’ Perception on Drug Availability at the Health
Facility
Clients perception n (%)
Always available 12 12
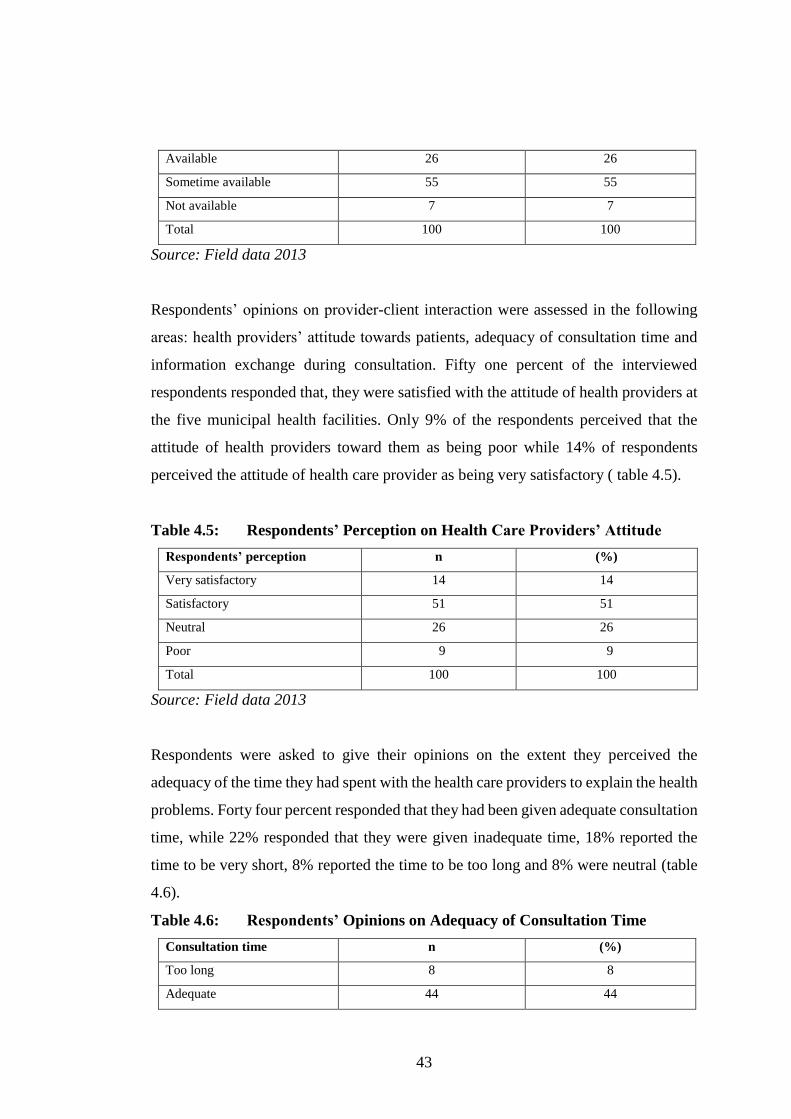
43
Available 26 26
Sometime available 55 55
Not available 7 7
Total 100 100
Source: Field data 2013
Respondents’ opinions on provider-client interaction were assessed in the following
areas: health providers’ attitude towards patients, adequacy of consultation time and
information exchange during consultation. Fifty one percent of the interviewed
respondents responded that, they were satisfied with the attitude of health providers at
the five municipal health facilities. Only 9% of the respondents perceived that the
attitude of health providers toward them as being poor while 14% of respondents
perceived the attitude of health care provider as being very satisfactory ( table 4.5).
Table 4.5: Respondents’ Perception on Health Care Providers’ Attitude
Respondents’ perception n (%)
Very satisfactory 14 14
Satisfactory 51 51
Neutral 26 26
Poor 9 9
Total 100 100
Source: Field data 2013
Respondents were asked to give their opinions on the extent they perceived the
adequacy of the time they had spent with the health care providers to explain the health
problems. Forty four percent responded that they had been given adequate consultation
time, while 22% responded that they were given inadequate time, 18% reported the
time to be very short, 8% reported the time to be too long and 8% were neutral (table
4.6).
Table 4.6: Respondents’ Opinions on Adequacy of Consultation Time
Consultation time n (%)
Too long 8 8
Adequate 44 44
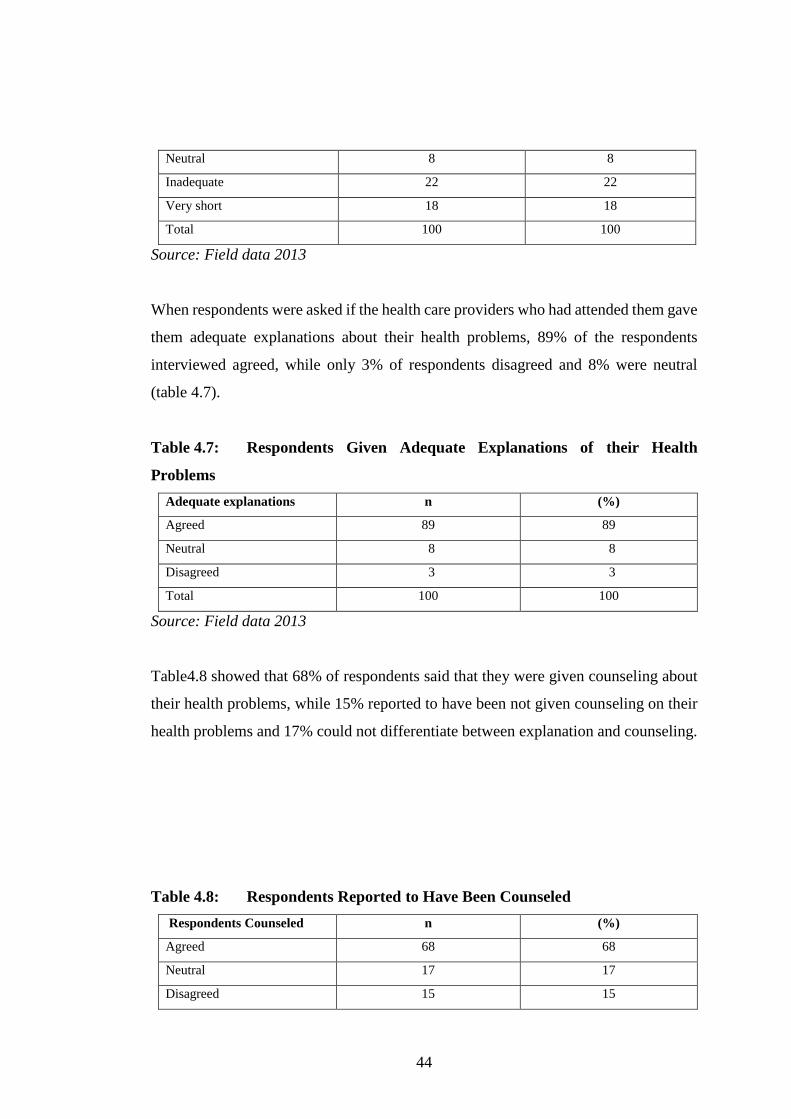
44
Neutral 8 8
Inadequate 22 22
Very short 18 18
Total 100 100
Source: Field data 2013
When respondents were asked if the health care providers who had attended them gave
them adequate explanations about their health problems, 89% of the respondents
interviewed agreed, while only 3% of respondents disagreed and 8% were neutral
(table 4.7).
Table 4.7: Respondents Given Adequate Explanations of their Health
Problems
Adequate explanations n (%)
Agreed 89 89
Neutral 8 8
Disagreed 3 3
Total 100 100
Source: Field data 2013
Table4.8 showed that 68% of respondents said that they were given counseling about
their health problems, while 15% reported to have been not given counseling on their
health problems and 17% could not differentiate between explanation and counseling.
Table 4.8: Respondents Reported to Have Been Counseled
Respondents Counseled n (%)
Agreed 68 68
Neutral 17 17
Disagreed 15 15
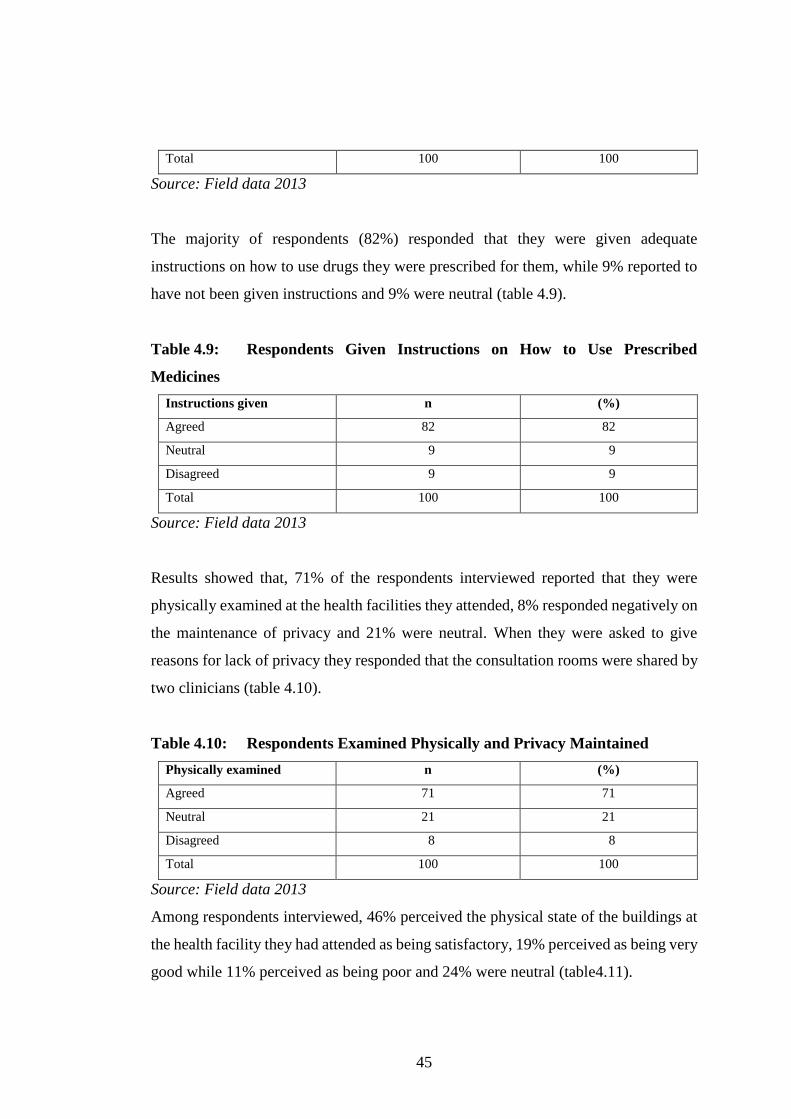
45
Total 100 100
Source: Field data 2013
The majority of respondents (82%) responded that they were given adequate
instructions on how to use drugs they were prescribed for them, while 9% reported to
have not been given instructions and 9% were neutral (table 4.9).
Table 4.9: Respondents Given Instructions on How to Use Prescribed
Medicines
Instructions given n (%)
Agreed 82 82
Neutral 9 9
Disagreed 9 9
Total 100 100
Source: Field data 2013
Results showed that, 71% of the respondents interviewed reported that they were
physically examined at the health facilities they attended, 8% responded negatively on
the maintenance of privacy and 21% were neutral. When they were asked to give
reasons for lack of privacy they responded that the consultation rooms were shared by
two clinicians (table 4.10).
Table 4.10: Respondents Examined Physically and Privacy Maintained
Physically examined n (%)
Agreed 71 71
Neutral 21 21
Disagreed 8 8
Total 100 100
Source: Field data 2013
Among respondents interviewed, 46% perceived the physical state of the buildings at
the health facility they had attended as being satisfactory, 19% perceived as being very
good while 11% perceived as being poor and 24% were neutral (table4.11).
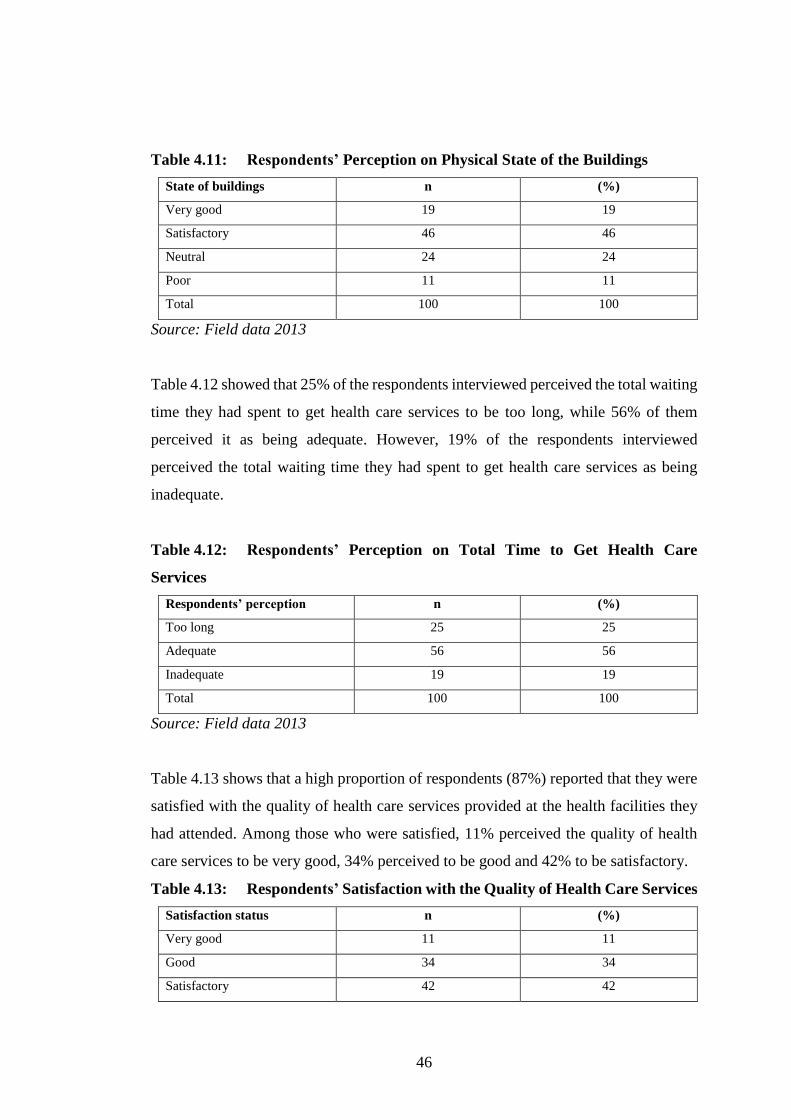
46
Table 4.11: Respondents’ Perception on Physical State of the Buildings
State of buildings n (%)
Very good 19 19
Satisfactory 46 46
Neutral 24 24
Poor 11 11
Total 100 100
Source: Field data 2013
Table 4.12 showed that 25% of the respondents interviewed perceived the total waiting
time they had spent to get health care services to be too long, while 56% of them
perceived it as being adequate. However, 19% of the respondents interviewed
perceived the total waiting time they had spent to get health care services as being
inadequate.
Table 4.12: Respondents’ Perception on Total Time to Get Health Care
Services
Respondents’ perception n (%)
Too long 25 25
Adequate 56 56
Inadequate 19 19
Total 100 100
Source: Field data 2013
Table 4.13 shows that a high proportion of respondents (87%) reported that they were
satisfied with the quality of health care services provided at the health facilities they
had attended. Among those who were satisfied, 11% perceived the quality of health
care services to be very good, 34% perceived to be good and 42% to be satisfactory.
Table 4.13: Respondents’ Satisfaction with the Quality of Health Care Services
Satisfaction status n (%)
Very good 11 11
Good 34 34
Satisfactory 42 42
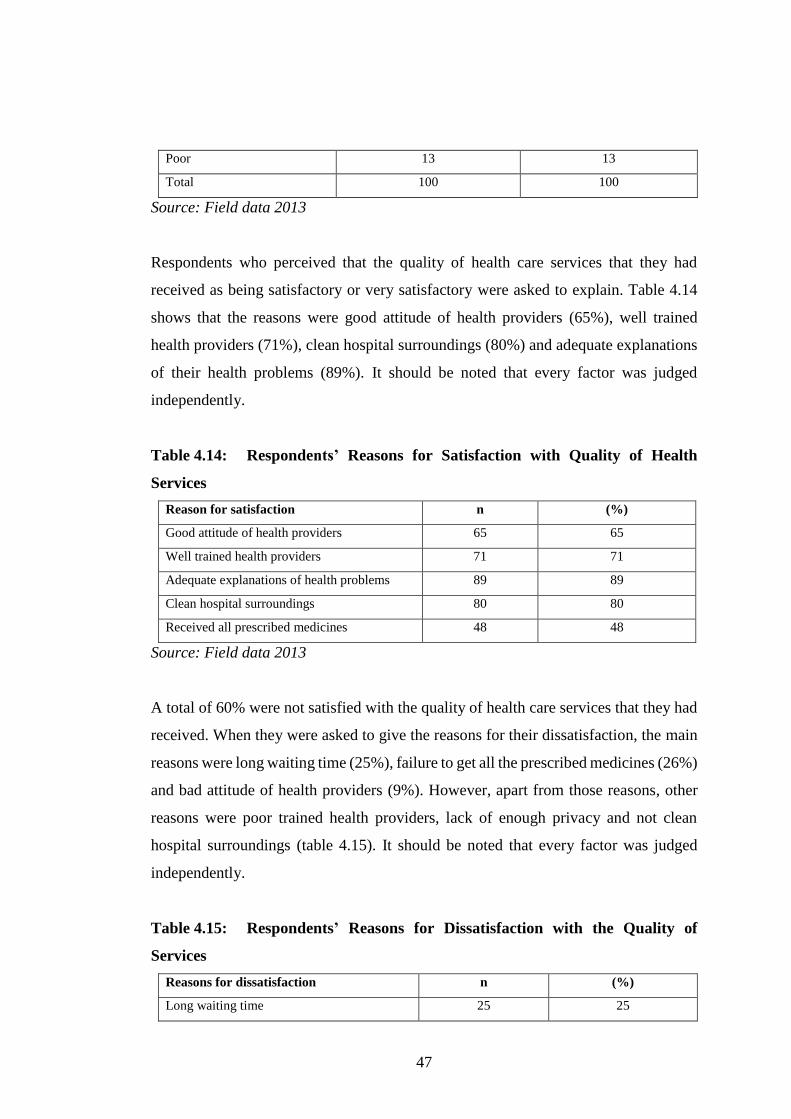
47
Poor 13 13
Total 100 100
Source: Field data 2013
Respondents who perceived that the quality of health care services that they had
received as being satisfactory or very satisfactory were asked to explain. Table 4.14
shows that the reasons were good attitude of health providers (65%), well trained
health providers (71%), clean hospital surroundings (80%) and adequate explanations
of their health problems (89%). It should be noted that every factor was judged
independently.
Table 4.14: Respondents’ Reasons for Satisfaction with Quality of Health
Services
Reason for satisfaction n (%)
Good attitude of health providers 65 65
Well trained health providers 71 71
Adequate explanations of health problems 89 89
Clean hospital surroundings 80 80
Received all prescribed medicines 48 48
Source: Field data 2013
A total of 60% were not satisfied with the quality of health care services that they had
received. When they were asked to give the reasons for their dissatisfaction, the main
reasons were long waiting time (25%), failure to get all the prescribed medicines (26%)
and bad attitude of health providers (9%). However, apart from those reasons, other
reasons were poor trained health providers, lack of enough privacy and not clean
hospital surroundings (table 4.15). It should be noted that every factor was judged
independently.
Table 4.15: Respondents’ Reasons for Dissatisfaction with the Quality of
Services
Reasons for dissatisfaction n (%)
Long waiting time 25 25
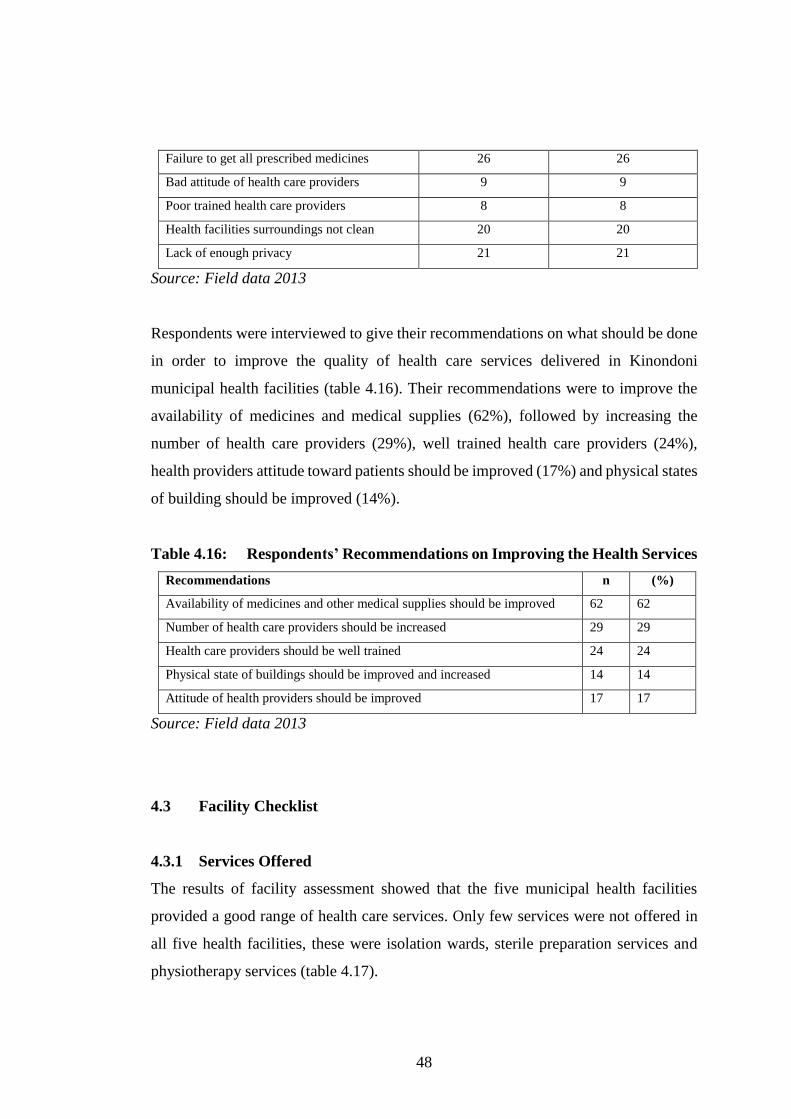
48
Failure to get all prescribed medicines 26 26
Bad attitude of health care providers 9 9
Poor trained health care providers 8 8
Health facilities surroundings not clean 20 20
Lack of enough privacy 21 21
Source: Field data 2013
Respondents were interviewed to give their recommendations on what should be done
in order to improve the quality of health care services delivered in Kinondoni
municipal health facilities (table 4.16). Their recommendations were to improve the
availability of medicines and medical supplies (62%), followed by increasing the
number of health care providers (29%), well trained health care providers (24%),
health providers attitude toward patients should be improved (17%) and physical states
of building should be improved (14%).
Table 4.16: Respondents’ Recommendations on Improving the Health Services
Recommendations n (%)
Availability of medicines and other medical supplies should be improved 62 62
Number of health care providers should be increased 29 29
Health care providers should be well trained 24 24
Physical state of buildings should be improved and increased 14 14
Attitude of health providers should be improved 17 17
Source: Field data 2013
4.3 Facility Checklist
4.3.1 Services Offered
The results of facility assessment showed that the five municipal health facilities
provided a good range of health care services. Only few services were not offered in
all five health facilities, these were isolation wards, sterile preparation services and
physiotherapy services (table 4.17).

