Embed Size (px)
Citation preview
Current Concepts
(Kth
HMK
Fth
E
The Disabled Throwing Shoulder: Spectrumof Pathologyd10-Year Update
W. Ben Kibler, M.D., John E. Kuhn, M.D., Kevin Wilk, P.T., D.P.T.,Aaron Sciascia, M.S., A.T.C., N.A.S.M.-P.E.S., Stephanie Moore, M.S., A.T.C.,
Kevin Laudner, Ph.D., A.T.C., Todd Ellenbecker, P.T.,Chuck Thigpen, Ph.D., P.T., A.T.C., and Tim Uhl, Ph.D., A.T.C., P.T., F.N.A.T.A.
Abstract: In the 10 years since the current concept series entitled “The Disabled Throwing Shoulder: Spectrum ofPathology” was conceived and written, many studies have been reported that add much more information to theunderstanding of the disabled throwing shoulder (DTS). The editors of Arthroscopy and the authors of the original seriesbelieved that an update to the original series would be beneficial to provide an organized overview of current knowledgethat could update the thought process regarding this problem, provide better assessment and treatment guidelines, andguide further research. A dedicated meeting, including current published researchers and experienced clinicians in thissubject, was organized by the Shoulder Center of Kentucky. The meeting was organized around 5 areas of the DTS thatwere highlighted in the original series and appear to be key in creating the DTS spectrum and to understanding andtreating the DTS: (1) the role of the kinetic chain; (2) the role and clinical evaluation of the scapula; (3) the role of deficitsin glenohumeral rotation, glenohumeral internal rotation deficit, and total range-of-motion deficit in the causation oflabral injury and DTS; (4) the role of superior labral (SLAP) injuries and rotator cuff injuries; and (5) the composition andprogression of rehabilitation protocols for functional restoration of the DTS. The meeting consisted of presentations withineach area, followed by discussions, and resulted in summaries regarding what is known in each area, what is not knownbut thought to be important, and strategies to implement and enlarge the knowledge base.
he series of articles entitled “The Disabled Throwing1-3
TShoulder: Spectrum of Pathology” presented asystematic, holistic overview of the known mechanics ofthe overhead throwing motion and a proposed relationof the mechanics to the dysfunction associated with
From the Shoulder Center of Kentucky (W.B.K., A.S.), Lexington, Kentucky; Va.W.), Birmingham, Alabama; the University of Kentucky (S.M., T.U.), Lexingerapy Associates (T.E.), Phoenix, Arizona; and Proaxis Physical Therapy (C.T.)The attendees of the Disabled Throwing Shoulder Summit were as follows: Tim Bawkins, M.D., W. Ben Kibler, M.D., Jed Kuhn, M.D., Kevin Laudner, Ph.D., A.D., Felix Savoie III, M.D., Aaron Sciascia, M.S., A.T.C., N.A.S.M.-P.E.S., Chuckevin Wilk, P.T.The consensus meeting was facilitated by an educational grant from Arthrex.The authors report the following potential conflict of interest or source of fundinunding provided partial data that were presented at the meeting. T.U. received ane Lexington Clinic in the amount of $250.00.Received June 11, 2012; accepted October 3, 2012.Address correspondence to Aaron Sciascia, M.S., A.T.C., N.A.S.M.-P.E.S., Shoul-mail: [email protected]� 2013 by the Arthroscopy Association of North America0749-8063/12406/$36.00http://dx.doi.org/10.1016/j.arthro.2012.10.009
Note: To access the supplementary tables and figures accompawww.arthroscopyjournal.org.
Arthroscopy: The Journal of Arthroscopic and Related Su
injuries to the shoulder. Through its emphasis on thekinetic chain contributions to force generation for themotion, possible sequencing of the pathophysiologic“cascade of injury,” treatment of all of the componentsof the intra-articular injuries, and the role of rehabilitation
nderbilt University (J.E.K.), Nashville, Tennessee; Champion Sports Medicineton, Kentucky; Illinois State University (K.L.), Bloomington, Illinois; Physio-, Greenville, South Carolina, U.S.A.utterfield, Ph.D., A.T.C., John Conway, M.D., Todd Ellenbecker, P.T., Richard.T.C., David Lintner, M.D., Stephanie Moore, M.S., A.T.C., Anthony Romeo,Thigpen, Ph.D., P.T., A.T.C., Tim Uhl, Ph.D., A.T.C., P.T., F.N.A.T.A., and
g in relation to this article: Major League Baseball Medical Grant Program.honorarium for attending and presenting at the meeting. Funds received from
der Center of Kentucky, 1221 South Broadway, Lexington, KY 40504, U.S.A.
nying this report, visit the January issue of Arthroscopy at
rgery, Vol 29, No 1 (January), 2013: pp 141-161 141

142 W. B. KIBLER ET AL.
in correcting all of the deficits, this series suggesteda common starting point for discussion of these injuriesand for future research.In the 10 years since this series was conceived and
written,many studies have been reported that addmuchmore information to the understanding of the disabledthrowing shoulder (DTS). The editors of Arthroscopy andthe authors of the original series believed that an updateto the original series would be beneficial to provide anorganized overview of current knowledge that couldupdate the thought process regarding this problem,provide better assessment and treatment guidelines, andguide further research.A dedicated meeting, including current published
researchers and experienced clinicians in this subject,was organized by the Shoulder Center of Kentucky. Themeeting was organized around 5 areas of the DTS thatwere highlighted in the original series and appear to bekey in creating the DTS spectrum and to understandingand treating the DTS: (1) the role of the kinetic chain; (2)the role and clinical evaluation of the scapula; (3) therole of deficits in glenohumeral (GH) rotation, gleno-humeral internal rotation deficit (GIRD), and total range-of-motion deficit (TROMD) in the causation of labralinjury and DTS; (4) the role of superior labral (SLAP)injuries and rotator cuff injuries; and (5) the compositionand progression of rehabilitation protocols for functionalrestoration of the DTS. The meeting consisted of presen-tations within each area, followed by discussions, andresulted in summaries regarding what is known in eacharea, what is not known but thought to be important, andstrategies to implement and enlarge the knowledge base.Each presentation included summaries of publishedstudies in each area and included the most currentongoing research studies from thepresenters’ institutions.Writing groups and editors then synthesized the infor-mation and consensus for each area. This article is in-tended to provide an overview of current research andconsidered opinion on this subject. As such, its purpose isthe same as the original series, but it reflects the progressin knowledge on this subject, highlights what is known,explores controversies, and suggests future directions.
Kinetic Chain, Scapula, and GHRotation Deficits
The DTS is most frequently the result of a process thatinvolves deficits in body segments that are proximal tothe shoulder and affect the shoulder joint anatomy.
Role of Kinetic ChainThe evidence that the overhead throwing motion is
developed and regulated through a sequential coordi-nated and task-specific kinetic chain of force develop-ment and a kinematic chain of sequential body positionsand motions is clearly established.4-7 This allows a uni-fying concept to understand the mechanics of the
overhead throwing motion. The term “kinetic chain” isused collectively to describe the results of both of thechains. The kinetic chain has several functions: (1)using integrated programs of muscle activation totemporarily link multiple body segments into 1 func-tional segment (e.g., the back leg in the cocking stanceand push off and the arm in long-axis rotation beforeball release or ball impact) to decrease the degrees offreedom in the entire motion7-9; (2) providing a stableproximal base for distal arm mobility; (3) maximizingforce development in the large muscles of the core andtransferring it to the hand6,8,10; (4) producing interac-tive moments at distal joints that develop more forceand energy than the joint itself could develop anddecrease the magnitude of the applied loads at the distaljoint4,11-15; and (5) producing torques that decreasedeceleration forces.4,14-17
The clinical implications of the use of the kinetic chainfor performance have been reported in several studies.At ball release, only 4 body motionsdtrunk rotation,shoulder internal rotation, elbow extension, and wristflexiondcontribute positively to ball velocity. However,all of the positive contributions to elbow extensionand wrist flexion are by interactive moments producedby proximal sequences of motion and position.11,13 Intennis, maximal speed of the racquet at ball impact iscorrelated most highly with the velocity of the back hipgoing from its lowest position in cocking to its highestposition in follow through.18 The difference in velocityof a baseball throw from slow to fast is most correlatedwith the speed of trunk rotation.11 The maximalvelocity of a ball throw is correlated to the extent ofbody segments used, with the slowest being arm usealone and the fastest being use of the legs and trunk.10
The sequential use of 5 key body positions and motionsis associated with maximal velocities and minimal jointloads.19 The fastest tennis serves are associated witha muscle activation pattern that uses the back legmuscles pushing up and through ball impact.20 Finally,the muscle pattern in baseball throwing involvessequential activation, both in onset timing and peakactivation, of the contralateral hip and oblique andabdominal muscles, proceeding to the posterior trunkmuscles and then to the scapula and shoulder muscles,ending in the proximal arm muscles.11
Clinical implications for injury risk have also beenreported. A mathematical model showed that a 20%reduction in trunk kinetic energy development resultedin a requirement of 33% more velocity or 70% moremass in the distal segments to maintain the sameenergy at ball impact.5 A tennis study showed that notadequately flexing the knees in the cocking phase whileserving resulted in a 17% increase in shoulder load anda 23% increase in elbow valgus load if resultant ballvelocity was maintained at speeds comparable to those inplayers flexing the knees.21 Decreased hip range of

DISABLED THROWING SHOULDER: 10-YEAR UPDATE 143
motion (ROM) is associated with shoulder injury andpoor throwing mechanics.22 Scapular dyskinesis is asso-ciated with rotator cuff disease,23 impingement,24-27 andinternal impingement.28-30
Methods of evaluation of kinetic chain function havebeen devised. Evaluation of kinetic chain function asa whole is difficult, because of the multi-segment,dynamic activity. Breaking the motion down into keypositions and motions that can be analyzed by videoor direct observation has been helpful. The baseballpitching motion can be evaluated by analyzing a set of 5progressive positions and motions (Table 1).19 Thetennis serve motion can be evaluated by analyzing a setof 6 “nodes,” or positions and motions that are corre-lated with optimal biomechanics (Table 1).8 These keypositions have been correlated with optimal forcedevelopment and minimal applied loads and can beconsidered the most efficient methods of coordinatingkinetic chain activation. There may be multiple indi-vidual variations in other parts of the kinetic chain, butthese are the most basic and the ones required to bepresent in all motions. Clinical evaluation of flexibilityand strength in the proximal kinetic chain segmentscan be helpful in determining deficits. Good screeningexaminations for hip/leg capability are the single-legstability series, 1-leg stance, and 1-leg half squat.31,32
Direct measurement of knee, hip, and back flexibility;strength; and rotation can be performed by standardphysical therapy measurements. A specific inclusiveprofile for evaluating anatomic areas most highlyassociated with shoulder injury, the High PerformanceProfile, has been developed by the United States TennisAssociation (http://www.usta.com/sportsmedicine).In summary, the kinetic chain is the mechanism by
which the body most effectively meets the demands ofthe overhead throwingmotion. The bodyworks as a unitin performance and may fail in multiple places in injury.
Table 1. Key Positions and Motions for Baseball Pitch andTennis Serve
Task Node
Baseball pitch Weight on back leg with trunk straightHip and trunk synchrony
Elbow at or above 90� of abduction withscapular retraction and hand on top of ball
Front foot directly toward home plateLong-axis rotation: shoulder internal
rotation and forearm pronation
Tennis serve Use of back foot to push offKnee flexion >10�
Back hip counter-rotation away fromnet and downward tilt
Trunk rotation away from net, with hip/trunkseparation angle of 30�
Arm cocking in scapular planeLong-axis rotation
A comprehensive evaluation program is necessary toevaluate the thrower, both in terms of injury potentialand understanding all alterations in injury. This willidentify the components of the “non-shoulder” deficitsthat are contributing to the shoulder injury and whoserestoration has been shown to maximize shoulderrehabilitation in addition to the shoulder deficits.33,34
However, there are limitations in the knowledgeregarding the kinetic chain. Although the kinetic chainalterations arewell documented in associationwith injuryand as negative contributors to optimal mechanics, it isunclear when these occur in the injury sequence and bywhat mechanisms they affect the DTS; moreover,the natural history of how they occur is unclear. It is notknownwhether they are exclusively a cause of pathologyor whether they are an effect of other pathologies. It isalso not known whether early identification and correc-tionof the alterationshave significant impact on improvedperformance or decreased injury incidence. Long-termlongitudinal studies areneeded to supply this information.Further studies should be performed to completely
characterize the kinetic chains of all overhead throwingactivities. Easily implemented and reliable clinical eval-uation methods for kinetic chain capability must beestablished, data on the cause-effect relation to the DTSshould be developed, and specific prevention studiesshould be organized.
Role of ScapulaStudies have accurately documented the composite
3-dimensional motions of the scapula in association witharm movement and throwing.35-38 They have showna pattern of progressive retraction, upward rotation,posterior tilt, and controlled internal/external rotationto maximize GH stability during arm motion. Throwershave specific compensations in position but display thesame direction of motions during arm motion.38 Devi-ations from these patterns are considered to haveimplications for injury.24,30,39,40
External shoulder impingement, internal shoulderimpingement,29 anterior capsular laxity,41 labral injury,1
and rotator cuff weakness,8 all of which can createsymptoms and/or exacerbate the dysfunction in the DTS,are found in associationwith scapular dyskinesis in a largepercentage of DTS patients.1,42 Addressing the dyskinesishas been shown to decrease impingement symptoms,43
improve rotator cuff strength,44 and decrease symptomsin labral injury (Stephanie Moore, data presented at theDisabled Throwing Summit). Specific rehabilitationprotocols have been developed to restore flexibility andstrength in the scapular stabilizing muscles. They includespecific methods of mobilizing the tight anterior coracoidmuscles (pectoralis minor, short head of the biceps) bycorner stretches.45 Early activation of the weakened andinhibited lower trapezius and serratus anterior can beachieved through the scapular stability series.33 More

144 W. B. KIBLER ET AL.
advanced rehabilitation can be achieved by prone exer-cises46 and kinetic chain diagonal exercises.47
To help establish the presence or absence of scapulardyskinesis in DTS patients and to thereby guide reha-bilitation efforts, an effective clinical observationmethodhas been developed.48-51 This method, recommendedafter a consensus meeting,50 has clinical utility similarto other tests of shoulder pathology and has beencorrelated with biomechanically determined scapularpositions and motions in symptomatic patients.51
The testing protocol starts with evaluation of inflexibil-ities (pectoralis minor52 and humeral rotation deficit53).The scapular resting position and dynamic motion can beevaluated by observing the scapula as the arms move intoforward flexion and descent.50 Medial border prominenceis characterized as “yes,” seen, dyskinesis present, or “no,”not seen, dyskinesis not present. Finally, the effect of dys-kinesis on symptoms can be estimated by correctivemaneuvers. The scapular assistance test creates posteriortilt and candecrease external impingement symptoms.54,55
The scapular retraction test54 or scapular reposition test56
creates external rotation and posterior tilt and can increasedemonstrated rotator cuff strength and decrease internalimpingement symptoms in labral injury.56,57
A rough measurement of pectoralis minor tightnessmay be obtained by having the patient stand againstthe wall and measuring the distance from the wall tothe anterior acromial tip. This can be performed witha “double-square” device with the patient standing withhis or her back against the wall.58 A bilateral measure-ment is taken (in inches or centimeters) to determinewhether there is a notable difference between theinvolved and noninvolved shoulder, with a side-to-sideasymmetry greater than 3 cm considered abnormal. Amore direct measurement can be obtained bymeasuringthe distance from the coracoid process to the fourth rib atthe rib/sternum articulation.52
In summary, the scapula plays key roles in shoulderfunction and the DTS. A clinically effective method ofevaluation has been developed, and specific effectiverehabilitation protocols exist.However, the precise correlation between scapular
position and injury is not known. It is unclear whetherscapular position is a cause or an effect, where in thecausation cascade it exerts its effects, and how muchalteration of the kinematics creates the pathologicallyrelated dyskinesis. It is also not known whether iden-tification or correction of dyskinesis is an effectiveinjury prevention activity.The most important future development would be to
move the evaluation process from a subjective evalua-tion that can reliably establish the presence or absence ofdyskinesis to an objective method that would also allowmeasurement and better determination of the effects oftreatment. Current investigations using a combinationof single planar measurements may provide an adequate
system. In addition, further information should bedeveloped regarding the exact cause and effect betweenscapular dyskinesis and the DTS.
GH Rotation DeficitsGH rotation has been identified as a key component in
normal and abnormal throwing mechanics. Alterationsin the magnitude of GH rotation are the most consis-tently found deficits associated with shoulder injury.Glenohumeral internal rotation (GIR) has receivedthe most attention, because it has been identified as keyto normal force development4,6; when altered beyondcertain levels, it changes GH kinematics1,59,60; and it isimplicated in shoulder30,61 and elbow injury.62 GIR isusually found to be asymmetrically decreased on thedominant side of throwers and servers. Glenohumeralexternal rotation (GER) has not been associated withinjury but is a key component of the cocking positioncoupled with shoulder horizontal abduction and scap-ular retraction. It is usually found to be asymmetricallyincreased on the dominant side. The total rotationalrange of motion (TROM) (GIR plus GER) is a usefulconcept to better understand the adaptations in rotationthat occur and gives early evidence of potentially dele-terious alterations in rotation. Most studies show thatTROM is symmetric in throwers and servers but shouldnot exceed 186� as an absolute number.Alterations in GIR and TROM become clinically
significant regarding injury risk when their magnitudebecomes associated with shoulder injury. The consensusof the meeting is that the terms “GIRD” and “TROMD”should be associated with only those rotation values atthe level of magnitude associated with injury and injuryrisk. However, there is lack of consensus about what thespecific threshold values should be. Traditional defini-tions suggested a side-to-side asymmetry in GIR greaterthan 20�. However, studies have shown that a GIRD ofas little as 11�63 and 18�61 is associated with shoulderinjury. In addition, a prospective study showed thata GIRD of 18� was related to a 1.9 times increased risk ofinjury.61 These values would also take into account thealteration in GIR due to osseous adaptation. However,because TROM should be symmetric, relatively smallchanges in symmetry of this number are likely signifi-cant. A 5� asymmetry in TROM has been shown to bepredictive of increased injury risk.61 The consensus ofthemeeting attendees is thatGIRDwill be definedas side-to-side asymmetry greater than 18� and TROMD willbe defined as side-to-side asymmetry greater than 5�.Although GIRD and TROMD may be considered predic-tive for shoulder injury, they are not causative by them-selves. They alter the normal GH kinematics and placeincreased load on adjacent joint structures, and theymaybe considered components of the shoulder at risk.59,60
Since alterations in GIR were first reported,64 multiplestudies have been conducted further describing it. GIR

DISABLED THROWING SHOULDER: 10-YEAR UPDATE 145
has been shown to decrease with years of throwingexposure,65,66 throughout a competitive season,67,68
and acutely after a throwing exposure.69,70 GIR andGIRD have also been shown to be different in theamount of change over 1 season between starters andrelievers.68 These data show that GIR, TROM, GIRD,and TROMD are dose or exposure dependent.Multiple studies have focused on possible bony, cap-
suloligamentous, and muscular factors for the observedand verified findings. Bony changes have been welldefined.71-73 Differential rotational strain has beenshown to alter the proximal humeral morphology,producing a slowing of the normal antetorsion processin the maturing bone, resulting in greater retrotorsion(Chuck Thigpen, data presented at summit). This changein torsion is reflected in a corresponding loss of GIR(C.T., data presented at summit). The 7 studies that haveexamined this difference show an average of an 11�
asymmetric decrease in GIR with a correspondingincrease in GER.71,72,74-78 It has been suggested that thisis a positive adaptation, with the increased GER allowingbetter ability to achieve the cocking position.3 Morerecent studies, presented at the dedicated meeting,suggest that the bony changes that create retrotorsionmay increase the posterior capsular and muscular strainas the arm moves into deceleration and create moresoft-tissue tension alteration (C.T., data presented atsummit). This would decrease the margin of safety intotal internal rotation so that further losses in GIR frommuscular or soft-tissue causes may be significant. Thismay explain the variability in the amount of GIR lossthat has been associated with labral injuries. Froma measurement standpoint, the bony changes alter themagnitude of degrees of GIR and GER, so a 10� to 12�
side-to-side asymmetry in GIR should not be consideredpathologic, as long as the TROM is symmetric.Capsuloligamentous changes that have been assumed
to result from scar tissue related to chronic tensileoverload have been well documented to alter GHkinematics.1,79 Experimental capsular plication has beenshown to cause the humeral head to displace anteriorly/superiorly in forward flexion and posteriorly/superiorlyin cocking.60 Thickened posterior capsules are com-monly seen on imaging of patients with superior labralinjuries,2,80 and clinical examinationand therapeutic tech-niques directed at detecting and correcting capsular com-ponents of joint mobility have been demonstrated.81-84
These changes do not account for the high percentage ofpatients without thickened capsules on imaging, for theacute changes in the magnitude of GIR after a throwingexposure,69,70 or for the frequently rapid alteration in GIRmeasurements with stretching programs.85,86 These moredynamic changes point to a muscular component incausation.The muscular component is related to acute and
chronic responses to strain, which then affect joint
ROM. An acute response to repetitive tensile strainin eccentric muscle contractions, actual “sarcomerepopping,” with separation of the sarcomere ends, hasbeen described.87,88 This muscle damage releases intra-muscular calcium, which mediates fibril contraction,resulting in muscle shortening. This process peaksbetween 4 and 18 hours after throwing and is modifi-able with gentle stretching at 12 hours. One chronicmuscle response to muscular strain is represented bythixotropy, an increased muscle stiffness that is medi-ated by exposure history of the muscle.88,89 Repetitiveexposure to strain can result in increased stiffnesswithin the muscles that can affect joint motion and isnot related to neurologic changes. The thixotropicresponse is modifiable by stretching within certainranges and velocities.87 Another muscle response isrelated to the architectural design of the rotator cuffmuscles. The pennation angle of these muscles makesthem most efficient at producing force through a shortmid ROM in abduction and internal rotation but alsomeans that they are poorly adapted to withstand largechanges in length.90 Experimental data suggest thatincreases in strain rate or strain length of these musclesbeyond their normal physiological limits will inducemuscular responses that increase internal stiffnessand decrease ROM.90 Data presented at the dedicatedmeeting showed that an exercise program thatincreased posterior shoulder muscle eccentric endur-ance and increased resistance to length change wasassociated with no loss of GIR through 1 baseball season(S.M., data presented at summit).Measurement accuracy of GH rotation is required for
evaluating these adaptations, because repeated measure-ments are required, and changes of 5� to 10� may bemeaningful. Most clinical studies now rely on the sameprotocol, with the arm at 90� of abduction in the plane ofthe scapula and using a bubble goniometer or digitalinclinometer.70,91
Each athlete should be placed in a supine positionon a flat, level surface. A second examiner should bepositioned above the athlete to properly stabilize thescapula during testing by applying a posteriorly directedforce to the coracoid to ensure that scapular movementdoes not occur. The humerus is supported on thesurface with the elbow placed at 90� and the arm ona bolster in the plane of the scapula.70 The followinglandmarks should be identified before placement of thegoniometer: the fulcrum set at the olecranon process ofthe elbow, the stationary arm perpendicular to the tableas documented by the bubble on the goniometer, andthe moving arm in line with the styloid process of theulna. The athlete’s humerus is then passively movedinto internal rotation. Rotation is taken to “tightness,”a point where no additional GH motion occurs unlessthe scapula moves or the examiner applies extra rota-tional stress. For external rotation, similar methods are

146 W. B. KIBLER ET AL.
used. TROM is then calculated as GIR plus GER. Theprocedures are repeated bilaterally to obtain measure-ments from both the throwing and non-throwingshoulder. This method has been shown to be highlyreproducible, with a test-retest reliability of 0.9670 andsensitivity to detection of meaningful change of 3�.The major gap in the knowledge regarding GIRD and
TROMD relates to the exact soft-tissue mechanisms thatcreate the motion loss and how much the bony adap-tations affect the “safe zone” of altered GIR. Moreprecise knowledge regarding the pathophysiology couldguide rehabilitation protocols to alter the progression ofthe deficit, provide the best conditioning to prevent thedeficit, and provide information about when GIRD iscontributing to the “shoulder at risk” of injury.1 Moreinformation should also be developed correlatingcorrection of GIRD and TROMD with change in injuryincidence.Specific intervention strategies to modify the changes
in GIR and TROM, as well as to correct GIRD andTROMD, should be better developed. Exercises needto include decreasing capsular stiffness and increasingcapsular mobility, decreasing muscular stiffness, andincreasing muscle eccentric strength and endurance.Another issue is the timing of these interventions:before the throwing/serving episode, immediately afterthe episode, between episodes, or a combination of all.Longitudinal studies tracking GIR, GER, TROM, GIRD,
and TROMDover the course of 1 or 2 seasons are neededto completely understand the effect of athletic exposureon shoulder motion. “Microcycles” of change over asingle athletic exposure or several athletic exposures canbe performed multiple times within a season to deter-mine whether patterns of change and recovery couldgive clues to impending injury. Histologic evaluation ofcapsular tissue could quantify the location and compo-sition of the capsular component. In addition, the effectof a dedicated program of identifying and modifyingGIRD and TROMD on injury incidence and performanceshould be completed. Emphasis should be placed onunderstanding the best balance of true stretching, tissuemobilization, and eccentric strengthening and enduranceexercises in the modification program. These investiga-tions should be performed for all overhead sports inwhich GIRD and TROMD have been identified.
Labral and Rotator Cuff Injuries: HowMuch Treatment?
Superior labral and rotator cuff injuries are the mostcommon GH pathoanatomic problems associated withdysfunction in the DTS. However, how these alterationsin anatomy contribute to the symptoms is not wellunderstood, with consequent uncertainty about evalu-ating and treating the observed findings. Informationhas been developed regarding the known roles of the
labrum in normal shoulder function and how injuriesof the labrum and rotator cuff can be most effectivelyevaluated. In addition, it appears that in higher-levelthrowers, some of the observed pathology may beadaptive and necessary for function.The approach to treatment of throwers with shoulder
pain has improved because the mechanisms behind thedevelopment of pathology are better known. However,many athletes are unable to return to throwing aftersurgery, despite near-anatomic restitution of their pre-senting pathology.Review of the mechanics behind pitching can provide
insight into howpathology seen in the thrower’s shoulderdevelops, the approach to observed pathologies, andthe reported rates of success. From this perspective, someof the pathology seen in the thrower’s shoulder maybe adaptive, in that the presence of the pathology maybe required for an athlete to throw at elite levels, andanatomic restoration is not only not required but may bedetrimental.
