Embed Size (px)
Citation preview

The Dizzy Patient4x4 Method
Dr Ahmad Alamadi FRCS
Consultant, HOD
Al Baraha Hospital

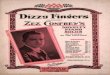
Vestibular Physiology
Orientation of our body in space is the primary function of the vestibular system. This is achieved by integration of signals from vestibular, visual and proprioceptive receptors at the level of brain stem.
Information regarding the movement of the head relative to the body is largely provided by paired vestibular sensory endorgans

Vestibular Sensory Endorgans

Cristae & Otolithic organ

Peripheral Vestibular System
EYES Proprioceptive Receptors
Central Vestibular Nuclei
Vestibulocerebellar tracts (VCT)
Vestibulospinal (VST)
Vestibulo-Ocular reflex (VOR)
Information Relay

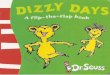
VOR
Keeps a stable retinal image during head movement
As the head moves in one direction there should be an equal and opposite conjugate movement of the eyes (sometime known as the doll’s eye maneuver)

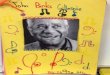
VOR Defect
Bilateral Defect : (for example from systemic aminoglycoside toxicity) the patient will complain of imbalance and a blurring of vision with head movement better known as oscillopsia
Unilateral defect : the equilibrium of the push-pull forces between the inner ears is altered. This result in a drift of the eyes away from side of lesion followed by a quick central nervous system (CNS) mediated saccade in a repetitive to and fro fashion better known as nystagmus.
Nystagmus is the cardinal sign of a central or peripheral vestibular disorder

History Steps
1. Organic Vs Psychogenic
2. Vestibular Vs Non vestibular
3. Peripheral Vs Central
4. Which Peripheral Vestibular Disorder

Organic Vs Psychogenic
Features Organic vestibular Psychogenic
Duration Usually well defined i.e. seconds, minutes or hours
(never a “flash”)
Variable from a “flash” to daysNot well defined
Frequency Except for benign paroxysmal positional vertigo (BPPV), rarely more than once a day
Constant or many times a day
Head Movement Intensifies symptoms Symptoms usually unaffected
Ataxia during spell Usually prominent Insignificant
Effect of Hyperventilation Not like the attack Often reproduces symptoms accurately

Vestibular Vs Non vestibular
True Vertigo (hallucination of movement relative to self) Vs Non specific Dizziness
Note patient with non specific dizziness need to be investigated for cardiac and neurological causes.
Patients with true vertigo have a vestibular disease which can be central or peripheral

Peripheral Vs Central
Ask for associated symptoms i.e. discharge, tinnitus, aural fullness and hearing loss
Ask for focal neurological complaints i.e. diplopia, dysphagia, dysarthria, paresis, parasthesia or incontinence and LOC.
Inner ear disorders should never be associated
with a loss of consciousness

Which Peripheral Vestibular Disorder
Benign paroxysmal positional vertigo (BPPV) seconds; several attacks /day; positional
Meniere's disease minutes to hours; tinnitus; fluctuating hearing loss; aural fullness
Recurrent Vestibulopathy minutes to hours
Vestibular Neuronitis (acute viral labyrinthitis) Hours to days

Examination Steps
1. Otological examination
2. Neurological examination
3. Special clinical vestibular tests
4. Important Diagnostic Tests

Otological examination
Otoscopy
Hearing assessment (Weber and Rinne tests)
Fistula Test

Neurological examination
Cranial Nerves
Cerebellar Tests
Oculomotor Tests Smooth pursuit, saccades, visual fixation and vergence
Balance Tests proprioception, Romberg’s and tandem gait tests (both eyes
open and closed).
When Smooth Pursuit is Normal it would be unlikely for a central disorder to be present

Special clinical vestibular tests
The Halmagyi maneuver
The head shake test
The oscillopsia test
VOR suppression test

Important Diagnostic Tests
Dix-Hallpike Positional Test
Hyperventilation Test

Conclusion
4 steps in History
x = 99% Diagnosis 4 steps in Examination

Soon on DVD and Internet
Interactive Multimedia Textbook of Otologywww.otologytextbook.com
Thank You