Embed Size (px)
Citation preview
The effect of 10 weeks of home‐based supervised
aerobic and resistance exercise training in
individuals with cystic fibrosis‐related diabetes
Sugumaran Muniandy, B.Sc.
This thesis is presented in fulfilment of the requirements for
the degree of Master of Science at The University of Western
Australia
School of Sport Science, Exercise and Health
Faculty of Life and Physical Sciences
February 2012

i
Abstract
Background: Regular exercise provides important benefits to individuals with cystic
fibrosis; however, no studies have investigated the effects of regular exercise in
patients with cystic fibrosis‐related diabetes (CFRD). This thesis examined the
effects of supervised home‐based aerobic and resistance exercise training on blood
glucose control, cardiorespiratory fitness, muscular strength, lung function, body
composition and quality of life in patients with CFRD. Methods: Six patients with
CFRD were recruited for this study. Participants were allocated to an exercise or a
control group for a period of 10 weeks, before crossing over to the alternative
group. A 10 week wash‐out period occurred between exercise and control periods.
During the exercise intervention, patients completed two sessions per week of
supervised, home‐based exercise involving a combination of aerobic and resistance
activities. During the control period, patients maintained their normal activity
routine. Outcome measures were assessed pre‐ and post‐intervention. Results:
Adherence to the exercise training was excellent, with each participant completing
all scheduled exercise sessions. Exercise training improved cardiorespiratory fitness
and muscular strength (p < 0.05), and tended to increase lean mass (p = 0.089).
There were no significant changes in glucose tolerance or glycaemic control as a
result of exercise intervention; however, following the equivalent control period
there was a worsening of glucose tolerance to an oral glucose load (p < 0.05) and a
tendency for increased fasting blood glucose levels (p = 0.09). There were no
significant changes in lung function or quality of life as a result of the intervention.
Conclusion: Regular exercise is beneficial for individuals with CFRD and should be
encouraged as part of routine management of the condition.
ii
Statement of Candidate Contribution
The work involved in designing and conducting the study described in this thesis has
been conducted primarily by Sugumaran Muniandy (the candidate), in consultation
with Assistant Professor Grant Landers, Assistant Professor Kym Guelfi (the
candidates supervisors) and Mr Jamie Wood And Dr Joey Kaye (Associate
Investigators). All participant recruitment and management was carried out by the
candidate, with the assistance of Mr Wood. The implementation of all exercise
training was conducted solely by the candidate. In addition, the candidate was
responsible for all data entry, management and analysis, as well as original drafting
of the thesis. Assistant Professor Grant Landers, Assistant Professor Kym Guelfi, Mr
Jamie Wood and Dr Joey Kaye have provided feedback for further drafts and
polishing of the thesis.
Student Signature………………………………………………………………………………….
Coordinating Supervisor Signature………………………………………………………
Declaration for theses containing published work and/or work prepared for
publication
This thesis does not contain work that I have published, nor work under review for
publication.
Student Signature………………………………………………………………………………….
Coordinating Supervisor Signature……………………………………………………….
iii
Acknowledgements
To the following people I wish to recognise and express my heartiest appreciation,
whose contributions have been unconditionally invaluable, enriching, future
direction and defining in making my thesis possible.
To my supervisors
Assistant Professor Grant Landers. For your wisdom, insight and generous
donation of precious time. Thank you for challenging and inspiring me throughout
this entire 2 years!
Assistant Professor Kym Guelfi. For your passion, insight and patience. I’m really
grateful for all the time giving me guidelines, advice, encouragement and great
support all throughout to make this thesis such an exciting one!
To the Hospital Staff
Mr Jamie Wood. For endless effort to arrange all technical support and your effort
has been invaluable through the years. Thanks you heaps!
Dr Joey Kaye. For giving me the great support. Thank you, your support has always
been welcome!
Dr Siobhain Mulrennan. For giving advice and assistance in my studies endlessly.
Sue Morey. For giving your precious time and guiding me through!
To my beloved wife Kogilavani S. Pavadai
For supporting me unconditionally throughout my entire time in Perth by giving me
endless moral support and encouragement to make this wonderful experience to
become reality. Thank you so much and love you forever!

iv
Table of Contents
Abstract………………………………………………………………………………………………………………. i
Statement of Candidate Contribution..………………………………………………………………… ii
Acknowledgments……………………………………………………………………………………………….. iii
Table of Contents……………………………………………………….……………………………………….. iv
Chapter One
Introduction and Review of the Literature…………………………………………………..…… 1
1.1 Cystic Fibrosis…………………………………………………………………………………………… 2
1.2 Pathogenesis of Cystic Fibrosis………………………………………………………….……… 3
1.3 Management of Cystic Fibrosis……………………………………………………….………… 5
1.4 Cystic Fibrosis‐Related Diabetes……………….……………………………………….…….. 6
1.5 Exercise and Cystic Fibrosis…………………………………………………………………..….. 10
1.6 Exercise and Cystic Fibrosis‐Related Diabetes………..………………………….…..… 18
1.7 Summary……………………………………………………………………………………………..…… 20
1.8 References…………………………………………………………………………………………..…… 22
Chapter Two
The effect of 10 weeks of home‐based supervised aerobic and resistance exercise
training in individuals with cystic fibrosis‐related diabetes………………………..…… 35
2.1 Introduction…………………………………………………………………………………………..… 36
2.2 Method and Procedures……………………………………………………………………..…… 38
2.2.1 Participants…………………………………………………………………………..…….. 38
v
2.2.2 Research Design…………………………………………………………………………… 40
2.2.3 Exercise Intervention…………………………………………………………..…....... 40
2.2.4 Outcome Measures……………………………………………………………........... 41
2.2.4a Assessment of Diabetes Control……………………………............. 42
2.2.4b Assessment of Cardiorespiratory Fitness…………………………… 43
2.2.4c Assessment of Muscular Strength ………………………………….… 44
2.2.4d Assessment of Pulmonary Function…………………………………… 44
2.2.4e Assessment of Body Composition……………………………......……44
2.2.4f Assessment of Quality of Life………………………………………….… 45
2.2.4g Evaluation the frequency and duration of hospitalisation.… 45
2.2.5 Statistical Analysis………………………………………………………………………… 45
2.3 Results………………………………………………………………………………………………….…. 46
2.3.1 Exercise Training Characteristics…………………………….………………….… 46
2.3.2 Effect of Exercise Training on Cardiorespiratory Fitness………..…..… 47
2.3.3 Effect of Exercise Training on Muscular Strength………………….……… 48
2.3.4 Effect of Exercise Training on Glycaemic Control….…………….……….. 49
2.3.5 Effect of Exercise Training on Body Composition….……………………… 49
2.3.6 Effect of Exercise Training on Quality of Life………………………..…….… 50
2.3.7 Effect of Exercise Training on Pulmonary Function…………….………… 52
2.3.8 Frequency and Duration of Hospitalisation………………………………..… 52
2.4 Discussion……………………………………………………………………………….…………….... 53
2.5 References……………………………………………………………………………………...………. 60
vi
Appendices
Appendix A Participant Information Sheet……………………………………………...………. 66
Appendix B Participant Consent Form…………………………………………………...………. 72
Appendix C Ethical Approval……………………………………………………………….....………. 74
Appendix D Cystic Fibrosis Questionnaire–Revised……………………………...…….……. 76

1
Chapter One
Introduction and Review of the Literature
2
1.1 Cystic Fibrosis
Cystic fibrosis (CF) is a genetic disorder caused by a single mutation in the gene that
encodes the CF transmembrane regulator protein (CFTR). This protein plays an
important role in chloride ion transport, which in turn influences the transport of
water and electrolytes in the cells of the respiratory, digestive and reproductive
systems (Brennan et al., 2004). Without this protein, there is accumulation of thick
secretions and progressive scarring, leading to destruction of target organs. In
particular, CF is characterised by recurrent lower respiratory tract infections due to
reduced clearance of respiratory secretions. Lung function declines progressively
over time, ultimately leading to respiratory failure and death. Other clinical
manifestations include nutrient malabsorption from impaired pancreatic enzyme
production, intestinal obstruction, male infertility and impairments in temperature
regulation and fluid balance due to altered sweat gland function (Rosenstein &
Cutting, 1998).
The incidence of CF is approximately 1 in 2500 in Caucasian populations, with 1 in
25 individuals being a carrier for the condition (Sinaasappel et al., 2002). Following a
positive result from a newborn screening test, diagnosis of the condition is usually
confirmed by a laboratory sweat test, which shows chloride concentrations of 60 to
70 mmol/L compared to 40 mmol/L in healthy individuals (Augarten et al., 1993;
Castellani & Massie, 2010; Davis & di Sant’Agnese, 1984; Farrell et al., 2008).
Although there is currently no cure for the disease, life expectance has improved
dramatically in recent years due to improved management of the condition.
Approximately 80% of children born with CF in the 1940’s died within the first year

3
of life, but today 95% of individuals with CF will live to at least 40 years of age
(Cohen‐Cymberknoh et al., 2011; Elborn et al., 1991). Given the increased life
expectancy of individuals with CF in today’s society, there is increasing interest in
enhancing the quality of life of these patients. In particular, exercise may play an
important role in the management of this condition given the likely benefits for
functional capacity, body composition and improving quality of life.
1.2 Pathogenesis of Cystic Fibrosis
Most healthy individuals have two healthy copies of the CFTR gene; however, only
one is needed to prevent CF (Chillon et al., 1995). In contrast, individuals with two
mutated alleles cannot produce CFTR protein, resulting in CF. Since the CF gene was
first identified in 1989, over 900 different CFTR mutations have been reported
(Farrell et al., 2008; Sheppard & Nicholson, 2002). The primary mechanism through
which the lack of CFTR protein results in the signs and symptoms of CF is through
dysfunction of the cyclic‐AMP‐dependent chloride channel. This alters chloride and
water transport, leading to dehydrated viscous secretions that cause progressive
obstruction, scarring and eventually destruction of target organs, especially the
lungs and pancreas (Clunes & Boucher, 2008). With respect to the lungs, there is
reduced clearance of respiratory secretions which provides the ideal reservoir for
microorganisms such as Psuedomonas aeruginosa. The epithelia, which would
normally eradicate such bacteria, fail to kill these microorganisms due to the
abnormally high salt concentration on the apical surface (Muhlebach et al., 1999;
Smith et al., 1996). Even with potent antibiotics Psuedomonas aeruginosa is difficult
to eradicate. Unfortunately, once this bacteria has established in the bronchial

4
region, chronic infection occurs which coincides with an increased inflammation
response and may ultimately lead to death from respiratory failure (Frederiksen et
al., 1997; Gilligan, 1991). In addition, the oxygen saturation at the lungs declines to
90% to 94% or lesser, depending on the severity of infection, in comparison to the
oxygen saturation of 99 to 100% in the general population (Betancourt et al., 1991).
Consequently, individuals with CF suffer recurrent infection and inflammation,
ultimately leading to increased mortality and morbidity (Prasad & Cerny, 2002).
In addition to the respiratory system, the digestive system is severely impaired in
individuals with CF. In particular, CF is associated with exocrine pancreatic
insufficiency, leading to impaired pancreatic enzyme production and therefore
nutrient malabsorption, leading to fatigue, weight loss, poor growth and
malnutrition (Shoemaker et al., 2008). Malabsorption is mainly characterised by foul
smelling loose stools, and if undetected or left untreated in the newborn leads to
severe malnutrition and growth failure (Giglio et al., 1997). In adults, malabsorption
causes poor weight gain and malnourishment, even in those with a healthy appetite
(Sinaasappel et al., 2002). Another factor contributing to the negative energy
balance observed in these individuals is gastroeosophageal reflux due to
maldigestion and pancreatic exacerbation (Edenborough & Morton, 2010; Pencharz
& Durie, 2000). Consequently, to maintain a normal BMI of 20 – 25 kg/m², the
recommended energy intake for CF patients is 120‐150% of normal daily energy
intake, however, most CF patients rarely achieve this.
1.3 Management of Cystic Fibrosis
5
Although there is currently no cure for CF, recent advances in the management of
the condition have extended the life expectancy of these individuals considerably.
Daily treatment regimens are aimed at managing chronic lung disease, infection,
exocrine pancreatic insufficiency and malnutrition to delay the ultimate decline in
organ function for as long as possible (Ramsey et al., 1992). In particular, given the
difficulties with malabsorption, individuals with CF are encouraged to follow a high‐
fat high‐protein diet, providing 120‐150% of the recommended daily energy intake
of a healthy individual (Pencharz & Durie, 2000). In addition, individuals with
pancreatic insufficiency are supplemented with fat‐soluble vitamins and pancreatic
enzyme preparations to assist with digestion (Wilson & Pencharz, 1998). If weight
cannot be maintained with such strategies, then tube feeding may be required.
With respect to managing the chronic lung disease associated with CF, vigorous
chest physiotherapy is recommended to clear thick and sticky secretions in the
respiratory system, which play a prominent role in early history of this disease. In
addition, treatment of airways infection with oral antibiotics may be effective in
delaying the colonization of microorganisms. However in the presence of severe
infections, intravenous antibiotics may be required to prevent the establishment of
chronic inflammation (Rosenfeld et al., 2003). For those admitted to hospital,
patients are treated symptomatically to the immediate problem, followed by
regular chest physiotherapy and inhaled mucolytics to improve airway clearance,
inhaled antibiotics to curb infections, as well as supplementation with pancreatic
enzymes and vitamins (Kettler et al., 2002). In some patients with advanced lung
disease, the best option to extend the lifespan for CF patients may be through lung
transplantation. From 1989 to 2002, 65 Australian CF patients were listed to receive