Pathomechanics of ThrowingThrowing is an extreme skill that requires the GH
joint to achieve incredible positions and experienceexceptionally high angular velocities and forces.14,92
To throw at high velocities, it has been recognizedthat a thrower must achieve certain nodes, or bodyand arm positions, in a specific progression to optimizethis skill.19,92 Achieving these nodes optimizes properpitching mechanics and may reduce injury. In addition,because it has been shown that the velocity of the pitchedball correlates with the amount of external rotation ofthe abducted arm in the late cocking phase of throwing,these nodes likely optimize the body’s ability to maxi-mize external rotation.93-95 The forces and position of theshoulder at maximal external rotation are impressive,14
with the arm in a position of 165 � 11�. This positionhas been called a “critical moment” in throwing and isthought to be a potential source of the development ofpathology in the thrower’s shoulder.14,96,97 Numerousstudies have shown this position to be responsible forhigh strain in the superior labrum98 and the developmentof SLAP lesions in cadaveric shoulder models.99,100 Withregard to the rotator cuff, this position of maximalGH joint external rotation is thought to produce articularsurface partial-thickness rotator cuff tears through com-pressive loads of internal impingement101,102 or, alter-natively, through external rotation tensile overload ofthe capsular portion of the rotator cuff.96,103 The repeatedtorsion in external rotation during throwing also leadsto the remodeling of the thrower’s humerus in externalrotation torsion.71,72,75,76,104 Bony remodeling alsooccurs on the scapular side of the dominant arm of thethrowerwith increased glenoid retroversion.71,74 Finally,physical examination tests of asymptomatic professionalbaseball players show asymmetry in inferior laxity as

DISABLED THROWING SHOULDER: 10-YEAR UPDATE 147
detected by the sulcus sign.105 These changes are thoughtto be adaptive and even protective of the thrower’sshoulder71,76,96,103,106 and likely exist so that the throwercan deliver the ball at high velocity effectively.
Labral Roles and Injuries in ThrowersAndrews107 was the first author to report lesions of
the superior glenoid labrum in throwing athletes, andSnyder et al.108 reported this lesion in other pop-ulations and developed the widely adopted and some-times modified classification system for SLAP tears. Thissystem is observational and is based on arthroscopicvisualization and criteria. As experience with this lesionincreased, its importance as a key factor in the DTS wasidentified1,59,80,109,110 and surgical techniques to treatthis lesion were developed. This lesion is also beingdiagnosed and treated more frequently in non-throwingpopulations. Current American Board of OrthopaedicSurgery data and New York State data indicate a largeincrease in the number of SLAP surgery repairs inthe last 10 years, from 4 per 100,000 population to22 per 100,000 population111; moreover, such repairsrepresent 10% of all shoulder procedures and havebecome the second most common shoulder arthroscopicprocedure.112
There is increasing evidence that SLAP lesions are beingpoorly diagnosed, overdiagnosed, or misdiagnosed, withresulting poor outcomes for diagnosis and treatment. Thestudies providing this evidence report on the imprecisionof physical examination tests,113 diagnostic imaging,114
and arthroscopic evaluation115 as sole determinants ofthe diagnosis and show variable results from surgicalrepair.116-118 Basic to correcting these outcomes is abetter understanding of when the anatomic alterationthat is called a SLAP injury is contributing to shoulderdysfunction (a clinically significant SLAP injury) andhowit should be treated to restore the role of the labrum inshoulder function.Labral roles in shoulder function have been tradi-
tionally identified as an attachment site for the biceps,a bumper to deepen the GH socket and to improvestability by minimizing GH translation, and an aid inincreasing capsular tension.119 However, labral rolesmay actually be more complex. The actual role of thesuperior labrum as a mechanical bumper is controver-sial. The amount of increased mechanical GH trans-lation after superior labral resection was only 10%,meaning that the superior labrum likely has functionalroles other than just a mechanical stability role.120
Recent biomechanical studies have highlighted 3 otherimportant functions for the labrum: (1) as a deformablestructure with high compliance interposed between 2surfaces to more evenly distribute contact pressuresbetween the surfaces, increase boundary lubrication,and maximize concavity/compression characteristics,much like a washer between 2 surfaces; (2) as a pressure
sensor maximizing proprioceptive feedback; and (3) asan attachment site for muscles and ligaments, to opti-mize their tension.119,121 Experimental labral releaseresulted in significant changes in capsular tension.119
Another cutting study showed increased GH translationthat was restored to normal by posterior superior labralrepair (Anthony Romeo, data presented at summit).The intact labrum would result in optimal GH kine-
matics in dynamic shoulder motion, resulting in smoothGH motion in rotation, stable ball-and-socket kine-matics, and maximal force transfer from the engine ofthe core and legs through a stable linkage at the shoulderto the deliverymechanism, the hand. The labrum shouldbe seen as a key component for functional GH stability.Many labral “injuries” diagnosed on imaging are not
clinically significant, in that they are not contributory tothe symptoms or dysfunction in the DTS. The clinicallysignificant SLAP injury is one in which the anatomicalteration in the labrum results in elements of theclinical history of the dysfunction that can be attributedto the loss of labral roles, and the injury can be high-lighted by specific physical examination tests that areclinically useful for detection of the injured labrum. It isa positive diagnosis, not a catch-all term in the presenceof shoulder pain of unknown etiology.The history findings suggestive of loss of labral roles
include pain on external rotation/cocking, indicatingincreased posterior-superior translation1,120,121; weaknessin clinical or functional arm strength, indicating pain and/or increased translation; symptoms of internal derange-ment (clicking, popping, catching, sliding), indicating lossof thebumper effect orwasher effect, or decreased capsulartension; and a feeling of a “dead arm,” indicating loss ofproprioceptive feedback, decreased capsular tension, andincreased translation. These are not exclusively seen ina labral injury but point toward the loss of labral roles.The literature, as well as the consensus of the meeting
attendees, suggests that there is not a specific clinicaltest that conclusively shows a clinically torn labrum ordistinguishes the clinically significant SLAP tear. How-ever, a comprehensive examination will show localand distant physiological and biomechanical deficitsthat are commonly associated with SLAP injury, needto be addressed in treatment, and have been found todecrease the DTS dysfunction. In addition, there arelabral examination tests that can provide intra-articularclues to the presence of a labral injury.Kinetic chain deficits are discovered on examination in
a majority of patients with SLAP injuries. Deficits inhip abductor or extensor strength, deficits in hip rotationflexibility, or core strength weakness have been identi-fied in 50%of SLAP injuries.3,31,80 They can be identifiedby the methods described in the section on the kineticchain.31,32,122 Scapular dyskinesis is frequently seen inpatients with labral injuries, as has been described in thesection on scapular dyskinesis.1,30,42

148 W. B. KIBLER ET AL.
Of the labral examination tests, the modified dynamiclabral shear test123 has been shown to be of high clinicalutility in the evaluation of labral injuries when the testis performed in the manner described. It is performedby abducting the arm and flexing the elbow to 90�. Thearm is then abducted in the scapular plane to above120� and externally rotated to tightness. A shear load isapplied to the joint by maintaining external rotationand horizontal abduction and lowering the arm from120� to 60� of abduction. A positive test is indicated byreproduction of the pain and/or a painful click or catchin the joint line along the posterior joint line between120� and 90� of abduction. The test has a sensitivity of0.72, specificity of 0.98, positive predictive value of0.97, and positive likelihood ratio of 31.6.123 Otherlabral examination tests advocated include the O’Brienactive compression test,124 the relocation test125 withpain as the indicator, and an anterior leveringmaneuver to place a posterior load and shear (RichardHawkins, data presented at summit).GIRD and TROMD are seen in virtually all patients
with SLAP injury and have been found to be predictiveof future injury in asymptomatic patients.61 Precise,reproducible measurement is possible with specificprotocols that stabilize the scapula and measure GHmotion with either a goniometer or inclinometer.53,91
Scapular forward posture has been implicated asa negative factor for success of nonoperative treatmentin SLAP injury (S.M., data presented at summit). Thisposture results from weaker posterior scapular musclesand tight pectoralis minor muscles.52 Clinical assess-ment by observation and palpation of the tight anteriorstructures and measurement by the double-squaremethod can be performed and have been shown to beclinically reliable.23,58
In addition, intra-articular examination tests canprovide clues to loss of labral roles. A positive painfularc-of-motion test in the Hawkins-type motion, with norelief by scapular posterior tilt in the scapula assistancetest,40 indicates increased translation. A positive O’Brienmaneuver indicates loss of the washer effect, increasedbiceps tension, and increased translation. The modifieddynamic labral shear test has been shown to have highclinical utility because it specifically replicates a peel-backphenomenon. A positive test indicates loss of biceps sta-bility, loss of thewasher effect, and increased translation.In summary, the physical examination can provide
findings that help construct a comprehensive picture ofthe anatomic and physiological deficits that exist andmay cause or exacerbate the SLAP injury and thatshould be the focus of a comprehensive rehabilitationprogram.
ImagingThe labral injury can be confirmed by magnetic reso-
nance imaging (MRI), MRI arthrography, or computed
tomography (CT) arthrogram but should not be definedby imaging. Specific criteria have been developed todistinguish a labral alteration, but MRI is best viewed asa static estimation of labral status with inconsistentrelation to the dynamic roles. A percentage of patientswill show “labral tears” without symptoms relating toloss of the labral roles.MRI studies in asymptomatic throwers114,126-129
(Table 2, available at www.arthroscopyjournal.org)have shown that cuff disease (including surprisinglyhigh levels of partial-thickness rotator cuff tears) andeffusionsdfindings that would normally be consideredpathologicdare often seen in an asymptomaticthrower’s shoulder and may not be a source of symp-toms. The aphorism “treat the patient, not the X-ray” isparticularly relevant in the thrower with DTS.The clinically significant SLAP injury as defined by
the history, physical examination, and/or imaging thatdifferentiates it from other sources of shoulder painneeds to be treated, but surgical treatment is rarely thefirst option.
Nonoperative Treatment of Labral TearsThough often recommended and performed, reha-
bilitation has not been widely studied, nor has itsoutcomes. There is only 1 case series in the literaturedescribing the results of nonoperative treatment ofSLAP lesions. Edwards et al.130 collected data usinga survey with validated outcome measures in 50 of 305patients with labral tears (response rate, 16.4%). In thisgroup 39 patients had symptomatic SLAP lesions diag-nosed by a positive O’Brien test, pain at the bicipitalgroove, and MRI with greater than 1 year of follow-up.All patients were treated nonoperatively with nonste-roidal anti-inflammatory drugs and a physical therapyprotocol focused on scapular stabilization and posteriorcapsule stretching. This protocol was considered success-ful in 19 (49%). In this group 18 patients were active insports before treatment and 15 performed overheadathletics. Of the 15 overhead athletes, 10 (67%) wereable to return to overhead athletics after nonoperativetreatment.Data presented at the dedicated meeting summarized
the findings for a Major League Baseball organization(David Lintner, data presented at summit). Theseplayers all had SLAP lesions and underwent physicaltherapy focusing on addressing the posterior capsulecontracture (GIRD), as well as scapular rehabilitation.Surgery was offered if the thrower had persistent paindespite improvements in GH motion and scapulardyskinesis. Nonoperative treatment at the Minor Lea-gue level had failed in many athletes, and they repeatedthe physical therapy program if they presented to thehead team physician with GIRD and scapular dyskine-sis. Over a 10-year period, 115 shoulder-related eventsrequired evaluation by the head team physician,

DISABLED THROWING SHOULDER: 10-YEAR UPDATE 149
representing 25 Major League players and 90 MinorLeague players. Of this group, 76 throwing athletes hadSLAP lesions and had follow-up of more than 1 yearafter treatment. Of these 76, 31 (41%) were effectivelymanaged nonoperatively, with 28 of 31 (90%) able toreturn to their prior level of play after treatment. Thiscompares with 6 of 9 throwers (67%) with SLAP lesiondebridement who were able to return to their priorlevel of play. Of the 36 patients who underwent SLAPlesion repair, 23 (64%) returned to their prior level. Ofthe 11 patients who had SLAP lesion repair and rotatorcuff repair, only 5 (45%) returned to their prior level ofplay. The combination of SLAP lesion repair and rotatorcuff surgery has been shown to have a poor prognosisin other reports.116,131
In addition, in another population of active but non-professional athletes (S.M., data presented at summit),it was shown that 51% of SLAP injuries proven byexamination and imaging will become functionallyasymptomatic with a 6- to 8-week guided rehabilitationprogram. The programs have been designed to specifi-cally address kinetic chain and scapular deficits, aswell asmuscleflexibility, strength, and strength balance deficits,discovered on physical examination and are describedin the section on rehabilitation.3,33
Surgical Treatment of SLAP LesionsThe results of current methods of surgical treatment
for superior labral tears in the thrower’s shoulder aresummarized in Table 3 (available at www.arthroscopyjournal.org).116,118,131-148 If return to play at thesame level or a higher level is used as the outcomemeasure of interest, only 5 of 22 series reported successrates at or above 85%. As shown, there is a great degreeof variation, with successful outcomes ranging from22% to 94%. This likely relates to the low levels ofevidence of these series, because there is no controllingfor acuity of the SLAP lesion, location of the SLAPlesion,116 presence of additional pathology, indicationsfor surgery, surgical technique, postoperative rehabili-tation protocols, and willingness of the athlete toreturn, all of which may affect the outcome. These poorresults point to the need for a more detailed under-standing of what intra-articular pathology needs to betreated and how it should be treated.If arthroscopy is recommended, the arthroscopic
evaluation of the suspected labral injury must bespecific to understand and treat the labral injury prop-erly. The arthroscopic findings most frequently associ-ated with a clinically significant labral injury include (1)a type II or higher lesion, denoting loss of attachmentfrom the glenoid108; (2) a peel-back phenomenon,indicating labral detachment, increased compliance,loss of washer effect, and loss of bumper effect1,120,121;(3) glenoid articular cartilage damage or chon-dromalacia, indicating increased translation149; (4) loss
of capsular tension, indicated by a drive-through sign,or loss of tension in the posterior band of the inferiorglenohumeral ligament; (5) increased posterior labralthickness, indicating increased translation and shearwith compression on the labrum; and/or (6) excessiveposterior inferior capsular thickness and scar, indicatingend-stage capsular damage that helps create GIRD.2
Care must be taken to differentiate labral detachmentfrom anatomic variants such as sublabral foramina,a Buford complex attachment of the middle GH liga-ment, or a meniscoid-like labral attachment that doesnot peel back.150
On the basis of these principles, arthroscopic treat-ment guidelines for labral injury include (1) evaluationof the peel-back phenomenon, labral injury andmobility, glenoid surface, and capsular tension by directvisualization; (2) preparation of the glenoid to maximizebone-to-labrum healing; (3) multiple anchor placementto secure at least 2-point fixation of the labrum on theposterior-superior glenoid (10:30 and 11:30 clock-facepositions in a right shoulder) (a double-loaded singleanchor is still only 1-point fixation); (4) placement ofenough posterior-superior anchors to eliminate the peel-back phenomenon; (5) evaluation of biceps mobilityafter anchor and suture placement to make sure there isadequate motion of the biceps in shoulder externalrotation; (6) rare placement of anchors and sutures inthe anterior-superior glenoid (12:00-o’clock position to2:30 clock-face position in a right shoulder) to reducethe chance of biceps tethering; (7) evaluation of theeffect of the labral repair on capsular tension by evalu-ation of the tautness of the posterior band of the inferiorglenohumeral ligament and elimination of the drive-through sign; (8) assessment of total GH rotation toensure that no external rotation has been lost; and (9)treatment of the associated pathology in the joint.
Surgical Treatment of Rotator Cuff TearsThe surgical treatment of rotator cuff tears in the
throwing athlete has receivedmore attention, but again,most studies have low levels of evidence140,151-157
(Table 4, available at www.arthroscopyjournal.org).Three different methods have been used to surgicallytreat partial-thickness rotator cuff tears: debridement;repair of delaminations in situ, without repair to bone;and repair of the partial tear to bone. In the high-demandpopulation of throwing athletes, by use of return to playat the same level or a better level as a primary outcome,the results of surgical treatment of partial-thicknessrotator cuff tears show moderate success140,151-155
(Table 4, available at www.arthroscopyjournal.org).Debridement produces return-to-throw rates of 16% to85%. Again, in these case series, there is no controllingfor the nature of the rotator cuff tear, the concomitantpathology, the indications for surgery, the postoperativemanagement, or the athlete’s willingness to return.

150 W. B. KIBLER ET AL.
There are few data on repair of delaminations withoutrepair to bone, but the early results seem promising, withreturn-to-play rates of 89%.Whena throwing athlete hasa partial tear that is repaired to bone, the return-to-playrates seems less optimal, with only one-third returningto the same level of play. In a similar vein, repair offull-thickness rotator cuff tears to bone in throwingathletes is met with dismal return-to-throw rates (8% forprofessional pitchers)156,157 (Table 5, available at www.arthroscopyjournal.org). These data suggest that theanatomic restoration of the rotator cuff has led to pooreroutcomes than a debridement or repair in situ.
Concept of Adaptive PathologyThrowing requires repetitive high loading of the
osseous and soft-tissue structures. To achieve theextremes of external rotation required for throwing withhigh velocity, these structures undergo adaptive remod-eling and possibly failure. The fact that MRI scans ofasymptomatic throwers show significant findings thatwould normally be considered the source of the athlete’spain suggests that these athletes have developed theseanatomic alterations to throw at high levels, just astheir humerus has remodeled into greater retroversion.Chronic SLAP lesions in throwersmay allow for increasesin external rotation required for throwing. Articular-sidepartial-thickness rotator cuff tears may represent failureof the tissue in external rotation, again allowing for theextremes of external rotation required for high-levelthrowing. It is conceivable that in some throwers, theanatomic repair of these structures will lead to aninability to achieve the extremes of external rotationrequired to throw at high velocity and may end theircareers. This may explain the relatively poor resultsobtained with the surgical treatment of the combinedlabral/rotator cuff pathology. The throwing athlete canbe considered on the edge of a cliff in terms of thedemands of the throwing motion on the anatomicstructures. Treatment of the DTS should put the athleteback on the edge of the cliff and not restore his or hershoulder to “normal” anatomy. This concept leads toa suggested approach to the symptomatic throwingathlete, described in the next section.
SurgerySurgery is to be used only after extensive and appro-
priate rehabilitation fails. The rehabilitation mustaddress deficits in internal rotation (GIRD) and totalrange ofmotion (TROMD), as well as scapular dyskinesisand kinetic chain deficits. If the athlete improves clini-cally with regard to GIRD, TROMD, and dyskinesis butstill has pain and cannot throw, surgery may be offeredin an attempt to salvage his or her career. Surgery shouldbe considered a method to improve the anatomy withinthe shoulder so that rehabilitation can be successful.When one is performing surgery, a minimalist approach
is ideal. In rotator cuff disease, debridement is likelypreferable to repair, and if repair is performed, a trans-tendinous repair of the delaminated rotator cuff is likelygoing to produce better outcomes than repair to bone.With regard to SLAP lesions, repair of the “peel-back”posterior labrum is performed surgically, but it isimportant to avoid overconstraining the bicep, whichserves as an important restraint to external rotation ofthe abducted arm.158
ConclusionsThrowing at high velocity requires extremes of GER
of the abducted arm, where extremely high forces areendured. Repeated throwing leads to bony remodelingof the humerus and glenoid. Many elite asymptomaticthrowers have findings on MRI that would normallybe considered pathologic. On the basis of our under-standing of throwing mechanics, these findings, alongwith the well-reported bony changes that affect thehumerus and glenoid, may be adaptive and may allowfor the extremes of external rotation that are requiredfor high-velocity throwing. The pathology often treatedsurgically in the thrower’s shoulder includes partial-thickness rotator cuff tears and SLAP lesions. In somethrowers, this pathology can also be considered adap-tive, because it allows the thrower to achieve theextremes of motion required to throw at high velocity.Clinically significant SLAP tears do exist. They
represent a relatively small subset of general patientswith shoulder pain but are common in intenselycompetitive overhead athletes as part of the DTS. Theoptimal integration of clinical history, physical exami-nation findings, imaging findings, and arthroscopiccriteria has not been formulated. Clinical efforts todetermine the SLAP injury that is associated withdysfunction should be related to demonstration, byhistory and physical examination, of loss of labral roles.Treatment guidelines should first emphasize a struc-tured rehabilitation program, because studies indicatethat around half of all lesions can be symptomaticallyresolved through rehabilitation. Surgical guidelinesshould also emphasize delineation of loss of labral rolesand their surgical restoration.Although the data are limited, nonoperative treat-
ment has been shown to be successful for a number ofelite and recreational athletes with SLAP lesions.Rehabilitation should be focused on treating GIRD,TROMD, scapular dyskinesis, and kinetic chain deficits.Surgical results for returning throwers to their formerlevel of play are not as high as we would hope.Throwers who have surgical repair of SLAP lesions withtreatment of rotator cuff tears have in past literatureshown poor rates of return to play. Throwers with full-thickness rotator cuff tears in the dominant arm whoundergo repair to bone also have poor rates of return toplay. As a result, surgery should be undertaken if the

DISABLED THROWING SHOULDER: 10-YEAR UPDATE 151
thrower continues to have pain despite corrections inGIRD and scapular dyskinesis. A surgical approachshould be considered career salvaging, and athletesshould be counseled on expectations.The following principles should be considered when
one is performing surgery on the thrower’s shoulder:(1) Surgery should be considered only after extensiveand appropriate rehabilitation has failed. (2) Thesurgical approach should be minimalistic, with theconcepts to repair as needed but not to achieve normalanatomic repair of the rotator cuff. (3) Surgery shouldbe considered as a last resort to attempt to salvagea thrower’s career, and throwers must be cognizant ofthe poor return-to-play rates.Areas worthy of future study include (1) optimizing
surgical techniques for SLAP repair, especially withregard to the location of the anchors, the type of suturesand knots, and postoperative management; (2) identi-fying the optimal surgical approach to the damagedrotator cuff; (3) decreasing the lengthy convalescencefor return after surgery; and (4) identifying the featuresthat distinguish the athlete with adaptive pathologyfrom the athlete who has fallen from the cliff edge andhas pathology that limits the ability to throw.
RehabilitationRehabilitation can play a key role in modifying the
dysfunctionof theDTSand reducing theneed for surgery.A clinically applicable rehabilitation and conditioningprogram to achieve these goals has been outlined(described in the “Recommended Exercise Program forRehabilitation and Conditioning” section). The programis outlined so that health care providers can use it clini-cally in the care of their patients with DTS. The primaryaim of this rehabilitation approach is to emphasize eval-uating and treating the entire body. Often, the source ofthe problemmay not be only at the site of pain; thereforeevaluating and treating the entire system are necessaryand beneficial for the outcome of the patient. The reha-bilitation program addresses 3 primary focus points:kinetic chain, shoulder mobility, and shoulder strength-ening. The rationale and evidence, when available, forthe interventions are then integrated into the 3-phaseexercise program.
1. Kinetic chaina. Leg drive and lower extremity strengthb. Hip mobilityc. Proximal core stabilityd. Dynamic core strength/powere. Scapular stabilization
2. Shoulder mobilitya. Restoring internal and external rotation deficits to
achieve safe total ROMb. Addressing joint restrictions in the spine and
shoulder complex
c. Addressing muscular flexibility imbalances in thespine and scapula
3. Arm strength and endurancea. Restoring scapular motor control for functional
and pain-free motionb. Facilitating inhibited orweak scapularmusculaturec. Integrating scapular exercises with functional
tasksd. Facilitating endurance and eccentric control by
advanced shoulder and scapular exercisese. Strengthening forearm, wrist, and hand
The DTS usually presents to the physician, physicaltherapist, or athletic trainer with the primary symp-tom of pain during throwing. It is well establishedin young throwing athletes that an increased volumeof pitching increases the risk of having shoulder orelbow pain by 2- to 3-fold.159 Early managementwould include modification of exposure to throwing,from decreasing throwing to complete restriction ifsymptoms are severe. The exact duration of this mod-ification or restriction is not known. The consensus isthat 2 to 3 weeks would allow acute inflammation tosubside and allow for improvement in tissue mobility.It is possible to see measurable strength changes in 3weeks, primarily because of neuromuscular coordina-tion changes.160-162 In practice, athletes frequently willonly take a few days off and may have to deal withrecurring issues of pain throughout the season. Thegroup consensus recommends setting a window oftime that would allow deficits to be addressed andsymptoms to resolve. This should be considered aperiod of active rest and rehabilitation, not completerest.
Kinetic ChainDuring the initial evaluation of the athlete’s kinetic
chain, deficits in hip mobility or single-leg stability arelikely to be identified. These deficits can be treatedduring the time of active rest. Nearly 50% of ballvelocity comes from leg-forward step and trunk rota-tion.163 Addressing deficits found in the trunk andlower extremity is important because the ability toaccelerate the elbow and wrist during throwing is due totorque generated more proximally in the trunk.Throwing performance may also benefit by targeting thecore musculature, given that increased pelvic velocityduring the arm-cocking phase and upper torso rotationduring the acceleration phase of throwing is positivelyrelated to ball velocity.164 Limitations of motion of thespine, hip, and the rest of the lower extremity should beaddressed. Typical hip motion in various baseballathletes has been studied previously22,165,166; a summaryof these values is presented in Table 6 (available at www.arthroscopyjournal.org) and should be used for re-establishing observed deficits.