49
Table 4.17: Various Services Provided in Municipal Health Facilities
Service Municipal Health Facility
M/nyamala Lugalo Sinza Magomeni Tandale
Operating theatre Available Available Available Unavailable Not available
Laboratory Available Available Available Available Available
Radiology Available Available Available Unavailable Unavailable
Blood bank Available Available Available Unavailable Unavailable
Dental unit Available Available Available Available Unavailable
Eye unit Available Available Available Available Unavailable
Physiotherapy Available Available Unavailable Unavailable Unavailable
Sterile unit Available Available Unavailable Unavailable Unavailable
Isolation ward Unavailable Unavailable Unavailable Unavailable Unavailable
Mortuary Available Available Available Unavailable Unavailable
Source: Field data 2013
4.3.2 State of Physical Structures
The buildings of Mwananyamala, Lugalo, Sinza and Tandale were in good physical
state with exception of Magomeni. The walls, ceiling boards, doors and windows were
found to be intact. It was noted that consultation rooms were not adequate in all
municipal health facility visited, as a result more than one clinicians shared one
consultation room except for specialist doctors. However, the rooms had adequate
space and well ventilated.
It was also noted that during physical examination visual privacy was maintained due
to presence of patient screens but audio privacy was difficult to maintain. In all five
health facilities, there were public toilets in the outpatient departments but they were
not clean and smelling. Some of them needed to be renovated.
4.3.3 Environmental Cleanliness
Overall cleanliness of the surroundings was good in all the five municipal health
facilities. There were neither long grasses nor piece of papers found scattered around
the facilities surroundings. All facilities had adequate solid and hazardous waste
50
materials collection and disposal facilities. Drainage systems were well functioning.
Also, all health facilities had adequate washing points near all service delivery and had
piped water and water storage tanks for ensuring constant flow of water.
CHAPTER FIVE
DISCUSSION OF THE FINDINGS
5.1 Introduction
This chapter presents the interpretation and discussion of the findings presented in
chapter four. Moreover, this chapter answers the questions on how and why the data
relate to the objectives of the study.

