Embed Size (px)
Citation preview

The Effect of a Single Episode of Short DurationHeart Rate Variability Biofeedback on Measuresof Anxiety and Relaxation States
Gabriell E. Prinsloo, Wayne E. Derman, Michael I. Lambert,and H. G. Laurie RauchUniversity of Cape Town
This study examines the acute effect of heart rate variability (HRV) biofeed-back on anxiety and relaxation states. Eighteen healthy males exposed towork-related stress were randomized into an HRV biofeedback group (BIO)or comparative group (COM). The device used by the COM group appearedidentical to the HRV biofeedback device, however, it did not provide bio-feedback, rather it displayed a wave which the subjects were instructed toobserve. Subjects completed a modified Stroop task before and after a 10-minintervention. The Spielberger Trait Anxiety Inventory (STAIT) was completedat recruitment, and the Spielberger State Anxiety Inventory (STAIS) andSmith Relaxation States Inventory 3 (SRSI3) were completed before and aftertesting. Subjects rated perceived efficacy and feelings of sleepiness using avisual analogue scale (VAS). Analysis of the VAS scores revealed that theCOM group felt sleepier than the BIO group after using the intervention.After testing, HRV biofeedback resulted in large improvements in scores formindfulness, energized positive feelings and basic relaxation, and the com-parative intervention resulted in a moderate improvement in basic relax-ation, small improvement in mindfulness, and no improvement in energizedpositive feelings. Both groups had moderate improvements in transcendence.There was a large decrease in state anxiety in the BIO group and moderatedecrease in the COM group. These findings suggest that although there wasbenefit to both interventions, a single episode of short duration HRV bio-feedback led to greater benefit and may be a valuable tool to include in the
Gabriell E. Prinsloo, Wayne E. Derman, Michael I. Lambert, and H. G. Laurie Rauch,MRC/UCT Research Unit for Exercise Science and Sports Medicine, University of Cape Town,Cape Town, South Africa.
We thank Helicor for providing funding for this study. We receive no remuneration formerchandise sold and therefore have no vested interest in the outcome of the study.
Correspondence concerning this article should be addressed to Gabriell E. Prinsloo,MRC/UCT Research Unit for Exercise Science and Sports Medicine, Department of HumanBiology, Faculty of Health Sciences, University of Cape Town, P.O. Box 115, Newlands, 7725,Cape Town, South Africa. E-mail: [email protected]
International Journal of Stress Management © 2013 American Psychological Association2013, Vol. 20, No. 4, 391–411 1072-5245/13/$12.00 DOI: 10.1037/a0034777
391
management of acute stress and anxiety.
Keywords: heart rate variability biofeedback, relaxation states, anxiety
Acute and chronic psychological stress is increasing in prevalence in theworld today. Acute stress leads to increased anxiety (American PsychologicalAssociation, 2012; National Institute of Mental Health, 2012), and chronicand extreme stress can lead to impaired cognitive performance (Orem, Petrac,& Bedwell, 2008; Sauro, Jorgensen, & Pedlow, 2003) as well as increasedrisk of chronic disease (Brotman, Golden, & Wittstein, 2007; Chandola,Brunner, & Marmot, 2006; Esch, Stefano, Fricchione, & Benson, 2002). Asa result of the high burden of stress and stress-related disease, it is increas-ingly important to identify effective stress management techniques. Interven-tions that are commonly used to reduce stress and anxiety include techniquessuch as progressive muscle relaxation (Lehrer, Woolfolk & Sime, 2007;Smith, 2005a), listening to relaxing and classical music (Burns et al., 2002;Labbe, Schmidt, Babin, & Pharr, 2007), cognitive–behavioral interventions(Richardson & Rothstein, 2008), and meditation (Krisanaprakornkit, Kri-sanaprakornkit, Piyavhatkul, & Laopaiboon, 2006; Williams, Kolar, Reger,& Pearson, 2001).
Heart rate variability (HRV) biofeedback is another intervention whichhas recently shown promise in the management of stress and anxiety (Sherlin,Gevirtz, Wyckoff, & Muench, 2009; Nolan et al., 2005) as well as beingbeneficial in the management of numerous diseases, both mental and physical(Hassett et al., 2007; Karavidas et al., 2007; Lehrer et al., 2004). HRVbiofeedback is similar to a concentrative meditation in that it is focused on aspecific sensory activity (Cahn & Polich, 2006). However, in addition toobserving the breath, one is actively controlling it in response to an externalbiofeedback stimulus.
The HRV biofeedback device measures heart rate and displays a wavewhich reflects respiratory sinus arrhythmia (RSA). This is the cyclical changein heart rate occurring in response to respiration. Using the RSA wave, usersare guided to breathe at resonance frequency (Muench, 2008), and to main-tain a cognitive focus so that real-time heart rate and respiration covaries ina perfect phase relationship. It is thought that breathing at the resonancefrequency “exercises” the baroreflex (Lehrer et al., 2003) resulting in im-proved autonomic function (Lehrer et al., 2003; Vaschillo, Vaschillo, &Lehrer, 2006).
Most relaxation techniques result in a nonspecific relaxation character-ized by decreased sympathetic arousal (Benson, 1975) and lead to a reductionof stress and anxiety (Eppley, Abrams, & Shear, 1989; Esch, Fricchione, &Stefano, 2003; Manzoni, Pagnini, Castelnuovo, & Molinari, 2008). However,different techniques may produce different specific effects (Lehrer et al.,
392 Prinsloo, Derman, Lambert, and Rauch
1983; Smith, 2004). Davidson has differentiated cognitive from somaticrelaxation effects (Davidson & Schwartz, 1976), although Smith (Smith,2005a; Smith, 2007) has identified four different categories of relaxationincluding mindfulness, energized positive feelings, basic relaxation, andtranscendence.
Mindfulness is a quality of attention rather than a technique (Chambers,Chuen Yee Lo, & Allen, 2008) and is characterized by a combination ofcomplete awareness of internal and external stimuli together with nonjudge-ment (Baer, 2003; Bishop et al., 2004; Kabat-Zinn, 2003). It has been shownto increase as a result of meditation (Brown & Ryan, 2003; Chambers et al.,2008; Carmody & Baer, 2008) as well as in response to HRV biofeedback incombination with mindfulness training (Kleen & Reitsma, 2011). Mindful-ness is associated with decreased anxiety (Chambers et al., 2008), increasedwell-being (Brown & Ryan, 2003) and EEG changes suggestive of increasedpositive emotions (Chan, Han, & Cheung, 2008).