152 W. B. KIBLER ET AL.
Strengthening and stability of the core and lowerextremity musculature are critical because of theircontributions to the throwing motion. During pitching,the stance or back leg balances the body weight duringthe wind-up and drives the body forward during thepush off, but the lead or front leg requires sufficientleg and hip strength to control the landing force of 72%of body weight.167 Deficits detected during screeningmay require further evaluation during rehabilitation todetermine whether they arise from lower extremity orcore deficits of inflexibility, strength, or lack of balance.Strengthening the core for returning to dynamic move-ments in throwing is different from prescribing stabiliza-tion exercises for spinal disorders. Abdominal musclesactivate in an orderly sequence from the ground upthrough the torso when throwing a ball.168 Thereforemuscles must be stiff enough to stabilize the joints butnot too stiff to impede the transfer of energy through thekinetic chain.168 One exercise does not target all theabdominal muscles; therefore a program that addressesthe anterior, lateral, and posterior sides of the torso shouldbe undertaken. Mat exercises emphasizing enduranceare good starting points, with consideration given topositions that limit stress to the shoulder. The athleteshould be engaged in lower extremity and core exercisessuch as rotational chop-and-lift activities that simulate thedemands of throwing.169 The use of unstable surfaces,such as stability balls or foam mats, has shown increasedcore activation170,171 and improvement in core strengthbut has not necessarily shown carryover into functionaltasks.172 Recently, a study in handball players using anunstable closed kinetic chain program that used a slingsuspension to train the core reported improvements inthrowing velocity of 5%.173
The relations established between leg and core motionsandkinetic chain force development to improve throwingvelocities provide a solid rationale for training the lowerextremity and core in specific routines for throwers. Thenature of the throwing task, combining stepping androtating, produces a complex motion that is necessary tosimulate in rehabilitation and conditioning for throwing.Specific routines and their effectiveness on increasingmobility, strength, or balance have not been completelydeveloped. Furthermore, the effect of enhancementof these functions on injury prevention is unknown.Dynamic core exercises are recommended to improveperformance particularly related to power, but whatspecific exercises and at what training regimen (numberof sets and repetitions) are appropriate for the variouslevels of throwing athletes are currently unknown.
Shoulder MobilityIndividuals with shoulder injury often present with
shoulder ROM deficits.63,82 Deficits in GIR and TROMcan be predictive of future injury.61,174 One study iden-tified that patients with resolution of shoulder symptoms
displayed greater improvement in glenohumeral hori-zontal adduction range of motion (GHA) than thosewith residual symptoms.83 As such, prevention andtreatment of shoulder motion deficits are critical compo-nents of an intervention program for throwing athletes.The goal of the intervention program is restoration of
ROM to acceptable values (Table 7, available at www.arthroscopyjournal.org). Deficits in GIR and TROMshouldbeaddressed to restore safeROMvalues; however,it is important to remember that ROM values are affectedbyprevious throwing activities for at least 24 hours.69 GIRof the throwing shoulder should bewithin 18� (range, 13�
to 20�) of the nondominant shoulder,61,174 TROM in thethrowing shoulder should be within 5� of the nondomi-nant shoulder, and TROM should not exceed 186� toavoid an increased risk of injury.61 The cross-body stretchand sleeper stretch target the posterior shoulder mus-culature and capsule to effectively improve GIR andGHA.85,175 Additional beneficial treatment techniquesinclude joint mobilizations,176 muscle energy tech-niques,177 and soft-tissue mobilization. Assessment andtreatment of GHA are becoming more important. Amultimodal treatment approach that included posteriorshoulder stretching and joint mobilization showed thatchange in GHA is as important as change in GIR inreduction of symptoms.83
Muscular adaptations that can alter scapular kine-matics during elevation can occur because of tightanterior structures such as the pectoralis minor. Pector-alis minor tightness has been identified on the dominantside of tennis players178 and is associated with increasedscapular anterior tilt and scapular internal rotation.52
Pectoralis minor tightness can be effectively treated withcorner stretching exercises.45
Only 1 study has investigated the efficacy of posteriorshoulder stretching in symptomatic patients.83Because theexact pathophysiology of shoulder mobility deficits is notknown, it is unknown which tissuesdmusculotendinous,joint capsule, or bonydmay be the source of the deficitand therefore should be the target for intervention. Theability to specifically address alterations in each of thesetissues will help give insights into the most effectiveintervention for restoring shoulder mobility. The role ofrehabilitation specialists in direct treatment and exercisesupervision versus home exercise is not clear becausestudies have provided mixed results.179-181 Further inves-tigation into treatment effectiveness and the level ofsupervision is needed to maximize effective care for theathlete. Continued investigation into shoulder mobilitythroughout the season, along with the baseline measures,mayhelp improve the ability to detect overuse injuries thatare evolving before the onset of symptoms.
Arm Strength and EnduranceThe strength and endurance of the athlete’s shoulder
musculature are important to allow normal throwing

DISABLED THROWING SHOULDER: 10-YEAR UPDATE 153
function. Asymptomatic throwers often present withgreater internal rotation strength compared withexternal rotation strength on the throwing side andtypically presentwith a 3:2 strength ratiowhenmeasuredisokinetically.182-185 Deficits in shoulder strength arepredictive of future injury, particularly in external rota-tion and supraspinatus activation.186 Athletes presentingwith shoulder symptoms are typically found to havestrength deficits of the rotator cuff187,188 and scapularmusculature,189 which may present with various move-ment patterns.190 Treatment of these deficits has manycommon themes and treatment protocols.191 Initialmanagement should focus on scapular musculaturecontrol, which facilitates stability to prepare the shouldermusculature for more dynamic and stressful exercises.Repeated emphasis of proper position and movementinstructions are important because many of the move-ment strategies learned are only temporary.192 Estab-lishmentof proximal stability suchas scapular orientationexercises should precede longer lever-arm activities(i.e., prone horizontal abduction exercises) to establishproximal functional control.33,193 Over-activation of theupper trapezius during elevation, indicating a muscularimbalance around the scapular force couple, has beenfound in injured shoulders.24,194 Scapular setting exer-cises have been shown to primarily activate the trapeziusmusculature193 and can facilitate muscular balancebetween the scapular force couple of the serratus anteriorand upper and lower trapezius.24,39,195 The focus of thescapular exercise program should be on the rhomboid,lower trapezius, and middle trapezius musculature.Facilitation of serratus anterior and lower trapeziusmusculature can be targeted with isometric adductionand extension exercises with continued focus on properscapular orientation of posterior tilting and retraction.196
Progression to dynamic exercises that incorporate allshoulder muscles and simulate function is the nextstage of rehabilitation. Exercises in this phase arefrequently individualized for specific goals, and directsupervision by a rehabilitation specialist is critical tomeet the individual’s needs and anticipated functionallevels.Most literature regarding electromyographic activity of
shoulder exercises has focused on which exercisesactivate specific muscles primarily during a particularexercise197-209 or activate them synergistically.210-212
However, studieshavealso shownhowparticularexercisesaffect scapular kinematics to ensure that proper motionsare being emphasized46,190,213 and improper motionsare de-emphasized.214 Scapular posterior tilting andretraction are facilitated with prone horizontal abductionand prone scapular retraction with the elbows flexed.46
It is well established that strengthening exercises willincrease strength, but there is limited information onhow these exercises affect sport performance parame-ters or prevent throwing injuries. Rotator cuff strength
and serve velocity have been significantly increased inelite tennis players with 6 weeks of isokinetic shoulderstrengthening using concentric and eccentric resistivetraining approaches.215,216 Recent evidence has shownthat incorporating plyometric and eccentric exerciseshas important benefits in developing power for over-head athletes.217-219 Plyometric exercise training regi-mens that last at least 10 weeks have resulted inincreased throwing velocities of approximately 2% intrained athletes.217,220 In adolescent throwers (aged11 to 15 years), throwing velocity was significantlyincreased by 2.2 mph with a 4-week elastic trainingregimen of 17 exercises performed for 20 to 25 repeti-tions.221 Throwing velocity can be improved withseveral intervention approaches. A study comparing6-week training programs with plyometric exercises,thrower’s 10 isotonic exercises, and pneumatic exer-cises showed significant improvements in throwingvelocity for all 3 programs (range, 1.2% to 2%).222 Ina similar group of adolescent baseball players, armendurance and leg strength significantly increased witha 2-month training program emphasizing endurancetraining (S.M., data presented at summit). Swaniket al.223 showed that a combination of elastic resistanceand isotonic exercises for 6 weeks before competitiveswimming season decreased the incidence of reportedshoulder pain episodes in 13 athletes in the traininggroup (1.8 � 2 incidents) compared with a controlgroup (4.6 � 4.7 incidents).Several different types of intervention strategy exist
in the literature, but none have shown the bestoutcomes.1,34,80,191,224,225 Better documentation ofcontent and outcomes of intervention approaches inoverhead throwing populations could determine whichinterventions are effective. Randomized controlledtrials are difficult to perform in this population but areimportant to delineate cause and effect of therapeuticinterventions and develop insights into the manage-ment of this population. Although many therapeuticexercises and protocols have been devised, it is notknown which exercises are primary and which exercisesare supplementary in recovering function or preventinginjuries. Volume of pitching and fatigue increase the riskof development of significant shoulder or elbow injury;therefore it is important that the exercises emphasizefatigue resistance for pitchers.226,227 However, eachposition has differing demands, so each exerciseprogram may need to focus on endurance (low loads/high repetitions) or on strength and power (low repe-titions/high loads). A combination is probably needed,but when and how exercise programs are applied arecurrently unknown. There is limited, but promising,evidence that other forms of training, such as plyomet-rics, are beneficial to performance parameters and mayhave injury prevention effects. Evidence of the effec-tiveness of eccentric training in managing common

154 W. B. KIBLER ET AL.
tendinopathies228,229 suggests that the limited studies inthe shoulder230,231 require further investigation, becauseeccentric loads have been implicated as causative factorsin maladaptations in the disabled overhead throwingathlete.
Recommended Exercise Program for Rehabilitationand ConditioningIn this report we describe an exercise program that is
primarily directed toward the nonoperative rehabilitationof athleteswithaDTS. It can alsobeused for postoperativerehabilitation whenmodified for the healing status of therepair. Finally, these exercises can form a base forconditioning and injury prevention programs. The sug-gested exercise program is based on literature review andconsensus of the clinical experiences among the meetingattendees. Many other specific exercises may also beeffective, but they should be used in progressions as out-lined. The exercise program is progressive and sequentialand is divided into 3 phases based on the level of disabilityand tissue irritability that exist. Movement through thephases is variable and based on achieving functionalcapabilities rather than adhering to specific time frames.Phase 1, the acute phase, should minimize loads on theinjured tissues, so it should focus on scapular and GHmuscular activation, particularly in correcting timing ofmuscular activation to ensure that both the scapularand GH muscles are working synchronously (Figs 1-22,available at www.arthroscopyjournal.org). Phase 2,the recovery phase, should focus on strengtheningand restoring core, kinetic chain, and progressiveisotonic strengthening (Figs 23-54, available at www.arthroscopyjournal.org). Phase 3, the functional phase,should focus on sport-specific actions and includesendurance and ballistic exercises (Figs 55-80, available atwww.arthroscopyjournal.org). Strengthening exercisesare oriented toward endurance with an emphasis onhigher repetitions and lower resistance.An athlete shoulddemonstrate the ability to perform 3 to 4 sets of 15 to20 repetitions with correct form before progressing toa greater resistance. Another way to challenge theendurance of the musculature has been introduced anddescribed by Wilk et al.,232 called the advanced throwers10 program. This program challenges the enduranceof the athlete with the application of sustained holdsand alternating arm motions and can be incorporatedin phase 2 or 3. The sequence described below is per-formed twice without rest between sets for a total of 60repetitions.The following exercise example is for a prone hori-
zontal abduction “T” exercise: Set 1 comprises 1 set of10 bilateral isotonic contractions. Set 2 comprises 1 setof 10 sustained holds with the uninvolved arm inhorizontal abduction while the involved arm performsunilateral isotonic contractions. Set 3 comprises 1 set of10 alternating isotonic contractions between arms with
a sustained isometric hold in horizontal abduction fromarm to arm.Daily stretching exercises should be completed either
statically or dynamically. Static stretches are to be heldfor 30 seconds and repeated 4 times. Dynamic stretchesare to be performed for 12 repetitions with a minimumhold time of no longer than 2 seconds. All stretchingshould be performed until a strong pull is experiencedbut without pain or neurologic symptoms. If thesesymptoms occur, the patient should move to a lessaggressive stretch or see a rehabilitation specialist forfurther instruction.
References1. Burkhart SS, Morgan CD, Kibler WB. The disabled
throwing shoulder: Spectrum of pathology. Part I: Patho-anatomy and biomechanics. Arthroscopy 2003;19:404-420.
2. Burkhart SS, Morgan CD, Kibler WB. The disabledthrowing shoulder: Spectrum of pathology. Part II:Evaluation and treatment of SLAP lesions in throwers.Arthroscopy 2003;19:531-539.
3. Burkhart SS, Morgan CD, Kibler WB. The disabledthrowing shoulder: Spectrum of pathology. Part III: TheSICK scapula, scapular dyskinesis, the kinetic chain, andrehabilitation. Arthroscopy 2003;19:641-661.
4. Putnam CA. Sequential motions of body segments instriking and throwing skills: Description and explana-tions. J Biomech 1993;26(suppl 1):125-135.
5. Kibler WB. Biomechanical analysis of the shoulderduring tennis activities. Clin Sports Med 1995;14:79-85.
6. Elliott BC, Marshall R, Noffal G. Contributions of upperlimb segment rotations during the power serve in tennis.J Appl Biomech 1995;11:443-447.
7. Davids K, Glazier P, Araújo D, Bartlett R. Movementsystems as dynamical systems: The functional role ofvariability and its implications for sports medicine. SportsMed 2003;33:245-260.
8. Lintner D, Noonan TJ, Kibler WB. Injury patterns andbiomechanics of the athlete’s shoulder. Clin Sports Med2008;27:527-552.
9. Sporns O, Edelman GM. Solving Bernstein’s problem: Aproposal for the development of coordinated movementby selection. Child Dev 1993;64:960-981.
10. Toyoshima S, Miyashita M. Force-velocity relation inthrowing. Res Q 1973;44:86-95.
11. Hirashima M, Kadota H, Sakurai S, Kudo K, Ohtsuki T.Sequential muscle activity and its functional role in theupper extremity and trunk during overarm throwing.J Sports Sci 2002;20:301-310.
12. Hirashima M, Kudo K, Watarai K, Ohtsuki T. Control of3D limb dynamics in unconstrained overarm throws ofdifferent speeds performed by skilled baseball players.J Neurophysiol 2007;97:680-691.
13. Hirashima M, Yamane K, Nakamura Y, Ohtsuki T.Kinetic chain of overarm throwing in terms of jointrotations revealed by induced acceleration analysis.J Biomech 2008;41:2874-2883.
14. Fleisig GS, Andrews JR, Dillman CJ, Escamilla RF.Kinetics of baseball pitching with implications about
DISABLED THROWING SHOULDER: 10-YEAR UPDATE 155
injury mechanisms. Am J Sports Med 1995;23:233-239.
15. Fleisig GS, Barrentine SW, Escamilla RF, Andrews JR.Biomechanics of overhand throwing with implicationsfor injuries. Sports Med 1996;21:421-437.
16. Young JL, Herring SA, Press JM, Casazza BA. Theinfluence of the spine on the shoulder in the throwingathlete. J Back Musculoskel Rehabil 1996;7:5-17.
17. Nieminen H, Niemi J, Takala EP, Viikari-Juntura E. Load-sharing patterns in the shoulder during isometric flexiontasks. J Biomech 1995;28:555-566.
18. Marshall R, Elliott BC. Long axis rotation: The missinglink in proximal to distal segment sequencing. J Sports Sci2000;18:247-254.
19. Davis JT, Limpisvasti O, Fluhme D, et al. The effect ofpitching biomechanics on the upper extremity in youthand adolescent baseball pitchers. Am J Sports Med 2009;37:1484-1491.
20. Girard O, Micallef JP, Millet GP. Lower-limb activityduring the power serve in tennis: Effects of performancelevel. Med Sci Sport Exerc 2005;37:1021-1029.
21. Elliott B, Fleisig G, Nicholls R, Escamilia R. Techniqueeffects on upper limb loading in the tennis serve. J SciMed Sport 2003;6:76-87.
22. Robb AJ, Fleisig G, Wilk K, Macrina L, Bolt B,Pajaczkowski J. Passive ranges of motion of the hips andtheir relationship with pitching biomechanics and ballvelocity in professional baseball pitchers. Am J Sports Med2010;38:2487-2493.
23. Kibler WB, Sciascia AD. Current concepts: Scapulardyskinesis. Br J Sport Med 2010;44:300-305.
24. Ludewig PM, Cook TM. Alterations in shoulder kinematicsand associated muscle activity in people with symptoms ofshoulder impingement. Phys Ther 2000;80:276-291.
25. Endo K, Ikata T, Katoh S, Takeda Y. Radiographicassessment of scapular rotational tilt in chronic shoulderimpingement syndrome. J Orthop Sci 2001;6:3-10.
26. Graichen H, Stammberger T, Bonél H, et al. Three-dimensional analysis of shoulder girdle and supra-spinatus motion patterns in patients with impingementsyndrome. J Orthop Res 2001;19:1192-1198.
27. Kibler WB, Sciascia AD. What went wrong and what todo about it: Pitfalls in the treatment of shoulderimpingement. Instr Course Lect 2008;57:103-112.
28. DrakosMC, Rudzki JR, Allen AA, Potter HG, Altchek DW.Internal impingement of the shoulder in the overheadathlete. J Bone Joint Surg Am 2009;91:2719-2728.
29. Mihata T, McGarry MH, Kinoshita M, Lee TQ. Excessiveglenohumeral horizontal abduction as occurs during thelate cocking phase of the throwingmotion can be critical forinternal impingement. Am J Sports Med 2010;38:369-382.
30. Laudner KG, Myers JB, Pasquale MR, Bradley JP,Lephart SM. Scapular dysfunction in throwers with path-ologic internal impingement. J Orthop Sport Phys Ther 2006;36:485-494.
31. Kibler WB, Press J, Sciascia AD. The role of core stabilityin athletic function. Sports Med 2006;36:189-198.
32. Crossley KM, Zhang WJ, Schache AG, Bryant A,Cowan SM. Performance on the single-leg squat taskindicates hip abductor muscle function. Am J Sports Med2011;39:866-873.
33. Kibler WB, McMullen J, Uhl TL. Shoulder rehabilitationstrategies, guidelines, and practice. Op Tech Sports Med2000;8:258-267.
34. Wilk KE, Meister K, Andrews JR. Current concepts in therehabilitation of the overhead throwing athlete. Am JSports Med 2002;30:136-151.
35. Ludewig PM, Cook TM, Nawoczenski DA. 3-Dimensionalscapular orientation and muscle activity at selectedpositions of humeral elevation. J Orthop Sport Phys Ther1996;24:57-65.
36. Ludewig PM, Phadke V, Braman JP, Hassett DR,Cieminski CJ, LaPrade RF. Motion of the shouldercomplex during multiplanar humeral elevation. J BoneJoint Surg Am 2009;91:378-389.
37. McClure PW, Michener LA, Sennett BJ, Karduna AR.Direct 3-dimensional measurement of scapular kine-matics during dynamic movements in vivo. J ShoulderElbow Surg 2001;10:269-277.
38. Myers JB, Laudner KG, Pasquale MR, Bradley JP,Lephart SM. Scapular position and orientation inthrowing athletes. Am J Sports Med 2005;33:263-271.
39. Ludewig PM, Reynolds JF. The association of scapularkinematics and glenohumeral joint pathologies. J OrthopSport Phys Ther 2009;39:90-104.
40. Kibler WB, McMullen J. Scapular dyskinesis and itsrelation to shoulder pain. J Am Acad Orthop Surg 2003;11:142-151.
41. Weiser WM, Lee TQ, McQuade KJ. Effects of simulatedscapular protraction on anterior glenohumeral stability.Am J Sports Med 1999;27:801-805.
42. Warner JJ, Micheli LJ, Arslanian LE, Kennedy J,Kennedy R. Scapulothoracic motion in normal shouldersand shoulders with glenohumeral instability and impinge-ment syndrome. Clin Orthop Relat Res 1992:191-199.
43. Michener LA, Walsworth MK, Burnet EN. Effectivenessof rehabilitation for patients with subacromial impinge-ment syndrome. J Hand Ther 2004;17:152-164.
44. Kibler WB. Rehabilitation of rotator cuff tendinopathy.Clin Sports Med 2003;22:837-848.
45. Borstad JD, Ludewig PM. Comparison of three stretchesfor the pectoralis minor muscle. J Shoulder Elbow Surg2006;15:324-330.
46. Oyama S, Myers JB, Wassinger CA, Lephart SM. Three-dimensional scapular and clavicular kinematics andscapular muscle activity during retraction exercises.J Orthop Sport Phys Ther 2010;40:169-179.
47. DeMayK,Danneels L, CagnieB,CoolsA.Are kinetic chainrowing exercises relevant in shoulder and trunk injuryprevention training? Br J Sport Med 2011;45:320 (abstract).
48. McClure PW, Tate AR, Kareha S, Irwin D, Zlupko E.A clinical method for identifying scapular dyskinesis, part1: Reliability. J Athl Train 2009;44:160-164.
49. Tate AR, McClure P, Kareha S, Irwin D, Barbe MF.A clinical method for identifying scapular dyskinesis, part2: Validity. J Athl Train 2009;44:165-173.
50. Kibler WB, Ludewig PM, McClure P, Uhl TL, Sciascia A.Scapula Summit 2009. J Orthop Sport Phys Ther 2009;39:A1-A13.
51. Uhl TL, Kibler WB, Gecewich B, Tripp BL. Evaluation ofclinical assessment methods for scapular dyskinesis.Arthroscopy 2009;25:1240-1248.
156 W. B. KIBLER ET AL.
52. Borstad JD, Ludewig PM. The effect of long versus shortpectoralis minor resting length on scapular kinematics inhealthy individuals. J Orthop Sport Phys Ther 2005;35:227-238.
53. Kibler WB, Sciascia AD, Thomas SJ. Glenohumeralinternal rotation deficit: Pathogenesis and response toacute throwing. Sports Med Arthrosc 2012;20:34-38.
54. Kibler WB. The role of the scapula in athletic function.Am J Sports Med 1998;26:325-337.
55. Rabin A, Irrgang JJ, Fitzgerald GK, Eubanks A. Theintertester reliability of the scapular assistance test.J Orthop Sport Phys Ther 2006;36:653-660.
56. Tate AR, McClure PW, Kareha S, Irwin D. Effect of thescapula reposition test on shoulder impingement symp-toms and elevation strength in overhead athletes.J Orthop Sport Phys Ther 2008;38:4-11.
57. Kibler WB, Sciascia AD, Dome DC. Evaluation ofapparent and absolute supraspinatus strength in patientswith shoulder injury using the scapular retraction test.Am J Sports Med 2006;34:1643-1647.
58. Kluemper M, Uhl TL, Hazelrigg H. Effects of stretchingand strengthening shoulder muscles on forward shoulderposture in competitive swimmers. J Sport Rehabil 2006;15:58-70.
59. Grossman MG, Tibone JE, McGarry MH, Schneider DJ,Veneziani S, Lee TQ. A cadaveric model of the throwingshoulder: A possible etiology of superior labrum anterior-to-posterior lesions. J Bone Joint Surg Am 2005;87:824-831.
60. Harryman DT II, Sidles JA, Clark JM, McQuade KJ,Gibb TD, Matsen FA III. Translation of the humeral headon the glenoid with passive glenohumeral motion. J BoneJoint Surg Am 1990;72:1334-1343.
61. Wilk KE, Macrina LC, Fleisig GS, et al. Loss of internalrotation and the correlation to shoulder injuries inprofessional baseball pitchers. Am J Sports Med 2011;39:329-335.
62. Dines JS, Frank JB, Akerman M, Yocum LA. Gleno-humeral internal rotation deficits in baseball players withulnar collateral ligament insufficiency. Am J Sports Med2009;37:566-570.
63. Myers JB, Laudner KG, Pasquale MR, Bradley JP,Lephart SM. Glenohumeral range of motion deficits andposterior shoulder tightness in throwers with pathologicinternal impingement. Am J Sports Med 2006;34:385-391.
64. Chandler TJ, Kibler WB, Uhl TL, Wooten B, Kiser A,Stone E. Flexibility comparisons of junior elite tennisplayers to other athletes.Am J Sports Med 1990;18:134-136.
65. Roetert EP, Ellenbecker TS, Brown SW. Shoulderinternal and external rotation range of motion innationally ranked junior tennis players: A longitudinalanalysis. J Strength Cond Res 2000;14:140-143.
66. Kibler WB, Chandler TJ, Livingston BP, Roetert EP.Shoulder range of motion in elite tennis players. Am JSports Med 1996;24:279-285.
67. Thomas SJ, Swanik KA, Swanik C, Huxel KC. Gleno-humeral rotation and scapular position adaptations aftera single high school female sports season. J Athl Train2009;44:230-237.
68. Freehill MT, Ebel BG, Archer KR, et al. Glenohumeralrange of motion in major league pitchers: Changes overthe playing season. Sports Health 2011;3:97-104.
69. Reinold MM, Wilk KE, Macrina LC, et al. Changes inshoulder and elbow passive range of motion afterpitching in professional baseball players. Am J Sports Med2008;36:523-527.
70. Kibler WB, Sciascia AD, Moore SD. An acute throwingepisode decreases shoulder internal rotation. Clin OrthopRelat Res 2012;470:1545-1551.
71. Crockett HC, Gross LB, Wilk KE, et al. Osseous adapta-tion and range of motion at the glenohumeral joint inprofessional baseball pitchers. Am J Sports Med 2002;30:20-26.
72. Reagan KM, Meister K, Horodyski MB, Werner DW,Carruthers C, Wilk K. Humeral retroversion and its rela-tionship to glenohumeral rotation in the shoulder ofcollege baseball players.Am J Sports Med 2002;30:354-360.
73. Meister K, Day T, Horodyski M, Kaminski TW,Wasik MP, Tillman S. Rotation motion changes in theglenohumeral joint of the adolescent/Little Leaguebaseball player. Am J Sports Med 2005;33:693-698.
74. Drakos MC, Barker JU, Osbahr DC, et al. Effective gle-noid version in professional baseball players. Am J Orthop2005;39:340-344.
