Embed Size (px)
Citation preview
Journal of Health Economics 26 (2007) 358–372
The earnings of U.S. health economists
John Cawley a,∗, Michael A. Morrisey b
a Department of Policy Analysis and Management, Cornell University,124 MVR Hall, Ithaca, NY 14853, United States
b Department of Health Care Organization and Policy, and Lister Hill Center for Health Policy,University of Alabama at Birmingham, United States
Received 28 April 2006; received in revised form 20 October 2006; accepted 24 October 2006Available online 28 November 2006
Abstract
This paper presents data from a 2005 survey of health economists who were U.S. members of the Interna-tional Health Economics Association or the Health Economics Special Interest Group of Academy Health.We present summary statistics of health economist earnings by rank and type of employer, estimate logearnings models as a function of education, experience, type of employer, and research productivity, andprovide summary statistics of starting salaries expected to be offered to new Ph.D. health economists bytype of employer. Our findings are compared to those for economics departments, business schools, schoolsof public health, and for health services researchers.© 2006 Elsevier B.V. All rights reserved.
JEL classification: I10; J44; I2
Keywords: Earnings; Labor market; Consulting; Salary
1. Introduction
The earnings of health economists are of interest because of the newness of the field, the varietyof educational entry points into the field, and the wide diffusion of health economists acrossdisparate academic units, government, and private sector employers. The first comprehensivestudy of the employment conditions of health economics was conducted in 1989 by Feldman andMorrisey (1990). This paper presents the results of a follow-up survey of health economists thatwas conducted in the Fall of 2005.
∗ Corresponding author at: Department of Policy Analysis and Management, Cornell University, 124 MVR Hall, Ithaca,NY 14853, USA. Tel.: +1 607 255 0952; fax: +1 607 255 4071.
E-mail address: [email protected] (J. Cawley).
0167-6296/$ – see front matter © 2006 Elsevier B.V. All rights reserved.doi:10.1016/j.jhealeco.2006.10.008

J. Cawley, M.A. Morrisey / Journal of Health Economics 26 (2007) 358–372 359
The research questions answered in this paper are: How much do health economists earn, bytype of employer and by academic rank? To what extent are type of degree, graduate program,experience and research productivity correlated with higher earnings? What factors influencethe probability that academics earn any consulting income, and the amount of consulting incomeearned conditional on earning any? In this paper we present summary statistics of health economistearnings by type of employer and by academic rank, estimate log earnings models as a function ofeducation, type of employer, experience, and research productivity, and provide summary statisticsof starting salaries expected to be offered to new Ph.D. health economists by type of employer.
2. Data: 2005 Survey of U.S. Health Economists
The survey was developed by the authors with the input and feedback of an advisory com-mittee consisting of Roger Feldman (chair), Sharon Arnold, Dick Arnould, Kate Bundorf, MikeHagan, Dave Knutson, and Kristine Metter. Email invitations and two follow-up reminders totake the survey were sent to a non-duplicated total of 1439 U.S. members of the InternationalHealth Economics Association (iHEA) and/or the Health Economics Interest Group of AcademyHealth. While there is an overlap in membership between the two organizations, the survey pro-cess prevented dual members from responding more than once. The online survey was openbetween October 24, 2005 and November 21, 2005 and was completed by 460 respondents, for aresponse rate of 32%. The relatively low response rate raises the issue of the generalizability ofthe findings. The direction of non-response bias, if any, is unclear. On the one hand, those withhigher opportunity costs of time may be less likely to respond and as a result we may underesti-mate salaries by rank. On the other hand, those with stronger interest in the survey topic may bemore likely to respond. Out of 460 respondents, 101 consider themselves to be neither a healtheconomist nor an economist who works in health; non-respondents may disproportionately fit thatcategorization.
Our response rate of 32% is lower than the response rate of 43% for a 2002 survey of healthservices researchers conducted by Academy Health (Resnick and Luft, 2004) and that of 54% forthe 1989 survey of health economists (Feldman and Morrisey, 1990). This decline in responserates by health economists and health services researchers is consistent with the general downwardtrend in survey response rates since the early 1990s (Biener et al., 2004). Studies have found noimpact of the decline in response rates on non-response bias (Curtin et al., 2000; Keeter et al.,2000) or the representation of population sub-groups (Biener et al., 2004).
This paper focuses on the responses to three survey questions. The first concerns primaryearnings: “In the last 12 months period, how much did you earn from your primary employer(including summer support, bonuses, and profit sharing but not housing allowance)?” The secondconcerns consulting income: “Over the past three years, how much do you earn PER YEAR outsideof your primary employment (e.g. book royalties, consultant or expert witness fees, etc.)?” Thethird question we focus on here concerns the salary offered to new health economists: “Whatis the approximate salary your department/agency/firm would pay for a newly minted Ph.D. ineconomics with a specialization in health?”
We excluded from the sample the following respondents: people who do not consider them-selves to be either a health economist or an economist who works on health topics (N = 101),those without a doctoral degree (N = 89), the self-employed (N = 10), unemployed (N = 7), orretired (N = 5), full-time graduate students (N = 36), and postdoctoral fellows (N = 12). These arenot unique individuals; for example, some respondents may be graduate students without a doc-toral degree; in that case they would be counted in two of those categories. The exclusions above

360 J. Cawley, M.A. Morrisey / Journal of Health Economics 26 (2007) 358–372
add up to 260 but only 163 unique individuals are deleted by those criteria, leaving us with asample of 297. Of these, we lack earnings data on 22, and missing data on other variables that weinclude in our earnings regressions reduce the sample to 222–145 academics and 77 working inthe government or private sector.