The category of energized positive feelings includes the subcategories offeeling energized as well as positive emotions or states of mind includinghappiness, hope, optimism, love, and thankfulness. Although no studies haveexamined the effect of HRV biofeedback on any of these emotions or states,other relaxation techniques have been associated with increased feelings ofhappiness (Davidson et al., 2003) and joy (Matsumoto & Smith, 2001).Positive emotions lead to increased emotional well-being (Fredrickson &Joiner, 2002) and reduced anxiety (Fredrickson, 2000), and improve theability to manage stress (Aspinwall, 1998) and stress-related health problems(Fredrickson, 2000).
The category of basic relaxation reflects the nonspecific relaxation seenin response to most relaxation techniques (Benson, 1975) and consists of bothphysical and mental relaxation. No other studies have examined the effects ofHRV biofeedback on feelings of relaxation. The final category of transcen-dence includes the feelings of awe and wonder, prayerfulness, deep mystery,and timelessness. Transcendence is defined as the state of being “aware ofsomething larger or greater than oneself” (Smith, 2005a) as well as the abilityto move beyond “self-centered consciousness” taking on a broader, clearerperspective (Ellermann & Reed, 2001; Levenson & Crumpler, 1996). Tran-scendence has been positively associated with emotional well-being (Cow-ard, 1996). The practice of Zen meditation has been associated with increasedprayerfulness (Gillani & Smith, 2001), however, no studies have investigatedthe effect of HRV biofeedback on forms of transcendence.
Based on this existing literature, we hypothesize that the use of HRVbiofeedback will lead to decreased anxiety, increased basic relaxation, withpossible increases in mindfulness. As men and women have different phys-iological and psychological responses to stress (Kudielka & Kirschbaum,2005; Wang et al., 2007), we have elected to test only men to limit hetero-
393HRV Biofeedback Affects Anxiety and Relaxation
geneity. Therefore, the aim of this study was to determine the effects of asingle episode of short duration heart rate variability biofeedback on differentrelaxation states and anxiety in men who experience psychosocial stress.
METHOD
Participants
Eighteen male volunteers (34 � 6 years) who were employed in seniormanagerial positions were recruited for this study. To be included volunteershad to have been exposed to work-related stress and subjectively rate theirown perception of life stress as high. Their trait anxiety was measured usingthe trait component of a Spielberger State–Trait Anxiety Inventory (STAIT;Spielberger, 1983) which they completed online.
A previous clinical diagnosis of anxiety-related disorders disqualifiedparticipation in the study. Further exclusion criteria included: previouslydiagnosed cardiac or psychiatric disorders, current use of psychotropic orheart rate altering medications or current use of stimulants or recreationaldrugs, as well as volunteers practicing regular meditation techniques. Vol-unteers were asked about their exercise practices as well as breathing andmeditation techniques as these would have had the greatest impact on theoutcome of the intervention. Volunteers who were technically unable to usethe biofeedback device or perform the modified Stroop task were excludedfrom the trial. This applied to two subjects, one of whom had chronic lowcirculation and so the device was unable to obtain a clear pulse reading. Theother subject was excluded as on completion of the familiarization Strooptask he still did not understand what to do and continued to confuse theresponse keys and, therefore, could not respond effectively.
Subjects were screened via e-mail. On arrival before the training sessiona brief history was taken by a medical doctor, to confirm the responses.Volunteers were instructed not to eat a heavy meal, ingest caffeine or alcohol,or exercise within 4 hr before arriving at the laboratory. Compliance waschecked before the onset of each testing session.
Subjects were then randomly assigned to either an HRV biofeedback(BIO) group or a comparative (COM) group using a process of stratifiedrandomization. Each group consisted of nine subjects. The initial group ofsubjects was matched into two groups based on age and thereafter subjectswere randomly assigned to either group. We decided to use a single inter-vention and comparative group design, as a crossover design may haveconfounded the interpretation in the event of there being any carry over fromthe intervention.
394 Prinsloo, Derman, Lambert, and Rauch

The study protocol was approved by the Research and Ethics Committeeof the University of Cape Town (Rec ref: 296/2005) in accordance with theDeclaration of Helsinki. All subjects signed informed consent prior to par-ticipation in the study.
Instruments
Validated questionnaires were used to assess anxiety and relaxationstates as this has been shown to increase the reliability of self-reported data(Hardt & Rutter, 2004). State anxiety was assessed using the state componentof the Spielberger State–Trait Anxiety Inventory (STAIS) and trait anxietyusing the trait component (STAIT; Spielberger, 1983). Each componentconsists of 20 self-report items measured using a 4-point Likert scale rangingfrom 1 (not at all) to 4 (very much so). This yields a total score which rangesfrom 20 to 80 points. The STAIT/S is a commonly used measure of anxiety(Walker, 1990) which shows good internal consistency and test–retest reli-ability across populations (Barnes, Harp, & Sik Jung, 2002).
Relaxation states were measured using the Smith Relaxation StatesInventory 3 (SRSI3; Smith, 2005b). This consists of 38 self-report itemsmeasured using a 6-point Likert scale ranging from 1 (not at all) to 6(maximum), which are combined into 19 relaxation states each with amaximum score of 6. The 19 relaxation states are divided into four categoriesloosely based on factor analytic research (Smith et al., 2000). The categoriesconsist of mindfulness, energized positive feelings, basic relaxation, andtranscendence. Reliability for the SRSI3 has yet to be determined, but theprevious version of the Smith Relaxation States Inventory (excluding thethree new sub categories of mindful acceptance, mindful centering, andmindful awakening) has been shown to be reliable (Smith, 2005a).
In addition, subjects were asked to rate the subjective efficacy of theintervention as well as feelings of sleepiness using a visual analogue scale(VAS) devised for this study. In response to each question, subjects scoredfrom 1 to 10 with 1 being not at all and 10 being extremely with regard tohelpfulness and sleepiness.
Procedure
Training and Familiarization Protocol
All subjects underwent a single standardized training session during theweek prior to the start of their experimental trials. A hand-held mobile heart
395HRV Biofeedback Affects Anxiety and Relaxation
rate variability biofeedback device (StressEraser™, Helicor, U.S.A.) vali-dated by Heilman, Handelman, Lewis, and Porges, 2008 was used for boththe training and the testing sessions in the BIO group. The device measuresthe real-time interbeat-interval (IBI) of the heart using finger photoplethys-mography (Muench, 2008). The IBI data are transformed and displayed as awave on a LCD screen, allowing users to see the real-time fluctuations oftheir pulse rates. This wave reflects respiratory sinus arrhythmia (RSA),which is the cyclical change in heart rate occurring in response to respiration.Using the RSA wave, users are guided to breathe at resonance frequency(Muench, 2008), and to maintain a cognitive focus so that real-time heart rateand respiration covaries in a perfect phase relationship. To achieve this, thesubjects were instructed to inhale until the RSA wave reached its peak andexhale until the wave started to rise again. The device rewards users withpoints based on the wavelength for each RSA cycle. If the wavelength meetsa certain threshold (10 s), users are given one point marked by three verticalsquares. Two vertical squares receive .5 point and one vertical squarereceives no credit. The goal is to accumulate continuous points during thesession. To assist users in obtaining points, the device anticipates the peak ofthe RSA wave based on its slope and marks the peak with a triangle. Thepeak of the wave indicates the moment heart rate deceleration is to begin,indicating the parasympathetic response. Users are instructed to begin theirexhale when the triangle appears. They are instructed to extend their exhalefor as long as possible until the wave begins to rise again. Although thedevice offers points based on RSA wavelength, users were instructed tomaximize RSA amplitude simply by following the RSA wave (e.g., inhaleuntil the wave stopped rising and exhale until the wave stops falling).