6
lung transplants at the Royal Prince Alfred Hospital in Sydney (Dobbin et al., 2004).
Of note, regular exercise is also encouraged to assist in maintaining pulmonary
function, promote deep breathing and coughing to expel thick mucus, increase
muscle mass, stimulate appetite and promote feelings of wellbeing in patients with
CF.
1.4 Cystic Fibrosis‐Related Diabetes
While management of CF has extended the life expectancy of these individuals
considerably, as people live longer, other complications of the condition have
become apparent. As previously mentioned, one organ severely affected by CF is
the pancreas. Unfortunately, long‐term damage to the pancreas can ultimately lead
to impaired function of the islet cells of the pancreas which are responsible for the
production of the hormone insulin, leading to a type of diabetes that is unique to
those with the disease called cystic fibrosis‐related diabetes (CFRD). CFRD occurs
increasingly with age, with fewer than 2% of those under 10 years of age having the
complication, while more than 50% of adults with CF have abnormal glucose
regulation by the time they reach 30 years of age (Alexander & Bridges, 2010). The
median age of onset is 18‐21 years (Moran et al., 2009), although recent Australian
statistics suggest that the incidence among those < 18 years is rising (Rana et al.,
2011). Of importance, the life expectancy of an individual with CFRD is reduced
when compared to those with CF alone (Moran et al., 1999; O’Riordan et al., 2008).
All types of diabetes are characterised by chronic hyperglycaemia due to
impairments in insulin secretion, action or both. In a healthy individual, when an
7
elevation of blood glucose levels is detected by the pancreas, the secretion of the
hormone insulin is stimulated which helps transport the glucose from the
bloodstream into the cells of the body for storage or use (Brennan et al., 2004). In
contrast, individuals with diabetes are unable to effectively control blood glucose
levels due to the body not producing enough insulin, or not responding well to the
insulin that is produced (i.e. insulin resistance). However, there are different types
of diabetes, with the two most common forms being type 1 and type 2 diabetes.
Type 1 diabetes is usually diagnosed in childhood, and results in elevated blood
glucose levels due to destruction of beta cells in the pancreas, leaving them unable
to produce insulin. As a result, these individuals must administer exogenous insulin
daily to control blood glucose levels. In contrast, type 2 diabetes is usually
diagnosed in adulthood and may be the result of a combination of the effects of
relative insulin deficiency and increased insulin resistance. Individuals with type 2
diabetes often do not need insulin injections, at least not in the early stages of the
condition. Instead, they take oral hypoglycaemic agents to assist the body to use
the insulin they already have. Risk factors for type 2 diabetes include being
overweight, hereditary, ethnic origin and lack of exercise (Goodyear & Kahn, 1998).
On the other hand, CFRD is a unique form of diabetes, sharing some features of
both type 1 and type 2 diabetes. Initially the condition presents with impaired
secretion of insulin in response to an oral glucose load, leading to postprandial
hyperglycaemia (Brennan et al., 2004; Moran et al., 1999). Of interest, fasting blood
glucose levels often appear normal during this early stage of the condition.
However, as the disease progresses, severe insulin deficiency may result, leading to
8
a requirement for regular insulin injections like those with type 1 diabetes (Dobson
et al., 2004). The signs and symptoms of CFRD include polyuria (excessive water loss
through frequent urination) and polydipsia (increased thirst due to loss of water).
Other symptoms may include weight loss or an unexplained decline in pulmonary
function beginning up to 4 years prior to the diagnosis of CFRD (Milla et al., 2000).
The precise factors contributing to the initial insulin resistance observed in CFRD is
unclear, although chronic infection and corticosteroid administration likely play a
role (Lippe et al., 1977). In fact, the presence of diabetes is greatly influenced by
intercurrent infection and patients often develop reduced glucose metabolism
during respiratory exacerbation, but then glucose metabolism improves or
normalises when their lung function improves (Tofe et al., 2005). However, there is
also a progressive decline in glucose metabolism over time, with patients becoming
more prone to diabetes as they age. For this reason, testing via an oral glucose
tolerance test (OGTT) to diagnose CFRD should only be conducted when the
patients status is clinically stable at least one month apart from acute pulmonary
infection (Cohen‐Cymberknoh et al., 2011; Costa et al., 2005). The criteria for the
diagnosis of CFRD following an OGTT include a fasting blood glucose ≥ 7 mM, or a
blood glucose value of ≥ 11 mM at 2 hours after a 75 g OGTT (Moran et al., 1999).
Regardless of the specific type of diabetes, if left untreated, chronic hyperglycaemia
may lead to a number of serious health complications, such as retinopathy,
nephropathy and neuropathy (Schwarzenberg et al., 2007). Each of these
complications results from micro‐damage to the small blood vessels of the retina of
the eye, kidneys and damage to the nerves respectively. Specific to individuals with
9
CFRD, impaired glucose regulation also has significant effects on an individual’s lung
function, leading to an increased rate of decline in pulmonary function (Koch et al.,
2001). Consequently, individuals with CFRD have increased risk of mortality and
morbidity compared to patients with CF alone (Brennan et al., 2004; Moran et al.,
1999).
Management of CFRD involves a focus on nutrition and pharmacological
intervention. Most patients require exogenous insulin administration at the time of
meals to compensate for the impaired insulin response to rising glucose levels,
however, little basal insulin is required. Consequently, insulin therapy often involves
multiple injections of short acting insulin each day in association with meal
consumption, followed by a small dose of long acting insulin administered before
bedtime (Moran et al., 1999). Fortunately, insulin therapy has been shown to
reduce long‐term diabetes‐related complications, improve lung function, weight
and nutritional state, at the same time as reducing infectious complications and
hospitalisations in individuals with CFRD (Dobson et al., 2004). In contrast, oral
hypoglycaemic agents are not promoted for managing CFRD, primarily due to the
limited research of their use (Moran et al., 1999). Potential issues with using these
drugs to manage blood glucose levels in CFRD include their inability to address the
primary problem of insulin deficiency, as well as side‐effects on the gastrointestinal
system, which may prove serious for individuals with CF due to their already
present issues relating to malabsorption. With respect to diet, the goal is to
maintain normal blood glucose levels; however the principles of achieving this are
very different to that used for the management of type 1 and type 2 diabetes
10
(Brennan et al., 2004). The same high energy intake that is promoted for those with
CF alone is encouraged due to the associated malabsorption, and there is no focus
on avoiding sugary, high glycaemic foods given their importance as a source of
energy, provided that intake is spread evenly throughout the day and sugary drinks
are not taken between meals (Mackie et al., 2003; Moran et al., 1999). Likewise, a
high fat intake (approximately 40% of total energy intake) is required to maintain
body weight (Brennan et al., 2004). Consequently, maintenance of normal blood
glucose levels is achieved by carefully balancing insulin administration with
sufficient nutritional intake. All individuals with CFRD should also conduct regular
self‐monitoring of blood glucose levels to assist with maintaining levels within the
appropriate range (minimum of 3‐4 times per day; Moran et al., 1999; Moran et al.,
2010).
1.5 Exercise and Cystic Fibrosis
Another factor that is promoted for the management of CF is exercise. Research
investigating the effect of exercise in CF began in the early 1970’s (Counahan &
Mearns 1975; Godfrey & Mearns, 1971; Keens et al., 1977), however only few
studies have extensively examined the physiological responses and adaptations to
exercise in this population. Of note, studies have suggested that individuals with CF
spent less time engaging in vigorous physical activities and are less fit than their
peers (Braggion et al., 1989; Nixon et al., 2001). Importantly, no study has stated
that exercise causes harm to patients with CF.
11
It is well established that participation in regular exercise has many benefits for the
general population including the prevention of cardiovascular disease; lowering of
blood lipids; lowering blood pressure; and improving insulin sensitivity (Fletcher et
al., 1996). Exercise also plays an important role in the prevention of obesity,
maintenance of muscle mass, bone mineral density, and functional capacity
(Fletcher et al., 1996). Furthermore, exercise has numerous positive benefits for
mental health such as reduced levels of anxiety, depression and enhanced
psychological well‐being and quality of life (Warburton et al., 2006; Wheatley et al.,
2011). Many of these effects of exercise may be particularly beneficial for
individuals with CF. For instance, maintaining adequate muscle mass and muscle
size is vital for CF individuals given their difficulties with gaining weight due to
pancreatic insufficiency, malabsorption and malnutrition. In addition, exercise‐
induced improvements in cardiorespiratory fitness and reduced breathlessness may
have a significant impact on enhancing participation in activities of daily living and
improving quality of life in CF patients. Promoting psychological well‐being through
exercise is also important given the high rates of depression among CF patients
(Quittner et al., 2008).
The role of exercise in improving cardiorespiratory fitness in individuals with CF has
been demonstrated in several studies. Orenstein et al. (1981) conducted a 3 month
exercise program (1 hour x 3 times per week for 12 weeks) in patients with CF. Each
exercise session commenced with a warm up phase consisting of 5 to 10 minutes of
stretching and flexibility exercises, followed by a period of jog‐walking at an
intensity of 70 to 85% of maximal heart rate (duration of 10 minutes at the start of
12
the intervention, progressing up to 30 minutes). Each session was concluded with a
5 minute cool down consisting of a slow walk followed by a fun phase where various
non‐competitive recreational games were organised to enable other CF patients
who were not involved in the program to join in regardless of their age and severity
of CF. Following this 12 week program, these researchers reported improved
cardiorespiratory fitness based on both peak rate of oxygen consumption and
significantly lower heart rates at submaximal workloads compared to a control
group which remained unchanged. Although the above‐mentioned study was
conducted in a clinical setting, home‐based exercise training may be preferred to a
centralised institution‐based training program to allow for individualised
supervision and to minimise the potential for transferring infection between
patients (Burdge et al., 1993; Ojeniyi et al., 2000). It has also been suggested that
home‐based interventions may be more feasible given that many patients live long
distances from CF centres (Orenstein et al., 2004). However, one limitation of these
programs may be the lack of supervision. A home‐based training program consisting
of 15 minutes of submaximal stationary cycling (at approximately 70% of maximum
heart rate) each day for a period of 3 months (with 2 sessions per week supervised
by a physiotherapist) has been shown to improve maximal exercise capacity
(maximal rate of oxygen consumption) and decrease the degree of limitation in
participation in activities of daily living compared to a control period of 2 months
prior to commencing the training program in which the participants were advised to
maintain their normal activities (de Jong et al., 1994).
13
There is also evidence to suggest benefits of participating in anaerobic activities for
children with CF (Klijn et al., 2004). In a randomised design, children were divided
into an exercise (n = 11) and a control group (n = 9). Those randomised to the
exercise group participated in a 12‐week program consisting of two 30‐45 minute
sessions per week. The training consisted of repeated anaerobic activities lasting 20
to 30 seconds. The control group continued their normal activities. The exercise
group showed significant improvements in both anaerobic performance and
cardiorespiratory fitness (assessed via a 30 second Wingate test and an incremental
test of peak oxygen consumption respectively) compared to the control patients
following the 12‐week intervention. Of importance, an increased level of
cardiorespiratory fitness in CF patients is associated with increased survival. Nixon
and colleagues (1992) found that those with a maximal rate of oxygen consumption
(the gold standard measure of cardiorespiratory fitness) greater than 82% of the
predicted value had an 83% 8 year survival rate, compared with a 28% 8 year
survival rate for those with a maximal rate of oxygen consumption less than 58% of
the predicted value.
In addition to the above‐mentioned benefits of regular exercise training for
improving cardiorespiratory fitness in individuals with CF, there is evidence to
suggest that regular aerobic exercise can slow the decline in lung function in CF
patients (Moorcroft et al., 2004; Schneiderman‐Walker et al., 2000). In the
previously described study of Orenstein and colleagues (1981), there was no change
in lung function (based on forced expired volume in 1 second; FEV1) following the
12‐week walk‐jog program, while FEV1 declined over the same period in the control

14
group. Similar results have been observed following longer periods of intervention.
For instance, in a randomised controlled trial of unsupervised home‐based exercise,
participants completed a minimum of 20 minutes of aerobic exercise at a heart rate
of approximately 150 beats/min 3 times a week over a period of 3 years
(Schneiderman‐Walker et al., 2000). Pulmonary function, based on both forced vital
capacity (FVC) and FEV1, declined more slowly in the exercise group, compared to a
control group that were advised to maintain their normal physical activity routine
throughout the study.
Likewise, O’Neill and co‐workers (1987) investigated the effectiveness of exercise in
reducing breathlessness in CF patients. Patients completed the Royal Canadian Air
Force 11 minute exercise protocol each day for a period of 2 months.
Breathlessness was determined via a visual analogue scale before and after a
submaximal cycling test administered pre and post‐intervention. Results indicated a
significant reduction in residual volume (RV) and feelings of breathlessness after
training. However, it is important to note that there was no control group in this
study to allow for comparison.
Another important benefit of exercise for CF patients may relate to sputum
clearance. Dwyer and co‐workers (2011) found improved ease of expectoration of
sputum following an acute bout of 20 minutes of aerobic exercise at a work rate
equivalent to 60% of peak oxygen uptake compared to rest in 14 adults with CF.
These authors suggested that the improved ease of expectoration may be related to
the increase in ventilation and respiratory flow rate during exercise increasing the
15
propulsion of mucus. Of note, treadmill exercise appeared to be more effective than
cycling exercise in decreasing sputum mechanical impedance in this study, perhaps
due to the trunk oscillations associated with treadmill walking (Dwyer et al., 2011).
Furthermore, the addition of exercise to chest physiotherapy may improve lung
function (Thomas et al., 1995) and the weight of sputum expectoration compared
to chest physiotherapy alone (Baldwin et al., 1994).
While regular aerobic exercise appears to have benefits for improving
cardiorespiratory fitness, reducing feelings of breathlessness, attenuating the
decline in lung function and acutely improving the ease of expectoration of sputum,
there is evidence to suggest that resistance training may also provide benefits for CF
patients. In particular, maintaining adequate muscle mass and muscle size is vital
for CF individuals given their difficulty with gaining weight due to pancreatic
insufficiency, malabsorption and malnutrition. Strauss and co‐workers (1987)
examined the effect of 6 months of variable weight training involving 3 sessions per
week of free and machine weights covering both the upper and lower body in 9 CF
patients. The resistance training program was preceded by a 3 month control period
to allow for comparison with the normal progression of the condition. Following the
6 months of resistance training there was significant increases in body mass, muscle
size (based on body circumferences), and muscular strength, while there was no
change in these parameters in the control period. In addition, it was noted that
while the RV and total lung capacity (TLC) declined during the preceding control
period, the RV and RV/TLC ratio improved following training. Such findings relating
to body mass and muscle size may be clinically important given the difficulty of
16
maintaining weight in this population. Of interest, this weight training program was
conducted in a clinical group setting; however, most patients involved in the study
preferred the training to be offered away from the hospital to make it more
convenient. Nonetheless, the reported benefits of resistance training appear
independent to those benefits observed with regular aerobic exercise training. This
raises the question as to the optimal mode of exercise for individuals with CF;
aerobic training, resistance training; or a combination of both?
The effects of aerobic and resistance training for individuals with CF have been
compared in a limited number of studies. Selvadurai and colleagues (2002) assigned
CF children, who were admitted to hospital with pulmonary infection into three
groups; an aerobic training group, a resistance training group and a control group.
Participants in the aerobic and resistance exercise training group were assigned 5
sessions per week of either aerobic training (30 minutes of running on a non‐
motorized treadmill or a stationary cycling at an intensity equivalent to 70%
maximal heart rate) or resistance training (five sets of 10 repetitions for a range of
exercises for both the upper and lower limbs against a graded resistance machine),
while the control group received standard chest physiotherapy. The mean duration
of hospital admission was similar between groups (approximately 19 days). Those
children who received aerobic training had significantly better peak aerobic
capacity, activity levels and quality of life, than children in the resistance group. In
contrast, the children in resistance group had better weight gain, lung function and
leg strength than those allocated to the aerobic training. Based on these findings it
was concluded that perhaps the combination of aerobic and resistance training may

17
provide optimal benefits for CF patients, given the unique benefits of both modes of
exercise for these individuals (Selvadurai et al., 2002).
Of importance, similar benefits have been observed in comparisons of home‐based
strength versus aerobic exercise programs. Orenstein et al., (2004), evaluated a
semi‐supervised, home‐based, training program conducted 3 times a week for 12
consecutive months comparing aerobic and strength training in children with CF.
Patients in the aerobic training group were given a stair stepping machine and
instructed to exercise five minutes per session, gradually increasing to 30 minutes
per session for 3 times per week. In contrast, those allocated to the resistance
training group were given a weight resistance machine, to perform bicep curls,
lateral pull‐downs, military and bench presses 3 times per week. The number of
sets, repetitions and load (resistance) was gradually increased over the year.
Interestingly, both groups showed significant improvements in strength, physical
work capacity and body weight. However, the lack of a ‘usual care’ control group in
this study makes it difficult to conclude whether these changes were directly a
result of the exercise training itself, or simply a result of natural growth changes
over a year.
To examine the effect of a combined aerobic and resistance training program in
patients with CF, Moorcroft and colleagues (2004) evaluated an individualized,
unsupervised, home‐based exercise program in CF patients over 1 year. The
program involved the completion of three 20‐minute sessions per week of whole
body aerobic exercise (jogging, swimming and cycling), combined with upper body

