Embed Size (px)
Citation preview

THE DYNAMICS OF CROUCH GAIT
IN CEREBRAL PALSY
A DISSERTATION
SUBMITTED TO THE DEPARTMENT OF MECHANICAL ENGINEERING
AND THE COMMITTEE ON GRADUATE STUDIES
OF STANFORD UNIVERSITY
IN PARTIAL FULFILLMENT OF THE REQUIREMENTS
FOR THE DEGREE OF
DOCTOR OF PHILOSOPHY
Katherine Muterspaugh Steele
July 2012

http://creativecommons.org/licenses/by-nc/3.0/us/
This dissertation is online at: http://purl.stanford.edu/ph453mr9252
© 2012 by Katherine Muterspaugh Steele. All Rights Reserved.
Re-distributed by Stanford University under license with the author.
This work is licensed under a Creative Commons Attribution-Noncommercial 3.0 United States License.
ii

I certify that I have read this dissertation and that, in my opinion, it is fully adequatein scope and quality as a dissertation for the degree of Doctor of Philosophy.
Scott Delp, Primary Adviser
I certify that I have read this dissertation and that, in my opinion, it is fully adequatein scope and quality as a dissertation for the degree of Doctor of Philosophy.
Thomas Andriacchi
I certify that I have read this dissertation and that, in my opinion, it is fully adequatein scope and quality as a dissertation for the degree of Doctor of Philosophy.
Jessica Rose
Approved for the Stanford University Committee on Graduate Studies.
Patricia J. Gumport, Vice Provost Graduate Education
This signature page was generated electronically upon submission of this dissertation in electronic format. An original signed hard copy of the signature page is on file inUniversity Archives.
iii

iv

v
ABSTRACT
Individuals with cerebral palsy commonly have gait pathologies that limit their
mobility and hinder activities of daily living. One of the most common gait
pathologies among individuals with cerebral palsy is crouch gait. Individuals who
walk in a crouch gait have excessive hip and knee flexion which makes walking
difficult and metabolically inefficient. If untreated, crouch gait can lead to joint pain,
bone deformities, and a loss of independent mobility. Current treatments for crouch
gait involve orthopaedic surgery and therapy; however, outcomes are inconsistent.
Clinicians need a better understanding of how the complexities of the neuromuscular
and musculoskeletal systems contribute to this pathologic gait pattern. The goal of this
dissertation was to examine the musculoskeletal dynamics of crouch gait in
individuals with cerebral palsy to better understand its biomechanical causes and
improve treatment of individuals with crouch gait.
There are many proposed causes of crouch gait including excessive muscle
activity from contracture or spasticity, muscle weakness, bone deformities, and
impaired voluntary control. To determine which of these factors contribute to crouch
gait requires an understanding of how individual muscles contribute to motion. We
generated the first three-dimensional musculoskeletal simulations of crouch gait to
evaluate how muscles contribute to joint and mass center acceleration. We found that
individuals with crouch gait use the same muscles to support and propel the body as
unimpaired gait. However, larger and more sustained muscle forces are required
during crouch gait.

vi
Many individuals with cerebral palsy and crouch gait also develop knee pain
later in life. Since cartilage growth and maintenance is dependent upon the loads
experienced during daily life, we sought to quanitfy how tibiofemoral forces change
during crouch gait. We determined that the compressive tibiofemoral force increases
quadratically with crouch severity and individuals who walk in a severe crouch gait
experience three times the load experienced during unimpaired gait. Elevated
tibiofemoral forces could compromise cartilage health and lead to knee pain.
Muscle weakness is commonly hypothesized as a cause of crouch gait and
many individuals with crouch gait participate in strength training programs. We
performed a meta-analysis of outcomes after strength training in individuals with
cerebral palsy and crouch gait and found that although muscle strength increases after
strength training, changes in gait kinematics are inconsistent. Some individuals with
crouch gait had significantly more knee extension during gait after strength training;
however, other individuals’ gait deteriorated. We determined that hamstring spasticity
may be a contraindication for strength training among individuals with cerebral palsy
and crouch gait; no individuals with hamstring spasticity had improved knee extension
after strength training.
We also used musculoskeletal simulation to evaluate how much muscle
strength is required to walk in a crouch gait compared to an unimpaired gait. We
found that crouch gait requires more quadriceps strength than unimpaired gait but
requires less hip abductor and ankle plantarflexor strength. These results suggest that
weakness of the hip abductors or ankle plantarflexors may contribute to crouch gait

vii
and strengthening these muscles may lead to more consistent outcomes after strength
training.
This dissertation examines the dynamics of crouch gait among individuals with
cerebral palsy including muscle contributions to motion, changes in joint loads, and
the effects of muscle weakness. This work provides a foundation for using
musculoskeletal modeling and simulation to examine complex gait pathologies and
also suggests exciting future areas of research to improve the care and treatment of
individuals with cerebral palsy and crouch gait.

viii

ix
ACKNOWLEDGEMENTS Over the past five years I have come to appreciate that earning a PhD is a team
effort that requires incredible collaborators and a tight support network. The
community is the best part of Stanford University and many people have helped to
make this dissertation a reality. The acknowledgements that follow only scratch the
surface and I thank the whole Stanford community for their help and encouragement.
First, I need to thank my advisor, Scott Delp and the Neuromuscular
Biomechanics Laboratory (NMBL). Dr. Delp has provided me with an excellent role
model for how to enjoy research and investigate important questions. The community
provided by NMBL has given me a safe place to explore the field of biomechanics,
take risks, and grow as an engineer and researcher. I especially want to thank Ajay
Seth, Ayman Habib, Jennifer Hicks, Melanie Fox, and Matt DeMers for their
invaluable advice, technical support, and collaboration. My day-to-day work would
also not have been the same without Melinda Cromie sitting across from me to bounce
ideas off of, ask questions, and pursue ideas like creating our own course.
Additionally, the lab would not function as smoothly without the constant attention
and support of Carolyn Mazenko – thank you.
I have also been fortunate enough to have an amazing team of collaborators
outside of NMBL. My reading committee members, Jessica Rose and Tom
Andriacchi, have been a continual source of support, critical evaluation, and clinical
insight. The opportunity to work at Lucille Packard Children’s Hospital with Jessica
Rose has provided me with a weekly reminder of the patients we are trying to help. I
would also like to thank Mike Schwartz from Gillette Children’s Specialty Healthcare

x
for not only providing an amazing source of clinical data but, more importantly, for
his insights and lively discussions. I am also thankful to have had the opportunity to
collaborate with Marjolein van der Krogt during her visits to Stanford. Diane Damiano
from the National Institutes of Health has served as a valuable clinical collaborator
and mentor. I hope to continue to work with all of these individuals in the future to
improve the lives of individuals with cerebral palsy.
I must also not forget to acknowledge that research requires money and a
variety of sources have helped to fund this work including an NSF Graduate Research
Fellowship and NIH grants R01-HD33929, R01-HD046814, and U54-GM072970.
Outside of research I have had an incredible community of friends who have
supported me and made the last five years enjoyable. A special thanks to the Barnes
couples, Matt, An, Mai, and our volleyball teams for providing humor and perspective
– the last five years would not have been the same without you. In addition, Sheri
Sheppard, ME Women+, ASEE, and my WISE group have kept me sane and given me
inspiration for the future.
Finally I need to thank my family for their constant love and support. Mom and
Dad, you have always been my anchor and an incredible source of inspiration and
encouragement. Dan, my wonderful husband, I am so happy that we get to share our
journey together as best friends. I also want to thank my extended family including
Kathleen Rand-Burke, the Saponases, the Wilhoits, and the whole Greencrest family
for their support. I love you all and can’t wait to see where our adventures together
lead next.

xi
CONTENTS Abstract ......................................................................................................................... v
Acknowledgements ...................................................................................................... ix
List of Tables .............................................................................................................. xiii
List of Figures ............................................................................................................. xv
1. Introduction .............................................................................................................. 1 1.1 Focus of the Dissertation ................................................................................................................ 3
1.2 Significance .................................................................................................................................... 4
1.3 Thesis Overview ............................................................................................................................. 8
2. Background ............................................................................................................... 9 2.1 Gait & Mobility ............................................................................................................................ 10
2.2 Cerebral Palsy ............................................................................................................................... 14
2.3 Crouch Gait .................................................................................................................................. 15
2.4 Musculoskeletal Simulation .......................................................................................................... 40
3. How do muscles contribute to support and progression during crouch gait? .. 47 Abstract ............................................................................................................................................. 48
3.1 Introduction .................................................................................................................................. 49
3.2 Methods ........................................................................................................................................ 51
3.3 Results .......................................................................................................................................... 55
3.4 Discussion ..................................................................................................................................... 60
4. How do muscle contributions to support and progression change with crouch
severity? ....................................................................................................................... 65 Abstract ............................................................................................................................................. 66
4.1 Introduction .................................................................................................................................. 67
4.2 Methods ........................................................................................................................................ 69
4.3 Results .......................................................................................................................................... 76
4.4 Discussion ..................................................................................................................................... 80
5. How does tibiofemoral contact force change during crouch gait? ..................... 85 Abstract ............................................................................................................................................. 86
5.1 Introduction .................................................................................................................................. 87
5.2 Methods ........................................................................................................................................ 89
5.3 Results .......................................................................................................................................... 95
5.4 Discussion ..................................................................................................................................... 98

xii
6. How much muscle strength is required to walk in a crouch gait? ................... 103 Abstract ...........................................................................................................................................104
6.1 Introduction .................................................................................................................................105
6.2 Methods ......................................................................................................................................107
6.3 Results .........................................................................................................................................113
6.4 Discussion ...................................................................................................................................116
7. What characteristics are associated with positive outcomes after strength
training for crouch gait? .......................................................................................... 123 Abstract ...........................................................................................................................................124
7.1 Introduction .................................................................................................................................125
7.2 Methods ......................................................................................................................................127
7.3 Results .........................................................................................................................................131
7.4 Discussion ...................................................................................................................................136
8. Conclusion ............................................................................................................. 141 8.1 Summary .....................................................................................................................................142
8.2 Future Work ................................................................................................................................143
References ................................................................................................................. 149
Appendix A: Chapter 3 Supplementary Material ................................................. 167 A.1 Effects of constraining EMG on muscle contributions ..............................................................167
A.2 Mass center and joint accelerations from all muscles ................................................................171
Appendix B: Chapter 5 Supplementary Material ................................................. 175 B.1: Calculating joint forces in OpenSim .........................................................................................175

xiii
LIST OF TABLES Table 4.1: Subject characteristics (average ± standard deviation) ............................... 70
Table 5.1: Subject characteristics (average ± standard deviation) ............................... 89
Table 6.1: Subject characteristics (average ± standard deviation) ............................. 107
Table 6.2: Description of muscle groups .................................................................... 113
Table 7.1: Summary of crouch subjects and training programs for all studies .......... 128
Table 7.2: Results of regression analyses for change in knee flexion angle and knee extensor strength ......................................................................................................... 135

xiv

xv
LIST OF FIGURES Figure 2.1: Kinematics during unimpaired gait (average ± one standard deviation, in degrees). ........................................................................................................................ 11
Figure 2.2: Kinetics including joint moments (Nm/kg) and powers (W/kg) during unimpaired gait (average ± one standard deviation). ................................................... 12
Figure 2.3: Average periods when the muscles are active during unimpaired gait from electromyography data collected at Lucille Packard Children’s Hospital. .................. 13
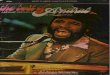
Figure 2.4: Average knee flexion during mild, moderate, and severe crouch gait compared to unimpaired gait and a musculoskeletal model illustrating a typical crouch gait pattern. ................................................................................................................... 16
Figure 2.5: Anatomy of the hamstrings, iliopsoas, and ankle plantarflexors (gastrocnemius and soleus) from the University of Washington Musculoskeletal Atlas. ...................................................................................................................................... 18
Figure 2.6: Meta-analysis of outcomes after hamstring lengthening including change in popliteal angle, change in knee flexion angle, and change in pelvic tilt. ................. 25
Figure 2.7: Map of visitors to the website with the simulations and documentation presented in this dissertation from July 1, 2011 to January 1, 2012 (http://www.simtk.org/home/crouchgait/). ................................................................... 41
Figure 3.1: OpenSim model shown at different phases of single-limb stance during crouch gait. The muscles shown in red are highly activated, while those in blue have a low activation level, as determined using the computed muscle control algorithm. .... 49
Figure 3.2: Comparison of simulated and experimentally-measured joint angles. Average kinematics for pelvis, hip, knee, and ankle are shown for all 10 subjects. The gray line and shaded regions are the experimentally-measured joint angles (± 1 standard deviation) and the black line and dashed-lines are the kinematics reproduced by the simulation (± 1 standard deviation). The simulated kinematics are not provided during double support as only single-limb stance was simulated. The simulated kinematics were within 1º of experimental kinematics (RMS error) for all trials. ...... 55
Figure 3.3: Comparison of the simulated and experimentally-measured hip, knee, and ankle moments for all 10 subjects. The gray line and shaded regions are the experimentally-measured joint moments (± 1 standard deviation) and the blue line and dashed-lines are the moments calculated by computed by multiplying the estimated muscle forces and moment arms (± 1 standard deviation). Joint moments are only shown during single-limb stance and swing since force plate data was not available during double support. .................................................................................................. 56

xvi
Figure 3.4: Comparison of EMG and simulated activation. The EMG signal and activation were normalized to a range of 0 to 1 between the maximum and minimum values for each subject. The gray line and shaded area represents the EMG data (± 1 standard deviation) over a full gait cycle, while the simulated activations during single-limb stance are shown in blue with the dashed lines showing ± 1 standard deviation. Note that estimated muscle activations are not provided during the double support periods of the gait cycle because only single-limb stance was simulated. ...... 57
Figure 3.5: Average contributions ± 1 standard deviation to hip, knee, and ankle angular accelerations during single-limb stance from the major muscle groups of the stance limb. Positive and negative accelerations correspond to extension and flexion, respectively. Note that the muscles with average values close to zero made small contributions throughout single-limb stance. ............................................................... 58
Figure 3.6: Contributions to mass center accelerations from the muscles providing the largest magnitude accelerations upward and downward and from gravity. Accelerations are shown for single-limb stance from opposite toe-off (OTO) to opposite heel contact (OHC). The vectors represent the average up/down and forward/backward acceleration of the mass center at each 5% of single-limb stance for all subjects. The magnitude of the accelerations in the forward/backward directions has the same scale as the up/down accelerations shown on the vertical-axis. Skeletal alignment was calculated by subtracting the accelerations due to muscles from the accelerations due to the ground reaction force. ............................................................ 59
Figure 4.1: Musculoskeletal model of an individual with cerebral palsy and crouch gait. Vertical and fore-aft accelerations of the mass center were calculated by analyzing muscle-driven simulations. .......................................................................... 69
Figure 4.2: Average hip, knee, and ankle flexion angles and moments during unimpaired gait and mild, moderate, and severe crouch gait. The joint moments are normalized by body mass (kg). .................................................................................... 72
Figure 4.3: Average ± 1 standard deviation of the EMG signal of each group (gray) and estimated muscle activations for each subject (black lines) from the quadriceps, hamstrings, gastrocnemius, and anterior tibialis during unimpaired gait and mild, moderate, and severe crouch gait. Only one individual with moderate crouch gait had EMG, thus we took the average of multiple gait cycles for comparison to the group. The magnitude of the EMG and activations were normalized from 0 to 1 based upon the minimum and maximum values during the gait cycle. ........................................... 75
Figure 4.4: The average (A) fore-aft and (B) vertical accelerations of the mass center during stance produced by each muscle and (C) the average muscle force during stance normalized by body weight (BW). Error bars are ± 1 standard error. A ‘*’ indicates a significant difference (p < 0.05) in the student’s t-test comparing unimpaired gait and crouch gait. An arrow indicates a significant change with crouch

xvii
severity (p < 0.05) from a one-way ANOVA comparing mild, moderate, and severe crouch gait. ................................................................................................................... 76
Figure 4.5: The average (A) fore-aft and (B) vertical accelerations produced per 1 newton of muscle force during stance of each muscle. Error bars are ± 1 standard error. A ‘*’ indicates a significant difference (p < 0.05) in the student’s t-test comparing unimpaired gait and crouch gait. An arrow indicates a significant change with crouch severity (p < 0.05) from a one-way ANOVA comparing mild, moderate, and severe crouch gait. ................................................................................................. 78
Figure 4.6: The fore-aft accelerations of the mass center produced by the vasti (gray line) and gastrocnemius (black line) during stance. The gray area shows the experimentally measured acceleration of the mass center (fore-aft ground reaction force normalized by body mass). .................................................................................. 79
Figure 5.1: Tibiofemoral contact forces expressed in multiples of body weight (BW) from experimental forces measured using an instrumented total knee replacement (TKR, gray) and estimated with the computer model (black). The average ± 1 standard deviation is shown from four trials. .............................................................................. 93
Figure 5.2: Comparison of EMG (gray, average ± one standard deviation over all gait cycles) and muscle activations from static optimization (black line) for the six subjects with crouch gait for whom EMG data was available. EMG and activations were normalized from zero to one for each subject based upon the minimum and maximum values over the gait cycle. Note that subject “Severe 1” did not have EMG data from the gastrocnemius. ........................................................................................................ 94
Figure 5.3: (A) Average knee flexion angle, (B) average compressive tibiofemoral force, and (C) average quadriceps force expressed as multiples of body weight (BW) during one gait cycle for the subjects who walked with an unimpaired gait and mild, moderate, and severe crouch gait. ................................................................................ 96
Figure 5.4: Correlation of average knee flexion angle during stance with average compressive tibiofemoral force during stance (black circles), average quadriceps force during stance (dark gray squares), average hamstrings force during stance (light gray triangles), and average gastrocnemius force during stance (black outlined diamonds). Tibiofemoral force and average quadriceps force are expressed as multiples of body weight (BW). A quadratic relationship described the change in both tibiofemoral force and quadriceps force with increasing crouch. .............................................................. 97
Figure 5.5: Average (A) tibiofemoral contact force, (B) quadriceps force, (C) hamstring force, and (D) gastrocnemius force during stance with the objective function shown in Eqn. 1 and weighting constants, minimizing activation with weighting constants, minimizing activation cubed with weighting constants, and minimizing activation squared with all weighting constants equal to one. ................ 101

xviii
Figure 6.1: Musculoskeletal models used to create dynamic simulations of gait for individuals that walked in an unimpaired gait pattern (left) and individuals with cerebral palsy who walked in mild (center) and moderate (right) crouch gait. .......... 109
Figure 6.2: The average hip, knee, and ankle (A) kinematics and (B) kinetics during unimpaired gait (dotted) and mild (light gray) and moderate (dark gray) crouch gait. Joint moments are normalized by body mass (kg). .................................................... 110
Figure 6.3: Comparison of the required strength for each muscle group of the unimpaired subjects (N=3) when using torso markers for inverse kinematics and without torso markers (average ± 1 standard error).. ................................................. 111
Figure 6.4: Required strength for each muscle group that was necessary to recreate each subject’s gait pattern expressed as percent of the maximum isometric force (average ± 1 standard deviation, * p < 0.05 from Fisher’s Least Significant Difference test). ............................................................................................................................ 114
Figure 6.5: Compensatory muscle action when a particular muscle group is weakened, expressed as the average change in muscle force over the gait cycle (times body weight, BW). For each muscle group, the change in force of the weakened muscle group and the change in force of the three muscles with the greatest change in force are shown (average ± 1 standard error). ..................................................................... 115
Figure 6.6: Average (A) kinematics and (B) kinetics for hip abduction and ankle plantarflexion for unimpaired children (N=82, dotted black) and individuals with cerebral palsy who walked in mild (N = 976, light gray) and moderate (N=209, dark gray) crouch gait who visited Gillette Children’s Specialty Healthcare. The peak hip abductor moment and ankle plantarflexor moment are smaller during mild and moderate crouch gait compared to unimpaired gait (ANOVA, p < 0.001). Joint moments are normalized by body mass (kg). ............................................................. 120
Figure 7.1: Summary of literature review and study selection. .................................. 128
Figure 7.2: Histograms of (A) percent change in knee extensor strength and (B) change in minimum knee flexion angle during gait after completing a strength training program. Subjects from each of the three studies are shown separately – Damiano (white), Eek (gray), and Unger (black). ..................................................................... 132
Figure 7.3: Average hip, knee, and ankle flexion angles for (A) all subjects, (B) the three subjects with the largest increase in knee extension (best outcomes), and (C) the three subjects with the largest increase in knee flexion (worst outcomes) before and after completing strength training program. Note that although there was no significant change in knee flexion for the group as a whole, there were subsets of subjects with significant positive and negative changes. ................................................................. 133
Figure 7.4: (A) Hamstring spasticity and (B) walking speed were associated with change in minimum knee flexion angle (KFA) during stance. .................................. 135

1
CHAPTER 1
INTRODUCTION

2
Walking provides an efficient way to explore and interact with the world;
however, it requires precise coordination of the neuromuscular and musculoskeletal
systems. If this coordination is impaired, an individual’s mobility and quality of life
can be compromised. When problems with movement arise, identifying the cause and
appropriate treatments is challenging.
Individuals with cerebral palsy represent a large population of individuals with
mobility problems. According to the United Cerebral Palsy Foundation, in the United
States alone nearly 800,000 individuals have cerebral palsy. Cerebral palsy is caused
by an injury to the brain that affects coordination and movement. Treatments to
improve mobility typically involve a combination of orthopaedic surgery and physical
therapy; however, outcomes from treatment are inconsistent and often unsatisfactory.
A recent study reported that only 48% of individuals with cerebral palsy had
significant improvements in gait following multi-level orthopaedic surgery (Hicks et
al., 2011).
The complexity of the neuromuscular and musculoskeletal systems hinders our
ability to effectively treat gait pathologies in individuals with cerebral palsy.
Identifying the causes and appropriate treatments for each individual is challenging.
Clinicians need a better understanding of the underlying mechanisms that contribute to
gait pathologies to design optimal treatment strategies. For example, many
orthopaedic surgeries target individual muscles; however, how individual muscles
contribute to motion during pathologic gait is not well understood. Clarifying these
contributions would empower clinicians and researchers to improve treatment.

3
Musculoskeletal modeling and simulation provides a powerful tool for
understanding the complexities of human movement and performing studies that
cannot be done experimentally. The Neuromuscular Biomechanics Laboratory at
Stanford University under the guidance of Scott Delp and researchers at other
institutions have helped to develop a freely-available software package, OpenSim, that
allows researchers and clinicians to study the musculoskeletal system. Using a
combination of experimental data and computational methods we can examine the
dynamics of human movement, including pathologic gait patterns in individuals with
cerebral palsy.
This dissertation harnesses musculoskeletal modeling and simulation to
improve our understanding of the dynamics of one of the most common gait
pathologies among individuals with cerebral palsy, crouch gait. Crouch gait,
characterized by excessive hip and knee flexion, is an inefficient gait pattern which, if
left untreated, can lead to joint pain, the formation of bone deformities, and an
inability to walk independently. Using musculoskeletal modeling and simulation, we
can examine the contributions of individual muscles, estimate joint loads, and explore
clinical hypotheses to improve our understanding and ability to treat crouch gait.
1.1 FOCUS OF THE DISSERTATION
The goal of this dissertation was to examine the dynamics of crouch gait in
individuals with cerebral palsy. We created three-dimensional musculoskeletal
simulations of gait that allowed us to probe how individual muscles give rise to

4
motion of the musculoskeletal system. We sought to understand important dynamic
factors that occur during crouch gait, including how muscles accelerate the body, how
joint loads change with crouch severity, and how muscle weakness can affect gait. We
found that crouch gait uses similar muscles to accelerate the body as unimpaired gait,
but requires larger and more sustained muscle forces to support the body - which
contributes to the inefficiency of this gait pattern. The larger muscle forces required to
support the body also contribute to increased joint loads. We determined that the
compressive tibiofemoral force increases quadratically with crouch severity (i.e., knee
flexion during stance) and individuals with severe crouch gait experience three-times
the tibiofemoral force compared to those with unimpaired gait. Muscle weakness may
also be an important contributor to crouch gait and we identified that weakness of
some muscle groups, such as the quadriceps, are not likely contributors to crouch gait,
while other muscle groups, such as the hip abductors and ankle plantarflexors, may
contribute to crouch gait. These analyses provide a foundation to understand the
mechanics of pathologic gait patterns and to guide the development of innovative
treatment strategies.
1.2 SIGNIFICANCE
The research questions addressed in this dissertation make important
contributions to both the biomechanics and clinical communities. Understanding the
dynamics of the musculoskeletal system can guide treatment planning and illuminate
the causes of pathological gait patterns; however, this endeavor requires sophisticated

5
tools to accurately examine the musculoskeletal system. This dissertation sought to
address important clinical problems while also establishing and sharing the tools
required. The primary contributions of the research presented in this dissertation are:
• Creating the first three-dimensional musculoskeletal simulations of
individuals with cerebral palsy. We developed the framework and processes
to create and critically analyze simulations of gait for individuals with cerebral
palsy and crouch gait. Previous studies have used musculoskeletal simulations
to examine unimpaired gait and we extended these methods to examine
important research questions for individuals with pathologic gait. These
simulations have also been made available to other researchers and clinicians
at: http://www.simtk.org/home/crouchgait/.
• Identifying the primary muscles that support and propel the body during
crouch gait. Walking requires a complex orchestration of muscle activity to
efficiently move the body from one point to another. We sought to identify
how muscle contributions to mass center acceleration change during crouch
gait. By creating musculoskeletal simulations of gait we were able to identify
that crouch gait uses similar muscle groups to support and propel the body as
unimpaired gait; however, crouch gait requires more sustained contributions
from muscles to support the body. Crouch gait also requires less gluteus
medius force to accelerate the mass center upward and greater ankle
plantarflexor force to accelerate the mass center forward.
• Quantifying the change in tibiofemoral contact force during crouch gait.
Knee pain is common among individuals with cerebral palsy; however, the

6
cause of the pain and appropriate treatments are not well understood. Increased
knee loading could compromise cartilage health and lead to knee pain. We
used musculoskeletal modeling to quantify changes in tibiofemoral force
during mild, moderate, and severe crouch gait. The magnitude of the
compressive tibiofemoral force increased quadratically with increasing crouch
severity; individuals with a severe crouch gait experienced peak loads up to six
times body weight as compared to two times body weight during unimpaired
gait.
• Examining how muscle weakness can lead to crouch gait. Muscle weakness
is commonly hypothesized as a contributor to crouch gait and is used to justify
strength training programs. However, an understanding of the mechanisms by
which muscle weakness contributes to crouch gait has not been previously
explored. Therefore, we used musculoskeletal modeling and simulation to
examine the amount of muscle strength required to walk in mild, moderate,
and severe crouch gait compared to unimpaired gait. The results of this
analysis showed that the amount of quadriceps strength required increased
quadratically with increasing crouch severity, suggesting that quadriceps
weakness does not contribute to crouch gait. However, crouch gait required
less hip abductor and ankle plantarflexor strength than unimpaired gait,
suggesting that crouch gait could be a compensatory gait pattern for weakness
of these muscle groups.
• Reviewing outcomes after strength training in individuals with crouch
gait. Over the past two decades strength training has become a popular

7
treatment strategy for individuals with cerebral palsy; however, reported
changes in muscle strength and gait after strength training are inconsistent
(Damiano et al., 2010). Previous studies included individuals with cerebral
palsy with many different gait pathologies which hindered interpretation of
their outcomes. Therefore, to examine the effects of strength training on
individuals with crouch gait, we performed a literature review, requested data
from the authors, and performed a meta-analysis of outcomes after strength
training. The results of this meta-analysis indicated that although individuals
with cerebral palsy and crouch gait were stronger after strength training,
changes in gait were inconsistent. Some subjects’ gait improved to within
normal limits after strength training while other subjects’ gait deteriorated.
• Determining that hamstring spasticity is associated with negative
outcomes after strength training in individuals with crouch gait. To
explore the subject-specific factors that could lead to inconsistent outcomes
after strength training in individuals with crouch gait, we performed regression
analyses with ten physical exam and gait characteristics that we hypothesized
could be associated with outcomes after strength training. The results of these
regression analyses identified that hamstring spasticity was associated with
negative outcomes after strength training; none of the subjects with hamstring
spasticity had improved knee extension during gait after strength training.

8
1.3 THESIS OVERVIEW
This dissertation is focused around five research studies that are presented as
self-contained journal articles. After this general introduction, Chapter 2 outlines the
background material related to gait, cerebral palsy, and musculoskeletal simulation
that is useful for interpreting the following chapters. Chapter 3 examines how muscles
contribute to joint and mass center accelerations during stance in mild crouch gait
(Steele et al., 2010, published in Journal of Biomechanics). Chapter 4 extends this
study to examine how muscle contributions to support and propulsion change with
crouch severity (manuscript in review). Chapter 5 quantifies tibiofemoral contact
forces during crouch gait (Steele et al., 2012, published in Gait & Posture). Chapter 6
explores the mechanisms by which muscle weakness could contribute to crouch gait
(manuscript in review). Chapter 7 examines changes in muscle strength and gait after
strength training in individuals with cerebral palsy and crouch gait (Steele et al., 2012,
published in Journal of Pediatric Rehabilitation Medicine). The final chapter of this
dissertation summarizes the important findings of these studies and outlines areas for
future research. The pronoun “we” is used throughout this dissertation to recognize
that research is a team process that requires input and collaboration from multi-
disciplinary teams. The individuals who contributed to these studies are listed at the
beginning of each chapter.

9
CHAPTER 2
BACKGROUND

10
2.1 GAIT & MOBILITY
Walking gives us the freedom to interact with the world and complete the
activities of daily living essential for both work and leisure. The average adult in the
United States takes approximately 6000 to 7000 steps per day (Tudor-Locke et al.,
2004). Beyond enabling mobility, walking has a direct and positive influence on
public health, with demonstrated benefits that include the lowering of rates of chronic
health problems, such as obesity and cardiovascular disease, and reducing medical
expenditures (Lee and Buchner, 2008).
Walking is a cyclic movement that can be accurately and consistently
described by kinematics (joint angles), kinetics (ground reaction forces and moments),
and muscle activity (electromyography). Motion analysis provides a tool to quantify
joint angles and moments during walking and can be used to analyze pathologic gait
patterns. During unimpaired gait, the gait cycle is divided into two primary phases:
stance, when the foot is on the ground (0-60% of the gait cycle), and swing, when the
foot is off the ground (60-100% of the gait cycle). The gait cycle begins with stance at
initial contact or heel strike (see Figure 2.1 for kinematics). At this point in the gait
cycle, the hip is flexed, the knee is near full extension and the ankle is near neutral. In
early stance, the ankle plantarflexes until the foot is in contact with the ground and the
knee flexes slightly. The mass center moves over the stance limb and the hip extends
during stance. The opposite foot contacts the ground at around 40-50% of the gait
cycle. In terminal stance, the ankle plantarflexes to propel the body forward and the
hip and knee flex until the foot is no longer in contact with the ground (at about 60%
of the gait cycle). During swing, the ankle dorsiflexes to clear the ground and the hip

11
flexes to advance the limb for the next step. The knee flexes during the first half of
swing and then extends to near full extension in the second half of swing to prepare
for the next gait cycle.
The magnitude and direction of the force exerted by the foot on the ground,
commonly termed the ground reaction force, can be measured using force plates and is
useful for calculating the moments at each joint. Joint moments describe the net
Figure 2.1: Kinematics during unimpaired gait (average ± one standard deviation, in degrees).