This is not technically resonance frequency breathing as time domainanalysis was used rather than frequency analysis; however, it does function-ally facilitate a similar breathing frequency. As the average respiratoryfrequency of the BIO group during the intervention was 0.10 � 0.01 Hz, andthat of the COM group was 0.25 � 0.05 Hz, it can be suggested that the BIOgroup were functionally achieving resonance frequency. The respiratory rateat which resonance frequency occurs ranges from 4.5 to 6.5 breaths/min(Vaschillo et al., 2006). Breathing at this frequency results in large increases inHRV and baroreflex gain (Lehrer et al., 2003) as well as optimizing respiratoryefficiency (Giardino, Chan, & Borson, 2004; Muench, 2008). In addition to theR-R wave, a cumulative score on the display screen enabled participants tomonitor the impact of their breathing on their HRV. Subjects were taughtpursed-lips abdominal breathing and were instructed to relax and breathe com-fortably without straining (Lehrer, Vaschillo, & Vaschillo, 2000).
The device used in the COM group was also manufactured by Helicor.It appeared identical to the BIO device but made use of a different algorithmto display a wave on the screen. The algorithm that generated this wave was
396 Prinsloo, Derman, Lambert, and Rauch

derived from the subject’s heart rate measured by the sensor, divided by 2plus a random number which ranged between 0% and 25% of the heart rate/2value. This result was then smoothed by averaging the calculation over 5 s.Subjects were informed that the wave represented their blood density andwere instructed to watch the wave while not thinking any stressful thoughts,and were not instructed to alter their breathing in any way. After both groupsof subjects had received their respective instructions, they completed aformal 10-min biofeedback session with either the BIO or COM device andtheir scores were recorded. A score of 30 or more on the BIO device wasindicative of a successful session.
Experimental Trial
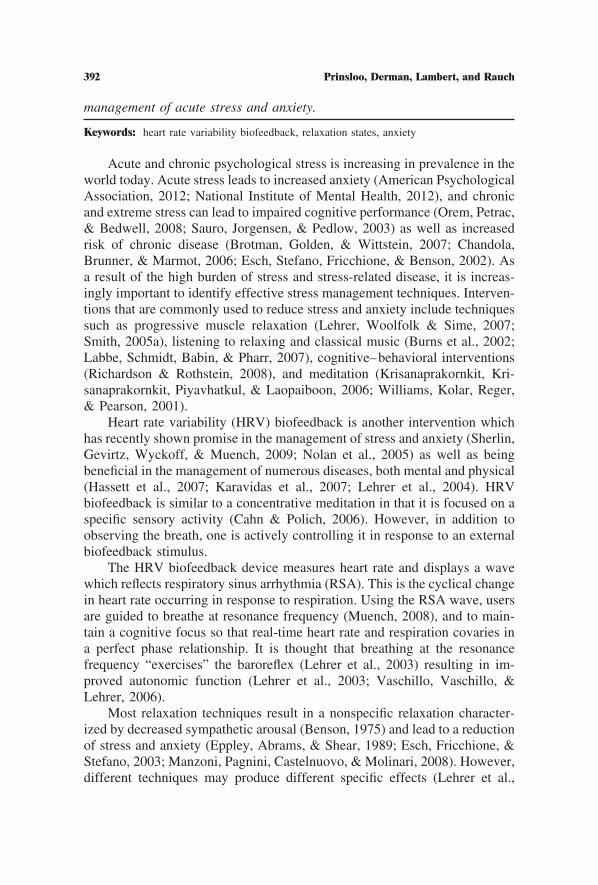
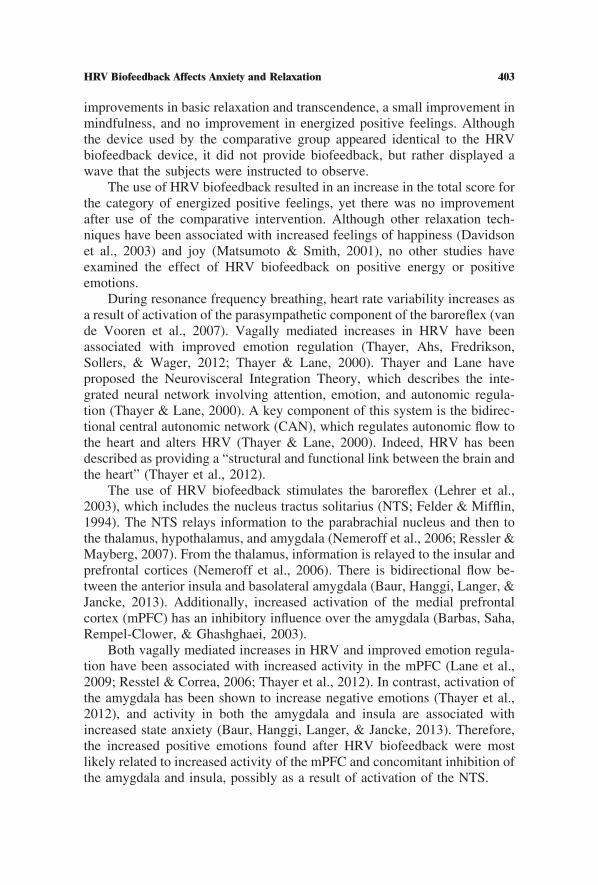
The time line for the experimental trial is shown in Figure 1. On arrivalat the laboratory, subjects completed the state component of a SpielbergerState–Trait Anxiety Inventory (STAIS; Spielberger, 1983) and the SmithRelaxation States Inventory 3 (SRSI3; Smith, 2010) and were reminded howto use their respective devices. Subjects then underwent a full familiarizationmodified Stroop task lasting 5 min and 24 s. After the familiarization test,electrodes and transducers were applied to the subjects and connected to aBiopac MP150WSW (Biopac Systems, Goleta, CA) to record electrocardio-gram (ECG), respiratory rate and electroencephalogram (EEG). The detaileddescription of the measurement and analysis of HRV, respiratory and EEGdata have been reported in previously published article (Prinsloo, Derman,Lambert & Rauch, 2013; Prinsloo, Rauch, Karpul & Derman, 2013).