18
exercises with weights. Following the exercise intervention, these researchers
reported significantly higher FVC and a tendency for a lesser decline in FEV1,
compared to a control group which maintained their normal activity levels. In
addition, lower blood lactate concentrations and heart rate responses to constant
load submaximal exercise were observed following the exercise program compared
to controls.
1.6 Exercise and Cystic Fibrosis‐Related Diabetes
Although the benefits of exercise for individuals with CF are well established, no
studies have investigated the effects of regular exercise in patients with CFRD.
While it is likely that exercise training in individuals with CFRD would result in
similar benefits in terms of cardiorespiratory fitness, breathlessness, sputum
clearance and muscle mass to those with CF alone, the effect on blood glucose
management is not known. This is surprising given the central role of regular
exercise for the management of both type 1 and type 2 diabetes mellitus (Horton,
1988). Whether exercise assists in the management of blood glucose levels in
individuals with CFRD is an important issue, given that chronic hyperglycaemia may
lead to a number of serious long‐term health complications, and has significant
effects on an individual’s lung function, leading to an increased rate of decline in
pulmonary function (Koch et al., 2001). Despite the lack of research in this area,
current guidelines recommend that patients with CFRD participate in moderate
aerobic exercise for at least 150 minutes each week (Moran et al., 2010).
19
The role of exercise in improving blood glucose management is related to the large
increase in glucose uptake by the working skeletal muscles during exercise
(Kristiansen et al., 2000). This increase in glucose uptake may result in an acute
lowering of blood glucose levels in those with hyperglycaemia. Furthermore,
exercise improves insulin sensitivity in both healthy individuals (Mikines et al.,
1988), as well as those with type 1 and type 2 diabetes (Cuff et al., 2003; Pederson
et al., 1980).
Although no studies have investigated the effect of exercise training in individuals
with CFRD, it is well established that regular exercise can improve glycaemic control
and insulin sensitivity in patients with type 2 diabetes (Albright et al., 2000; Boule et
al., 2001; Dunstan et al., 2002). More specifically, Sigal and colleagues (2007) have
shown that 22 weeks of aerobic or resistance exercise training improves glycaemic
control in individuals with type 2 diabetes, however, the greatest improvements
were obtained when a combination of aerobic and resistance training were
performed. The benefits of a combined program of aerobic and resistance exercise
for the management of blood glucose levels are further supported by the study of
Maiorana and co‐workers (2002). These researchers reported that 8 weeks of
training, consisting of 1 hour circuit training (combined aerobic and resistance
exercise) three times per week resulted in a significant lowering of glycated
haemoglobin and fasting blood glucose levels in individuals with type 2 diabetes.
Likewise, Cuff and colleagues (2003) revealed greater improvements in insulin
sensitivity (based on glucose requirements during a hyperinsulinaemic‐euglycaemic
clamp) following 16 weeks of combined aerobic (treadmill, stationary bicycle,

20
recumbent stepper, elliptical trainer and rowing machine at 60 – 75% of heart rate
reserve) and resistance exercise (2 sets of 12 repetitions of leg press, leg curl, hip
extension, chest press and lat pull down) training performed 3 days per week,
compared to aerobic exercise alone and a no‐exercise control group in obese post‐
menopausal women with type 2 diabetes.
In contrast, no studies have examined the effects of exercise (aerobic or resistance‐
based) in individuals with CFRD. Rather, the focus of management of CFRD is based
on nutrition and pharmacologic intervention through exogenous insulin
administration (Brennan et al., 2004). Future studies are needed to determine if
regular exercise is indeed beneficial for individuals with CFRD, both in terms of
improving glycaemic control, as well as other aspects of health and well‐being that
have been previously shown to be improved with regular exercise training in those
with CF alone.
1.7 Summary
Regular exercise provides important benefits to individuals with CF. In particular,
regular aerobic exercise training has been shown to improve cardiorespiratory
fitness, sputum expectoration and slow the decline in lung function. These benefits
are of particular importance in CF patients given that they may have a significant
impact on enhancing participation in activities of daily living and improving quality
of life. Furthermore, increased cardiorespiratory fitness has been associated with
increased survival in this population. On the other hand, regular resistance training
provides important benefits for maintaining muscle mass and muscle strength.

21
Based on these unique benefits of both aerobic and resistance exercise training in
individuals in CF, it has been suggested that a combination of these two modes of
exercise may provide optimal benefits for this population. However, despite these
well‐established benefits of exercise for individuals with CF, no studies have
investigated the effects of regular exercise in patients with CFRD. While it is likely
that exercise training in individuals with CFRD would result in similar benefits in
terms of cardiorespiratory fitness, breathlessness, sputum clearance and muscle
mass to those with CF alone, the effect on blood glucose management is not
known. This is important given the association of chronic hyperglycaemia with an
increased rate of decline in pulmonary function. Of note, home‐based exercise
training may be preferred to a centralised institution‐based training program to
allow for individualised supervision and to minimise the potential for transferring
infection between patients. It has also been suggested that home‐based
interventions may be more feasible given that many patients live long distances
from CF centres. However, one limitation of these programs may be the lack of
supervision. Therefore, the purpose of this thesis was to examine the effects of 10
weeks of supervised home‐based aerobic and resistance exercise training on blood
glucose control, cardiorespiratory fitness, muscular strength, lung function, body
composition and quality of life in patients with CFRD.
22
1.8 References
Albright, A., Franz, M., Hornsby, G., Kriska, A., Marrero, D., Ullrich, I., Verity, L.S.
(2000). Exercise and type 2 diabetes. Medicine and Science in Sports and Exercise;
32: 1345 – 1360.
Alexander, S., Bridges, N. (2010). Cystic fibrosis related diabetes. Practical Diabetes
International; 27 (5): 198 – 200.
Augarten, A., Kerem, B.S., Yahav, Y., Noiman, S., Rivlin, Y., Tal, A., Blau, H., Ben‐Turl,
L., Szeinberg, A., Kerem, E. (1993). Mild cystic fibrosis and normal or borderline
sweat test in patients with the 3849 + 10k b C–T mutation. Lancet; 342: 25 – 26.
Baldwin, D.R., Hill, A.L., Peckham, D.G., Knox, A.J. (1994). Effect of addition of
exercise to chest physiotherapy on sputum expectoration and lung function in
adults with cystic fibrosis. Respiratory Medicine; 88 (1): 49 – 53.
Betancourt, M., Slade, G., Dinwiddie, R. (1991). Oxygen saturation in cystic fibrosis.
Archives of Disease in Childhood; 66: 1075 – 1076.
Boule, N.G., Haddad, E., Kenny, G.P., Wells G.A., Sigal, R.J. (2001). Effects of exercise
on glycemic control and body mass in type 2 diabetes mellitus. Journal of American
Medical Association; 286 (10): 1218 – 1227.
23
Braggion, C., Cornacchia, M., Miano, A., Schena, F., Verlato, G., Mastellay, G. (1989).
Exercise tolerance and effects of training in young patients with cystic fibrosis and
mild airways obstruction. Paediatric Pulmonology; 7 (3): 145 ‐ 152.
Brennan, A.L., Geddes, D.M., Gyi, K.M., Baker, E.H. (2004). Clinical importance of
cystic fibrosis‐related diabetes. Journal of Cystic Fibrosis; 3: 209 – 222.
Burdge, D.R., Nakielna, E.M., Noble, M.A. (1993). Case–control and vector studies of
nosocomial acquisition of Pseudomonas cepacia in adults patients with cystic
fibrosis. Chicago Journal; 128 (14): 127 – 130.
Castellani, C., Massie, J. (2010). Emerging issues in cystic fibrosis newborn
screening. Current Opinion in Pulmonary Medicine; 16 (6): 584 – 590.
Chillon, M., Casals, T., Mercier, B., Bassas, L., Lissens, W., Silber, S., Romey, M., Ruiz‐
Romero, J., Verlingue, C., Claustres, M., Nunes, V., Ferec, C., Estivill, X. (1995).
Mutations in cystic fibrosis gene in patients with congenital absence of the vas
deferens. The New England Journal of Medicine; 332 (22): 1475 – 1480.
Clunes, M.T., Boucher, R.C. (2008). Front–runner for pharmacotherapeutic
correction of the airways ion transport defect in cystic fibrosis. Current Opinion in
Pharmacology; 8 (3): 292 – 299.
24
Cohen‐Cymberknoh, M., Shoseyov, D., Kerem, E. (2011). Managing cystic fibrosis:
strategies that increase life expectancy and improve quality of life. American Journal
of Respiratory and Critical Care Medicine; 183: 1463 – 1471.
Costa, M., Potvin, S., Berthiaume, Y., Gauthier, L., Jeanneret, A., Lavoie, A.,
Levesque, R., Chiasson, J.L., Rabasa‐Lhoret, R. (2005). Diabetes: a major co‐
morbidity of cystic fibrosis. Diabetes and Metabolism; 31 (3): 221 – 232.
Counahan, R., Mearns, M.B. (1975). Prevalence of atopy and exercise‐induced
bronchial lability in relatives of patients with cystic fibrosis. Archives of Disease in
Childhood; 50: 477 – 481.
Cuff, D.J., Meneilly, G.S., Martin, A., Ignaszewski, A., Tildesley, H.D., Frohlich, J.J.
(2003). Effective exercise modality to reduce insulin resistance in woman with type
2 diabetes. Diabetes Care; 26: 2977 – 2983.
Davis, P.B., di Sant’Agnese, P.A. (1984). Diagnosis and treatment of cystic fibrosis:
an update. Chest; 85 (6): 802 – 809.
de Jong, W., Grevink, R.G., Roorda, R.J., Kaptein, A.A., van der Schans, C.P. (1994).
Effect of a home exercise training program in patients with cystic fibrosis. Chest;
105 (2): 463 – 468.

25
Dobbin, C., Maley, M., Harkness, J., Benn, R., Malouf, M., Glanville, A., Bye, P.
(2004). The impact of pan‐resistant bacterial pathogens on survival after lung
transplantation in cystic fibrosis: results from a single large referral centre. Journal
of Hospital Infection; 5 (4): 277 – 282.
Dobson, L., Sheldon, C.D., Hattersley, A.T. (2004). Understanding cystic‐ fibrosis‐
related diabetes: best thought of as insulin deficiency? Journal of Royal Society of
Medicine; 97: 26 – 35.
Dunstan, D.W., Daly, R.M., Owen, N., Jolley, D., De Courten, M., Shaw, J., Zimmet, P.
(2002). High‐intensity resistance training improves glycemic control in older
patients with type 2 diabetes. Diabetes Care; 25 (10): 1729 – 1736.
Dwyer, T.J., Alison, J.A., McKeough, Z.J., Daviskas, E., Bye, P.T.P. (2011). Effects of
exercise on respiratory flow and sputum properties in patients with cystic fibrosis.
Chest; 139: (4): 870 – 877.
Edenborough, F.P., Morton, A.M. (2010). Cystic Fibrosis – A guide clinicians in
reproductive and obstetric medicine. Fetal and Maternal Medicine Review; 21: (1)
36 – 54.
Elborn, J.S., Shale, D.J., Britton, J.R. (1991). Cystic fibrosis: current survival and
population estimates to the year 2000. An International Journal of Respiratory
Medicine; 46: 881 – 885.
26
Farrell, P.M., Rosenstein, B.J., White, T.B., Accurso, F.J., Castellani, C., Cutting, G.R.,
Durie, P.R., LeGrys, V.A., Massie, J., Parad, R.B., Rock, M.J., Campbell III, P.W. (2008).
Guidelines for diagnosis of cystic fibrosis in newborns through older adults: Cystic
Fibrosis Foundation Consensus Report. The Journal of Pediatrics; 153: S4 ‐ S14.
Fletcher, G.F., Balady, G., Blair, S.N., Blumenthal, J., Caspersen, C., Chaitman, B.,
Epstein, S., Froelicher, E.S.S., Froelicher, V.F., Pina, I.L., Pollock, M.L. (1996).
Statement on exercise: benefits and recommendations for physical activity
programs for all Americans. Circulation; 94: 857 – 862
Frederiksen, B., Koch, C., Hoiby, N. (1997). Antibiotic treatment of initial
colonization with pseudomonas aeruginosapostpones chronic infection and
prevents deterioration of pulmonary function in cysticfibrosis. Pediatric
Pulmonology; 23 (5): 330 – 335.
Giglio, L., Candusso, M., Orazoi, C.D., Mastella, G., Faraguna, D. (1997). Failure to
thrive: the earliest feature of cystic fibrosis in infants diagnosed by neonatal
screening. Acta Paediatric; 86 (11): 1162 – 1165.
Gilligan, P.H. (1991). Microbiology of airways disease in patients with cystic fibrosis.
Clinical Microbiology Reviews; 4: 35 – 51.