Four respondents appeared to list their earnings in increments of thousands (e.g. 100, 150,200); we multiply these four salaries by 1000. We are not able to determine whether consultingincomes reported in three digits were also intended to be interpreted as increments of thousands,so no similar adjustment was made.
3. Methods and empirical results
3.1. Earnings from primary employer: distribution and summary statistics
We start by presenting the distribution of responses. Fig. 1 depicts the distribution of earningsfrom the primary employer in the past 12 months (which includes any summer money) for aca-demics of all ranks. Each bar in the histogram is $5000 wide. Due to outliers with high salaries,the mean ($114,573, indicated by the dashed line) exceeds the median ($100,000, indicated bythe dotted line).
Fig. 2 presents the distribution of past-year earnings for nonacademics. Again, due to out-liers with high salaries, the mean ($128,566, indicated by the dashed line) exceeds the median($118,500, indicated by the dotted line).
Summary statistics of health economists’ salaries by basic characteristics are presented inTable 1. For all health economists in 2005, the average earnings from the primary employer in thelast 12 months are $119,499. Average salaries differ by sector of employment. The average salaryof health economists employed in the academy ($114,573) is $13,933 lower than that of health
Fig. 1. Academic health economists’ 12-month earnings from primary employer. Notes: (1) The dotted line indicates themedian ($100,000) and the dashed line indicates the mean ($114,573). (2) The histogram bars are in $5000 increments.

J. Cawley, M.A. Morrisey / Journal of Health Economics 26 (2007) 358–372 361
Fig. 2. Non-academic health economists’ 12-month earnings from primary employer. Notes: (1) The dotted line indicatesthe median ($118,500) and the dashed line indicates the mean ($128,566). (2) The histogram bars are in $5000 increments.
economists employed outside the academy ($128,566); this difference is statistically significantat the 5% level. This difference is driven by the salary gap for health economists with doctoratesother than an economics Ph.D. (e.g. Ph.D. in health services research or Sc.D. in economics); forthis group, the average salary in the academy ($99,333) is $25,565 less than the average salaryoutside the academy ($124,898); this difference is statistically significant at the 5% level. The
Table 1Earnings by type of employer and degree (mean, standard deviation, and sample size in cell)
Employer All health economists Those with economicsdoctorates
Those with other academicdoctorates
All (academic andnonacademic)
$119,499 (47,546), N = 250 $123,796† (49,772), N = 181 $108,225† (39,272), N = 69
Academic $114,573* (43,048), N = 162 $120,435† (47,034), N = 117 $99,333*† (24,889), N = 45All nonacademic $128,566* (53,966), N = 88 $129,940 (54,269), N = 64 $124,898* (54,130), N = 24Government $104,786 (25,018), N = 30 $108,335 (25,924), N = 24 $90,592 (15,375), N = 6Not-for-profit $122,472 (39,504), N = 36 $118,357 (41,012), N = 28 $136,875 (31,791), N = 8For-profit $170,962 (76,456), N = 22 $200,181 (67,758), N = 12 $135,900 (74,322), N = 10
(1) Table lists responses to question, “In the last 12-month period, how much did you earn from your primary employer(including summer support, bonuses, and profit sharing but not housing allowance)?”. (2) Economists are those whoreceived a Ph.D. in economics, non-economists are those who received a Ph.D. in another subject or another formof doctorate than a Ph.D. (3) Asterisk (*) indicates that difference in means between academic and nonacademics isstatistically significant at the 5% level. In other words, the asterisk indicates a statistically significant difference in meansacross rows within a column. (4) † indicates that difference in means between those with economics doctorates andthose with other doctorates is statistically significant at the 5% level. In other words, it indicates a statistically significantdifference in means across columns within a row. Tests were conducted for all employers, for academic employers, andfor all nonacademic employers pooled, but not within types of nonacademic jobs due to small sample size.

362 J. Cawley, M.A. Morrisey / Journal of Health Economics 26 (2007) 358–372
difference in average salaries between academics and non-academics with economics Ph.D.s issmaller ($9505) and not statistically significant.
Average salaries also differ by type of doctoral degree. For academics and nonacademicspooled, the average salary of those with a Ph.D. in economics ($123,796) is $15,571 higherthan the average salary of those with other academic doctorates ($108,225); this difference isstatistically significant at the 5% level. Among academics, the average salary of economics Ph.D.s($120,435) is $21,102 higher than the average salary of those with other doctorates ($99,333); thisdifference is also statistically significant. Among nonacademics, the difference in average salarybetween economics Ph.D.s and those with other doctorates is smaller ($5042) and not statisticallysignificant.
Table 2 reports earnings for doctorally trained health economists employed in The Academy.Here we make distinctions by rank and the period of the contract as well as by the nature of thedegree. Because of the multiple ways we are cutting the data, there are some thin or even emptycells in Table 2. Here and elsewhere we suppress the values of any cell containing fewer thanthree responses. In general, we have few responses from professors with doctorates other thanPh.D.s; this scarcity of responses undoubtedly reflects the relatively short time that many of thesedegrees have been available.