Subjects were then instructed to relax with their eyes closed for 5 min(Rest 1). Immediately after the baseline period and without moving, subjects
PREP
START R1 S1 INTERVENTION R2 S2 FINISH
Ques�onnaires completed
Compara�ve interven�on
Modified Stroop task
Prepara�on
Rest period
HRV Biofeedback Interven�on PREP
Figure 1. Diagram depicting the time line of the protocol during the experimental trial. HRV �heart rate variability; R1 � First rest period; S1 � First Stroop task; R2 � Second rest period;S2 � Second Stroop task.
397HRV Biofeedback Affects Anxiety and Relaxation
were instructed to open their eyes and complete the preintervention Strooptask (Stroop 1) which lasted 5 min 24 s in duration. Subjects then completeda 10-min intervention with either the BIO or COM device. After the inter-vention, subjects completed a further 5-min rest period (Rest 2) with theireyes closed before completing a postintervention Stroop task (Stroop 2).After the final measurements, subjects completed posttesting STAIS andSRSI3 questionnaires, as well as the VAS.
Modified Stroop Task
We modified the original Stroop color-word task (Stroop, 1935) so thatsubjects responded by pressing keypad buttons instead of responding ver-bally. The color word component was previously validated by Rauch, John,St. Clair Gibson, Noakes, and Vaughan (2005). In addition, we added aworking memory component which required the subjects to count the cumu-lative total number of white squares that appeared throughout the test andreport the total number at the end of each Stroop. This value was comparedbetween Stroop 1 and 2. They were not told how many squares there were inthe test, only that they were randomly generated.
In total 108 cues were randomly presented, 18 incongruent colorwords in each of the four colors red, blue, green, and yellow (72incongruent words in total); 18 gray words; and 18 white squares. The useof the gray words ensured that subjects had to read and recognize thecolor words rather than just noticing the colors, thereby invoking theStroop effect (Stroop, 1935). The subjects were asked to respond as quicklyand as accurately as possible by pressing one of four response buttons toindicate either the color of the word (if the word was written in color ink), orthe word itself (if the word was written in gray ink).
The Stroop test is an effective means of inducing cognitive stress in thelaboratory (Renaud & Blondin, 1997). It provided a complex cognitivechallenge which included three elements of executive functioning: updatingof working memory, mental set shifting and inhibition of prepotent responses(Miyake et al., 2000). Counting squares tests the updating of workingmemory and responding to the color words tests inhibition of prepotentresponses together with the delicate balancing of the speed–accuracy trade-off (Forstmann et al., 2008).
RESULTS
A comparison of subject characteristics, STAIT and VAS scores betweengroups were analyzed using an independent t-test. Differences in STAIS and
398 Prinsloo, Derman, Lambert, and Rauch
SRSI3 scores between groups were analyzed using repeated measures anal-ysis of variance (ANOVA). Specifically, differences in the main effects(group and time) and the interaction of Group � time were determined. ATukey’s post hoc test was used to determine specific differences in the eventof there being a significant interaction effect.
Cohen’s d effect sizes (Cohen, 1988) were calculated on the STAIS andscores for the four major SRSI3 categories. Effect sizes were calculated foreach group using the formula d � posttest mean � pretest mean/(combinedstandard deviation of all pre- and posttest values). We regarded an effect sizeof 0.2–0.5 as having a small effect, 0.5–0.8 as having a moderate effect, and0.8 or greater as having a large effect (Cohen, 1988). Effect sizes of 0.5 orgreater were regarded as meaningful. All parametric data are described asmean � standard deviation (SD). A p value of � 0.05 was considered to bestatistically significant.
The BIO and COM groups were similar in age (33 � 6 vs. 34 � 6 years,respectively), body mass index (28.7 � 6.8 vs. 27.2 � 4.5 kg/m2, respec-tively) and adherence to exercise training (3 � 1 vs. 3 � 1 units, respectively)measured on a scale of 1 to 5 (1 � less than once a month, 5 � every day).
During the training session scores for the BIO intervention were 41 � 7points, with eight of the nine subjects having a score above 30 and a lowestscore of 29. During testing the scores were 46 � 5 points with all scoresabove 30 and a lowest score of 38.
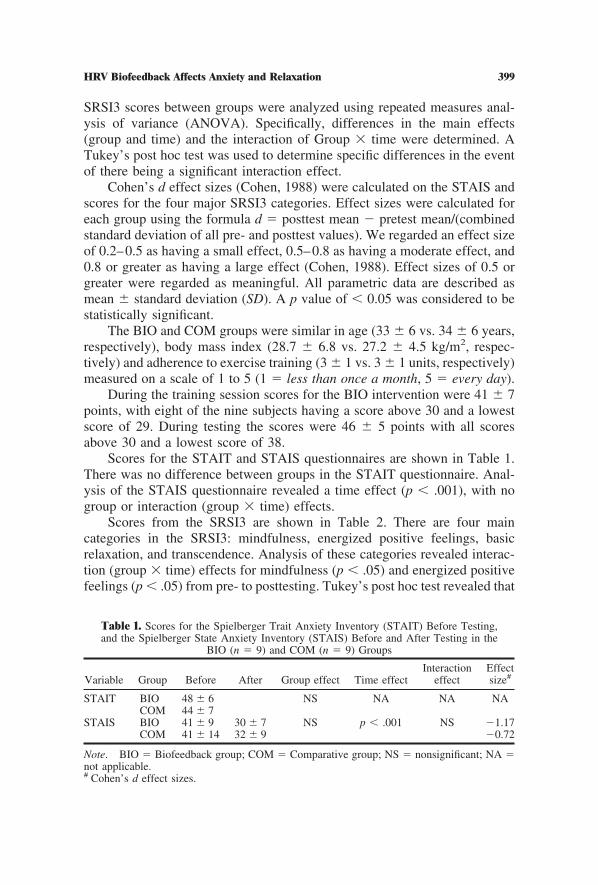
Scores for the STAIT and STAIS questionnaires are shown in Table 1.There was no difference between groups in the STAIT questionnaire. Anal-ysis of the STAIS questionnaire revealed a time effect (p � .001), with nogroup or interaction (group � time) effects.