27
Godfrey, S., Mearns, M. (1971). Pulmonary function and response to exercise in
cystic fibrosis, Archives of Disease in Childhood; 46 (246): 144 –151.
Goodyear, L.J., Kahn, B.B. (1998). Exercise, glucose, transport, and insulin sensitivity.
Annual Reviews of Medicine; 49: 235 – 261.
Horton, E.S. (1988). Role and management of exercise in diabetes mellitus.
Diabetes Care; 2 (11): 201 – 211.
Keens, T.G., Krastins, I.R., Wannamaker, E.M., Levinson, H., Crozier, D.N., Bryan, A.C.
(1977). Ventilatory muscle endurance training in normal subject and patients.
American Review of Respiratory Disease; 116: 853 – 860.
Kettler, L.J., Sawyer, S.M., Winefield, H.R., Greville, H.W. (2002). Determinants of
adherence in adults with cystic fibrosis. International Journal of Respiratory
Medicine; 57 (5): 459 – 464.
Klijn, P.H.C., Oudshoorn, A., van der Ent, C.K., Cornelis, K., van der Net, J., Kimpen,
J.L., Helders, P.J.M. (2004). Effect of anaerobic training in children with cystic
fibrosis: a randomized control study. Chest; 125 (4): 1299 – 1305.
Koch, C., Rainisio, M., Madessani, U., Harms, H.K., Hodson, M.E., Mastella, G.,
McKenzie, S.G., Navarro, J., Strandvik, B. (2001). Presence of cystic fibrosis‐related
diabetes mellitus is tightly linked to poor lung function in patients with cystic
28
fibrosis: data from the European Epidemiologic Registry of cystic fibrosis. Pediatric
Pulmonology; 32(5): 343 – 350.
Kristiansen, S., Gade, J., Wojtaszewski, J.F.P., Kiens, B., Ritcher, E.A. (2000). Glucose
uptake is increased in trained vs. untrained muscle during heavy exercise. Journal of
Applied Physiology; 89 (3): 1151 – 1158.
Lippe, B.M., Sperling, M.A., Dooley, R.R. (1977). Pancreatic alpha and beta cell
functions in cystic fibrosis. Journal of Pediatrics; 90: 751 – 755.
Mackie, A.D.R., Thornton, S.J., Edenborough, F.P. (2003). Cystic fibrosis‐related
diabetes. Diabetic Medicine; 20, 425 – 436.
Maiorana, A., O’Driscoll, G., Goodman, C., Taylor, R., Green, D. (2002). Combined
aerobic and resistance exercise improves glycemic control and fitness in type 2
diabetes. Diabetes Research and Clinical Practise; 56 (2): 115 – 123.
Mikines, K.J., Sonne, B., Farrell, P.A., Tronier, B., Galbo, H. (1988). Effect of physical
exercise on sensitivity and responsiveness to insulin in humans. American Journal of
Physiology Endocrinology and Metabolism; 254: E248 – E259.
Milla, C.E., Warwick, W.J., Moran, A. (2000). Trends in pulmonary function in
patients with cystic fibrosis correlate with the degree of glucose intolerance at
baseline. American Journal of Respiratory Critical Care Medicine; 162: 891 – 895.
29
Moorcroft, A.J., Dodd, M.E., Morris, J., Webb, A.K. (2004). Individualised
unsupervised exercise training in adults with cystic fibrosis: a 1 year randomized
controlled trial. International Journal of Respiratory Medicine; 59(12): 1074 – 1080.
Moran, A., Brunzell, C., Choen, R.C., Katz, M., Marshall, B.C., Onady, G., Robinson,
K.A., Sabadosa, K.A., Stecenko, A., Slovis, B. (2010). Clinical care guidelines for cystic
fibrosis‐related diabetes: a position statement of the American Diabetes Association
and a clinical practice guideline od the Cystic Fibrosis Foundation, endorsed by the
Pediatric Endocrine Society. Diabetes Care; 33(12): 2697 – 2716.
Moran, A., Dunitz, J., Nathan, B., Saeed, A., Holme, B., Thomas, W. (2009). Cystic
fibrosis‐related diabetes: current trends in prevalence, incidence, and mortality.
Diabetes Care; 32 (9): 1626 – 1631.
Moran, A., Hardin, D., Rodman, D., Allen, H.F., Beall, R.J., Borowitz, D., Brunzell, C.,
Campbell III, P.W., Chesrown, S.E., Dunchow, C., Fink, R.J., Fitsimmons, S.C.,
Hamilton, N., Hirsch, I., Howenstone, M.S., Klein, D.J., Madhun, Z., Pencharz, P.B.,
Quittner, A.L., Robbins, M.K., Schindler, T., Schissel, K., Schwarzenberg, S.J.,
Stallings, V.A., Tullis, D.E., Zipt, W.B. (1999). Diagnosis, screening and management
of cystic fibrosis related diabetes, Diabetes Research and Clinical Practice; 45: 61 –
73.
30
Muhlebach, M.S., Stewart, P.W., Leigh, M.W., Noah, T.L. (1999). Quantitation of
inflammatory responses to bacteria in young cystic fibrosis and control patients.
American Journal of Respiratory and Critical Care Medicine; 160: 186 –191.
Nixon, P.A., Orenstein, D.M., Kelsey, S.F., Doershuk, C.F. (1992). Prognostic value of
exercise testing in patients with cystic fibrosis. New England Journal of Medicine;
327: 1785 – 1788.
Nixon, P.A., Orenstein, D.M., Kelsey, S.F. (2001). Habitual physical activity in
children and adolescents with cystic fibrosis. Medicine and Science in Sports and
Exercise; 33(1): 30 – 35.
Ojeniyi, B., Frederiksen, B., Hoiby, N. (2000). Pseudomonas aeruginosa cross –
infection among patients with cystic fibrosis during a winter camp. Pediatric
Pulmonology; 29: 177 – 181
O’Neill, P.A., Dodds, M., Phillips, B., Poole, J., Webb, A.K. (1987). Regular exercise
and reduction of breathlessness in patients with cystic fibrosis. British Journal of
Diseases of the Chest; 81: 62 – 69.
Orenstein, D.M., Franklin, B.A., Doershuk, C.F., Hellerstein, H.K., Germann, K.J.,
Horowitz, J.G., Stern, R.C. (1981). Exercise conditioning and cardiopulmonary fitness
in cystic fibrosis: the effects of a three‐month supervised running program. Chest;
80: 392 – 398.
31
Orenstein, D.M., Hovell , M.F., Mulvihill, M., Keating, K.K., Hofstetter, C.R., Kelsey,
S., Morris, K., Nixon, P.A. (2004). Strength vs aerobic training in children with cystic
fibrosis, Chest; 126 (4): 1204 – 1214.
O’Riordan, S.M.P., Robinson, P.D., Donaghue, K.C., Moran, A. (2008). Management
of cystic fibrosis‐related diabetes. Pediatric Diabetes; 9: 338 – 344.
Pederson, O. Beck‐Nielsen, H., Heding, L. (1980). Increased insulin receptors after
exercise in patients with insulin‐dependent diabetes mellitus. New England Journal
of Medicine; 302(16): 886 – 892.
Pencharz, P.B., Durie, P.R. (2000). Pathogenesis of malnutrition in cystic fibrosis, and
its treatment. Clinical Nutrition; 196: 387 – 394.
Prasad, S.A., Cerny, F.J. (2002). Factors that influence adherence to exercise and
their effectiveness: Application to cystic fibrosis. Pediatric Pulmonology; 34 (1): 66 –
72.
Quittner, A. L., Baker, D. H., Carolyn, S., Grimley, M.E., Kristen, M., Ivette, C. (2008).
Prevalence and impact of depression in cystic fibrosis. Current Opinion in Pulmonary
Medicine; 14 (6): 582 – 588.
32
Ramsey, B.W., Farrell, P.M., Pencharz, P.B. (1992). Nutritional assessment and
management in cystic fibrosis: a consensus report. American Journal of Clinical
Nutrition; 55 (1): 108 – 116.
Rana, M., Munns, C.F., Selvadurai, H.C., Simonds, S., Cooper, P.J., Woodhead, H.J.,
Hameed, S., Verge, C.F., Lafferty, A.R., Crock, P.A., Craig, M.E. (2011). Increased
detection of cystic‐fibrosis‐related diabetes in Australia. Archives of Disease in
Childhood, 96: 823 – 826.
Rosenfeld, M., Ramsey, B.W., Gibson, R.L. (2003). Pseudomonas acquisition in
young patients with cystic fibrosis: pathophysiology, diagnosis, and management.
Current Opinion Pulmonary Medicine; 9 (6): 492 – 497.
Rosenstein, B.J., Cutting, G.R. (1998). The diagnosis of cystic fibrosis: A consensus
statement. The Journal of Pediatrics; 132: 589 – 595.
Schneiderman‐Walker, J., Pollock, S.L., Corey, M., Wilkes, D.D., Canny, G.J., Pedder,
L.R., Reisman, J.J. (2000). A randomized controlled trial of a 3 –year home exercise
program in cystic fibrosis. The Journal of Paediatrics; 136 (3): 304 ‐ 310.
Schwarzenberg, S.J., Thomas, W., Olsen, T.W., Grover, T., Walk, D., Milla, C., Moran,
A. (2007). Microvascular complications in cystic fibrosis‐ related diabetes. Diabetes
Care; 30 (5): 1056 – 1061.
33
Selvadurai, H.C., Blimkie, C.J., Meyers, N., Mellis, C.M., Cooper, P.J., and Van
Asperen, P.P. (2002). Randomized controlled study of in–hospital exercise training
program in children with cystic fibrosis. Pediatric Pulmonology; 33(3): 194 – 200.
Sheppard, M.N., Nicholson, A.G. (2002). The pathology of cystic fibrosis. Current
Diagnostic Pathology; 8 (1): 50 – 59.
Shoemaker, M.J., Hurt, H., Arndt, L. (2008). The evidence regarding exercise training
in the management of cystic fibrosis: A systematic review. Journal of
Cardiopulmonary Physical Therapy; 19: (3) 75 – 83.
Sigal, R.J., Kenny, G.P., Boulé, N.G., Wells, G.A., Prud’homme, D., Fortier, M., Reid,
R.D., Tulloch, H., Coyle, D., Phillips, P., Jennings, A., Jaffey, J. (2007). Effect of aerobic
training, resistance training, or both on glycemic control in type 2 diabetes: a
randomized trial. Annuals of Internal Medicine; 147: 357 – 369.
Sinaasappel, M., Stern, M., Littelwood, J., Wolfe, S., Steinkamp, G., Heijerman, H.G.
M., Robberrecht, E., Doring, G. (2002). Nutrition in patients with cystic fibrosis: a
European Consensus. Journal of Cystic Fibrosis; 2: 51 – 75.
Smith, J.J., Travis, S.M., Greenberg, E.P., Welsh, M.J. (1996). Cystic fibrosis airways
epithelia fail to kill bacteria because of abnormal airway surface fluid. Cell; 85 (2):
229 – 236.
34
Strauss, G.D., Osher, A., Wang, C.I., Goodrich, E., Gold, F., Colman, W., Stabile, M.,
Dobrenchuk, A., Keens, T.G. (1987). Variable weight training in cystic fibrosis. Chest;
92: 273 – 276.
Thomas, J., Cook, D.J., Brooks, D. (1995). Chest physical therapy management of
patients with cystic fibrosis: a meta‐analysis. American Journal of Respiratory and
Critical Care Medicine; 151(3): 846 – 850.
Tofe, S., Moreno, J.C., Maiz, L., Alonso, M., Escobar, H., Barrio, R. (2005). Insulin‐
secretion abnormalities and clinical deterioration related to impaired glucose
tolerance in cystic fibrosis. European Journal of Endocrinology; 152: 241 – 247.
Warburton, D.E.R., Nicol, C.W., Bredin, S.S.D. (2006). Health benefits of physical
activity: the evidence. Journal of Canadian Medical Association; 174 (6): 801 – 809.
Wheatley, C.M., Wilkins, B.W., Snyder, E.M. (2011). Exercise Is Medicine in Cystic
Fibrosis. Exercise and Sport Sciences Reviews; 39(3): 155 – 160.
Wilson, D.C., Pencharz, P.B. (1998). Nutrition and cystic fibrosis, Nutrition; 14 (10):
792 – 795.

35
Chapter Two
The effect of 10 weeks of home‐based
supervised aerobic and resistance exercise
training in individuals with cystic fibrosis‐
related diabetes

36
2.1 Introduction
Cystic fibrosis (CF) is the most common (1 in 2500 live births) autosomal recessive
condition in Caucasians leading to premature death. The condition results from a
single gene mutation resulting in defective production of a protein called the cystic
fibrosis transmembrane regulator (CFTR; Sheppard & Nicholson, 2002; Ratjen &
Döring, 2003). This genetic mutation causes dysfunction of cAMP‐dependent
chloride channels, which influence the water and electrolyte composition of
secretions of the respiratory, digestive and reproductive systems (Sheppard &
Nicholson, 2002). This leads to dehydrated viscous secretions that cause progressive
obstruction, scarring and eventually destruction of target organs, especially the
lungs and pancreas. In particular, CF is characterised by recurrent lower respiratory
tract infections due to impaired clearance of dehydrated respiratory secretions, and
subsequent bacterial colonisation (Wat & Doull, 2003). Lung function declines
progressively over time, ultimately leading to respiratory failure and death (Gilligan,
1991). Although there is currently no cure for the disease, life expectancy has
improved dramatically in recent years due to improved management of the
condition (Cohen‐Cymberknoh et al., 2011; Elborn et al., 1991; Simmonds et al.,
2010). However, with this increase in survival, other complications of the condition
have become apparent. In particular, long‐term damage to the pancreas can
ultimately lead to impaired function of the islet cells which are responsible for the
production of the hormone insulin, leading to a type of diabetes that is unique to
those with the disease called cystic fibrosis‐related diabetes (CFRD). As age
increases CFRD is more common, with more than 50% of adults with CF having
abnormal glucose regulation by the time they reach 30 years of age (Alexander &

37
Bridges, 2010). Of importance, chronic high blood glucose may have a long term
effects on lung function, possibly leading to an increased rate of decline in
pulmonary function in individuals with CF (Koch et al., 2001). Other long term
complications, such as retinopathy, nephropathy and neuropathy (Schwarzenberg
et al., 2007) are also associated with CFRD. Consequently, individuals with CFRD
have increased risk of mortality and morbidity compared to patients with CF alone
(Bismuth et al., 2008; Brennan et al., 2004; Moran et al., 1999; O’Riordan et al.,
2008).
Management of CFRD involves a focus on nutrition and pharmacological
intervention. While regular exercise provides important benefits to individuals with
CF, no studies have investigated the effects of regular exercise in patients with
CFRD. Regular aerobic exercise training has been shown to improve
cardiorespiratory fitness (de Jong et al., 1994; Orenstein et al., 1981), and slow the
decline in lung function in patients with CF (Orenstein et al., 1981; Schneiderman‐
Walker et al., 2000). On the other hand, regular resistance training provides
important benefits for maintaining muscle mass and muscle strength in CF
individuals (Selvadurai et al., 2002; Strauss et al., 1987). Based on these unique
benefits of aerobic and resistance exercise training, it has been suggested that a
combination of these two modes of exercise may provide optimal benefits for this
population (Selvadurai et al., 2002). However, the effect of regular exercise on
blood glucose management in CFRD is not known. Home‐based exercise training
may be preferred to a centralised institution‐based training program to allow for
individualised supervision and to minimise the potential for transferring infection
38
between patients (Burdge et al., 1993; Ojeniyi et al., 2000). It has also been
suggested that home‐based interventions may be more feasible given that many
patients live long distances from CF centres (Orenstein et al., 2004; Strauss et al.,
1987). However, one limitation of these programs may be the lack of supervision.
Therefore, the purpose of this study was to examine the effects of 10 weeks of
supervised home‐based aerobic and resistance exercise training on blood glucose
control, cardiorespiratory fitness, muscular strength, lung function, body
composition and quality of life in patients with CFRD.
2.2 Methods and Procedures
2.2.1 Participants
Six patients with CFRD (men n = 3; women n = 3) were recruited from the adult
cystic fibrosis clinic at Sir Charles Gairdner Hospital, Perth, Western Australia, to
participate in this study from September 2010 to August 2011. Patients were
considered ineligible for the study if they were less than 18 years of age, had an
acute respiratory exacerbation, forced expiratory volume below 30% of predicted
value at baseline, were pregnant, or living outside the radius of metropolitan Perth.
One participant was unable to complete the intervention period after baseline data
collection due to a severe respiratory exacerbation requiring extended
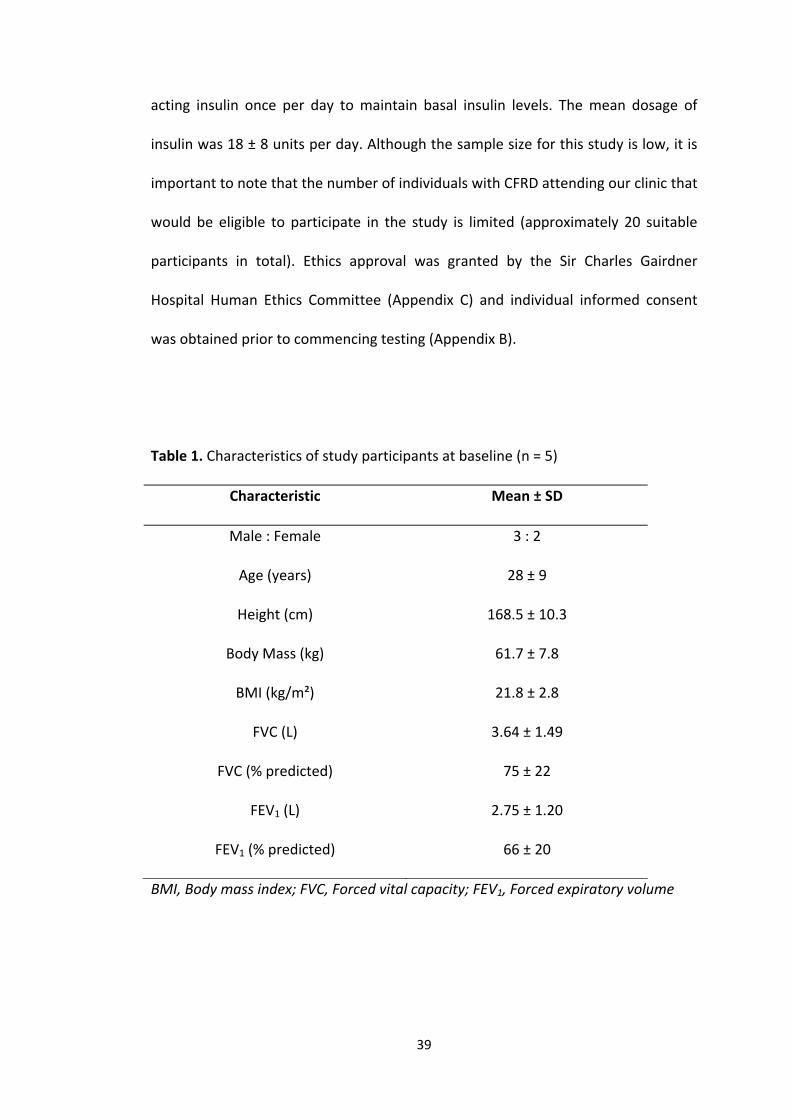
hospitalisation. The characteristics of the remaining five participants that were
included in final data analysis are shown in Table 1. All participants self‐
administered between 1 to 4 insulin injections per day. The regime of two patients
consisted of short‐acting insulin alone, while the remaining three participants used
a combination of short‐acting insulin 2‐3 times per day to cover meals and long‐
39
acting insulin once per day to maintain basal insulin levels. The mean dosage of
insulin was 18 ± 8 units per day. Although the sample size for this study is low, it is
important to note that the number of individuals with CFRD attending our clinic that
would be eligible to participate in the study is limited (approximately 20 suitable
participants in total). Ethics approval was granted by the Sir Charles Gairdner
Hospital Human Ethics Committee (Appendix C) and individual informed consent
was obtained prior to commencing testing (Appendix B).
Table 1. Characteristics of study participants at baseline (n = 5)
Characteristic Mean ± SD
Male : Female 3 : 2
Age (years) 28 ± 9
Height (cm) 168.5 ± 10.3
Body Mass (kg) 61.7 ± 7.8
BMI (kg/m²) 21.8 ± 2.8
FVC (L) 3.64 ± 1.49
FVC (% predicted) 75 ± 22
FEV1 (L) 2.75 ± 1.20
FEV1 (% predicted) 66 ± 20
BMI, Body mass index; FVC, Forced vital capacity; FEV1, Forced expiratory volume
40
2.2.2 Research Design
Participants were randomly allocated to either a 10 week exercise intervention or a
10 week control period, before a 10 week wash‐out period and crossing over to the
alternative intervention. Participants allocated to the exercise intervention were
required to participate in 10 weeks of supervised, home‐based exercise training
(two 1 hour sessions per week of combined aerobic and resistance training), whilst
during the 10 week control period participants were required to continue with their
normal activity routine. Outcome measures were assessed pre‐ and post‐
intervention. Each participant was recruited and commenced the intervention
during different months of the year (from September 2010 – May 2011), minimising
the risk of any potential bias in results based on seasonal variation in outcome
measures.
2.2.3 Exercise Intervention
The exercise intervention involved 10 weeks of supervised, home‐based aerobic and
resistance exercise training. The participants completed 2 sessions per week, for a
duration of 1 hour each (20 sessions in total), with the investigator visiting their
home to conduct the training. This method of home‐based training was preferred to
a centralised institution‐based training program to allow for individualised
supervision and to minimise the potential for transferring infection between
patients. Each session commenced with 20 minutes of aerobic exercise at 70% of
age‐predicted heart rate max on a stationary bike (Healthstream, Marquee Series;
U3MB103) that was provided to each participant to keep in their home for the
duration of the intervention. If participants improved over the course of the training
41
period the workload increased, while maintaining the same heart rate. This was
followed by 3 sets of 12 repetitions of the following exercises covering each major
muscle group of the body: (bicep curls, triceps extension, shoulder press, dead lift,
flat bench press, squat and calf raises). Between each set, participants were given
20 seconds of recovery. On completion of all 3 sets of each exercise, 2 minutes of
rest was given for muscle recovery before moving on to the next exercise. Initially,
the load (kg) to be lifted for each exercise was individually calculated based on 30%
of 6 repetition maximum (RM) for the upper body and 50% of 6‐RM for the lower
body, this was based on prior pilot testing. The load lifted was increased every 2
weeks in increments of 5%. At the end of each training session, 5 minutes of static
stretching was completed.
For safety purposes, each participant’s oxygen saturation (SpO₂) was continuously
assessed via a pulse oximeter (Nonin Onyx, PureSAT technology, Hudiksvall Sweden)
during stationary cycling, and before and after each set of resistance exercises.
Supplemental oxygen was available at all times in case an unexpected drop in SpO₂
occurred. In addition, blood glucose levels were assessed before and after each
training session using a glucometer (OptiumXceed, Abbott Technologies, California,
USA). Exercise training did not commence unless the patient’s blood glucose was >
5 and < 15 mM. The investigator was trained in the recognition and management of
hypoglycaemia and appropriate therapies, including the administration of
intramuscular glucagon if necessary, which was available in case of hypoglycaemia.
2.2.4 Outcome Measures