Table 2 indicates that, predictably, average earnings rise with rank. For self-identified healtheconomists with Ph.D.s in economics, the average earnings for those on 9-month contracts risesfrom $82,315 for assistant professors to $91,847 for associate professors (an 11.6% increase)to $150,645 for professors (a 64.0% increase over associate professors); the difference betweenassociate and full professors is statistically significant at the 5% level.
Among economics-Ph.D. health economists with 12-month contracts, average earnings riseby 28.9% from assistant ($84,100) to associate ($108,428) and by 58.0% from associate to full($171,357); both of these differences in means are statistically significant at the 5% level. Data byrank and length of contract for health economists with other academic doctorates are scarce, butthe difference in average earnings of associate professors on 12-month contracts ($96,167) andprofessors on 12-month contracts ($135,600) is statistically significant at the 5% level. We alsofind that the average earnings of professors on 9-month contracts differ by type of doctorate; theaverage earnings of those with economics Ph.D.s ($150,645) is $45,645 higher than the averageearnings of those with other doctorates ($105,000); this difference is statistically significant at the5% level.
Average earnings by rank and contract length by academic unit are shown in Table 3. Facultyin colleges of arts and sciences and business schools tend to have 9-month contracts, whilefaculty in schools of medicine and public health tend to have 12-month contracts. While there arecounter-examples, those cells are quite sparse and the estimates, therefore, are unreliable.
Table 3 indicates that mean earnings of assistant professors in business schools ($110,561 forthose on 9-month contracts) is $38,644 higher than that of assistant professors in colleges of artsand sciences ($71,917 for those on 9-month contracts); this difference is statistically significantat the 5% level.
The average earnings of professors on 12-month contracts is higher in schools of medicine($194,500) than in schools of public health ($151,653), but this difference just falls short ofstatistical significance at the 5% level.
In Table 4 we compare the earnings of academic health economists in our survey with com-parable data from economics departments, schools of business, and schools of public health. Themore general economics department data were recorded by the American Economic AssociationUniversal Academic Questionnaire (AEA UAQ) and are reported by Scott and Siegfried (2006).

J.Caw
ley,M.A
.Morrisey
/JournalofHealth
Econom
ics26
(2007)358–372
363
Table 2Earnings by academic rank and contract type (mean, standard deviation, and sample size in cell)
Rank Economics Ph.D.s Other academic doctoral degrees
9-month contract 12-month contract 9-month contract 12-month contract
Assistant professor 82,315 (29,196), N = 21 84,100 (23,961), N = 16 94,116 (22,258), N = 12 91,777 (21,100), N = 18Associate professor 91,847 (25,867), N = 16 108,428* (20,851), N = 16 – 96,167 (16,448), N = 6Professor 150,645*† (34,786), N = 28 171,357* (49,085), N = 21 105,000† (22,913), N = 3 135,600* (29,177), N = 5
(1) Table lists responses to question, “In the last 12-month period, how much did you earn from your primary employer (including summer support, bonuses, and profit sharingbut not housing allowance)?”, separately by whether the respondent indicated that they were employed on a 9-month or 12-month contract. (2) Economists are those who receiveda Ph.D. in economics, Other Academic Degrees are those who received a Ph.D. in another subject or another form of doctorate than a Ph.D. (3) A dash indicates that the cellcontains fewer than three respondents. (4) Asterisk (*) indicates that the difference in salary between that and the previous (lower) rank is statistically significant. For example,an asterisk in the Associate Professor cell indicates that the average salary in that rank is significantly higher than the average salary in the Assistant Professor rank. (5) For norank is the average 12-month salary greater than the average 9-month salary. (6) † indicates that the average salary of that length in that rank is significantly different for thosewith economics doctorates and those with other academic doctorates.

364J.C
awley,M
.A.M
orrisey/JournalofH
ealthE
conomics
26(2007)
358–372
Table 3Earnings by academic rank, contract type, and academic unit (mean, standard deviation, and sample size in cell)
Rank Arts and sciences Business school Public health Medicine
9-monthcontract
12-monthcontract
9-monthcontract
12-monthcontract
9-monthcontract
12-monthcontract
9-monthcontract
12-monthcontract
Assistantprofessor
71,917 (19,331), N = 12 – 110,561 (32,996), N = 10 114,575 (27,809), N = 4 79,333 (12,423), N = 3 77,588 (28,478), N = 9 – 90,428 (15,628), N = 14
Associateprofessor
83,167 (23,353), N = 6 – – – 112,000 (36,496), N = 3 102,167 (13,763), N = 12 – 111,736 (20,824), N = 4
Professor 144,000 (47,571), N = 9 – 135,305 (32,637), N = 10 – 167,000 (31,072), N = 5 151,653 (39,859), N = 13 – 194,500 (54,881), N = 8
(1) Table lists responses to question, “In the last 12-month period, how much did you earn from your primary employer (including summer support, bonuses, and profit sharing but not housing allowance)?”, separately
by whether the respondent indicated that they were employed on a 9-month or 12-month contract. (2) A dash indicates that the cell contains fewer than three respondents.