51
5.2 Provider – Client Interaction
Health service provider - client interactions include not only the attitudes of health
providers but also how the provider took trouble to make a proper diagnosis and
communicate information about the illness and management to the client.
Interpersonal relationship is an important factor for clients’ choice of the health facility
to get care. In a study done in Sri Lanka it was found that poor relationships between
public health providers and clients made clients to seek out health care services from
private health facilities, despite the fact that public health institutions had skilled and
technical competent health care providers (Russell, 2005). This study showed that 65%
of respondents were satisfied with the attitude of health providers in the five municipal
health facilities. However, a slight proportion of respondents (9%) perceived the
attitude of health providers to be poor.
Adequate consultation time is important in order to enable the provider to come up
with the correct diagnosis and appropriate management of the clients’ illness. In this
study, 44% of respondents interviewed perceived the consultation time they had spent
with the clinicians as being adequate. This study however, did not measure the actual
consultation time that respondents spent with their clinicians. Similarly, Msamanga et
al, (1996) in a study done in Mara and Kilimanjaro established an even higher
proportion (97.5%) of respondents who reported that the consultation time with health
care providers as being adequate.
Information exchange is also important during client – provider interactions. It
explains the flow of health information between the health care provider and the client.
Adequate information given to the client is very important for better compliance with
the treatment and hence improvement of quality of health services (Baker, 1990). In
this study, information exchange was assessed by asking the respondents in the
questionnaires whether they were given explanation about their health problems,
counseling, and advice on how to use the drugs prescribed to them and their side
effects.
52
Results showed that 89% of respondents interviewed agreed to have been given
adequate explanation about their health problems, while 68% agreed to have been
given counseling on their health problems and 82% agreed to have been given
adequate instructions on how to use drugs prescribed to them. However, the study did
not involve direct observation of the interaction between the health care provider and
the client but the study was limited to respondents’ perceptions on what they
experienced during their interactions with the health care providers. Similar findings
were reported by Mallya (2004) who established that 69% of the clients using user fee
interviewed reported to have been given adequate information about their health
problems.
The study findings also showed that 71% reported to have had physical examination
done. The issue of privacy during physical examination was also assessed as an
important part of provider – client interactions. The results showed that 21% reported
to have lacked privacy during physical examination. The possible explanation for this
was that two clinicians were sharing one consultation room.
5.3 Availability of Medicines and Medical Supplies
Availability of medicines, medical supplies and equipment is necessary for delivery of
health services. These items are important because they save lives, improve health of
the patients, promote trust of patients to the health delivery system and enhance
participation and ownership of the services. Most of deaths and causes of sufferings
and disabilities can be prevented, treated or alleviated with essential medicines,
medical supplies and equipment.
Availability of medicines and medical supplies in health facilities is one of the factors
that make patients to visit them for services. Some health facilities are preferred to
others due to this fact. The availability of drugs at the health facility is among the most
important components of the quality of primary health care services and therefore a
primary determinant of utilization of health care services (Msamanga et al, 1996). This
study showed that 55% of respondents interviewed reported that drugs were sometimes
53
available at the municipal health facilities they had attend, while a small proportion
(7%) reported that drugs were not available.
Similarly, studies done in other parts of the country have also established inadequate
drug availability to be problem. In a study done in Bagamoyo district, 63.6% of
patients interviewed reported that drugs were not available at all the time (Mallya,
2004). Another study done in Moshi rural district found that 92% of respondents in
public health units reported that drugs were available only in some days of the month
(Adam, 2001). However, this study did not study the cause of drug shortage in
Kinondoni municipal health facilities.
5.4 Waiting Time
Waiting time is that duration of time the patient spends waiting before receiving health
care services. Patients at health facilities often experience long queues. The problem
is largely attributed to the shortage of staff. On the other hand, some facilities serve a
very large population with limited equipment, shortage of drugs and other medical
supplies.
The results from this study showed that respondents spent long time in waiting to get
investigations done than waiting for other services (25%). They mentioned long queue
as the main reason for spending a lot of time. This was also confirmed during the
assessment of adequacy of rooms for various services using check list where it was
noted that there is only one laboratory and one radiology unit. These were being used
by all patients regardless of health financing option used, hence, delay in receiving
services occurred.
Long waiting time was also mentioned in the NHIF implementation report as one of
the factor causing dissatisfaction of clients with the quality of health care services
received under National Health Insurance Fund (NHIF, 2012).
54
5.5 Physical State of Buildings
Physical state of buildings was also assessed as an important aspect of health care
services delivery. About 65% of respondents interviewed perceived that physical state
of buildings in the municipal health facilities that they had attended to be satisfactory.
The main reason of satisfaction is likely to be due to the fact that the buildings of the
five municipal health facilities have been rehabilitated recently and in addition
renovation of some of the buildings was still going on while in some facilities (Lugalo
and Sinza) construction of new buildings were still going on as it was observed during
physical assessment of the physical state of the facilities buildings using a facility
checklist.
5.6 Patients’ Satisfaction or Dissatisfaction with Health Services Delivery
Patients’ satisfaction is regarded as one of the desired outcome of health care services
and is increasingly being used as a measure of the quality of care as it was stated by
Parasurman et al (1988) and Donabedian (1997). The results of this study showed that
87% of the respondents interviewed were satisfied with the quality of health care
services they had received.
When respondents were asked to give the reasons for their satisfaction with the quality
of services they had received, the majority mentioned good attitude of health care
providers (65%) and health providers are well trained. These were followed by
structural factors such as cleanliness of the health facility surroundings (80%) and
availability of drugs (48%). The findings of this study showed that providers’ attitude
towards clients is the most powerful determinant factor of client satisfaction with the
quality of health care services.
Although it is difficult for a client to judge health care providers’ technical skills due
to information asymmetry that exist between patients and providers, a higher
proportion of the interviewees reported great satisfaction with health care providers’
technical skills. This might be due to the fact that clients tend to have trust in the public
health facilities and in the technical competence of public health care providers as have
been established elsewhere (Russell, 2005). The findings of this study also conform to
the findings established by Msamanga et al (1996) which showed that perceived
55
providers’ technical competence and provider-patient interactions to be the main
factors which determined clients’ satisfaction with the quality of health care services.
In this study, structural elements of quality were mostly mentioned as dissatisfying
factors particularly poor availability of medicines and medical supplies (26%) and long
waiting time (25%), followed by lack of privacy (21%), bad attitude of health care
providers (9%) and poor trained health care providers (8%). The findings from the
studies done from other developing countries also showed that long waiting time is
associated with the highest level of dissatisfaction with quality of health care.
5.7 Contributions of Health Insurance towards Improvement of Health Services
The primary purpose of health insurance is to generate revenue. In public sectors fees
are usually introduced to supplement public funds when those sectors fail to keep up
with the cost of providing services to meet increasing demand. Although the primary
purpose is to generate revenue but the total amount of revenue generated is unlikely to
be sufficient to meet the growing need and demand for high quality health care services
(Newbrander and Sacca, 1996).
The introduction of health insurance in the government health facilities has been one
of the most visible policy changes associated with changes from government
dominated health services to market oriented health services financing provision.
Since government resources were decreased while demand have been increased in
many countries, more private resources have been needed to increase the quality and
quantity of health services (Newbrander and Sacca, 1996).
NHIF was viewed as a means of generating additional revenue in the health sector,
improving quality of health services as well as promoting equity, accessibility and
efficiency in the use of public health services in Tanzania (MOH, 1997). Many studies
have been done to assess the impact of health insurance on the quality of health care
services. In some countries evidence indicated that insurance improved quality of
health care and attendance in public health facilities, while in some areas insurances
are reported to have caused under utilization of health services.
56
Assessment of equity implication of health sector user in Tanzania found that there is
limited positive evidence that insurance have in general achieved their objectives of
sustainability, drug availability, quality care and access to the poor. In this study,
respondents perceived that insurance played a role towards improvement of health care
services. The study revealed that a higher proportion of respondents (87%) were
satisfied with the quality of health care services provided at the health facilities they
had attended. Among those who were satisfied, 11% perceived the quality of health
care to be very good, 34% perceived to be good and 42% perceived to be satisfactory.
5.8 Improving the Quality of Health Care Services
According to the 2009 – 2015 Health Sector Strategic Plan III, quality in health
services is working according to specific standards which aim at improving the health
status of individuals and communities, reducing suffering due to diseases and illness
and increasing client’s satisfaction. At the same time efficiency and effectiveness is
increased (MOHSW, 2008). However, the concept of service quality should be
approached from the customer’s perception which determines the level of service
quality and satisfaction. Therefore, the customer is the best judge of the quality of
service and not the service provider (Edvarsson, 1998).
Availability of medicines, at the health facility is usually perceived as the most
important measure in improving the quality of health care services in many
communities (Msamanga et al, 1996). In this study, availability of medicines was
reported to be a problem. More than half (55%) of respondents responded that
medicines were sometimes available at the health facilities they attended. A similar
situation was reported in Bagamoyo district where it was observed that 63.6% of
respondents interviewed, reported that despite the introduction of health insurance,
shortage of medicines was one of the main problem that affected quality of health
services (Mallya, 2004).
Another important measure in improving the quality of health care services as
perceived by respondents is physical condition of the facility buildings. However, the
57
organizational, aspects such as number of staffs, qualification of staff, administrative
and managerial procedures are also important. This is due to the fact that poor quality
of health care services can also be contributed by poor performance of health workers
due to lack of knowledge, inability to translate sufficient acquired through training into
appropriate attitude and performance, and low staff morale and motivation caused by
meager wages and poor working environment.
In this study, in order to improve the quality of health care services, respondents
interviewed suggested that availability of medicines, medical supplies and equipment
should be improved (62%), the number of staff should be increased (29%), staff should
be well trained (24%), attitude of health workers should be improved (17%), physical
state of buildings should be improved (14%) and time to get services should be
improved.
5.9 Market Failure
Market failure is a concept within economic theory where the allocation of goods and
services by a free market is not efficient. There is the problem which prevents the
market from operating efficiently. Market failure refers to a situation where the market
in theory is supposed to function but may fail to do so in practice. The prevalence of
market failure is due to lack of conviction in favor of markets, the inflexibility of
intervening government agencies and political forces that enable certain interest
groups to benefit at the expense of society as a whole (Winston, 2006).
In health care market, the illnesses and the diseases of the patients and their treatments
and investigations are the commodities that are traded. Thus illness and diseases and
their investigations and treatment have a market value. Kenneth (1963) identified that
health care is inherently subject to market failure. While the government might be able
to improve some of the institutional and organization deficiencies, it will not be able
to improve all market deficiencies since some of the problems facing the government
are similar to those facing the market (Stiglitz, 1989).