42
Outcome measures were obtained at baseline (pre‐intervention) and 10 weeks later
(post intervention), and again following the wash‐out period pre‐ and post‐
intervention. All testing was completed in the Department of Respiratory Medicine
at Sir Charles Gairdner Hospital during two separate visits. For the first visit,
participants arrived in the morning in a fasted state to complete a 75 g oral glucose
tolerance test (OGTT). After completion of the OGTT, participants were allowed to
eat and drink, before measures of body composition, lung function,
cardiorespiratory fitness, quality of life and 6‐RM testing for each resistance
exercise listed previously were obtained. Following these tests, each participant was
fitted with a continuous glucose monitoring system (CGMS) to monitor glycaemia
for the subsequent 3 days. The second visit was scheduled 3 days later to allow for
removal of the CGMS.
2.2.4a Assessment of Diabetes Control
Prior to arrival for the first testing visit, patients were instructed to fast overnight
for 10 hours. Upon arrival to the hospital, a fasting blood sample was taken from
an antecubital vein, prior to the ingestion of a 75 g of glucose solution. Further
blood samples were obtained at 60 and 120 minutes post‐ingestion to monitor the
blood glucose response to the oral glucose load. Later that day, a CGMS (Guardian
System, Medtronic, USA) was fitted by a nurse experienced in the procedure to
allow for the assessment of daily glucose exposure for the subsequent 3 days
(Mastrototaro, 2000). The device was inserted in the abdominal wall, 5 cm lateral to
the navel according to the manufacturer’s specifications. For the subsequent 3 days,
participants calibrated the CGMS four times daily using their personal blood glucose
43
monitor. Following the 3 days of monitoring, each participant returned to the
hospital for removal of the device by the same nurse to allow for subsequent
uploading of stored data and analysis using Medtronic Carelink iPro software. The
percentage of time spent in (3.8‐10.0 mM) above (>10.0 mM) or below (<0.38 mM)
the normal glucose range was determined over the 3‐day period. Finally the mean
number of excursion above and below these limits was also recorded. Participants
were blinded to their glucose values to ensure that they would not alter their
behaviour based on real‐time feedback. Although participants were instructed to
maintain their normal food intake and physical activity patterns over the 3‐day
monitoring period, this was not quantitatively monitored given the already highly
demanding nature of managing CF alone.
2.2.4b Assessment of Cardiorespiratory Fitness
Cardiorespiratory fitness was assessed by two separate commonly used submaximal
exercise tests. First, participants were asked to perform a modified shuttle test
(Bradley et al., 1999). This test has previously been shown to be a reliable and
sensitive measure of exercise capacity in adults with CF (Bradley et al., 2000).
Briefly, the test consisted of 15‐levels of externally paced walking (or running) up
and down a 10 m course. The course was identified by two cones inset 0.5 m from
either end to avoid the need for abrupt changes in direction. The speed at which
the participant walked was dictated by an audio signal played on CD player and
progressively increased at each level, with the participant continuing until they
could not keep pace with the required speed for two consecutive laps, or if their
SpO2 dropped below 84%.

44
As cycling was used in the intervention program a second submaximal aerobic test
using cycling was conducted. Following 20 minutes of rest, participants were then
required to complete the Physical Work Capacity (PWC)‐170 test. This submaximal
cycling test consists of 3 levels of progressively increasing workload from which the
heart rate response to exercise is monitored to determine the workload at which a
heart rate of 170 bpm would be expected to be achieved (Gore et al., 1999). Prior to
each test, blood glucose level and SpO₂ level were assessed for each participant to
confirm that it was safe to proceed with the exercise.
2.2.4c Assessment of Muscular Strength
The 6‐RM for each patient was assessed for a range of different resistance exercises
including bicep curl, triceps extension, shoulder press, dead lift, flat bench press,
squat and calf raise. This allowed for an assessment of muscular strength, as well as
to assist with determining the appropriate load to be prescribed in the home‐based
exercise program as described earlier.
2.2.4d Assessment of Pulmonary Function
Patients performed at least three tests of pulmonary function (Medgraphics
CPFS/D, Medical Graphics Corporation, USA) to determine forced vital capacity
(FVC), forced expiratory volume (FEV1) and the FEV1/FVC. The highest result among
the three tests was documented. To ensure repeatability of results, the patient’s
trunk and neck remained erect in an upright sitting position during the manoeuvers,
45
with the patient looking straight forward during the entire test without bending
over (Miller et al., 2005).
2.2.4e Assessment of Body Composition
Body mass was measured to the nearest 0.1 kg using digital scales (TANITA model
HD 309). Height was measured by a Body meter (SECA Model 208), with
participants requested to stand bare feet below the center of the measuring
tongue, leaning against the wall with the back straight, heels resting together
against the wall and the hands loosely by the side. Based on the height and body
mass measured, each participant’s body mass index (BMI) was calculated. In
addition, dual energy X‐ray absorptiometry (DEXA; Discovery A S/N 82641) was
performed to assess body composition (lean muscle mass, fat mass and bone
mineral density) pre and post‐intervention. Briefly, this required participants to lie
supine on a scanning bed for 5‐10 minutes, while a low dose x–ray was
administered (Rochet et al., 1994).
2.2.4f Assessment of Quality of Life
Quality of life was assessed pre‐ and post‐intervention using the revised cystic
fibrosis questionnaire (CFQ‐R; Appendix E; Quittner et al., 2011). This questionnaire
was specifically developed for individuals with cystic fibrosis and consists of 50
questions that are grouped into four domains including; demographics, quality of
life, daily activities and symptom difficulties.
2.2.4g Evaluation the Frequency and Duration of Hospitalisation
46
Each participant’s hospital records were monitored throughout the intervention
period, to evaluate the frequency and duration of hospital admissions due to CFRD
problems.
2.2.5 Statistical Analysis
Data were analysed using SPSS version 17.0 (SPSS, Chicago, Illinois), with
significance set at p < 0.05. Two‐way (group x time) repeated measures ANOVA
were used to determine the effect of the intervention on each outcome variable,
with post‐hoc pair‐wise comparisons performed to determine where any
differences lay. Area under the curve (AUC) was calculated using the trapezoidal
rule for glucose exposure during the OGTT.
2.3 Results
2.3.1 Exercise Training Characteristics
The characteristics of the home‐based, supervised exercise training program are
shown in Table 2. Each participant completed all 20 scheduled sessions (100%
compliance). Blood glucose levels were acutely lowered in response to exercise, but
were maintained within an appropriate range, with an average of 1 hypoglycaemic
episode per participant throughout the entire 10 week exercise intervention period.
All episodes were mild in nature (ranged between 3.2‐3.8 mM) and were treated
immediately. Oxygen saturation before and after exercise was maintained at
appropriate levels, with no requirement to administer supplemental oxygen.
Despite the 100% compliance rate to the exercise program, it is important to note
that one participant completed the exercise intervention period only, since she was
47
unable to complete to control period due to time constraints. Therefore 5
participants completed the full exercise intervention period and 4 completed the
equivalent control period.
Table 2. Characteristics of the 10 week home‐based supervised exercise program
(mean ± SD).
Variables
Compliance (% sessions completed) 100%
Blood glucose (mM) pre‐session 9.8 ± 2.1
Blood glucose (mM) post‐session 7.3 ± 1.5*
Episodes of hypoglycaemia 1 ± 2
Oxygen saturation (%) pre‐session 96 ± 3
Oxygen saturation (%) post‐session 95 ± 3*
* Indicates significant difference (p < 0.05) from pre‐session.
2.3.2 Effect of Exercise Training on Cardiorespiratory Fitness
The effect of the exercise and control period on cardiorespiratory fitness (based on
the PWC170 and modified shuttle test) are shown in Table 3. There was no change in
cardiorespiratory fitness indicators following the 10 week control period. In
contrast, the PWC170 (in kpm/min and kpm/kg/min) was significantly improved
following the 10 week home‐based supervised exercise training program (p = 0.018
and p = 0.033 respectively). Likewise, there was a significant improvement in the
total distance covered (p = 0.042) and maximum speed (p = 0.04) in the modified