J.Caw
ley,M.A
.Morrisey
/JournalofHealth
Econom
ics26
(2007)358–372
365
Table 4Comparison across surveys of academic health economist earnings by school
Economics departments Business schools Schools of public health
Our survey AEA UAQ Our survey AACSB Our survey ASPH
Sample Health economistswith facultyappointments and9-month contracts ineconomicsdepartments
U.S. economicsdepartments
Health economistswith facultyappointments and9-month contracts inbusiness schools
Survey of U.S.business schools
Health economistswith facultyappointments and12-month contractsin schools of publichealth
Survey of U.S.schools ofpublic health
Earnings information Earnings in past 12months fromacademic employer
Meanacademic-yearsalary by rank indepartment
Earnings in past 12months fromacademic employer
9-month salary Earnings in past 12months fromacademic employer
12-month salaryof non-M.D.faculty
When data collected Fall 2005 Fall 2005 Fall 2005 Fall 2004 Fall 2005 Fall 2005Assistant professor $81,367 (30,097)
N = 18$71,112 N = 150 $110,561 (32,996)
N = 10$73,924 $77,588 (28,478)
N = 9$77,439
Associate professor $88,692 (18,842)N = 6
$79,806 N = 174 – $78,576 $102,167 (13,763)N = 12
$97,387
Professor $137,789 (38,117)N = 14
$101,652N = 194
$135,305 (32,637)N = 10
$107,732 $151,653 (39,859)N = 13
$136,576
(1) For AEA UAQ results see Scott and Siegfried (2006); we report the average across department types (highest degree granted is Ph.D., M.A., or B.A.) of the mean salary byrank. (2) Economics departments may be located in colleges of arts and sciences or in business schools. (3) For AACSB results see AACSB (2004). (4) AACSB average salaries,reported in 2004 dollars, have been converted to 2005 dollars to adjust for inflation. (5) For ASPH results see ASPH (2005). (6) Neither AACSB nor ASPH report standarddeviations or sample sizes associated with mean salaries by rank. The UAQ results are reported separately by highest degree granted by the department; we average across thesegroups and therefore do not have access to overall standard deviations. A dash indicates fewer than three observations in the cell.
366 J. Cawley, M.A. Morrisey / Journal of Health Economics 26 (2007) 358–372
The earnings for health economists in economics departments are higher at each rank than theaverage salary across economists of all fields in economics departments. The difference is roughly$10,000 for assistant professors, $9000 for associate professors, and $36,000 for professors, ineach case favoring the health economists. However, recall that while the UAQ reports only 9-month salaries, our survey obtained reported average annual earnings and, therefore, includes anysummer support.
In Table 4, the middle columns compare the earnings of health economists with appointmentsin business schools to salaries of all economists in business schools. The latter data are reported inthe Association to Advance Collegiate Schools of Business (AACSB, 2004) annual salary survey.While our sample of business school health economists is quite small, it does suggest that thesehealth economists are paid better than their business school general economist colleagues. Wesuspect that this may stem in part from selection bias with only the larger business schools offeringcourse work in health economics. Another difference is that our income data are on an annualbasis and the AACSB averages correspond to the 9-month academic year.
The last columns of Table 4 compare our survey data with those for schools of public health(specifically, all full-time non-physician non-chair faculty regardless of discipline). These data arebased upon 12-month appointments only (ASPH, 2006). The reported data for assistant professorsare almost identical. Associate and full professor health economists appear to receive highersalaries than the average public health faculty member by rank.
Another relevant comparisons are health services researchers more broadly. Resneck and Luft(2004) found, in a 2002 survey of members of Academy Health, median salaries of $79,000($85,763 in 2005$) for assistant professors, $100,000 ($108,560 in 2005$) for associate professors,and $134,000 ($145,471 in 2005$) for full professors. Note that while this sample includesmembers of a national health services research organization, it may include significant numbersof people who do not self-identify as either a health economist or an economist who studies healthtopics.
3.2. Earnings equation estimates for health economists
We next estimate log earnings models in order to determine how various factors correlatewith earnings for health economists. We estimate earnings models in the spirit of Mincer (1974):log earnings are regressed on measures of education, experience, experience squared, and othermeasures of human capital and demographic characteristics:
lny = β0 + β1s + β2x + β3x2 + u
where s indicates schooling and x and x2 are experience and experience squared. In a chapter inthe Handbook of Labor Economics on “Wage Determinants”, Willis (1986) describes the Mincerequation as “the standard human capital earnings function” (p. 526) and reviews the large literaturethat has estimated it empirically.
Table 5 presents the mean of each independent variable (column 1) as well as log earningsregression results for academics (column 2) and non-academics (column 3). The omitted categoriesare such that the reference person is an unmarried white male with a Ph.D. in economics; inregressions for academics the reference person has a tenure-track appointment in an economicsdepartment in a college of arts and sciences and is employed on a 9-month contract, and inthe regressions for nonacademics the reference person has a job in government and no facultyappointment.