75. Osbahr DC, Cannon DL, Speer KP. Retroversion of thehumerus in the throwing shoulder of college baseballpitchers. Am J Sports Med 2002;30:347-353.
76. Pieper HG. Humeral torsion in the throwing arm ofhandball players. Am J Sports Med 1998;26:247-253.
77. Chant CB, Litchfield R, Griffin S, Thain LM. Humeralhead retroversion in competitive baseball players and itsrelationship to glenohumeral rotation range of motion.J Orthop Sport Phys Ther 2007;37:514-520.
78. Myers JB, Oyama S, Goerger BM, Rucinski TJ,Blackburn JT, Creighton RA. Influence of humeral torsionon interpretation of posterior shoulder tightness measuresin overhead athletes. Clin J Sports Med 2009;19:366-371.
79. Thomas SJ, Swanik CB, Higginson JS, et al. A bilateralcomparison of posterior capsule thickness and its corre-lation with glenohumeral range of motion and scapularupward rotation in collegiate baseball players. J ShoulderElbow Surg 2011;20:708-716.
80. Burkhart SS, Morgan CD, Kibler WB. Shoulder injuriesin overhead athletes, the “dead arm” revisited. Clin SportsMed 2000;19:125-158.
81. Tyler TF, Roy T, Nicholas SJ, Gleim GW. Reliability andvalidity of a newmethod of measuring posterior shouldertightness. J Orthop Sports Phys Ther 1999;29:262-274.
82. Tyler TF, Nicholas SJ, Roy T, Gleim GW. Quantificationof posterior capsule tightness and motion loss in patientswith shoulder impingement. Am J Sports Med 2000;28:668-673.
83. Tyler TF, Nicholas SJ, Lee SJ, Mullaney M, McHugh MP.Correction of posterior shoulder tightness is associatedwith symptom resolution in patients with internalimpingement. Am J Sports Med 2010;38:114-119.
84. Myers JB, Oyama S, Wassinger CA, et al. Reliability,precision, accuracy, and validity of posterior shouldertightness assessment in overhead athletes. Am J SportsMed 2007;35:1922-1930.
85. Laudner KG, Sipes RC, Wilson JT. The acute effects ofsleeper stretches on shoulder range of motion. J AthlTrain 2008;43:359-363.
DISABLED THROWING SHOULDER: 10-YEAR UPDATE 157
86. Sauers E, August A, Snyder A. Fauls stretching routineproduces acute gains in throwing shoulder mobility incollegiate baseball players. J Sport Rehabil 2007;16:28-40.
87. Proske U, Morgan DL. Do cross-bridges contribute to thetension during stretch of passive muscle? J Muscle Res CellMotil 1999;20:433-442.
88. Proske U, Morgan DL. Muscle damage from eccentricexercise: Mechanism, mechanical signs, adaptation andclinical applications. J Physiol 2001;537:333-345.
89. Whitehead NP, Weerakkody NS, Gregory JE, Morgan DL,Proske U. Changes in passive tension of muscle in humansand animals after eccentric exercise. J Physiol 2001;533:593-604.
90. Butterfield TA. Eccentric exercise in vivo: Strain-inducedmuscle damage and adaptation in a stable system. ExercSport Sci Rev 2010;38:51-60.
91. Wilk KE, Reinold MM, Macrina LC, et al. Glenohumeralinternal rotation measurements differ depending onstabilization techniques. Sports Health 2009;1:131-136.
92. Dillman CJ, Fleisig GS, Andrews JR. Biomechanics ofpitching with emphasis upon shoulder kinematics.J Orthop Sport Phys Ther 1993;18:402-408.
93. Atwater AE. Biomechanics of overarm throwing move-ments and of throwing injuries. Exerc Sport Sci Rev 1975;7:43-85.
94. Matsuo T, Escamila RF, Fleisig GS, Barrentine SW,Andrews JR. Comparison of kinematic and temporalparameters between different pitch velocity groups. J ApplBiomech 2001;17:1-13.
95. Wang YT, Ford HT III, Ford HT Jr, Shin DM. Three-dimensional kinematic analysis of baseball pitching inacceleration phase. Percept Mot Skills 1995;80:43-48.
96. Ryu RK, Dunbar WHV, Kuhn JE, et al. Comprehensiveevaluation and treatment of the shoulder in the throwingathlete. Arthroscopy 2002;18:70-89.
97. Burkhart SS, Morgan CD. The peel-back mechanism: Itsrole in producing and extending posterior type II SLAPlesions and its effect on SLAP repair rehabilitation.Arthroscopy 1998;14:637-640.
98. Pradhan RL, Itoi E, Hatakeyama Y, Urayama M, Sato K.Superior labral strain during the throwing motion:A cadaveric study. Am J Sports Med 2001;29:488-492.
99. Kuhn JE, Lindholm SR, Huston LJ, Soslowsky LJ,Blasier RB. Failure of the biceps-superior labral complex:A cadaveric biomechanical investigation comparing thepositions of late cocking and early deceleration. Arthros-copy 2003;19:373-379.
100. Shepard MF, Dugas JR, Zeng N, Andrews JR. Differencesin the ultimate strength of the biceps anchor and thegeneration of type II superior labral anterior posteriorlesions in a cadaveric model. Am J Sports Med 2004;32:1197-1201.
101. Jobe CM. Superior glenoid impingement: Expandedspectrum. Arthroscopy 1995;11:530-537.
102. Walch G, Boileau P, Noel E, Donell ST. Impingement ofthe deep surface of the supraspinatus tendon on theposterosuperior glenoid rim: An arthroscopic study.J Shoulder Elbow Surg 1992;1:238-245.
103. Kuhn JE, Bey MJ, Huston LJ, Blasier RB, Soslowsky LJ.Ligamentous restraints to external rotation of thehumerus in the late-cocking phase of throwing. A
cadaveric biomechanical investigation. Am J Sports Med2000;28:200-205.
104. Levine W, Brandon ML, Stein BS, Gardner TR,Bigliani LU, Ahmad CS. Shoulder adaptive changes inyouth baseball players. J Shoulder Elbow Surg 2006;15:562-566.
105. Bigliani LU, Codd TP, Connor PM, Levine WN,Littlefield MA, Hershon SJ. Shoulder motion and laxityin the professional baseball player. Am J Sports Med 1997;25:609-613.
106. Edwards BT, Walch G. Techniques in internal impinge-ment surgery: Humeral derotational osteotomy. In:Barber FA, Fischer SP, eds. Surgical techniques for theshoulder and elbow. New York: Thieme, 2003;72-76.
107. Andrews JR. Glenoid labrum tears related to the longhead of the biceps. Am J Sports Med 1985;13:337-341.
108. Snyder SJ, Karzel RP, Del Pizzo W, Ferkel RD,Friedman MJ. SLAP lesions of the shoulder. Arthroscopy1990;6:274-279.
109. Jazrawi LM, McCluskey GM III, Andrews JR. Superiorlabral anterior and posterior lesions and internalimpingement in the overhead athlete. Instr Course Lect2003;52:43-63.
110. Trantalis JN, Lo IK. Superior labral anterior-posterior(SLAP) tears: Recent advances and outcomes. CurrOrthop Pract 2008;19:530-534.
111. Onyekwelu I, Khatib O, Zuckerman JD, Rokito AS,Kwon YW. The rising incidence of arthroscopic superiorlabrum anterior and posterior (SLAP) repairs. J ShoulderElbow Surg 2012;21:728-731.
112. Weber SC, Martin DF, Seiler JG III, Harrast JJ. Incidencerates, complications, and outcomes as reported byAmerican Board of Orthopedic Surgery. Part II candi-dates. Am J Sports Med 2012;40:1538-1543.
113. McFarland EG, Kim TK, Savino RM. Clinical assessmentof three common tests for superior labral anterior-posterior lesions. Am J Sports Med 2002;30:810-815.
114. Jost B, Zumstein M, Pfirrmann CW, Zanetti M, Gerber C.MRI findings in throwing shoulders: Abnormalitiesin professional handball players. Curr Orthop Pract 2005;434:130-137.
115. Gobezie R, Zurakowski D, Lavery K, Millett PJ, Cole BJ,Warner JJ. Analysis of interobserver and intraobservervariability in the diagnosis and treatment of SLAP tearsusing the Snyder classification. Am J Sports Med 2008;36:1373-1379.
116. Morgan CD, Burkhart SS, Palmeri M, Gillespie M. TypeII SLAP lesions: Three subtypes and their relationships tosuperior instability and rotator cuff tears. Arthroscopy1998;14:553-565.
117. Radkowski CA, Chhabra A, Baker CL III, Tejwani SG,Bradley JP. Arthroscopic capsulolabral repair for poste-rior shoulder instability in throwing athletes comparedwith nonthrowing athletes. Am J Sports Med 2008;36:693-699.
118. Rhee RG, Lee DH, Lim CT. Unstable isolated SLAP lesion:Clinical presentation and outcome of arthroscopic fixa-tion. Arthroscopy 2005;21:1099-1104.
119. Pagnani MJ, Warren RF. Instability of the shoulder. In:Nicholas JA, Hershman EB, eds. The upper extremity insports medicine. St. Louis: Mosby, 1995;173-208.
158 W. B. KIBLER ET AL.
120. Bankart AS, Cantab MC. Recurrent or habitual dislocationof the shoulder joint. Clin Orthop Relat Res 1993;291:3-6.
121. Veeger HEJ, van der Helm FCT. Shoulder function: Theperfect compromise between mobility and stability.J Biomech 2007;40:2119-2129.
122. Leetun DT, Ireland ML, Willson JD, Ballantyne BT,Davis IM. Core stability measures as risk factors for lowerextremity injury in athletes. Med Sci Sport Exerc 2004;36:926-934.
123. Kibler WB, Sciascia AD, Hester P, Dome D, Jacobs C.Clinical utility of new and traditional exam tests forbiceps and superior glenoid labral injuries. Am J SportsMed 2009;37:1840-1847.
124. O’Brien SJ, Pagnani MJ, Fealy S, McGlynn SR,Wilson JB. The active compression test: A new andeffective test for diagnosing labral tears and acromio-clavicular joint abnormality. Am J Sports Med 1998;26:610-613.
125. Jobe FW, Kvitne RS. Shoulder pain in the overhand orthrowing athlete the relationship of anterior instabilityand rotator cuff impingement. Orthop Rev 1989;18:963-975.
126. Connor PM, Banks DM, Tyson AB, Coumas JS,D’Alessandro DF. Magnetic resonance imaging ofthe asymptomatic shoulder of overhead athletes: A 5-year follow-up study. Am J Sports Med 2003;31:724-727.
127. Halbrecht JL, Tirman P, Atkin D. Internal impingementof the shoulder: Comparison of findings between thethrowing and nonthrowing shoulders of college baseballplayers. Arthroscopy 1999;15:253-258.
128. Jerosch J, Castro WH, Drescher H, Assheuer J. Magneticresonance morphologic changes in shoulder joints ofworld class water polo players. Sportverletz Sportschaden1993;7:109-114 (in German).
129. Miniaci A, Mascia AT, Salonen DC, Becker EJ. Magneticresonance imaging of the shoulder in asymptomaticprofessional baseball players. Am J Sports Med 2002;30:66-73.
130. Edwards SL, Lee JA, Bell JE, et al. Nonoperative treat-ment of superior labrum anterior posterior tears:Improvements in pain, function, and quality of life. Am JSports Med 2010;38:1456-1461.
131. Neri BR, ElAttrache NS, Owsley KC, Mohr K, Yocum LA.Outcome of type II superior labral anterior posteriorrepairs in elite overhead athletes: Effect of concomitantpartial-thickness rotator cuff tears. Am J Sports Med 2011;39:114-120.
132. Brockmeier SF, Voos JE, Williams RJ III, et al. Outcomesafter arthroscopic repair of type-II SLAP lesions. J BoneJoint Surg Am 2009;91:1595-1603.
133. Cerynik DL, Ewald TJ, Sastry A, Amin NH, Liao JG,Tom JA. Outcomes of isolated glenoid labral injuries inprofessional baseball pitchers. Clin J Sports Med 2008;18:255-258.
134. Cohen DB, Coleman S, Drakos MC, et al. Outcomes ofisolated type II SLAP lesions treated with arthroscopicfixation using a bioabsorbable tack. Arthroscopy 2006;22:136-142.
135. Cohen SB, Sheridan S, Ciccotti MG. Return to sports forprofessional baseball players after surgery of theshoulder or elbow. Sports Health 2011;3:105-111.
136. Cordasco FA, Steinmann S, Flatow EL, Bigliani LU.Arthroscopic treatment of glenoid labral tears. Am JSports Med 1993;21:425-431.
137. Field LD, Savoie FH III. Arthroscopic suture repair ofsuperior labral detachment lesions of the shoulder. Am JSports Med 1993;21:783-790.
138. Friel NA, Karas V, Slabaugh MA, Cole BJ. Outcomes oftype II superior labrum, anterior to posterior (SLAP)repair: Prospective evaluation at a minimum two-yearfollow-up. J Shoulder Elbow Surg 2010;19:859-867.
139. Glasgow SG, Bruce RA, Yacobucci GN, Torg JS. Arthro-scopic resection of glenoid labral tears in the athlete: Areport of 29 cases. Arthroscopy 1992;8:48-54.
140. Ide J, Maede S, Takagi K. Arthroscopic transtendinousrepair of partial-thickness articular-side tears of therotator cuff: Anatomical and clinical study. Am J SportsMed 2005;33:1672-1679.
141. Kim SH, Ha KI, Kim SH, Choi HJ. Results of arthroscopictreatment of superior labral lesions. J Bone Joint Surg Am2002;84:981-985.
142. Neuman BJ, Boisvert CB, Reiter B, Lawson K,Ciccotti MG, Cohen SB. Results of arthroscopic repair oftype II superior labral anterior posterior lesions inoverhead athletes: Assessment of return to preinjuryplaying level and satisfaction. Am J Sports Med 2011;39:1883-1888.
143. Pagnani MJ, Speer KP, Altchek DW, Warren RF,Dines DM. Arthroscopic fixation of superior labral lesionsusing a biodegradable implant: A preliminary report.Arthroscopy 1995;11:194-198.
144. Paletta GA. Results of arthroscopic treatment of SLAPtears in the throwing athlete. Presented at the ClosedMeeting of the American Shoulder and Elbow Surgeons,Scottsdale, AZ, October 20-23, 2010.
145. Ricchetti ET, Weidner Z, Lawrence JT, Sennett BJ,Huffman GR. Glenoid labral repair in Major LeagueBaseball pitchers. Int J Sports Med 2010;31:265-270.
146. Sanders KD. Results of arthroscopic treatment of SLAPtears in the throwing athlete. Presented at the AnnualConference of the American Society of Shoulder andElbow Therapists, Santa Barbara, CA, September 3-6,2008.
147. Yoneda M, Hirooka A, Saito S, Yamamoto T, Ochi T,Shino K. Arthroscopic stapling for detached superiorglenoid labrum. J Bone Joint Surg Br 1991;73:746-750.
148. Yung PS, Fong DT, Kong MF, et al. Arthroscopic repair ofisolated type II superior labrum anterior-posterior lesion.J Knee Surg Sports Traumatol Arthrosc 2008;16:1151-1157.
149. Savoie FH, Field LD, Atchinson S. Anterior superiorinstability with rotator cuff tearing: SLAC lesion. OrthopClin North Am 2001;32:457-461.
150. Burkhart SS, Lo IK, Brady PC. Burkhart’s view of theshoulder: A cowboy’s guide to advanced shoulder arthroscopy.Philadelphia: Lippincott Williams and Wilkins, 2006;3-316.
151. Andrews JR, Broussard TS, Carson WG. Arthroscopy ofthe shoulder in the management of partial tears of therotator cuff: A preliminary report. Arthroscopy 1985;1:117-122.
152. Conway JE. Arthroscopic repair of partial-thicknessrotator cuff tears and SLAP lesions in professional
DISABLED THROWING SHOULDER: 10-YEAR UPDATE 159
baseball players. Orthop Clin North Am 2001;32:443-456.
153. Payne LZ, Altchek DW, Craig EV, Warren RF. Arthro-scopic treatment of partial rotator cuff tears in youngathletes: A preliminary report. Am J Sports Med 1997;25:299-305.
154. Reynolds SB, Dugas JR, Cain EL, McMichael CS,Andrews JR. Debridement of small partial-thicknessrotator cuff tears in elite overhead athletes. Clin OrthopRelat Res 2008;466:614-621.
155. Riand N, Boulahia A, Walch G. Posterosuperiorimpingement of the shoulder in the athlete: Results ofarthroscopic debridement in 75 patients. Rev Chir OrthopReparatrice Appar Mot 2002;88:19-27 (in French).
156. Liem D, Lichtenberg S, Magosch P, Habermeyer P.Arthroscopic rotator cuff repair in overhead-throwingathletes. Am J Sports Med 2008;36:1317-1322.
157. Mazoue CG, Andrews JR. Repair of full-thickness rotatorcuff tears in professional baseball players. Am J Sports Med2006;34:182-189.
158. Kuhn JE, Wiesner R, Schewe T. External rotation of theglenohumeral joint: Ligament restraints and muscleeffects in the neutral and abducted positions. J ShoulderElbow Surg 2005;14:S39-S48.
159. Lyman S, Fleisig GS, Andrews JR, Osinski ED. Effect ofpitch type, pitch count, and pitching mechanics on risk ofelbow and shoulder pain in youth baseball pitchers. Am JSports Med 2002;30:463-468.
160. Rutherford OM, Jones DA. The role of learning andcoordination in strength training. Eur J Appl Physiol OccupPhysiol 1986;55:100-105.
161. Sale DG. Neural adaptation to resistance training. Med SciSport Exerc 1988;20:S135-S145.
162. Jones DA, Rutherford OM, Parker DF. Physiologicalchanges in skeletal muscle as a result of strengthtraining. Quant J Exp Physiol 1989;74:233-256.
163. Toyoshima S, Hoshikawa T, Miyashita M. Contributions ofbody parts to throwing performance. In: Biomechanics IV.Baltimore: University Park Press, 1974;169-174.
164. Stodden DF, Fleisig GS, McLean SP, Lyman SL,Andrews JR. Relationship of pelvis and upper torsokinematics to pitched baseball velocity. J Appl Biomech2001;17:164-172.
165. Tippett SR. Lower extremity strength and active range ofmotion in college baseball pitchers: A comparisonbetween stance leg and kick leg. J Orthop Sport Phys Ther1986;8:10-14.
166. Laudner KG, Moore SD, Sipes RC, Meister K. Functionalhip characteristics of baseball pitchers andposition players.Am J Sports Med 2010;38:383-391.
167. MacWilliams BA, Choi T, Perezous MK, Chao EY,McFarland EG. Characteristic ground-reaction forces inbaseball pitching. Am J Sports Med 1998;26:66-71.
168. McGill SM, Karpowicz A, Fenwick CM. Ballisticabdominal exercises: Muscle activation patterns duringthree activities along the stability/mobility continuum.J Strength Cond Res 2009;23:898-905.
169. Voight M, Hoogenboom BJ, Cook G. The chop and liftreconsidered: Integrating neuromuscular principles intoorthopedic and sports rehabilitation. N Am J Sports PhysTher 2008;3:151-159.
170. Imai A, Kaneoka K, Okubo Y, et al. Trunk muscleactivity during lumbar stabilization exercises on botha stable and unstable surface. J Orthop Sports Phys Ther2010;40:369-375.
171. Escamilla RF, Lewis C, Bell D, et al. Core muscle acti-vation during Swiss ball and traditional abdominalexercises. J Orthop Sports Phys Ther 2010;40:265-276.
172. Stanton R, Reaburn PR, Humphries B. The effect ofshort-term Swiss ball training on core stability andrunning economy. J Strength Cond Res 2004;18:522-528.
173. Saeterbakken AH, van den Tillaar R, Seiler S. Effectof core stability training on throwing velocity infemale handball players. J Strength Cond Res 2011;25:712-718.
174. Shanley E, Rauh MJ, Michener LA, Ellenbecker TS,Garrison JC, Thigpen CA. Shoulder range of motionmeasures as risk factors for shoulder and elbow injuriesin high school softball and baseball players. Am J SportsMed 2006;39:1997-2006.
175. McClure P, Balaicuis J, Heiland D, Broersma ME,Thorndike CK, Wood A. A randomized controlledcomparison of stretching procedures for posteriorshoulder tightness. J Orthop Sport Phys Ther 2007;37:108-114.
176. Manske RC, Meschke M, Porter A, Smith B, Reiman M.A randomized controlled single-blinded comparison ofstretching versus stretching and joint mobilization forposterior shoulder tightness measured by internal rota-tion motion loss. Sports Health 2010;2:94-100.
177. Moore SD, Laudner KG, McLoda TA, Shaffer MA. Theimmediate effects of muscle energy technique onposterior shoulder tightness: A randomized controlledtrial. J Orthop Sport Phys Ther 2011;41:400-407.
178. Cools AM, Johansson FR, Cambier DC, Velde AV,Palmans T, Witvrouw EE. Descriptive profile of scap-ulothoracic position, strength, and flexibility variables inadolescent elite tennis players. Br J Sport Med 2010;44:678-684.
179. van Linschoten R, van Middelkoop M, Berger MY, et al.Supervised exercise therapy versus usual care for patel-lofemoral pain syndrome: An open label randomisedcontrolled trial. BMJ 2009;339:b4074.
180. Bennell K, Coburn S, Wee E, Green S, Harris A,Forbes A, Buchbinder R. Efficacy and cost-effectivenessof a physiotherapy program for chronic rotator cuffpathology: A protocol for a randomised, double-blind,placebo-controlled trial. BMC Musculoskelet Disord 2007;8:86-98.
181. Deyle GD, Allison SC, Matekel RL, et al. Physical therapytreatment effectiveness for osteoarthritis of the knee: Arandomized comparison of supervised clinical exerciseand manual therapy procedures versus a home exerciseprogram physical therapy. Phys Ther 2005;85:1301-1317.
182. Brown LP, Niehues SL, Harrah A, Yavorsky P,Hirshman HP. Upper extremity range of motion and iso-kinetic strength of the internal and external shoulderrotators inMajor League Baseball players.Am J Sports Med1988;16:577-585.
183. Ellenbecker TS, Mattalino A. Concentric isokineticshoulder internal and external rotation strength in
160 W. B. KIBLER ET AL.
professional baseball pitchers. J Orthop Sport Phys Ther1997;25:323-328.
184. Mulligan IJ, BiddingtonWB, Barnhart BD, Ellenbecker TS.Isokinetic profile of shoulder internal and external rotatorsof high school aged baseball pitchers. J Strength Cond Res2004;18:861-866.
185. Wilk KE, Andrews JR, Arrigo CA, Keirns MA, Erber DJ.The strength characteristics of internal and externalrotator muscles in professional baseball pitchers. AmJ Sports Med 1993;21:61-66.
186. Byram IR, Bushnell BD, Dugger K, Charron K,Harrell FE Jr, Noonan TJ. Preseason shoulder strengthmeasurements in professional baseball pitchers: Identi-fying players at risk for injury. Am J Sports Med 2010;38:1375-1382.
187. Merolla G, De Santis E, Campi F, Paladini P, Porcellini G.Supraspinatus and infraspinatus weakness in overheadathletes with scapular dyskinesis: Strength assessmentbefore and after restoration of scapular musculaturebalance. Musculoskelet Surg 2010;94:119-125.
188. Stickley CD, Hetzler RK, Freemyer BG, Kimura IF. Iso-kinetic peak torque ratios and shoulder injury history inadolescent female volleyball players. J Athl Train2008;43:571-577.
189. CoolsAM,WitvrouwEE,DeclercqGA,VanderstraetenGG,Cambier DC. Evaluation of isokinetic force production andassociated muscle activity in the scapular rotators duringa protraction-retraction movement in overhead athleteswith impingement symptoms. Br J Sport Med 2004;38:64-68.
190. Roy JS, Moffet H, McFadyen BJ. Upper limb motorstrategies in persons with and without shoulderimpingement syndrome across different speeds ofmovement. Clin Biomech 2008;23:1227-1236.
191. Ellenbecker TS, Cools A. Rehabilitation of shoulderimpingement syndrome and rotator cuff injuries:An evidence-based review. Br J Sport Med 2010;44:319-327.
192. Roy JS, Moffet H, McFadyen BJ, Lirette R. Impact ofmovement training on upper limb motor strategies inpersons with shoulder impingement syndrome. SportsMed Arthrosc Rehabil Ther Technol 2009;1:8.
193. Mottram SL, Woledge RC, Morrissey D. Motion analysisstudy of a scapular orientation exercise and subjects’ability to learn the exercise. Man Ther 2009;14:13-18.
194. Lin JJ, Hsieh SC, Cheng WC, Chen WC, Lai Y. Adaptivepatterns of movement during arm elevation test inpatients with shoulder impingement syndrome. J OrthopRes 2010;29:653-657.
195. Inman VT, Saunders M, Abbot LC. Observations on thefunction of the shoulder joint. J Bone Joint Surg Am1944;26:1-30.
196. Kibler WB, Sciascia AD, Uhl TL, Tambay N,Cunningham T. Electromyographic analysis of specificexercises for scapular control in early phases of shoulderrehabilitation. Am J Sports Med 2008;36:1789-1798.
197. Blackburn TA, White B, McLeod WD, Wofford L. EMGanalysis of posterior rotator cuff exercises. Athl Train1990;25:40-45.
198. McCann PD, Wootten ME, Kadaba MP, Bigliani LU.A kinematic and electromyographic study of shoulder
rehabilitation exercises. Clin Orthop Relat Res 1993:179-188.
199. Malanga GA, Jenp YN, Growney ES, An KN. EMGanalysis of shoulder positioning in testing and strength-ening the supraspinatus. Med Sci Sport Exerc 1996;28:661-664.
200. Cordasco FA, Wolfe IN, Wootten ME, Bigliani LU. Anelectromyographic analysis of the shoulder duringa medicine ball rehabilitation program. Am J Sports Med1996;24:386-392.