12
moments that are produced by muscles or other passive structures across a joint.
During unimpaired gait, there is a hip extension and hip adduction moment during
stance, a relatively small knee moment that fluctuates between flexion and extension,
and an ankle dorsiflexion moment that increases throughout stance and peaks in
terminal stance (Figure 2.2).
Coordinated muscle activity is required to produce the joint moments shown
above. Muscle activity can be monitored and measured during gait using
electromyography (EMG). During unimpaired gait, EMG has shown that the
quadriceps are active during early stance and gastrocnemius activity increases during
Figure 2.2: Kinetics including joint moments (Nm/kg) and powers (W/kg) during unimpaired gait(average ± one standard deviation).

13
mid and terminal stance (Figure 2.3). In terminal stance and early swing, there is a
burst of rectus femoris activity and the anterior tibialis activates to dorsiflex the ankle.
At the end of swing, the quadriceps and hamstring are active to prepare the limb for
the next gait cycle.
Determining how muscle activity measured from EMG contributes to motion
can be difficult due to the complexities of the musculoskeletal system and the
inconsistencies between EMG magnitude and muscle force. Dynamic coupling
describes the ability of muscles to accelerate joints they do not cross (Zajac and
Gordon, 1989). Since the human body is a system of bodies connected by joints, if a
muscle generates acceleration at one joint it will produce resulting accelerations at
other joints in the system. For example, during stance, activity of the ankle
plantarflexors not only plantarflexes the ankle but also accelerates the knee into
extension; this is commonly referred to as the plantarflexion-knee extension couple
(Gage and Schwartz, 2001; Gage and Schwartz, 2004). Musculoskeletal modeling and
simulation, which will be described in more detail in section 2.4, can be used to
examine how muscles contribute to these complex motions. Previous studies have
Figure 2.3: Average periods when the muscles are active during unimpaired gait from EMG data collected at Lucille Packard Children’s Hospital.

14
demonstrated that during unimpaired gait, the vasti and gluteus maximus support the
body and slow forward progression in early stance, the gluteus medius helps to
support the body during mid stance, and the gastrocnemius and soleus support and
propel the body forward during late stance (Neptune et al., 2001; Anderson and Pandy,
2003; Liu et al., 2006). Understanding how these complicated interactions change
during pathologic gait patterns such as crouch gait is one of the primary objectives of
this dissertation.
2.2 CEREBRAL PALSY
Cerebral palsy is an umbrella term used to describe an injury to the brain at or
near the time of birth that causes problems with movement and coordination. Common
causes of brain injury include hypoxic-ischemia, infections, head injury, and jaundice.
The prevalence of cerebral palsy in the developed world is estimated at between 1.2
and 3.6 cases per 1000 individuals, depending on geographic region and
socioeconomic status (Yeargin-Allsopp et al., 2008; Blair, 2010). The average lifetime
cost for individuals with cerebral palsy was estimated at $921,000 per individual in
2003 (National Institutes of Health).
Cerebral palsy is commonly characterized by the degree of involvement and
movement pattern. Cerebral palsy which affects only one side (right or left) of the
body is referred to as hemiplegia. Diplegia refers to when just the lower limbs are
affected and quadriplegia refers to when the arms and legs are affected. Common
types of altered movement include: spastic, characterized by heightened stretch- or

15
velocity-dependent muscle activation; dystonic, characterized by sustained or
intermittent muscle contractions; ataxic, characterized by decreased muscle tone and
unsteady, shaky movement; and dyskinetic, characterized by involuntary motions (also
referred to as athetoid). Spastic cerebral palsy is the most common type and affects
between 77 and 93% of individuals with cerebral palsy. This dissertation will focus on
individuals with spastic diplegic cerebral palsy.
2.3 CROUCH GAIT
Crouch gait is one of the most common gait pathologies in individuals with
spastic diplegic cerebral palsy. Among pediatric patients who visited one clinical gait
lab, 69% had the increased knee flexion in stance characteristic of crouch gait (Wren
et al., 2005). One of the first descriptions of crouch gait appeared in a manuscript in
1890 by E.H. Bradford who described a gait pattern in which “the heel is not placed
upon the ground, the knee is bent, and the knee is thrown to the inner side.”
Today, crouch gait is an umbrella term for a spectrum of gait patterns that all
share the common feature of excessive knee flexion during stance. Some authors (Lin
et al., 2000; Chambers, 2001; Young et al., 2010) have refined the definition of crouch
gait to differentiate between gait patterns such as jump gait, characterized by excessive
ankle plantarflexion and knee flexion at initial contact which resolves by terminal
stance; apparent equinus, characterized by excessive knee flexion throughout stance
with the heel off the ground; and crouch gait, characterized by calcaneal gait (i.e., flat-
footed, heel contact) and excessive knee flexion throughout stance. This dissertation

16
focuses on individuals with crouch gait who have excessive knee flexion throughout
stance with the heel on the ground (Figure 2.4).
Gait pathologies such as crouch gait negatively affect mobility and are
inefficient due to muscle co-contraction, altered movement patterns, and the use of
assistive devices (see Waters and Mulroy, 1999, for a review). One study reported a
100% increase in the physiological cost of outdoor locomotion (Raja et al., 2007)
among individuals with cerebral palsy and various gait pathologies. Individuals with
cerebral palsy demonstrate slower walking speeds (Campbell and Ball, 1978; Rose et
al., 1990), which makes it difficult for them to keep up with peers. Crouch gait can
also contribute to pain, joint degeneration, and the formation of bone deformities
(Rosenthal and Levine, 1977; Lloyd-Roberts et al., 1985; Murphy, 2009). As
individuals with cerebral palsy and crouch gait enter adulthood, knee pain, hip
subluxation, osteoarthritis, lumbar spondylosis, and cervical stenosis commonly
develop (Murphy, 2009). Furthermore, the gait of individuals with cerebral palsy
deteriorates over time, especially without treatment (Johnson et al., 1997; Bell et al.,
Figure 2.4: Average knee flexion during mild, moderate, and severe crouch gait compared to unimpairedgait and a musculoskeletal model illustrating a typical crouch gait pattern.

17
2002; Rose et al., 2010). In combination, these factors lead to reduced mobility which
limits individuals’ ability to accomplish activities of daily living and negatively affects
quality of life.
There are many proposed causes of crouch gait, including poor neuromuscular
control, impaired balance, altered muscle physiology, and skeletal deformities.
Although cerebral palsy is caused by an injury to the brain, most treatments currently
target the musculoskeletal limitations of individuals with cerebral palsy that result
from the brain injury and limit mobility. The following sections outline
musculoskeletal factors that may contribute to crouch gait and synthesize treatment
options for crouch gait.
2.3.1 CAUSES OF CROUCH: EXCESSIVE FORCE
Excessive force from muscles or passive structures can restrict joint range of
motion and contribute to crouch gait. Muscle contracture, defined as a passive
resistance to stretch, and muscle spasticity, defined as a velocity-dependent resistance
to stretch, are common in individuals with cerebral palsy. Contracture, spasticity, or
over-activity of muscles during movement may contribute to crouch gait by limiting
hip, knee, and ankle motion. Excessive force from the hamstrings, gastrocnemius, and
iliopsoas are the most commonly cited potential contributors to crouch gait and are
common targets for surgical and therapeutic treatments.

18
Hamstrings
Hamstrings contracture, spasticity, or over-activity is thought to contribute to
crouch gait by limiting knee extension during terminal swing or stance. The bi-
articular hamstrings, including the semimembranosus, semitendinousus, and biceps
femoris long head have knee flexion and hip extension moment arms. The biceps
femoris short head is the only uni-articular knee flexor and shares a distal tendon with
the biceps femoris long head. The hamstrings are often grouped into the medial
hamstrings (semimembranosus and semitendinousus) and the lateral hamstrings
(biceps femoris long head and short head), based upon their insertion points distal to
the knee. The hamstrings are hypothesized to contribute to crouch gait because limited
hamstring range of motion and prolonged hamstrings activity during stance have been
reported among individuals with crouch gait (Hoffinger et al., 1993).
Figure 2.5: Anatomy of the hamstrings, iliopsoas, and ankle plantarflexors (gastrocnemius and soleus)from the University of Washington Musculoskeletal Atlas.

19
Determining if the hamstrings cause crouch gait is difficult due to the
complexities of the musculoskeletal system. Due to dynamic coupling, bi-articular
muscles, such as the hamstrings, can accelerate a joint in a direction opposite of the
muscle’s moment arm. Thus, although the bi-articular hamstrings have a knee flexion
moment arm, during activities such as walking, the hamstrings could contribute to
knee extension due to dynamic coupling.
Musculoskeletal modeling and electrical stimulation studies have confirmed
that the bi-articular hamstrings can accelerate the knee into extension through dynamic
coupling if they generate sufficiently large hip extension moments. Electrical
stimulation of the hamstrings in a standing posture has demonstrated that the action of
the hamstrings changes from flexing the knee to extending the knee with increasing
crouch (Stewart et al., 2008). Musculoskeletal simulations have shown that during
unimpaired gait the hamstrings have a knee extension potential (Arnold et al., 2005)
and do not contribute significantly to swing limb knee flexion (Arnold et al., 2007),
although they are active in terminal swing. During crouch gait, the hamstrings have a
small knee extension potential during stance (Hicks et al., 2008, see Chapter 3) and the
hip and knee extension potentials of the hamstrings do not decrease like other muscles
with increasing crouch severity (Hicks et al., 2008) or increasing tibial torsion (Hicks
et al., 2007). These results suggest that excessive force from the hamstrings may not
contribute to the excessive knee flexion characteristic of crouch gait. However, tight
hamstrings due to muscle contracture may still limit knee range of motion. An
experimental study using an exoskeleton built to mimic muscle contracture in
unimpaired individuals found that hamstring contracture did increase knee flexion in

20
terminal swing and early stance (Matjacic and Olensek, 2007) and, therefore,
hamstring contracture may contribute to crouch gait.
There are a variety of clinical exams that are commonly used to determine if
the hamstrings should be treated in an individual with cerebral palsy and crouch gait.
Traditionally, passive physical exams including popliteal angle (maximum extension
of the knee when the patient is supine and the hip is flexed to 90°) and straight leg
raise (maximum hip flexion when the patient is supine and the knee is fully extended)
have been used to measure range of motion of the hamstrings. However, the
association between these measures and gait are not clear. Popliteal angle has been
reported to have a poor correlation with knee flexion during walking (Thompson et al.,
2001; Desloovere et al., 2006) while straight leg raise has been reported to have a
significant correlation to change in knee flexion during gait after surgery (Thometz et
al., 1989). Static physical exam measures may not be ideal for determining the
contribution of the hamstrings to dynamic activities such as gait.
An alternative to static exam measures is calculating musculotendon length
and velocity of the hamstrings during gait using musculoskeletal modeling. Arnold et
al. (2006) examined preoperative and postoperative peak musculotendon length and
velocity of the semimembranosus in 152 subjects with cerebral palsy and observed a
relationship between musclotendon length and velocity and surgical outcome (Delp et
al., 1996; Arnold et al., 2006a; Arnold et al., 2006b). Subjects whose hamstrings peak
lengths or velocities during gait remained short or slow after surgery were unlikely to
have improved knee extension. These results suggest that indicators measured during a
functional activity, such as musculotendon length and velocity, could provide better

21
information for surgical decision making than static exam measures. While measuring
musculotendon lengths and velocities cannot determine whether short musculotendon
lengths are the cause of crouch gait or a result the gait pattern, Van der Krogt et al.
(2007) reported that unimpaired individuals walking in a crouch gait did not have
short or slow hamstrings; this suggests that evidence of short or slow hamstrings in
individuals with cerebral palsy may indicate that the hamstrings are contributing to
crouch gait.
Spasticity of the hamstrings is evaluated using a combination of the Ashworth
Scale, Tardieu Scale, and EMG patterns during gait. Excess hamstring activity during
stance has been suggested to indicate spastic hamstrings (Crenna, 1998); however, the
hamstrings may be active during this time to assist with hip and knee extension. The
spastic velocity threshold, defined as the angular velocity of the joint at which
inappropriate muscle activity is triggered, provides a more quantitative measure for
assessing muscle spasticity. Spastic velocity threshold of the hamstrings has been
shown to be associated with peak knee angular velocity during maximum speed
walking suggesting that hamstrings spasticity could limit knee angular velocity during
gait (Tuzson et al., 2003). More quantitative measures of spasticity are required to
clarify how hamstring spasticity may contribute to crouch gait and to provide
clinically relevant exams.
Surgical treatment for the hamstrings in individuals with crouch gait can
involve lengthening, releasing, or transferring the hamstrings. Release or transfer of a
muscle theoretically eliminates unwanted contributions to motion at a given joint
while musculotendon lengthening reduces passive tension and may diminish the

22
spastic reflex. Little is known however about how these procedures alter muscle
properties or change the force-length or force-velocity properties of muscles. A study
by Granata et al. (2000) noted that although kinematics improved after musculotendon
lengthening, angular velocities and muscle activations did not change significantly.
These findings may indicate that musculotendon lengthening changes the range of
motion of a muscle but does not change the threshold velocity that triggers spasticity.
Hamstring lengthening has been a treatment used by orthopaedic surgeons for
over a century (Bradford, 1890) and is currently the most common surgery for treating
tight or spastic hamstrings. Multiple reviews recommend the use of distal hamstring
lengthening for the treatment of crouch gait (Green and McDermott, 1942; Pollock,
1962; Fixsen, 1979; Gage, 1990). To evaluate the outcomes after hamstring
lengthening we performed a meta-analysis of outcomes after distal hamstring
lengthening. The outcomes included in this analysis were (1) change in popliteal
angle, a clinical exam used to measure the passive range of motion of the hamstrings,
(2) change in knee flexion angle during gait, and (3) change in pelvic tilt during gait
(Figure 2.6). We also compared outcomes for surgeries that lengthened both the
medial and lateral hamstrings versus lengthening only the medial hamstrings.
The results of this meta-analysis indicated that after distal hamstring
lengthening, popliteal angle improved by an average of 19° (Fig. 3, 95% CI: 14-24);
however, the range of improvement in popliteal angle varied from 4° (Gannotti et al.,
2007) to 40° (Baumann et al., 1980). There was no significant difference in the change
in popliteal angle between lengthening the medial and lateral hamstrings versus the
medial hamstrings alone. Knee extension during gait also improved after hamstring

23
lengthening. The average change was 12.8° more knee extension at initial contact
(95% CI: 8.9-16.7) and 10.9° more knee extension during stance (95% CI 6.6-15).
Lengthening the medial and lateral hamstrings increased knee extension at initial
contact and during stance significantly more than lengthening only the medial
hamstring. At initial contact, lengthening the medial and lateral hamstrings increased
knee extension by 13.4° (95% CI 5.5-21.5) versus 9.5° (95% CI, 4-15, p = 0.027) for
lengthening only the medial hamstrings. Knee extension during stance increased by
14.6° (95% CI 3.8-25.5) when lengthening both the medial and lateral hamstrings
versus 6.5° (95% CI, 0.6-12.5, p < 0.001) for lengthening only the medial hamstrings.
Improvements in hip internal rotation (Steinwender et al., 2000; Lovejoy et al., 2007)
and spasticity (Vlachou et al., 2009) have also been reported after hamstring
lengthening but require further study. Despite changes in kinematics, temporal-spatial
parameters have been reported to have minimal changes when normalized by height
(Thometz et al., 1989; van der Linden et al., 2003).
A variety of adverse outcomes have been reported after hamstring lengthening
including increased anterior pelvic tilt, stiff-knee gait, exaggerated lumbar lordosis,
genu recurvatum, and nerve palsy (Hsu and Li, 1990). From the results of the meta-
analysis, the average change in pelvic tilt was 3° increased anterior pelvic tilt (95% CI,
0 – 6). The largest reported change was a 14° increase in anterior pelvic tilt (Rodda et
al., 2006). There was no significant difference in the change in anterior pelvic tilt
(student’s t-test, p=0.17) between lengthening the medial and lateral hamstrings and
lengthening the medial hamstrings. DeLuca et al. (1998) reported an increase in
anterior pelvic tilt when pelvic tilt was within normal limits before surgery and both

24
the medial and lateral hamstrings were lengthened. Multiple studies have also noted
that if anterior pelvic tilt was greater than 16° before surgery, lengthening the
hamstrings did not further increase anterior pelvic tilt (DeLuca et al., 1998; van der
Linden et al., 2003).
Genu recurvatum, hyperextension of the knee during stance, developed in an
average of 11% of subjects after hamstring lengthening in the studies included in the
meta-analysis. Reported risk factors for genu recurvatum included a jump knee gait
pattern and ankle plantarflexor spasticity (Thometz et al., 1989; Adolfsen et al., 2007).
Karol et al. (2008) reported development of nerve palsy, characterized by numbness,
loss of motor function in the foot, or hypersensitivity of the foot in 9.6% of subjects
who underwent hamstring lengthening. Subjects that were at higher risk for nerve
palsy were older, non-ambulatory, or non-communicative. Katz et al. (2004) suggested
that monitoring the evoked potential of the sciatic nerve during surgery may be an
effective way to prevent nerve damage. Muscle weakness is also a common concern
following musculotendon surgery; however, Damiano et al. (1999) reported that
hamstring strength recovered within nine months after lengthening surgery. The
possibility of adverse outcomes after distal hamstring lengthening warrant caution and
judicious lengthening; however, the improvements in knee extension during stance
and passive range of motion support distal hamstring lengthening for the treatment of
crouch gait.

25
Figure 2.6: Meta-analysis of outcomes after hamstring lengthening including change in popliteal angle, change in knee flexion angle, and change in pelvic tilt.

26
Less common surgical treatment options for the hamstrings include proximal
hamstring lengthening, hamstring transfer, and hamstring release. Proximal hamstring
lengthening has been recommended if there is no knee flexion contracture but the
hamstrings are still tight (Fixsen, 1979). Reimers (1974) compared proximal and distal
lengthening and noted that the advantages of the proximal lengthening include a less
visible scar, no plaster casts, shorter periods of immobilization, and access to other
proximal muscles for treatment; however, the author recommended distal lengthening
if more than 5° of knee flexion contracture is present since proximal lengthening does
not affect the short head of the biceps femoris. The effects of proximal lengthening on
gait have not been investigated.
Transferring the hamstrings to the femoral condyles was a popular procedure
in the 1950s and 60s (Eggers, 1952; Eggers and Evans, 1963); however, this procedure
is thought to cause excessive genu recurvatum, a loss of active knee flexion, decreased
pelvic stability, a stiff gait, and accentuated lumbar lordosis (Pollock, 1962; Pollock
and English, 1967; Roosth, 1971; Reimers, 1974; Ray and Ehrlich, 1979; Grujic and
Aparisi, 1982; Young et al., 2010). Keats and Kambin (1962) noted better results
when hamstring transfer was combined with patellar advancement. These early
procedures lacked gait analysis to objectively analyze surgical outcomes. More
recently, Metaxiotis et al. (2004) converted the semitendinousus and gastrocnemius to
monoarticular muscles by transfer to the femur and tibia, respectively, in 20 children
with spastic diplegia and found improved knee extension during stance and
hyperextension in 5 out of 40 limbs. These authors argued that muscle transfer may
prevent muscle weakness that may occur after lengthening procedures.

27
Proximal hamstring release has also been investigated as a treatment for
hamstring contracture. Although this procedure corrected knee flexion deformity and
hamstring range of motion during physical exam (Seymour and Sharrard, 1968;
Drummond et al., 1974; Sharps et al., 1984; Smith and Stevens, 1989), it increased the
risk of lumbar lordosis (Sharps et al., 1984) and genu recurvatum (Drummond et al.,
1974). Drummond et al. (1974) does not recommend proximal hamstring release for
the treatment of crouch gait.
Femoral extension osteotomy and patellar tendon advancement have recently
been proposed as an alternative to distal hamstring lengthening. Femoral extension
osteotomy has been reported to improve knee flexion contractures and increase knee
range of motion during gait (de Morais Filho et al., 2008; Stout et al., 2008). Stout et
al. (2008) reported post-operative knee function that was within normal limits when
femoral extension osteotomy was combined with patellar advancement. Hamstring
length and velocity were also found to increase following femoral extension
osteotomy and patellar tendon advancement without concomitant hamstring surgery
(Healy et al., 2011). Recommended indications for surgery include a persistent crouch
despite treatment, a knee flexion contracture between 10 and 30°, and a quadriceps lag
greater than 10° (Stout et al., 2008). Contraindications include a knee flexion
contracture greater than 30°, femoral malrotation greater than 30°, or patella baja
(Novacheck et al., 2009). Further study of femoral extension osteotomy is warranted
for the treatment of crouch gait.
Non-surgical treatment options for the hamstrings include neruomuscular
toxins such as botulinum toxin type A and baclofen. A limited number of studies have

28
examined the effects of neuromuscular toxins on crouch gait. Thompson et al. (1998)
performed a study of 10 subjects with crouch gait who were treated with isolated
hamstring botulinum toxin type A injections and found a significant increase in medial
hamstring length during gait, an improvement of 15° in knee extension, and increased
walking speed (Thompson et al., 1998). Others have noted improved knee extension in
stance following combination of multi-level botulinum toxin injection, casting, and
orthoses (Corry et al., 1999; Hesse et al., 2000; Papadonikolakis et al., 2003; Scholtes
et al., 2006; Scholtes et al., 2007); however, these improvements in gait may not be
maintained after 12 weeks (Corry et al., 1999; Scholtes et al., 2007). Thompson et al.
(1998) recommended that botulinum toxin is most effective for individuals with
spasticity rather than muscle contracture, since the neuromuscular toxin affects the
neuromuscular junction and not the passive material properties of the muscle. These
recommendations are supported by Sutherland et al. (1996) who found that passive
range of motion of the ankle plantarflexors was not improved after treatment with
botulinum toxin type A. The disadvantages of neuromuscular toxins are that the
effects decrease over a period of three to six months, repeated treatments are less
effective, and the toxins may have negative long-term effects on muscle physiology.
More research on the physiological effects of neuromuscular toxins and long-term
follow-up studies are required to evaluate the efficacy of neuromuscular toxins for the
treatment of crouch gait.

29
Hip flexors
The iliacus and psoas are the primary mono-articular hip flexors and excessive
force due to contracture, spasticity, or over-activity of these muscles could contribute
to excess hip flexion during crouch gait. Excess hip flexion can also contribute to
excess knee flexion through the need to maintain sagittal plane balance (Young et al.,
2010) and through accelerations generated by dynamic coupling. Musculoskeletal
simulations have shown that the psoas has a large knee flexion potential during stance
in both unimpaired (Arnold et al., 2005) and crouch gait (Hicks et al., 2008).
Furthermore, an experimental study using an exoskeleton to mimic muscle contracture
in unimpaired individuals found that hip flexion contracture increased crouch gait
(Matjacic and Olensek, 2007).
The Thomas test, prone hip extension test (Staheli test), and hamstring shift
test are common physical exams used to measure hip flexion contracture and
determine if the hip flexors require treatment in individuals with crouch gait. Similar
to physical exams for the hamstrings, there is no correlation between passive physical
exams and hip motion during gait (Lee et al., 2011). Musculotendon length and
velocity can also be calculated for the hip flexors during gait. Delp et al. (1996)
reported that psoas lengths were more than two standard deviations shorter in
individuals with cerebral palsy and crouch gait than during unimpaired gait. However,
caution needs to be taken when using psoas length to determine if the psoas should be
surgically lengthened since unimpaired individuals walking in a crouch gait also have
short psoas (van der Krogt et al., 2007), suggesting that psoas lengths cannot be used
to differentiate between short psoas that are a cause of crouch gait or a consequence of

30
the crouch posture. Additionally, psoas lengths are sensitive to femoral anteversion
(Schutte et al., 1997) which is commonly not included in musculoskeletal models.
The most common surgical interventions for hip flexors in individuals with
crouch gait are lengthening or releasing the hip flexors. Many methods of lengthening
the hip flexors have been shown to reduce hip flexion contractures, including division
of all hip flexors except the psoas (Roosth, 1971), psoas tenotomy (Nene et al., 1993),
and psoas recession at the pelvic brim (Patrick, 1996; Sutherland et al., 1997;
Novacheck et al., 2002; Zwick et al., 2002). Roosth (1971) reported that relieving hip
flexion contracture resulted in a more erect posture, reduced lumbar lordosis, and
improved balance. A potential adverse outcome of these procedures is reduced active
hip flexion capacity. There is conflicting evidence on the effects of psoas recession at
the pelvic brim on active hip flexion; some studies have reported that subjects
maintain active hip flexion after recession (Sutherland et al., 1997; Novacheck et al.,
2002), but others have reported decreased active hip flexion after surgery (Zwick et
al., 2002). An increased tendency toward genu recurvatum has also been noted when
psoas recession is combined with hamstring lengthening (Zwick et al., 2002; Ma et al.,
2006). DeLuca et al. (1998) recommends lengthening the psoas if hip flexion
contracture is greater than 15°, while Davids et al. (2004) recommends iliopsoas
recession if hip flexion contracture is greater than 30°.

31
Ankle Plantarflexors
The gastrocnemius has a knee flexion moment arm and excess force due to
spasticity, contracture, or over-activity could contribute to excess knee flexion during
crouch gait. The contribution of the gastrocnemius to crouch gait is complicated by the
fact that it shares an insertion through the Achilles tendon with the uni-articular
soleus. Musculoskeletal simulation studies have shown that these two muscles have
significantly different contributions to movement. The gastrocnemius contributes to
knee and hip flexion while the soleus contributes to hip and knee extension during
stance in both unimpaired (Arnold et al., 2005) and crouch gait (Hicks et al., 2008 and
see Chapter 3). Yet, both muscles have been shown to contribute to upward support of
the mass center during crouch gait (see Chapters 3 and 4).
To determine if the gastrocnemius is contributing to crouch gait, clinicians
typically measure ankle range of motion with the knee flexed and the knee extended to
differentiate between soleus and gastrocnemius contracture. Baddar et al. (2002) also
suggested examining the correlation between ankle and knee motion during single-
limb stance; a correlation between knee extension and ankle plantarflexion in
individuals with crouch gait could indicate that the gastrocnemius is restricting knee
motion. Musculotendon lengths and velocities have not been used to examine
gastrocnemius function during crouch gait. Spasticity of the gastrocnemius is often
measured with the Ashworth Scale or by monitoring gastrocnemius EMG activity
during stance (Crenna, 1998).
The most common treatment for the ankle plantarflexors is musculotendon
lengthening of the gastrocnemius, soleus, or both muscles; however, the efficacy of

32
these procedures in individuals with crouch gait is a debated subject. There is
conflicting evidence on the effect of gastrocnemius and soleus lengthening on crouch
gait, likely due to the wide variety of surgical techniques used and the effects of
concomitant surgeries. The gastrocnemius and soleus can be lengthened by a Z-
lengthening, step lengthening, sliding lengthening, tenotomy or subcutaneous
lengthening of the Achilles tendon. The gastrocnemius can be lengthened using the
Strayer, Baker, and Vulpius techniques which leave the soleus intact. Reported
changes in crouch gait after lengthening the gastrocnemius and soleus or the
gastrocnemius alone have been similar; an 8° change in knee extension at initial
contact (Baddar et al., 2002; Galli et al., 2005; Galli et al., 2009), but no significant
change in mid stance knee flexion (Baddar et al., 2002; Orendurff et al., 2002; Galli et
al., 2005). Van der Linden et al. (2003) found that patients who did not have a
gastrocnemius lengthening in conjunction with a hamstring lengthening had 6° more
plantarflexion at initial contact. Musculoskeletal models have shown that tendoachilles
lengthening can significantly reduce the force generating capacity of the plantarflexors
(Delp et al., 1995). Since the gastrocnemius and soleus both contribute to upward
acceleration of the mass center during crouch gait (see Chapters 3 and 4), lengthening
these muscles could compromise individuals’ ability to support themselves. The
appropriate candidates for surgical intervention and the amount of ankle plantarflexor
lengthening are important areas for further investigation.

33
Passive Structures
In addition to excessive force from muscles, excessive force from passive
structures surrounding the hip and knee can also contribute to crouch gait. A fixed hip
or knee flexion contracture is caused by excessive tightness of the passive structures
surrounding the joint. Indicators for fixed contracture include restricted passive range
of motion which persists when an individual is under anesthesia and muscles are not
taut. Treatments for a fixed knee flexion contracture include knee capsulotomy,
anterior femoral hemiepiphysiodesis (also known as “guided growth”), and serial
casting. Knee capsulotomy combined with hamstring lengthening has been reported to
improve popliteal angle by 22° (Woratanarat et al., 2009) while serial casting has been
reported to reduce knee flexion contracture by 12° (Westberry et al., 2006). However,
recurrence of fixed knee flexion contractures is common after both of these
procedures, especially in younger patients. Anterior femoral hemiepiphysiodesis
involves applying staples to the anterior surface of the femur over the growth plate,
resulting in a curvature of the femur during growth. The average reported correction of
knee flexion contracture is 0.9°/month, for a total correction of 12.7° (Kramer and
Stevens, 2001; Klatt and Stevens, 2008). This procedure is minimally invasive and
requires no immobilization, which allows for immediate resumption of bracing and
physical therapy. Klatt et al. (2008) recommended anterior femoral
hemiepiphysiodesis for subjects with greater than 10° knee flexion deformity and
more than 12 months of growth remaining. Changes in gait following these procedures
have not been reported and represent an important area for future research.