J.Caw
ley,M.A
.Morrisey
/JournalofHealth
Econom
ics26
(2007)358–372
367Table 5Log earnings and consulting income mean of regressors (column 1) coefficients and standard errors in parentheses (columns 2–5)Variable (1) (2) (3) (4) (5)
Mean of variable Log earnings – academics Log earnings – non-academics Any consulting –academics
Ln average consulting income– academics
Ph.D. in health services research 0.149 −0.0154 (0.061) 0.0104 (0.11) −0.434 (0.46) 0.815* (0.46)Ph.D. in other than economics or HSR 0.099 0.000244 (0.066) −0.278** (0.12) −0.341 (0.50) 0.587 (0.50)Doctorate other than Ph.D. 0.014 0.267 (0.24) −0.591*** (0.21) 2.063 (1.70)M.D. 0.018 0.245* (0.13) 0.0451 (0.30) 1.182 (0.91)Masters degree other than economics or M.D. 0.099 −0.0972 (0.073) −0.00921 (0.11) 0.0980 (0.85) −0.197 (0.57)Ph.D. in economics from top five departments 0.099 0.164*** (0.060) 0.0948 (0.17) −0.817 (0.56) −0.218 (0.44)Ph.D. in economics from top twenty departments 0.212 −0.0276 (0.051) 0.125 (0.091) −0.254 (0.52) 0.279 (0.39)Years since Ph.D. 13.455 0.0181** (0.0088) 0.0423** (0.017) 0.0723 (0.100) −0.00705 (0.068)Years since Ph.D. squared 274.815 −0.000347 (0.00025) −0.000916* (0.00049) −0.00450 (0.0031) −0.000181 (0.0018)Years with current employer 8.284 −0.0401*** (0.0092) −0.0196 (0.017) 0.0203 (0.093) −0.0840 (0.071)Years with current employer squared 132.905 0.00127*** (0.00029) 0.000819 (0.00052) 0.00102 (0.00029) 0.00151 (0.0023)Female 0.360 −0.0451 (0.040) 0.04510.0 (0.075) −0.331 (0.37) −0.824*** (0.31)Race: nonwhite 0.108 0.0466 (0.064) −0.102 (0.093) 0.0741 (0.51) −0.677 (0.55)Married 0.847 0.0428 (0.052) −0.0129 (0.091) 1.064** (0.47) −0.274 (0.47)Employed in business school 0.145 0.160** (0.069) −0.439 (0.58) 0.201 (0.55)Employed in school of public health 0.283 −0.0430 (0.088) 0.721 (1.06) −0.496 (0.66)Employed in medical school 0.166 0.0180 (0.094) −0.913 (0.91) −0.347 (0.71)Employed in public policy department or school 0.055 −0.124 (0.11) −0.183 (1.00) −0.990 (0.82)Employed in other department 0.152 0.0100 (0.090) −1.090 (0.84) −0.426 (0.72)Employed outside of economics department 0.738 0.145* (0.075) 0.764 (0.68) −0.265 (0.59)Has 12-month contract 0.524 −0.0116 (0.050) 0.438 (0.49) −0.343 (0.37)Not on tenure track 0.124 −0.112* (0.063) −0.620 (0.61) 0.451 (0.48)Hours worked per week 47.027 0.00210 (0.0020) 0.00464 (0.0040) −0.0208 (0.017) −0.0284* (0.014)Number of journal articles published 34.171 0.00886*** (0.0014) 0.00496 (0.0038) 0.0290 (0.025) 0.0288** (0.011)Number of journal articles published, squared 2903.306 −0.0000243*** (0.0000053) −0.00000835 (0.000026) −0.0000499 (0.00019) −0.0000649 (0.00019)Received formal outside job offer in past 3 years 0.333 −0.0117 (0.044) −0.0904 (0.078) −0.0436 (0.39) 0.350 (0.35)Has administrative appointment 0.228 0.121** (0.052) 0.978 (0.82) 0.316 (0.37)Employed in not-for-profit nonacademic organization 0.417 0.0250 (0.078)Employed in for-profit organization 0.208 0.425*** (0.11)Also has a faculty appointment 0.292 0.0119 (0.081)Constant 11.06*** (0.13) 11.03*** (0.22) 0.956 (1.16) 10.50*** (1.00)Observations 217 145 72 136 118R-squared 0.75 0.66 0.39
(1) Data: self-identified health economists with doctorate. (2) Statistical significance indicated as follows: ***p < 0.01, **p < 0.05, *p < 0.1. (3) The omitted categories are such that the reference person is an unmarried white male with
a Ph.D. in economics; in regressions for academics the reference person has a tenure-track appointment in an economics department in a college of arts and sciences and is employed on a 9-month contract, and in the regressions for
nonacademics the reference person has a job in government and no faculty appointment. (4) Number of observations of academics in column 4 is less than that in column 2 for two reasons. First, four respondents had to be dropped from
the probit regression for any consulting income (column 4) because there was no variation in whether one had consulting income within their particular educational attainment category (Doctorate other than Ph.D., or M.D.). The second
reason is that five fewer respondents answered the question about consulting income (column 4) than that about the earnings through primary employer (column 2). (5) Unless indicated otherwise below, means are for the academic and
nonacademic samples pooled. (6) Means of the following variables are for academics only: indicators for type of academic unit, have 9-month contract, not tenure track. (7) Means of the following variables are for nonacademics only:
employed in not-for-profit organization, employed in for-profit organization, also has a faculty appointment.
368 J. Cawley, M.A. Morrisey / Journal of Health Economics 26 (2007) 358–372
The regression results in column 2 indicate that academic health economists with an M.D.degree in addition to their doctorate earn 27.7% more.1 Among non-academics, those with Ph.D.sin something other than economics or health services research earned 24.2% less, and those witha doctorate other than a Ph.D. earned 44.6% less than those with Ph.D.s in economics.