48
shuttle test following the exercise intervention, indicating an improvement in
functional capacity.
Table 3. Effect of 10 weeks of home‐based supervised aerobic and resistance
exercise training (EX) or control (CON) on cardiorespiratory fitness in individuals
with cystic fibrosis‐related diabetes (mean ± SD).
Pre CON Post CON Pre EX Post EX
PWC170
PWC170 (kpm/min) 832 ± 164 880 ± 196 754 ± 149 910 ± 201*
PWC170 (kpm/kg/min) 13.3 ± 2.8 14.6 ± 4.7 12.2 ± 1.9 14.5 ± 3.0*
Modified Shuttle Test
Distance covered (m) 1052 ± 408 1052 ± 408 750 ± 319 1098 ± 318*
Maximum speed (km/hr) 8.5 ± 1.8 8.5 ± 1.8 7.2 ± 1.5 8.8 ± 1.3*
* Indicates significant difference (p < 0.05) from pre‐exercise intervention.
2.3.3 Effect of Exercise Training on Muscular Strength
The change in strength (based on 6‐RM for a range of different resistance exercises)
over the 10 week intervention period is shown in Table 4. There was no change in 6‐
RM during the control period for any of the exercises, except for flat bench lift in
which a significant decline in strength was noted (p = 0.034). On the other hand,
following the exercise intervention, there was a significant increase in strength for
all exercises (bicep curl p = 0.02; triceps extension p = 0.016; shoulder press p =
0.018; dead lift p = 0.018; flat bench press p = 0.005; squat p = 0.008), although the
increase in 6‐RM for the calf raise did not achieve statistical significance (p = 0.084).
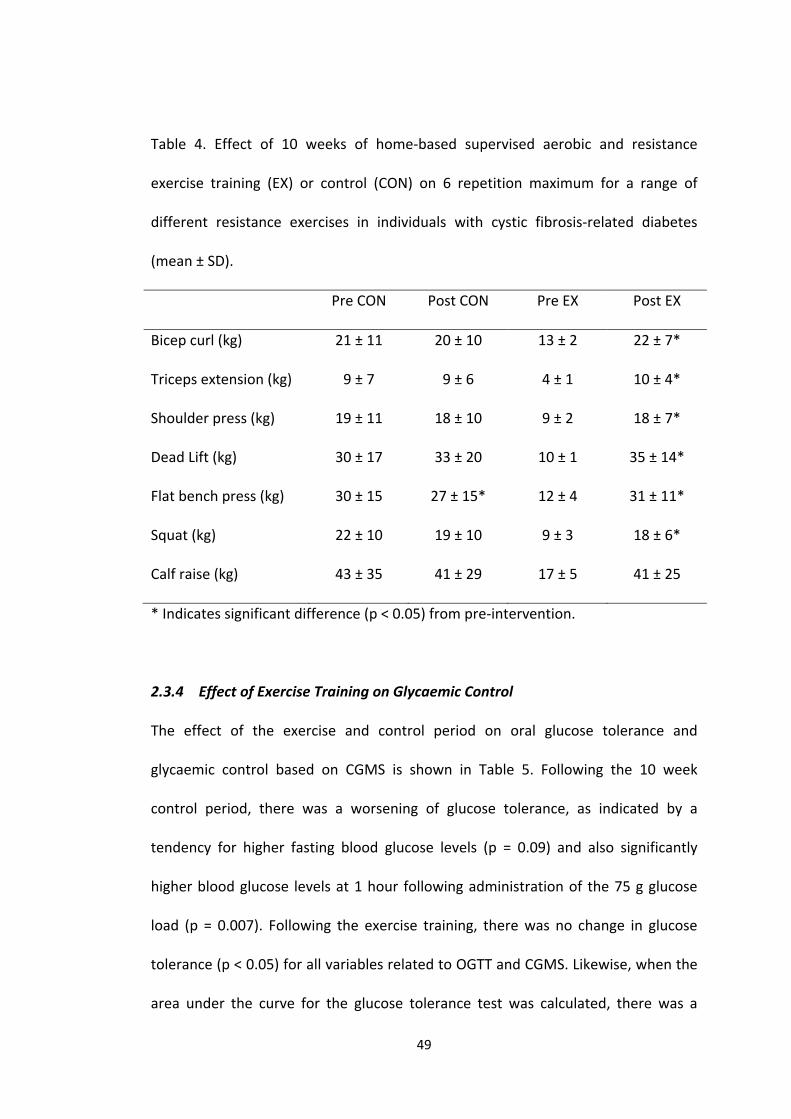
49
Table 4. Effect of 10 weeks of home‐based supervised aerobic and resistance
exercise training (EX) or control (CON) on 6 repetition maximum for a range of
different resistance exercises in individuals with cystic fibrosis‐related diabetes
(mean ± SD).
Pre CON Post CON Pre EX Post EX
Bicep curl (kg) 21 ± 11 20 ± 10 13 ± 2 22 ± 7*
Triceps extension (kg) 9 ± 7 9 ± 6 4 ± 1 10 ± 4*
Shoulder press (kg) 19 ± 11 18 ± 10 9 ± 2 18 ± 7*
Dead Lift (kg) 30 ± 17 33 ± 20 10 ± 1 35 ± 14*
Flat bench press (kg) 30 ± 15 27 ± 15* 12 ± 4 31 ± 11*
Squat (kg) 22 ± 10 19 ± 10 9 ± 3 18 ± 6*
Calf raise (kg) 43 ± 35 41 ± 29 17 ± 5 41 ± 25
* Indicates significant difference (p < 0.05) from pre‐intervention.
2.3.4 Effect of Exercise Training on Glycaemic Control
The effect of the exercise and control period on oral glucose tolerance and
glycaemic control based on CGMS is shown in Table 5. Following the 10 week
control period, there was a worsening of glucose tolerance, as indicated by a
tendency for higher fasting blood glucose levels (p = 0.09) and also significantly
higher blood glucose levels at 1 hour following administration of the 75 g glucose
load (p = 0.007). Following the exercise training, there was no change in glucose
tolerance (p < 0.05) for all variables related to OGTT and CGMS. Likewise, when the
area under the curve for the glucose tolerance test was calculated, there was a
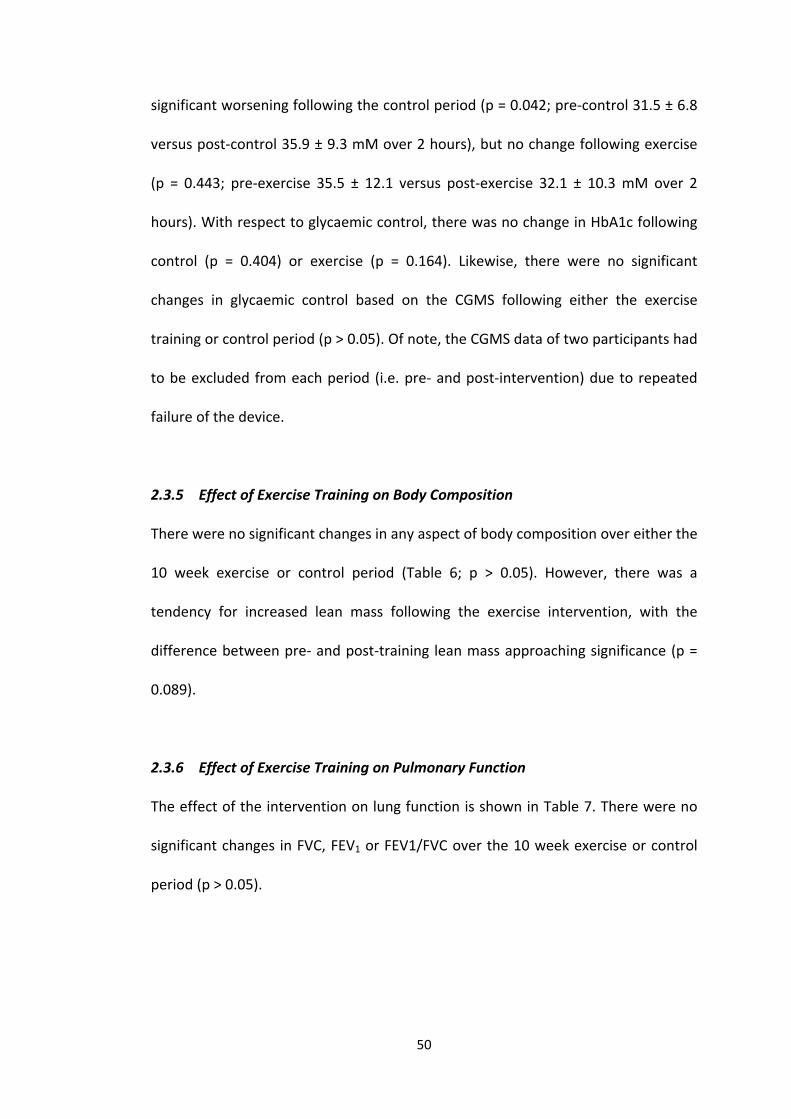
50
significant worsening following the control period (p = 0.042; pre‐control 31.5 ± 6.8
versus post‐control 35.9 ± 9.3 mM over 2 hours), but no change following exercise
(p = 0.443; pre‐exercise 35.5 ± 12.1 versus post‐exercise 32.1 ± 10.3 mM over 2
hours). With respect to glycaemic control, there was no change in HbA1c following
control (p = 0.404) or exercise (p = 0.164). Likewise, there were no significant
changes in glycaemic control based on the CGMS following either the exercise
training or control period (p > 0.05). Of note, the CGMS data of two participants had
to be excluded from each period (i.e. pre‐ and post‐intervention) due to repeated
failure of the device.
2.3.5 Effect of Exercise Training on Body Composition
There were no significant changes in any aspect of body composition over either the
10 week exercise or control period (Table 6; p > 0.05). However, there was a
tendency for increased lean mass following the exercise intervention, with the
difference between pre‐ and post‐training lean mass approaching significance (p =
0.089).
2.3.6 Effect of Exercise Training on Pulmonary Function
The effect of the intervention on lung function is shown in Table 7. There were no
significant changes in FVC, FEV1 or FEV1/FVC over the 10 week exercise or control
period (p > 0.05).
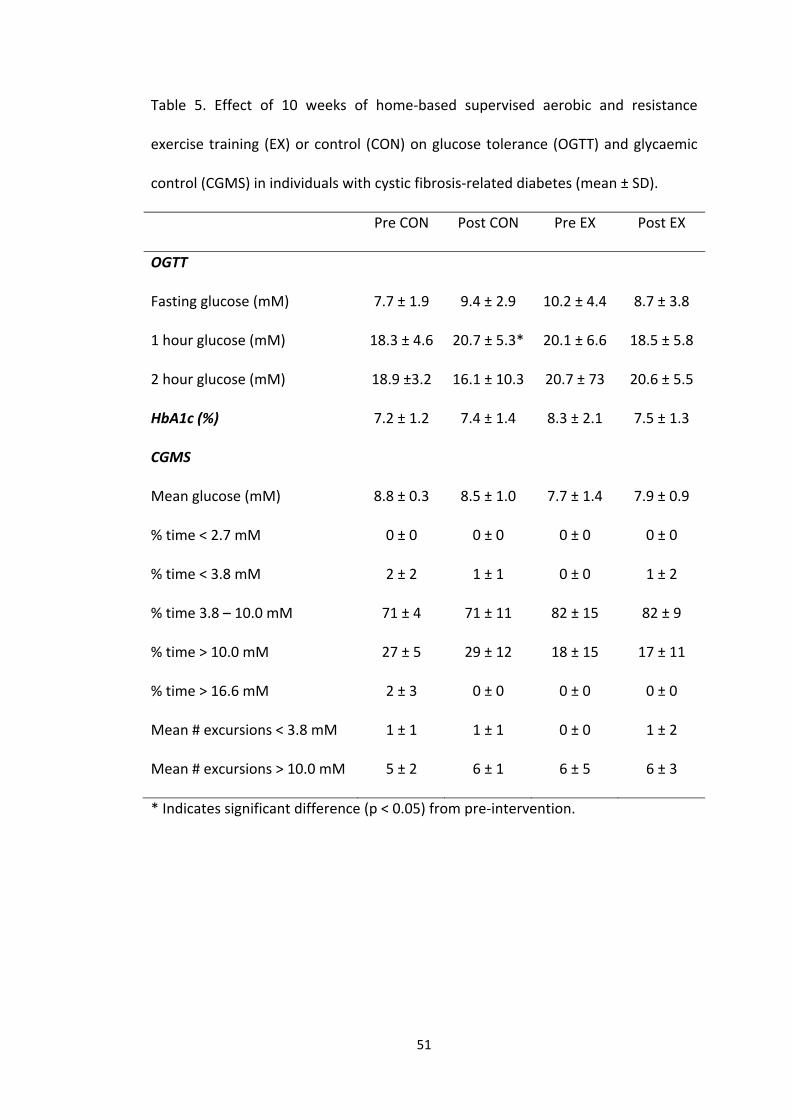
51
Table 5. Effect of 10 weeks of home‐based supervised aerobic and resistance
exercise training (EX) or control (CON) on glucose tolerance (OGTT) and glycaemic
control (CGMS) in individuals with cystic fibrosis‐related diabetes (mean ± SD).
Pre CON Post CON Pre EX Post EX
OGTT
Fasting glucose (mM) 7.7 ± 1.9 9.4 ± 2.9 10.2 ± 4.4 8.7 ± 3.8
1 hour glucose (mM) 18.3 ± 4.6 20.7 ± 5.3* 20.1 ± 6.6 18.5 ± 5.8
2 hour glucose (mM) 18.9 ±3.2 16.1 ± 10.3 20.7 ± 73 20.6 ± 5.5
HbA1c (%) 7.2 ± 1.2 7.4 ± 1.4 8.3 ± 2.1 7.5 ± 1.3
CGMS
Mean glucose (mM) 8.8 ± 0.3 8.5 ± 1.0 7.7 ± 1.4 7.9 ± 0.9
% time < 2.7 mM 0 ± 0 0 ± 0 0 ± 0 0 ± 0
% time < 3.8 mM 2 ± 2 1 ± 1 0 ± 0 1 ± 2
% time 3.8 – 10.0 mM 71 ± 4 71 ± 11 82 ± 15 82 ± 9
% time > 10.0 mM 27 ± 5 29 ± 12 18 ± 15 17 ± 11
% time > 16.6 mM 2 ± 3 0 ± 0 0 ± 0 0 ± 0
Mean # excursions < 3.8 mM 1 ± 1 1 ± 1 0 ± 0 1 ± 2
Mean # excursions > 10.0 mM 5 ± 2 6 ± 1 6 ± 5 6 ± 3
* Indicates significant difference (p < 0.05) from pre‐intervention.
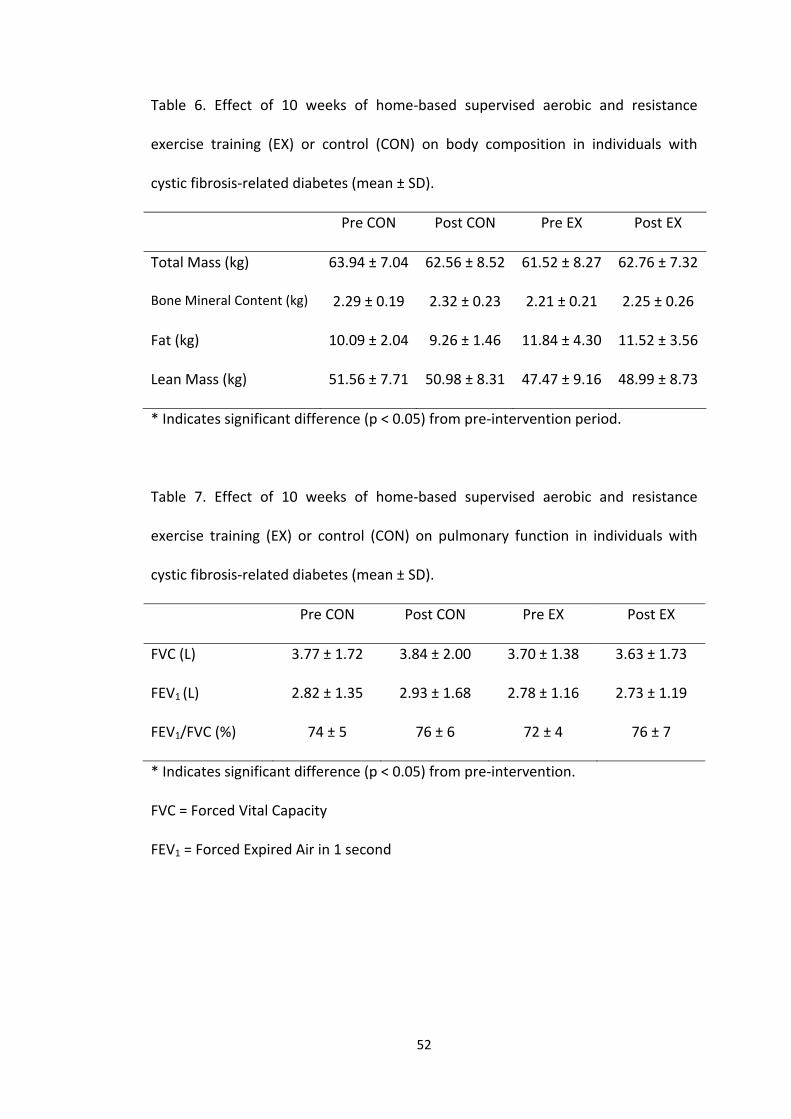
52
Table 6. Effect of 10 weeks of home‐based supervised aerobic and resistance
exercise training (EX) or control (CON) on body composition in individuals with
cystic fibrosis‐related diabetes (mean ± SD).
Pre CON Post CON Pre EX Post EX
Total Mass (kg) 63.94 ± 7.04 62.56 ± 8.52 61.52 ± 8.27 62.76 ± 7.32
Bone Mineral Content (kg) 2.29 ± 0.19 2.32 ± 0.23 2.21 ± 0.21 2.25 ± 0.26
Fat (kg) 10.09 ± 2.04 9.26 ± 1.46 11.84 ± 4.30 11.52 ± 3.56
Lean Mass (kg) 51.56 ± 7.71 50.98 ± 8.31 47.47 ± 9.16 48.99 ± 8.73
* Indicates significant difference (p < 0.05) from pre‐intervention period.
Table 7. Effect of 10 weeks of home‐based supervised aerobic and resistance
exercise training (EX) or control (CON) on pulmonary function in individuals with
cystic fibrosis‐related diabetes (mean ± SD).
Pre CON Post CON Pre EX Post EX
FVC (L) 3.77 ± 1.72 3.84 ± 2.00 3.70 ± 1.38 3.63 ± 1.73
FEV1 (L) 2.82 ± 1.35 2.93 ± 1.68 2.78 ± 1.16 2.73 ± 1.19
FEV1/FVC (%) 74 ± 5 76 ± 6 72 ± 4 76 ± 7
* Indicates significant difference (p < 0.05) from pre‐intervention.
FVC = Forced Vital Capacity
FEV1 = Forced Expired Air in 1 second
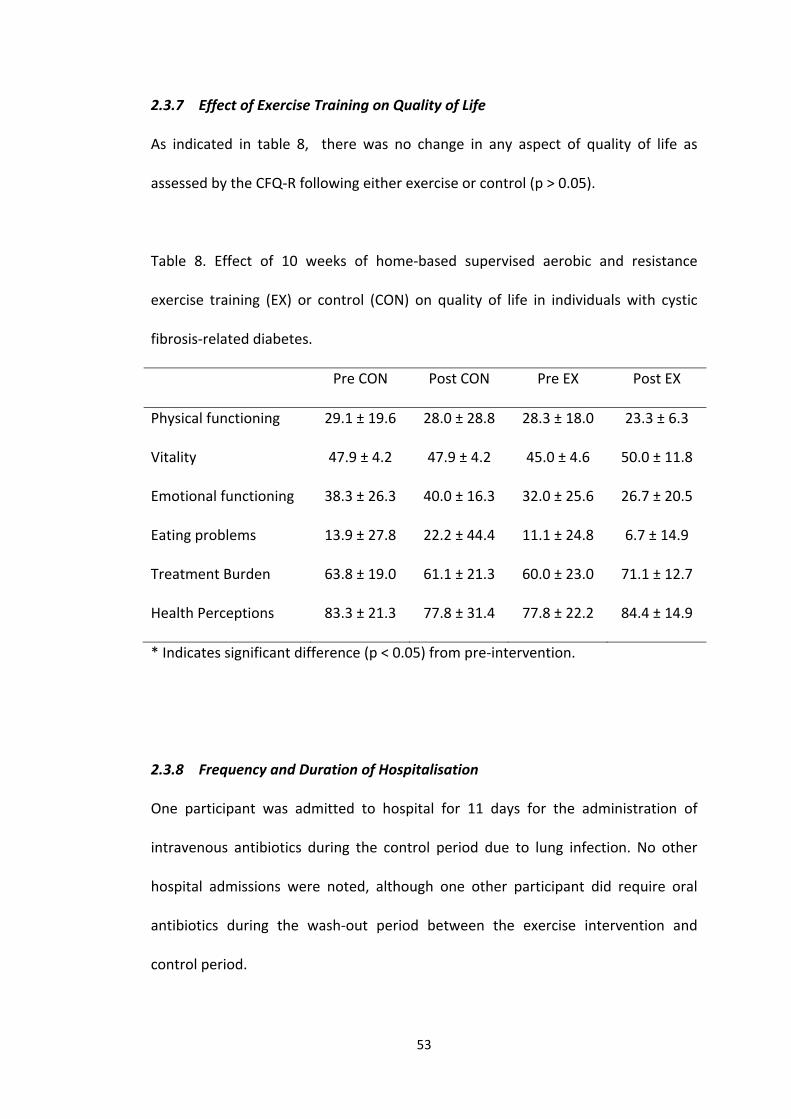
53
2.3.7 Effect of Exercise Training on Quality of Life
As indicated in table 8, there was no change in any aspect of quality of life as
assessed by the CFQ‐R following either exercise or control (p > 0.05).
Table 8. Effect of 10 weeks of home‐based supervised aerobic and resistance
exercise training (EX) or control (CON) on quality of life in individuals with cystic
fibrosis‐related diabetes.
Pre CON Post CON Pre EX Post EX
Physical functioning 29.1 ± 19.6 28.0 ± 28.8 28.3 ± 18.0 23.3 ± 6.3
Vitality 47.9 ± 4.2 47.9 ± 4.2 45.0 ± 4.6 50.0 ± 11.8
Emotional functioning 38.3 ± 26.3 40.0 ± 16.3 32.0 ± 25.6 26.7 ± 20.5
Eating problems 13.9 ± 27.8 22.2 ± 44.4 11.1 ± 24.8 6.7 ± 14.9
Treatment Burden 63.8 ± 19.0 61.1 ± 21.3 60.0 ± 23.0 71.1 ± 12.7
Health Perceptions 83.3 ± 21.3 77.8 ± 31.4 77.8 ± 22.2 84.4 ± 14.9
* Indicates significant difference (p < 0.05) from pre‐intervention.
2.3.8 Frequency and Duration of Hospitalisation
One participant was admitted to hospital for 11 days for the administration of
intravenous antibiotics during the control period due to lung infection. No other
hospital admissions were noted, although one other participant did require oral
antibiotics during the wash‐out period between the exercise intervention and
control period.
54
2.4 Discussion
Although the benefits of regular exercise for patients with CF are reasonably well
established, no studies have investigated the effects of regular exercise training in
individuals with CFRD. This is despite the central role of regular exercise for the
management of both type 1 and type 2 diabetes mellitus (Horton, 1988). For the
first time, we have examined the effects of 10 weeks of supervised home‐based
aerobic and resistance exercise training on blood glucose control, cardiorespiratory
fitness, muscular strength, lung function, body composition and quality of life in
patients with CFRD. Despite the small cohort that could be included in the present
study, we found that exercise training improved cardiorespiratory fitness and
muscular strength, and tended to increase lean body mass. However, there were no
significant changes in glucose tolerance or glycaemic control following the exercise
intervention, likely as a result of the small sample size; although following the
equivalent control period there was a worsening of glucose tolerance to an oral
glucose load and a tendency for increased fasting blood glucose levels. While there
were no significant changes in lung function or quality of life as a result of the
intervention, this study shows that 10 weeks of combined aerobic and resistance
training in the home of patients with CFRD is both feasible and warmly welcomed.
The improvement in cardiorespiratory fitness following the exercise intervention is
consistent with previous research in patients with CF alone. Orenstein et al. (1981)
showed improved cardiorespiratory fitness based on both peak rate of oxygen
consumption and significantly lower heart rates at submaximal workloads following
a 12 week program of jog‐walking and non‐competitive recreational games (1 hour
55
x 3 times per week) in patients with CF compared to an inactive control group.
Likewise, 12 weeks of home‐based stationary cycling performed daily (with 2
sessions per week supervised) has been shown to improve the maximal rate of
oxygen consumption compared to a control period of 2 months prior to
commencing the training program in which participants were advised to maintain
their normal activities (de Jong et al., 1994). Of interest, the present study has
shown increased cardiorespiratory fitness with as little as 2 sessions of exercise per
week. This is important given the potential implications for enhancing participation
in activities of daily living (de Jong et al., 1994) and the relationship between
increased levels of cardiorespiratory fitness and survival in CF (Nixon et al., 1992).
The improvement in muscular strength in the present study supports a previous
observation of increased strength following resistance training in patients with CF
alone. Strauss and co‐workers (1987) reported significant increases in muscular
strength, body mass and muscle size (based on body circumferences) following 6
months of variable weight training involving 3 sessions per week of free and
machine weights covering both the upper and lower body in 9 CF patients. The
resistance training program was preceded by a 3 month control period to allow for
comparison with the normal progression of the disease. Here, we have shown that
improvements in strength can be obtained in as little as 10 weeks, with a program
of combined aerobic and resistance exercise. These improvements in strength were
associated with a tendency for increased lean muscle mass as measured using the
gold‐standard DEXA. Perhaps these results would have reached statistical
significance with a longer intervention period or a greater number of participants.
56
Nonetheless, these trends are likely important given that maintaining adequate
muscle mass is vital for CF individuals due to their difficulties with gaining weight as
a result of malabsorption and malnutrition. Indeed, body mass is an important
predictor of morbidity and mortality among children with CF (Orenstein et al.,
2004).
With respect to lung function, we saw no change in FVC or FEV1 following 10 weeks
of exercise training or control. Previous research has reported a slower rate of
decline in lung function over a 3 year period in CF patients that completed 3
sessions per week of unsupervised home‐based aerobic exercise compared to CF
controls (Schneiderman‐Walker et al., 2000). Likewise, resistance training has been
shown to be beneficial in slowing the decline in lung function in CF, with improved
residual volume (RV) and RV/total lung capacity ratio following 6 months of
resistance training, contrasted with a decline in FVC and RV during a preceding
control period (Strauss et al., 1987). When combined, 1 year of aerobic and
resistance training resulted in significantly higher FVC and a tendency for a lesser
decline in FEV1 in CF patients, compared to a control group which maintained their
normal activity levels (Moorcroft et al., 2004). The contrasting lack of attenuation in
the decline in lung function observed in the present study is likely a result of the
relatively short duration of the intervention period in comparison with the above‐
mentioned studies. In support of this notion, no change in pulmonary function was
observed by de Jong and coworkers (1994) following their exercise intervention
which was of a similar duration to the present study (12 weeks). Future research
should investigate the effect of longer periods of aerobic and resistance exercise
57
training on pulmonary function in individuals with CFRD given the strong association
between high glucose levels and pulmonary decline.
While it is not surprising that the benefits of exercise for cardiorespiratory fitness,
muscular strength and muscle mass in CFRD are similar to those observed in
patients with CF alone, the effect on blood glucose management has not previously
been reported. This is an important issue given that chronic hyperglycaemia may
lead to a number of serious long‐term health complications, and is associated with
an increased rate of decline in pulmonary function (Koch et al., 2001). The role of
exercise in improving blood glucose management is related to the large increase in
glucose uptake by the working skeletal muscles during exercise (Kristiansen et al.,
2000). This increase in glucose uptake may result in an acute lowering of blood
glucose levels in those with hyperglycaemia. For the first time, this study
demonstrates that a session of aerobic and resistance exercise acutely lowers blood
glucose levels in patients with CFRD. Of importance, this acute lowering of
glycaemia maintained glucose within an appropriate range (mean lowering from 9.8
to 7.3 mM), with an average of only 1 episode of mild hypoglycaemia (ranged from
3.2 – 3.8 mM) detected post‐exercise throughout the 10 week intervention.
Nonetheless, the fact that some episodes of post‐exercise hypoglycaemia were
experienced highlights the need to encourage patients to always check blood
glucose levels before and after exercise.
Although the transient lowering of blood glucose resulting from an acute session of
combined aerobic and resistance exercise may be beneficial for patients with CFRD,