34
2.3.1 CAUSES OF CROUCH: INADEQUATE FORCE
The inability of muscles to generate sufficient force to support and propel the
body may also contribute to crouch gait. Weakness may be the result of reduced
physiological cross-sectional area, lack of volitional control, previous surgeries, or
altered muscle physiology. Muscle weakness is well-documented among individuals
with cerebral palsy. Children with cerebral palsy have been shown to have
significantly weaker quadriceps, hamstrings, hip extensors, and ankle muscles
compared to their unimpaired peers (Damiano et al., 1995a; Wiley and Damiano,
1998). During crouch gait, a correlation between knee extensor strength and knee
extension during stance has also been reported (Damiano et al., 1995a; Rethlefsen et
al., 1999) suggesting that muscle weakness may contribute to crouch gait.
From a biomechanics perspective, individuals who walk in a crouch gait may
not be able to generate the required forces and accelerations to achieve an upright gait.
During crouch gait, the hip and knee flexion moments increase dramatically during
stance. Musculoskeletal simulation studies have shown that the hamstrings, gluteus
maximus, vasti, and ankle plantarflexors are the primary contributors to hip and knee
extension during stance in both unimpaired gait (Arnold et al., 2005) and crouch gait
(see Chapter 3). Muscle weakness in any of these muscle groups could contribute to
crouch if individuals are not able to adequately extend their hips and knees or support
their body weight. During swing, the primary contributors to knee extension are the
hip extensors and ankle plantarflexors (Arnold et al., 2007). If these muscles are weak,
knee extension at initial contact could be diminished and the subject may not be able
to reach full knee extension during stance. A crouch posture also diminishes the ability

35
of lower-extremity muscles to extend the hip and knee (Hicks et al., 2007). Therefore,
to create the same angular accelerations of the hip and knee in a crouch posture
requires more muscle force than in an upright posture. These factors magnify the
effects of muscle weakness.
Compensation for weak muscles by other muscle groups could also contribute
to crouch gait. For example, Jonkers et al. (2003) showed that the gluteus maximus,
plantarflexors, and hamstrings play complementary roles to control the stance limb
during unimpaired gait. If one of these muscle groups is impaired, the other muscles
may be recruited to compensate for weakness; however, compensation could have
negative consequences during gait. For example, if gluteus maximus is weak,
increased hamstring and gastrocnemius activity to support the body could increase
knee flexion.
Inadequate muscle force can also be a result of previous surgical interventions,
such as lengthening the Achilles tendon. Musculoskeletal modeling studies have
demonstrated that over-lengthening the Achilles tendon can reduce the amount of
force the ankle plantarflexors can produce (Delp et al., 1995). Adverse outcomes after
Achilles tendon lengthening include excess ankle dorsiflexion and knee flexion
(Sutherland and Cooper, 1978). Wiley et al. (1998) noted that individuals who had
prior Achilles lengthening tended to have weaker plantarflexors, but the difference
was not significant. The prevalence of a crouch gait pattern after lengthening the
Achilles tendon has been reported between 0 and 50% (Bernthal et al.; Craig and van
Vuren, 1976; Segal et al., 1989; Damron et al., 1993; Abel et al., 1999; Borton et al.,
2001; Dietz et al., 2006). De Morais Filho et al. (2010) reported that subjects with a

36
minimum knee flexion angle greater than 30° during stance were more likely to have
had an Achilles lengthening than subjects who did not walk in a crouch gait after
orthopaedic surgery; however, subjects who received an Achilles lengthening surgery
may have been more severely impaired or other factors could have contributed to
crouch gait. These studies indicate that musculotendon lengthening surgery can reduce
the force generating capacity of a muscle and could increase the risk of crouch gait.
Altered musculoskeletal physiology due to impaired development can also
contribute to crouch gait by altering the amount of force a muscle can produce in a
given position. Patella alta refers to an abnormally high patella in relation to the
femur and is thought to be caused by excessive tension in the patellar tendon. This
condition is common in individuals with spastic cerebral palsy. Rosenthal and Levine
(1977) found patella alta in over 50% of patients with spastic cerebral palsy. The
effect of patella alta on the moment generating capacity of the quadriceps is unclear;
Sutherland et al. (1978) reported that patella alta reduces the moment generating
capacity of the quadriceps in all positions except extreme knee flexion, but more
recent studies have indicated that patella alta increases the quadriceps’ moment
generating capacity (Ward et al., 2005; Luyckx et al., 2009). Sheehan et al. (2008)
examined the patellar tendon moment arm in subjects with cerebral palsy, many of
whom had patella alta, and found no significant changes in the patellar tendon moment
arm. If left untreated, patella alta can cause fragmentation of the distal pole of the
patella as a result of excess tension (Rosenthal and Levine, 1977) or patella tendon
rupture (O'Sullivan et al., 2010).

37
Quadriceps lag is another common impairment found in individuals with
cerebral palsy which refers to a lack of full, active knee extension. Individuals with
quadriceps lag may be able to produce sufficient strength when the knee is flexed;
however, the quadriceps are weak when the knee is near full extension. No research is
currently available describing the underlying mechanisms of quadriceps lag and the
influence of quadriceps lag on crouch gait.
The most common treatment option for individuals with cerebral palsy and
muscle weakness is strength training. Studies have shown that strength training can
improve muscle strength in individuals with cerebral palsy to within normal limits
(Damiano et al., 1995b; Dodd et al., 2002; Mockford and Caulton, 2008).
Furthermore, strength training has been shown to improve walking velocity (Damiano
et al., 1995a) and knee extension during gait (Damiano et al., 1995b; Unger et al.,
2006). More recently, inconsistent outcomes among subjects with crouch gait have
been noted. Damiano et al. (2010) reported that after strength training of the hip and
knee extensors some individuals with crouch gait had improved knee extension while
others had more knee flexion during gait. Preliminary results suggest that these
differences in outcome may be related to hamstring spasticity (see Chapter 7); subjects
without hamstring spasticity had better outcomes. Unfortunately, most strength
training studies include subjects with many different gait patterns and do not examine
changes in gait before and after strength training which makes understanding the
efficacy of these programs difficult. Further, more controlled studies are required to
determine which individuals have positive outcomes after strength training programs.

38
Orthoses can also be used to compensate for muscle weakness. For the
treatment of crouch gait, ankle foot orthoses (AFOs) have been shown to have no
effect on knee extension during gait (Abel et al., 1998; Rethlefsen et al., 1999;
Wesdock and Edge, 2003; Brehm et al., 2008). Hassani et al. (2004) reported a
significant improvement in minimum stance knee flexion with both hinged and
dynamic AFOs; however, this study was not specific to individuals with crouch gait.
A more promising AFO for the treatment of crouch gait is the floor reaction AFO.
Several studies have noted a significant improvement in knee extension in stance with
the use of floor reaction AFOs in subjects with greater than 15° of knee flexion during
stance (Lucareli et al., 2007; Rogozinski et al., 2009). Brehm et al. (2008) reported
that improvement in metabolic cost with AFOs was significantly correlated with
minimum knee flexion angle during stance. These results suggest that AFOs that
improve knee flexion could produce a more energy-efficient gait pattern for
individuals with cerebral palsy.
2.3.1 CAUSES OF CROUCH: BONE DEFORMITIES
Rotational deformities of the tibia and/or femur are common in children with
cerebral palsy - a consequence of altered bone loading during development. A tibial
torsion deformity is an excess twisting of the tibia about its long axis and may be an
internal or external rotation. Femoral anteversion deformity is an excess internal twist
of the femoral neck with respect to the shaft of the femur. These deformities may
contribute to crouch gait by altering the moment arms, and hence moment generating
capacity, of muscles. Because the moments generated by muscles at joints can result in

39
motions at other joints due to dynamic coupling, a muscle affected by a bone
deformity may result in movement abnormalities at other joints it does not cross.
Bone deformities may also alter foot ground interaction which can impact
muscle function at joints throughout the body. For example, musculoskeletal modeling
found that although tibial torsion has a minimal effect on the moment arms of muscles
crossing the ankle joint, it has a significant adverse effect on the acceleration produced
by muscles crossing the hip and knee (Hicks et al., 2007). Musculoskeletal modeling
studies have demonstrated that tibial torsion significantly reduces the ability of
muscles to extend the hip and knee (Hicks et al., 2007; Hicks et al., 2008) and support
the mass center (Schwartz and Lakin, 2003). For example, a 30° external tibial torsion
deformity reduces the capacity of major lower-limb extensors including the gluteals
and soleus to extend the knee by over 10%. Hicks et al. (2007) also reported a greater
incidence of crouch gait in subjects with more than 30° of tibial torsion (70% vs.
40%). No studies have been performed on the effects of femoral anteversion on the
dynamic function of muscles during gait.
Distal tibial derotation osteotomies are performed at many clinical centers and
have been shown to be successful in correcting alignment of the tibia with few
complications (Dodgin et al., 1998; Selber et al., 2004; Ryan et al., 2005). Studies that
have reviewed patient outcomes report improved gait function (Stefko et al., 1998;
Selber et al., 2004; Ryan et al., 2005); however, sagittal plane kinematics are not
reported. Analyzing the effects of tibial derotation osteotomies are further complicated
by the fact that the procedure is typically performed as part of multi-level orthopaedic

40
surgery, not a randomized clinical trial, which makes it difficult to isolate the effects
of the tibial derotation osteotomy on gait compared to other concomitant surgeries.
Femoral derotation osteotomies have also been shown to be safe and effective
in correcting femoral alignment; however, there is limited evidence connecting
femoral derotation osteotomies to improvements in crouch gait. Ouunpuu et al. (2002)
et al. performed a prospective analysis with 97 subjects looking at short and long term
outcomes. In addition to improved hip alignment, they also reported improved mean
stance knee flexion, but almost all patients had concomitant treatment, including
hamstrings lengthening.
Foot deformities such as plano pes valgus are also common in individuals with
cerebral palsy and crouch gait. Similar to rotational bone deformities, foot deformities
could also impair the ability of muscles to extend the hip and knee; however, a direct
study of the effects of foot deformities on crouch gait has not been done and is an
important area for future study.
2.4 MUSCULOSKELETAL SIMULATION
The complexities of the human musculoskeletal system make it difficult to
evaluate, diagnose, and treat gait pathologies in individuals with cerebral palsy.
Musculoskeletal modeling and simulation provides a tool for examining this complex
system and evaluating problems with human movement. The benefits of modeling and
simulation include the ability to examine the effect of individual components of

41
complex systems, to perform studies that could not be done experimentally, and to ask
‘what-if’ questions.
OpenSim is a freely-available software that allows researchers and clinicians to
create musculoskeletal models of humans and animals and critically evaluate the
kinematics, kinetics, muscle contributions, and other forces in the system (Delp et al.,
2007). Furthermore, OpenSim allows researchers to share models and simulations,
expand the software, and critically evaluate one another’s work. All of the simulations
created as part of this dissertation are provided for other researchers to download,
evaluate, and use at http://www.simtk.org/home/crouchgait/ (Figure 2.7).
The process to create a musculoskeletal simulation depends upon the specific
question that is being investigated; however, the following paragraphs outline the
basic steps in the process. All investigations start with the selection or creation of a
Figure 2.7: Map of visitors to the website with the simulations and documentation presented in thisdissertation from July 1, 2011 to January 1, 2012 (http://www.simtk.org/home/crouchgait/).

42
musculoskeletal model. For the investigations included in this dissertation, a model of
the lower-limbs and torso which is based upon cadaver and physiological
measurements was used (Delp et al., 1990). This model included 19 degrees of
freedom including three translations and three rotations at the pelvis, a ball-and-socket
joint between the pelvis and torso at approximately the third lumbar vertebrae (i.e.,
L3), a ball-and-socket joint at each hip, a planar joint with coupled translations at each
knee, and revolute joints at each ankle. The muscles were modeled as line segments
with multiple lines of action for muscles with broad attachments. A lumped parameter
Hill-type muscle model generated forces as a function of muscle fiber length and
velocity, tendon length, and activation.
For each subject, the musculoskeletal model is scaled to the subject’s size
based upon anthropometric measurements. This includes scaling segment lengths,
masses, and inertias as well as muscle and tendon lengths. Experimental data from a
motion capture laboratory is used to estimate the subject’s kinematics, or joint angles.
In a motion capture laboratory, subjects perform gait or other movements with
reflective markers on their body that can be tracked by a camera system.
Electromyography and ground reaction forces can also be collected concurrently. In
OpenSim, this data is used to estimate the joint angles, or kinematics, by positioning
the model in a position that minimizes the error between experimental markers and
markers placed on the model using inverse kinematics. These kinematics can then be
coupled with ground reaction forces to calculate joint moments using inverse
dynamics. The kinematics and kinetics calculated from these processes can then be
used to compare a subject’s gait to other individuals.

43
To create a three-dimensional musculoskeletal simulation, the final step is to
determine the muscle excitations needed to produce the subject’s motion. However,
due to modeling and experimental errors, the model’s motion is not dynamically
consistent (Kuo, 1998) with measured ground reaction force (i.e. force ≠ mass x
acceleration). To account for these inaccuracies, non-physiological forces and
moments called residuals are applied to the pelvis. Since these forces are non-
physiological, we minimize the magnitude of these forces using the residual reduction
algorithm which makes small changes in measurements we know have error (such as
joint angles and the location of the torso mass center) to reduce the magnitude of these
residual forces (Delp et al., 2007).
After this step, we can then more confidently estimate muscle excitations. It is
challenging to estimate muscle excitations and forces because each joint in the
musculoskeletal system is crossed by more muscles than its degrees of freedom.
Therefore, we use computed muscle control which combines an optimization problem
with a feedback controller to determine the set of muscle excitations that minimize the
sum of muscle activations squared and tracks the subject’s measured motion (Thelen
et al., 2003; Thelen and Anderson, 2006). If an estimate of the distribution of muscle
forces is the primary outcome of interest in a research study, other less-
computationally expensive methods can be used to estimate muscle activations and
forces, such as static optimization. Static optimization estimates muscle forces by
determining the set of muscle forces required to satisfy the equations of motion at each
time step while minimizing an objective function (e.g., minimizing the sum of
activation squared). The advantages of using computed muscle control over static

44
optimization is that it includes the activation-deactivation timing of muscles, the
effects of musculotendon compliance, and does not allow muscle excitations to change
instantaneously from one time step to the next; however, computed muscle control is
more computationally expensive. The muscle activations or forces estimated with
either of these processes can be compared to experimental electromyography and
muscle excitations can be constrained to electromyography data if there are significant
differences.
Determining the accelerations generated by individual muscles can be useful in
many studies, including Chapters 3 and 4 of this dissertation, to understand how
individual muscles contribute to motion. A perturbation or induced acceleration
analysis can be used to estimate the accelerations produced by individual muscles. A
perturbation analysis estimates these accelerations by applying a unit force to the
muscle of interest, integrating forward a small amount in time (typically 20-30 ms),
and then calculating the accelerations based upon changes in position (Liu et al.,
2006). This analysis uses a spring-damper element applied at the experimentally
measured center of pressure to model foot-floor contact. An induced acceleration
analysis calculates the accelerations produced by a muscle by explicitly solving the
equations of motion and a constraint equation that represents contact between the foot
and the ground (Zajac and Gordon, 1989; Hamner et al., 2010). An advantage of the
induced acceleration analysis is that it is much more computationally efficient than a
perturbation analysis; however, both analyses are dependent upon the foot-ground
contact models used which may not accurately reproduce the interaction between the

45
foot and ground and is an important area for future investigation (Hamner et al., 2010;
Dorn et al., 2011).
There are limitations and challenges to using musculoskeletal modeling and
simulation. Results are based upon inputs and, thus, if the models do not accurately
represent the subject’s physiology or if there are errors in the experimental motion
capture data, the results may not be representative of the subject. The musculoskeletal
models included in this dissertation are scaled from a generic model of an adult which
was created from averaged experimental data. We assume the children with cerebral
palsy included in our study do not have significant bone deformities or altered muscle
physiology compared to typically-developing children; however, the line of action and
properties of muscles may be altered in individuals with cerebral palsy. Creating
subject-specific musculoskeletal models and more quantitative measures of altered
musculoskeletal physiology is an important area for future research. To check if our
simulations recreate experimental data we also compare our kinematics, kinetics, and
muscle activity to experimental measures. These challenges in creating and evaluating
simulations emphasize the importance of maintaining high standards in the analysis of
musculoskeletal simulations and, whenever possible, partnering simulation studies
with experimental measures.
Musculoskeletal modeling and simulation provides a platform for critically
evaluating complex systems and movements. The following chapters document how
this process can be used to examine the dynamics of crouch gait in individuals with
cerebral palsy. This represents a foundation for future researchers and clinicians to
build upon by improving models, creating new computational analyses, and

46
developing experimental tools to couple with simulation. The ultimate goal of this
work is to improve not only our understanding of pathologic gait patterns, but to
improve treatment and quality of life for these individuals.

47
CHAPTER 3
HOW DO MUSCLES CONTRIBUTE TO SUPPORT AND PROGRESSION DURING CROUCH GAIT?
Journal of Biomechanics (2010), vol. 43, pp. 2099-2105
Katherine M. Steele Ajay Seth Jennifer L. Hicks Michael H. Schwartz Scott L. Delp

48
ABSTRACT
Pathological movement patterns like crouch gait are characterized by abnormal
kinematics and muscle activations that alter how muscles support the body weight
during walking. Individual muscles are often the target of interventions to improve
crouch gait, yet the roles of individual muscles during crouch gait remain unknown.
The goal of this study was to examine how muscles contribute to mass center
accelerations and joint angular accelerations during single-limb stance in crouch gait
and compare these contributions to unimpaired gait. Subject-specific dynamic
simulations were created for ten children who walked in a mild crouch gait and had no
previous surgeries. The simulations were analyzed to determine the acceleration of the
mass center and angular accelerations of the hip, knee, and ankle generated by
individual muscles. The results of this analysis indicate that children walking in
crouch gait have less passive skeletal support of body weight and utilize substantially
higher muscle forces to walk than unimpaired individuals. Crouch gait relies on the
same muscles as unimpaired gait to accelerate the mass center upward, including the
soleus, vasti, gastrocnemius, gluteus medius, rectus femoris, and gluteus maximus.
However, during crouch gait these muscles are active throughout single-limb stance,
in contrast to the modulation of muscle forces seen during single-limb stance in
unimpaired gait. Subjects walking in a crouch gait rely more on proximal muscles,
including the gluteus medius and hamstrings, to accelerate the mass center forward
during single-limb stance than subjects with unimpaired gait.

49
3.1 INTRODUCTION
Crouch gait, a common movement pattern among individuals with cerebral
palsy, is characterized by excessive flexion of the hip, knee, and ankle during the
stance phase of gait. This walking pattern is inefficient (Rose et al., 1989; Waters and
Mulroy, 1999) and if left untreated can lead to joint pain (Jahnsen et al., 2004),
formation of boney deformities (Graham and Selber, 2003), and loss of independent
gait (Johnson et al., 1997; Opheim et al., 2009). Clinicians try to identify muscles that
can be strengthened, surgically lengthened, or otherwise treated to enable a more erect
and efficient walking pattern. Little is known, however, about how individual muscles
contribute to joint and mass center motions during crouch gait; thus, it is difficult to
design treatment plans that target muscles most likely to improve gait dynamics.
Figure 3.1: OpenSim model shown at different phases of single-limb stance during crouch gait. The muscles shown in red are highly activated, while those in blue have a low activation level, as determinedusing the computed muscle control algorithm.

50
Humans have developed an efficient walking pattern to achieve forward
progression while supporting body weight. Several studies (Anderson and Pandy,
2003; Neptune et al., 2004; Arnold et al., 2005; Kimmel and Schwartz, 2006; Liu et
al., 2006) have examined how muscles accelerate the joints and mass center during
unimpaired gait. These studies have shown that during early stance the vasti and
gluteus maximus support the body and slow forward progression, while in late stance
the gastrocnemius and soleus support body weight and propel the body forward
(Anderson and Pandy, 2003; Neptune et al., 2004; Liu et al., 2006). Liu et al. (2008)
demonstrated that the roles of these muscles are maintained over a range of walking
speeds.
Changes in joint kinematics and muscle activation patterns during crouch gait
alter how muscles contribute to joint and mass center accelerations. Hicks et al. (2008)
analyzed the potential of individual muscles to accelerate the hip and knee, per unit
force, in crouched walking postures. This analysis revealed that a crouched posture
markedly reduces the potential of several major lower-extremity muscles to generate
extension accelerations of the hip and knee and increases the joint flexion
accelerations from gravity. While this prior study determined the direction (i.e. flexion
or extension) of the accelerations generated by important muscles, the magnitudes of
the accelerations generated by muscles depend on muscle forces, which have not been
estimated for subjects with crouch gait.
Determining how muscles contribute to joint angular accelerations and mass
center accelerations during crouch gait can clarify the role of muscles during this
abnormal walking pattern and elucidate biomechanical consequences of treatments

51
such as surgically lengthening muscles. Thus, the goal of the present study was to
quantify angular accelerations of the hip, knee, and ankle generated by stance-limb
muscles during the single-limb stance phase of crouch gait by creating and analyzing
the first subject-specific dynamic simulations of crouch gait. Additionally, we
characterized how muscles accelerate the mass center, which provides a holistic view
of how muscles contribute to motion of the body during gait. The simulations are
freely available at www.simtk.org, enabling other researchers to reproduce the results
of this study and to perform additional analyses.
3.2 METHODS
3.2.1 SUBJECTS
Ten subjects with spastic diplegic cerebral palsy – age: 8.1 ± 1.7 yrs, height:
1.25 ± 0.09 m, weight: 27.1 ± 9.1 kg, leg length: 0.65 ± 0.06 m (average ± standard
deviation) – were selected from a database of subjects examined at Gillette Children’s
Specialty Healthcare (St. Paul, MN). Each subject included in the study: 1) walked
with a mild crouch gait (minimum knee flexion 15 - 40º during stance), 2) did not
walk in equinus and achieved at least 0º of dorsiflexion during his or her physical
exam, 3) had no previous surgeries, and 4) had no significant torsional skeletal
deformities (less than 30º of tibial torsion and femoral anteversion). All subjects
and/or guardians provided informed written consent for the data collection; analyses of
the data were performed in accordance with the regulations of all participating
institutions.

52
Motion analysis data was collected and kinematics determined using a 12-
camera system (Vicon Motion Systems, Lake Forest, CA) and a standard marker
measurement protocol (Davis et al., 1991). Four force plates (AMTI, Watertown, MA)
were used to record ground reaction forces and moments, which were sampled at 1080
Hz and low-pass filtered at 20 Hz. Our analysis focused on single support because a
lack of consecutive force plate strikes precluded the analysis of double support.
Subjects walked at a self-selected walking speed of 0.92 ± 0.18 m/s. Surface
electromyography (EMG) signals were recorded for nine of the ten subjects from the
medial hamstrings, biceps femoris long head, rectus femoris, gastrocnemius, and
tibialis anterior (Motion Lab Systems, Baton Rouge, LA). EMG was sampled at 1080
Hz, band-pass filtered between 20 and 400 Hz, rectified, and low-pass filtered at 10
Hz. EMG for each muscle was normalized from zero to one based on the minimum
and maximum values of that muscle over all trials for each subject.
3.2.2 DYNAMIC SIMULATION
A generic musculoskeletal model (lower extremities from Delp et al., 1990 and
torso from Anderson and Pandy, 1999) with 19 degrees of freedom and 92
musculotendon actuators was scaled to each subject according to their anthropometric
measurements (Figure 3.1). The degrees of freedom included a ball-and-socket joint
located at approximately the third lumbar vertebra between the pelvis and torso, ball-
and-socket joints at each hip, a planar joint with coupled translations at each knee, and
revolute joints at each ankle. A subject-specific simulation of the single-limb stance
phase of gait was then generated using OpenSim, a freely available biomechanical

53
simulation package (Delp et al., 2007), www.simtk.org. Double support was not
included in this study due to a lack of consecutive force plate strikes in the small set of
subjects who met our inclusion criteria. Kinematic and ground reaction force data
were imported into OpenSim, where the computed muscle control Algorithm
determined the muscle excitations that generated a forward dynamic simulation that
minimized the difference between the experimental and simulated gait kinematics
(Thelen et al., 2003; Thelen and Anderson, 2006). Estimated muscle activations were
scaled in the same manner as the EMG signals, and compared to the experimentally-
measured EMG signals to evaluate the fidelity of the simulation’s muscle activation
timing.
To test the sensitivity of the results to errors in muscle activation timing, we
constrained the simulated activations to match the shape and normalized magnitude of
the EMG for the 10 muscles for which EMG was recorded for one subject (See
Appendix A). When there was a disagreement between the EMG and simulated
activations, the normalized magnitude of the EMG was used to define maximum and
minimum bounds on the magnitude of the simulated activations. Although adding
these constraints changed the magnitude of the contribution of each muscle the
direction (e.g., flexion/extension) did not change. Since these changes in magnitudes
did not alter the conclusions drawn from analyzing this simulation, we chose not to
constrain activations for other subjects.
A perturbation analysis was used to determine the joint angular accelerations
and mass center accelerations generated by each muscle in the model (Liu et al.,
2006). In this analysis, one newton of additional force (the perturbation) was applied

54
to each muscle separately and the model’s equations of motion integrated forward in
time by 20 ms. These parameters for the perturbation analysis were chosen based upon
a sensitivity analysis and experience from previous studies (Neptune et al., 2001;
Goldberg et al., 2004). Evaluating the change in position of each joint and the mass
center after 20 ms, we determined the accelerations generated by each muscle by
assuming constant acceleration over this brief period. This quantity represents the
potential of each muscle to accelerate each joint and the mass center per newton of
force. A muscle’s contribution to joint and mass center accelerations was computed by
multiplying the muscle’s potential by its estimated force from the simulation at each
time step. Upward accelerations of the mass center were considered to contribute to
support of the body and forward accelerations were considered to contribute to
progression of the body. The contributions of each muscle to mass center accelerations
in the subjects with crouch gait were compared to two age, size, and speed matched,
unimpaired subjects (age: 8.6 ± 2.2 yrs; weight: 33.6 ± 10.6 kg; speed: 1.08 ± 0.1 m/s;
leg length: 0.71 ± 0.08 m) for whom motion analysis data were also collected at
Gillette Children’s Specialty Healthcare. The simulation data for these unimpaired
subjects have been previously reported (Liu et al., 2008) and are available at
www.simtk.org.

55
3.3 RESULTS
The muscle-driven simulation of each subject tracked all experimental joint
angles with an RMS error of less than 1° (Figure 3.2). The resultant joint moments
computed by multiplying the estimated muscle forces and moment arms also matched
the joint moments computed by inverse dynamics with an RMS error of less than 1
Nm (Figure 3.3).
Figure 3.2: Comparison of simulated and experimentally-measured joint angles. Average kinematics for pelvis, hip, knee, and ankle are shown for all 10 subjects. The gray line and shaded regions are the experimentally-measured joint angles (± 1 standard deviation) and the black line and dashed-lines are the kinematics reproduced by the simulation (± 1 standard deviation). The simulated kinematics are not provided during double support as only single-limb stance was simulated. The simulated kinematics were within 1º of experimental kinematics (RMS error) for all trials.

56
The normalized simulated activations and EMG showed similar on and off
patterns during single-limb stance (Figure 3.4). Differences between estimated
excitations and EMG included excessive rectus femoris activity during swing and
reduced biceps femoris activity during terminal swing in the simulations.
Figure 3.3: Comparison of the simulated and experimentally-measured hip, knee, and ankle moments for all 10 subjects. The gray line and shaded regions are the experimentally-measured joint moments (± 1 standard deviation) and the blue line and dashed-lines are the moments calculated by computed by multiplying the estimated muscle forces and moment arms (± 1 standard deviation). Joint moments are only shown during single-limb stance and swing since force plate data was not available during double support.

57
Subjects walking in crouch gait utilized higher muscle forces than the
unimpaired subjects. The average total muscle force of all stance-limb muscles during
single-limb stance in crouch gait was 8.6 ± 0.6 times body weight versus 5.3 ± 0.7
times body weight in unimpaired gait. The primary contributors to hip extension were
the gluteus maximus, posterior gluteus medius, and bi-articular hamstrings, while the
primary contributors to knee extension were the vasti, gluteus maximus, and soleus
Figure 3.4: Comparison of EMG and simulated activation. The EMG signal and activation were normalizedto a range of 0 to 1 between the maximum and minimum values for each subject. The gray line and shadedarea represents the EMG data (± 1 standard deviation) over a full gait cycle, while the simulated activationsduring single-limb stance are shown in blue with the dashed lines showing ± 1 standard deviation. Note thatestimated muscle activations are not provided during the double support periods of the gait cycle becauseonly single-limb stance was simulated.

58
(Figure 3.5). The iliacus and psoas muscles generated substantial flexion accelerations
of all three joints. The rectus femoris generated hip flexion acceleration.
The largest upward accelerations of the mass center were from the soleus,
followed by the vasti, then gastrocnemius, gluteus medius, rectus femoris, and gluteus
maximus (Figure 3.6). This subset of muscles provided 90% of the total upward
acceleration of the mass center generated by all muscles of the stance limb during
crouch gait and unimpaired gait. The ankle plantarflexors contributed more to support
during crouch gait, whereas the gluteus medius provided more support during
unimpaired gait. The primary muscles that accelerated the mass center downward
(Figure 3.6) included the anterior tibialis, iliopsoas, biceps femoris short head, hip
adductors (adductor longus, brevis, and magnus), and medial hamstrings
(semimembranosus and semitendinosus). The downward acceleration of the mass
center from gravity was larger in crouch gait as less support was provided by skeletal
alignment than in unimpaired gait (Figure 3.6).
-30000
-20000
-10000
0
10000
20000
30000
Glut Max Glut Med Bi-Art Hams Rectus Vasti Iliopsoas Gastroc Soleus
Hip
Knee
Ankle
Angu
lar A
ccel
erat
ion
(º/s
2 )ex
tfle
x
Figure 3.5: Average contributions ± 1 standard deviation to hip, knee, and ankle angular accelerationsduring single-limb stance from the major muscle groups of the stance limb. Positive and negativeaccelerations correspond to extension and flexion, respectively. Note that the muscles with average valuesclose to zero made small contributions throughout single-limb stance.

59
Acce
lera
tion
(m/s
2 )A
ccel
erat
ion
(m/s
2 )
-1
0
1
2
3
4
5
6
OTO OHCOTO OHC
Soleus
-1
0
1
2
3
4
5
6
OTO OHCOTO OHC
Vasti
-1
0
1
2
3
4
5
6
OTO OHCOTO OHC
Crouch Gait
Unimpaired Gait
Gastrocnemius
-1
0
1
2
3
4
5
6
OTO OHC
Gluteus Medius
-1
0
1
2
3
4
5
6
OTO OHCOTO OHC
Gluteus Medius
-1
0
1
2
3
4
5
6
OTO OHC
Rectus Femoris
-1
0
1
2
3
4
5
6
OTO OHCOTO OHC
Rectus Femoris
-1
0
1
2
3
4
5
6
OTO OHCOTO OHC
UP
FORWARD
Gluteus Maximus
-10
-8
-6
-4
-2
0
Biceps Femoris Short HeadIliopsoas Hip Adductors
Skeletal AlignmentTibialis Anterior Gravity-10
-8
-6
-4
-2
0
-10
-8
-6
-4
-2
0
-10
-8
-6
-4
-2
0
-10
-8
-6
-4
-2
0
-10
-8
-6
-4
-2
0
Acc
eler
atio
n (m
/s2 )
Acc
eler
atio
n (m
/s2 )
OTO OHCOTO OHC OTO OHCOTO OHC OTO OHCOTO OHC
OTO OHCOTO OHCOTO OHCOTO OHC
0
1
2
3
4
5
OTO OHCOTO OHC
Figure 3.6: Contributions to mass center accelerations from the muscles providing the largestmagnitude accelerations upward and downward and from gravity. Accelerations are shown for single-limb stance from opposite toe-off (OTO) to opposite heel contact (OHC). The vectors represent theaverage up/down and forward/backward acceleration of the mass center at each 5% of single-limbstance for all subjects. The magnitude of the accelerations in the forward/backward directions has thesame scale as the up/down accelerations shown on the vertical-axis. Skeletal alignment was calculatedby subtracting the accelerations due to muscles from the accelerations due to the ground reaction force.