201. Hintermeister RA, Lange GW, Schultheis JM, Bey MJ,Hawkins RJ. Electromyographic activity and applied loadduring shoulder rehabilitation exercises using elasticresistance. Am J Sports Med 1998;26:210-220.
202. Suenaga N, Minami A, Fujisawa H. Electromyographicanalysis of internal rotational motion of the shoulder invarious arm positions. J Shoulder Elbow Surg 2003;12:501-505.
203. Decker MJ, Tokish JM, Ellis HB, Torry MR,Hawkins RJ. Subscapularis muscle activity duringselected rehabilitation exercises. Am J Sports Med2003;31:126-134.
204. Ekstrom RA, Bifulco KM, Lopau CJ, Andersen CF,Gough JR. Comparing the function of the upper andlower parts of the serratus anterior muscle using surfaceelectromyography. J Orthop Sport Phys Ther 2004;34:235-243.
205. Reinold MM, Wilk KE, Fleisig GS, et al. Electromyo-graphic analysis of the rotator cuff and deltoid muscu-lature during common shoulder external rotationexercises. J Orthop Sport Phys Ther 2004;34:385-394.
206. Myers JB, Pasquale MR, Laudner KG, Sell TC,Bradley JP, Lephart SM. On-the-field resistance tubingexercises for throwers: An electromyographic analysis.J Athl Train 2005;40:15-22.
207. Ekstrom RA, Soderberg GL, Donatelli RA. Normalizationprocedures using maximum voluntary isometriccontractions for the serratus anterior and trapeziusmuscles during surface EMG analysis. J ElectromyogrKinesiol 2005;15:418-428.
208. Moseley JB Jr, Jobe FW, Pink M, Perry J, Tibone J. EMGanalysis of the scapular muscles during a shoulder reha-bilitation program. Am J Sports Med 1992;20:128-134.
209. Townsend H, Jobe FW, Pink M, Perry J. Electromyo-graphic analysis of the glenohumeral muscles duringa baseball rehabilitation program. Am J Sports Med1991;19:264-272.
210. Ludewig PM, Hoff MS, Osowski EE, Meschke SA,Rundquist PJ. Relative balance of serratus anterior andupper trapezius muscle activity during push-up exer-cises. Am J Sports Med 2004;32:484-493.
211. Cools AM, Declercq GA, Cambier DC, Mahieu NN,Witvrouw EE. Trapezius activity and intramuscularbalance during isokinetic exercise in overhead athleteswith impingement symptoms. Scand J Med Sci Sports 2007;17:25-33.
212. Maenhout A, Van Praet K, Pizzi L, Van Herzeele M,Cools A. Electromyographic analysis of knee push upplus variations: What is the influence of the kinetic chainon scapular muscle activity? J Orthop Sport Phys Ther2010;40:169-179.
DISABLED THROWING SHOULDER: 10-YEAR UPDATE 161
213. Roy JS, Moffet H, Hébert LJ, Lirette R. Effect of motorcontrol and strengthening exercises on shoulder func-tion in persons with impingement syndrome: A single-subject study design. Man Ther 2009;14:180-188.
214. Thigpen CA, Padua DA, Morgan N, Kreps C, Karas SG.Scapular kinematics during supraspinatus rehabilitationexercise: A comparison of full-can versus empty-cantechniques. Am J Sports Med 2006;34:644-652.
215. Ellenbecker TS, Davies GJ, Rowinski MJ. Concentricversus eccentric isokinetic strengthening of the rotatorcuff. Objective data versus functional test. Am J SportsMed 1988;16:64-69.
216. Mont MA, Cohen DB, Campbell KR, Gravare K,Mathur SK. Isokinetic concentric versus eccentrictraining of shoulder rotators with functional evaluationof performance enhancement in elite tennis players. AmJ Sports Med 1994;22:513-517.
217. Carter AB, Kaminski TW, Douex AT Jr, Knight CA,Richards JG. Effects of high volume upper extremityplyometric training on throwing velocity and functionstrength ratios of the shoulder rotators in college baseballplayers. J Strength Cond Res 2007;21:208-215.
218. Davies GJ, Matheson JW. Shoulder plyometrics. SportsMed Arthrosc 2001;9:1-18.
219. Ebben WP, Hintz MJ, Simenz CJ. Strength and condi-tioning practices of Major League Baseball strength andconditioning coaches. J Strength CondRes2005;19:538-546.
220. McEvoy KP, Newton RU. Baseball throwing speed andbase running speed: The effects of ballistic resistancetraining. J Strength Cond Res 1998;12:216-221.
221. Escamilla RF, Fleisig GS, Yamashiro K, et al. Effects of a 4-week youth baseball conditioning program on throwingvelocity. J Strength Cond Res 2010;24:3247-3254.
222. Escamilla RF, Ionno M, deMahy MS, et al. Comparisonof three baseball-specific 6-week training programs onthrowing velocity in high school baseball players.J Strength Cond Res 2012;26:1767-1781.
223. Swanik KA, Lephart SM, Huxel K. The effect of func-tional training on the incidence of shoulder pain andstrength in intercollegiate swimmers. J Sport Rehabil2002;11:140-154.
224. Sciascia AD, Kibler WB. The pediatric throwing athlete:What is the real problem? Clin J Sport Med 2006;16:471-477.
225. Wilk KE, Obma P, Simpson CD, Cain EL, Dugas JR,Andrews JR. Shoulder injuries in the overhead athlete.J Orthop Sport Phys Ther 2009;39:38-54.
226. Fleisig GS, Andrews JR, Cutter GR, et al. Risk of seriousinjury for young baseball pitchers: A 10-year prospectivestudy. Am J Sports Med 2011;39:253-257.
227. Lyman S, Fleisig GS, Waterbor JW, et al. Longitudinalstudy of elbow and shoulder pain in youth baseballpitchers. Med Sci Sports Exerc 2001;33:1803-1810.
228. Alfredson H, Pietilä T, Jonsson P, Lorentzon R. Heavy-load eccentric calf muscle training for the treatment ofchronic Achilles tendinosis. Am J Sports Med 1998;26:360-366.
229. Young MA, Cook JL, Purdam CR, Kiss ZS, Alfredson H.Eccentric decline squat protocol offers superior results at12 months compared with traditional eccentric protocolfor patellar tendinopathy in volleyball players. Br J SportMed 2005;39:102-105.
230. Jonsson P, Wahlström P, Ohberg L, Alfredson H.Eccentric training in chronic painful impingementsyndrome of the shoulder: Results of a pilot study. KneeSurg Sports Traumatol Arthrosc 2006;14:76-81.
231. Bernhardsson S, Klintberg IH, Wendt GK. Evaluationof an exercise concept focusing on eccentric strengthtraining of the rotator cuff for patients with sub-acromial impingement syndrome. Clin Rehabil 2011;25:69-78.
232. Wilk Ke, Yenchak AJ, Arrigo CA, Andrews JR. Theadvanced throwers ten exercise program: a new exerciseseries for enhanced dynamic shoulder control in theoverhead throwing athlete. Phys Sportsmed 2011;39:90-97.
233. Ide J, Maede S, Takagi K. Sports activity after arthro-scopic superior labral repair using suture anchors inoverhead-throwing athletes. Am J Sports Med 2005;33:507-514.
234. Andrews JR, Carson WG, McLeod WD. Glenoid labrumtears related to the long head of the biceps. Am J SportsMed 1985;13:337-341.
235. Ellenbecker TS, Ellenbecker GA, Roetert EP, Silva RT,Keuter G, Sperling F. Descriptive profile of hip rotationrange of motion in elite tennis players and professionalbaseball pitchers. Am J Sports Med 2007;35:1371-1376.
236. Baltaci G, Johnson R, Kohl H. Shoulder range of motioncharacteristics in collegiate baseball players. J Sports MedPhys Fitness 2001;41:236-242.
237. Wilk KE, Macrina LC, Arrigo C. Passive range of motioncharacteristics in the overhead baseball pitcher and theirimplications for rehabilitation. Clin Orthop Relat Res2012;470:1586-1594.
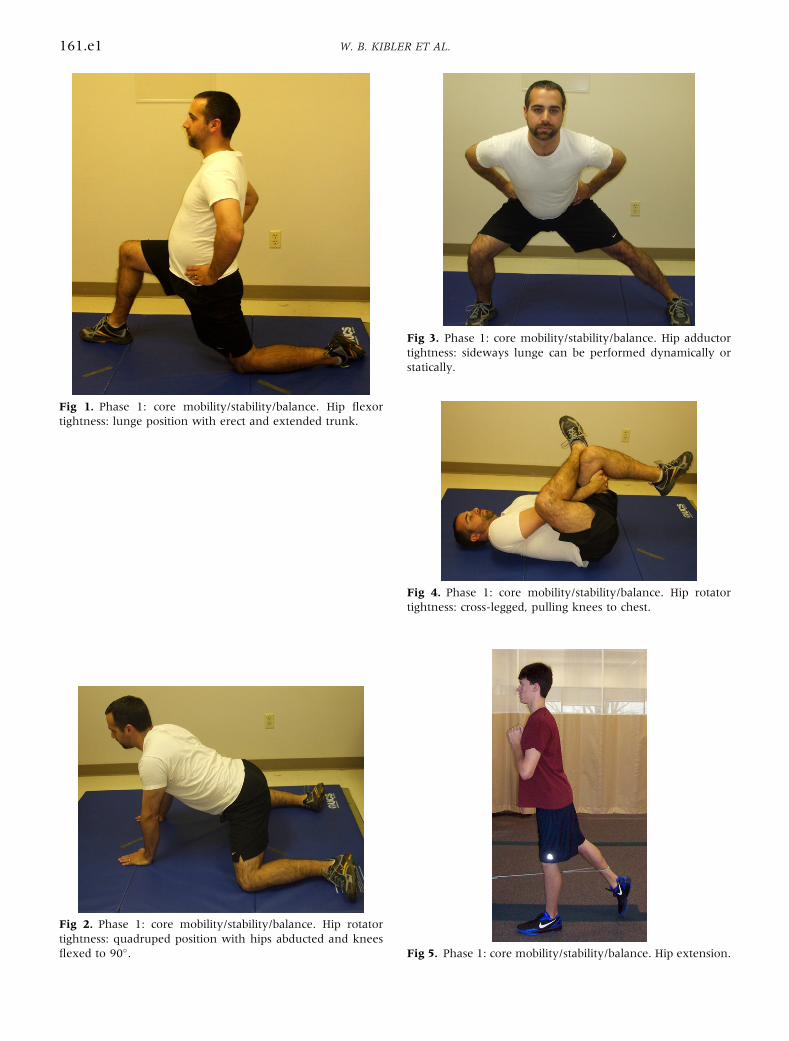
Fig 2. Phase 1: core mobility/stability/balance. Hip rotatortightness: quadruped position with hips abducted and kneesflexed to 90�.
Fig 3. Phase 1: core mobility/stability/balance. Hip adductortightness: sideways lunge can be performed dynamically orstatically.
Fig 4. Phase 1: core mobility/stability/balance. Hip rotatortightness: cross-legged, pulling knees to chest.
Fig 5. Phase 1: core mobility/stability/balance. Hip extension.
Fig 1. Phase 1: core mobility/stability/balance. Hip flexortightness: lunge position with erect and extended trunk.
161.e1 W. B. KIBLER ET AL.
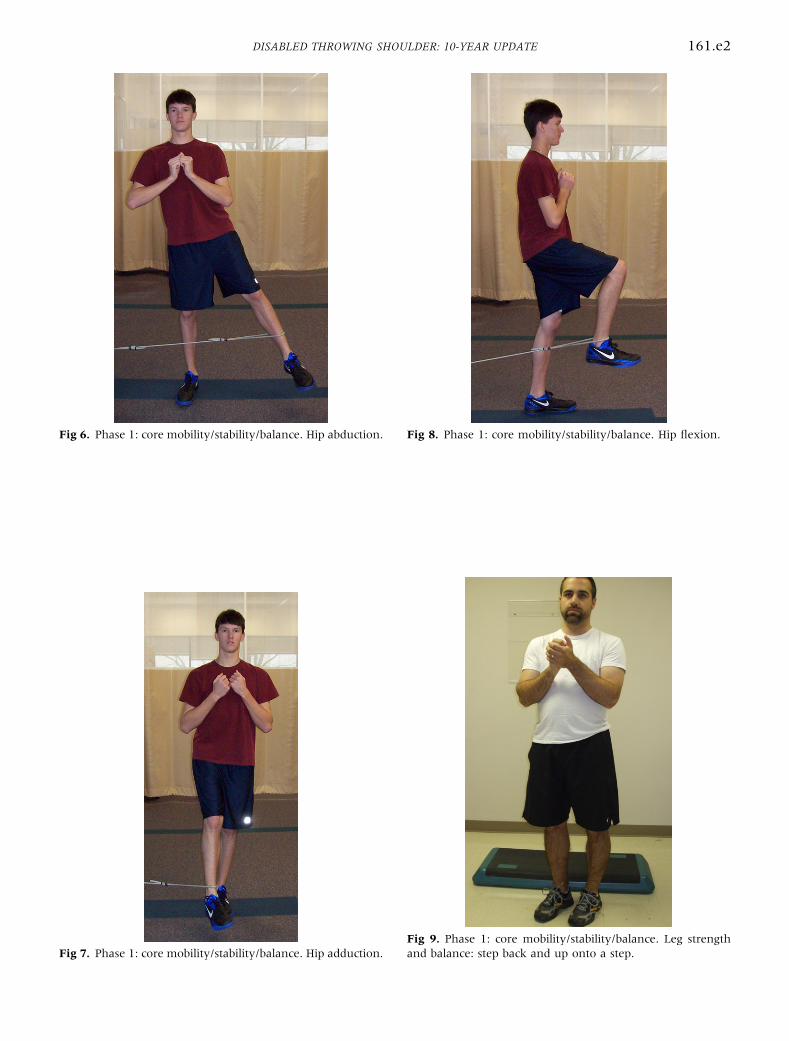
Fig 9. Phase 1: core mobility/stability/balance. Leg strengthand balance: step back and up onto a step.Fig 7. Phase 1: core mobility/stability/balance. Hip adduction.
Fig 8. Phase 1: core mobility/stability/balance. Hip flexion.Fig 6. Phase 1: core mobility/stability/balance. Hip abduction.
DISABLED THROWING SHOULDER: 10-YEAR UPDATE 161.e2
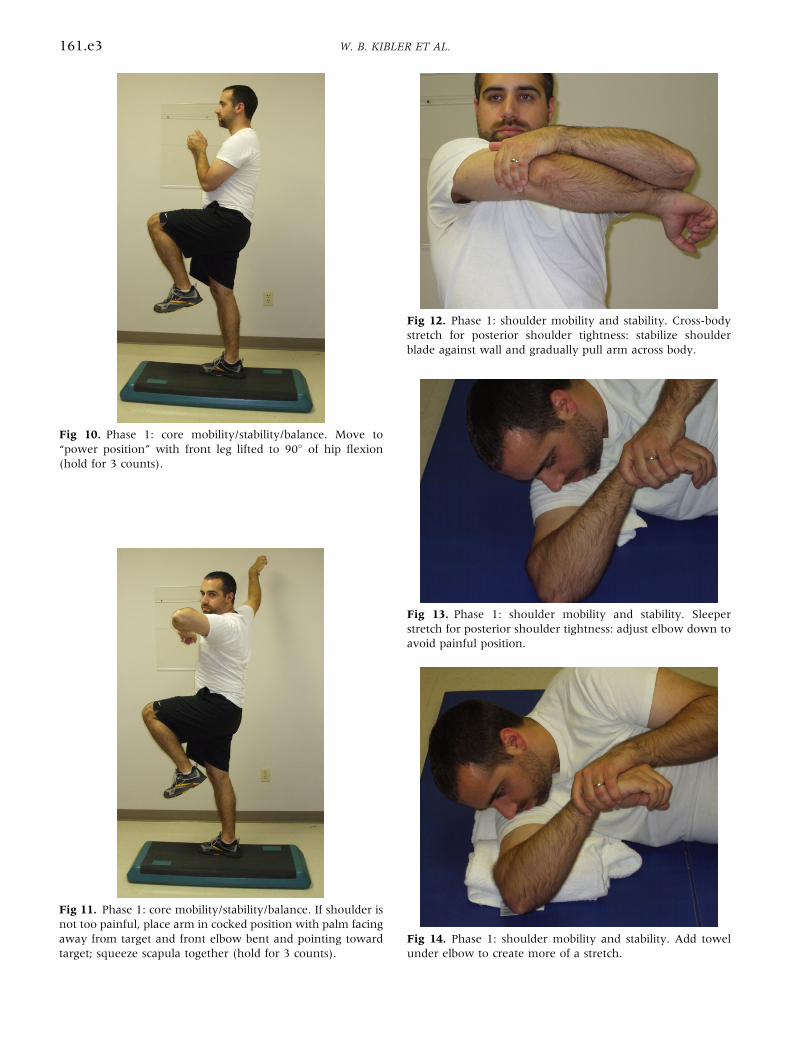
Fig 11. Phase 1: core mobility/stability/balance. If shoulder isnot too painful, place arm in cocked position with palm facingaway from target and front elbow bent and pointing towardtarget; squeeze scapula together (hold for 3 counts).
Fig 12. Phase 1: shoulder mobility and stability. Cross-bodystretch for posterior shoulder tightness: stabilize shoulderblade against wall and gradually pull arm across body.
Fig 13. Phase 1: shoulder mobility and stability. Sleeperstretch for posterior shoulder tightness: adjust elbow down toavoid painful position.
Fig 14. Phase 1: shoulder mobility and stability. Add towelunder elbow to create more of a stretch.
Fig 10. Phase 1: core mobility/stability/balance. Move to“power position” with front leg lifted to 90� of hip flexion(hold for 3 counts).
161.e3 W. B. KIBLER ET AL.
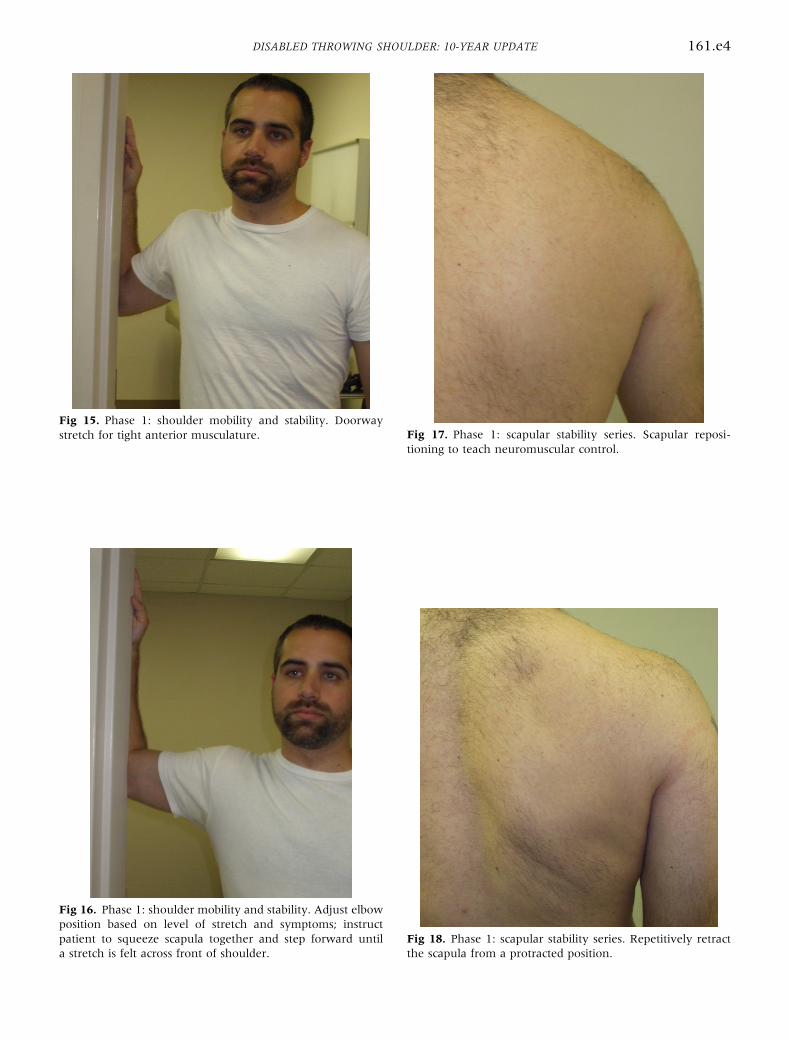
Fig 16. Phase 1: shoulder mobility and stability. Adjust elbowposition based on level of stretch and symptoms; instructpatient to squeeze scapula together and step forward untila stretch is felt across front of shoulder.
Fig 17. Phase 1: scapular stability series. Scapular reposi-tioning to teach neuromuscular control.
Fig 18. Phase 1: scapular stability series. Repetitively retractthe scapula from a protracted position.
Fig 15. Phase 1: shoulder mobility and stability. Doorwaystretch for tight anterior musculature.
DISABLED THROWING SHOULDER: 10-YEAR UPDATE 161.e4
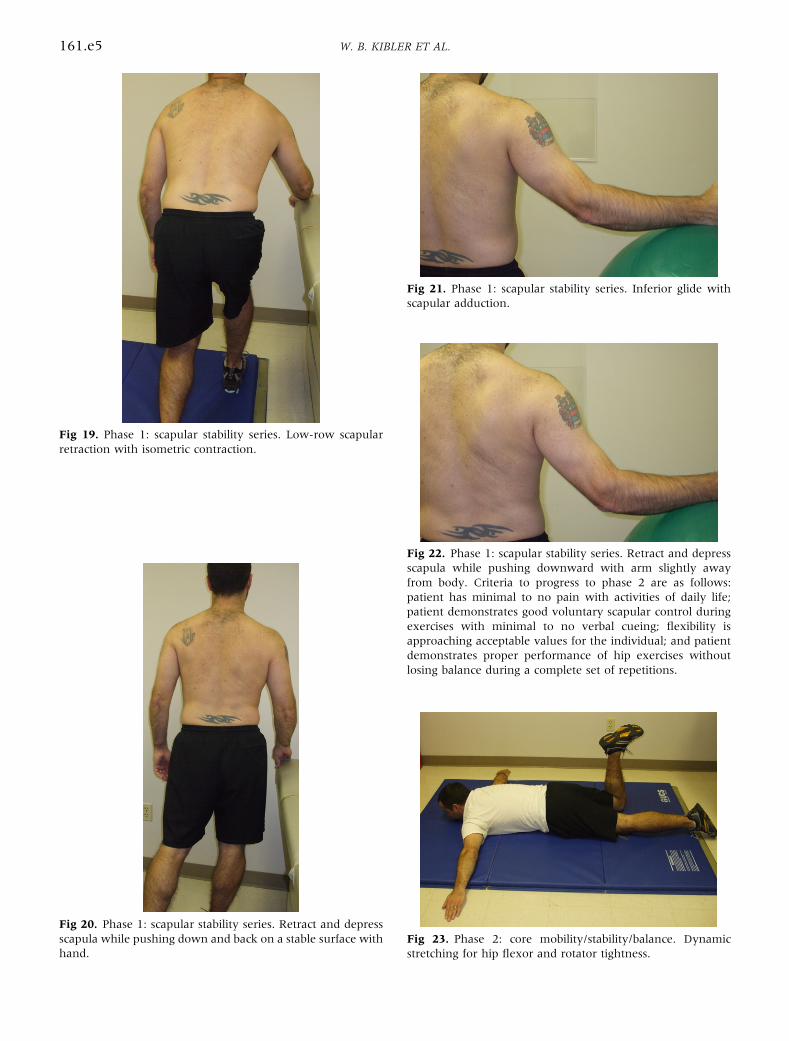
Fig 19. Phase 1: scapular stability series. Low-row scapularretraction with isometric contraction.
Fig 20. Phase 1: scapular stability series. Retract and depressscapula while pushing down and back on a stable surface withhand.
Fig 21. Phase 1: scapular stability series. Inferior glide withscapular adduction.
Fig 22. Phase 1: scapular stability series. Retract and depressscapula while pushing downward with arm slightly awayfrom body. Criteria to progress to phase 2 are as follows:patient has minimal to no pain with activities of daily life;patient demonstrates good voluntary scapular control duringexercises with minimal to no verbal cueing; flexibility isapproaching acceptable values for the individual; and patientdemonstrates proper performance of hip exercises withoutlosing balance during a complete set of repetitions.
Fig 23. Phase 2: core mobility/stability/balance. Dynamicstretching for hip flexor and rotator tightness.
161.e5 W. B. KIBLER ET AL.
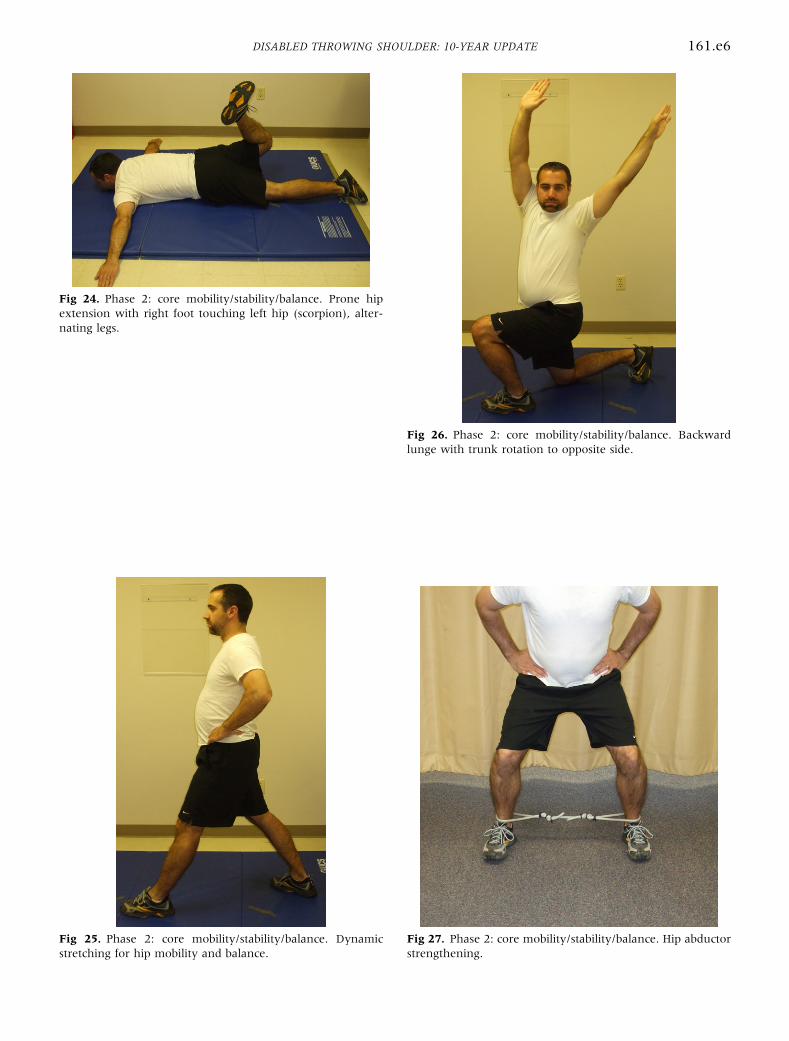
Fig 24. Phase 2: core mobility/stability/balance. Prone hipextension with right foot touching left hip (scorpion), alter-nating legs.