58
the main benefit of exercise for those with impaired glucose regulation relates to
improved glycaemic control in the longer‐term. Ten weeks of exercise training did
not significantly improve the blood glucose response to an oral glucose load in CFRD
patients in the present study. However, it was interesting to note that glucose
tolerance declined following the equivalent control period. The lack of improved
glucose response to an oral glucose load may not be unexpected given that the
benefits of exercise typically lie in improved sensitivity to insulin at peripheral sites,
whereas insulin sensitivity is not the predominant contributing factor in CFRD
(Bismuth et al., 2008). Instead, insulin secretion is blunted and delayed in CFRD
patients (Hartling et al., 1988). Whether the worsening of glucose tolerance
following the control period represents a natural progression of the disease is not
known, since no studies have monitored glucose tolerance in CFRD over similar
time‐periods to the present study. Furthermore, future studies should seek to
assess the insulin response to an oral glucose load in association the blood glucose
response as assessed here, to allow for estimations of insulin secretion in response
to exercise training.
It is interesting to note that despite the acute lowering of blood glucose resulting
from each exercise session, there was no overall improvement in glycaemic control
as indicated by the HbA1c and CGMS results. Perhaps more regular exercise (i.e.
more than twice per week) may be required for these acute benefits to translate to
longer‐term glycaemic control. Alternatively, it may be that patients altered their
nutritional intake as a result of the exercise intervention. Nutritional intake was not
quantitatively monitored in the present study in order to ease the burden of what is