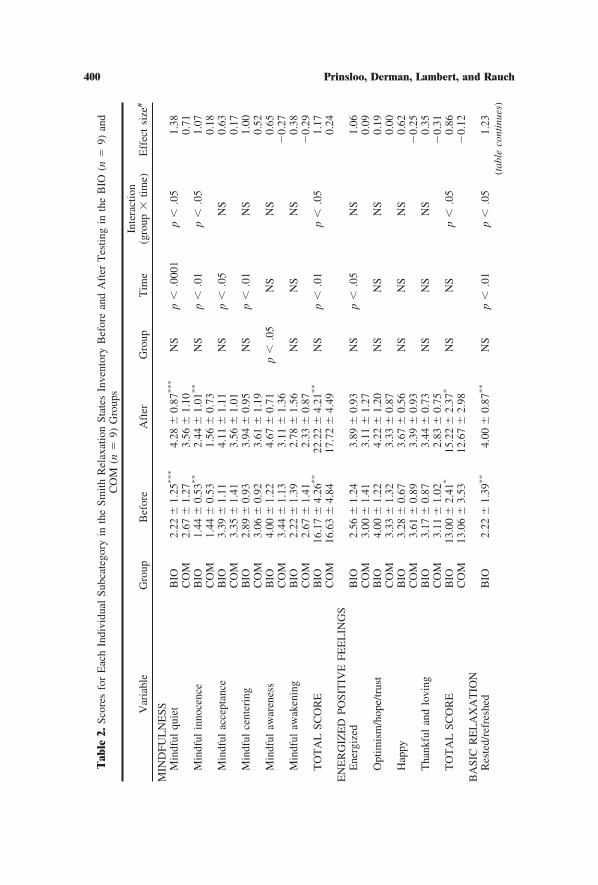
Scores from the SRSI3 are shown in Table 2. There are four maincategories in the SRSI3: mindfulness, energized positive feelings, basicrelaxation, and transcendence. Analysis of these categories revealed interac-tion (group � time) effects for mindfulness (p � .05) and energized positivefeelings (p � .05) from pre- to posttesting. Tukey’s post hoc test revealed that
Table 1. Scores for the Spielberger Trait Anxiety Inventory (STAIT) Before Testing,and the Spielberger State Anxiety Inventory (STAIS) Before and After Testing in the
BIO (n � 9) and COM (n � 9) Groups
Variable Group Before After Group effect Time effectInteraction
effectEffectsize#
STAIT BIO 48 � 6 NS NA NA NACOM 44 � 7
STAIS BIO 41 � 9 30 � 7 NS p � .001 NS �1.17COM 41 � 14 32 � 9 �0.72
Note. BIO � Biofeedback group; COM � Comparative group; NS � nonsignificant; NA �not applicable.# Cohen’s d effect sizes.
399HRV Biofeedback Affects Anxiety and Relaxation
Tab
le2.
Scor
esfo
rE
ach
Indi
vidu
alSu
bcat
egor
yin
the
Smith
Rel
axat
ion
Stat
esIn
vent
ory
Bef
ore
and
Aft
erT
estin
gin
the
BIO
(n�
9)an
dC
OM
(n�
9)G
roup
s
Var
iabl
eG
roup
Bef
ore
Aft
erG
roup
Tim
eIn
tera
ctio
n(g
roup
�tim
e)E
ffec
tsi
ze#
MIN
DFU
LN
ESS
Min
dful
quie
tB
IO2.
22�
1.25
***
4.28
�0.
87***
NS
p�
.000
1p
�.0
51.
38C
OM
2.67
�1.
273.
56�
1.10
0.71
Min
dful
inno
cenc
eB
IO1.
44�
0.53
**
2.44
�1.
01**
NS
p�
.01
p�
.05
1.07
CO
M1.
44�
0.53
1.56
�0.
730.
18M
indf
ulac
cept
ance
BIO
3.39
�1.
114.
11�
1.11
NS
p�
.05
NS
0.63
CO
M3.
35�
1.41
3.56
�1.
010.
17M
indf
ulce
nter
ing
BIO
2.89
�0.
933.
94�
0.95
NS
p�
.01
NS
1.00
CO
M3.
06�
0.92
3.61
�1.
190.
52M
indf
ulaw
aren
ess
BIO
4.00
�1.
224.
67�
0.71
p�
.05
NS
NS
0.65
CO
M3.
44�
1.13
3.11
�1.
36�
0.27
Min
dful
awak
enin
gB
IO2.
22�
1.39
2.78
�1.
56N
SN
SN
S0.
38C
OM
2.67
�1.
412.
33�
0.87
�0.
29T
OT
AL
SCO
RE
BIO
16.1
7�
4.26
**
22.2
2�
4.21
**
NS
p�
.01
p�
.05
1.17
CO
M16
.63
�4.
8417
.72
�4.
490.
24E
NE
RG
IZE
DPO
SIT
IVE
FEE
LIN
GS
Ene
rgiz
edB
IO2.
56�
1.24
3.89
�0.
93N
Sp
�.0
5N
S1.
06C
OM
3.00
�1.
413.
11�
1.27
0.09
Opt
imis
m/h
ope/
trus
tB
IO4.
00�
1.22
4.22
�1.
20N
SN
SN
S0.
19C
OM
3.33
�1.
323.
33�
0.87
0.00
Hap
pyB
IO3.
28�
0.67
3.67
�0.
56N
SN
SN
S0.
62C
OM
3.61
�0.
893.
39�
0.93
�0.
25T
hank
ful
and
lovi
ngB
IO3.
17�
0.87
3.44
�0.
73N
SN
SN
S0.
35C
OM
3.11
�1.
022.
83�
0.75
�0.
31T
OT
AL
SCO
RE
BIO
13.0
0�
2.41
*15
.22
�2.
37*
NS
NS
p�
.05
0.86
CO
M13
.06
�3.
5312
.67
�2.
98�
0.12
BA
SIC
RE
LA
XA
TIO
NR
este
d/re
fres
hed
BIO
2.22
�1.
39**
4.00
�0.
87**
NS
p�
.01
p�
.05
1.23
(tab
leco
ntin
ues)
400 Prinsloo, Derman, Lambert, and Rauch
Tab
le2.
(con
tinu
ed)
Var
iabl
eG
roup
Bef
ore
Aft
erG
roup
Tim
eIn
tera
ctio
n(g
roup
�tim
e)E
ffec
tsi
ze#
CO
M2.
22�
1.30
2.44
�1.
420.
17D
isen
gage
men
tB
IO2.
17�
1.09
3.22
�1.
35N
Sp
�.0
1N
S0.
81C
OM
2.28
�0.
832.
67�
1.20
0.38
Phys
ical
rela
xatio
nB
IO1.
77�
0.52
3.10
�0.
95N
Sp
�.0
01N
S1.
32C
OM
1.88
�1.
032.
84�
1.06
0.85
Men
tal
rela
xatio
nB
IO2.
85�
0.98
3.55
�1.
09N
Sp
�.0
1N
S0.
66C
OM
2.66
�1.
163.