Fig 25. Phase 2: core mobility/stability/balance. Dynamicstretching for hip mobility and balance.
Fig 26. Phase 2: core mobility/stability/balance. Backwardlunge with trunk rotation to opposite side.
Fig 27. Phase 2: core mobility/stability/balance. Hip abductorstrengthening.
DISABLED THROWING SHOULDER: 10-YEAR UPDATE 161.e6
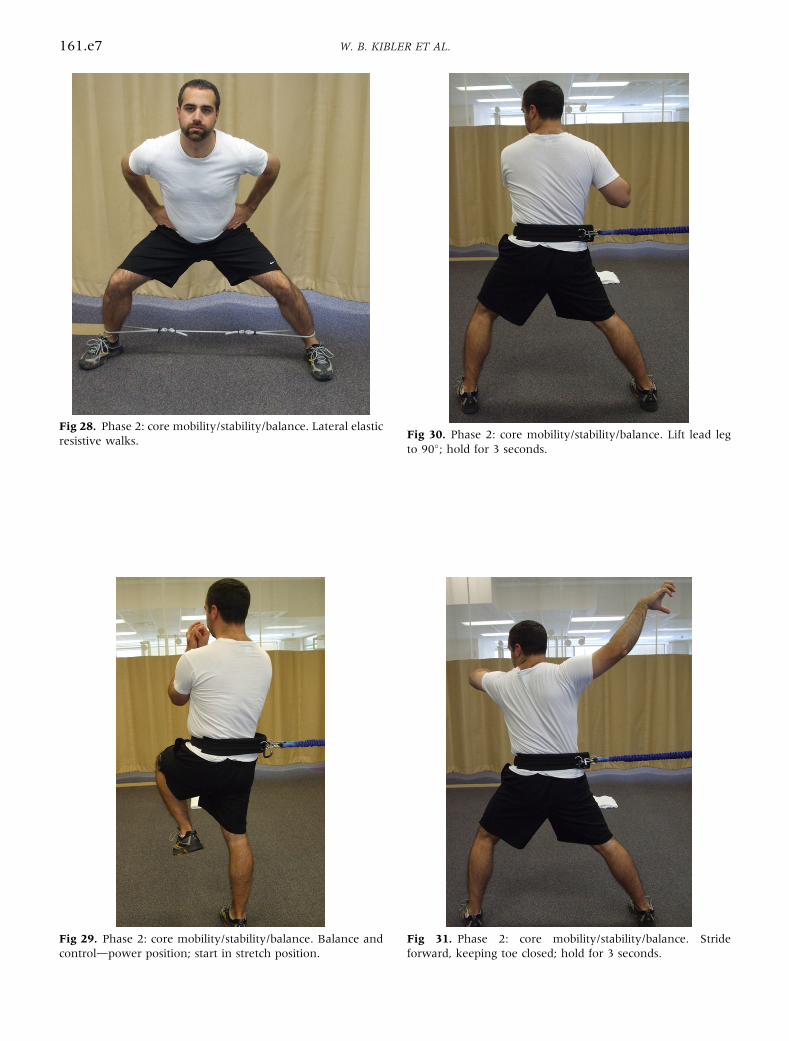
Fig 28. Phase 2: core mobility/stability/balance. Lateral elasticresistive walks.
Fig 29. Phase 2: core mobility/stability/balance. Balance andcontroldpower position; start in stretch position.
Fig 30. Phase 2: core mobility/stability/balance. Lift lead legto 90�; hold for 3 seconds.
Fig 31. Phase 2: core mobility/stability/balance. Strideforward, keeping toe closed; hold for 3 seconds.
161.e7 W. B. KIBLER ET AL.
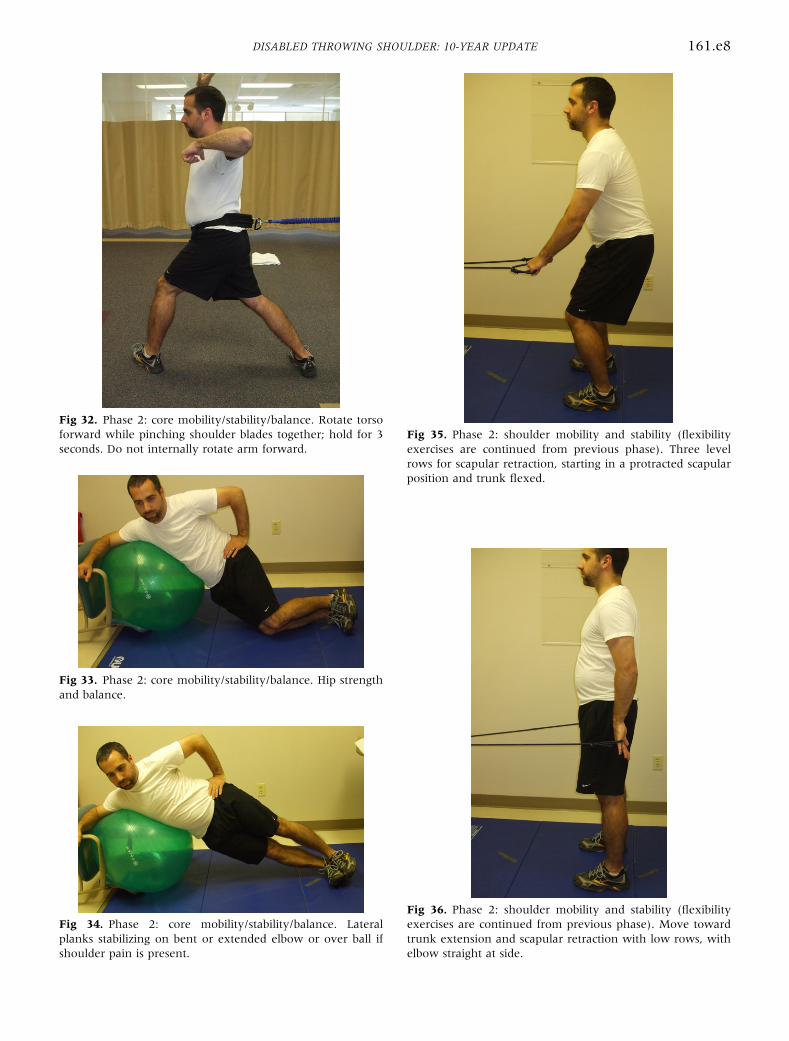
Fig 32. Phase 2: core mobility/stability/balance. Rotate torsoforward while pinching shoulder blades together; hold for 3seconds. Do not internally rotate arm forward.
Fig 33. Phase 2: core mobility/stability/balance. Hip strengthand balance.
Fig 34. Phase 2: core mobility/stability/balance. Lateralplanks stabilizing on bent or extended elbow or over ball ifshoulder pain is present.
Fig 35. Phase 2: shoulder mobility and stability (flexibilityexercises are continued from previous phase). Three levelrows for scapular retraction, starting in a protracted scapularposition and trunk flexed.
Fig 36. Phase 2: shoulder mobility and stability (flexibilityexercises are continued from previous phase). Move towardtrunk extension and scapular retraction with low rows, withelbow straight at side.
DISABLED THROWING SHOULDER: 10-YEAR UPDATE 161.e8
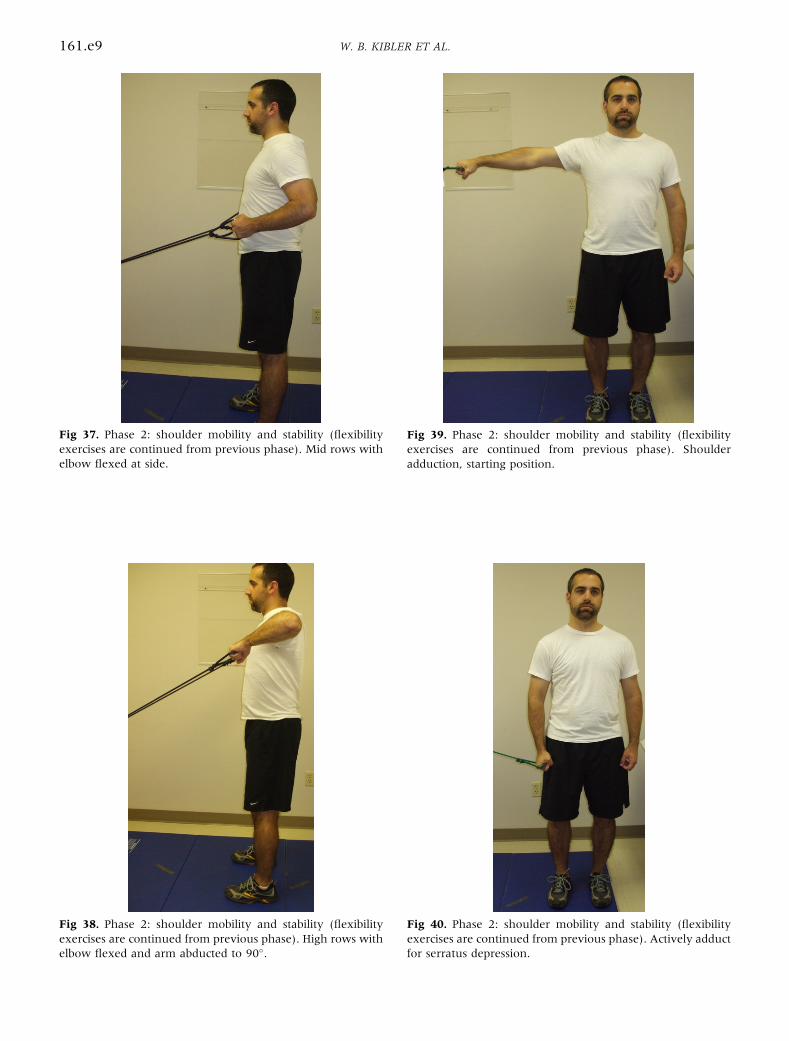
Fig 37. Phase 2: shoulder mobility and stability (flexibilityexercises are continued from previous phase). Mid rows withelbow flexed at side.
Fig 38. Phase 2: shoulder mobility and stability (flexibilityexercises are continued from previous phase). High rows withelbow flexed and arm abducted to 90�.
Fig 39. Phase 2: shoulder mobility and stability (flexibilityexercises are continued from previous phase). Shoulderadduction, starting position.
Fig 40. Phase 2: shoulder mobility and stability (flexibilityexercises are continued from previous phase). Actively adductfor serratus depression.
161.e9 W. B. KIBLER ET AL.
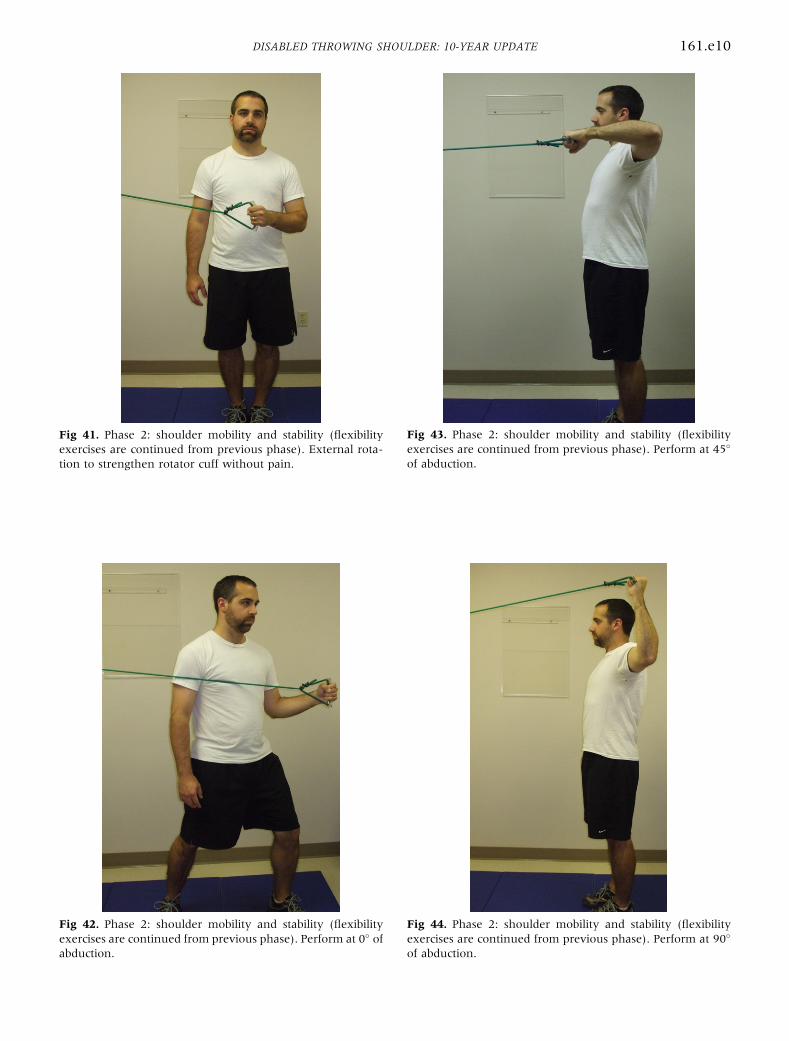
Fig 41. Phase 2: shoulder mobility and stability (flexibilityexercises are continued from previous phase). External rota-tion to strengthen rotator cuff without pain.
Fig 42. Phase 2: shoulder mobility and stability (flexibilityexercises are continued from previous phase). Perform at 0� ofabduction.
Fig 43. Phase 2: shoulder mobility and stability (flexibilityexercises are continued from previous phase). Perform at 45�
of abduction.
Fig 44. Phase 2: shoulder mobility and stability (flexibilityexercises are continued from previous phase). Perform at 90�
of abduction.
DISABLED THROWING SHOULDER: 10-YEAR UPDATE 161.e10
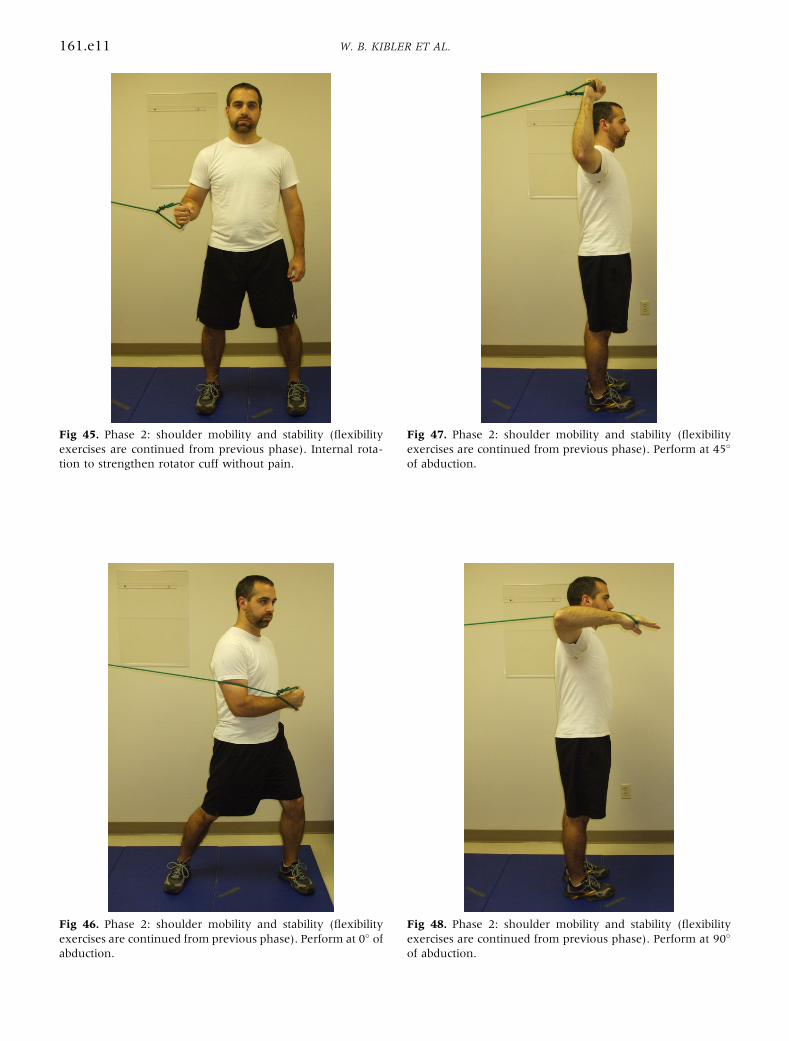
Fig 45. Phase 2: shoulder mobility and stability (flexibilityexercises are continued from previous phase). Internal rota-tion to strengthen rotator cuff without pain.
Fig 46. Phase 2: shoulder mobility and stability (flexibilityexercises are continued from previous phase). Perform at 0� ofabduction.
Fig 47. Phase 2: shoulder mobility and stability (flexibilityexercises are continued from previous phase). Perform at 45�
of abduction.
Fig 48. Phase 2: shoulder mobility and stability (flexibilityexercises are continued from previous phase). Perform at 90�
of abduction.
161.e11 W. B. KIBLER ET AL.
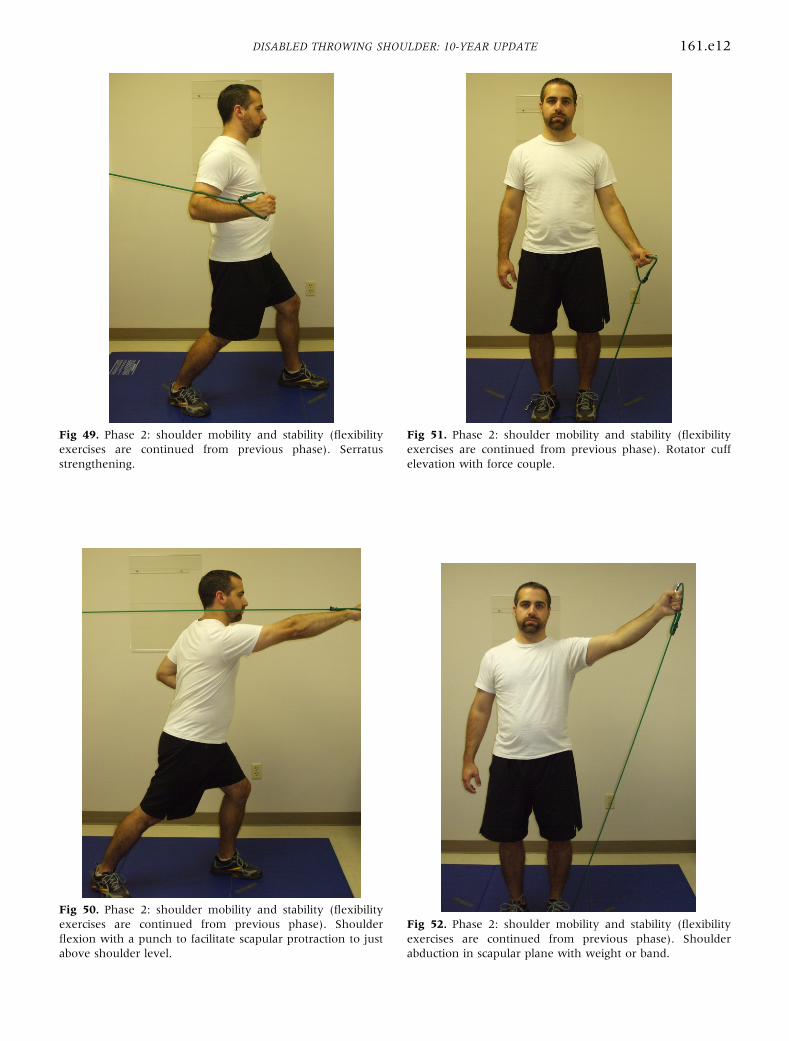
Fig 49. Phase 2: shoulder mobility and stability (flexibilityexercises are continued from previous phase). Serratusstrengthening.
Fig 50. Phase 2: shoulder mobility and stability (flexibilityexercises are continued from previous phase). Shoulderflexion with a punch to facilitate scapular protraction to justabove shoulder level.
Fig 51. Phase 2: shoulder mobility and stability (flexibilityexercises are continued from previous phase). Rotator cuffelevation with force couple.
Fig 52. Phase 2: shoulder mobility and stability (flexibilityexercises are continued from previous phase). Shoulderabduction in scapular plane with weight or band.
DISABLED THROWING SHOULDER: 10-YEAR UPDATE 161.e12
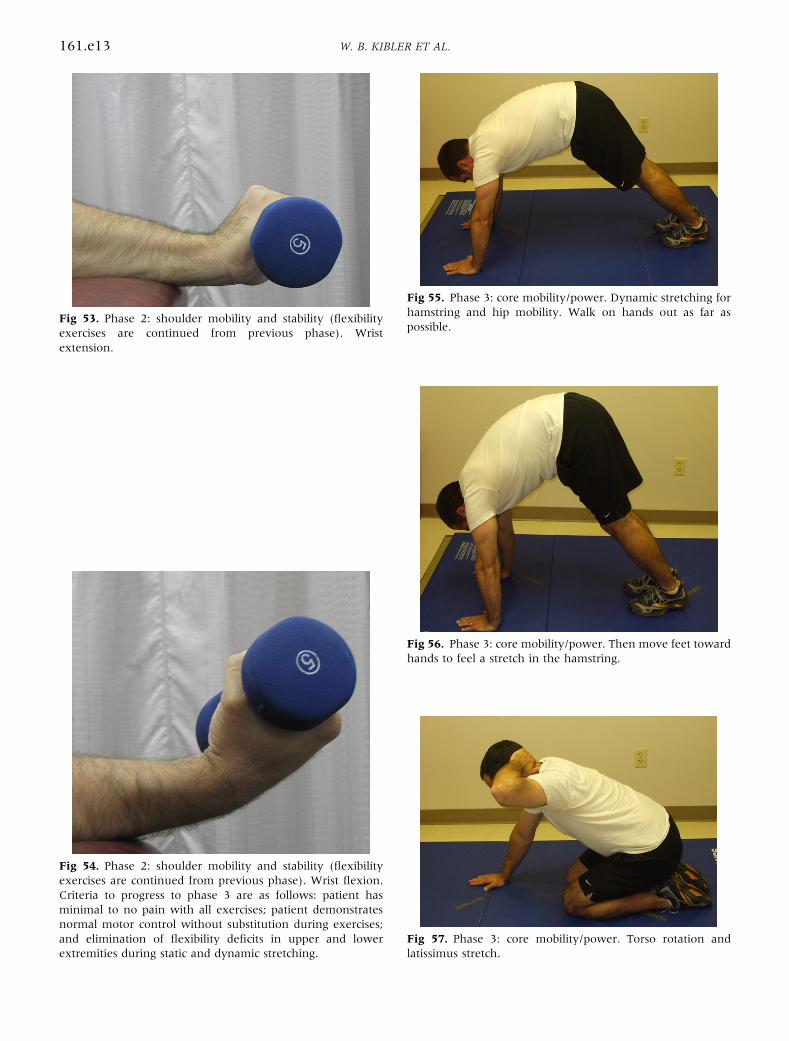
Fig 53. Phase 2: shoulder mobility and stability (flexibilityexercises are continued from previous phase). Wristextension.
Fig 54. Phase 2: shoulder mobility and stability (flexibilityexercises are continued from previous phase). Wrist flexion.Criteria to progress to phase 3 are as follows: patient hasminimal to no pain with all exercises; patient demonstratesnormal motor control without substitution during exercises;and elimination of flexibility deficits in upper and lowerextremities during static and dynamic stretching.
Fig 55. Phase 3: core mobility/power. Dynamic stretching forhamstring and hip mobility. Walk on hands out as far aspossible.
Fig 56. Phase 3: core mobility/power. Then move feet towardhands to feel a stretch in the hamstring.
Fig 57. Phase 3: core mobility/power. Torso rotation andlatissimus stretch.
161.e13 W. B. KIBLER ET AL.