60
Although the muscles that contributed to the vertical acceleration of the mass
center were similar in crouch gait and unimpaired gait, the profile of the accelerations
differed between the two groups (Figure 3.6). Accelerations of the mass center
generated by muscles during unimpaired gait tended to modulate substantially over the
period of single-limb stance, whereas the stance-limb muscles provided more constant
contributions to mass center accelerations throughout single-limb stance in crouch
gait.
The largest contributors to forward progression during the single-limb stance
phase of crouch gait were the bi-articular hamstrings, gluteus medius, and gluteus
maximus. The gastrocnemius, rectus femoris, vastus, iliopsoas, and hip adductors
slowed forward progression. In contrast, during unimpaired gait, the vasti and soleus
slowed forward progression during early single-limb stance while the gastrocnemius
accelerated the mass center forward in late single-limb stance. The contributions of all
stance-limb muscles to joint and mass center accelerations are provided in Appendix
A.2.
3.4 DISCUSSION
In this study we created the first muscle-actuated simulations of subjects with
crouch gait, which provide insight into how individual muscles contribute to joint
angular accelerations and mass center accelerations during single-limb stance.
Analysis of these simulations indicates that crouch gait is characterized by larger
muscle forces than unimpaired gait to support body weight and propel the body

61
forward throughout single-limb stance. These larger forces were necessary to support
the body in part due to the fact that the skeleton provided less body weight support in
crouch gait, as well as the reduced capacity of muscles to extend the joints (Hicks et
al., 2008) in a crouched posture.
Subjects with crouch gait utilized the same muscle groups to support the body
as unimpaired gait; however, they employed a different support strategy during single-
limb stance. Supporting the body in unimpaired gait requires precise orchestration of
muscle activations, with dramatic modulation of muscle activity throughout single-
limb stance. In contrast, during crouch gait, the support muscles were active
throughout single-limb stance and generated relatively constant accelerations of the
mass center. Subjects with crouch gait also used a different strategy to move the mass
center forward during single-limb stance, relying more on proximal muscles than the
unimpaired subjects.
These different strategies for support and progression during single-limb stance
may underlie why some individuals with cerebral palsy adopt a crouch gait. Given the
excessive muscle activity common in these subjects, they may adopt a support strategy
where muscles are activated consistently throughout single-limb stance. Driving
forward progression with more proximal muscles may also allow subjects to rely less
on controlling distal leg muscles, which are often more severely effected in patients
with cerebral palsy (Carr et al., 1993; Wiley and Damiano, 1998). The use of proximal
muscles for forward progression and walking with slightly flexed knees are also
characteristics of immature gait in unimpaired children (Farmer, 2003). This suggests

62
that some children with cerebral palsy may adopt crouch gait as a feasible gait pattern
given their neurological limitations.
Understanding how individual muscles contribute to joint and mass center
accelerations can help to clarify the effects of treatment. For example, the ankle
plantarflexors are common targets for surgical lengthening in patients with crouch
gait. The gastrocnemius is highly active in stance and has a knee-flexion moment arm,
which might play a role in the excessive knee flexion associated with crouch gait. The
results from our simulations indicate that although the gastrocnemius and soleus both
generate ankle plantarflexion accelerations, they have different effects at the hip and
knee. While the soleus contributes to hip and knee extension throughout single-limb
stance, the gastrocnemius generates flexion accelerations at both joints. Despite these
differences, both muscles accelerate the mass center upward and contribute to support.
The contribution of the gastrocnemius to support indicates that the muscle’s role as an
extensor of the ankle is more significant to the acceleration of the mass center than its
role as a flexor of the hip and knee.
Our subject-specific simulations of crouch gait demonstrate that the soleus is
an important crouch-countering muscle. The soleus not only extends all three joints,
but provides the largest contribution to body weight support, and thus should not be
weakened in this patient population. Furthermore, our results suggest that weakening
the gastrocnemius could compromise a patient’s ability to support his or her body
weight and may lead to excessive dorsiflexion. While lengthening the gastrocnemius
may reduce hip and knee flexion accelerations by reducing the muscle’s force, a
patient may still walk in a crouched posture after a gastrocnemius lengthening if the

63
soleus and other muscles cannot compensate for the decreased contribution to support
from gastrocnemius. These possible negative effects of weakening the gastrocnemius
agree with studies that predicted decreased active moment-generating capacity after
lengthening the gastrocnemius (Delp et al., 1995) and that demonstrated increased
knee flexion after decreasing gastrocnemius activity (Sutherland et al., 1980).
Testing the accuracy of muscle forces estimated from dynamic simulations is
one of the challenges in creating subject-specific simulations. The simulations tracked
the experimental kinematics and joint moments closely, but we observed some
differences between EMG patterns and simulated activations. Given that maximum
voluntary contractions were not available from the study subjects, we could not
directly compare the magnitude of the EMG with the estimated activations. Even if the
magnitude of a muscle’s force changes, the direction of its acceleration (e.g.,
flexion/extension) would be the same since, according to the equations of motion,
direction is determined by the inertial properties of the model, muscle paths, and
posture of the model. We tested the impact of constraining activations to better match
the shape and normalized magnitude of the EMG and found that resulting alterations
in muscle activations did not impact the conclusions of the study.
Previous investigations have tested the induced acceleration analysis technique
used in this study by comparing estimated accelerations to accelerations produced
when individual muscles are electrically stimulated (Stewart et al., 2007; Hernandez et
al., 2008; Stewart et al., 2008; Hunter et al., 2009). These studies have shown that
stimulating a muscle produces accelerations in the same direction as predicted by the
induced acceleration analysis. Future studies that use electrical stimulation to examine

64
the accelerations generated by individual muscles during crouch gait could assist in
further testing the results presented here.
These simulations were generated for individuals who walked flat-footed in a
mild crouch gait. The results of this study may not be extensible to other crouch gait
populations, such as patients with equinus, excessive dorsiflexion, or more severe
knee flexion. Additionally, this study examined single-limb stance and was not able to
explore double support due to a lack of force plate data. However, single-limb stance
is clinically important since an inability to support the mass center during this period
may contribute to crouch gait. Future studies examining double support would provide
valuable information about propulsion and the transition from stance to swing.
The muscle-actuated dynamic simulations generated in this study provide
insights into the support and progression strategies used in crouch gait. The
differences between crouch and unimpaired gait revealed that individuals who walk in
a crouch gait utilize similar muscles to support the mass center but different muscles
to propel the mass center forward during single-limb stance. The results of this study
can be used to identify muscles that are used to support the mass center during crouch
gait for interventions such as strength training, and to inform surgical decision-
making. Although we can measure muscle activity and kinematics during gait,
simulation provides a tool to quantify how the activity of individual muscles
contribute to movement and can lead to a deeper understanding of the biomechanics
underlying crouch gait.

65
CHAPTER 4
HOW DO MUSCLE CONTRIBUTIONS TO SUPPORT AND PROGRESSION CHANGE WITH CROUCH SEVERITY?
Manuscript in review
Katherine M. Steele Ajay Seth Jennifer L. Hicks Michael H. Schwartz Scott L. Delp

66
ABSTRACT
The goals of this study were to determine if the muscle contributions to vertical
and fore-aft acceleration of the mass center differ between crouch gait and unimpaired
gait and if these muscle contributions change with crouch severity. Examining muscle
contributions to mass center acceleration provides insight into the roles of individual
muscles during gait and can provide guidance for treatment planning. We calculated
vertical and fore-aft accelerations using musculoskeletal simulations of typically-
developing children and children with cerebral palsy and crouch gait. Analysis of
these simulations revealed that during unimpaired gait the quadriceps produce large
upward and backward accelerations during early stance, whereas the ankle
plantarflexors produce large upward and forward accelerations later in stance. In
contrast, during crouch gait, the quadriceps and ankle plantarflexors produce large,
opposing fore-aft accelerations throughout stance. The quadriceps force required to
accelerate the mass center upward was significantly larger in crouch gait than in
unimpaired gait and increased with crouch severity. The gluteus medius accelerated
the mass center upward during mid stance in unimpaired gait; however, during crouch
gait the upward acceleration produced by the gluteus medius was significantly
reduced. During unimpaired gait the quadriceps and ankle plantarflexors accelerate the
mass center at different times, efficiently modulating fore-aft accelerations. However,
during crouch gait, the quadriceps and ankle plantarflexors produce fore-aft
accelerations at the same time and the opposing fore-aft accelerations generated by
these muscles contributes to the inefficiency of crouch gait.

67
4.1 INTRODUCTION
Many individuals with cerebral palsy walk in a crouch gait pattern
characterized by excess hip and knee flexion (Wren et al., 2005). Walking in a
crouched posture can lead to joint pain (Jahnsen et al., 2004) and bone deformities
(Graham and Selber, 2003) and is inefficient (Rose et al., 1989; Waters and Mulroy,
1999). Understanding how muscles accelerate the mass center during crouch gait may
provide insight about the underlying mechanics and inefficiencies associated with this
gait pattern.
Previous studies have documented how muscles accelerate the mass center
during unimpaired gait (Neptune et al., 2001; Anderson and Pandy, 2003; Liu et al.,
2008) and have shown that the same muscles that accelerate the mass center upward
also modulate fore-aft acceleration (Liu et al., 2006). Examining muscle contributions
to mass center acceleration can provide insight into the role of individual muscles and
the control strategy used during gait. During unimpaired gait, the vasti and gluteus
maximus accelerate the mass center upward and backward in early stance, the gluteus
medius accelerates the mass center upward in mid stance, and the ankle plantarflexors
accelerate the mass center upward and forward in late stance (Neptune et al., 2001;
Anderson and Pandy, 2003; Liu et al., 2008). This coordinated muscle activity uses
different muscle groups at different periods of stance to efficiently modulate vertical
and fore-aft mass center acceleration.
How muscles modulate vertical and fore-aft accelerations of the mass center
during crouch gait and how these accelerations change with crouch severity is not well
understood. Previous work has shown that similar muscles accelerate the mass center

68
upward during the single-limb stance phase of both mild crouch gait and unimpaired
gait (Steele et al., 2010). However, the role of muscles during the double support
phase, when fore-aft accelerations are largest, is not known for crouch gait. The ability
of muscles such as the gluteus medius and soleus to extend the hip and knee (Hicks et
al., 2008) and accelerate the mass center upward (Correa et al., 2012) has been shown
to decrease in a crouched posture; however, the effect of crouch severity on muscle
contributions to mass center acceleration has not been investigated. Alterations in the
ability of muscles to generate vertical and fore-aft accelerations of the mass center
may change the strategy used to accelerate the mass center during crouch gait and
contribute to the inefficiency of this gait pattern.
The goals of this study were to determine whether: (1) the magnitude and
timing of muscle contributions to vertical and fore-aft accelerations differ between
crouch gait and unimpaired gait, and (2) the muscle contributions to vertical and fore-
aft accelerations change with crouch severity. To calculate muscle contributions to
mass center accelerations we created three-dimensional musculoskeletal simulations
of gait for typically-developing children and children with cerebral palsy and varying
degrees of crouch gait (Figure 4.1). Examining how individual muscles contribute to
vertical and fore-aft accelerations can elucidate the mechanics of crouch gait and
inform treatment strategies.

69
4.2 METHODS
Nine children with cerebral palsy were selected from a database of subjects
who had undergone motion analysis at Gillette Children’s Specialty Healthcare. The
selection criteria for the subjects included: (1) a diagnosis of spastic diplegic cerebral
palsy, (2) a minimum knee flexion angle during stance greater than 15°, and (3) a
tibial and femoral torsion deformity less than 30° (Hicks et al., 2007). We also
required that the subjects did not use an assistive device during the motion analysis
and had at least two consecutive force plate strikes. Nine subjects with crouch gait
were divided into three groups based on minimum knee flexion angle during stance:
15 - 30° knee flexion was defined as mild crouch gait, 30 - 50° was defined as
moderate crouch gait, and 50° or larger was defined as severe crouch gait (Table 4.1).
Figure 4.1: Musculoskeletal model of an individual with cerebral palsy and crouch gait. Vertical and fore-aft accelerations of the mass center were calculated by analyzing muscle-driven simulations.

70
Table 4.1: Subject characteristics (average ± standard deviation) Age
(years) Height (cm)
Weight (kg)
KFA* (deg)
Unimpaired 10 ± 3 144 ± 16 36 ± 9 -2 ± 4 Mild Crouch 9 ± 1 124 ± 10 24 ± 4 18 ± 2 Moderate Crouch 11 ± 2 136 ± 6 43 ± 31 34 ± 2 Severe Crouch 14 ± 2 157 ± 12 41 ± 8 64 ± 20 * KFA: Minimum knee flexion angle during stance
The typically-developing children were selected from a group of subjects who
also visited Gillette Children’s Specialty Healthcare for motion analysis and whose
gait has been previously simulated (Liu et al., 2008). Previous studies demonstrated
consistent contributions to vertical and fore-aft accelerations during gait in typically-
developing children; thus, we chose three subjects with an age range similar to the
subjects with crouch gait (Table 4.1).
Motion analysis data was collected using a 12-camera system (Vicon Motion
Systems, Lake Forest, CA) and a standard marker measurement protocol (Davis et al.,
1991). Ground reaction forces were measured with four force plates (AMTI,
Watertown, MA). All subjects walked barefoot at their self-selected speed. Surface
electromyography (EMG) was recorded from the rectus femoris, hamstrings,
gastrocnemius, and anterior tibialis (Motion Laboratory Systems, Baton Rouge, LA)
for nine of the subjects. The nine subjects who had EMG data available included three
typically-developing subjects, three mild crouch gait subjects, one moderate crouch
gait subject, and two severe crouch gait subjects. The EMG signals were sampled at
1080 Hz, band-pass filtered between 20 and 400 Hz, rectified, and low-pass filtered at
10 Hz. The magnitude of the EMG signal was normalized for each muscle group from
zero to one based on the minimum and maximum values observed during the motion

71
analysis. Since EMG was not available for all subjects, we averaged the processed
EMG signals for each group of subjects for comparison to simulated muscle
activations.
To create dynamic musculoskeletal simulations of gait, we used a
musculoskeletal model with 19 degrees of freedom and 92 musculotendon actuators
(lower extremities from Delp et al., 1990 and torso from Anderson and Pandy, 1999).
The degrees of freedom in the model included three translations and three rotations of
the pelvis, a ball-and-socket joint between the pelvis and the torso located at the third
lumbar vertebrae, ball-and-socket joints at each hip, a custom joint with coupled
translations and rotations at each knee, and a revolute joint at each ankle. This model
has previously been used to model typically-developing children (Liu et al., 2006; Liu
et al., 2008) and children with cerebral palsy (Hicks et al., 2008; Reinbolt et al., 2008;
Steele et al., 2010). The model was scaled according to anthropometric measurements
for each subject using OpenSim (Delp et al., 2007). We scaled the maximum isometric
force of all muscles by height-squared (Jaric et al., 2002).
Inverse kinematics, which minimizes the difference between experimental
marker trajectories and markers placed on the model, was used to calculate joint
angles (Figure 4.2). Joint moments were calculated for each subject using inverse
dynamics (Figure 4.2).

72
Figure 4.2: Average hip, knee, and ankle flexion angles and moments during unimpaired gait and mild,moderate, and severe crouch gait. The joint moments are normalized by body mass (kg).

73
A dynamic simulation of one gait cycle was generated for each subject. The
residual reduction algorithm (RRA) was used to reduce residuals at the pelvis (Delp et
al., 2007). Residuals are non-physiological forces and moments applied at the pelvis
that balance dynamic inconsistencies resulting from experimental errors and modeling
assumptions. RRA reduced these residuals by making small changes to measurements
that may have experimental error including the position of the torso mass center
(changes were less than 2 cm in magnitude) and the kinematics (changes were less
than 2° for all joint angles). Using the adjusted model and kinematics determined from
RRA, the computed muscle control algorithm (CMC) was used to estimate the muscle
forces required to track each subject’s kinematics (Thelen et al., 2003; Thelen and
Anderson, 2006). At each time step, CMC determines the distribution of muscle
activations, such that model accelerations match the experimental accelerations for all
degrees of freedom. The algorithm accounts for muscle activation and contraction
dynamics, which includes the muscle force-length-velocity relationship. The
distribution of muscle activations was determined by minimizing the sum of muscle
activations squared at each time step. The estimated muscle activations from CMC
were qualitatively compared to the average EMG signal for each gait pattern;
constraints on muscle excitations were used when the simulated muscle activity was
inconsistent with the EMG signals.
An induced acceleration analysis was used to compute the contributions of
individual muscles to vertical and fore-aft mass center accelerations (Zajac, 1989;
Riley and Kerrigan, 1999; Anderson and Pandy, 2003; Hamner et al., 2010) at each
time point of a subject’s gait simulation. This analysis solves the model’s equations of

74
motion, including foot-floor contact constraint equations, to determine the
contributions of gravity, velocity, and each muscle force to the mass center
acceleration. The contact constraint equations used in this analysis enforce a rolling
without slipping constraint to model the foot-floor interaction (Hamner et al., 2010).
The musculoskeletal simulations recreated the dynamics of gait for the
typically-developing children and children with cerebral palsy. The average residual
forces and moments applied at the mass center of the pelvis were 9.7 N and 16.5 Nm,
less than 10% of body weight and body weight*height, respectively, for all subjects.
The on-off timing and magnitude of the simulated activations and electromyography
were qualitatively similar (Figure 4.3); however, there were some deviations, such as
decreased quadriceps activity during early swing of unimpaired gait and increased
gastrocnemius activity during swing of severe crouch gait. These differences had
minimal effects on muscle contributions to vertical and fore-aft accelerations of the
mass center, since these accelerations are generated predominately during stance.
To determine if the muscle contributions to vertical and fore-aft accelerations
differed between unimpaired gait and crouch gait, we performed a student’s t-test with
a significance level of 0.05. To determine if contributions to vertical and fore-aft
accelerations changed with crouch severity we used a one-way ANOVA to compare
mild, moderate, and severe crouch gait with a significance level of 0.05. We used two
methods to examine relative timing of muscle contributions to mass center
accelerations. The first method, a covariance analysis, examined the covariance of the
contributions to fore-aft accelerations of major muscle groups over the gait cycle to
determine if they differed between unimpaired gait and crouch gait (using a student’s

75
t-test) or with crouch severity (using a one-way ANOVA). The second method was to
calculate the area under the fore-aft acceleration versus gait cycle curves for major
muscle groups to determine if they differed between unimpaired gait and crouch gait
(using the student’s t-test) or with crouch severity (using a one-way ANOVA).
Figure 4.3: Average ± 1 standard deviation of the EMG signal of each group (gray) and estimated muscleactivations for each subject (black lines) from the quadriceps, hamstrings, gastrocnemius, and anteriortibialis during unimpaired gait and mild, moderate, and severe crouch gait. Only one individual withmoderate crouch gait had EMG, thus we took the average of multiple gait cycles for comparison to thegroup. The magnitude of the EMG and activations were normalized from 0 to 1 based upon the minimumand maximum values during the gait cycle.

76
4.3 RESULTS
The vasti (p = 0.03) and rectus femoris (p = 0.03) produced greater backward
acceleration of the mass center and the gastrocnemius (p = 0.02) and soleus (p = 0.05)
produced greater forward acceleration of the mass center during crouch gait than
unimpaired gait (Figure 4.4A). The forward acceleration produced by the soleus
increased with crouch severity (p = 0.001). In contrast, the fore-aft accelerations
produced by the gluteus medius (p < 0.001) and iliopsoas (p = 0.02) were significantly
smaller in crouch gait than in unimpaired gait.
The downward acceleration of the mass center from gravity was greater (p =
0.001) during crouch gait than unimpaired gait (Figure 4.4B). In the erect posture of
unimpaired gait, a larger portion of body weight is supported by skeletal alignment
than in a crouched posture and, thus, the acceleration of the mass center due to gravity
Figure 4.4: The average (A) fore-aft and (B) vertical accelerations of the mass center during stanceproduced by each muscle and (C) the average muscle force during stance normalized by body weight(BW). Error bars are ± 1 standard error. A ‘*’ indicates a significant difference (p < 0.05) in the student’st-test comparing unimpaired gait and crouch gait. An arrow indicates a significant change with crouchseverity (p < 0.05) from a one-way ANOVA comparing mild, moderate, and severe crouch gait.

77
is reduced. The contribution of the tibialis anterior to downward acceleration was
greater during crouch gait than unimpaired gait; however, muscle contributions to
downward acceleration of the mass center were small relative to gravity. The vasti,
gastrocnemius, and soleus produced the largest upward accelerations of the mass
center during crouch gait and unimpaired gait. The upward acceleration produced by
the gluteus medius was significantly less during crouch gait than unimpaired gait. The
upward acceleration produced by the gastrocnemius decreased with crouch severity (p
= 0.02).
The forces produced by the vasti (p = 0.04) and rectus femoris (p = 0.01) were
significantly greater in crouch gait than in unimpaired gait, and vasti force increased
(p = 0.005) with crouch severity (Figure 4.4C). The change in vasti force was larger
than the change in upward and backward accelerations produced by the vasti because
of a diminished capacity of the vasti to accelerate the mass center in a crouch posture
(Figure 4.5). For example, vasti force during severe crouch gait increased by 340%
compared to unimpaired gait, but the upward acceleration produced by the vasti only
increased by 184% because the upward acceleration produced per newton of muscle
force of the vasti decreased by 54% in severe crouch gait.
The relative timing and magnitude of the fore-aft accelerations generated by
the vasti and gastrocnemius differed between crouch gait and unimpaired gait, as
indicated by changes in the covariance and area under the fore-aft acceleration curves
(Figure 4.6). In unimpaired gait, the vasti accelerated the mass center upward and
backward during early stance and the ankle plantarflexors accelerated the mass center
upward and forward during late stance. The covariance of the fore-aft accelerations

78
generated by the vasti and gastrocnemius during unimpaired gait was close to zero
(-0.08 ± 0.03), indicating that these muscles were active at different times of the gait
cycle. During crouch gait, the vasti and ankle plantarflexors both contributed to fore-
aft accelerations throughout stance, resulting in large, opposing fore-aft accelerations.
The covariance of the fore-aft accelerations generated by the vasti and gastrocnemius
was -0.71 ± 0.14 during crouch gait, significantly different than unimpaired gait (p =
0.03), indicating that these muscles were active at similar times and accelerated the
mass center in opposite directions. Additionally, the areas under the fore-aft
acceleration curves of the vasti (p = 0.01) and gastrocnemius (p = 0.02) were
significantly greater in crouch gait than in unimpaired gait due to these muscles’
sustained contributions to fore-aft accelerations during crouch gait.
Figure 4.5: The average (A) fore-aft and (B) verticalaccelerations produced per 1 newton of muscle force duringstance of each muscle. Error bars are ± 1 standard error. A ‘*’indicates a significant difference (p < 0.05) in the student’s t-test comparing unimpaired gait and crouch gait. An arrowindicates a significant change with crouch severity (p < 0.05)from a one-way ANOVA comparing mild, moderate, andsevere crouch gait.

79
Figure 4.6: The fore-aft accelerations of the mass center produced by the vasti (gray line) andgastrocnemius (black line) during stance. The gray area shows the experimentally measured accelerationof the mass center (fore-aft ground reaction force normalized by body mass).

80
4.4 DISCUSSION
As in unimpaired gait, two muscle groups, the quadriceps and ankle
plantarflexors, were largely responsible for accelerating the mass center upward and
modulating fore-aft acceleration during crouch gait. However, unlike unimpaired gait,
these muscles contributed to mass center accelerations throughout stance and
produced large, opposing fore-aft accelerations. During crouch gait, the ankle
plantarflexors accelerated the mass center upward and forward while the vasti
accelerated the mass center upward and backward throughout stance. The coordination
of quadriceps and ankle plantarflexor activity during unimpaired gait provides an
efficient strategy (Liu et al., 2006) which also allows for modulation of speed by
increasing or decreasing quadriceps and plantarflexor muscle force proportionally
across the gait cycle (Liu et al., 2008). This system is compromised during crouch
gait, and muscles are required to make more sustained contributions to vertical and
fore-aft accelerations. These sustained contributions contribute to the inefficiency of
crouch gait and require individuals with crouch gait to adopt a different strategy for
speed modulation.
A crouched posture increases the demand on muscles to accelerate the mass
center upward due to a decrease in skeletal support and an increase in the knee
extensor moment. The quadriceps and ankle plantarflexors produce the greatest
upward acceleration of the mass center during crouch gait, but the gluteus medius’
ability to accelerate the mass center upward is significantly reduced compared to
unimpaired gait (Correa et al., 2012). During unimpaired gait, the gluteus medius
accelerates the mass center upward in mid stance during the transition from quadriceps

81
to ankle plantarflexors activity. During crouch gait, the gluteus medius contribution to
upward acceleration is reduced and a different strategy is needed to support the mass
center in mid stance. Furthermore, the upward acceleration produced per newton of
muscle force decreases with crouch severity for both the quadriceps and ankle
plantarflexors (Hicks et al., 2008) and other muscles may need to be recruited to
accelerate the mass center upward. Previous experimental studies have also reported
increased quadriceps demand (Perry et al., 1975; Hsu et al., 1993) and prolonged ankle
plantarflexor activity during crouch gait (Thomas et al., 1996).
Understanding how muscles contribute to vertical and fore-aft accelerations
can assist in evaluating treatment options. Demand on the vasti and rectus femoris was
greater during crouch gait and may contribute to fatigue. Strength training or other
programs that improve the endurance of these muscles may improve the overall
endurance of individuals with crouch gait. The ankle plantarflexors were also critical
muscles for accelerating the mass center upward and forward during crouch gait and
may be targets for strength training programs. Engsberg et al. (2006) reported an
improvement in knee flexion during stance after strengthening the ankle
plantarflexors. Similarly, ankle foot orthoses may assist the ankle plantarflexors and
improve the efficiency of crouch gait (Lucareli et al., 2007; Rogozinski et al., 2009).
From a surgical perspective, weakening or reducing the force-generating capacity of
the gastrocnemius or soleus by musculotendon lengthening, neuromuscular toxins, or
other procedures could reduce an individual’s ability to accelerate their mass center
upward or forward.

82
Simulation enables analysis of the accelerations produced by muscles;
however, there are limitations to these methods. The models used in this study were
scaled from adult models and may not reflect bone deformities or altered muscle
physiology of individuals with cerebral palsy. We excluded subjects with significant
bone deformities. However, measurements of how muscle physiology changes in
individuals with cerebral palsy are needed to incorporate the effects of contracture,
spasticity, and other pathologies. These changes in muscle physiology would not
affect the direction of the vertical or fore-aft accelerations produced by each muscle,
but could affect the relative magnitude of force produced by different muscles. To
estimate muscle forces, we minimized activation squared and compared estimated
activations to EMG. EMG data was available from a few muscles in a subset of the
subjects and, although the estimated activations were similar to EMG during stance
when muscles predominately contribute to mass center accelerations, the EMG data
was noisy and varied between subjects. EMG from more muscle groups and analysis
of other minimization criteria could improve simulations of individuals with cerebral
palsy. This study also had a limited number of subjects and may not have had the
power to detect some differences in muscle contributions to vertical and fore-aft
accelerations. We have made the simulations included in this study freely available
on-line for other researchers to evaluate and use for future research
(https://simtk.org/home/crouchgait).
By creating musculoskeletal simulations of individuals with cerebral palsy and
crouch gait, we have determined that a different strategy is used to accelerate the mass
center during crouch gait. The quadriceps and ankle plantarflexors are the primary

83
muscle groups that accelerate the mass center upward; however, sustained activity of
these muscles during stance produces large, opposing fore-aft accelerations – like
driving with your parking brake on. Future studies that examine the metabolic costs of
crouch gait and explore why individuals adopt a crouch gait pattern will be critical for
improving treatment and quality of life. Examining how individual muscles contribute
to gait using musculoskeletal simulation provides a foundation for these future studies
and a basis for clinicians and researchers to understand the underlying mechanics of
gait pathologies.

84

85
CHAPTER 5
HOW DOES TIBIOFEMORAL CONTACT FORCE CHANGE DURING CROUCH GAIT?
Gait & Posture (2012), vol. 35, pp. 556-60
Katherine M. Steele Matt DeMers Michael H. Schwartz Scott L. Delp

86
ABSTRACT
Crouch gait, a common walking pattern in individuals with cerebral palsy, is
characterized by excessive flexion of the hip and knee. Many subjects with crouch gait
experience knee pain, perhaps because of elevated muscle forces and joint loading.
The goal of this study was to examine how muscle forces and compressive
tibiofemoral force change with the increasing knee flexion associated with crouch gait.
Muscle forces and tibiofemoral force were estimated for three unimpaired children and
nine children with cerebral palsy who walked with varying degrees of knee flexion.
We scaled a generic musculoskeletal model to each subject and used the model to
estimate muscle forces and compressive tibiofemoral forces during walking. Mild
crouch gait (minimum knee flexion 20-35°) produced a peak compressive tibiofemoral
force similar to unimpaired walking; however, severe crouch gait (minimum knee
flexion > 50°) increased the peak force to greater than 6 times body weight, more than
double the load during unimpaired gait. This increase in compressive tibiofemoral
force was due primarily to increases in quadriceps force during crouch gait, which
increased quadratically with average stance phase knee flexion (i.e., crouch severity).
Increased quadriceps force contributes to larger tibiofemoral and patellofemoral
loading which may contribute to knee pain in individuals with crouch gait.

87
5.1 INTRODUCTION
Crouch gait is a common pathological walking pattern adopted by individuals
with cerebral palsy that is characterized by excessive hip and knee flexion. Walking in
a crouched posture is inefficient (Rose et al., 1989; Waters and Mulroy, 1999) and can
lead to joint pain and compromise an individual’s walking ability (Opheim et al.,
2009). Surgical and therapeutic treatments for crouch gait aim to produce a more
upright posture to improve walking efficiency and prevent joint pain and deterioration.
Altered loads on the knee can have adverse effects on joint health. Cartilage
and bone growth and maintenance depend on the loads experienced during daily life
(Carter and Wong, 1988; Wong and Carter, 2003), and abnormal loading can lead to
joint pain, cartilage degeneration (Eckstein et al., 2002), and the formation of bone
deformities (Graham and Selber, 2003). Joint pain can be a significant contributor to
walking deterioration in adults with cerebral palsy. Jahnsen et al. (2004) found that
41% of adults with diplegic cerebral palsy reported significant knee pain.
To develop successful treatment strategies for crouch gait, surgeons and
therapists need to understand how joint loads change with increasing knee flexion
during crouch gait and how joint loads may change with altered knee flexion.
Treatments are aimed at reducing the excessive knee flexion associated with crouch
gait, but it is unclear if changes in knee flexion will alter joint loads. Quantifying the
relationship between knee flexion, muscle forces, and the compressive force on the
tibia during gait could help clinicians determine if a more upright posture could reduce
the risks caused by altered joint loading.