26�
0.73
0.60
Slee
pine
ssB
IO1.
67�
1.27
2.22
�0.
79N
SN
SN
S0.
52C
OM
2.00
�1.
352.
50�
1.00
0.42
TO
TA
LSC
OR
EB
IO10
.67
�3.
5616
.09
�3.
65N
Sp
�.0
01N
S1.
21C
OM
11.0
5�
3.93
13.7
1�
3.80
0.67
TR
AN
SCE
ND
EN
CE
Aw
ean
dw
onde
rB
IO2.
61�
0.93
3.00
�1.
32N
SN
SN
S0.
35C
OM
1.78
�0.
672.
44�
1.01
0.74
Pray
erfu
lB
IO2.
33�
1.22
3.00
�1.
21N
SN
SN
S0.
52C
OM
2.11
�1.
272.
22�
1.09
0.10
Dee
pm
yste
ryB
IO2.
56�
1.24
2.78
�1.
20N
SN
SN
S0.
19C
OM
2.33
�1.
002.
56�
1.24
0.20
Tim
eles
s,bo
undl
ess,
infin
iteB
IO2.
44�
0.88
3.00
�1.
41N
SN
SN
S0.
47C
OM
2.00
�1.
222.
56�
1.13
0.47
TO
TA
LSC
OR
EB
IO9.
94�
2.04
11.7
8�
4.12
NS
p�
.05
NS
0.56
CO
M8.
22�
2.33
9.78
�3.
110.
56
Not
e.B
IO�
Bio
feed
back
grou
p;C
OM
�C
ompa
rativ
egr
oup;
NS
�no
n-si
gnifi
cant
.#
Coh
en’s
def
fect
size
s.T
ukey
’spo
stho
cte
st.*
p�
.05.
BIO
ener
gize
dpo
sitiv
efe
elin
gsto
tals
core
.**
p�
.01.
BIO
min
dful
inno
cenc
epr
evs
.BIO
min
dful
inno
cenc
epo
st.
BIO
min
dful
ness
tota
lsco
re.B
IOre
sted
/ref
resh
edpr
evs
.BIO
rest
ed/r
efre
shed
post
.***
p�
.001
.BIO
min
dful
quie
tpre
vs.B
IOm
indf
ulqu
ietp
ost.
401HRV Biofeedback Affects Anxiety and Relaxation

the BIO group increased their score for both mindfulness (p � .01) andenergized positive feelings (p � .05). In addition, there was a time effect formindfulness (p � .01), basic relaxation (p � .001), and transcendence (p �.05). Effect sizes were also calculated for each category.
In the first category of mindfulness, there were interaction effects formindful quiet (p � .05) and innocence (p � .05). Tukey’s post hoc testrevealed that the BIO group increased their scores for both mindful quiet(p � .001) and mindful innocence (p � .01). In addition, there were timeeffects for mindful quiet (p � .0001), mindful innocence (p � .01), mindfulacceptance (p � .05), and mindful centering (p � .01), and a group effect formindful awareness (p � .05). No group, time, or interaction (group � time)effects were found for mindful awakening.
In the category of energized positive feelings, there was a time effect (p �.05) for the category of energized. No group, time, or interaction (group �time) differences were found for optimism/hope/trust, happiness, or feelingthankful and loving.
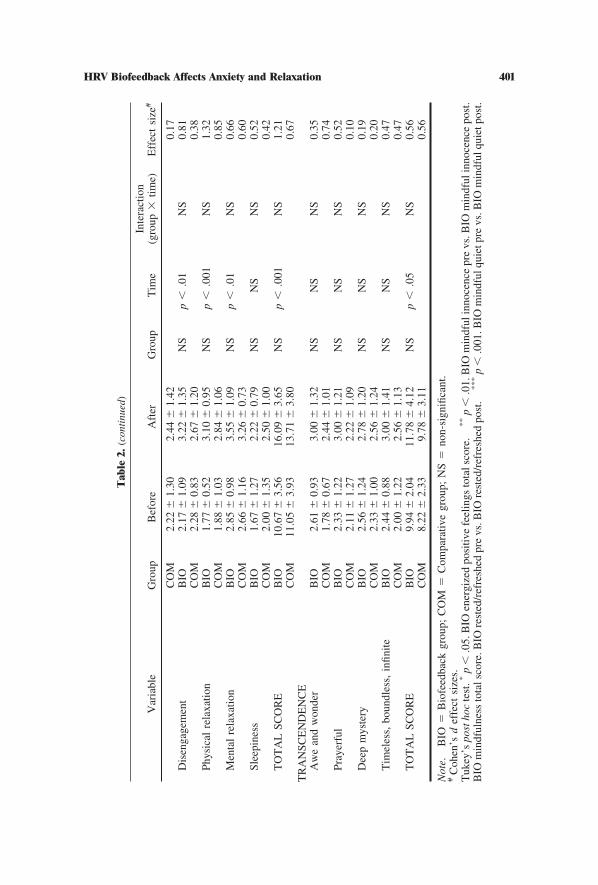
In the category of basic relaxation, there was an interaction effect forfeeling rested and refreshed (p � .05). Tukey’s post hoc test revealed that theBIO group felt more rested and refreshed after than before testing (p � .01).In addition, there were time effects for rested and refreshed (p � .01),disengagement (p � .01), physical relaxation (p � .001), and mental relax-ation (p � .01). No group, time, or interaction (group � time) effects werefound for sleepiness before and after testing.
Finally, in the category of transcendence, no group, time, or interaction(group � time) differences were found for awe and wonder, feeling prayer-ful, deep mystery, or feeling timeless/boundless/infinite.
There were no differences in scores for helpfulness of the device (7 � 1vs. 6 � 2 units, BIO vs. COM) or sleepiness after 5 (4 � 3 vs. 6 � 3 units,BIO vs. COM) or 10 min (5 � 3 vs. 7 � 2 units, BIO vs. COM) of using thedevice; however, the COM group felt more sleepy than the BIO group (5 �3 vs. 7 � 2 units, BIO vs. COM, p � .05) during the rest period after theintervention (Rest 2).
DISCUSSION
The main finding of this study is that a single session of short durationHRV biofeedback resulted in large improvements in total scores for ener-gized positive feelings, mindfulness, and basic relaxation, and a moderateimprovement in transcendence from pre- to posttesting. These changes oc-curred despite the stress induced by the Stroop task (Renaud & Blondin,1997). In contrast, the comparative intervention resulted in only moderate
402 Prinsloo, Derman, Lambert, and Rauch
improvements in basic relaxation and transcendence, a small improvement inmindfulness, and no improvement in energized positive feelings. Althoughthe device used by the comparative group appeared identical to the HRVbiofeedback device, it did not provide biofeedback, but rather displayed awave that the subjects were instructed to observe.