58
In this study, availability of drugs and medical supplies found to be a problem in all
five municipal health facilities. The study revealed that only 12% of respondents
interviewed reported that drugs were always available, 26% reported that drugs were
available, while 55% reported that drugs were sometimes available and 7% reported
that drugs were not available. A quarter of clients (25%) perceive waiting time to be
long.
5.10 Government Failure
Government fails when an intervention is unwarranted because markets are performing
well or when the intervention fails to correct a market problem efficiently (Winston,
2006). Government failure is the public sector analogy to market failure and occurs
when the government intervention causes more inefficient allocation of goods and
resources than would occur without the intervention. Some types of interventions such
as taxes, subsidies, price control and regulations including attempts to collect market
failure may also lead to an inefficient allocation of resources which may make the
matter worse rather than better.
In Tanzania the health care services were previously provided free of charge. The
government was the main provider of health services in the country and the sole source
of health financing. However, the problems of implementation of vertical programs,
inappropriate utilization of manpower, improperly financing referral system, shortage
of staff and inadequate medicines and medical supplies made the government to
change its role from that of provider to facilitator and adopt user fee as alternative
health financing mechanism (MOH, 1997).
This study showed that 26% of respondents were dissatisfied with the quality of health
delivered due to failure to get all the prescribed medicine, 25% due to long waiting
time, 21% due to lack of privacy and 17% due to bad attitude of and poor trained health
care providers.
59
CHAPTER SIX
SUMMARY, CONCLUSIONS AND RECOMMENDATIONS
6.1 Introduction
This chapter summarizes the findings of the study, presents conclusions and makes
recommendations.
6.2 Summary
A cross section study was conducted in Kinondoni municipal health facilities in April
to May 2013 with the main objective of assessing delivery of health care services as
perceived by civil servants using NHIF. A total of 100 respondents were interviewed.
60
Respondents were selected using convenience sampling method. A structured
questionnaire and facility check lists were used to collect data.
The study findings showed that health provider – patient interaction was perceived to
be satisfactory with 51% of respondents. Eighty nine percent of respondents reported
to be given adequate explanations of their health problems, while 82% reported to be
given adequate instructions on how to use prescribed medicine, 68% agreed to be
counseled and 71% reported to have been physically examined. The majority of
respondents (80%) were satisfied with the cleanliness of facility surroundings.
Respondents were also interviewed on the aspect of duration of time they spent waiting
to get services. A quarter of respondents interviewed (25%) perceived waiting time to
be too long, while 56% perceived to be adequate. Availability of drugs was reported
to be a problem in this study, more than half (55%) of respondents responded that
drugs were sometimes available at the facility they attended. The level of respondents
satisfaction with the quality of health care services was high (87%) with a small
proportion (13%) being dissatisfied mainly due to lack of privacy and failure to get all
prescribed medicines.
In order to improve the delivery of health care services respondents suggested that
availability of medicines, medical supplies and equipments should be improved. The
government should ensure that the health care providers are well trained and adequate.
Furthermore, the time spent to get services, physical state of buildings and attitude of
health care providers should be improved. The researcher recommended that
respondent’s opinions should be considered in strategic planning to improve delivery
of quality health care services.
6.3 Conclusion
The study revealed that respondents were satisfied with the health care services
delivered by the Kinondoni municipal health facilities. Respondents were satisfied
with the quality of health care services they had received in Kinondoni municipal
health facilities, particularly on consultation time, information sharing and patient –