88
Perry et al., (1975) examined knee forces in a static crouched posture using a
cadaver model and reported increasing compressive tibiofemoral force with increasing
knee flexion. In dynamic activities, such as walking, we expect larger joint forces than
in a static posture due to the additional muscle forces required to support the body
weight during movement and propel the body forward (Liu et al., 2008). Compressive
tibiofemoral forces during unimpaired walking have been reported in the range of 2-3
times body weight (Shelburne et al., 2005; D'Lima et al., 2006; Mundermann et al.,
2008; Kutzner et al., 2010). During crouch gait, muscle forces in the stance-limb are
higher than during unimpaired walking (Steele et al., 2010). Since muscle forces are
the primary contributors to joint loading (Inman, 1947; Sasaki and Neptune, 2010), we
expect that compressive tibiofemoral forces are higher during crouch gait, yet the
relationship between crouch gait severity and the compressive tibiofemoral force
remains unknown.
The purpose of this study was to estimate the magnitude of the compressive
tibiofemoral force during crouch gait and examine how this force changes with crouch
severity. To achieve this goal we estimated the muscles forces and the compressive
force on the tibia in unimpaired children and children with cerebral palsy who walked
in varying degrees of crouch severity. We used a freely-available biomechanics
software package, OpenSim (Delp et al., 2007), to scale a musculoskeletal model to
each individual and estimate muscle joint loads based upon each individual’s gait
dynamics.

89
5.2 METHODS
5.2.1 SUBJECTS
The subjects for this study were selected from a database of patients treated at
Gillette Children’s Specialty Healthcare (St. Paul, MN; Table 5.1). Nine subjects with
spastic diplegic cerebral palsy were selected to cover a broad range of crouch severity
and were divided evenly into three groups: mild crouch gait (minimum knee flexion
angle of 20-35º), moderate crouch gait (minimum knee flexion angle of 35-50º), and
severe crouch gait (minimum knee flexion angle greater than 50º). All subjects walked
with excess knee and hip flexion and had at least 5º of ankle dorsiflexion during
stance. We excluded subjects that had greater than 30º of femoral or tibial torsion,
which can affect muscle moment arms and the ability of muscles to generate
accelerations (Hicks et al., 2007).
Table 5.1: Subject characteristics (average ± standard deviation) N Age
(yrs) Height (cm)
Weight (kg)
Speed/Height (s-1)
Minimum KFA* (deg)
Unimpaired 3 10.3 ± 3.4 145 ± 16 36.3 ± 8.8 0.79 ± 0.1 1.7 ± 5.5 Mild Crouch 3 8.8 ± 0.8 123 ± 7 24.2 ± 3.6 0.67 ± 0.1 19.1 ± 3.8 Moderate Crouch 3 9.2 ± 2.9 123 ± 15 43.1 ± 37 0.63 ± 0.1 36.1 ± 4.0 Severe Crouch 3 14.0 ±2.3 158 ± 12 40.1 ± 6.8 0.61 ± 0.1 58.6 ± 5.6 *KFA: knee flexion angle during walking
Three unimpaired subjects were chosen who were representative of the age and
stature of the subjects with cerebral palsy. Additionally, a subject with an
instrumented total knee replacement (TKR, age: 80 yrs, weight: 64 kg, walking
speed/height: 0.74 s-1) was included to provide experimental measurements of the
compressive tibiofemoral force for comparison with forces estimated from the
musculoskeletal model. This subject was not included in subsequent comparisons

90
between unimpaired gait and crouch gait due to differences in age and stature in
relation to the other subjects.
5.2.2 MOTION ANALYSIS
Motion analysis data was collected at Gillette Children’s Specialty Healthcare
(St. Paul, MN) using a 12-camera system (Vicon Motion Systems, Lake Forest, CA),
four force plates (AMTI, Watertown, MA), and a standard marker protocol (Davis et
al., 1991). Ground reaction forces and moments were sampled at 1080 Hz and low-
pass filtered at 20 Hz. Electromyography (EMG) was collected for six of the crouch
gait subjects from the quadriceps, hamstrings, and gastrocnemius (Motion Laboratory
Systems, Baton Rouge, LA). The EMG data was sampled at 1080 Hz, band-pass
filtered between 20 and 400 Hz, rectified, and low-pass filtered at 10 Hz. All subjects
walked at their self-selected speed and achieved two consecutive force plate strikes
during which only one foot contacted each force plate. The motion analysis data for
the subject with the instrumented TKR was obtained from www.simtk.org where it is
freely available for researchers (Zhao et al., 2007).
5.2.3 MUSCULOSKELETAL MODELING
A generic musculoskeletal model based upon adult cadaver data (Delp et al.,
1990) with 19 degrees of freedom and 92 musculotendon actuators was scaled to each
subject according to anthropometric measurements. This musculoskeletal model has
been used for studies involving unimpaired children and children with cerebral palsy
(Hicks et al., 2008; Liu et al., 2008; Reinbolt et al., 2008). The degrees of freedom in

91
the musculoskeletal model included six degrees of freedom at the pelvis, a ball-and-
socket joint at the third lumbar vertebra between the pelvis and torso, a ball-and-
socket joint at each hip, a planar joint with coupled translations at each knee
(Yamaguchi and Zajac, 1989), and a revolute joint at each ankle. Joint angles during
walking were calculated by minimizing the error between experimental marker
trajectories and markers placed on the model at locations corresponding to the
experimental markers.
Static optimization was used to calculate the muscle forces required to
reproduce the joint moments of each subject throughout the gait cycle. To distribute
muscle forces, static optimization was used to minimize the objective function:
1
where N is the number of muscles in the model, a is the activation level (between zero
and one) of each muscle, and c is an integer weighting constant for each muscle with a
default value of one. The weighting constants were determined by comparing
calculated compressive tibiofemoral force to the experimentally measured force for
the subject with the instrumented TKR, as described below.
The compressive tibiofemoral force was calculated using the joint reaction
analysis in OpenSim. A detailed description of this analysis is provided in Appendix
B.1. Briefly, the tibiofemoral force was calculated as a point load acting on the tibial
plateau using the Newton-Euler equation:
∑ (2)

92
In Equation 2, is the force from the femur on the tibia, [M]tibia is the matrix of
inertial properties of the tibia, is the six dimensional angular and linear
acceleration of the tibia, is the force from the foot on the tibia, and and
are the muscle forces and gravitational forces acting on the tibia. The
compressive tibiofemoral force was calculated as the component of parallel to
the longitudinal axis of the tibia and used for all subsequent analyses.
For the subject with the instrumented TKR, we varied the static optimization
weighting constants for the major muscle groups that cross the knee: the hamstrings,
gastrocnemius, and quadriceps. The hamstrings included independent muscle models
for the semimembranosus, semitendinousus, biceps femoris long head, and biceps
femoris short head. The quadriceps included independent muscle models for the rectus
femoris, the vastus medialis, the vastus intermedius, and the vastus lateralis. The same
weighting constant was applied to all muscles in each group and the results for the
muscles within each group were compared and, if found to be similar, were combined
to facilitate analysis. The weighting constants were given integer values between one
and ten. We performed static optimization for all combinations of integer weighting
constants and calculated the resulting compressive tibiofemoral force. The peak
compressive force was compared to the experimentally measured force, and we
selected the combination of weighting constants that had the minimum average value
and resulted in a difference between the estimated and experimental peak compressive
force of less than 20% body weight. The set of weighting constants that met this
criterion was a weight of three for the hamstrings, seven for the gastrocnemius, and

93
one for the quadriceps. This combination of weighting constants resulted in a root
mean square error of 0.28 times body weight and an average error of 0.02 times body
weight over the gait cycle between the estimated force and the experimental
measurements (Figure 5.1). These weighting constants were then used to perform
static optimization for all other subjects. OpenSim’s joint reaction analysis algorithm
was used to calculate the compressive tibiofemoral force for one representative gait
cycle for each subject.
To evaluate whether muscle activations calculated from static optimization
reflected the subjects’ muscle activity we qualitatively compared the estimated muscle
activations to EMG recordings during stance for the six subjects for whom EMG data
was available (Figure 5.2). EMG and estimated muscle activations indicated that the
quadriceps were active during stance. Hamstring activity decreased during stance in
both the EMG and estimated muscle activations; however, estimated muscle
activations decreased earlier in stance than indicated by EMG for some of the subjects.
For these subjects, increased hamstring activity during stance would have increased
estimates of the compressive tibiofemoral contact force. The gastrocnemius muscle
Figure 5.1: Tibiofemoral contact forces expressed in multiples of body weight (BW) from experimental forces measured using an instrumented total knee replacement (TKR, gray) and estimated with the computermodel (black). The average ± 1 standard deviation is shown from four trials.

94
was active during the majority of stance in both the EMG and estimated muscle
activations.
Figure 5.2: Comparison of EMG(gray, average ± one standarddeviation over all gait cycles) andmuscle activations from staticoptimization (black line) for thesix subjects with crouch gait forwhom EMG data was available.EMG and activations werenormalized from zero to one foreach subject based upon theminimum and maximum valuesover the gait cycle. Note thatsubject “Severe 1” did not haveEMG data from thegastrocnemius.

95
5.3 RESULTS
Compressive tibiofemoral force was higher during moderate and severe crouch
gait than during unimpaired gait (Figure 5.3). Subjects with a mild crouch gait had
similar compressive tibiofemoral forces to subjects with unimpaired gait. The
maximum force during mild crouch gait was 3.2 ± 0.4 times body weight compared to
3.0 ± 0.5 times body weight during unimpaired gait. Maximum force during a
moderate crouch gait was 4.2 ± 1.2 times body weight. During a severe crouch gait
maximum force was 6.5 ± 0.7 times body weight.
Compressive tibiofemoral force during stance exhibited two peaks in
unimpaired and crouch gait. These two peaks in the tibiofemoral force coincided with
the two characteristic peaks of the ground reaction force. The largest tibiofemoral
forces occurred during early and late stance with smaller forces in mid stance and
swing. During unimpaired gait, the primary contributors to compressive tibiofemoral
force were the quadriceps in early stance and the gastrocnemius during late stance.
During crouch gait, the quadriceps were the primary contributors to tibiofemoral force
throughout stance.

96
There was a quadratic relationship between the average knee flexion angle
during stance and the average compressive tibiofemoral force during stance (r2 = 0.97,
Figure 5.4). The relationship is described by:
0.0013 0.06 2.54 (3)
Figure 5.3: (A) Average knee flexion angle,(B) average compressive tibiofemoral force,and (C) average quadriceps force expressed asmultiples of body weight (BW) during onegait cycle for the subjects who walked with anunimpaired gait and mild, moderate, andsevere crouch gait.

97
where Fknee is the average compressive tibiofemoral force during stance, and Ө is the
average knee flexion angle during stance with values from 15 to 70° of flexion.
The increase in average compressive tibiofemoral force during stance with
increasing crouch severity was primarily due to an increase in quadriceps force. The
average quadriceps force during stance also increased quadratically with knee flexion
angle (r2=0.99, Figure 5.4) with the relationship:
0.0011 0.03 0.7 (4)
The average force produced by the hamstrings during stance did not change
with knee flexion; however, the average force of gastrocnemius decreased with crouch
severity. Individuals with crouch gait had smaller ankle plantarflexor moments during
terminal stance.
Figure 5.4: Correlation of average knee flexion angle during stance with average compressive tibiofemoralforce during stance (black circles), average quadriceps force during stance (dark gray squares), averagehamstrings force during stance (light gray triangles), and average gastrocnemius force during stance (blackoutlined diamonds). Tibiofemoral force and average quadriceps force are expressed as multiples of bodyweight (BW). A quadratic relationship described the change in both tibiofemoral force and quadricepsforce with increasing crouch.

98
5.4 DISCUSSION
Individuals who walk in a moderate or severe crouch gait experience
substantially greater compressive tibiofemoral forces than individuals with an
unimpaired gait; however, individuals who walk in a mild crouch gait have similar
compressive tibiofemoral forces to unimpaired gait. The increase in tibiofemoral force
was primarily due to the increase in quadriceps force required to support the body
during crouch gait. There was a quadratic increase in quadriceps force with increasing
knee flexion which is similar to a reported quadratic increase in EMG magnitude in
static, crouch postures (Hsu et al., 1993). The increase in quadriceps force with crouch
severity not only contributes to increased tibiofemoral load but would also increase
patellofemoral load (Dhaher and Kahn, 2002) and may give rise to knee pain in
individuals with cerebral palsy and crouch gait. To reduce the average compressive
tibiofemoral force and quadriceps force during stance to within one standard deviation
of the average during unimpaired gait, individuals with crouch gait need to achieve an
average knee flexion angle less than 25° during stance.
Compressive tibiofemoral force during crouch gait reported here are slightly
higher than those estimated by Perry et al. (1975), who used statically loaded cadavers
in a crouch posture. Perry determined the compressive tibiofemoral force at 30 and
45° of knee flexion to be 2.9 and 3.8 times body weight, respectively, whereas we
found the maximum force during a crouch gait with an average knee flexion angle of
30 and 45° to be 3.3 and 4.1 times body weight. The static cadaver testing
implemented by Perry did not include contributions from the gastrocnemius or
hamstring muscles to compressive tibiofemoral force. The small difference in

99
compressive tibiofemoral force between standing and walking demonstrates that,
although walking requires additional muscle force to propel the body forward (Steele
et al., 2010), the increased quadriceps demand arising from a static crouched posture
accounts for the majority of the increased tibiofemoral force. The tibiofemoral contact
force of the unimpaired children included in this analysis were also similar to
previously reported results (Shelburne et al., 2005; D'Lima et al., 2006; Mundermann
et al., 2008; Kutzner et al., 2010).
Our calculation of compressive tibiofemoral force depends on the accuracy of
estimated muscle activations. The estimated muscle activations showed patterns
similar to EMG such as increased activity of the quadriceps; however, EMG activity
was available for a limited number of muscles in six of the subjects. When muscle
activations differed from the EMG signals the optimization tended to underestimate
muscle activity compared to EMG signals. This suggests that the optimization
functions commonly used for unimpaired walking may not be appropriate for
individuals with cerebral palsy who have altered motor control and muscle
physiology. Muscle over-activity and excess co-contraction are common in individuals
with cerebral palsy. Greater muscle forces due to co-contraction would increase the
estimated tibiofemoral contact forces, suggesting that our calculations of compressive
tibiofemoral force may be low estimates.
We compared our calculated tibiofemoral forces to experimental forces from
an instrumented total knee replacement, but this did not provide a robust evaluation of
knee forces during crouch gait. The total knee replacement data was used to select the
static optimization weighting constants that reduced the error between the estimated

100
and measured compressive tibiofemoral force. Different weighting constants may be
appropriate for younger patients or patients with gait pathology. In this study, the
weighting constants penalized recruitment of the hamstrings and gastrocnemius, which
resulted in the recruitment of other muscles to actuate the hip and ankle without
increasing the compressive load on the tibia. Although the quadriceps are the major
contributors to compressive tibiofemoral force, increasing the quadriceps’ weighting
constant did not reduce the estimated tibiofemoral force since no other muscles could
replace the quadriceps’ function at the knee.
To test the sensitivity of our results to the objective function we evaluated how
estimated tibiofemoral contact force changed with altering the weighting constants and
the power of activation. The quadratic relationship between knee flexion angle and
tibiofemoral contact force and quadriceps force was similar in all tested objective
functions (Figure 5.5). Using a linear objective function resulted in an average
reduction in tibiofemoral contact force during stance of 7% while an objective
function that minimized activation cubed increased tibiofemoral contact force during
stance by 11%. Using weighting constants of one for all muscles also increased the
estimated tibiofemoral contact force during stance by an average of 15% due primarily
to a 10% average increase in gastrocnemius force during stance. Future studies that
measure compressive tibiofemoral force from individuals with instrumented total knee
replacements walking in pathologic gait patterns, such as crouch gait, could provide
further points of comparison for model-based estimates of compressive tibiofemoral
force and help to determine the optimal objective functions.

101
Figure 5.5: Average (A) tibiofemoral contact force, (B) quadriceps force, (C) hamstring force, and (D)gastrocnemius force during stance with the objective function shown in Eqn. 1 and weighting constants,minimizing activation with weighting constants, minimizing activation cubed with weighting constants,and minimizing activation squared with all weighting constants equal to one.

102
This study has demonstrated that walking in a moderate or severe crouch gait
increases the compressive tibiofemoral force, which could be contributing to joint pain
and cartilage degeneration. Surgeries and therapies that produce a more upright
walking posture will reduce forces at the knee and may help moderate the adverse
effects of excessive joint loading.

103
CHAPTER 6
HOW MUCH MUSCLE STRENGTH IS REQUIRED TO WALK IN A CROUCH GAIT?
Publication in review
Katherine M. Steele Marjolein M. van der Krogt Michael H. Schwartz Scott L. Delp

104
ABSTRACT
Muscle weakness is commonly cited as a cause of crouch gait in individuals
with cerebral palsy; however, outcomes after strength training are variable and
mechanisms by which muscle weakness may contribute to crouch gait are unclear.
Understanding how much muscle strength is required to walk in a crouch gait
compared to an unimpaired gait may provide insight into how muscle weakness
contributes to crouch gait and assist in the design of strength training programs. The
goal of this study was to examine how much muscle groups could be weakened before
crouch gait becomes impossible. To investigate this question, we first created muscle-
driven simulations of gait for three typically-developing children and six children with
cerebral palsy who walked with varying degrees of crouch severity. We then simulated
muscle weakness by systematically reducing the maximum isometric force of each
muscle group until the simulation could no longer reproduce each subject’s gait. This
analysis indicated that moderate crouch gait required significantly more knee extensor
strength than unimpaired gait. In contrast, moderate crouch gait required significantly
less hip abductor strength than unimpaired gait, and mild crouch gait required
significantly less ankle plantarflexor strength than unimpaired gait. The reduced
strength required from the hip abductors and ankle plantarflexors during crouch gait
suggests that weakness of these muscle groups may contribute to crouch gait and that
these muscle groups are potential targets for strength training.

105
6.1 INTRODUCTION
Cerebral palsy is caused by a lesion to the brain that occurs at or near the time
of birth and results in impaired movement. It is the most common childhood
movement disorder and affects approximately 3.6 of every 1000 children born in the
United States (Yeargin-Allsopp et al., 2008). Many individuals with cerebral palsy
walk in a crouch gait pattern characterized by excessive flexion of the hip, knee, and
ankle during the stance phase of gait. Walking in a crouch is inefficient and can lead to
joint pain (Jahnsen et al., 2004) and bone deformities (Graham and Selber, 2003).
There are many suggested causes of crouch gait, including contracted
hamstrings, contracted hip flexors, impaired balance, foot deformities, impaired
proprioception, and muscle weakness (Gage, 1990). Muscle weakness can be caused
by various mechanisms such as impaired motor control and reduced physiological
cross-sectional area of muscles. Muscle weakness is common in individuals with
cerebral palsy (Damiano et al., 1995b; Wiley and Damiano, 1998), and strength
training is often incorporated into therapy (Dodd et al., 2002; Pippenger and Scalzitti,
2004; Mockford and Caulton, 2008). Although individuals with cerebral palsy can
increase their muscle strength after completing a strength training program (Damiano
et al., 1995b; Dodd et al., 2002; Mockford and Caulton, 2008), the improvements in
gait after strength training are variable. Previous studies have reported improvements
in knee extension (Damiano et al., 1995a) and functional walking tests after strength
training (Blundell et al., 2003; Dodd et al., 2003); however, other studies have found
no significant change in walking tests (Kerr et al., 2006; Liao et al., 2007) or
deterioration in gait for some subjects (Damiano et al., 2010).

106
A rationale for strength training is that individuals with crouch gait may not
have adequate strength to walk in an upright posture. However, previous studies have
shown that walking in a crouch gait requires a greater knee extensor moment (Hsu et
al., 1993; Lin et al., 2000) and greater total muscle force (Steele et al., 2010) than
walking in an upright gait. Although crouch gait requires larger forces in some
muscles, there may be other muscles that are too weak to achieve an upright gait
pattern. Unimpaired gait has been shown to be most sensitive to weakness of the ankle
plantarflexors, hip abductors, and hip flexors (van der Krogt et al., 2012). Comparing
the amount of muscle strength required during crouch gait to unimpaired gait can
provide insight into how muscle weakness contributes to crouch gait and how strength
training could improve gait.
The aim of this study was to examine how much muscle groups could be
weakened before walking in a crouch gait becomes impossible. We used a
musculoskeletal model in which it was possible to reduce the force-generating
capacity of particular muscle groups to simulate weakness. We created muscle-driven
simulations of unimpaired subjects and subjects with cerebral palsy who walked in
varying degrees of crouch gait. For each subject, we examined how much particular
muscle groups could be weakened before the simulation could no longer reproduce the
subject’s gait pattern. Identifying muscle groups that require less strength to walk in a
crouch gait than unimpaired gait may suggest which muscles may be too weak to walk
in an upright posture and may be targets for strength training programs.

107
6.2 METHODS
Three typically-developing children and six children with spastic diplegic
cerebral palsy (Table 6.1) were selected from a database of subjects who had visited
Gillette Children’s Specialty Healthcare for motion analysis. Three-dimensional
motion analysis data was collected using a 12-camera system (Vicon Motion Systems,
Lake Forest, CA) and a standard marker measurement protocol (Davis et al., 1991).
Ground reaction forces were measured with four force plates (AMTI, Watertown,
MA), sampled at 1080 Hz, and low-pass filtered at 20 Hz. All subjects walked
barefoot at their self-selected speed without walking aids.
Table 6.1: Subject characteristics (average ± standard deviation) N Age
(years) Height (cm)
Weight (kg)
Unimpaired 3 10 ± 3 144 ± 16 36 ± 9 Mild Crouch 3 9 ± 1 124 ± 10 24 ± 4 Moderate Crouch 3 11 ± 2 136 ± 6 43 ± 31
The subjects with cerebral palsy all walked in a crouch gait and had a
minimum knee flexion angle during stance greater than 15° and a maximum ankle
dorsiflexion angle during stance greater than 5°. The crouch subjects were divided
evenly into two groups based upon crouch severity: mild crouch gait (N=3, minimum
knee flexion angle of 15-30°) and moderate crouch gait (N=3, minimum knee flexion
angle of 30-50°).
Muscle-driven simulations were created that represent the gait dynamics of
each subject using OpenSim, a freely available biomechanical simulation package
(Delp et al. (2007), http://opensim.stanford.edu). Using simulation allowed us to

108
selectively weaken particular muscle groups, account for some of the complexities of
the musculoskeletal system, such as the force-length-velocity relationship of muscle,
and examine the compensatory actions from other muscles in response to simulated
muscle weakness. A generic musculoskeletal model (lower extremities from Delp et
al., 1990, and torso from Anderson and Pandy, 1999) with 19 degrees of freedom and
92 musculotendon actuators was scaled to each subject using anthropometric
measurements (Figure 6.1). The degrees of freedom in this model included three
rotations and translations of the pelvis, a ball-and-socket joint between the pelvis and
torso at the third lumbar vertebra, a ball-and-socket joint at each hip, a planar joint
with coupled translations at each knee, and a revolute joint at each ankle. The
maximum isometric forces of the muscles in the model were geometrically scaled by
height-squared of each subject. We scaled muscle strength by height-squared because
muscle strength is proportional to a muscle’s physiological cross-sectional area, which
is correlated with height-squared in adults and children (Schantz et al., 1983; Parker et
al., 1990; Jaric et al., 2002).

109
Joint angles were calculated for one walking trial for each subject by
computing the joint angles that minimize the difference between experimental marker
positions and virtual markers placed on the model (Figure 6.2A). Joint moments were
calculated using inverse dynamics (Figure 6.2B). To determine the motion of the
torso, experimental marker data was available for all of the unimpaired subjects and
three of the six subjects with crouch gait. For the individuals without torso markers,
torso position was set to 20° lumbar flexion, 0° lumbar bending, and 0° lumbar
rotation. To test the effects of torso position, we completed the analysis for the
Figure 6.1: Musculoskeletal models used to create dynamic simulations of gait for individuals that walkedin an unimpaired gait pattern (left) and individuals with cerebral palsy who walked in mild (center) andmoderate (right) crouch gait.

110
unimpaired subjects with and without torso markers and found no significant
differences in the results (Figure 6.3).
Figure 6.2: The average hip, knee, and ankle (A) kinematics and (B) kinetics during unimpaired gait(dotted) and mild (light gray) and moderate (dark gray) crouch gait. Joint moments are normalized by bodymass (kg).

111
The residual reduction algorithm was used to improve the dynamic consistency
of the simulation (Delp et al., 2007). This algorithm makes small changes to
kinematics (< 2°) and the torso mass center location (< 2 cm) to reduce the residual
forces applied to the pelvis. After running the residual reduction algorithm, the
residual forces were less than 10% of body weight and the residual moments were less
than 10% of body weight times height for all subjects. Muscle excitations were
estimated using the computed muscle control (CMC) algorithm, which determines a
set of muscle excitations that recreates the subject’s kinematics (Thelen et al., 2003;
Thelen and Anderson, 2006). At each time step, CMC determines the set of muscle
excitations that produce the forces that generate measured accelerations for all degrees
of freedom taking into account muscle activation dynamics and force-length-velocity
properties. The distribution of muscle excitations among redundant actuators was
determined by minimizing the sum of activations-squared at each time step. Idealized
torque actuators, known as reserve actuators, were included for each degree of
freedom in the model to provide extra torque if the muscles could not generate the
Figure 6.3: Comparison of the required strength for each muscle group of the unimpaired subjects (N=3)when using torso markers for inverse kinematics and without torso markers (average ± 1 standard error).There was no significant difference in the results with or without torso markers.

112
measured accelerations. Reserve actuator torques were used to determine when the
muscles could no longer produce the subject’s motion.
To assess the accuracy of the simulation we compared the simulated
kinematics and kinetics to experimental data. The simulated joint angles reproduced
the joint angles calculated by inverse kinematics with a maximum difference of less
than 2°. Additionally, the sum of the moments generated by the muscle forces at each
degree of freedom reproduced the joint moments computed using the residual
reduction algorithm with an average root mean square error of 1.7 ± 0.9 Nm across all
subjects.
To determine how much particular muscle groups could be weakened, each of
seven muscle groups were sequentially weakened by systematically reducing the
maximum isometric force of each muscle in the group. Table 6.2 lists the muscles in
each group. Each muscle group was weakened in isolation. We reduced the maximum
isometric force until the CMC algorithm could no longer determine a set of muscle
excitations that would recreate the subject’s dynamics with an error less than 2° for all
degrees of freedom and torques from the reserve actuators that were less than 10% of
the maximum joint moment at each degree of freedom. We used the bisection method
(Burden and Faires, 1985) to determine how much the maximum isometric force of
each muscle group could be reduced. This method searches through the space of all
possible values for the maximum isometric force by iteratively taking the middle of an
interval representing the maximum and minimum possible values from previous
iterations until it converges upon the minimum value that could recreate the subject’s

113
dynamics. This point was termed the required muscle strength for each muscle group
and was expressed as a percent of the muscle group’s maximum isometric force.
Table 6.2: Description of muscle groups Name Description Gluteus Maximus Three musculotendon actuators representing the medial, intermediate, and
lateral components of the muscle Hip Abductors Gluteus medius and gluteus minimus each modeled as three musculotendon
actuators representing the anterior, intermediate, and posterior components of the muscle
Iliopsoas Iliacus and psoas each modeled by a single musculotendon actuator Hamstrings Three musculotendon actuators representing the bi-articular hamstrings
including the biceps femoris long head, semimembranosus, and semitendinousus
Quadriceps Four musculotendon actuators representing the rectus femoris, vastus medials, vastus intermedius, and vastus lateralis
Ankle Plantarflexors Three musculotendon actuators representing the soleus and the medial and lateral heads of the gastrocnemius
Ankle Dorsiflexors Musculotendon actuators representing the anterior tibialis, extensor digitorum, extensor hallus longus, and peroneus tertius
Because of the limited number of subjects, we used a protected Fisher’s Least
Significant Difference test to determine if the required muscle strength was different
between unimpaired gait and mild and moderate crouch gait. We first performed a
one-way ANOVA for each muscle group; if the p-value of the one-way ANOVA was
less than 0.1 we then performed a Fisher’s Least Significant Difference test to
determine differences between gait patterns with a significance level of 0.05. We also
performed regression analyses to determine if required muscle strength changed with
crouch severity.
6.3 RESULTS
The strength, or force-generating capacity, required from each muscle group
could be reduced substantially while the model could still produce the dynamics of

114
unimpaired gait and crouch gait (Figure 6.4). This occurs in the simulations because
neither unimpaired gait nor crouch gait requires maximum strength, and other muscles
can compensate for the diminished strength of a particular muscle group. When we
reduced the maximum isometric force of one muscle group, the activation level of that
muscle group increased and other compensatory actions arose from muscles with
similar function (Figure 6.5). For example, the strength required from the gluteus
maximus could be reduced to near zero in the simulations and the dynamics of
unimpaired gait and crouch gait could be maintained. The gluteus maximus represents
about 35% of the hip extension moment generating capacity; thus, when its strength is
reduced, other muscles, such as the gluteus medius and bi-articular hamstrings
increase their activity level.
Figure 6.4: Required strength for each muscle group that was necessary to recreate each subject’s gaitpattern expressed as percent of the maximum isometric force (average ± 1 standard deviation, * p < 0.05from Fisher’s Least Significant Difference test). Crouch gait required more quadriceps strength and lesship abductor and ankle plantarflexor strength than unimpaired gait.

115
Moderate crouch gait required significantly more quadriceps strength than
unimpaired gait and mild crouch gait (Figure 6.4). Furthermore, the quadriceps
strength required increased quadratically with crouch severity (r2=0.75). This trend is
largely due to the greater knee extensor moment required from inverse dynamics
during stance in crouch gait compared to unimpaired gait (see knee extensor moment
in Figure 6.2B).
The hip abductor strength required was significantly less during moderate
crouch gait than unimpaired gait (Figure 6.4) and decreased linearly with crouch
severity (r2= 0.58). The hip abductor moment required from inverse dynamics was
Figure 6.5: Compensatory muscle action when a particular muscle group is weakened, expressed as theaverage change in muscle force over the gait cycle (times body weight, BW). For each muscle group, thechange in force of the weakened muscle group and the change in force of the three muscles with thegreatest change in force are shown (average ± 1 standard error).