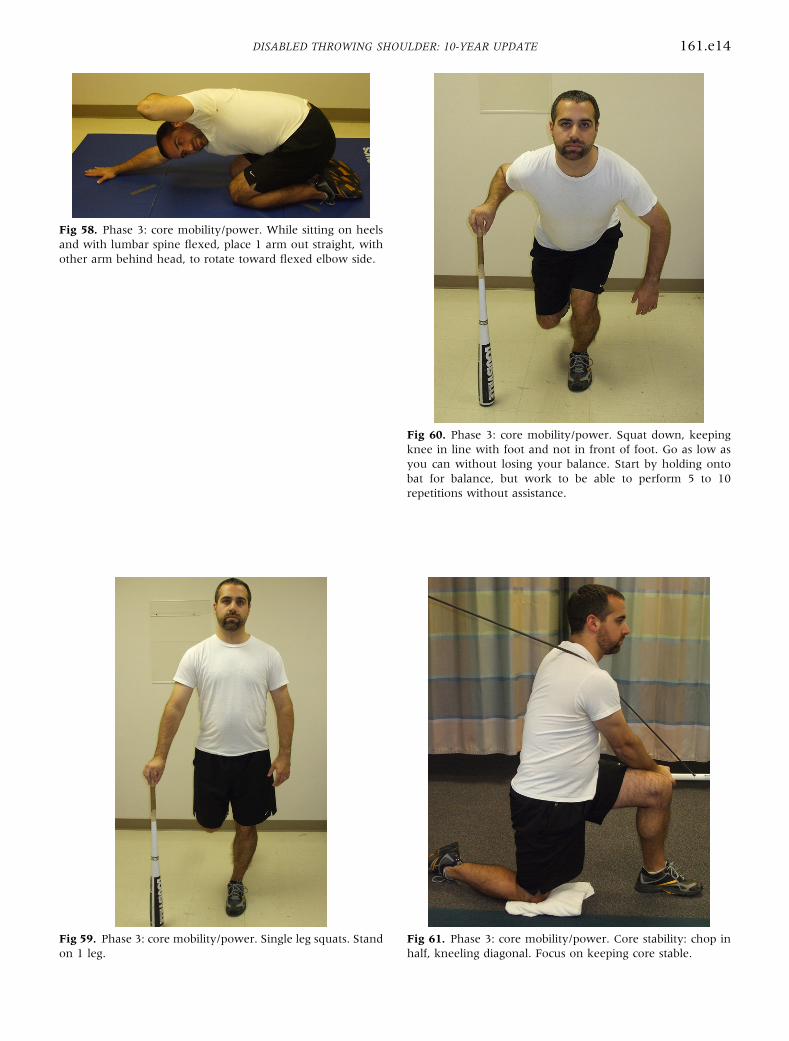
Fig 58. Phase 3: core mobility/power. While sitting on heelsand with lumbar spine flexed, place 1 arm out straight, withother arm behind head, to rotate toward flexed elbow side.
Fig 59. Phase 3: core mobility/power. Single leg squats. Standon 1 leg.
Fig 60. Phase 3: core mobility/power. Squat down, keepingknee in line with foot and not in front of foot. Go as low asyou can without losing your balance. Start by holding ontobat for balance, but work to be able to perform 5 to 10repetitions without assistance.
Fig 61. Phase 3: core mobility/power. Core stability: chop inhalf, kneeling diagonal. Focus on keeping core stable.
DISABLED THROWING SHOULDER: 10-YEAR UPDATE 161.e14
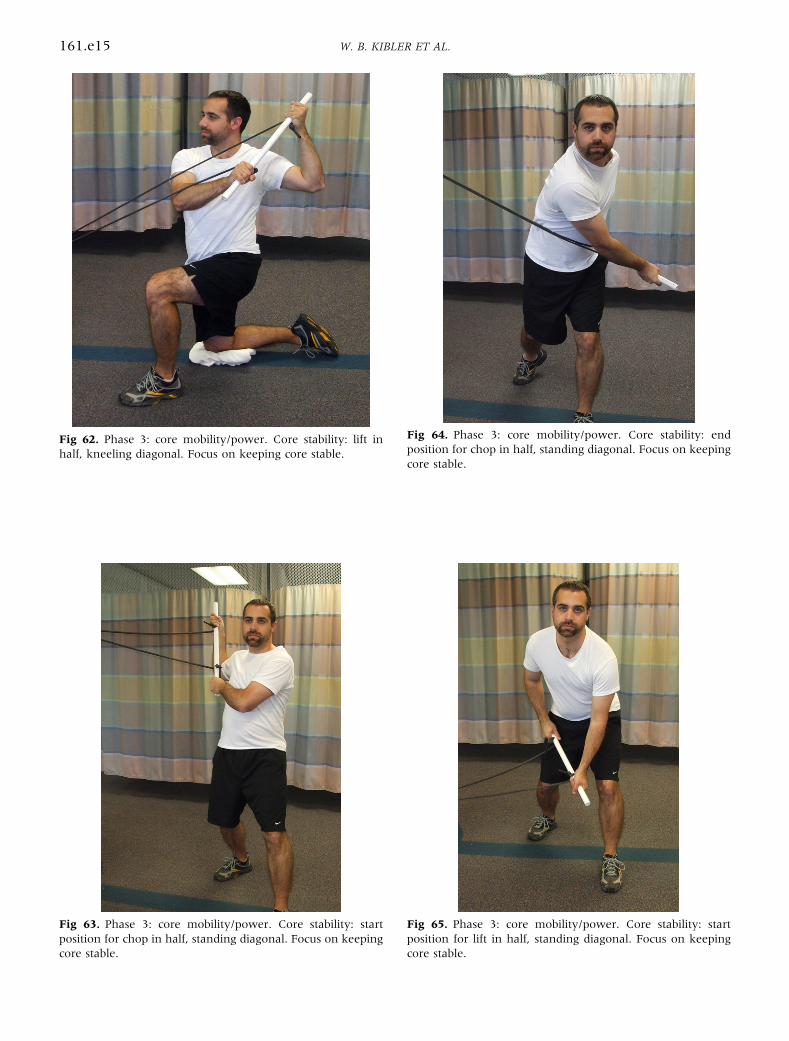
Fig 62. Phase 3: core mobility/power. Core stability: lift inhalf, kneeling diagonal. Focus on keeping core stable.
Fig 63. Phase 3: core mobility/power. Core stability: startposition for chop in half, standing diagonal. Focus on keepingcore stable.
Fig 64. Phase 3: core mobility/power. Core stability: endposition for chop in half, standing diagonal. Focus on keepingcore stable.
Fig 65. Phase 3: core mobility/power. Core stability: startposition for lift in half, standing diagonal. Focus on keepingcore stable.
161.e15 W. B. KIBLER ET AL.
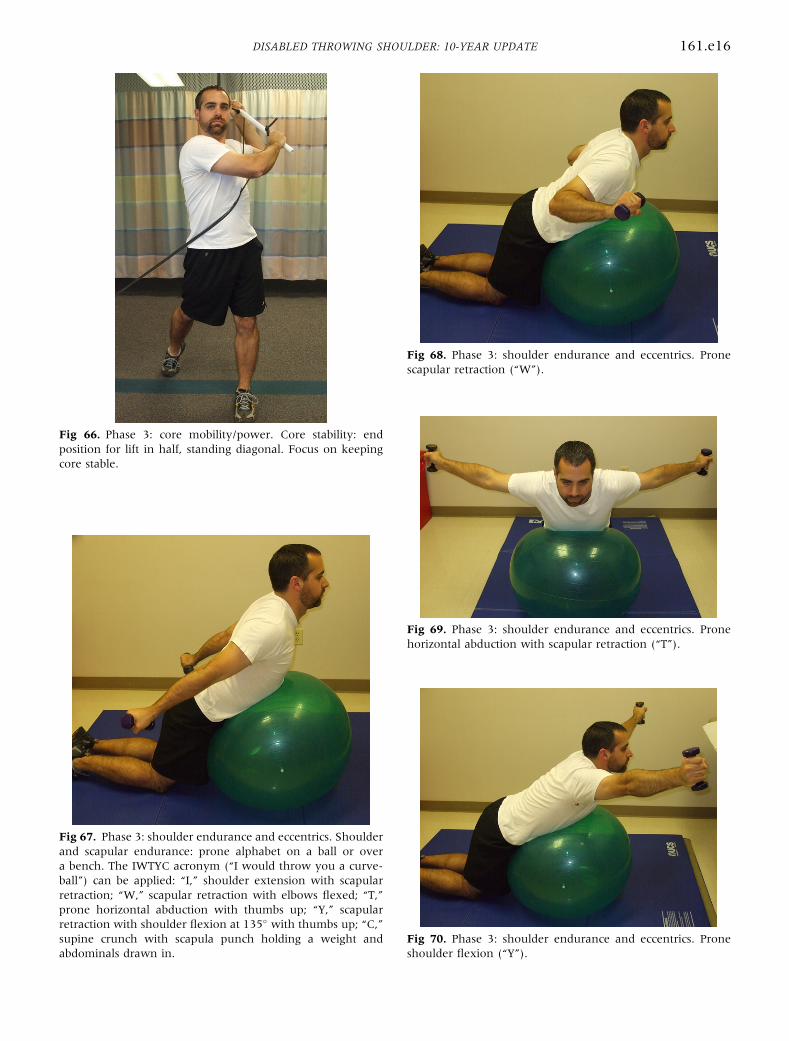
Fig 66. Phase 3: core mobility/power. Core stability: endposition for lift in half, standing diagonal. Focus on keepingcore stable.
Fig 67. Phase 3: shoulder endurance and eccentrics. Shoulderand scapular endurance: prone alphabet on a ball or overa bench. The IWTYC acronym (“I would throw you a curve-ball”) can be applied: “I,” shoulder extension with scapularretraction; “W,” scapular retraction with elbows flexed; “T,”prone horizontal abduction with thumbs up; “Y,” scapularretraction with shoulder flexion at 135� with thumbs up; “C,”supine crunch with scapula punch holding a weight andabdominals drawn in.
Fig 68. Phase 3: shoulder endurance and eccentrics. Pronescapular retraction (“W”).
Fig 69. Phase 3: shoulder endurance and eccentrics. Pronehorizontal abduction with scapular retraction (“T”).
Fig 70. Phase 3: shoulder endurance and eccentrics. Proneshoulder flexion (“Y”).
DISABLED THROWING SHOULDER: 10-YEAR UPDATE 161.e16
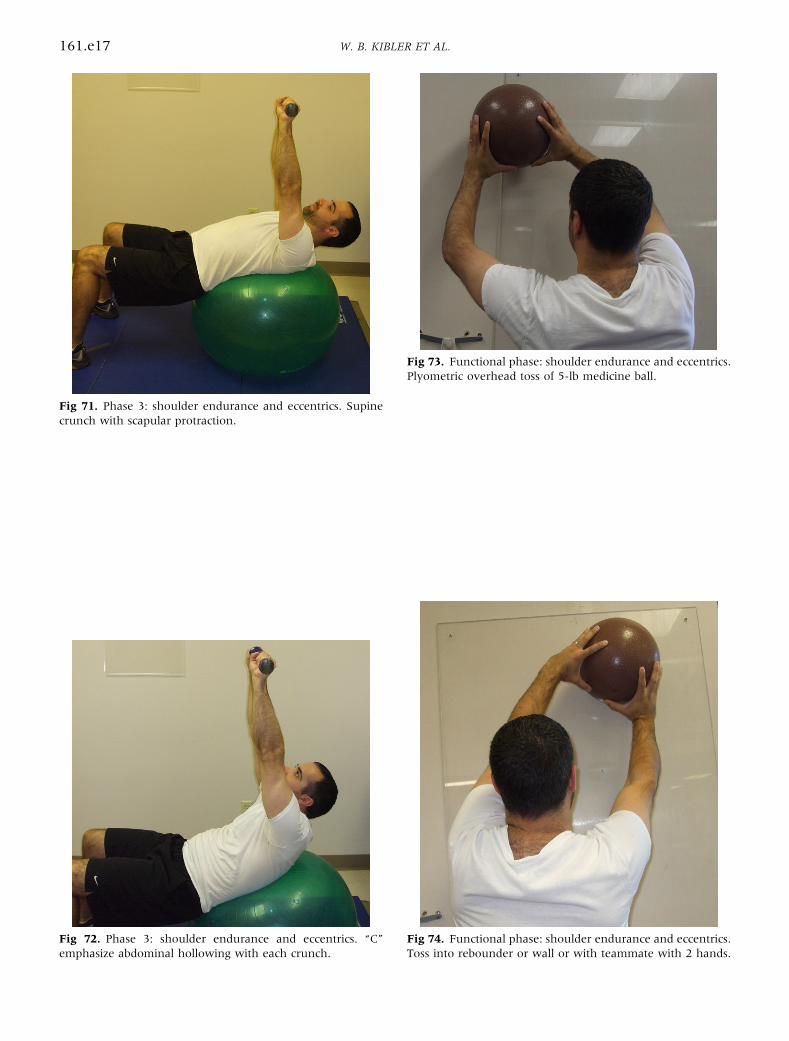
Fig 71. Phase 3: shoulder endurance and eccentrics. Supinecrunch with scapular protraction.
Fig 72. Phase 3: shoulder endurance and eccentrics. “C”emphasize abdominal hollowing with each crunch.
Fig 73. Functional phase: shoulder endurance and eccentrics.Plyometric overhead toss of 5-lb medicine ball.
Fig 74. Functional phase: shoulder endurance and eccentrics.Toss into rebounder or wall or with teammate with 2 hands.
161.e17 W. B. KIBLER ET AL.
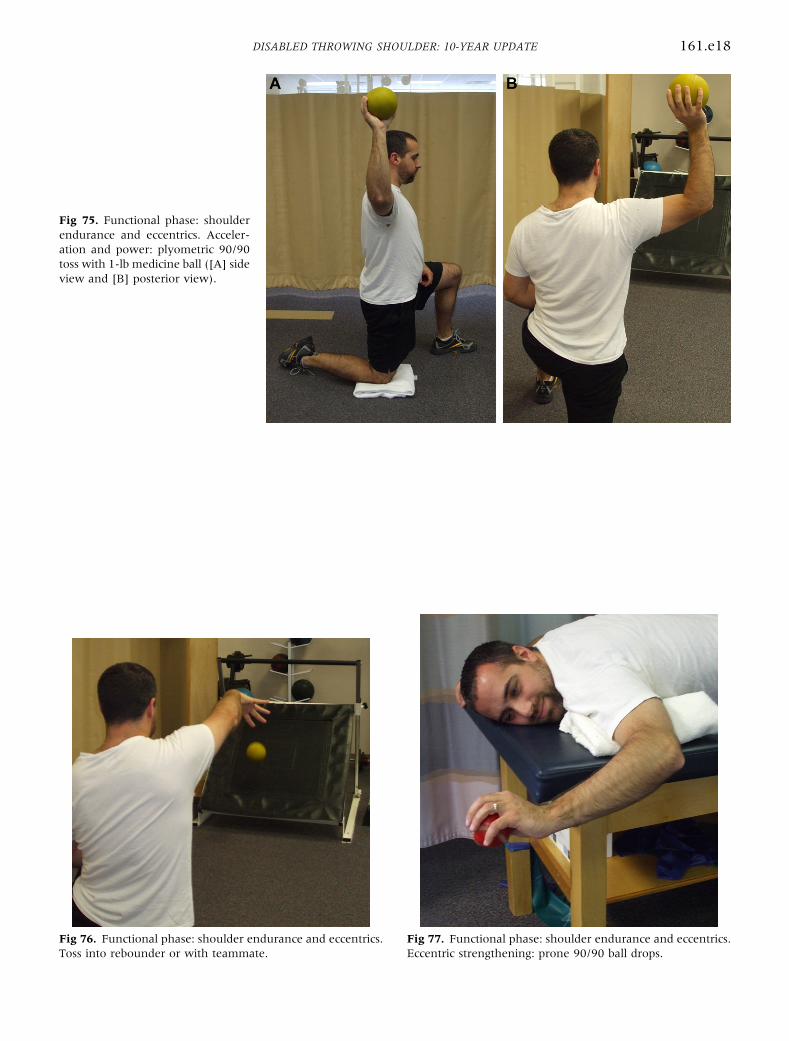
Fig 75. Functional phase: shoulderendurance and eccentrics. Acceler-ation and power: plyometric 90/90toss with 1-lb medicine ball ([A] sideview and [B] posterior view).
Fig 76. Functional phase: shoulder endurance and eccentrics.Toss into rebounder or with teammate.
Fig 77. Functional phase: shoulder endurance and eccentrics.Eccentric strengthening: prone 90/90 ball drops.
DISABLED THROWING SHOULDER: 10-YEAR UPDATE 161.e18
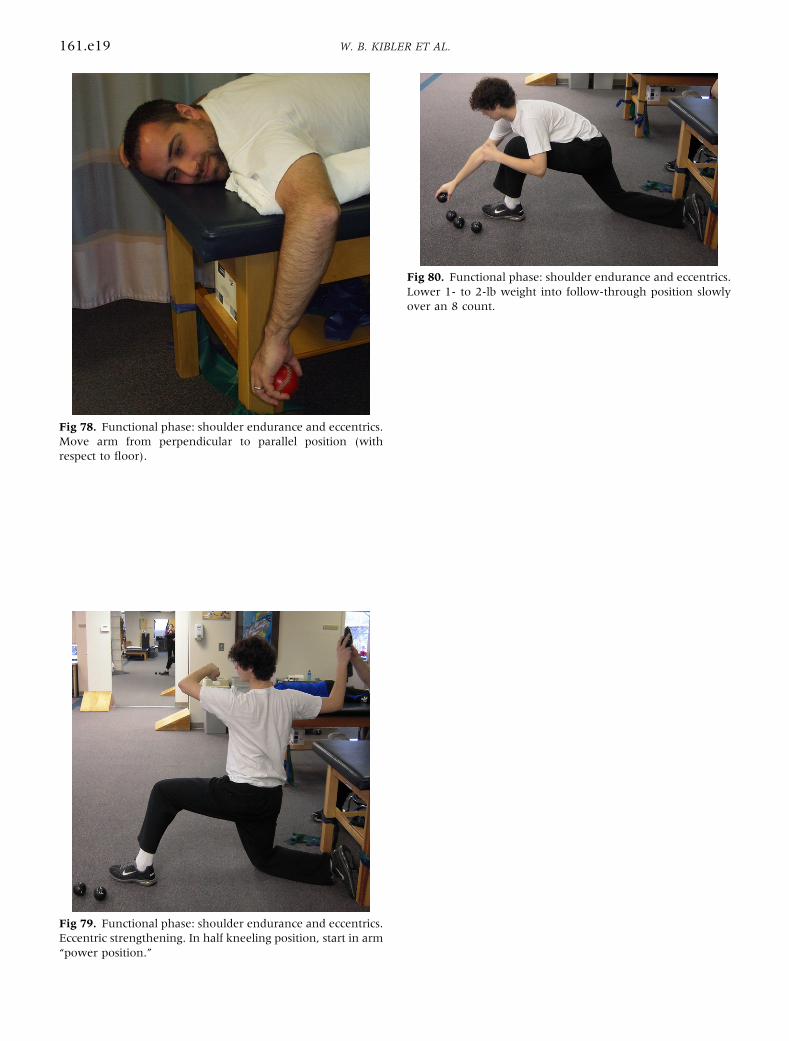
Fig 78. Functional phase: shoulder endurance and eccentrics.Move arm from perpendicular to parallel position (withrespect to floor).
Fig 79. Functional phase: shoulder endurance and eccentrics.Eccentric strengthening. In half kneeling position, start in arm“power position.”
Fig 80. Functional phase: shoulder endurance and eccentrics.Lower 1- to 2-lb weight into follow-through position slowlyover an 8 count.
161.e19 W. B. KIBLER ET AL.
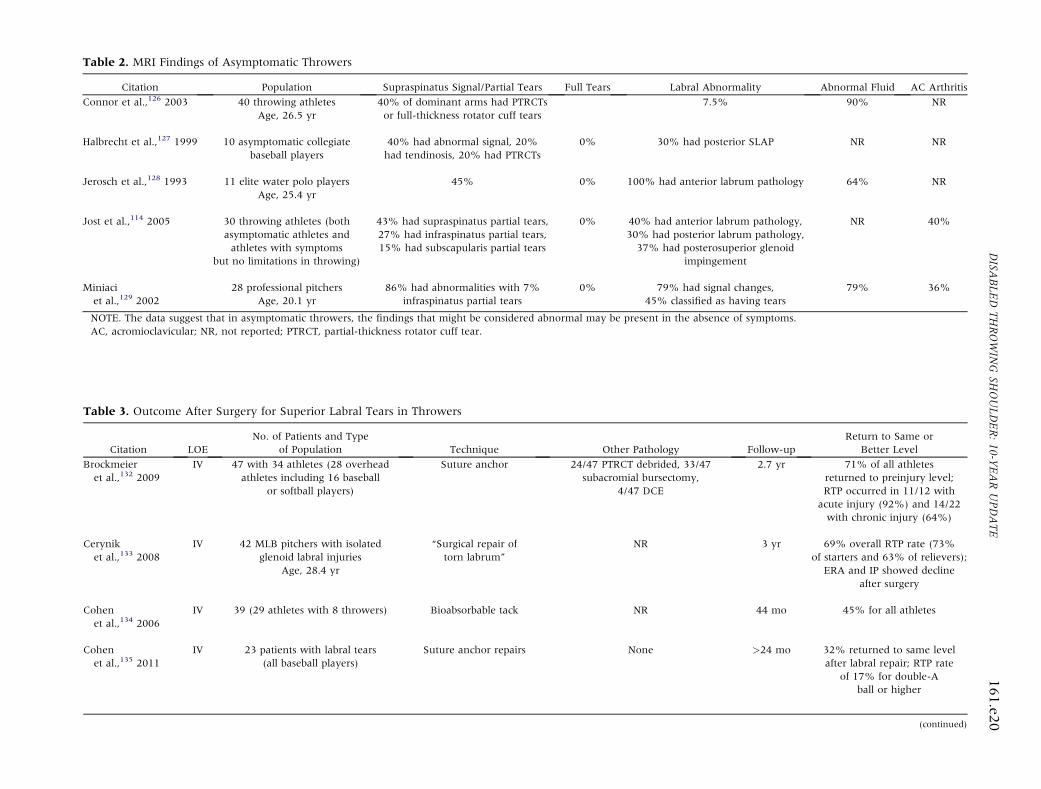
Table 2. MRI Findings of Asymptomatic Throwers
Citation Population Supraspinatus Signal/Partial Tears Full Tears Labral Abnormality Abnormal Fluid AC Arthritis
Connor et al.,126 2003 40 throwing athletesAge, 26.5 yr
40% of dominant arms had PTRCTsor full-thickness rotator cuff tears
7.5% 90% NR
Halbrecht et al.,127 1999 10 asymptomatic collegiatebaseball players
40% had abnormal signal, 20%had tendinosis, 20% had PTRCTs
0% 30% had posterior SLAP NR NR
Jerosch et al.,128 1993 11 elite water polo playersAge, 25.4 yr
45% 0% 100% had anterior labrum pathology 64% NR
Jost et al.,114 2005 30 throwing athletes (bothasymptomatic athletes andathletes with symptoms
but no limitations in throwing)
43% had supraspinatus partial tears,27% had infraspinatus partial tears,15% had subscapularis partial tears
0% 40% had anterior labrum pathology,30% had posterior labrum pathology,37% had posterosuperior glenoid
impingement
NR 40%
Miniaciet al.,129 2002
28 professional pitchersAge, 20.1 yr
86% had abnormalities with 7%infraspinatus partial tears
0% 79% had signal changes,45% classified as having tears
79% 36%
NOTE. The data suggest that in asymptomatic throwers, the findings that might be considered abnormal may be present in the absence of symptoms.AC, acromioclavicular; NR, not reported; PTRCT, partial-thickness rotator cuff tear.
Table 3. Outcome After Surgery for Superior Labral Tears in Throwers
Citation LOENo. of Patients and Type
of Population Technique Other Pathology Follow-upReturn to Same or
Better Level
Brockmeieret al.,132 2009
IV 47 with 34 athletes (28 overheadathletes including 16 baseball
or softball players)
Suture anchor 24/47 PTRCT debrided, 33/47subacromial bursectomy,
4/47 DCE
2.7 yr 71% of all athletesreturned to preinjury level;RTP occurred in 11/12 with
acute injury (92%) and 14/22with chronic injury (64%)
Ceryniket al.,133 2008
IV 42 MLB pitchers with isolatedglenoid labral injuries
Age, 28.4 yr
“Surgical repair oftorn labrum”
NR 3 yr 69% overall RTP rate (73%of starters and 63% of relievers);
ERA and IP showed declineafter surgery
Cohenet al.,134 2006
IV 39 (29 athletes with 8 throwers) Bioabsorbable tack NR 44 mo 45% for all athletes
Cohenet al.,135 2011
IV 23 patients with labral tears(all baseball players)
Suture anchor repairs None >24 mo 32% returned to same levelafter labral repair; RTP rate
of 17% for double-Aball or higher
(continued)
DISA
BLEDTHROWIN
GSH
OULDER:10-Y
EARUPDATE
161.e2
0
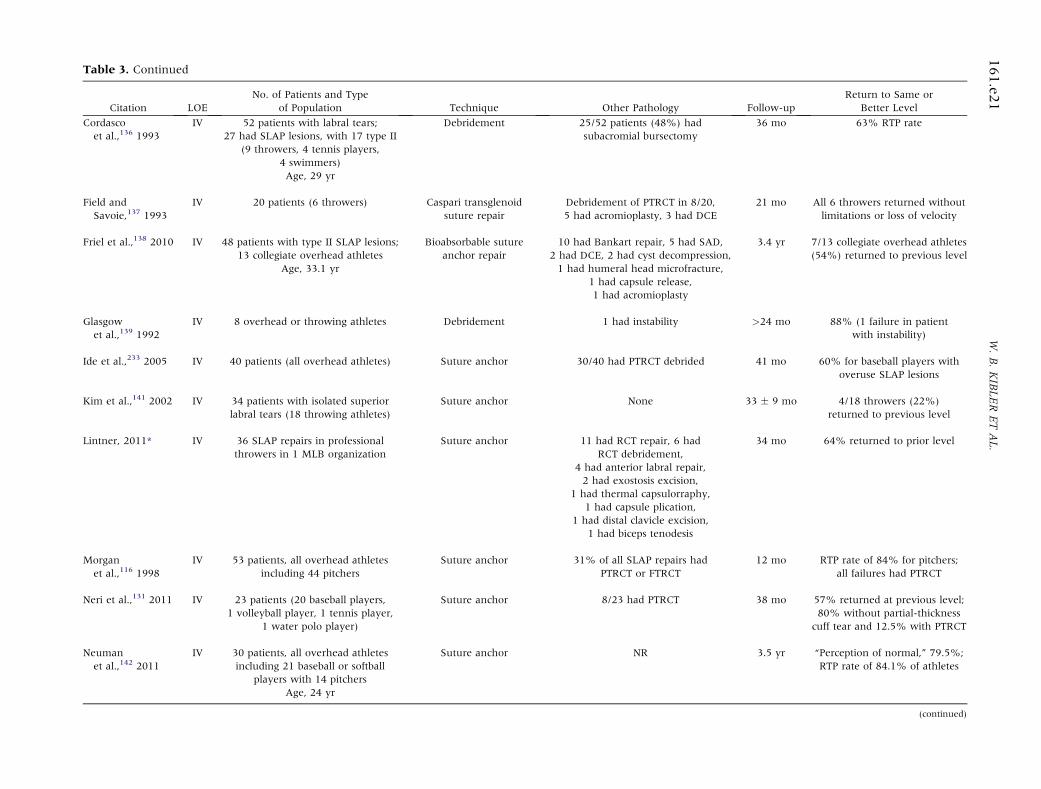
Table 3. Continued
Citation LOENo. of Patients and Type
of Population Technique Other Pathology Follow-upReturn to Same or
Better Level
Cordascoet al.,136 1993
IV 52 patients with labral tears;27 had SLAP lesions, with 17 type II
(9 throwers, 4 tennis players,4 swimmers)Age, 29 yr
Debridement 25/52 patients (48%) hadsubacromial bursectomy
36 mo 63% RTP rate
Field andSavoie,137 1993
IV 20 patients (6 throwers) Caspari transglenoidsuture repair
Debridement of PTRCT in 8/20,5 had acromioplasty, 3 had DCE
21 mo All 6 throwers returned withoutlimitations or loss of velocity
Friel et al.,138 2010 IV 48 patients with type II SLAP lesions;13 collegiate overhead athletes
Age, 33.1 yr
Bioabsorbable sutureanchor repair
10 had Bankart repair, 5 had SAD,2 had DCE, 2 had cyst decompression,1 had humeral head microfracture,
1 had capsule release,1 had acromioplasty
3.4 yr 7/13 collegiate overhead athletes(54%) returned to previous level
Glasgowet al.,139 1992
IV 8 overhead or throwing athletes Debridement 1 had instability >24 mo 88% (1 failure in patientwith instability)
Ide et al.,233 2005 IV 40 patients (all overhead athletes) Suture anchor 30/40 had PTRCT debrided 41 mo 60% for baseball players withoveruse SLAP lesions
Kim et al.,141 2002 IV 34 patients with isolated superiorlabral tears (18 throwing athletes)
Suture anchor None 33 � 9 mo 4/18 throwers (22%)returned to previous level
Lintner, 2011* IV 36 SLAP repairs in professionalthrowers in 1 MLB organization
Suture anchor 11 had RCT repair, 6 hadRCT debridement,
4 had anterior labral repair,2 had exostosis excision,
1 had thermal capsulorraphy,1 had capsule plication,
1 had distal clavicle excision,1 had biceps tenodesis
34 mo 64% returned to prior level
Morganet al.,116 1998
IV 53 patients, all overhead athletesincluding 44 pitchers
Suture anchor 31% of all SLAP repairs hadPTRCT or FTRCT
12 mo RTP rate of 84% for pitchers;all failures had PTRCT
Neri et al.,131 2011 IV 23 patients (20 baseball players,1 volleyball player, 1 tennis player,
1 water polo player)
Suture anchor 8/23 had PTRCT 38 mo 57% returned at previous level;80% without partial-thickness
cuff tear and 12.5% with PTRCT
Neumanet al.,142 2011
IV 30 patients, all overhead athletesincluding 21 baseball or softball
players with 14 pitchersAge, 24 yr
Suture anchor NR 3.5 yr “Perception of normal,” 79.5%;RTP rate of 84.1% of athletes
(continued)
161.e2
1W.B.KIBLERETAL.