The National Research Council (1995) ranked Chicago, Harvard, MIT, Stanford, and Princetonas the top five economics departments; an academic health economist who earned a Ph.D. ineconomics from one of these institutions earned 17.8% more than those who earned Ph.D.s fromdepartments ranked 21 or lower. Stock and Siegfried (2001) found that economists (of all fields)who received their Ph.D. in 1996–1997 from a department in the top 6 of the 1993 NationalResearch Council rankings earned 12% more than those who received their economics Ph.D.from a department ranked 48 or lower.
Total work experience (defined as years since obtaining one’s highest degree) was correlatedwith earnings for both academics and nonacademics. The total work experience associated withmaximum earnings was 26.1 years for academics and 23.1 years for nonacademics.2
We also examined the correlation of earnings with employer-specific experience and find thatthe pattern is U-shaped: earnings fall through 15.8 years of experience before rising over theremaining range of experience. The initial decline is likely due to the rate of increase in marketsalaries exceeding internal pay raises with the result that, among faculty of equal work experiencesince Ph.D., those recently hired have higher salaries than those hired several years ago. It is lessclear why earnings rise with employer-specific experience at higher levels of such experience.One possible explanation is selective attrition – the only faculty who stay that long are thosewho are well-compensated; those who remain less well-paid relative to those of the same totalexperience leave for other employers.
Demographic characteristics (gender, race, marital status) had no statistically significant corre-lation with the earnings of health economists. Those employed in business schools earned 17.4%more. Previous estimates of the business school premium for economists in all fields of researchare: 19% among those who received their Ph.D. in 1996–1997 (Stock and Siegfried, 2001) and26% among those who earned their Ph.D. in 2001–2002 (Siegfried and Stock, 2004). We foundno other significant correlations of earnings with employment in other academic units. Economicsemployed in colleges of arts and sciences but outside of economics departments earned 15.6%more than those in economics departments. Academics whose appointments are not on the tenuretrack earn an average of 10.6% less than academics on the tenure track. Academics with an admin-istrative appointment (e.g. center director, department chair, or Dean) earn 12.8% more. Amongnon-academics, those employed by for-profit firms earned an average of 53% more than those ingovernment service.
The results reported in Table 5 confirm that publishing enhances the earnings of academichealth economists; specifically, the number of journal articles increased income at a decreasingrate. (The coefficients imply a peak in earnings at 182 publications, but only three individualsreport that many publications, so we are comfortable generalizing that publishing enhances theearnings of academics.) Number of publications was not significantly correlated with earningsfor nonacademic health economists. We have not included rank or the attainment of tenure in theacademic earnings equation because these tend to be determined by (and are therefore strongly
1 In the semi-log functional form, the percentage impact of an indicator variable on the linear (untransformed) outcomeis eβ − 1 (Kennedy, 1998).
2 The experience associated with maximum earnings was calculated as – �1/(2�2), where �1 is the coefficient on linearexperience and �2 is the coefficient on experience squared.
J. Cawley, M.A. Morrisey / Journal of Health Economics 26 (2007) 358–372 369
correlated with) number of publications and experience. (When academic rank and tenure wereincluded, rank had no statistically meaningful correlation with earnings, tenure was positivelycorrelated with earnings, and the coefficients on experience and number of publications andfell.)
In general, observed characteristics explain most of the variance in earnings; specifically,75% of the variation in log earnings for academics and 66% of the variation in log earnings fornonacademics.
3.3. Consulting income among academics
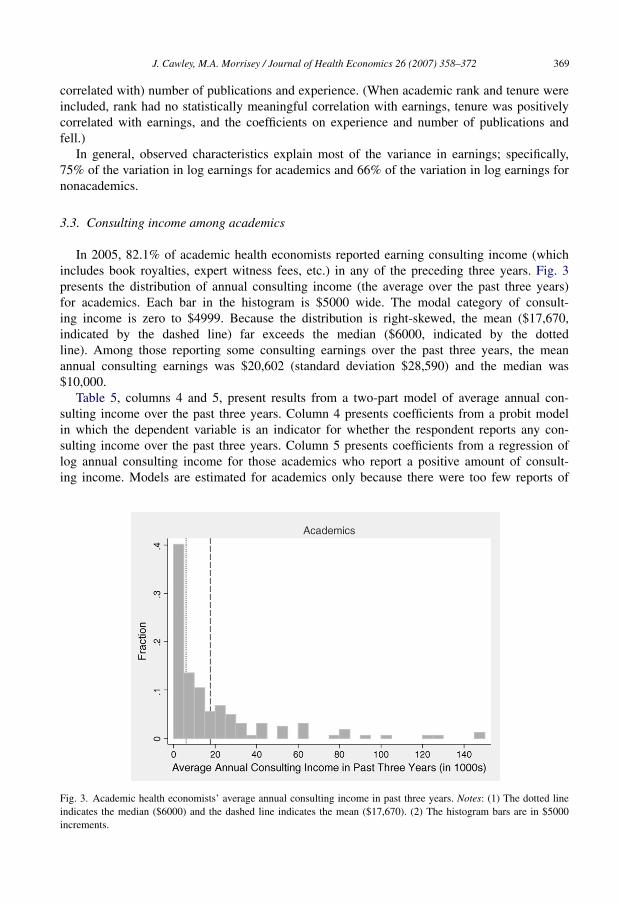
In 2005, 82.1% of academic health economists reported earning consulting income (whichincludes book royalties, expert witness fees, etc.) in any of the preceding three years. Fig. 3presents the distribution of annual consulting income (the average over the past three years)for academics. Each bar in the histogram is $5000 wide. The modal category of consult-ing income is zero to $4999. Because the distribution is right-skewed, the mean ($17,670,indicated by the dashed line) far exceeds the median ($6000, indicated by the dottedline). Among those reporting some consulting earnings over the past three years, the meanannual consulting earnings was $20,602 (standard deviation $28,590) and the median was$10,000.