61
provider interactions based on the attitude of health providers towards patients.
Respondents were also satisfied with physical states of facilities buildings and
cleanliness of the facilities surroundings.
Respondents perceived that health insurance played a great role towards the
improvement of health care services by improving the availability of medicines,
medical supplies and equipments to some extent. However, the study has also shown
that respondents perceived shortage of medicines, medical supplies and equipments as
a problem in all the municipal health facilities in Kinondoni. The study also revealed
that respondents’ perceived overall waiting time to be long (25%) and lack of privacy
due to shortage of consultation rooms.
In order to improve the delivery of health care services, respondents suggested that
availability of medicines, medical supplies and equipments should be improved. The
health care providers should be well trained and improved in number. The attitude of
health care providers, time spent to get services and physical state of buildings should
be improved.
6.4 Recommendations
In light of the above information and findings, the study came up with the following
recommendations on improving the delivery of health care services.
6.4.1 Specific Recommendations
(i.) Important measures should be taken to improve the availability of
medicines, medical supplies and equipments in the municipal health
facilities assessed.
(ii.) Respondent’s opinions on improving the quality of health care services
and their suggestions on how to improve the delivery of health care
services should be taken into consideration when planning strategies
targeted to improve the quality of health care services.
62
6.4.2 General Recommendations
(i.) The government through the Ministry of Health and Social Welfare
should identify the areas that need to be improved or restructured with
the aim of improving health and health delivery system by developing
and implementing efficient and effective plans.
(ii.) Before making plans and commitments for the introduction of social
insurance financing, the government should look more widely at the
exiting health care financing and provision arrangements. Insurance
should not be seen as a way of shifting core responsibilities for overall
regulation and policy making.
6.4.3 Areas for Further Researches
This study was conducted only in Kinondoni municipal, Dar es Salaam region. It is
hereby recommended that, the study be conducted in other municipal of Dar es Salaam
or other areas in Tanzania to confirm the findings. More research should be done
because the research has shown dissatisfaction in some areas in delivery of health care
services.
REFERENCES
Abel-Smith, B. and Rawal, P. (1992). Can the poor afford free health services? A case
study of Tanzania. Health Policy and Planning; vol, 7 (4): 329
– 341.
Adam, J. and Kamuzora, F. (2008). Research methods for business and social studies.
Mzumbe University.
Andaleb, S.S (2001). Service quality Perception and Patient Satisfaction: A study of
Hospitals in Developing Countries. Social Sciences and
Medicine;Vol 5:1359 – 1370.
63
Baltussen, R.M., Haddad, S. and Sauerborn, R.S. (2001). Perceived Quality of Care of
Primary Health Services in Burkina Faso. Health Policy and
Planning; Vol 17:42 – 48.
Berman, P. (1995). Health Sector Reform: Making Development Sustainable. Health
Policy; 32 : 13 – 28.
Brown, L.D., Franco, L.M., Rafeh, N., & Hatzell, T. (1991). Quality Assurance of
Health Care in Developing Countries: Quality Assurance
Project; USA; Johns Hopkins University School of Hygiene
and Public Health. .
Cohen, L.L. (2000). Research methods in education. London, Routledge Falmer.
Cooper, D.R. and Schindler, P.S (2003). Business research methods. Tata Mc Graw-
Hill Publishing Company Ltd, New Delhi.
Donabedian, A. (1980). Exploration in Quality Assessment and Monitoring. The
Definition of Quality and Approaches to its Assessment.
Health Administration Press.
Donabedian, A. (1997). The Quality of Health Care; How Can it be Assessed ?
Archives of Pathology and Laboratory Medicine; Vol 121
(11): 1145 – 51.
Edvarsson, B.O., (1988). Service Quality in Customer Relationships: A study of
Critical Incidents in Mechanical Engineering Companies. The
Service Industries Journal 8, No 4, July pp 427 – 445.
Ellis, R. and Stephenson, E (1992). Analysis of the Demand for Inpatient and
Outpatient Care for Imbaba Hospital Cairo. World Bank:
Financing and Sustainability Project Paper No:1 Egypt.
64
Fabricant, S. and Kamara C (1990). The Financing of Community Health Services in
Sierra Leone. Bamako Initiative Technical Report. UNICEF.
Griffin, C. and Shaw, R. (1995). Health Insurance in Sub-Saharan Africa: Aims,
Findings and Policy Implication, in Word Bank Discussion
Papers. Africa Technical Department Series No 294.
Korte, R. (1992). Financing Health Services in Sub-Saharan Africa. Options for
Decision Makers During Adjustment. Social Sciences and
Medicine.
Kothari, C.R (2004). Research methodology, methods and techniques. Second revised
edition, New age international (P) Ltd.
Levin, R.I and Rubin, D.S (2002). Statistics for management. Prentice – Hall of India
Private Ltd. New Delhi.
Litvack, J. and Bodart, C (1993). User Fees Plus Quality Equal Improved Access to
Health Care. Results of Field Experiment in Cameroon. Social
Science and Medicine; Vol 37 (3) : 369 – 387.
Maier, B. and Urassa, D (1997). Quality Assessment of Hospitals in Tanga Region.
Ministry of Health and Family Health Project Tanzania (GTZ).
Mallya, R. (2004). Role of Cost Sharing on Quality of Health Care: Community and
Patients’ Perception in Bagamoyo. A dissertation Submitted
in Partial Fulfillment of the Requirements for the Degree of
Master of Public Health of the University of Dar es Salaam.
McPake, B., Hanson, K. and Hills. (1992). Experience Today of Implementing Bamako
Initiative: A Review and Country Case Studies. London
School of Hygiene and Tropical Medicine.