116
also reduced in crouch gait compared to unimpaired gait, especially during terminal
stance (see hip abductor moment in Figure 6.2B). The muscles that were weakened in
the simulation included the gluteus medius and the gluteus minumus, which represent
about 70% of the hip abductor moment generating capacity, and few other muscles
can compensate for weakness of these muscles.
The ankle plantarflexor strength required was significantly less during mild
crouch gait than during unimpaired gait (Figure 6.4). The ankle plantarflexor moment
required from inverse dynamics during early and mid stance was larger during crouch
gait; however, the peak plantarflexor moment required in terminal stance was reduced
during crouch gait (see ankle plantarflexor moment in Figure 6.2B).
The ankle dorsiflexor strength required was similar across all gait patterns
(Figure 6.4). No consistent differences in the amount of hamstring or iliopsoas
strength required were identified between unimpaired gait and crouch gait.
6.4 DISCUSSION
Our results indicate that the required knee extensor strength increased with
crouch severity, required hip abductor strength was reduced in moderate crouch gait,
and required ankle plantarflexor strength was reduced in mild crouch. Identifying
which muscle groups require more or less strength during crouch gait than unimpaired
gait can provide insight into how muscle weakness, or a reduced force-generating
capacity, could contribute to crouch gait and provide guidance for strength training
programs. Weakness of muscle groups that require more strength during crouch gait

117
than unimpaired gait, such as the quadriceps, are not likely contributors to crouch gait;
however, weakness of muscle groups that require less strength during crouch gait than
unimpaired gait could contribute to crouch gait. Weakness of the hip abductors and
ankle plantarflexors may preclude individuals with crouch gait from achieving an
upright gait pattern, and these muscle groups may be important targets for strength
training programs.
The focus of this study was to isolate the effects of reduced force-generating
capacity on the dynamics of crouch gait; however, multiple mechanisms including
reduced physiological cross-sectional area, impaired neural drive, altered selective
motor control, and reduced voluntary force capacity can contribute to muscle
weakness. Neural mechanisms such as reduced voluntary force capacity (Elder et al.,
2003; Rose and McGill, 2005) and muscle properties such as reduced physiological
cross-sectional area (Moreau et al., 2009) have been documented in individuals with
cerebral palsy. Future investigations are required to differentiate between these
mechanisms.
The small number of subjects available for simulation and analysis is a
limitation of this study. Some of the muscle groups, such as the hamstrings and
iliopsoas, had variable results which may require a larger number of subjects to
understand the relationship between required strength and crouch gait.
Our analysis demonstrated that moderate crouch gait places a greater demand
on the quadriceps than unimpaired gait. This suggests that if subjects are able to walk
in a crouch gait that they have sufficient force-generating capacity to walk in an
upright gait. Previous studies have reported an increase in quadriceps activity with

118
crouch severity measured using electromyography taken during a static crouch posture
(Hsu et al., 1993) or estimated from cadavers positioned in a crouch posture (Perry et
al., 1975). Strength training programs designed for individuals with cerebral palsy and
crouch gait have targeted the hip and knee extensors (Damiano et al., 1995a; Damiano
et al., 2010) and reported inconsistent improvements in knee extension. The results of
our study may help to explain the inconsistent outcomes after these strength training
programs because crouch gait requires greater quadriceps force than unimpaired gait
and may not contribute to crouch gait in some individuals. However, case studies have
documented a lack of force-generating capacity when the knee is near full extension in
some individuals with cerebral palsy (Gage and Novacheck, 2001). Thus, although
crouch gait required more quadriceps strength than unimpaired gait, if individuals with
crouch gait cannot generate sufficient force when the knee is in full extension,
quadriceps weakness may still contribute to crouch gait. Examining the relationship
between quadriceps strength and knee flexion angle is an important area for further
investigation in individuals with cerebral palsy.
Moderate crouch gait required less hip abductor strength than unimpaired gait
and mild crouch gait required less ankle plantarflexor strength than unimpaired gait. In
the subjects included in this study, we also observed from inverse dynamics reduced
hip abductor moments and ankle plantarflexor moments during stance. To investigate
if reduced joint moments were present in a larger population, we examined the
kinematic and kinetic data for all crouch gait subjects who visited Gillette Children’s
Specialty Healthcare from February 1994 to January 2010. This analysis included 82
typically-developing children, 976 mild crouch gait subjects and 209 moderate crouch

119
gait subjects using the same criteria described in the methods. A comparison of the hip
abductor moment in this larger population indicated that the hip abductor moment
during crouch gait was significantly reduced compared to unimpaired gait (Figure
6.6), as determined by a one-way ANOVA (p < 0.001). Additionally, the ankle
plantarflexor moment during terminal stance was significantly reduced during crouch
gait (p < 0.001) and the ankle dorsiflexion angle during stance increased with crouch
severity (p < 0.001). Our simulations revealed a significant decrease in the ankle
plantarflexor strength required during mild crouch gait compared to unimpaired gait,
but not during moderate crouch gait. As the ankle dorsiflexion angle increases with
crouch severity, the ankle plantarflexion moment arms of the gastrocnemius and
soleus decrease, which would require greater ankle plantarflexor force to produce the
required ankle plantarflexor moment.

120
Ankle plantarflexor weakness has previously been noted as a potential cause of
crouch gait (Gage, 1990). Previous studies have reported that ankle plantarflexor
strength in individuals with diplegic cerebral palsy is reduced to 40-60% of age-
matched typically-developing peers (Wiley and Damiano, 1998; Elder et al., 2003).
Potential causes of ankle plantarflexor weakness include impaired control, over-
lengthening of the Achilles tendon, or effects from injections of neural toxins.
Outcome studies after surgical lengthening of the Achilles tendon have noted an
Figure 6.6: Average (A) kinematics and (B) kinetics for hip abduction and ankle plantarflexion forunimpaired children (N=82, dotted black) and individuals with cerebral palsy who walked in mild (N =976, light gray) and moderate (N=209, dark gray) crouch gait who visited Gillette Children’s SpecialtyHealthcare. The peak hip abductor moment and ankle plantarflexor moment are smaller during mild andmoderate crouch gait compared to unimpaired gait (ANOVA, p < 0.001). Joint moments are normalized bybody mass (kg).

121
increased risk of crouch gait (Damron et al., 1994; Dietz et al., 2006). These results
support the theory that some individuals may adopt crouch gait as a result of weak
ankle plantarflexors. Engsberg et al. (2006) found that strengthening the ankle
plantarflexors improved knee extension during stance in individuals with cerebral
palsy.
Limited information is available regarding hip abductor strength in individuals
with cerebral palsy. Wiley et al. (1998) reported that average hip abductor strength in
individuals with diplegic cerebral palsy was 55% of age-matched typically-developing
children. Hip abductor weakness has previously been associated with a Trendelenburg
gait pattern, characterized by exaggerated torso bending in the coronal plane (Perry,
1992). To examine if torso motion contributed to the reduced hip abductor moment
during crouch gait, we compared the torso motion of the subjects with crouch gait who
had torso markers and crouch gait subjects from Gillette Children’s Specialty
Healthcare who had torso markers (mild crouch gait N=31, moderate crouch gait
N=10) to unimpaired gait (N=82). We found no significant difference in torso bending
during mild and moderate crouch gait compared to unimpaired gait, suggesting that
crouch posture rather than torso motion contributed to the reduced hip abductor
strength required during crouch gait. Further study is required to determine the extent
of hip abductor weakness in individuals with crouch gait and if strengthening the hip
abductors improves crouch gait.
This study used muscle-driven simulations to examine how much the
maximum isometric force of particular muscle groups could be reduced and maintain
the dynamics of crouch gait compared to unimpaired gait. The simulations allowed us

122
to examine the effects of individual muscle group weakness that could not be
elucidated with other methods. The results of this study suggest that crouch gait
requires greater quadriceps strength than unimpaired gait; however, moderate crouch
gait requires less hip abductor strength and mild crouch gait requires less ankle
plantarflexor strength than unimpaired gait. Future studies that investigate the effects
of strengthening the hip abductors or ankle plantarflexors on crouch gait can further
improve our understanding of how weakness of these muscles contributes to crouch
gait and assist in the design of strength training programs that improve walking ability.

123
CHAPTER 7
WHAT CHARACTERISTICS ARE ASSOCIATED WITH POSITIVE OUTCOMES AFTER STRENGTH TRAINING FOR CROUCH GAIT?
Journal of Pediatric Rehabilitation Medicine, (2012), vol. 5, pp. 99-106
Katherine M. Steele Diane L. Damiano Meta Nyström Eek Marianne Unger Scott L. Delp

124
ABSTRACT
Muscle weakness may contribute to crouch gait in individuals with cerebral
palsy, and some individuals participate in strength training programs to improve
crouch gait. Unfortunately, improvements in muscle strength and gait are inconsistent
after completing strength training programs. The purpose of this study was to examine
changes in knee extensor strength and knee extension angle during walking after
strength training in individuals with cerebral palsy who walk in crouch gait and to
determine subject characteristics associated with these changes. A literature review
was performed of studies published since January 2000 that included strength training,
three-dimensional motion analysis, and knee extensor strength measurements for
individuals with cerebral palsy. Three studies met these criteria and individual subject
data was obtained from the authors for thirty crouch gait subjects. Univariate
regression analyses were performed to determine which of ten physical examination
and motor performance variables were associated with changes in strength and knee
extension during gait. Change in knee extensor strength ranged from a 25% decrease
to a 215% increase, and change in minimum knee flexion angle during gait ranged
from an improvement of 9º more knee extension to 15º more knee flexion. Individuals
without hamstring spasticity had greater improvement in knee extension after strength
training. Hamstring spasticity was associated with an undesired increase in knee
flexion during walking. Subject-specific factors such as hamstring spasticity may be
useful for predicting which subjects will benefit from strength training to improve
crouch gait.

125
7.1 INTRODUCTION
Crouch gait, a common movement pattern in individuals with cerebral palsy, is
characterized by excessive knee flexion during the stance-phase of gait. There are
several proposed causes of crouch gait, including contracted hamstrings, weak ankle
plantarflexors, contracted hip flexors, impaired balance, general muscle weakness, and
foot malalignment (Gage, 1990). If left untreated, crouch gait can lead to joint pain
(Jahnsen et al., 2004), bone deformities (Graham and Selber, 2003), and walking
limitations (Johnson et al., 1997; Opheim et al., 2009). Treatment of crouch gait
frequently involves orthopaedic surgery. Surgery can be effective in reducing
excessive knee flexion, correcting bony deformities, and improving walking ability
(Rodda et al., 2006). However, surgery does not correct underlying muscle weakness.
Weakness of the extensor muscles in the lower extremity is present in many
individuals with cerebral palsy (Damiano et al., 1995b; Wiley and Damiano, 1998).
Weakness in individuals with a crouch gait could compromise their ability to generate
the muscle forces required to produce an upright gait pattern. Muscles such as the
gluteus maximus, vasti, gastrocnemius, and soleus are major contributors to
supporting body weight during crouch gait (Steele et al., 2010); therefore,
strengthening these muscles could potentially improve an individual’s ability to walk
in a more upright posture.
There is conflicting evidence on the efficacy of strength training in cerebral
palsy. Individuals with cerebral palsy can gain muscle strength after participation in
strength training programs (Healy, 1958; McCubbin and Shasby, 1985), but the
functional changes after a strength training program are variable. Damiano et al.

126
(1995a) observed improvement in knee extension at initial contact during walking and
increased stride length after strength training, and Blundell et al. (2003) and Dodd et
al. (2003) demonstrated an improvement in functional tests after strength training.
Other studies have not found significant changes in functional tests (Kerr et al., 2006;
Liao et al., 2007), or observed increased knee flexion during gait in some subjects
after strength training (Damiano et al., 2010). There is a lack of consensus regarding
the efficacy of strength training in individuals with cerebral palsy (Dodd et al., 2002;
Mockford and Caulton, 2008; Scholtes et al., 2008; Scianni et al., 2009), and it is
unclear which muscles should be strengthened to improve crouch gait.
It is challenging to characterize the efficacy of strength training programs in
individuals with cerebral palsy because most studies include individuals with different
gait patterns and levels of impairment. Furthermore, most studies only report average
changes and do not document individual outcomes. This makes it difficult to
understand the variability in outcomes between subjects and confounds efforts to
determine which subjects benefit from strength training. Individuals with cerebral
palsy represent a heterogeneous population. Strengthening may not be effective in all
individuals with crouch gait, and a better understanding of the characteristics
associated with improved strength and function following strength training is needed.
The goals of this study were to: (1) examine the variability in outcomes after
progressive resistance strength training for individuals with cerebral palsy who walk in
a crouch gait, and (2) identify the subject characteristics associated with gains in
strength and improved knee extension during gait after strength training. To achieve
this goal we performed a literature search for studies that combined three-dimensional

127
motion analysis and a progressive resistance strength training program for subjects
with crouch gait. Data from studies that met these criteria (Unger et al., 2006; Eek et
al., 2008; Damiano et al., 2010) were used to create a database of strength
measurements and walking kinematics before and after strength training. We
performed regression analyses to identify characteristics associated with gains in
strength and improvement in knee extension.
7.2 METHODS
7.2.1 LITERATURE REVIEW
To investigate the effects of strength training in individuals with cerebral palsy
who walk with a crouch gait, we performed a literature search for studies published
since January 2000 that included (1) a progressive resistance strength training
program, (2) a three-dimensional motion analysis before and after strength training,
and (3) a goal of improved knee extension for individuals who walked in a crouch
gait. The time period was chosen to increase the likelihood that individual data not
included in the manuscript would be retrievable. PubMED was used as the search
database in addition to scanning reference lists. A combination of the following search
terms was used: cerebral palsy AND strength AND (training OR program). 58 articles
were identified in the initial literature search that had been published since January
2000 (Figure 7.1). Of these articles, 32 were review articles, post-operative
rehabilitation programs, or not strength training programs for individuals with cerebral
palsy. Additionally, 23 articles were excluded that did not include three-dimensional

128
motion analysis, knee extensor strength measurements, or a progressive resistance
strength training protocol.
Three studies (Unger et al., 2006; Eek et al., 2008; Damiano et al., 2010) were
identified that met all criteria (Table 7.1). The first authors were contacted and agreed
to collaborate in this study. Subject information, physical exam measures, muscle
strength data, and gait kinematics were collected for all subjects in each study. All
studies were performed according to the human subject research requirement at their
respective institutions. All data shared as part of this analysis was de-identified.
Table 7.1: Summary of crouch subjects and training programs for all studies
Study N Age (yrs)
Height (cm)
Weight (kg) Training Program
Damiano (2010)
7 8.1 ± 2.6 118 ± 13 20.5 ± 4.8 8 weeks (3 times/week) Progressive resistance with weight machines & cuffs Targeted hip and knee extensors
Unger (2006)
17 16.2 ± 1.4 158 ± 12 51.5 ± 9.5 8 weeks (1-3 times/week) Progressive resistance with weights & resistance bandsFull body
Eek (2008)
6 12.4 ± 1.6 145 ± 9 40.5 ± 9.2 8 weeks (3 times/week) Progressive resistance with weights & resistance bandsTargeted 4 muscle groups per child
Total 30 13.7 ± 3.8 147 ± 20 42.4 ± 15.2
Literature SearchDatabase: PubMedN = 72
Published since January 2000N = 58
Screened titles and abstracts
Excluded (N = 32)Post‐op rehabilitation: 4Not strength training program: 14Review articles: 14Included (N = 26)
Evaluated inclusion criteria
Excluded (N = 23)Not progressive resistance training: 10No 3D motion analysis: 11Did not measure knee extensor strength: 2Included (N = 3)
Figure 7.1: Summary of literature review and study selection.

129
7.2.2 Subject Selection
Individuals who walked in a crouch gait pattern were selected from each study.
Crouch gait was defined as a minimum knee flexion angle greater than 10º during
stance. Thirty subjects met this criterion and were included in the study (Table 7.1).
The subjects included 14 who had a mild crouch with a minimum knee flexion angle
less than 20°, 12 who had a moderate crouch gait with a minimum knee flexion angle
between 20° and 30°, and 3 who had a minimum knee flexion angle greater than 30°.
The average minimum knee flexion angle during stance was 20°. GMFCS levels were
available for two of the studies (Eek et al., 2008; Damiano et al., 2010) and the crouch
gait subjects included 3 GMFCS Level I, 6 GMFCS Level II, and 4 GMFCS Level III.
All studies excluded subjects who had surgery within the past 12 months.
7.2.3 STRENGTH TRAINING PROGRAMS
The studies consisted of 8-week progressive resistance strength training
programs including both home and therapist-supervised training sessions and targeted
a range of muscle groups. The subjects in the program reported by Damiano et al.
(2010) were younger than the other two studies and participated in a program targeting
the hip and knee extensors in therapist-supervised sessions three times per week.
Unger et al. (2006) organized a school-based circuit strength training program that
subjects completed one to three times per week. Eek et al. (2008) designed
individualized strength training programs that targeted four lower-extremity muscle
groups that subjects completed three times per week (twice at home and once at a

130
physiotherapy clinic). Detailed information on each study is provided in the original
publications.
7.2.4 OUTCOMES MEASURES
Since the focus of this study is on individuals with a crouch gait, we examined
change in knee extensor strength and change in minimum knee flexion angle during
stance after strength training. Knee extensor strength was measured using an isokinetic
strength assessment at 30°/s (Damiano et al., 2010) or an isometric strength
assessment using a dynamometer (Unger et al., 2006; Eek et al., 2008). Change in
knee extensor strength was calculated as the percent change in maximum knee
extensor torque after strength training. Change in minimum knee flexion angle was
calculated from kinematics obtained from three-dimensional motion analysis.
7.2.5 SUBJECT-SPECIFIC CHARACTERISTICS
Ten subject characteristics were selected based upon literature and clinical
experience that could be associated with changes in knee extensor strength and knee
extension during gait. These included: (1) hamstring spasticity, (2) popliteal angle, (3)
knee flexion at initial contact, (4) minimum knee flexion angle during stance, (5)
quadriceps strength, (6) age, (7) height, (8) weight, (9) walking speed, and (10) Gross
Motor Function Classification System (GMFCS) level. All characteristics were
measured before the strength training program.
Hamstring spasticity, popliteal angle, and GMFCS level were only available
for the subjects in studies by Damiano et al. (2010) and Eek et al. (2008). Hamstring

131
spasticity was included as a binary variable with an Ashworth score ≥ 2 indicating
hamstring spasticity.
7.2.6 REGRESSION ANALYSES
Univariate linear regression analyses were performed between each of the 10
subject-specific characteristics and the two outcome measures, (1) change in knee
extensor strength and (2) change in minimum knee flexion angle during stance, to
determine which characteristics had the strongest association with each outcome
measure. A random effect term for “study” was also included in each model to account
for between-study variation (Pinheiro and Bates, 2009). No corrections were made for
multiple comparisons (Rothman, 1990). To compare the relative effects of the
characteristics, we performed a multivariate linear regression analysis that included all
the characteristics with a significant association for each outcome measure (p < 0.05).
Significant associations were also checked for confounding effects of age, height, and
weight. All statistics were performed using R, a statistical analysis package (www.r-
project.org/index.html).
7.3 RESULTS
The 30 crouch gait subjects had variable changes in knee extensor strength and
minimum knee flexion angle during gait after completing a strength training program.
The average change in knee extensor strength was a 23% increase; however, the range
varied from a 25% decrease to a 215% increase (Figure 7.2). The average change in

132
minimum knee flexion angle after strength training for the group was 0º; however, the
range varied from an improvement of 9º more knee extension to a deterioration of 15º
more knee flexion (Figure 7.2).
Although the average knee kinematics of the group suggest that the strength
training program had no effect on knee kinematics (Figure 7.3), examining the
changes in knee flexion for the subjects with the best and worst outcomes
demonstrates that some subjects had substantial improvements while others had
deterioration after completing the strength training program. For example, the top ten
Figure 7.2: Histograms of (A) percent change in knee extensor strength and (B) change in minimum knee flexion angle during gait after completing a strength training program. Subjects from each of the three studies are shown separately – Damiano (white), Eek (gray), and Unger (black). A negative change in minimum knee flexion angle indicates a more upright posture, or a positive outcome, after strength training. Note that in all three studies the outcomes were variable between subjects.

133
percent of subjects had an average improvement of 9° more knee extension during
stance, whereas the bottom ten percent of subjects, with the greatest increase in
minimum knee flexion, had an average change of 10° more knee flexion. After the
strength training program, the subjects with the best outcomes achieved knee
extension within normal limits in late stance.
Figure 7.3: Average hip, knee, and ankle flexion angles for (A) all subjects, (B) the three subjects with the largest increase in knee extension (best outcomes), and (C) the three subjects with the largest increase in knee flexion (worst outcomes) before and after completing strength training program. Note that although there was no significant change in knee flexion for the group as a whole, there were subsets of subjects with significant positive and negative changes.

134
There was a significant association between change in minimum knee flexion
angle and change in minimum hip flexion angle (slope = 0.59, p = 0.001) suggesting
that individuals with improved knee extension also had improved hip extension after
strength training. There was no association between change in knee flexion angle and
change in maximum dorsiflexion angle during stance. Average hip flexion angle and
ankle dorsiflexion angle did not change significantly after strength training for the
group, but the inter-subject variability was similar to the variability in change in knee
flexion angle.
Hamstring spasticity was associated with change in minimum knee flexion
angle after strength training (Table 7.2). No subject with an Ashworth Score ≥ 2 had
an improvement in knee flexion angle after strength training (Figure 7.4). Individuals
with a hamstring Ashworth score equal to one had an average improvement of 3° more
knee extension, and 4 out of 6 of these subjects showed improved knee extension after
the strength training program. The association between hamstring spasticity and
change in knee flexion angle was maintained after controlling for age, height, and
weight. Walking speed recorded before the strength training program was also
associated with change in minimum knee flexion angle (p = 0.03); individuals who
walked faster were more likely to have improved knee extension after the strength
training program (Figure 7.4). However, when included in a multi-regression analysis
with hamstring spasticity, walking speed did not add additional information to the
model and was no longer significant. Walking speed was correlated with hamstring
spasticity (r2 = -0.55), indicating that individuals with hamstring spasticity tended to
walk slower.

135
Table 7.2: Results of regression analyses for change in knee flexion angle and knee extensor strength Kinematics: Strength:
Minimum knee flexion angle Knee extensor strength Coeff S.E. p-value p-adj** Coeff S.E. p-value
Hamstring spasticity* 8.51 3.06 0.02 0.006 0.13 0.1 0.21 Popliteal angle* (deg) -0.14 0.15 0.36 -0.01 0.005 0.11 KFA at initial contact (deg) 0.12 0.08 0.12 0.005 0.006 0.43 Min KFA (deg) -0.05 0.12 0.66 -0.002 0.01 0.77 Knee extensor strength (Nm/kg) 6.43 21.2 0.76 -2.83 0.79 0.11 Age (yr) -0.35 0.28 0.22 -0.02 0.03 0.45 Height (cm) -0.08 0.05 0.13 < 0.001 < 0.001 0.99 Weight (kg) -0.07 0.07 0.35 < 0.002 0.01 0.52 Walking speed/height (s-1) -16.7 6.95 0.02 0.02 0.01 0.57 0.99 GMFCS level* 2.51 2.62 0.36 0.03 0.13 0.79 p < 0.05 Each regression analysis included a random effects term, “study,” as a covariate. Coeff, Regression coefficient; S.E., Standard Error; GMFCS, Gross Motor Function Classification System * Data available for subjects from studies by Damiano and Eek ** Adjusted for age, height, and weight
There were no significant associations between the subject characteristics and
percent change in knee extensor strength (Table 7.2). There was also no relationship
between the change in minimum knee flexion angle and change in knee extensor
strength (R2 = 0.0).
Figure 7.4: (A) Hamstring spasticity and (B) walking speed were associated with change in minimum knee flexion angle (KFA) during stance with a p-value < 0.05.

136
7.4 DISCUSSION
Individuals with cerebral palsy who walk in a crouch gait have inconsistent
outcomes after strength training. Although the majority of subjects had an increase in
knee extensor strength, the change in knee extension during gait was variable. Some
individuals had an improvement in knee extension during gait that was comparable to
outcomes after orthopaedic surgery (Adolfsen et al., 2007); however, other subjects
with crouch gait walked with greater knee flexion after strength training. Determining
which subjects will improve knee extension after strength training is necessary to
determine who should participate in these programs.
Hamstring spasticity was associated with more knee flexion after strength
training. Strength training in subjects with hamstring spasticity to improve crouch gait
is not supported by our analysis. However, from the small sample included in this
study, it does not appear that strength training exacerbated spasticity. The Ashworth
score for the hamstrings changed for only two subjects after strength training; one
subject had a lower Ashworth score and another had a higher Ashworth score. The
association between hamstring spasticity and increased knee flexion after strength
training may be a result of increased muscle strength amplifying the effects of
excessive muscle activity during gait. Future studies should incorporate more
quantitative spasticity measurements and evaluate spasticity of multiple muscle groups
before and after strength training.
No significant associations were found between the subject characteristics and
change in quadriceps strength. The lack of associations may be confounded by the
different methods used for measuring knee extensor strength between studies. Not all

137
subjects included in this analysis increased quadriceps strength after completing a
strength training program; therefore, future studies to explain the variability in
changes in strength between subjects would be valuable. Other factors such as
selective motor control, hip range of motion, or rotational deformities may contribute
to variability in change in knee extensor strength.
The change in knee flexion angle after strength training was significantly
correlated with change in hip flexion angle but not with change in ankle dorsiflexion
angle. The individuals included in this study walked with varying degrees of ankle
dorsiflexion during stance which likely contributed to the lack of correlation between
change in knee and ankle angle. Eight of the thirty individuals included in this study
had a maximum dorsiflexion angle during stance of less than 5°. We tested to see if
the outcomes or regression models were different for those individuals who walked
with reduced dorsiflexion during stance; however, there were no significant
differences. Future studies that examine differences between subgroups of crouch gait
could further improve our ability to determine the optimal treatment for each subject.
Strength training programs designed for individuals who walk in a crouch gait,
including those in this analysis, have focused on strengthening the hip and knee
extensors. However, weakness of these muscle groups may not be a primary cause of
crouch gait. During normal gait, the vasti and gluteus maximus support the body
weight in early stance and the ankle plantarflexors support the body weight in terminal
stance (Liu et al., 2008). In crouch gait, the knee extensor moment during stance is
larger, which requires higher forces to be generated by the knee extensors. These
larger loads may lead to patellar fracture or patella alta (Rosenthal and Levine, 1977;

138
Murphy, 2009; O'Sullivan et al.). Since walking in an erect gait requires less strength
than walking in crouch gait, strengthening of the knee extensors may not correct
crouch gait in some subjects.
In contrast, ankle plantarflexor weakness is commonly cited as a potential
cause of crouch gait (Gage, 1990). A previous study examined the effects of ankle
plantarflexor strengthening and reported an improvement in knee flexion during
stance, although the study was not specific to individuals with crouch gait (Engsberg
et al., 2006). If we could identify the primary cause of crouch gait in each individual
this would improve our ability to target the correct muscles for strength training
programs or other treatment strategies.
The limited number of subjects and combination of outcomes from three
centers limits the power of this analysis. No corrections were made for multiple
comparisons, which increases the probability of Type I errors in our statistical
analysis. This analysis also combined data from three independent studies performed
according to different protocols at different institutions. The change in knee flexion
angle and percent change in knee extensor strength were similar in magnitude at all
three institutions and all three studies had variable outcomes between subjects. The
limited number of subjects also limited the number of subject characteristics that could
be included in the analysis. Additionally, other factors that were not included in the
original studies such as selective motor control, range of motion, and spasticity in
other muscle groups could be important predictors of outcomes after strength training.
There may also be benefits of strength training programs that are not captured by the

139
outcome measures included in this analysis such as increased physical activity,
improved cardiovascular health, and enhanced self-image (Faigenbaum et al., 2009).
The Ashworth score was used by the studies included in this analysis to measure
hamstring spasticity; however, more quantitative measures of spasticity would be
desirable. Due to these limitations, future studies are required to test the
generalizability of the results.
The goal of strength training studies in individuals with cerebral palsy should
be to identify those subjects with the greatest likelihood for a positive outcome. Some
subjects benefit from progressive resistance strength training, but it is unlikely that
strengthening is the ideal therapy for all subjects. Methods that determine which
subjects are unlikely to respond well can save resources of patients, clinicians, and
care-givers. Understanding how characteristics such as spasticity and changes in
muscle strength affect functional outcomes are important areas for future research to
inform the design of optimal, subject-specific treatments.

140

141
CHAPTER 8
CONCLUSION

142
8.1 SUMMARY
This dissertation presents the first three-dimensional musculoskeletal
simulations of individuals with cerebral palsy and has contributed to our
understanding of how muscle contributions, joint loads, and the effects of muscle
weakness change in individuals with cerebral palsy and crouch gait. The simulations
created for these analyses have been made freely-available for researchers and
clinicians to download, use, and evaluate at http://www.simtk.org/home/crouchgait/.
This work has provided insight into the underlying dynamics of crouch gait and
created pathways to improve treatment.
The first objective of this dissertation was to examine how individual muscles
contribute to motion during crouch gait. Chapters 3 and 4 evaluated how muscles
contribute to joint and mass center accelerations to support and propel the body during
crouch gait and how these contributions change with crouch severity. The results of
these analyses indicated that crouch gait uses similar muscles to support and propel the
body as unimpaired gait; however, larger and more sustained muscle activity is
required during crouch gait, which contributes to the inefficiencies of this gait pattern.
The second objective of this dissertation was to examine how the compressive
tibiofemoral force changes in individuals with cerebral palsy and crouch gait (Chapter
5). Knee pain is common among individuals with crouch gait and the results of this
study demonstrated that tibiofemoral load increases quadratically with crouch severity.
Individuals who walk in a severe crouch gait experience three-times the tibiofemoral
load than during unimpaired gait. The elevated tibiofemoral forces during crouch gait
could contribute to cartilage degeneration and knee pain.

143
The final objective of this dissertation was to examine one of the common
suggested causes of crouch gait: muscle weakness. We used musculoskeletal
simulations to determine how much muscle groups can be weakened and still
reproduce mild and moderate crouch gait (Chapter 6). The results of this analysis
demonstrated that crouch gait requires greater quadriceps strength but less hip
abductor and ankle plantarflexor strength than unimpaired gait; suggesting that these
latter muscles may be better targets for strength training programs. We also performed
a meta-analysis of individuals with crouch gait who had participated in strength
training programs (Chapter 7). This analysis demonstrated that outcomes after strength
training are inconsistent, even among individuals with cerebral palsy and crouch gait.
Hamstring spasticity was associated with poor outcomes after strength training and
may be a contraindication for strength training.
8.2 FUTURE WORK
The work presented in this dissertation has created a foundation of knowledge
about the dynamics of crouch gait in individuals with cerebral palsy. The simulations
created as part of this dissertation are available on-line for other researchers to use,
evaluate, and extend (http://www.simtk.org/home/crouchgait/). For example, the
results of these simulations provide a foundation to investigate important questions to
improve the evaluation and treatment of individuals with cerebral palsy such as:
• What are the actions of the hamstrings during crouch gait and how does
musculotendon lengthening of the hamstrings improve knee extension in some
individuals?