Table 5, columns 4 and 5, present results from a two-part model of average annual con-sulting income over the past three years. Column 4 presents coefficients from a probit modelin which the dependent variable is an indicator for whether the respondent reports any con-sulting income over the past three years. Column 5 presents coefficients from a regression oflog annual consulting income for those academics who report a positive amount of consult-ing income. Models are estimated for academics only because there were too few reports of
Fig. 3. Academic health economists’ average annual consulting income in past three years. Notes: (1) The dotted lineindicates the median ($6000) and the dashed line indicates the mean ($17,670). (2) The histogram bars are in $5000increments.

370 J. Cawley, M.A. Morrisey / Journal of Health Economics 26 (2007) 358–372
consulting income among government and private-sector employees to estimate models for thatsample.
Table 5, column 4, indicates that virtually no observed characteristics were significantly cor-related with the probability that academics earned any consulting income; the only exception isthat married individuals were 17.1% more likely to earn any consulting income.
Table 5, column 5, presents the log consulting income regression for those who earned anyconsulting income. Among health economists with some consulting income, women earned 56.1%less than men. (The unconditional means are $24,652 for men and $11,357 for women; the mediansare $14,500 for men and $5000 for women.) We also find that health economists with Ph.D.s inhealth services research earn 125% more in consulting than those with Ph.D.s in economics. (Theunconditional means are $25,125 for those with health services research Ph.D.s and $19,697 forthose with economics Ph.D.s; the medians are $15,000 for health services research Ph.D.s and$10,000 for economics Ph.D.s.)
We also find evidence of a tradeoff between academic work and consulting: those who worklonger hours at their academic job earn less consulting income; e.g. a 10-h per week increase inacademic work is associated with 28.4% less consulting income. However, we also find evidencethat publishing in academic journals raises consulting income. (While the coefficients implyconsulting income peaks at 222 published articles, only one individual in the sample reports thatmany publications.)
3.4. Salaries to be offered to new Ph.D. health economists
Table 6 lists the salaries expected to be offered to new Ph.D. health economists, by type ofemployer. The mean salary expected to be offered to new hires is greater in Business Schools thanin Colleges of Arts & Sciences, and greater in Medicine than in Public Health, and greater in For-Profit than Not-for-Profit nonacademic institutions, but none of these differences are statisticallysignificant.
We can compare the starting salary estimates reported by health economists in economicsdepartments with contemporaneous estimates given in other surveys that document actual startingsalaries in the field of economics as a whole. Two comparison surveys are the American EconomicAssociation Universal Academic Questionnaire (UAQ) and the survey conducted by the Center
Table 6Nine-month or 12-month salary expected to be offered to new Ph.D. health economist (mean, standard deviation, andsample size in cell)
9-month contract 12-month contract
Arts and sciences $74,261 (12,166), N = 23 $78,333 (12,583), N = 3Business school $79,700 (17,619), N = 20 $128,333 (25,658), N = 3Public health $65,100 (9,960), N = 10 $77,793 (13,075), N = 29Medicine – $80,181 (16,147), N = 22Government – $72,621 (10,122), N = 25Not-for-profit – $79,444 (16,669), N = 27For-profit – $86,667 (15,679), N = 21
(1) Table lists responses to question, “What is the approximate salary your department/agency/firm would pay for a newlyminted Ph.D. in economics with a specialization in health? Is this salary based on 9 months or 12 months?” (2) Surveymay include multiple respondents from the same department, leading to biased estimates of the mean offer across alldepartments that may hire health economists. (3) – indicates that the cell contained fewer than three responses.

J. Cawley, M.A. Morrisey / Journal of Health Economics 26 (2007) 358–372 371
Table 7Comparison of 9-month salaries expected to be offered to new economics Ph.D.s by economics departments, by survey
Our survey AEA UAQ CBER CBER
Sample Health economistswith primaryappointment ineconomicsdepartment
U.S. economicsdepartments
U.S. economicsdepartments
U.S. economicsdepartments
Information aboutoffer
9-month salarythat respondentsin economicsdepartmentsestimate would beoffered to newPh.D. healtheconomist
Meanacademic-yearsalary offered tonew assistantprofessors ineconomics
9-month salaryoffered to neweconomics Ph.D.sin 2005
9-month salaryexpected to beoffered to neweconomics Ph.D.sin 2006
When datacollected
Fall 2005 Fall 2005 Fall 2005 Fall 2005
Expected oroffered salary tonew economicsPh.D. assistantprofessors
73,889 (11,741),N = 36
71,724, N = 63 81,812 (10,855),N = 39
84,070 (10,447),N = 39
(1) Table lists responses to question, “What is the approximate salary your department/agency/firm would pay for a newlyminted Ph.D. in economics with a specialization in health? Is this salary based on 9 months or 12 months?” (2) Surveymay include multiple respondents from the same department, leading to biased estimates of the mean offer across alldepartments that may hire health economists. (3) For AEA UAQ results see Scott and Siegfried (2006); we report theaverage across department types (highest degree granted is Ph.D., M.A., or B.A.). (4) For CBER results see Deck et al.(2006).
for Business and Economic Research (CBER) at the University of Arkansas. Both surveys recordthe actual 9-month salary offered to new hires by economics departments in the past year; incontrast, our survey asked health economists to estimate how much their department would offera new economics Ph.D.