65
Msamanga, G.I., Urassa, D.P. and Mujinja, P.G.M. (1996). Equity of Access to Public,
Private not for Profit and Private for Profit Health Facilities
in Two Regions of Tanzania. A Research Report Submitted to
UNICEF New York and Ottawa Canada.
Mujinja, P. and Mabala, R. (1992). Charging for Health Services in Non -
Governmental Health Facilities in Tanzania. Bamako
Initiative Technical Report Series No.7. UNICEF, New York.
Mwabu, G. and Wang’ombe, J. (1995). User Charges in Kenya: Health Services
Pricing Reform in Kenya: 1989 – 1993 International Health
Policy Program Working Paper.
National Health Insurance Fund Act (1999). Law of Tanzania Chapter 408.
National Health Insurance Corporation (2008). South Korea.
National Health Insurance Fund (2006). Annual Report 2005/2006.
National Health Insurance Fund (2012). Report Submitted to the Members of the
Permanent Committee of Social Services of the Parliament of
Tanzania.
Newbrander, W. and Sacca, S. (1996). Cost Sharing and Access to Health Care for
Poor: Equity Experiences in Tanzania. A study Carried Out
Under Basics Project for USAID, Africa Bureau.
Nolan, B. and Turbat, V. (1993). Cost Recovery in Public Health Services in Sub-
Saharan Africa. Economic Development Institute, World
Bank. Washington D.C

66
Nolan, B. and Turbat, V. (1995). Cost Recovery in Health Services in Sub-Saharan
Africa. World Bank: Washington D.C
Norm, C. and Weber, A. (1994). Social Health Insurance; A Guide Book for Planning.
Parasurman, A., Zeithaml, V.A., & Berry, L.L., (1988). A Conceptual Model of
Service Quality and its Implications for Future Research.
Journal of Marketing, 49: 41 – 50.
Russel, S. and Gilson, L. (1997). User Fees Policies to Promote Health Service Access
for the Poor: International Journal of Health Services, Vol
27(2): 359-379.
Shafaeddin, S.M., (2004). Who is the Master? Who is the Servant? Market or
Government? An Alternative Approach: Towards a
Coordination system. United Nations Conference on Trade
and Development Discussion Paper No 175. Available from:
http://www.unctad/org/DP/2004/9 [Accessed 25/03/2013].
Shaw, R. (1995). User Fees in Sub-Saharan Africa; Aims, Findings and Policy
Implications. World Bank Discussion Papers, Africa
Technical Series 294. World Bank: Washington D.C
Shepard, D., Vian, K. and Kleinau, E.F. (1995). Performance of Four Health Insurance
Programs in Rural and Urban Areas of Democratic Republic
of Congo in Financing Health Services Through User Fees and
Insurance. Case studies From Sub-Saharan Africa. World
Bank Discussion Papers 294.
Shillingi, V. and Mutalemwa, D.K. (2012). Health Services Delivery by Bukoba
Municipal Council: What has Quality got to do with it? ESRF
Discussion Paper.

67
The United Republic of Tanzania, (1994). Proposal for Health Sector Reforms.
Ministry of Health. Dar es Salaam.
The United Republic of Tanzania, (1997). Proposal for National Health Insurance
Scheme for Formal Sector Employees. Ministry of Health. Dar
es Salaam.
The United Republic of Tanzania, (1999). Evaluation of Cost Sharing Program
Implementation of User Fees in Public Hospitals in Tanzania.
Ministry of Health. Dar es Salaam.
The United Republic of Tanzania, (2000). Quality Assurance Training Guidelines for
Health Workers. Ministry of Health. Dar es Salaam.
The United Republic of Tanzania, (2001). Tanzania Performance Improvement
Initiative; Assessment of Community Perceptions on Quality
of Services. Ministry of Health. Dar es Salaam.
The United Republic of Tanzania (2002). National Health Policy. Ministry of Health.
Dar es Salaam.
The United Republic of Tanzania (2008). Health Sector Strategic Plan III July 2009 –
June 2015.Ministry of Health and Social Welfare. Dar es
Salaam.
The World Fact Book (2008). Population Estimation.
Van der Geest, S. (2002). User Fees and Drugs; What Did the Health Reform in
Zambia Achieve? Journal of Health Policy and Planning, Vol
15 (1): 59 – 65.
White, B. (2002). Writing your MBA dissertation. London: Continuum.

68
Winston, C. (2006). Government Failure versus Market Failure. Microeconomics
Policy Research and Government Performance. Available
from: http://www.barnesandnoble.com/w/government-failure-
versus-market-failure-clifford-winston [Accessed
25/03/2013].
World Bank (1993). World Development Report: Investing in Health. World Bank:
Washington D.C.
APPENDICES
Appendix 1: The Informed Concert
Hallo, I am doing a study on Delivery of Health Care Services in Kinondoni Municipal
Health Facilities with a particular attention to Civil servants using NHIF. I am coming
from Mzumbe University. The information obtained from this study will help to
inform the policy makers and implementers about the quality of health care services
as perceived by users, and will help them to make appropriate changes so as to improve
quality of health care services in Kinondoni municipal health facilities.
All information obtained from this study will be confidential and will only be used for
the purpose of the study. It will not be disclosed or released to anyone except the
authorized person. Your participation is voluntary and will be highly appreciated. Your
name will not appear on the questionnaire therefore, nobody will be able to know from
whom the information has been obtained.

69
Do you agree to be interviewed? (Start interview if he/she responds positively, if
respond negatively thank him/her and approach another client).

70
Appendix 2: Client Questionnaire (English Version)
QUESTIONNAIRE NO ………………………………………….……………………
DATE……………………………………………………………………………..……
NAME OF THE INTERVIEWER……………………………………………..………
NAME OF THE HEALTH FACILITY…………………………………………..……
1. Sex: Male…………………… Female…………………(tick appropriate)
2. Age (in years)…………………………………………………………………
3. Marital status (circle the appropriate)
(i) Single
(ii) Married
(iii) Divorced
(iv) Widowed
4. Educational status
(i) Primary education
(ii) Secondary education
(iii) Post secondary education
(iv) Others (specify)………………………………………………………
5. Where do you live?..…………………...……………………………………
6. Which mode of transport did you use to come here?
(i) On foot
(ii) Public transport
(iii) Tax
(iv) Others (specify)………………………………………………………
71
7. What is the reason that made you to come to this health facility? (multiple
answers are allowed)
(i) Close to where I live
(ii) Directed by a friend/relative
(iii) A friend/relative works here
(iv) I was given a referral
(v) Good quality of health care services
8. How did you pay for the health care services that you have received today?
(i) Through NHIF
(ii) Through user fees
9. For how long have you been a member of NHIF? ........................................
10. What is the problem(s) that made you to come to this health facility?
(State)…………………………………………………………………………
11. On a scale of 1 – 5 upon arriving at the reception how were you received by
the health worker?
(i) Very politely
(ii) Politely
(iii) Neutral
(iv) Not politely
(v) Rude
12. On a scale of 1 – 5 how did the doctor receive you when you entered the
doctor’s room?
(i) Very politely
(ii) Politely
(iii) Neutral
(iv) Rude
(v) Very rude
72
13. On a scale of 1 – 5 did you feel comfortable when you were explaining your
problems to the doctor?
(i) Very comfortable
(ii) Comfortable
(iii) Neutral
(iv) Uncomfortable
(v) Very uncomfortable
14. On the scale of 1- 5, in your opinion how did you find the time the doctor spent
listening to you?
(i) Adequate
(ii) Inadequate
(iii) Too long
(iv) I don’t know
(v) Very short
15. Were you told what disease is affecting you?
(i) Strongly agree
(ii) Agree
(iii) Neutral
(iv) Disagree
(v) Strongly disagree
16. What type of health problem do you have?
(i) Acute
(ii) Chronic
73
17. On a scale of 1 – 5 did the doctor give you adequate explanations about your
health problem?
(i) Strongly agree
(ii) Agree
(iii) Neutral
(iv) Disagree
(v) Strongly disagree
18. On a scale of 1 – 5 were you given an opportunity to ask questions regarding
to your health problem?
(i) Strongly agree
(ii) Agree
(iii) Neutral
(iv) Disagree
(v) Strongly disagree
19. On the scale of 1 – 5 were you given counseling regarding to your health
problem?
(i) Strongly agree
(ii) Agree
(iii) Neutral
(iv) Disagree
(v) Strongly disagree
20. On the scale of 1 – 5 did the doctor examine you physically?
(i) Strongly agree
(ii) Agree
(iii) Neutral
(iv) Disagree
(v) Strongly disagree
74
21. Were you given explanation about the procedure before you were examined?
(i) Strongly agree
(ii) Agree
(iii) Neutral
(iv) Disagree
(v) Strongly disagree
22. How did you find the time the doctor spent in examining you?
(i) Adequate
(ii) Inadequate
(iii) Too long
23. Was the nurse present during physical examination?
(i) Strongly agree
(ii) Agree
(iii) Neutral
(iv) Disagree
(v) Strongly disagree
24. On the scale of 1 – 5 did the doctor recommend any investigations?
(i) Strongly agree
(ii) Agree
(iii) Neutral
(iv) Disagree
(v) Strongly disagree
25. On a scale of 1 – 5 if yes, were you able to get all investigations done?
(i) Strongly agree
(ii) Agree
(iii) Neutral
(iv) Disagree
(v) Strongly disagree

75
26. If no, what is the reason(s) why the investigations were not done? (multiple
answers are allowed)
(i) Non functioning equipment
(ii) Reagents out of stock
(iii) Technician was not present
(iv) The investigation was not done at the health facility
(v) Others (specify)………………………………………………………
27. Where you told how your disease would be managed?
(i) Strongly agree
(ii) Agree
(iii) Neutral
(iv) Disagree
(v) Strongly disagree
28. Were any medicines prescribed for you?
(i) Strongly agree
(ii) Agree
(iii) Neutral
(iv) Disagree
(v) Strongly disagree
29. If yes, did you get all the prescribe medicine?
(i) Strongly agree
(ii) Agree
(iii) Neutral
(iv) Disagree
(v) Strongly disagree
30. Is there any reason why you did not get all or some of the prescribed medicine?
76
(i) Strongly agree
(ii) Agree
(iii) Neutral
(iv) Disagree
(v) Strongly disagree
31. Where you given enough instructions on how to use the prescribed medicine?
(i) Strongly agree
(ii) Agree
(iii) Neutral
(iv) Disagree
(v) Strongly disagree
32. Were you told the side effects of the medicines prescribed?
(i) Strongly agree
(ii) Agree
(iii) Neutral
(iv) Disagree
(v) Strongly disagree
33. In your opinion how do you find the availability of medicines in this health
facility?
(i) Always available
(ii) Available
(iii) Sometime available
(iv) Not available
34. Were you told next appointment?
(i) Strongly agree