The use of HRV biofeedback resulted in an increase in the total score forthe category of energized positive feelings, yet there was no improvementafter use of the comparative intervention. Although other relaxation tech-niques have been associated with increased feelings of happiness (Davidsonet al., 2003) and joy (Matsumoto & Smith, 2001), no other studies haveexamined the effect of HRV biofeedback on positive energy or positiveemotions.
During resonance frequency breathing, heart rate variability increases asa result of activation of the parasympathetic component of the baroreflex (vande Vooren et al., 2007). Vagally mediated increases in HRV have beenassociated with improved emotion regulation (Thayer, Ahs, Fredrikson,Sollers, & Wager, 2012; Thayer & Lane, 2000). Thayer and Lane haveproposed the Neurovisceral Integration Theory, which describes the inte-grated neural network involving attention, emotion, and autonomic regula-tion (Thayer & Lane, 2000). A key component of this system is the bidirec-tional central autonomic network (CAN), which regulates autonomic flow tothe heart and alters HRV (Thayer & Lane, 2000). Indeed, HRV has beendescribed as providing a “structural and functional link between the brain andthe heart” (Thayer et al., 2012).
The use of HRV biofeedback stimulates the baroreflex (Lehrer et al.,2003), which includes the nucleus tractus solitarius (NTS; Felder & Mifflin,1994). The NTS relays information to the parabrachial nucleus and then tothe thalamus, hypothalamus, and amygdala (Nemeroff et al., 2006; Ressler &Mayberg, 2007). From the thalamus, information is relayed to the insular andprefrontal cortices (Nemeroff et al., 2006). There is bidirectional flow be-tween the anterior insula and basolateral amygdala (Baur, Hanggi, Langer, &Jancke, 2013). Additionally, increased activation of the medial prefrontalcortex (mPFC) has an inhibitory influence over the amygdala (Barbas, Saha,Rempel-Clower, & Ghashghaei, 2003).
Both vagally mediated increases in HRV and improved emotion regula-tion have been associated with increased activity in the mPFC (Lane et al.,2009; Resstel & Correa, 2006; Thayer et al., 2012). In contrast, activation ofthe amygdala has been shown to increase negative emotions (Thayer et al.,2012), and activity in both the amygdala and insula are associated withincreased state anxiety (Baur, Hanggi, Langer, & Jancke, 2013). Therefore,the increased positive emotions found after HRV biofeedback were mostlikely related to increased activity of the mPFC and concomitant inhibition ofthe amygdala and insula, possibly as a result of activation of the NTS.
403HRV Biofeedback Affects Anxiety and Relaxation
Although both interventions resulted in improvement in overall mind-fulness as well as several of the subcategories of mindfulness, HRV biofeed-back led to greater improvement than the comparative intervention, both inoverall mindfulness and in the subcategories of mindful quiet and mindfulinnocence. This suggests that subjects using the HRV biofeedback increasedtheir awareness of internal and external stimuli (Baer, 2003; Bishop et al.,2004; Kabat-Zinn, 2003).
There is little research on the neuroscience of mindfulness or the rela-tionship between mindfulness and HRV. However, both increased HRV andincreased mindfulness have been associated with activation of the prefrontalcortex (Creswell, Way, Eisenberger & Lieberman, 2007; Thayer et al., 2012).Increasing HRV leads to improved attention (Thayer & Brosschot, 2005;Thayer & Lane, 2000), which has been associated with greater mindfulness(Moore & Malinowski, 2009). Both HRV and mindfulness have also beenassociated with emotion regulation (Hayes & Feldman, 2004; Roemer et al.,2009; Thayer et al., 2012), and mindfulness may be associated with theconcurrent increases in positive emotions (Chan et al., 2008). Althoughmindfulness has been shown to increase as a result of meditation (Zeidan,Johnson, Diamond, David, & Goolkasian, 2010) as well as in response toHRV biofeedback in combination with mindfulness training (Kleen & Re-itsma, 2011), this is the first study to look at the effect of HRV biofeedbackalone.
Finally, HRV biofeedback led to greater increases in the basic relaxationsubcategory of feeling rested and refreshed. Increased activation of themedial prefrontal cortex and the resulting inhibition of the amygdala andhypothalamus (Barbas et al., 2003), as described above, contribute to im-proved coping mechanisms and self-regulation (Maier & Watkins, 2010),which may facilitate feelings of relaxation and refreshment.
Both interventions led to increased total scores in the category of basicrelaxation as well as subcategories of disengagement, physical, and mentalrelaxation. This is perhaps not surprising, as both interventions involvefocusing attention on a single variable, which has been shown to increaserelaxation (Benson, 1993). However, the HRV biofeedback had a large effectsize and the comparative intervention a moderate effect size, suggesting thatgreater benefit is achieved when focused attention was combined withbiofeedback-induced slow breathing. Both interventions also led to moder-ately increased total scores in the category of transcendence. No other studieshave examined the effects of HRV biofeedback on feelings of relaxation oron forms of transcendence.
In addition to changes in relaxation states, changes in measures ofanxiety were found. Both groups felt less anxious after testing as indicated bya significant time effect. Although there was no interaction effect, the BIOgroup had a large effect size and the COM group a moderate effect size. A
404 Prinsloo, Derman, Lambert, and Rauch

similar study revealed that both the HRV biofeedback and comparativeintervention groups experienced decreased state anxiety, with the HRVbiofeedback group having a greater decrease (Sherlin et al., 2009). Theauthors used a 15-min intervention as opposed to the 10-min intervention inthis study, which could have accounted for the additional interaction effect.Other studies have also shown a reduction in state anxiety with HRVbiofeedback but in combination with psychotherapy (Mikosch et al., 2010;Reiner, 2008).
Although there were no differences in sleepiness before or after testingbetween groups, the VAS score revealed that the COM group felt sleepierthan the BIO group during the rest period immediately after the intervention.This, together with other results, may be suggestive of somatic relaxation inthe BIO group, and both cognitive and somatic relaxation in the COM group(Davidson & Schwartz, 1976).
The hand held HRV biofeedback device is easy to use, doesn’t requirethe assistance of other individuals, and can be used for short periods of timeas needed throughout the day. Furthermore, benefit is derived from a singlesession of biofeedback and a single training session. Our findings togetherwith other research suggest that HRV biofeedback would be a valuableintervention to include in the management of stress and anxiety (Nolan et al.,2005; Sherlin et al., 2009) as well as in the treatment and prevention of stressand anxiety-related disorders (Karavidas et al., 2007; Zucker, Samuelson,Muench, Greenberg, & Gevirtz, 2009).