144
• How sensitive are musculoskeletal simulations of individuals with cerebral
palsy to (1) altered muscle properties such as contracture, (2) kinematics and
structure of the foot, and (3) alignment and orientation of the knee?
• What are the effects of femoral extension osteotomy and other skeletal
procedures on the kinematics, muscle activity, joint loading, and
musculotendon lengths during gait?
• Does crouch gait provide a more stable posture than upright gait?
• How does the simulated muscle activity during crouch gait in individuals with
cerebral palsy differ from unimpaired individuals voluntarily walking in a
crouch gait?
The results of the studies included in this dissertation also suggest exciting
avenues for future work using both simulation and experimentation. The following
sections outline important areas of future work that can further expand our
understanding of gait pathologies and lead to innovative treatment strategies:
• How is muscle physiology different in individuals with cerebral palsy?
Altered muscle physiology including contracture and spasticity are common
among individuals with cerebral palsy; however, the mechanics of how muscle
physiology changes and the effects these changes have on gait are not well
understood. Future studies should quantify changes in muscle physiology in
individuals with cerebral palsy. Quantifying these changes will allow
researchers and clinicians to generate improved muscle models, develop more

145
physiologically representative simulations, and improve our understanding of
how altered muscle physiology affects the dynamics of gait pathologies.
• How do the dynamics of gait change after surgical intervention?
Multi-level orthopaedic surgery is a common treatment for individuals with
cerebral palsy and consists of multiple surgeries including musculotendon
lengthenings, rotational osteotomies, and various other procedures.
Musculoskeletal modeling and simulation can be used to evaluate the
dynamics of gait before and after surgery to provide a more quantitative
understanding of the effects of these procedures on each subject’s ability to
produce an efficient gait pattern.
• How can predictive modeling be used to examine pathologic gait patterns?
The simulations created as part of this dissertation are based upon experimental
motion capture data that is used to estimate the muscle excitations required to
reproduce each subject’s motion. An alternative method is to use predictive
computational methods to evaluate what gait pattern a model will adopt with a
given objective function. These methods allow researchers to investigate
‘what-if’ questions and could provide a new platform for evaluating the
mechanisms that cause crouch gait and predicting surgical outcomes.
• How does increased tibiofemoral loading affect cartilage health?
Knee pain is common among individuals with cerebral palsy and crouch gait
and this dissertation demonstrated that tibiofemoral force increases with crouch
severity. Future studies should investigate if these increased loads affect

146
cartilage growth, maintenance, or development in individuals with cerebral
palsy.
• How does spasticity affect outcomes after strength training?
The meta-analysis of strength training outcomes included in this dissertation
found an association between hamstring spasticity and poor outcomes after
strength training in individuals with cerebral palsy and crouch gait.
Investigations are required to determine if these results extend to a larger
population and if spasticity in other muscle groups could also be predictive of
outcomes after strength training.
• How does strengthening the hip abductors and ankle plantarflexors affect
crouch gait?
Crouch gait requires less hip abductor and ankle plantarflexor force than
unimpaired gait, suggesting that crouch gait may be a compensation for
weakness of these muscle groups. Future studies should investigate if strength
training programs that target the hip abductors and/or the ankle plantarflexors
have more consistent, positive outcomes than current strength training
programs.
• How can modeling and simulation be integrated into the clinic?
Modeling and simulation provides a wide variety of information that clinicians
can use in surgical and therapeutic decision-making. The framework,
methodology, and tools for integrating this information into the clinic will need
to be developed to accelerate the translation from research to clinical
outcomes.

147
The long term goal of the work presented in this dissertation and the proposed
studies outlined above is to improve quality of life for individuals with cerebral palsy.
The freedom to walk, explore, and interact with the world is a skill that many of us
take for granted every day. Through the combination of musculoskeletal modeling and
simulation, experimental studies, and clinical outcomes we can help individuals with
gait pathologies achieve this freedom throughout their life.

148

149
REFERENCES Economic costs associated with mental retardation, cerebral palsy, hearing loss, and vision impairment--United States, 2003, MMWR Morb Mortal Wkly Rep, 53, 57-9, 2004. Abel, M.F., Damiano, D.L., Pannunzio, M. and Bush, J., 1999. Muscle-tendon surgery in diplegic cerebral palsy: functional and mechanical changes. J Pediatr Orthop 19, 366-75. Abel, M.F., Juhl, G.A., Vaughan, C.L. and Damiano, D.L., 1998. Gait assessment of fixed ankle-foot orthoses in children with spastic diplegia. Arch Phys Med Rehabil 79, 126-33. Adolfsen, S.E., Ounpuu, S., Bell, K.J. and DeLuca, P.A., 2007. Kinematic and kinetic outcomes after identical multilevel soft tissue surgery in children with cerebral palsy. J Pediatr Orthop 27, 658-67. Anderson, F.C. and Pandy, M.G., 1999. A Dynamic Optimization Solution for Vertical Jumping in Three Dimensions. Comput Methods Biomech Biomed Engin 2, 201-231. Anderson, F.C. and Pandy, M.G., 2003. Individual muscle contributions to support in normal walking. Gait Posture 17, 159-69. Arnold, A.S., Anderson, F.C., Pandy, M.G. and Delp, S.L., 2005. Muscular contributions to hip and knee extension during the single limb stance phase of normal gait: a framework for investigating the causes of crouch gait. J Biomech 38, 2181-9. Arnold, A.S., Liu, M.Q., Schwartz, M.H., Ounpuu, S. and Delp, S.L., 2006a. The role of estimating muscle-tendon lengths and velocities of the hamstrings in the evaluation and treatment of crouch gait. Gait Posture 23, 273-81. Arnold, A.S., Liu, M.Q., Schwartz, M.H., Ounpuu, S., Dias, L.S. and Delp, S.L., 2006b. Do the hamstrings operate at increased muscle-tendon lengths and velocities after surgical lengthening? J Biomech 39, 1498-506. Arnold, A.S., Thelen, D.G., Schwartz, M.H., Anderson, F.C. and Delp, S.L., 2007. Muscular coordination of knee motion during the terminal-swing phase of normal gait. J Biomech 40, 3314-24. Baddar, A., Granata, K., Damiano, D.L., Carmines, D.V., Blanco, J.S. and Abel, M.F., 2002. Ankle and knee coupling in patients with spastic diplegia: effects of gastrocnemius-soleus lengthening. J Bone Joint Surg Am 84-A, 736-44.

150
Baumann, J.U., Ruetsch, H. and Schurmann, K., 1980. Distal hamstring lengthening in cerebral palsy. An evaluation by gait analysis. Int Orthop 3, 305-9. Bell, K.J., Ounpuu, S., DeLuca, P.A. and Romness, M.J., 2002. Natural progression of gait in children with cerebral palsy. J Pediatr Orthop 22, 677-82. Bernthal, N.M., Gamradt, S.C., Kay, R.M., Wren, T.A., Cuomo, A.V., Reid, J., Bales, J. and Otsuka, N.Y., Static and dynamic gait parameters before and after multilevel soft tissue surgery in ambulating children with cerebral palsy. J Pediatr Orthop 30, 174-9. Blair, E., 2010. Epidemiology of the cerebral palsies. Orthop Clin North Am 41, 441-55. Blundell, S.W., Shepherd, R.B., Dean, C.M., Adams, R.D. and Cahill, B.M., 2003. Functional strength training in cerebral palsy: a pilot study of a group circuit training class for children aged 4-8 years. Clin Rehabil 17, 48-57. Borton, D.C., Walker, K., Pirpiris, M., Nattrass, G.R. and Graham, H.K., 2001. Isolated calf lengthening in cerebral palsy. Outcome analysis of risk factors. J Bone Joint Surg Br 83, 364-70. Bradford, E., 1890. The surgical treatment of spastic paralysis in children. The Journal of Bone and Joint Surgery 1, 7. Brehm, M.A., Harlaar, J. and Schwartz, M., 2008. Effect of ankle-foot orthoses on walking efficiency and gait in children with cerebral palsy. J Rehabil Med 40, 529-34. Burden, R.L. and Faires, J.D., 1985. 2.1 The Bisection Algorithm. In: (Eds.), Numerical analysis. Prindle, Weber & Schmidt, Boston, Mass., pp. x, 676 p. Campbell, J. and Ball, J., 1978. Energetics of walking in cerebral palsy. Orthop Clin North Am 9, 374-7. Carr, L.J., Harrison, L.M., Evans, A.L. and Stephens, J.A., 1993. Patterns of central motor reorganization in hemiplegic cerebral palsy. Brain 116 ( Pt 5), 1223-47. Carter, D.R. and Wong, M., 1988. The role of mechanical loading histories in the development of diarthrodial joints. J Orthop Res 6, 804-16. Chambers, H.G., 2001. Treatment of functional limitations at the knee in ambulatory children with cerebral palsy. Eur J Neurol 8 Suppl 5, 59-74.

151
Correa, T.A., Schache, A.G., Graham, H.K., Baker, R., Thomason, P. and Pandy, M.G., 2012. Potential of lower-limb muscles to accelerate the body during cerebral palsy gait. Gait Posture Corry, I.S., Cosgrove, A.P., Duffy, C.M., Taylor, T.C. and Graham, H.K., 1999. Botulinum toxin A in hamstring spasticity. Gait Posture 10, 206-10. Craig, J.J. and van Vuren, J., 1976. The importance of gastrocnemius recession in the correction of equinus deformity in cerebral palsy. J Bone Joint Surg Br 58, 84-7. Crenna, P., 1998. Spasticity and 'spastic' gait in children with cerebral palsy. Neurosci Biobehav Rev 22, 571-8. D'Lima, D.D., Patil, S., Steklov, N., Slamin, J.E. and Colwell, C.W., Jr., 2006. Tibial forces measured in vivo after total knee arthroplasty. J Arthroplasty 21, 255-62. Damiano, D.L., Abel, M.F., Pannunzio, M. and Romano, J.P., 1999. Interrelationships of strength and gait before and after hamstrings lengthening. Journal of Pediatric Orthopaedics 19, 352. Damiano, D.L., Arnold, A.S., Steele, K.M. and Delp, S.L., 2010. Can strength training predictably improve gait kinematics? A pilot study on the effects of hip and knee extensor strengthening on lower-extremity alignment in cerebral palsy. Phys Ther 90, 269-79. Damiano, D.L., Kelly, L.E. and Vaughn, C.L., 1995a. Effects of quadriceps femoris muscle strengthening on crouch gait in children with spastic diplegia. Phys Ther 75, 658-67; discussion 668-71. Damiano, D.L., Vaughan, C.L. and Abel, M.F., 1995b. Muscle response to heavy resistance exercise in children with spastic cerebral palsy. Dev Med Child Neurol 37, 731-9. Damron, T.A., Breed, A.L. and Cook, T., 1993. Diminished knee flexion after hamstring surgery in cerebral palsy patients: prevalence and severity. J Pediatr Orthop 13, 188-91. Damron, T.A., Greenwald, T.A. and Breed, A.L., 1994. Chronologic outcome of surgical tendoachilles lengthening and natural history of gastroc-soleus contracture in cerebral palsy. A two-part study. Clin Orthop Relat Res 301, 249-255. Davids, J.R., Ounpuu, S., DeLuca, P.A. and Davis, R.B., 3rd, 2004. Optimization of walking ability of children with cerebral palsy. Instr Course Lect 53, 511-22.

152
Davis, R., Ounpuu, S., Tyburski, D. and Gage, J., 1991. A gait analysis data collection and reduction technique. Hum Mov Sci 10, 575–587. de Morais Filho, M.C., Kawamura, C.M., Kanaji, P.R. and Juliano, Y., 2010. The relation of triceps surae surgical lengthening and crouch gait in patients with cerebral palsy. J Pediatr Orthop B 19, 226-30. de Morais Filho, M.C., Neves, D.L., Abreu, F.P., Juliano, Y. and Guimaraes, L., 2008. Treatment of fixed knee flexion deformity and crouch gait using distal femur extension osteotomy in cerebral palsy. J Child Orthop 2, 37-43. Delp, S.L., Anderson, F.C., Arnold, A.S., Loan, P., Habib, A., John, C.T., Guendelman, E. and Thelen, D.G., 2007. OpenSim: open-source software to create and analyze dynamic simulations of movement. IEEE Trans Biomed Eng 54, 1940-50. Delp, S.L., Arnold, A.S., Speers, R.A. and Moore, C.A., 1996. Hamstrings and psoas lengths during normal and crouch gait: implications for muscle-tendon surgery. J Orthop Res 14, 144-51. Delp, S.L., Loan, J.P., Hoy, M.G., Zajac, F.E., Topp, E.L. and Rosen, J.M., 1990. An interactive graphics-based model of the lower extremity to study orthopaedic surgical procedures. IEEE Trans Biomed Eng 37, 757-67. Delp, S.L., Statler, K. and Carroll, N.C., 1995. Preserving plantar flexion strength after surgical treatment for contracture of the triceps surae: a computer simulation study. J Orthop Res 13, 96-104. DeLuca, P.A., Ounpuu, S., Davis, R.B. and Walsh, J.H., 1998. Effect of hamstring and psoas lengthening on pelvic tilt in patients with spastic diplegic cerebral palsy. J Pediatr Orthop 18, 712-8. Desloovere, K., Molenaers, G., Feys, H., Huenaerts, C., Callewaert, B. and Van de Walle, P., 2006. Do dynamic and static clinical measurements correlate with gait analysis parameters in children with cerebral palsy? Gait Posture 24, 302-13. Dhaher, Y.Y. and Kahn, L.E., 2002. The effect of vastus medialis forces on patello-femoral contact: a model-based study. J Biomech Eng 124, 758-67. Dietz, F.R., Albright, J.C. and Dolan, L., 2006. Medium-term follow-up of Achilles tendon lengthening in the treatment of ankle equinus in cerebral palsy. Iowa Orthop J 26, 27-32.

153
Dodd, K.J., Taylor, N.F. and Damiano, D.L., 2002. A systematic review of the effectiveness of strength-training programs for people with cerebral palsy. Arch Phys Med Rehabil 83, 1157-64. Dodd, K.J., Taylor, N.F. and Graham, H.K., 2003. A randomized clinical trial of strength training in young people with cerebral palsy. Dev Med Child Neurol 45, 652-7. Dodgin, D.A., De Swart, R.J., Stefko, R.M., Wenger, D.R. and Ko, J.Y., 1998. Distal tibial/fibular derotation osteotomy for correction of tibial torsion: review of technique and results in 63 cases. J Pediatr Orthop 18, 95-101. Dorn, T.W., Lin, Y.C. and Pandy, M.G., 2011. Estimates of muscle function in human gait depend on how foot-ground contact is modelled. Comput Methods Biomech Biomed Engin 15, 657-68. Drummond, D.S., Rogala, E., Templeton, J. and Cruess, R., 1974. Proximal hamstring release for knee flexion and crouched posture in cerebral palsy. J Bone Joint Surg Am 56, 1598-602. Eckstein, F., Faber, S., Muhlbauer, R., Hohe, J., Englmeier, K.H., Reiser, M. and Putz, R., 2002. Functional adaptation of human joints to mechanical stimuli. Osteoarthritis Cartilage 10, 44-50. Eek, M.N., Tranberg, R., Zugner, R., Alkema, K. and Beckung, E., 2008. Muscle strength training to improve gait function in children with cerebral palsy. Dev Med Child Neurol 50, 759-64. Eggers, G.W., 1952. Transplantation of hamstring tendons to femoral condyles in order to improve hip extension and to decrease knee flexion in cerebral spastic paralysis. J Bone Joint Surg Am 34 A, 827-30. Eggers, G.W. and Evans, E.B., 1963. Surgery in Cerebral Palsy. J Bone Joint Surg Am 45, 1275-305. Elder, G.C., Kirk, J., Stewart, G., Cook, K., Weir, D., Marshall, A. and Leahey, L., 2003. Contributing factors to muscle weakness in children with cerebral palsy. Dev Med Child Neurol 45, 542-50. Engsberg, J.R., Ross, S.A. and Collins, D.R., 2006. Increasing ankle strength to improve gait and function in children with cerebral palsy: a pilot study. Pediatr Phys Ther 18, 266-75. Faigenbaum, A.D., Kraemer, W.J., Blimkie, C.J., Jeffreys, I., Micheli, L.J., Nitka, M. and Rowland, T.W., 2009. Youth resistance training: updated position statement

154
paper from the national strength and conditioning association. J Strength Cond Res 23, S60-79. Farmer, S.E., 2003. Key factors in the development of lower limb co-ordination: implications for the acquisition of walking in children with cerebral palsy. Disabil Rehabil 25, 807-16. Fixsen, J.A., 1979. Surgical treatment of the lower limbs in cerebral palsy: a review. J R Soc Med 72, 761-5. Gage, J.R., 1990. Surgical treatment of knee dysfunction in cerebral palsy. Clin Orthop Relat Res 45-54. Gage, J.R. and Novacheck, T.F., 2001. An update on the treatment of gait problems in cerebral palsy. J Pediatr Orthop B 10, 265-74. Gage, J.R. and Schwartz, M.H., 2001. Dynamic deformities and lever arm considerations. In: Paley (Eds.), Principles of Deformity. Springer, Berlin, pp. 761-775. Gage, J.R. and Schwartz, M.H., 2004. Pathological gait and lever-arm dysfunction. In: Gage (Eds.), The Treatment of Gait Problems in Cerebral Palsy. Mac Keith Press, London, pp. 180-204. Galli, M., Cimolin, V., Crivellini, M. and Albertini, G., 2005. Gait analysis before and after gastrocnemius fascia lengthening in children with cerebral palsy. J Appl Biomater Biomech 3, 98-105. Galli, M., Cimolin, V., Crivellini, M. and Albertini, G., 2009. Long-term evaluation of isolated gastrocnemius fascia lengthening in children with cerebral palsy using gait analysis. J Pediatr Orthop B 18, 228-33. Gannotti, M.E., Gorton, G.E., 3rd, Nahorniak, M.T., Masso, P.D., Landry, B., Lyman, J., Sawicki, R., Hagedorn, K., Ross, E. and Warner, J., 2007. Postoperative gait velocity and mean knee flexion in stance of ambulatory children with spastic diplegia four years or more after multilevel surgery. J Pediatr Orthop 27, 451-6. Goldberg, S.R., Anderson, F.C., Pandy, M.G. and Delp, S.L., 2004. Muscles that influence knee flexion velocity in double support: implications for stiff-knee gait. J Biomech 37, 1189-96. Graham, H. and Selber, P., 2003. Musculoskeletal aspects of cerebral palsy. Journal of Bone & Joint Surgery, British Volume 85, 157-166.

155
Granata, K.P., Abel, M.F. and Damiano, D.L., 2000. Joint angular velocity in spastic gait and the influence of muscle-tendon lengthening. J Bone Joint Surg Am 82, 174-86. Green, W.T. and McDermott, L., 1942. Operative treatment of cerebral palsy of spastic type. Journal of the American Medical Association 118, 434. Grujic, H. and Aparisi, T., 1982. Distal hamstring tendon release in knee flexion deformity. Int Orthop 6, 103-6. Hamner, S.R., Seth, A. and Delp, S.L., 2010. Muscle contributions to propulsion and support during running. J Biomech 43, 2709-16. Hassani, S., Roh, J., Ferdjallah, M., Reiners, K., Kuo, K., Smith, P. and Harris, G., 2004. Rehabilitative orthotics evaluation in children with diplegic cerebral palsy: kinematics and kinetics. Conf Proc IEEE Eng Med Biol Soc 7, 4874-6. Healy, A., 1958. 2 Methods of Weight-Training for Children with Spastic Type of Cerebral-Palsy. Research Quarterly 29, 389-395. Healy, M.T., Schwartz, M.H., Stout, J.L., Gage, J.R. and Novacheck, T.F., 2011. Is simultaneous hamstring lengthening necessary when performing distal femoral extension osteotomy and patellar tendon advancement? Gait Posture 33, 1-5. Hernandez, A., Dhaher, Y. and Thelen, D.G., 2008. In vivo measurement of dynamic rectus femoris function at postures representative of early swing phase. J Biomech 41, 137-44. Hesse, S., Brandl-Hesse, B., Seidel, U., Doll, B. and Gregoric, M., 2000. Lower limb muscle activity in ambulatory children with cerebral palsy before and after the treatment with Botulinum toxin A. Restor Neurol Neurosci 17, 1-8. Hicks, J., Arnold, A., Anderson, F., Schwartz, M. and Delp, S., 2007. The effect of excessive tibial torsion on the capacity of muscles to extend the hip and knee during single-limb stance. Gait Posture 26, 546-52. Hicks, J.L., Delp, S.L. and Schwartz, M.H., 2011. Can biomechanical variables predict improvement in crouch gait? Gait Posture 34, 197-201. Hicks, J.L., Schwartz, M.H., Arnold, A.S. and Delp, S.L., 2008. Crouched postures reduce the capacity of muscles to extend the hip and knee during the single-limb stance phase of gait. J Biomech 41, 960-7. Hoffinger, S.A., Rab, G.T. and Abou-Ghaida, H., 1993. Hamstrings in cerebral palsy crouch gait. J Pediatr Orthop 13, 722-6.

156
Hsu, A.T., Perry, J., Gronley, J.K. and Hislop, H.J., 1993. Quadriceps force and myoelectric activity during flexed knee stance. Clin Orthop Relat Res 254-62. Hsu, L.C. and Li, H.S., 1990. Distal hamstring elongation in the management of spastic cerebral palsy. J Pediatr Orthop 10, 378-81. Hunter, B.V., Thelen, D.G. and Dhaher, Y.Y., 2009. A three-dimensional biomechanical evaluation of quadriceps and hamstrings function using electrical stimulation. IEEE Trans Neural Syst Rehabil Eng 17, 167-75. Inman, V.T., 1947. Functional aspects of the abductor muscles of the hip. J Bone Joint Surg Am 29, 607-19. Jahnsen, R., Villien, L., Aamodt, G., Stanghelle, J.K. and Holm, I., 2004. Musculoskeletal pain in adults with cerebral palsy compared with the general population. J Rehabil Med 36, 78-84. Jaric, S., Ugarkovic, D. and Kukolj, M., 2002. Evaluation of methods for normalizing muscle strength in elite and young athletes. J Sports Med Phys Fitness 42, 141-51. Johnson, D.C., Damiano, D.L. and Abel, M.F., 1997. The evolution of gait in childhood and adolescent cerebral palsy. J Pediatr Orthop 17, 392-6. Jonkers, I., Stewart, C. and Spaepen, A., 2003. The complementary role of the plantarflexors, hamstrings and gluteus maximus in the control of stance limb stability during gait. Gait & Posture 17, 264-272. Karol, L.A., Chambers, C., Popejoy, D. and Birch, J.G., 2008. Nerve palsy after hamstring lengthening in patients with cerebral palsy. J Pediatr Orthop 28, 773-6. Katz, K., Attias, J., Weigl, D., Cizger, A. and Bar-On, E., 2004. Monitoring of the sciatic nerve during hamstring lengthening by evoked EMG. J Bone Joint Surg Br 86, 1059-61. Keats, S. and Kambin, P., 1962. An evaluation of surgery for the correction of knee-flexion contracture in children with cerebral spastic paralysis. The Journal of Bone and Joint Surgery 44, 1146. Kerr, C., McDowell, B., Cosgrove, A., Walsh, D., Bradbury, I. and McDonough, S., 2006. Electrical stimulation in cerebral palsy: a randomized controlled trial. Dev Med Child Neurol 48, 870-6. Kimmel, S.A. and Schwartz, M.H., 2006. A baseline of dynamic muscle function during gait. Gait Posture 23, 211-21.

157
Klatt, J. and Stevens, P.M., 2008. Guided growth for fixed knee flexion deformity. J Pediatr Orthop 28, 626-31. Kramer, A. and Stevens, P.M., 2001. Anterior femoral stapling. J Pediatr Orthop 21, 804-7. Kuo, A.D., 1998. A least-squares estimation approach to improving the precision of inverse dynamics computations. J Biomech Eng 120, 148-59. Kutzner, I., Heinlein, B., Graichen, F., Bender, A., Rohlmann, A., Halder, A., Beier, A. and Bergmann, G., 2010. Loading of the knee joint during activities of daily living measured in vivo in five subjects. J Biomech 43, 2164-73. Lee, I.M. and Buchner, D.M., 2008. The importance of walking to public health. Med Sci Sports Exerc 40, S512-8. Lee, K.M., Chung, C.Y., Kwon, D.G., Han, H.S., Choi, I.H. and Park, M.S., 2011. Reliability of physical examination in the measurement of hip flexion contracture and correlation with gait parameters in cerebral palsy. J Bone Joint Surg Am 93, 150-8. Liao, H.F., Liu, Y.C., Liu, W.Y. and Lin, Y.T., 2007. Effectiveness of loaded sit-to-stand resistance exercise for children with mild spastic diplegia: a randomized clinical trial. Arch Phys Med Rehabil 88, 25-31. Lin, C.J., Guo, L.Y., Su, F.C., Chou, Y.L. and Cherng, R.J., 2000. Common abnormal kinetic patterns of the knee in gait in spastic diplegia of cerebral palsy. Gait Posture 11, 224-32. Liu, M.Q., Anderson, F.C., Pandy, M.G. and Delp, S.L., 2006. Muscles that support the body also modulate forward progression during walking. J Biomech 39, 2623-30. Liu, M.Q., Anderson, F.C., Schwartz, M.H. and Delp, S.L., 2008. Muscle contributions to support and progression over a range of walking speeds. J Biomech 41, 3243-52. Lloyd-Roberts, G.C., Jackson, A.M. and Albert, J.S., 1985. Avulsion of the distal pole of the patella in cerebral palsy. A cause of deteriorating gait. J Bone Joint Surg Br 67, 252-4. Lovejoy, S.A., Tylkowski, C., Oeffinger, D. and Sander, L., 2007. The effects of hamstring lengthening on hip rotation. J Pediatr Orthop 27, 142-6.

158
Lucareli, P.R., Lima Mde, O., Lucarelli, J.G. and Lima, F.P., 2007. Changes in joint kinematics in children with cerebral palsy while walking with and without a floor reaction ankle-foot orthosis. Clinics (Sao Paulo) 62, 63-8. Luyckx, T., Didden, K., Vandenneucker, H., Labey, L., Innocenti, B. and Bellemans, J., 2009. Is there a biomechanical explanation for anterior knee pain in patients with patella alta?: influence of patellar height on patellofemoral contact force, contact area and contact pressure. J Bone Joint Surg Br 91, 344-50. Ma, F.Y., Selber, P., Nattrass, G.R., Harvey, A.R., Wolfe, R. and Graham, H.K., 2006. Lengthening and transfer of hamstrings for a flexion deformity of the knee in children with bilateral cerebral palsy: technique and preliminary results. J Bone Joint Surg Br 88, 248-54. Matjacic, Z. and Olensek, A., 2007. Biomechanical characterization and clinical implications of artificially induced crouch walking: Differences between pure iliopsoas, pure hamstrings and combination of iliopsoas and hamstrings contractures. J Biomech 40, 491-501. McCubbin, J. and Shasby, G., 1985. Effects of isokinetic exercise on adolescents with cerebral palsy. Adapted Physical Activity Quarterly 2, 56-64. Metaxiotis, D., Wolf, S. and Doederlein, L., 2004. Conversion of biarticular to monoarticular muscles as a component of multilevel surgery in spastic diplegia. J Bone Joint Surg Br 86, 102-9. Mockford, M. and Caulton, J.M., 2008. Systematic review of progressive strength training in children and adolescents with cerebral palsy who are ambulatory. Pediatr Phys Ther 20, 318-33. Moreau, N.G., Teefey, S.A. and Damiano, D.L., 2009. In vivo muscle architecture and size of the rectus femoris and vastus lateralis in children and adolescents with cerebral palsy. Dev Med Child Neurol 51, 800-6. Mundermann, A., Dyrby, C.O., D'Lima, D.D., Colwell, C.W., Jr. and Andriacchi, T.P., 2008. In vivo knee loading characteristics during activities of daily living as measured by an instrumented total knee replacement. J Orthop Res 26, 1167-72. Murphy, K.P., 2009. Cerebral palsy lifetime care - four musculoskeletal conditions. Dev Med Child Neurol 51 Suppl 4, 30-7. Nene, A.V., Evans, G.A. and Patrick, J.H., 1993. Simultaneous multiple operations for spastic diplegia. Outcome and functional assessment of walking in 18 patients. J Bone Joint Surg Br 75, 488-94.

159
Neptune, R.R., Kautz, S.A. and Zajac, F.E., 2001. Contributions of the individual ankle plantar flexors to support, forward progression and swing initiation during walking. J Biomech 34, 1387-98. Neptune, R.R., Zajac, F.E. and Kautz, S.A., 2004. Muscle mechanical work requirements during normal walking: the energetic cost of raising the body's center-of-mass is significant. J Biomech 37, 817-25. Novacheck, T.F., Stout, J.L., Gage, J.R. and Schwartz, M.H., 2009. Distal femoral extension osteotomy and patellar tendon advancement to treat persistent crouch gait in cerebral palsy. Surgical technique. J Bone Joint Surg Am 91 Suppl 2, 271-86. Novacheck, T.F., Trost, J.P. and Schwartz, M.H., 2002. Intramuscular psoas lengthening improves dynamic hip function in children with cerebral palsy. J Pediatr Orthop 22, 158-64. O'Sullivan, R., Walsh, M., Kiernan, D. and O'Brien, T., 2010. The knee kinematic pattern associated with disruption of the knee extensor mechanism in ambulant patients with diplegic cerebral palsy. Clin Anat 23, 586-92. Opheim, A., Jahnsen, R., Olsson, E. and Stanghelle, J.K., 2009. Walking function, pain, and fatigue in adults with cerebral palsy: a 7-year follow-up study. Dev Med Child Neurol 51, 381-8. Orendurff, M.S., Aiona, M.D., Dorociak, R.D. and Pierce, R.A., 2002. Length and force of the gastrocnemius and soleus during gait following tendo Achilles lengthenings in children with equinus. Gait Posture 15, 130-5. Ounpuu, S., DeLuca, P., Davis, R. and Romness, M., 2002. Long-term effects of femoral derotation osteotomies: an evaluation using three-dimensional gait analysis. J Pediatr Orthop 22, 139-45. Papadonikolakis, A.S., Vekris, M.D., Korompilias, A.V., Kostas, J.P., Ristanis, S.E. and Soucacos, P.N., 2003. Botulinum A toxin for treatment of lower limb spasticity in cerebral palsy: gait analysis in 49 patients. Acta Orthop Scand 74, 749-55. Parker, D.F., Round, J.M., Sacco, P. and Jones, D.A., 1990. A cross-sectional survey of upper and lower limb strength in boys and girls during childhood and adolescence. Ann Hum Biol 17, 199-211. Patrick, J.H., 1996. Techniques of psoas tenotomy and rectus femoris transfer: "new" operations for cerebral palsy diplegia--a description. J Pediatr Orthop B 5, 242-6. Perry, J., 1992. Gait analysis: normal and pathological function. SLACK Inc., New Jersey.