77
(ii) Agree
(iii) Neutral
(iv) Disagree
(v) Strongly disagree
35. Have you been to any other health facility to get treatment for the same
problem?
(i) Strongly agree
(ii) Agree
(iii) Neutral
(iv) Disagree
(v) Strongly disagree
36. Do you know how much you have paid for various services that you have
received?
(i) Registration…………………………………….………………………
(ii) Medicines………………………………………………………………
(iii) Investigations………………………………………………………..…
(iv) Others………………………………………………………………..…
37. On the scale of 1 – 5 in your opinion were the services that you have received
worth the money you paid?
(i) Strongly agree
(ii) Agree
(iii) Neutral
(iv) Disagree
(v) Strongly disagree
38. On a scale of 1 – 5 in your opinion how did you find the time you spent to get
services in various departments?
(i) Adequate
78
(ii) Inadequate
(iii) Reasonable
(iv) Too long
(v) Too short
39. On a scale of 1 – 5 how did you find the comfort ability of the waiting area?
(i) Very satisfactory
(ii) Satisfactory
(iii) Neutral
(iv) Poor
(v) Very poor
40. On a scale of 1 – 5 in your opinion how did you find the attitude of health
workers whom you came into contact with?
(i) Very satisfactory
(ii) Satisfactory
(iii) Neutral
(iv) Poor
(v) Very poor
41. Please give explanations of your answer………………………………………
42. On scale of 1 – 5 how did you find the cleanliness of the facility building?
(i) Very satisfactory
(ii) Satisfactory
(iii) Neutral
(iv) Poor
(v) Very poor
43. On a scale of 1 – 5 how did you find the cleanliness of the surroundings?
(i) Very satisfactory
(ii) Satisfactory
79
(iii) Not satisfactory
(iv) Poor
(v) Very poor
44. On the scale of 1 – 5 what can you say about physical state of the buildings?
(i) Very good
(ii) Satisfactory
(iii) Neutral
(iv) Poor
(v) Very poor
45. Please give explanation of your answer………………………………………
46. In your opinion how do you perceive about the quality of health care services
provided in this health facility?
(i) Very good
(ii) Good
(iii) Satisfactory
(iv) Poor
(v) Very poor
47. Are you satisfied with the quality of health services that you have received
today?
(i) Strongly agree
(ii) Agree
(iii) Neutral
(iv) Disagree
(v) Strongly disagree
48. In your opinion do health workers use good language?
(i) Strongly agree
(ii) Agree
80
(iii) Neutral
(iv) Disagree
(v) Strongly disagree
49. In your opinions are staffs well trained?
(i) Strongly agree
(ii) Agree
(iii) Neutral
(iv) Disagree
(v) Very disagree
50. In your opinions how can the quality of health care services in this health
facility improved?
…………………………………………………………………………………
…………………………………………………………………………………
…………………………………………………………………………………
…………………………………………………………………………………
…………………………………………………………………………………
…………………………………………………………………………………
…………………………………………………………………………………
…………………………………………………………………………………
81
Appendix 3: Clients Questionnaire (Swahili Version)
FOMU YA MASWALI
SWALI NAMBA……………………………………………………………………
TAREHE…………………………………………………………………………….
JINA LA MUULIZA MASWALI…………………………………………………..
1. Jinsia: Mwanaume…………………….Mwanamke…………………………
2. Umri (miaka)…………………………………………………………………
3. Hali ya ndoa (zungushia jibu sahihi)
(i.) Sijaoa/sijaolewa
(ii.) Nimeoa/nimeolewa
(iii.) Nimeachika
(iv.) Mjane
4. Kiwango cha elimu
(i.) Elimu ya msingi
(ii.) Elimu ya sekondari
(iii.) Zaidi ya elimu ya sekondari
(iv.) Elimu nyingine (eleza)
5. Unaishi wapi?.....................................................................................................
6. Umetumia usafiri gani kuja hapa?
(i.) Kwa miguu
(ii.) Kwa usafiri wa umma
(iii.) Kwa teksi
(iv.) Usafiri wa aina nyingine (eleza)
82
7. Sababu iliyosababisha uje kupata matibabu hapa (jibu zaidi ya moja
linaruhusiwa)
(i.) Karibu na mahali ninapoishi
(ii.) Nimeelekezwa na rafiki/jamaa
(iii.) Nilipewa rufaa
(iv.) Huduma nzuri afya zinazotolewa
8. Umelipia gharama za matibabu uliyopata kwa njia gani?
(i.) Kwa kutumia bima ya afya
(ii.) Kwa kutumia malipo kwa mtumiaji
9. Umekuwa mwanachama wa mfuko wa bima ya afya kwa muda gani?
10. Tatizo gani limesababisha uje kupata matibabu hapa?
11. Katika skeli ya 1 – 5 ulipofika hospitali ulipokelewaje na mtoa huduma?
(i.) Kwa ukarimu sana
(ii.) Kwa ukarimu
(iii.) Kawaida
(iv.) Bila ukarimu
(v.) Kwa jeuri
12. Katika skeli ya 1 – 5 daktari alikupokeaje ulipoingia ofisini kwake ?
(i.) Kwa ukarimu sana
(ii.) Kwa ukarimu
(iii.) Kawaida
(iv.) Kwa jeuri
(v.) Kwa jeuri sana

83
13. Katika skeli ya 1 – 5 ulijisikiaje wakati unamweleza daktari matatizo yako?
(i.) Vizuri sana
(ii.) Vizuri
(iii.) Kawaida
(iv.) Vibaya
(v.) Vibaya sana
14. Katika skeli ya 1 – 5 kwa maoni yako unaoje muda aliotumia daktari kusikiliza
Matatizo yako ?
(i) Unatosha
(i.) Hautoshi
(ii.) Mrefu sana
(iii.) Sijui
(iv.) Mfupi sana
15. Uliambiwa unasumbuliwa na ugonjwa gani ?
(i.) Niliambiwa kabisa
(ii.) Niliambiwa
(iii.) Sina uhakika
(iv.) Sikuambiwa
(v.) Sikuambiwa kabisa
16. Una tatizo gani la kiafya?
(i.) La muda mfupi
(ii.) La muda mrefu
84
17. Katika skeli ya 1 – 5 daktari alikupa maelezo ya kutosha kuhusu matatizo yako
Ya kiafya?
(i.) Nakubaliana kabisa
(ii.) Nakubali
(iii.) Sina uhakika
(iv.) Sikubali
(v.) Sikubaliani kabisa
18. Katika skeli ya 1 – 5 ulipewa muda wa kuuliza maswali kuhusu matatizo yako
Ya kiafya ?
(i.) Nakubalina kabisa
(ii.) Nakubali
(iii.) Sina uhakika
(iv.) Sikubali
(v.) Sikubaliani kabisa
19. Katika skeli ya 1 – 5, ulipewa ushauri nasaha kuhusu matatizo yako ya kiafya?
(i.) Ndiyo, nilipewa
(ii.) Nilipewa
(iii.) Sina uhakika
(iv.) Sikupewa
(v.) Sikupewa kabisa
20. Katika skeli ya 1 – 5 daktari alikupima?
(i.) Ndiyo, alinipima
(ii.) Alinipima
(iii.) Sina uhakika
(iv.) Hakunipima
(v.) Hakunipima kabisa
21. Katika skeli ya 1 – 5, ulipewa maelezo kabla ya kupimwa ?