Table 7 compares the starting salaries documented in our 2005 survey to those of the 2005UAQ and 2005 CBER. We limit our sample to estimates provided by health economists workingin economics departments to facilitate the comparison. The average estimated starting salary ineconomics departments is $73,889 in our sample compared to $71,724 for economics departmentsin the UAQ sample (Scott and Siegfried, 2006), and $81,812 across all economics departmentsin the CBER sample (Deck et al., 2006). In addition to documenting actual offers in the past year(2004–2005), the CBER also asked economics departments to predict what 9-month salary theywould offer to a starting assistant professor in 2005–2006; the average estimate was $84,070.
4. Limitations
There are several important limitations to this study. The first is that the response rate wasrelatively low at 32%. This raises the issue of the generalizability of the findings. The relativelysmall numbers of respondents in certain cells limit our power to detect differences across groups.However, the direction of bias, if any, is unclear. On the one hand, one would expect those withhigher opportunity costs of time to be less likely to respond. On the other, those with stronger

372 J. Cawley, M.A. Morrisey / Journal of Health Economics 26 (2007) 358–372
interest in the survey topic are more likely to respond. Any bias is further complicated by theunusual nature of our survey universe. The U.S. membership of iHEA and the members of theAcademyHealth Health Economics Interest Group contain members who may have joined toparticipate in an international conference or because they have an interest in the field but notnecessarily a vocation. We excluded 101 responses because the respondents did not considerthemselves to be either health economists or economists who work in health. Non-respondents maydisproportionately fit that categorization.The other major limitation relates to the usual problemsof analysis with a single cross section. We do not observe the professional life-cycle of healtheconomists. Our data allow us only to look at different cohorts at the same point in time. Weacknowledge that our single cross-section will reflect factors and events around the time of thesurvey, e.g. the budgets of public universities. Despite these limitations, this study has shed lighton one important labor market worthy of study: our own.
Acknowledgments
We thank the advisory committee that helped formulate the survey of U.S. Health Economists:Roger Feldman (chair), Sharon Arnold, Dick Arnould, Kate Bundorf, Mike Hagan, Dave Knutson,and Kristine Metter. We also thank Tom McGuire, Sean Nicholson, John Siegfried, and twoanonymous referees for helpful comments and suggestions.
References
Association to Advance Collegiate Schools of Business (AACSB), 2004. “2004–2005 Salary Survey Executive Summary.”Online at: http://www.aacsb.edu/knowledgeservices/home/SS-04ExecutiveSummary.pdf.
Association of Schools of Public Health (ASPH), 2006. School of Public Health Full Time Faculty Salary Range Survey,ASPH February 24, 2006, Washington, DC.
Biener, L., Garrett, C.A., Gilpin, E.A., Roman, A.M., Currivan, D.B., 2004. Consequences of declining survey responserates for smoking prevalence estimates. American Journal of Preventive Medicine 27 (3), 254–257.
Curtin, R., Presser, S., Singer, E., 2000. The effects of response rate changes on the index of consumer sentiment. PublicOpinion Quarterly 64, 413–428.
Deck, K.A., Collins, J.T., Currington, W.P., 2006. Survey of the Labor Market for New Ph.D. Hires in Economics,2006–2007. Unpublished manuscript, Center for Business and Economic Research and Department of Economics,University of Arkansas.
Feldman, R., Morrisey, M.A., 1990. Health economics: a report on the field. Journal of Health Politics Policy and Law15 (3), 627–646.
Keeter, S., Miller, C., Kohut, A., Groves, R.M., Presser, S., 2000. Consequences of reducing nonresponse in a NationalTelephone Survey. Public Opinion Quarterly 64, 125–148.
Kennedy, P., 1998. A Guide to Econometrics: Fourth Edition. MIT Press, Cambridge, MA.Mincer, Jacob, 1974. Schooling, Experience, and Earnings. Columbia University Press, New York.National Research Council, 1995. Research-Doctorate Programs in the United States: Continuity and Change. National
Academy Press, Washington, DC.Resneck, Jack, Luft, Harold, 2004. How Health policy and health services researchers are compensated: analysis of a
nationwide salary survey. Medical Care Research and Review 61 (3), 392–408.Scott, C.E., Siegfried, J.J., 2006. American Economic Association Universal Academic Questionnaire Summary Statistics.
American Economic Review: Papers and Proceedings 96 (2).Siegfried, J.J., Stock, W.A., 2004. The labor market for new Ph.D. economists in 2002. American Economic Review
Papers and Proceedings 94 (2), 272–285.Stock, W.A., Siegfried, J.J., 2001. So you want to earn a Ph.D. in economics: how much do you think you’ll make?
Economic Inquiry 39 (2), 320–335.Willis, R.J., 1986. Wage determinants: a survey and reinterpretation of human capital earnings functions. In: Ashenfelter,
Layard (Eds.), Handbook of Labor Economics, vol. 1. Amsterdam, North Holland, pp. 525–602.