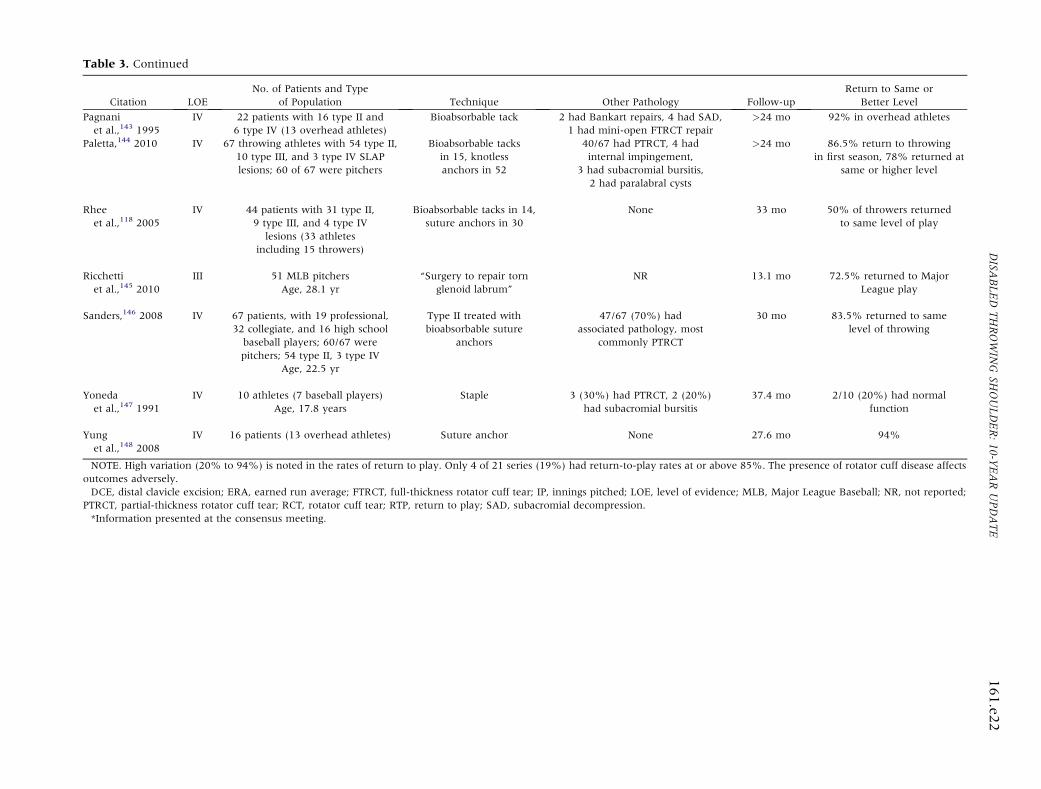
Citation LOENo. of Patients and Type
of Population Technique Other Pathology Follow-upReturn to Same or
Better Level
Pagnaniet al.,143 1995
IV 22 patients with 16 type II and6 type IV (13 overhead athletes)
Bioabsorbable tack 2 had Bankart repairs, 4 had SAD,1 had mini-open FTRCT repair
>24 mo 92% in overhead athletes
Paletta,144 2010 IV 67 throwing athletes with 54 type II,10 type III, and 3 type IV SLAPlesions; 60 of 67 were pitchers
Bioabsorbable tacksin 15, knotlessanchors in 52
40/67 had PTRCT, 4 hadinternal impingement,
3 had subacromial bursitis,2 had paralabral cysts
>24 mo 86.5% return to throwingin first season, 78% returned at
same or higher level
Rheeet al.,118 2005
IV 44 patients with 31 type II,9 type III, and 4 type IV
lesions (33 athletesincluding 15 throwers)
Bioabsorbable tacks in 14,suture anchors in 30
None 33 mo 50% of throwers returnedto same level of play
Ricchettiet al.,145 2010
III 51 MLB pitchersAge, 28.1 yr
“Surgery to repair tornglenoid labrum”
NR 13.1 mo 72.5% returned to MajorLeague play
Sanders,146 2008 IV 67 patients, with 19 professional,32 collegiate, and 16 high school
baseball players; 60/67 werepitchers; 54 type II, 3 type IV
Age, 22.5 yr
Type II treated withbioabsorbable suture
anchors
47/67 (70%) hadassociated pathology, most
commonly PTRCT
30 mo 83.5% returned to samelevel of throwing
Yonedaet al.,147 1991
IV 10 athletes (7 baseball players)Age, 17.8 years
Staple 3 (30%) had PTRCT, 2 (20%)had subacromial bursitis
37.4 mo 2/10 (20%) had normalfunction
Yunget al.,148 2008
IV 16 patients (13 overhead athletes) Suture anchor None 27.6 mo 94%
NOTE. High variation (20% to 94%) is noted in the rates of return to play. Only 4 of 21 series (19%) had return-to-play rates at or above 85%. The presence of rotator cuff disease affectsoutcomes adversely.DCE, distal clavicle excision; ERA, earned run average; FTRCT, full-thickness rotator cuff tear; IP, innings pitched; LOE, level of evidence; MLB, Major League Baseball; NR, not reported;
PTRCT, partial-thickness rotator cuff tear; RCT, rotator cuff tear; RTP, return to play; SAD, subacromial decompression.*Information presented at the consensus meeting.
Table 3. ContinuedDISA
BLEDTHROWIN
GSH
OULDER:10-Y
EARUPDATE
161.e2
2
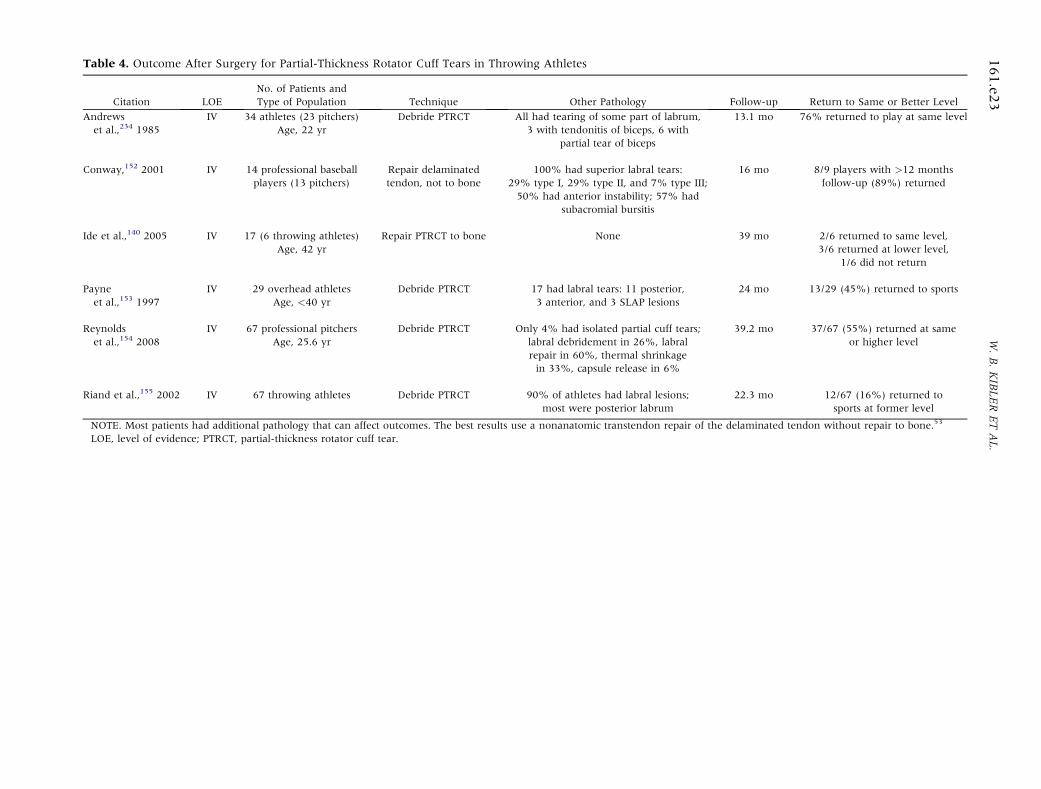
Table 4. Outcome After Surgery for Partial-Thickness Rotator Cuff Tears in Throwing Athletes
Citation LOENo. of Patients andType of Population Technique Other Pathology Follow-up Return to Same or Better Level
Andrewset al.,234 1985
IV 34 athletes (23 pitchers)Age, 22 yr
Debride PTRCT All had tearing of some part of labrum,3 with tendonitis of biceps, 6 with
partial tear of biceps
13.1 mo 76% returned to play at same level
Conway,152 2001 IV 14 professional baseballplayers (13 pitchers)
Repair delaminatedtendon, not to bone
100% had superior labral tears:29% type I, 29% type II, and 7% type III;50% had anterior instability; 57% had
subacromial bursitis
16 mo 8/9 players with >12 monthsfollow-up (89%) returned
Ide et al.,140 2005 IV 17 (6 throwing athletes)Age, 42 yr
Repair PTRCT to bone None 39 mo 2/6 returned to same level,3/6 returned at lower level,
1/6 did not return
Payneet al.,153 1997
IV 29 overhead athletesAge, <40 yr
Debride PTRCT 17 had labral tears: 11 posterior,3 anterior, and 3 SLAP lesions
24 mo 13/29 (45%) returned to sports
Reynoldset al.,154 2008
IV 67 professional pitchersAge, 25.6 yr
Debride PTRCT Only 4% had isolated partial cuff tears;labral debridement in 26%, labralrepair in 60%, thermal shrinkagein 33%, capsule release in 6%
39.2 mo 37/67 (55%) returned at sameor higher level
Riand et al.,155 2002 IV 67 throwing athletes Debride PTRCT 90% of athletes had labral lesions;most were posterior labrum
22.3 mo 12/67 (16%) returned tosports at former level
NOTE. Most patients had additional pathology that can affect outcomes. The best results use a nonanatomic transtendon repair of the delaminated tendon without repair to bone.53
LOE, level of evidence; PTRCT, partial-thickness rotator cuff tear.
161.e2
3W.B.KIBLERETAL.
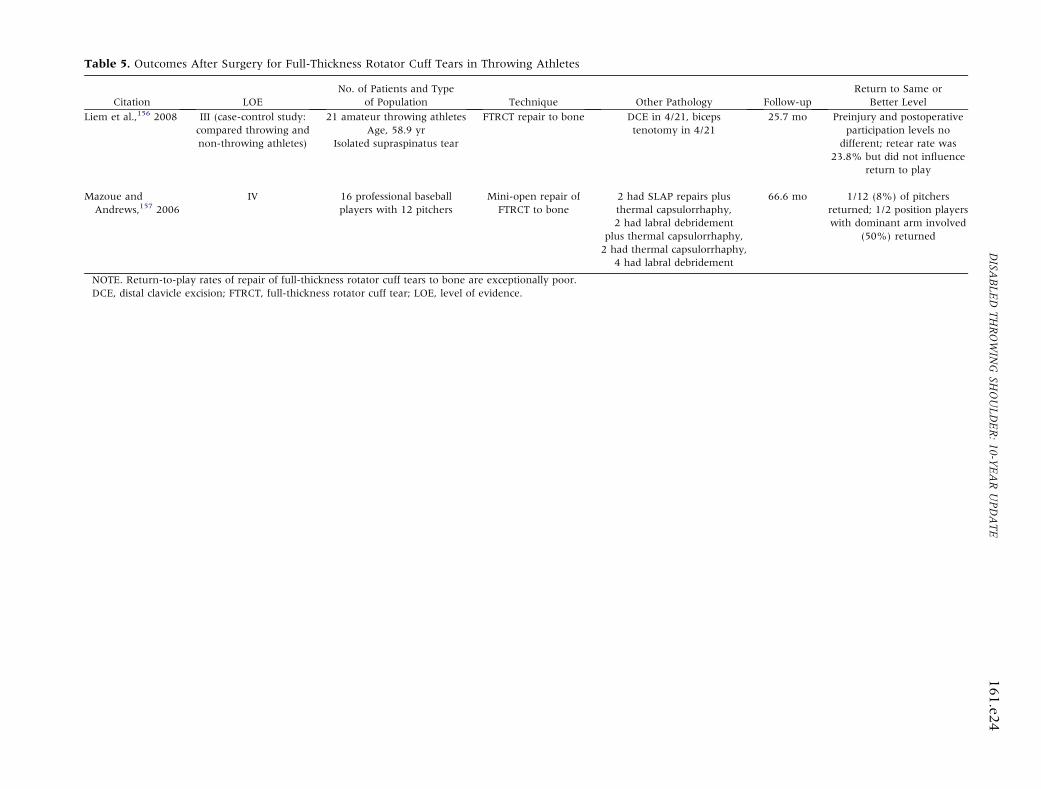
Table 5. Outcomes After Surgery for Full-Thickness Rotator Cuff Tears in Throwing Athletes
Citation LOENo. of Patients and Type
of Population Technique Other Pathology Follow-upReturn to Same or
Better Level
Liem et al.,156 2008 III (case-control study:compared throwing andnon-throwing athletes)
21 amateur throwing athletesAge, 58.9 yr
Isolated supraspinatus tear
FTRCT repair to bone DCE in 4/21, bicepstenotomy in 4/21
25.7 mo Preinjury and postoperativeparticipation levels no
different; retear rate was23.8% but did not influence
return to play
Mazoue andAndrews,157 2006
IV 16 professional baseballplayers with 12 pitchers
Mini-open repair ofFTRCT to bone
2 had SLAP repairs plusthermal capsulorrhaphy,2 had labral debridement
plus thermal capsulorrhaphy,2 had thermal capsulorrhaphy,
4 had labral debridement
66.6 mo 1/12 (8%) of pitchersreturned; 1/2 position playerswith dominant arm involved
(50%) returned
NOTE. Return-to-play rates of repair of full-thickness rotator cuff tears to bone are exceptionally poor.DCE, distal clavicle excision; FTRCT, full-thickness rotator cuff tear; LOE, level of evidence.
DISA
BLEDTHROWIN
GSH
OULDER:10-Y
EARUPDATE
161.e2
4
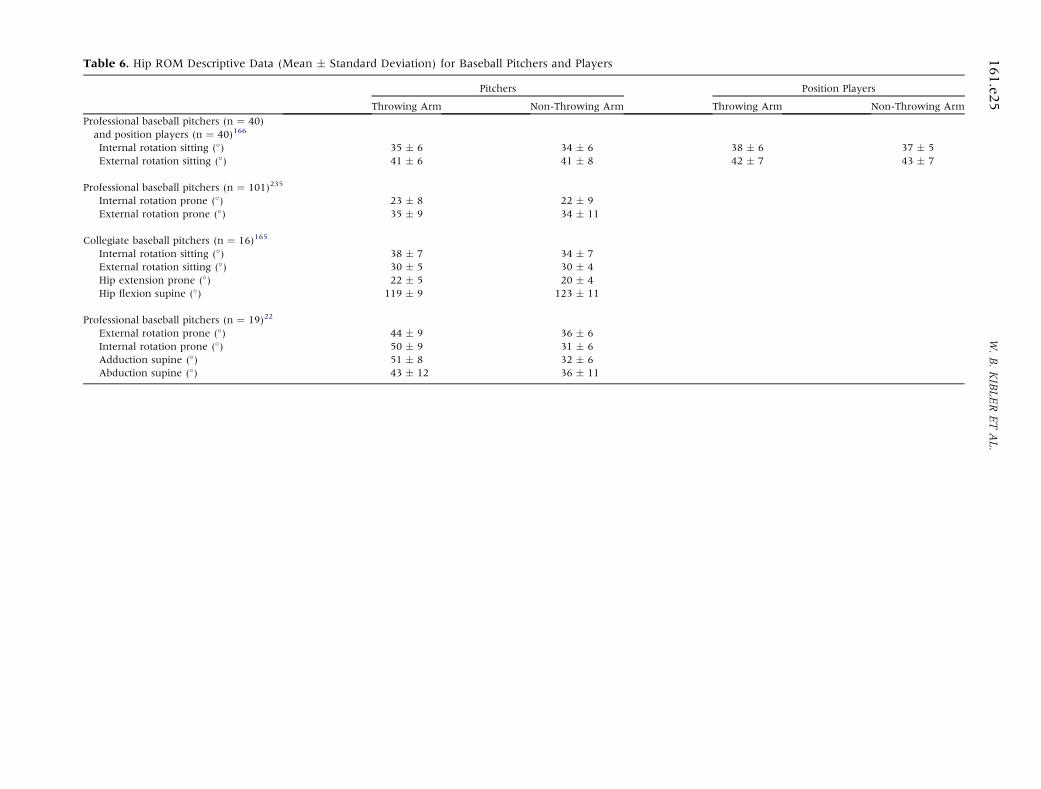
Table 6. Hip ROM Descriptive Data (Mean � Standard Deviation) for Baseball Pitchers and Players
Pitchers Position Players
Throwing Arm Non-Throwing Arm Throwing Arm Non-Throwing Arm
Professional baseball pitchers (n ¼ 40)and position players (n ¼ 40)166
Internal rotation sitting (�) 35 � 6 34 � 6 38 � 6 37 � 5External rotation sitting (�) 41 � 6 41 � 8 42 � 7 43 � 7
Professional baseball pitchers (n ¼ 101)235
Internal rotation prone (�) 23 � 8 22 � 9External rotation prone (�) 35 � 9 34 � 11
Collegiate baseball pitchers (n ¼ 16)165
Internal rotation sitting (�) 38 � 7 34 � 7External rotation sitting (�) 30 � 5 30 � 4Hip extension prone (�) 22 � 5 20 � 4Hip flexion supine (�) 119 � 9 123 � 11
Professional baseball pitchers (n ¼ 19)22
External rotation prone (�) 44 � 9 36 � 6Internal rotation prone (�) 50 � 9 31 � 6Adduction supine (�) 51 � 8 32 � 6Abduction supine (�) 43 � 12 36 � 11
161.e2
5W.B.KIBLERETAL.
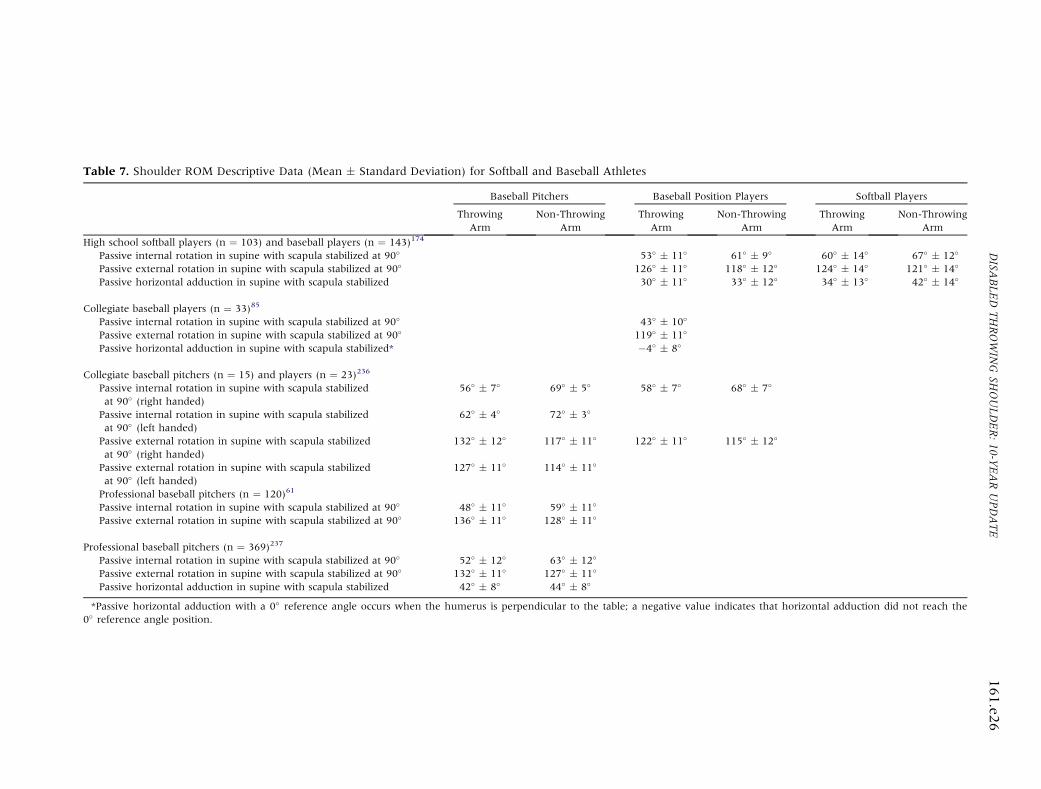
Table 7. Shoulder ROM Descriptive Data (Mean � Standard Deviation) for Softball and Baseball Athletes
Baseball Pitchers Baseball Position Players Softball Players
ThrowingArm
Non-ThrowingArm
ThrowingArm
Non-ThrowingArm
ThrowingArm
Non-ThrowingArm
High school softball players (n ¼ 103) and baseball players (n ¼ 143)174
Passive internal rotation in supine with scapula stabilized at 90� 53� � 11� 61� � 9� 60� � 14� 67� � 12�
Passive external rotation in supine with scapula stabilized at 90� 126� � 11� 118� � 12� 124� � 14� 121� � 14�
Passive horizontal adduction in supine with scapula stabilized 30� � 11� 33� � 12� 34� � 13� 42� � 14�
Collegiate baseball players (n ¼ 33)85
Passive internal rotation in supine with scapula stabilized at 90� 43� � 10�
Passive external rotation in supine with scapula stabilized at 90� 119� � 11�
Passive horizontal adduction in supine with scapula stabilized* �4� � 8�
Collegiate baseball pitchers (n ¼ 15) and players (n ¼ 23)236
Passive internal rotation in supine with scapula stabilizedat 90� (right handed)
56� � 7� 69� � 5� 58� � 7� 68� � 7�
Passive internal rotation in supine with scapula stabilizedat 90� (left handed)
62� � 4� 72� � 3�
Passive external rotation in supine with scapula stabilizedat 90� (right handed)
132� � 12� 117� � 11� 122� � 11� 115� � 12�
Passive external rotation in supine with scapula stabilizedat 90� (left handed)
127� � 11� 114� � 11�
Professional baseball pitchers (n ¼ 120)61
Passive internal rotation in supine with scapula stabilized at 90� 48� � 11� 59� � 11�
Passive external rotation in supine with scapula stabilized at 90� 136� � 11� 128� � 11�
Professional baseball pitchers (n ¼ 369)237
Passive internal rotation in supine with scapula stabilized at 90� 52� � 12� 63� � 12�
Passive external rotation in supine with scapula stabilized at 90� 132� � 11� 127� � 11�
Passive horizontal adduction in supine with scapula stabilized 42� � 8� 44� � 8�
*Passive horizontal adduction with a 0� reference angle occurs when the humerus is perpendicular to the table; a negative value indicates that horizontal adduction did not reach the0� reference angle position.
DISA
BLEDTHROWIN
GSH
OULDER:10-Y
EARUPDATE
161.e2
6