85
(i.) Ndiyo nilipewa
(ii.) Nilipewa
(iii.) Sina uhakika
(iv.) Sikupewa
(v.) Sikupewa kabisa
22. Unaonaje muda aliotumia daktari kukupima?
(i.) Unatosha
(ii.) Hautoshi
(iii.) Mrefu sana
23. Katika skeli ya 1 – 5, nesi alikuwepo wakati unapimwa?
(i.) Ndiyo, alikewepo
(ii.) Alikuwepo
(iii.) Sina uhakika
(iv.) Hakuwepo
(v.) Hakuwepo kabisa
24. Katika skeli ya 1 – 5, daktari alishauri ufanyiwe vipomo?
(i.) Ndiyo, alishauri
(ii.) Alishauri
(iii.) Sina uhakika
(iv.) Hakushauri
(v.) Hakushauri kabisa
25. Katika skeli ya 1 – 5, kama alishauri, ulipata vipomo vyote?
(i.) Ndiyo, nilipata
(ii.) Nilipata
(iii.) Sina uhakika
(iv.) Sikupata
(v.) Sikupata kabisa
26. Kama hukupata, kwanini hukupata (jibu zaidi ya moja linaruhusiwa)
86
(i.) Vifaa vya kupimia vilikuwa havifanyi kazi
(ii.) Hakukuwa na kemikali za kupimia
(iii.) Hapakuwa na mtaalam wa kupima
(iv.) Kipimo hakikuwa kinafanyika hapo
(v.) Sababu zingine (eleza)
27. Katika skeli ya 1 – 5, uliambiwa jinsi ugonjwa wako utavyotibiwa?
(i.) Ndiyo, niliambiwa
(ii.) Niliambiwa
(iii.) Sina uhakika
(iv.) Sikuambiwa
(v.) Sikuambiwa kabisa
28. Katika skeli ya 1 – 5, uliandikiwa dawa?
(i.) Ndiyo niliandikiwa
(ii.) Niliandikiwa
(iii.) Sina uhakika
(iv.) Sikuandikiwa
(v.) Sikuandikiwa kabisa
29. Katika skeli ya 1 – 5, kama uliandikiwa, ulipata dawa zote?
(i.) Ndiyo, nilipata zote
(ii.) Nilipata
(iii.) Sina uhakika
(iv.) Sikupata
(v.) Sikupata kabisa
30. Katika skeli ya 1 – 5, kuna sababu iliyosababisha usipate dawa zote?
87
(i.) Ndiyo, ipo
(ii.) Ipo
(iii.) Sina uhakika
(iv.) Hakuna
(v.) Hakuna kabisa
31. Katika skeli ya 1 – 5, ulipewa maelezo kuhusu utumiaji wa dawa?
(i.) Ndiyo nilipewa
(ii.) Nilipewa
(iii.) Sina uhakika
(iv.) Sikupewa
(v.) Sikupewa kabisa
32. Katika skeli ya 1 – 5, uliambiwa madhara ya hizo dawa?
(i.) Ndiyo, niliambiwa
(ii.) Niliambiwa
(iii.) Sina uhakika
(iv.) Sikuambiwa
(v.) Sikuambiwa kabisa
33. Kwa maoni yako unaonaje upatikanaji wa dawa katika hospitali hii?
(i.) Zinapatikana muda wote
(ii.) Zinapatikana
(iii.) Wakati mwingine zinapatikana
(iv.) Hazipatikani
34. Katika skeli ya 1 – 5, uliambiwa tarehe ya kurudi?

88
(i.) Ndiyo, niliambiwa
(ii.) Niliambiwa
(iii.) Sina uhakika
(iv.) Sikuambiwa
(v.) Sikuambiwa kabisa
35. Uliwahi kufika katika hospitali yoyote kupata matibabu kwa tatizo hili?
(i.) Ndiyo, niliwahi
(ii.) Niliwahi
(iii.) Sina uhakika
(iv.) Sijawahi
(v.) Sijawahi kabisa
36. Unajua gharama uliyolipia huduma mbalimbali za matibabu ulizopata?
(i.) Kujiandikisha…………………………………………………………..
(ii.) Dawa………………………………………………………….……….
(iii.) Vipimo…………………………………………………………………
(iv.) Huduma nyingine……………………………………………….……..
37. Katika skeli ya 1 – 5, huduma ulizopata zinalingana na gharama uliyolipa?
(i.) Ndiyo, zinalingana
(ii.) Zinalingana
(iii.) Sina uhakika
(iv.) Hazilingani
(v.) Hazilingani kabisa
38. Katika skeli ya 1 – 5, kwa maoni yako unaonaje muda uliotumia kupata
huduma Katika idara mbalimbali?
89
(i.) Unatosha
(ii.) Hautoshi
(iii.) Kawaida
(iv.) Mrefu sana
(v.) Mfupi sana
39. Katika skeli ya 1 – 5, unaonaje sehemu ya mapokezi?
(i.) Inaridhisha sana
(ii.) Inaridhisha
(iii.) Kawaida
(iv.) Hairidhishi
(v.) Hairidhishi kabisa
40. Katika skeli ya 1 – 5, kwa maoni yako unaonaje mwenendo wa watoa huduma?
(i.) Unaridhisha sana
(ii.) Unaridhisha
(iii.) Kawaida
(iv.) Mbaya
(v.) Mbaya sana
41. Tafadhali, toa maelezo ya jibu lako
…………………………………………………………………………………
42. Katika skeli ya 1 – 5, unaonaje usafi wa majengo ya hospitali hii?
(i.) Unaridhisha sana
(ii.) Unaridhisha
(iii.) Kawaida
(iv.) Hauridhishi
(v.) Hauridhishi kabisa
43. Katika skeli ya 1 – 5, unaonaje usafi wa mazingira ya hospitali hii?
(i.) Unaridhisha sana
(ii.) Unaridhisha
90
(iii.) Kawaida
(iv.) Hauridhishi
(v.) Hauridhishi kabisa
44. Katika skeli ya 1 – 5, unasemaje kuhusu hali ya majengo?
(i.) Nzuri sana
(ii.) Nzuri
(iii.) Inaridhisha
(iv.) Mbaya
(v.) Mbaya sana
45. Tafadhali, toa maelezo ya jibu lako
…………………………………………………………………………………
…………………………………………………………………………………
…………………………………………………………………………………
46. Kwa maoni yako unaonaje ubora wa huduma zitolewazo katika hospitali hii?
(i.) Nzuri sana
(ii.) Nzuri
(iii.) Zinaridhisha
(iv.) Mbaya
(v.) Mbaya sana
47. Katika skeli ya 1 – 5, umeridhika na ubora wa huduma ulizopata leo?
(i.) Nimeridhika sana
(ii.) Nimeridhika
(iii.) Kawaida
(iv.) Sijaridhika
(v.) Sijaridhika kabisa
48. Kwa maoni yako, watoa huduma wanatumia lugha nzuri?
(i.) Ndiyo, nakubali
(ii.) Nakubali
91
(iii.) Kawaida
(iv.) Sikubali
(v.) Sikubali kabisa
49. Kwa maoni yako, watoa huduma ya afya wamepata mafunzo ya kutosha?
(i.) Nakubali kabisa
(ii.) Nakubali
(iii.) Kawaida
(iv.) Sikubali
(v.) Sikubali kabisa
50. Kwa maoni yako, kwa namna gani huduma za afya zinaweza kuboreshwa?
.............................................................................................................................
.............................................................................................................................
.............................................................................................................................
.............................................................................................................................
Appendix 4: Facility Check List to Assess Health Services Delivered
CHECK LIST NO…………………………………………………………………….
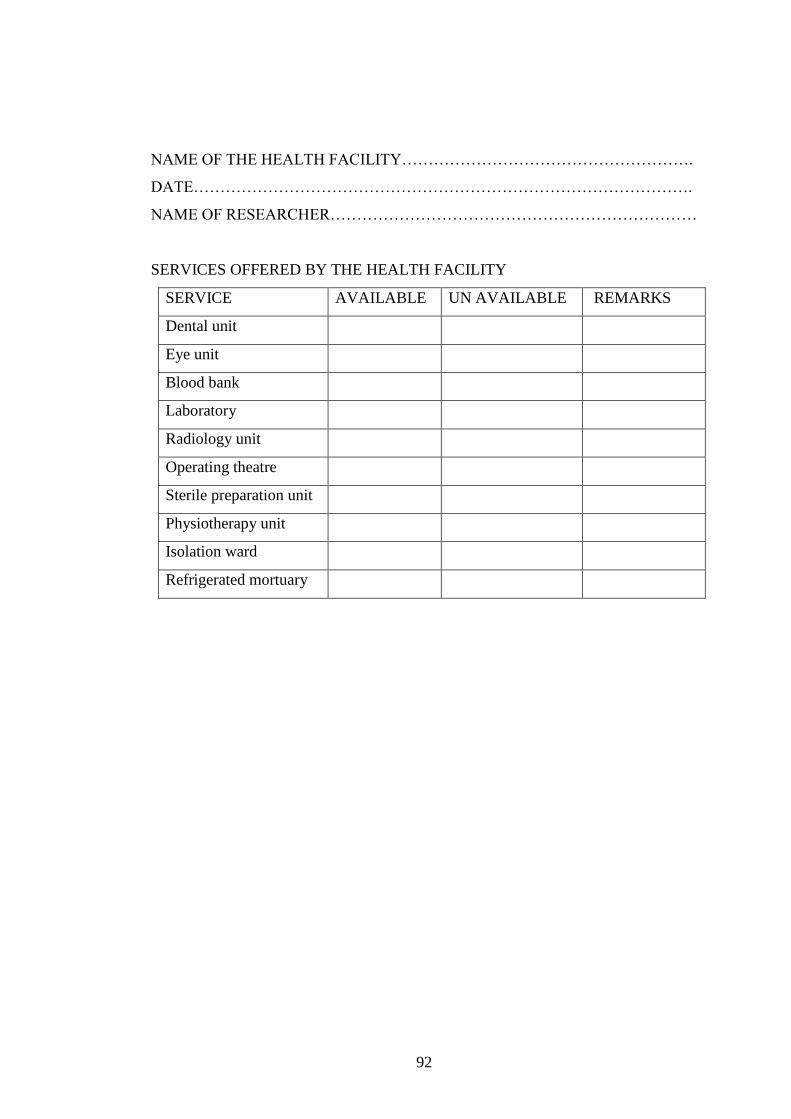
92
NAME OF THE HEALTH FACILITY……………………………………………….
DATE………………………………………………………………………………….
NAME OF RESEARCHER……………………………………………………………
SERVICES OFFERED BY THE HEALTH FACILITY
SERVICE AVAILABLE UN AVAILABLE REMARKS
Dental unit
Eye unit
Blood bank
Laboratory
Radiology unit
Operating theatre
Sterile preparation unit
Physiotherapy unit
Isolation ward
Refrigerated mortuary





