160
Perry, J., Antonelli, D. and Ford, W., 1975. Analysis of knee-joint forces during flexed-knee stance. J Bone Joint Surg Am 57, 961-7. Pinheiro, J.C. and Bates, D.M., 2009. Mixed-effects models in S and S-PLUS. Springer Verlag, Pippenger, W.S. and Scalzitti, D.A., 2004. What are the effects, if any, of lower-extremity strength training on gait in children with cerebral palsy? Phys Ther 84, 849-58. Pollock, G.A., 1962. Surgical treatment of cerebral palsy. J Bone Joint Surg Br 44-B, 68-81. Pollock, G.A. and English, T.A., 1967. Transplantation of the hamstring muscles in cerebral palsy. J Bone Joint Surg Br 49, 80-6. Raja, K., Joseph, B., Benjamin, S., Minocha, V. and Rana, B., 2007. Physiological cost index in cerebral palsy: its role in evaluating the efficiency of ambulation. J Pediatr Orthop 27, 130-6. Ray, R.L. and Ehrlich, M.G., 1979. Lateral hamstring transfer and gait improvement in the cerebral palsy patient. J Bone Joint Surg Am 61, 719-23. Reimers, J., 1974. Contracture of the hamstrings in spastic cerebral palsy. A study of three methods of operative correction. J Bone Joint Surg Br 56, 102-9. Reinbolt, J., Fox, M., Arnold, A. and Delp, S.L., 2008. Importance of Preswing Rectus Femoris Activity in Stiff-Knee Gait. Journal of Biomechanics Rethlefsen, S., Kay, R., Dennis, S., Forstein, M. and Tolo, V., 1999. The effects of fixed and articulated ankle-foot orthoses on gait patterns in subjects with cerebral palsy. J Pediatr Orthop 19, 470-4. Riley, P.O. and Kerrigan, D.C., 1999. Kinetics of stiff-legged gait: induced acceleration analysis. IEEE Trans Rehabil Eng 7, 420-6. Rodda, J.M., Graham, H.K., Nattrass, G.R., Galea, M.P., Baker, R. and Wolfe, R., 2006. Correction of severe crouch gait in patients with spastic diplegia with use of multilevel orthopaedic surgery. J Bone Joint Surg Am 88, 2653-64. Rogozinski, B.M., Davids, J.R., Davis, R.B., 3rd, Jameson, G.G. and Blackhurst, D.W., 2009. The efficacy of the floor-reaction ankle-foot orthosis in children with cerebral palsy. J Bone Joint Surg Am 91, 2440-7.

161
Roosth, H.P., 1971. Flexion deformity of the hip and knee in spastic cerebral palsy: treatment by early release of spastic hip-flexor muscles. Journal of Bone and Joint Surgery 53-A, 1489-1510. Rose, G.E., Lightbody, K.A., Ferguson, R.G., Walsh, J.C. and Robb, J.E., 2010. Natural history of flexed knee gait in diplegic cerebral palsy evaluated by gait analysis in children who have not had surgery. Gait Posture 31, 351-4. Rose, J., Gamble, J.G., Burgos, A., Medeiros, J. and Haskell, W.L., 1990. Energy expenditure index of walking for normal children and for children with cerebral palsy. Dev Med Child Neurol 32, 333-40. Rose, J., Gamble, J.G., Medeiros, J., Burgos, A. and Haskell, W.L., 1989. Energy cost of walking in normal children and in those with cerebral palsy: comparison of heart rate and oxygen uptake. J Pediatr Orthop 9, 276-9. Rose, J. and McGill, K.C., 2005. Neuromuscular activation and motor-unit firing characteristics in cerebral palsy. Dev Med Child Neurol 47, 329-36. Rosenthal, R.K. and Levine, D.B., 1977. Fragmentation of the distal pole of the patella in spastic cerebral palsy. J Bone Joint Surg Am 59, 934-9. Rothman, K.J., 1990. No adjustments are needed for multiple testing. Epidemiology 1, 43-46. Ryan, D.D., Rethlefsen, S.A., Skaggs, D.L. and Kay, R.M., 2005. Results of tibial rotational osteotomy without concomitant fibular osteotomy in children with cerebral palsy. J Pediatr Orthop 25, 84-8. Sasaki, K. and Neptune, R., 2010. Individual muscle contributions to the axial knee joint contact force during normal walking. Journal of Biomechanics Schantz, P., Randall-Fox, E., Hutchison, W., Tyden, A. and Astrand, P.O., 1983. Muscle fibre type distribution, muscle cross-sectional area and maximal voluntary strength in humans. Acta Physiol Scand 117, 219-26. Scholtes, V.A., Dallmeijer, A.J., Knol, D.L., Speth, L.A., Maathuis, C.G., Jongerius, P.H. and Becher, J.G., 2006. The combined effect of lower-limb multilevel botulinum toxin type a and comprehensive rehabilitation on mobility in children with cerebral palsy: a randomized clinical trial. Arch Phys Med Rehabil 87, 1551-8. Scholtes, V.A., Dallmeijer, A.J., Knol, D.L., Speth, L.A., Maathuis, C.G., Jongerius, P.H. and Becher, J.G., 2007. Effect of multilevel botulinum toxin a and comprehensive rehabilitation on gait in cerebral palsy. Pediatr Neurol 36, 30-9.

162
Scholtes, V.A., Dallmeijer, A.J., Rameckers, E.A., Verschuren, O., Tempelaars, E., Hensen, M. and Becher, J.G., 2008. Lower limb strength training in children with cerebral palsy--a randomized controlled trial protocol for functional strength training based on progressive resistance exercise principles. BMC Pediatr 8, 41. Schutte, L.M., Hayden, S.W. and Gage, J.R., 1997. Lengths of hamstrings and psoas muscles during crouch gait: effects of femoral anteversion. J Orthop Res 15, 615-21. Schwartz, M. and Lakin, G., 2003. The effect of tibial torsion on the dynamic function of the soleus during gait. Gait Posture 17, 113-8. Scianni, A., Butler, J.M., Ada, L. and Teixeira-Salmela, L.F., 2009. Muscle strengthening is not effective in children and adolescents with cerebral palsy: a systematic review. Aust J Physiother 55, 81-7. Segal, L.S., Thomas, S.E., Mazur, J.M. and Mauterer, M., 1989. Calcaneal gait in spastic diplegia after heel cord lengthening: a study with gait analysis. J Pediatr Orthop 9, 697-701. Selber, P., Filho, E.R., Dallalana, R., Pirpiris, M., Nattrass, G.R. and Graham, H.K., 2004. Supramalleolar derotation osteotomy of the tibia, with T plate fixation. Technique and results in patients with neuromuscular disease. J Bone Joint Surg Br 86, 1170-5. Seymour, N. and Sharrard, W.J., 1968. Bilateral proximal release of the hamstrings in cerebral palsy. J Bone Joint Surg Br 50, 274-7. Sharps, C.H., Clancy, M. and Steel, H.H., 1984. A long-term retrospective study of proximal hamstring release for hamstring contracture in cerebral palsy. J Pediatr Orthop 4, 443-7. Sheehan, F.T., Seisler, A.R. and Alter, K.E., 2008. Three-dimensional in vivo quantification of knee kinematics in cerebral palsy. Clin Orthop Relat Res 466, 450-8. Shelburne, K.B., Torry, M.R. and Pandy, M.G., 2005. Muscle, ligament, and joint-contact forces at the knee during walking. Med Sci Sports Exerc 37, 1948-56. Smith, J.T. and Stevens, P.M., 1989. Combined adductor transfer, iliopsoas release, and proximal hamstring release in cerebral palsy. J Pediatr Orthop 9, 1-5. Steele, K.M., Seth, A., Hicks, J.L., Schwartz, M.S. and Delp, S.L., 2010. Muscle contributions to support and progression during single-limb stance in crouch gait. J Biomech 43, 2099-2105.

163
Stefko, R.M., de Swart, R.J., Dodgin, D.A., Wyatt, M.P., Kaufman, K.R., Sutherland, D.H. and Chambers, H.G., 1998. Kinematic and kinetic analysis of distal derotational osteotomy of the leg in children with cerebral palsy. J Pediatr Orthop 18, 81-7. Steinwender, G., Saraph, V., Zwick, E.B., Uitz, C. and Linhart, W., 2000. Assessment of hip rotation after gait improvement surgery in cerebral palsy. Acta Orthop Belg 66, 259-64. Stewart, C., Postans, N., Schwartz, M.H., Rozumalski, A. and Roberts, A., 2007. An exploration of the function of the triceps surae during normal gait using functional electrical stimulation. Gait Posture 26, 482-8. Stewart, C., Postans, N., Schwartz, M.H., Rozumalski, A. and Roberts, A.P., 2008. An investigation of the action of the hamstring muscles during standing in crouch using functional electrical stimulation (FES). Gait Posture 28, 372-7. Stout, J.L., Gage, J.R., Schwartz, M.H. and Novacheck, T.F., 2008. Distal femoral extension osteotomy and patellar tendon advancement to treat persistent crouch gait in cerebral palsy. J Bone Joint Surg Am 90, 2470-84. Sutherland, D.H. and Cooper, L., 1978. The pathomechanics of progressive crouch gait in spastic diplegia. Orthop Clin North Am 9, 143-54. Sutherland, D.H., Cooper, L. and Daniel, D., 1980. The role of the ankle plantar flexors in normal walking. J Bone Joint Surg Am 62, 354-63. Sutherland, D.H., Kaufman, K.R., Wyatt, M.P. and Chambers, H.G., 1996. Injection of botulinum A toxin into the gastrocnemius muscle of patients with cerebral palsy: a 3-dimensional motion analysis study. Gait & Posture 4, 269-279. Sutherland, D.H., Zilberfarb, J.L., Kaufman, K.R., Wyatt, M.P. and Chambers, H.G., 1997. Psoas release at the pelvic brim in ambulatory patients with cerebral palsy: operative technique and functional outcome. Journal of Pediatric Orthopaedics 17, 563-70. Thelen, D.G. and Anderson, F.C., 2006. Using computed muscle control to generate forward dynamic simulations of human walking from experimental data. J Biomech 39, 1107-15. Thelen, D.G., Anderson, F.C. and Delp, S.L., 2003. Generating dynamic simulations of movement using computed muscle control. J Biomech 36, 321-8. Thomas, S.S., Moore, C., Kelp-Lenane, C. and Norris, C., 1996. Simulated gait patterns: the resulting effects on gait parameters, dynamic electromyography, joint moments, and physiological cost index. Gait & Posture 4, 100-107.

164
Thometz, J., Simon, S. and Rosenthal, R., 1989. The effect on gait of lengthening of the medial hamstrings in cerebral palsy. J Bone Joint Surg Am 71, 345-53. Thompson, N.S., Baker, R.J., Cosgrove, A.P., Corry, I.S. and Graham, H.K., 1998. Musculoskeletal modelling in determining the effect of botulinum toxin on the hamstrings of patients with crouch gait. Dev Med Child Neurol 40, 622-5. Thompson, N.S., Baker, R.J., Cosgrove, A.P., Saunders, J.L. and Taylor, T.C., 2001. Relevance of the popliteal angle to hamstring length in cerebral palsy crouch gait. J Pediatr Orthop 21, 383-7. Tudor-Locke, C., Bassett, D.R., Swartz, A.M., Strath, S.J., Parr, B.B., Reis, J.P., Dubose, K.D. and Ainsworth, B.E., 2004. A preliminary study of one year of pedometer self-monitoring. Ann Behav Med 28, 158-62. Tuzson, A.E., Granata, K.P. and Abel, M.F., 2003. Spastic velocity threshold constrains functional performance in cerebral palsy. Arch Phys Med Rehabil 84, 1363-8. Unger, M., Faure, M. and Frieg, A., 2006. Strength training in adolescent learners with cerebral palsy: a randomized controlled trial. Clin Rehabil 20, 469-77. van der Krogt, M.M., Delp, S.L. and Schwartz, M.H., 2012. How robust is human gait to muscle weakness? Gait Posture 36, 113-9. van der Krogt, M.M., Doorenbosch, C.A. and Harlaar, J., 2007. Muscle length and lengthening velocity in voluntary crouch gait. Gait Posture 26, 532-8. van der Linden, M.L., Aitchison, A.M., Hazlewood, M.E., Hillman, S.J. and Robb, J.E., 2003. Effects of surgical lengthening of the hamstrings without a concomitant distal rectus femoris transfer in ambulant patients with cerebral palsy. J Pediatr Orthop 23, 308-13. Vlachou, M., Pierce, R., Davis, R.M. and Sussman, M., 2009. Does tendon lengthening surgery affect muscle tone in children with cerebral palsy? Acta Orthop Belg 75, 808-14. Ward, S.R., Terk, M.R. and Powers, C.M., 2005. Influence of patella alta on knee extensor mechanics. J Biomech 38, 2415-22. Waters, R.L. and Mulroy, S., 1999. The energy expenditure of normal and pathologic gait. Gait Posture 9, 207-31.

165
Wesdock, K.A. and Edge, A.M., 2003. Effects of wedged shoes and ankle-foot orthoses on standing balance and knee extension in children with cerebral palsy who crouch. Pediatr Phys Ther 15, 221-31. Westberry, D.E., Davids, J.R., Jacobs, J.M., Pugh, L.I. and Tanner, S.L., 2006. Effectiveness of serial stretch casting for resistant or recurrent knee flexion contractures following hamstring lengthening in children with cerebral palsy. J Pediatr Orthop 26, 109-14. Wiley, M.E. and Damiano, D.L., 1998. Lower-extremity strength profiles in spastic cerebral palsy. Dev Med Child Neurol 40, 100-7. Wong, M. and Carter, D.R., 2003. Articular cartilage functional histomorphology and mechanobiology: a research perspective. Bone 33, 1-13. Woratanarat, P., Dabney, K.W. and Miller, F., 2009. [Knee capsulotomy for fixed knee flexion contracture]. Acta Orthop Traumatol Turc 43, 121-7. Wren, T.A., Rethlefsen, S. and Kay, R.M., 2005. Prevalence of specific gait abnormalities in children with cerebral palsy: influence of cerebral palsy subtype, age, and previous surgery. J Pediatr Orthop 25, 79-83. Yamaguchi, G.T. and Zajac, F.E., 1989. A planar model of the knee joint to characterize the knee extensor mechanism. J Biomech 22, 1-10. Yeargin-Allsopp, M., Van Naarden Braun, K., Doernberg, N.S., Benedict, R.E., Kirby, R.S. and Durkin, M.S., 2008. Prevalence of cerebral palsy in 8-year-old children in three areas of the United States in 2002: a multisite collaboration. Pediatrics 121, 547-54. Young, J.L., Rodda, J., Selber, P., Rutz, E. and Graham, H.K., 2010. Management of the knee in spastic diplegia: what is the dose? Orthop Clin North Am 41, 561-77. Zajac, F.E., 1989. Muscle and tendon: properties, models, scaling, and application to biomechanics and motor control. Crit Rev Biomed Eng 17, 359-411. Zajac, F.E. and Gordon, M.E., 1989. Determining muscle's force and action in multi-articular movement. Exerc Sport Sci Rev 17, 187-230. Zhao, D., Banks, S.A., Mitchell, K.H., D'Lima, D.D., Colwell, C.W., Jr. and Fregly, B.J., 2007. Correlation between the knee adduction torque and medial contact force for a variety of gait patterns. J Orthop Res 25, 789-97.

166
Zwick, E.B., Saraph, V., Zwick, G., Steinwender, C., Linhart, W.E. and Steinwender, G., 2002. Medial hamstring lengthening in the presence of hip flexor tightness in spastic diplegia. Gait Posture 16, 288-96.

167
APPENDIX A: CHAPTER 3 SUPPLEMENTARY MATERIAL A.1 EFFECTS OF CONSTRAINING EMG ON MUSCLE CONTRIBUTIONS
A comparison of estimated activations to normalized EMG (gray area) before (dashed line) and after (solid line) constraints were applied to improve agreement between the timing, normalized magnitude, and shape for one subject.
0
0.2
0.4
0.6
0.8
1
0
0.2
0.4
0.6
0.8
1
0
0.2
0.4
0.6
0.8
1
0
0.2
0.4
0.6
0.8
1
0
0.2
0.4
0.6
0.8
1
0
0.2
0.4
0.6
0.8
1
0
0.2
0.4
0.6
0.8
1
0
0.2
0.4
0.6
0.8
1
0
0.2
0.4
0.6
0.8
1
0
0.2
0.4
0.6
0.8
1
Rectus Femoris
Stance Limb
Medial Hamstrings
20 30 40 50 70 80 90 100
20 30 40 50 70 80 90 100
20 30 40 50 70 80 90 100
20 30 40 50 70 80 90 100
20 30 40 50 70 80 90 100
Lateral Hamstrings
Anterior Tibialis
Gastrocnemius
EMGUnconstrained ActivationConstrained Activation
Swing Limb
Nor
mal
ized
Act
ivat
ion
Nor
mal
ized
Act
ivat
ion
Nor
mal
ized
Act
ivat
ion
Nor
mal
ized
Act
ivat
ion
Nor
mal
ized
Act
ivat
ion
% Gait Cycle % Gait Cycle

168
Hip, knee, and ankle accelerations with and without constraining activations to EMG as shown above. Positive and negative accelerations correspond to extension and flexion, respectively. The average change in the magnitude of each muscle’s contribution to acceleration was 16, 16, and 15% at the hip, knee, and ankle, respectively.

169
A comparison of mass center contributions before (solid gray lines) and after (dotted red lines) constraining activations to EMG as shown above. Each line represents the direction of the horizontal and vertical acceleration generated at 5% increments through single-limb stance. The scale of the horizontal accelerations are equivalent to the vertical scale. The magnitude of vertical and horizontal mass center accelerations generated by each muscle changed by 10 and 3%, on average. Note that there are small changes in magnitude; however, the direction of the acceleration does not change after constraining the activations.

170

171
A.2 MASS CENTER AND JOINT ACCELERATIONS FROM ALL MUSCLES
Average acceleration generated at the mass center by all muscle compartments of the stance limb. Each line represents the direction of the horizontal and vertical accelerations generated by a muscle at 5% increments through single-limb stance. The scale of the horizontal accelerations are equivalent to the vertical scale.
Gluteus mediusGluteus medius 1 Gluteus medius 2 Gluteus medius 3
Acce
lera
tion
(m/s
2 )
0
0.5
1
1.5
0
0.5
1
1.5
0
0.5
1
1.5
Gluteus mediusGluteus medius 1 Gluteus medius 2 Gluteus medius 3
Acce
lera
tion
(m/s
2 )
0
0.5
1
1.5
0
0.5
1
1.5
0
0.5
1
1.5
0
0.5
1
1.5
0
0.5
1
1.5
0
0.5
1
1.5
UP
FORWARD
Crouch GaitUnimpaired Gait
Gluteus minimusGluteus minimus 1 Gluteus minimus 2 Gluteus minimus 3
Acce
lera
tion
(m/s
2 )
0
0.2
0.4
0
0.2
0.4
0
0.2
0.4
Gluteus minimusGluteus minimus 1 Gluteus minimus 2 Gluteus minimus 3
Acce
lera
tion
(m/s
2 )
0
0.2
0.4
0
0.2
0.4
0
0.2
0.4
0
0.2
0.4
0
0.2
0.4
0
0.2
0.4
Hamstrings
Acce
lera
tion
(m/s
2 )
Semimembranosus Semitendinosus Biceps femoris long head Biceps femoris short head
-0.4
-0.2
0
0.2
0.4
-0.4
-0.2
0
0.2
0.4
-0.4
-0.2
0
0.2
0.4
-0.4
-0.2
0
0.2
0.4
Hamstrings
Acce
lera
tion
(m/s
2 )
Semimembranosus Semitendinosus Biceps femoris long head Biceps femoris short head
-0.4
-0.2
0
0.2
0.4
-0.4
-0.2
0
0.2
0.4
-0.4
-0.2
0
0.2
0.4
-0.4
-0.2
0
0.2
0.4
-0.4
-0.2
0
0.2
0.4
-0.4
-0.2
0
0.2
0.4
-0.4
-0.2
0
0.2
0.4
-0.4
-0.2
0
0.2
0.4
Hip flexorsIliacus Psoas Sartorius
Acce
lera
tion
(m/s
2 )
-0.6
-0.4
-0.2
0
-0.6
-0.4
-0.2
0
-0.6
-0.4
-0.2
0
Hip flexorsIliacus Psoas Sartorius
Acce
lera
tion
(m/s
2 )
-0.6
-0.4
-0.2
0
-0.6
-0.4
-0.2
0
-0.6
-0.4
-0.2
0
-0.6
-0.4
-0.2
0
-0.6
-0.4
-0.2
0
-0.6
-0.4
-0.2
0
OtherTensor fascia lata Quadratus Femoris Gemmelus Piriformus
Acce
lera
tion
(m/s
2 )
-0.2
0
0.2
0.4
0.6
-0.2
0
0.2
0.4
0.6
-0.2
0
0.2
0.4
0.6
-0.2
0
0.2
0.4
0.6
-0.2
0
0.2
0.4
0.6
-0.2
0
0.2
0.4
0.6
-0.2
0
0.2
0.4
0.6
-0.2
0
0.2
0.4
0.6
Gluteus maximusGluteus maximus 1 Gluteus maximus 2 Gluteus maximus 3
Acce
lera
tion
(m/s
2 )
0
0.2
0.4
0.6
0.8
1
1.2
0
0.2
0.4
0.6
0.8
1
1.2
0
0.2
0.4
0.6
0.8
1
1.2
Gluteus maximusGluteus maximus 1 Gluteus maximus 2 Gluteus maximus 3
Acce
lera
tion
(m/s
2 )
0
0.2
0.4
0.6
0.8
1
1.2
0
0.2
0.4
0.6
0.8
1
1.2
0
0.2
0.4
0.6
0.8
1
1.2
0
0.2
0.4
0.6
0.8
1
1.2
0
0.2
0.4
0.6
0.8
1
1.2
0
0.2
0.4
0.6
0.8
1
1.2

172
UP
FORWARD
Crouch GaitUnimpaired Gait
Hip adductorsAdductor magnus 1 Adductor magnus 2 Adductor magnus 3 Adductor Longus
Adductor brevis Pectineus Gracilis
Acce
lera
tion
(m/s
2 )A
ccel
erat
ion
(m/s
2 )
-0.4
-0.2
0
-0.4
-0.2
0
-0.4
-0.2
0
-0.4
-0.2
0
-0.4
-0.2
0
-0.4
-0.2
0
-0.4
-0.2
0
Hip adductorsAdductor magnus 1 Adductor magnus 2 Adductor magnus 3 Adductor Longus
Adductor brevis Pectineus Gracilis
Acce
lera
tion
(m/s
2 )A
ccel
erat
ion
(m/s
2 )
-0.4
-0.2
0
-0.4
-0.2
0
-0.4
-0.2
0
-0.4
-0.2
0
-0.4
-0.2
0
-0.4
-0.2
0
-0.4
-0.2
0
-0.4
-0.2
0
-0.4
-0.2
0
-0.4
-0.2
0
-0.4
-0.2
0
-0.4
-0.2
0
-0.4
-0.2
0
-0.4
-0.2
0
QuadricepsRectus femoris Vastus medialis Vastus intermedius Vastus lateralis
Acc
eler
atio
n (m
/s2 )
0
1
2
3
0
1
2
3
0
1
2
3
0
1
2
3
QuadricepsRectus femoris Vastus medialis Vastus intermedius Vastus lateralis
Acc
eler
atio
n (m
/s2 )
0
1
2
3
0
1
2
3
0
1
2
3
0
1
2
3
0
1
2
3
0
1
2
3
0
1
2
3
0
1
2
3
Ankle plantarflexorsMedial gastrocnemius Lateral gastrocnemius Soleus Tibialis posterior
Acc
eler
atio
n (m
/s2 )
0
1
2
3
4
5
6
0
1
2
3
4
5
6
0
1
2
3
4
5
6
0
1
2
3
4
5
6
Ankle plantarflexorsMedial gastrocnemius Lateral gastrocnemius Soleus Tibialis posterior
Acc
eler
atio
n (m
/s2 )
0
1
2
3
4
5
6
0
1
2
3
4
5
6
0
1
2
3
4
5
6
0
1
2
3
4
5
6
0
1
2
3
4
5
6
0
1
2
3
4
5
6
0
1
2
3
4
5
6
0
1
2
3
4
5
6
OtherTibialis anterior Peroneus brevis Peroneus longus Peroneus tertius
Flexor digitorum longus Flexor hallicus longus Extensor digitorum longus Extensor hallicus longus
Acce
lera
tion
(m/s
2 )A
ccel
erat
ion
(m/s
2 )
-1
-0.8
-0.6
-0.4
-0.2
0
0.2
-1
-0.8
-0.6
-0.4
-0.2
0
0.2
-1
-0.8
-0.6
-0.4
-0.2
0
0.2
-1
-0.8
-0.6
-0.4
-0.2
0
0.2
-0.4
-0.2
0
-0.4
-0.2
0
-0.4
-0.2
0
-0.4
-0.2
0
OtherTibialis anterior Peroneus brevis Peroneus longus Peroneus tertius
Flexor digitorum longus Flexor hallicus longus Extensor digitorum longus Extensor hallicus longus
Acce
lera
tion
(m/s
2 )A
ccel
erat
ion
(m/s
2 )
-1
-0.8
-0.6
-0.4
-0.2
0
0.2
-1
-0.8
-0.6
-0.4
-0.2
0
0.2
-1
-0.8
-0.6
-0.4
-0.2
0
0.2
-1
-0.8
-0.6
-0.4
-0.2
0
0.2
-1
-0.8
-0.6
-0.4
-0.2
0
0.2
-1
-0.8
-0.6
-0.4
-0.2
0
0.2
-1
-0.8
-0.6
-0.4
-0.2
0
0.2
-1
-0.8
-0.6
-0.4
-0.2
0
0.2
-0.4
-0.2
0
-0.4
-0.2
0
-0.4
-0.2
0
-0.4
-0.2
0
-0.4
-0.2
0
-0.4
-0.2
0
-0.4
-0.2
0
-0.4
-0.2
0

173
Average angular acceleration (± 1 standard deviation) generated at the hip, knee, and ankle by all muscle compartments of the stance limb during single-limb stance in crouch gait.
Gluteus maximus
Gluteus mediusGluteus medius 1 Gluteus medius 2 Gluteus medius 3
Acce
lera
tion
(deg
/s2 )
Gluteus minimusGluteus minimus 1 Gluteus minimus 2 Gluteus minimus 3
Acce
lera
tion
(deg
/s2 )
Hamstrings
Acce
lera
tion
(deg
/s2 )
Semimembranosus Semitendinosus Biceps femoris long head Biceps femoris short head
Hip flexorsIliacus Psoas Sartorius
Gluteus maximus 1 Gluteus maximus 2 Gluteus maximus 3Ac
cele
ratio
n (d
eg/s
2 )Ac
cele
ratio
n (d
eg/s
2 )
OtherTensor fascia lata Quadratus Femoris Gemmelus Piriformus
Acce
lera
tion
(deg
/s2 )
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
HipKneeAnkle

174
Hip adductorsAdductor magnus 1 Adductor magnus 2 Adductor magnus 3 Adductor Longus
Adductor brevis Pectineus Gracilis
Acce
lera
tion
(deg
/s2 )
Acc
eler
atio
n (d
eg/s
2 )
QuadricepsRectus femoris Vastus medialis Vastus intermedius Vastus lateralis
Ankle plantarflexorsMedial gastrocnemius Lateral gastrocnemius Soleus Tibialis posterior
OtherTibialis anterior Peroneus brevis Peroneus longus Peroneus tertius
Flexor digitorum longus Flexor hallicus longus Extensor digitorum longus Extensor hallicus longus
Acce
lera
tion
(deg
/s2 )
Acce
lera
tion
(deg
/s2 )
Acc
eler
atio
n (d
eg/s
2 )Ac
cele
ratio
n (d
eg/s
2 )
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
-5000
0
5000
HipKneeAnkle

175
APPENDIX B: CHAPTER 5 SUPPLEMENTARY MATERIAL B.1: CALCULATING JOINT FORCES IN OPENSIM
The joint reaction analysis in OpenSim applies a general method to calculate
joint loads transferred between two contacting bodies. This method computes the
resultant forces and moments that represent the internal loads carried by the joint
structure. For example, this study reports joint forces representing the sum of contact
forces between the tibial and femoral cartilage and all ligament forces crossing the
tibiofemoral joint.
OpenSim uses multibody dynamics and simulation methods from Simbody, a
free and open source library for representing rigid body dynamics
(https://simtk.org/home/simbody). Simbody constructs models as tree structures in
which rigid bodies connect in kinematic chains that can branch with joints or
reconnect with constraints. The equations of motion of the system are represented in
terms of the generalized coordinates and generalized forces of the model. Solving
these generalized equations of motion does not require calculating internal forces,
such as the joint contact forces. Therefore, the joint reaction analysis in OpenSim
incorporates a post-processing procedure that uses the muscle forces and joint
kinematics to calculate resultant joint loads.
Figure B.1 shows an example model consisting of segments linked in a
kinematic chain. Joints between these segments do not need to have classical
engineering definitions, such as a revolute joint or spherical joint, but instead can have
more physiologic descriptions. For example, the motion between body segments

176
and may be described by splines that couple the rotations and translations of the
knee. For each time point in an analysis, a recursive operation begins with the most
distal bodies and progresses proximally to calculate the joint loads. The force at each
joint is calculated by performing a force balance on the body distal to the joint.
A single step in this recursive procedure is analogous to constructing a free
body diagram for each rigid body and resolving the point load that must be applied to
Figure B.1: (A) Example kinematic chain of body segments that can be represented in OpenSim. The joint between body segments Si and Si-1 is described by splines that represent an elliptical surface (Seth et al., 2010) and thus need not be an idealized pin joint. (B) Single-body system used to calculate , the reaction load at the proximal joint of Si. The calculation is in terms of Si’s inertial forces, muscle forces (black arrows), other external forces, and the previously calculated reaction force at the distal joint.

177
the joint to balance the forces and motions of the body. To calculate , the resultant
forces and moments at joint i, the body distal to joint i, , is treated as an independent
body with known kinematics in a global reference frame. In the example system
(Figure B.1), represents the six dimensional vector of known angular and linear
accelerations of . Since these accelerations are reconstructed from Simbody’s
generalized equations of motion, they capture any kinematic complexity in the joint
description. and represent the previously calculated forces and
moments applied by external loads and musculotendon actuators respectively.
represents the joint reaction load applied at the distal joint. is known since it
was calculated in the previous recursive step. Using the known generalized
coordinates ( ) and generalized speeds ( ) of the body segment and all other applied
forces, the desired resultant force is calculated as the vector sum:
∑ ∑
The sum requires that all terms be described in a common reference frame located at
the body origin, thus is the joint force and moment expressed at the body origin.
is the six-by-six mass matrix for body segment i. represents
constraint forces applied to the body, if applicable. Since the all terms other than
result from generalized coordinates and forces previously solved by Simbody, we can
calculate the moment and force at the body origin, and , that are required to
balance the equation. Finally, expressed at the body origin is shifted to an
equivalent moment and force, and , at the joint center:

178
0
where is the vector pointing from the body origin to the joint location.
The joint reaction analysis algorithm is available in OpenSim versions 1.9 and
later. The value of this algorithm is that it leverages the generalized coordinate
representation and rich set of joint definitions provided by Simbody and OpenSim and
provides a free tool for researchers to use to calculate joint loads for any
musculoskeletal structure.