59
already a highly demanding disease management regime. Therefore, we cannot
exclude the possibility that patients ate more carbohydrates or high glycaemic index
foods throughout the exercise program. While this may be beneficial in maintaining
adequate body mass, adjustments in insulin therapy may be required if substantial
changes in diet result from regular exercise training. Finally, it must be
acknowledged that the limited sample size in the present study makes detecting
meaningful differences in glycaemic control difficult. Although the number of
individuals attending our clinic that were eligible to participate in this study was
limited to 20, we had hoped to recruit 10‐12 to the study. Despite our best efforts,
this was not achieved likely due to the fragile nature of the condition and
requirements of study participation, despite the potential benefits. Although the
change in HbA1c in response to exercise was non‐significant, it is worth noting that
three out of five participants experienced a decrease in HbA1c of > 1% following the
10 weeks of supervised exercise. Given this clinically meaningful reduction in some
participants, this may be a trend worth pursuing in future studies with a greater
number of study participants.
In summary, this study has shown that 10 weeks of supervised home‐based aerobic
and resistance exercise training resulted in improved cardiorespiratory fitness and
muscular strength, and tended to increase lean body mass. In contrast, exercise
training did not enhance lung function, quality of life, glucose tolerance or
glycaemic control; however, following the equivalent control period there was a
worsening of glucose tolerance to an oral glucose load, suggesting that exercise
may attenuate further declines in glucose tolerance. Although the current sample
60
size was low, it is important to note that the number of individuals with CFRD
attending our clinic that would be eligible to participate in the study was limited.
After excluding those with acute pulmonary exacerbations during the time of
recruitment, this number was further decreased. Future studies with a greater
sample size is needed to confirm if regular exercise is indeed beneficial for
improving glycaemic control in individuals with CFRD, this increase in participants
may be obtained from a multi‐sited study. On the other hand, a strength of the
present study was the supervised nature of the exercise intervention. Orenstein and
colleauges (2004) noted that the best results have been achieved in CF populations
with supervised programs, and as previously mentioned, home‐based exercise
training may be preferred to a centralised institution‐based training program to
allow for individualised supervision and to minimise the potential for transferring
infection between patients (Burdge et al., 1993; Ojeniyi et al., 2000). The present
study shows that 10 weeks of combined aerobic and resistance training in the home
of patients with CFRD is both feasible and warmly welcomed, based on the 100%
compliance rate. Considering the illness and requirements for participation, this is a
remarkable compliance rate. In order to minimise the logistical constraints of
increasing the frequency of exercise, future studies could examine the benefits of
scheduling additional unsupervised sessions throughout the week for patients with
CFRD. Increasing the frequency of exercise may be particularly important for those
with CFRD in terms of improving glycaemic control.
61
2.5 References
Alexander, S., Bridges, N. (2010). Cystic fibrosis related diabetes. Practical Diabetes
International; 27 (5): 198 – 200.
Bismuth, E., Laborde, K., Taupin, P., Velho, G., Ribault, V., Jennane, F., Grasset, E.,
Sermet, I., de Blic, J., Lenoir, G., Robert, J.J. (2008). Glucose tolerance and insulin
secretion, morbidity, and death in patients with cystic fibrosis. Journal of Pediatrics;
152; 540 – 545.
Bradley, J., Howard, J., Wallace, E., Elborn, S. (1999). Validity of a modified shuttle
test in adult cystic fibrosis. Thorax; 54: 437‐439.
Bradley, J., Howard, J., Wallace, E., Elborn, S. (2000). Reliability, repeatability, and
sensitivity of the modified shuttle test in adult cystic fibrosis. Chest; 117: 1666‐1671.
Brennan, A.L., Geddes, D.M., Gyi, K.M., Baker, E,H. (2004). Clinical importance of
cystic fibrosis‐related diabetes. Journal of Cystic Fibrosis; 3: 209 – 222.
Burdge, D.R., Nakielna, E.M., Noble, M.A. (1993). Case–control and vector studies of
nosocomial acquisition of Pseudomonas cepacia in adults patients with cystic
fibrosis. Chicago Journal; 128 (14): 127 – 130.
62
Cohen‐Cymberknoh, M., Shoseyov, D., Kerem, E. (2011). Managing cystic fibrosis:
Strategies that increase life expectancy and improve quality of life. American
Journal of Respiratory and Critical Care Medicine; 183: 1463 – 1471.
de Jong, W., Grevink, R.G., Roorda, R.J., Kaptein, A.A., van der Schans, C.P. (1994).
Effect of a home exercise training program in patients with cystic fibrosis. Chest;
105 (2): 463 ‐ 468.
Elborn, J.S., Shale, D.J., Britton, J.R. (1991). Cystic fibrosis: current survival and
population estimates to the year 2000. An International Journal of Respiratory
Medicine; 46: 881 ‐ 885.
Gilligan, P.H. (1991). Microbiology of airways disease in patients with cystic fibrosis.
Clinical Microbiology Reviews; 4: 35 – 51.
Gore, C.J., Michael, B,L., Adrian, B., Neville, O. (1999). Utility of PWC75% as an
estimate of aerobic power epidemiological and population‐based study. Journal of
Medicine and Science in Sports & Exercise; 31 (2): 348 – 351.
Hartling, S.G., Garne, S., Binder, C., Heilmann, C., Petersen, W., Petersen, K.E., Koch,
C. (1988). Proinsulin, insulin, and c‐peptide in cystic fibrosis after and oral glucose
tolerance test. Diabetes Research; 7: 165 – 169.
63
Horton, E.S. (1988). Role and management of exercise in diabetes mellitus.
Diabetes Care; 2 (11): 201 – 211.
Koch, C., Rainisio, M., Madessani, U., Harms, H.K., Hodson, M.E., Mastella, G.,
McKenzie, S.G., Navarro, J., Strandvik, B.; Investigators of the European
Epidemiologic Registry of Cystic Fibrosis. (2001). Presence of cystic fibrosis‐related
diabetes mellitus is tightly linked to poor lung function in patients with cystic
fibrosis: data from the European Epidemiologic Registry of cystic fibrosis. Pediatric
Pulmonology; 32(5): 343‐350.
Kristiansen, S., Gade, J., Wojtaszewski, J.F.P., Kiens, B., Ritcher, E.A. (2000). Glucose
uptake is increased in trained vs. untrained muscle during heavy exercise. Journal of
Applied Physiology; 89 (3): 1151 – 1158.
Mastrototaro, J.J. (2000). The miniMed Continuous Glucose Monitor System.
Diabetes Technology and Therapeutics; 2: (1) 13 – 18.
Miller, M.R., Hankinson, J., Brusasco, V., Burgos, F., Casaburi, R., Coates, A.,
Crapo, R., Enright, P., van der Grinten, C.P., Gustafsson, P., Jensen, R., Johnson,
D.C., Maclntyre, N., McKay, R., Navajas, D., Pederson, O.F., Pellegrino, R., Viegi G.,
Wanger, J. (2005). Standardisation of Spirometry. European Respiratory Journal; 26:
319 – 338.
64
Moorcroft, A.J., Dodd, M.E., Morris, J., Webb, A.K. (2004). Individualised
unsupervised exercise training in adults with cystic fibrosis: a 1 year randomized
controlled trial. International Journal of Respiratory Medicine; 59(12): 1074 – 1080.
Moran, A., Hardin, D., Rodman, D., Allen, H.F., Beall, R.J., Borowitz, D., Brunzell, C.,
Campbell III, P.W., Chesrown, S.E., Dunchow, C., Fink, R.J., Fitsimmons, S.C.,
Hamilton, N., Hirsch, I., Howenstone, M.S., Klein, D.J., Madhun, Z., Pencharz, P.B.,
Quittner, A.L., Robbins, M.K., Schindler, T., Schissel, K., Schwarzenberg, S.J.,
Stallings, V.A., Tullis, D.E., Zipt, W.B. (1999). Diagnosis, screening and management
of cystic fibrosis related diabetes, Diabetes Research and Clinical Practice; 45: 61 –
73.
Nixon, P.A., Orenstein, D.M., Kelsey, S.F., Doershuk, C.F. (1992). Prognostic value of
exercise testing in patients with cystic fibrosis. New England Journal of Medicine;
327: 1785 – 1788.
Ojeniyi, B., Frederiksen, B., Hoiby, N. (2000). Pseudomonas aeruginosa cross –
infection among patients with cystic fibrosis during a winter camp. Pediatric
Pulmonology; 29: 177 – 181
Orenstein, D.M., Franklin, B.A., Doershuk, C.F., Hellerstein, H.K., Germann, K.J.,
Horowitz, J.G., Stern, R.C. (1981). Exercise conditioning and cardiopulmonary fitness
in cystic fibrosis: the effects of a three‐month supervised running program. Chest;
80: 392 – 398.
65
Orenstein, D.M., Hovell , M.F., Mulvihill, M., Keating, K.K., Hofstetter, C.R., Kelsey,
S., Morris, K., Nixon, P.A. (2004). Strength vs aerobic training in children with cystic
fibrosis, Chest; 126 (4): 1204 – 1214.
O’Riordan, S.M.P., Robinson, P.D., Donaghue, K.C., Moran, A. (2008). Management
of cystic fibrosis‐related diabetes. Pediatric Diabetes; 9: 338 ‐ 344.
Quittner, A.L., Sawicki, G.S, McMullen, A., Rasouliyan, L., Pasta, D.J., Yegin, A.,
Konstan, M.W. (2011) Psychometric evaluation of the cystic fibrosis questionnaire‐
revised in a national sample. Quality of Life Research; Epub ahead of print.
Ratjen, F., Döring, G. (2003). Cystic fibrosis. The Lancet; 361: 681‐689.
Rochet, T., Slosman, D.O., Pichard, C., Belli, D.C. (1994).Body composition analysis
by dual‐energy X‐ray absorptiometry in adults with cystic fibrosis. Chest; 106 (3):
800 – 805.
Schneiderman‐Walker, J., Pollock, S.L., Corey, M., Wilkes, D.D., Canny, G.J., Pedder,
L.R., Reisman, J.J. (2000). A randomized controlled trial of a 3–year home exercise
program in cystic fibrosis. Journal of Paediatrics; 136(3): 304 ‐ 310.
66
Schwarzenberg, S.J., Thomas, W., Olsen, T.W., Grover, T., Walk, D., Milla, C., Moran,
A. (2007). Microvascular complications in cystic fibrosis‐ related diabetes. Diabetes
Care; 30 (5): 1056 – 1061.
Selvadurai, H.C., Blimkie, C.J., Meyers, N., Mellis, C.M., Cooper, P.J., Van Asperen,
P.P. (2002). Randomized controlled study of in–hospital exercise training program
in children with cystic fibrosis. Pediatric Pulmonology; 33(3): 194 – 200.
Sheppard, M.N., Nicholson, A.G. (2002). The pathology of cystic fibrosis. Current
Diagnostic Pathology; 8 (1): 50 – 59.
Simmonds, N.J., MacNeill, S.J., Cullinan, P., Hodson, M.E. (2010). Cystic fibrosis and
survival to 40 years: a case‐ control study. Journal of European Respiratory; 6: 1277
– 1283.
Strauss, G.D., Osher, A., Wang, C.I., Goodrich, E., Gold, F., Colman, W., Stabile, M.,
Dobrenchuk, A., Keens, T.G. (1987). Variable weight training in cystic fibrosis. Chest;
92: 273 – 276.
Wat, D., Doull, I. (2003). Respiratory virus infections in cystic fibrosis. Pediatric
Respiratory Reviews; 4: 172‐177.
67
Appendix A
Participant Information Sheet
68
PARTICIPANT INFORMATION SHEET
CYSTIC FIBROSIS RELATED DIABETES AND EXERCISE IMPACT OF A SUPERVISED EXERCISE TRAINING PROGRAM ON GLYCAEMIC CONTROL AND NUTRITIONAL STATUS IN ADULTS WITH CYSTIC FIBROSIS RELATED DIABETES
TRIAL NUMBER: 2010-042
Investigators: Jamie Wood, Senior CF Physiotherapist, Physiotherapy Department, SCGH Dr Joey Kaye, HOD, Endocrinology, SCGH Dr Siobhain Mulrennan, Consultant, Respiratory Medicine, SCGH Sue Morey, Nurse Practitioner, Respiratory Medicine, SCGH Dr Grant Landers, A. Professor, School of Sport Science, UWA Dr Kym Guelfi, A. Professor, School of Sport Science, UWA Sugumaran Muniandy, MSc student, UWA Please take time to read the following information carefully and discuss it with your friends, family and respiratory physician if you wish. Ask us any question if some part of the information is not clear to you or if you would like more information. Please do this before you sign this consent form. Who is funding this study? This study is to be internally funded by the department of Endocrinology, Sir Charles Gairdner Hospital Contact persons: Should you have questions about the study you may contact: Jamie Wood: Phone No. 08 9346 3333 Pager 4658 Dr Siobhain Mulrennan Phone No: 08 9346 3333 Dr Joey Kaye: Phone No. 08 9346 3333 All study participants will be provided with a copy of the Information Sheet and Consent Form for their personal records. You may decide to be in the study or not take part at all. If you do decide to take part in this study, you may stop at any time. However, before you decide, it is important that you understand why this research is being done and what it will involve. Whatever your decision, this decision will not lead to any penalty or affect your regular medical care or any benefit to which you are otherwise entitled. The following information sheet will explain the study and will include details such as:
o Why this trial might be suitable for you; o The possible risks (side-effects) and benefits of the new medicine;
69
o The type, frequency and risks of any medical tests or procedures required by the trial;
o The nature of your participation including how many visits you will make to the hospital
o Your rights and responsibilities o Alternative treatments available to you.
What is the purpose of the study? The purpose of this study is to evaluate the effects of a supervised, home-based exercise program on the blood sugar control, nutritional status and exercise capacity in patients with cystic fibrosis related diabetes. Why is this study suitable to me? You may be suitable for this study as you have previously been diagnosed with cystic fibrosis related diabetes. How long will I be in this study? You will be involved in the study for approximately 40 weeks. What will happen if I decide to be in this study? The study will be approximately 40 weeks in duration. During the first 2 weeks baseline assessments will be completed. These tests will be repeated at 3, 6 and 9 months (total of 4 times) during the study. These include:
A Blood test to assess blood glucose parameters Continuous glucose monitoring system (CGMS): This involves a small
device being implanted superficially under the skin on your abdomen. The device will remain for 72 hours and will provide a continuous readout of your blood sugar levels for that time period. During this 3 day period we would also like you to keep a diet diary, to ensure that when re-testing occurs you are able to reproduce a similar diet in this time period
DEXA (bone densitometry) scan to assess lean muscle mass Exercise capacity via a cycle ergometer test and a modified shuttle
test Quality of life survey
Each set of the tests listed above will require you to attend Sir Charles Gairdner Hospital on up to 3 separate days within a 2 week period. Each visit will take up to 3 hours of your time. You will then be randomly assigned into Group A or Group B. If you are in group A, you will complete a 3 month supervised exercise training program, followed by a 6 month period of your usual routine. If you are in Group B, you will continue your usual daily routine for 6 months, and then complete a 3 month supervised exercise training program. The 3 month exercise program consists of twice weekly supervised home based exercise sessions. Each session will be 60 minutes in duration. During these sessions the exercise performed will be upper and lower body toning and strength exercises with light weights, as well as cardiovascular exercise on a stationary bicycle. A trained exercise physiologist from the University of Western Australia will supervise your sessions to ensure your safety and that you get the maximum possible benefit from the exercise. All of the necessary
70
exercise equipment will be provided to you at no cost. Are there any reasons I should not be in this study? Study staff will discuss these with you in detail and will be directed at ensuring that this trial is both safe and appropriate for you. Criteria which will exclude you from the study are as follows:
- Resting or exercise induced hypoxaemia (low oxygen levels) requiring oxygen therapy
- Significant musculoskeletal disease preventing exercise - If you are listed for lung transplantation - If you are receiving steroid therapy for any condition - Pregnancy
What are the costs to me? There are no costs to subjects in this trial. Tests required to be performed can be planned to coincide with your routine outpatient clinic appointments. What are the possible benefits of taking part? By taking part and completing the 3 month exercise program, you will potentially see improvements in your exercise capacity, strength, lean muscle mass and weight. You may also experience an improvement in your perceived quality of life. The purpose of this study is to evaluate whether these improvements will also lead to an improvement in your blood sugar control. How will my safety be ensured? During the exercise sessions you will be closely monitored by a qualified exercise professional. Your blood sugar levels will be checked before exercise commences, and your oxygen levels will be monitored during and after you finish exercising. An oxygen cylinder will be available for use if your oxygen levels become abnormally low during exercise. All exercise performed will be individualised to your needs, and you will be shown how to stretch appropriately to prevent any soft tissue injuries. Do not hesitate at any time to contact the cystic fibrosis team at SCGH, on (08) 9346 3333, if you have any concerns regarding your health during this study. What alternatives do I have to going on this study? If you do not wish to take part in this study, you will still be offered advice regarding exercise from your physiotherapist, during your routine outpatient clinic appointments. The cystic fibrosis and endocrinology consultants will continue to monitor your diabetes appropriately if you decide not to take part in this study. What are the possible side effects, risks and discomforts of taking part? As with any exercise program, soft tissue injury is a potential risk. During your exercise sessions you will be supervised by a qualified exercise professional, who will show you how to stretch appropriately before your
71
workout, and tailor your exercise program to suit your individual requirements. You may be at risk of having an episode of hypoglycaemia, or low blood sugar levels, following exercise. To minimise this risk, your exercise trainer will assess your blood sugar levels with a capillary (or finger prick) test prior to exercise. If your blood sugars are low before your session, you may be required to eat before you commence to ensure your blood sugar level is maintained at an appropriate level. Another risk involved during exercise is low blood oxygen levels, or hypoxaemia. To be included in this study, you must be able to exercise without the use of oxygen. However patients with cystic fibrosis are more likely to have lower blood oxygen levels while exercising, especially if you have an exacerbation of your symptoms. As a precaution, your blood oxygen levels will be monitored during and after you have finished exercising, with a finger probe oximeter. An oxygen cylinder will be available to use if you experience an episode of low blood oxygen levels. You will be required to have 4 blood tests during the study, which may cause slight discomfort. You will also be required to have your blood sugars checked before exercise sessions via capillary or ‘finger prick’ with a blood sugar level monitor. This may cause a small amount of pain in your finger when performed. A continuous glucose monitoring system (CGMS) is a device inserted under the skin on your abdomen for three days, providing a constant reading of your blood sugars. It is inserted by Sue Morey (Respiratory Medicine Nurse Practitioner), and may cause a small amount of pain or discomfort while inserted. CGMS is commonly used amongst patients at SCGH with CF related diabetes, and you may have had this performed in the past. You will have the CGMS 4 times during this study. There is an extremely small risk of infection from the insertion of the CGMS. A DEXA scan assesses your body composition, providing information regarding what percentage of your body is muscle and fat. You will require 4 scans during this study. It involves lying down on your back for up to 30 minutes on the scanner. You are not required to be put ‘into’ a scanner, such as during an MRI, therefore you should not experience any issues if you suffer from claustrophobia. Stopping study treatment early: If for any reason this study needs to be stopped early, you will be notified immediately by the study investigators. The reasons for stopping will be explained to you, and you will continue with your usual medical management by the cystic fibrosis and endocrinology teams. What happens at the end of the study? At the end of the study, you will continue to be provided with your usual care by the cystic fibrosis and endocrinology teams. Exercise equipment will be returned to the investigators for use with other patients. You will not continue

72
to be provided with supervision for exercise after you have completed the study, but will still be offered ongoing advice from the cystic fibrosis physiotherapist at your usual outpatient clinic appointments. What if something goes wrong? You will receive the best medical care available during and after the trial. In the unlikely event of your being harmed from taking part in this trial, you will be provided with the necessary care. Medical treatment will be provided at no cost to you for research-related harm. The term “research-related harm” means both physical and mental injury caused by the product or procedures required by the trial. Will my taking part in this study be kept confidential? The researchers will need to collect personal data about you, which may be sensitive, eg. Date of birth and relevant health information. The researchers may also need to get some of your health information from other health service providers, eg pathology laboratory, endocrinology and respiratory medicine. Any personal or health information will be kept private and confidential. It will be stored securely and only authorised persons, who understand it must be kept confidential, will have access to it. Your study details will be given a number so that your identity will not be apparent. The trial records will be kept in the Department of Respiratory Medicine at SCGH during the study and in a locked archive indefinitely.
The result of the research will be made available to other professionals through medical journals or meetings, but you will not be identifiable in these communications. By taking part in this study you agree not to restrict the use of any data even if you withdraw. Your rights under any applicable data protection laws are not affected. Will I find out the results of the study? The results of this study are intended for publication in relevant journals, and for presentation at relevant scientific meetings. The results will also made available to subjects at your request after the study is completed. Please be aware that no identifiable data will be made available at any time, to protect the identity of participants in the study. Who has reviewed the study? The Sir Charles Gairdner Group Human Research Ethics Committee has reviewed this study and has given its approval for the conduct of this research trial. In doing so this study conforms to the principles set out by the National Statement on Ethical Conduct in Human Research and according tothe Good Clinical Practice Guidelines. In the case of a medical emergency please present to the Emergency Department
at Sir Charles Gairdner Hospital for assessment

73
Appendix B Participant Consent Form
74
CONSENT FORM IMPACT OF A SUPERVISED EXERCISE TRAINING PROGRAM ON GLYCAEMIC CONTROL AND NUTRITIONAL STATUS IN ADULTS WITH CYSTIC FIBROSIS RELATED DIABETES Investigators: Jamie Wood, Senior CF Physiotherapist, Physiotherapy Department, SCGH Dr Joey Kaye, HOD, Endocrinology, SCGH Dr Siobhain Mulrennan, Consultant, Respiratory Medicine, SCGH Sue Morey, Nurse Practitioner, Respiratory Medicine, SCGH Dr Grant Landers, A. Professor, School of Sport Science, UWA Dr Kym Guelfi, A. Professor, School of Sport Science, UWA Sugumaran Muniandy, Msc student, UWA Subject Name: ___________________________ DOB: ______________ 1. I have been given clear information (verbal and written) about this study
and have been given time to consider whether I want to take part. 2. I have been told about the possible advantages and risks of taking part in
the study and I understand what I am being asked to do. 3. I have been able to have a member of my family or a friend with me while I
was told about the study. I have been able to ask questions and all questions have been answered satisfactorily.
4. I know that I do not have to take part in the study and that I can withdraw
at any time during the study without affecting my future medical care. My participation in the study does not affect any right to compensation, which I may have under statute or common law.
5. I agree to take part in this research study and for the data obtained to be
published provided my name or other identifying information is not used. If you are unclear about anything you have read in the Participant Information Sheet or this Consent Form, please speak to your doctor before signing this Consent Form. Name of Participant Signature of Participant Date Name of Investigator Signature of Investigator Date
75
Appendix C Ethical Approval
76

77
Appendix D Cystic Fibrosis Questionnaire ‐ Revised
78

79
80
81





