A limitation of this study is the small sample size. Therefore, onecriticism of this study might be insufficient statistical power. However, weare confident that the sample size is large enough as we accepted an effectsize of 0.5 as meaningful. HRV biofeedback resulted in effect sizes largerthan 0.5 for changes in anxiety, changes in the four main categories ofrelaxation states as well as changes in 13 of the 19 subcategories.
This study might not be representative of the entire population. Weelected to test only men in an attempt to limit heterogeneity as men andwomen have different responses to stress (Kudielka & Kirschbaum, 2005;Wang et al., 2007). Further research needs to be done to examine the benefitof HRV biofeedback for women. This sample also specifically looks at menin senior managerial positions, and so may not be representative of all jobdescriptions. Furthermore, although the Stroop test has been shown to be aneffective stressor (Renaud & Blondin, 1997), it may not be representative ofstress induced outside the laboratory.
It might be argued that the intervention period was very short and that theresulting changes might, therefore, be difficult to interpret. However, as thecontrol intervention did not lead to the changes evident after HRV biofeed-back, we are certain that the differences found are real. We were specificallyinterested in the acute effect of 10 min of biofeedback, as this is the period
405HRV Biofeedback Affects Anxiety and Relaxation
recommended by the manufacturer for clinical use. The minimum recom-mended time per session is 5 min with a goal to accumulate a total of 20 minper day (Muench, 2008). Although the benefits described above wereachieved with only 10 min of intervention, greater benefits may be achievedwith a longer duration of intervention as described by Sherlin, Gevirtz,Wyckoff, and Muench (2009), as well as with regular training as often majorimprovements in relaxation states occur only after a few weeks of training(Ghoncheh & Smith, 2004).
In conclusion, although both interventions facilitated reduced anxietyand increased scores for mindfulness, basic relaxation, and transcendence,HRV biofeedback had added benefit with greater increases in scores formindfulness and basic relaxation, as well as increased energized positivefeelings. Further, although there was no difference in sleepiness after testing,immediately after the intervention the HRV biofeedback group felt alert yetthe comparative group felt sleepy.
REFERENCES
American Psychological Association. (2012). The different kinds of stress. Retrieved fromhttp://www.apa.org/helpcenter/stress-tips.aspx
Aspinwall, L. G. (1998). Rethinking the role of positive affect in self-regulation. Motivationand Emotion, 22, 1–32. doi:10.1023/A:1023080224401
Baer, R. A. (2003). Mindfulness training as a clinical intervention: A conceptual and empiricalreview. Clinical Psychology: Science and Practice, 10, 125–143. doi:10.1093/clipsy.bpg015
Barbas, H., Saha, S., Rempel-Clower, N., & Ghashghaei, T. (2003). Serial pathways fromprimate prefrontal cortex to autonomic areas may influence emotional expression. BMCNeuroscience, 4, 25. doi:10.1186/1471-2202-4-25
Barnes, L. L. B., Harp, D., & Sik Jung, W. (2002). Reliability generalization of scores on theSpielberger state-trait anxiety inventory. Educational and Psychological Measurement,62, 603–618. doi:10.1177/0013164402062004005
Baur, V., Hanggi, J., Langer, N., & Jancke, L. (2013). Resting-state functional and structuralconnectivity within an insula-amygdala route specifically index state and trait anxiety.Biological Psychiatry, 73, 85–92. doi:10.1016/j.biopsych.2012.06.003
Benson, H. (1975). The relaxation response. New York, NY: Morrow.Benson, H. (1993). The relaxation response. In D. Goleman & J. Gurin (Eds.), Mind/body
medicine: How to use your mind for better health (pp. 233–257). Yonkers, NY: ConsumerReports Books.
Bishop, S. R., Lau, M., Shapiro, S., Carlson, L., Anderson, N. D., Carmody, J., & Devins, G.(2004). Mindfulness: A proposed operational definition. Clinical Psychology: Science andPractice, 11, 230–241. doi:10.1093/clipsy.bph077
Brotman, D. J., Golden, S. H., & Wittstein, I. S. (2007). The cardiovascular toll of stress.Lancet, 370, 1089–1100. doi:10.1016/S0140-6736(07)61305-1
Brown, K. W., & Ryan, R. M. (2003). The benefits of being present: Mindfulness and its rolein psychological well-being. Journal of Personality and Social Psychology, 84, 822–848.doi:10.1037/0022-3514.84.4.822
Burns, J. L., Labbe, E., Arke, B., Capeless, K., Cooksey, B., Steadman, A., & Gonzales, C.(2002). The effects of different types of music on perceived and physiological measuresof stress. Journal of Music Therapy, 39, 101–116.
406 Prinsloo, Derman, Lambert, and Rauch
Cahn, B. R., & Polich, J. (2006). Meditation states and traits: EEG, ERP, and neuroimagingstudies. Psychological Bulletin, 132, 180–211. doi:10.1037/0033-2909.132.2.180
Carmody, J., & Baer, R. A. (2008). Relationships between mindfulness practice and levels ofmindfulness, medical and psychological symptoms and well-being in a mindfulness-basedstress reduction program. Journal of Behavioral Medicine, 31, 23–33. doi:10.1007/s10865-007-9130-7
Chambers, R., Chuen Yee Lo, B., & Allen, N. B. (2008). The impact of intensive mindfulnesstraining on attentional control, cognitive style and affect. Cognitive Therapy and Re-search, 32, 303–322. doi:10.1007/s10608-007-9119-0
Chan, A. S., Han, Y. M., & Cheung, M. C. (2008). Electroencephalographic (EEG)measurements of mindfulness-based Triarchic body-pathway relaxation technique: Apilot study. Applied Psychophysiology and Biofeedback, 33, 39 – 47. doi:10.1007/s10484-008-9050-5
Chandola, T., Brunner, E., & Marmot, M. (2006). Chronic stress at work and the metabolicsyndrome: Prospective study. British Medical Journal, 332, 521–525. doi:10.1136/bmj.38693.435301.80
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.). Hillsdale, NJ:Erlbaum.
Coward, D. D. (1996). Self-transcendence and correlates in a healthy population. NursingResearch, 45, 116–121. doi:10.1097/00006199-199603000-00011
Creswell, J. D., Way, B. M., Eisenberger, N. I., & Lieberman, M. D. (2007). Neura correlatesof dispositional mindfulness during affect labeling. Psychosomatic Medicine, 69, 560–565. doi:10.1097/PSY.0b013e3180f6171f
Davidson, R. J., Kabat-Zinn, J., Schumacher, J., Rosenkranz, M., Muller, D., Santorelli, S. F.,. . . Sheridan, J. F. (2003). Alterations in brain and immune function produced bymindfulness meditation. Psychosomatic Medicine, 65, 564–570. doi:10.1097/01.PSY.0000077505.67574.E3
Davidson, R. J., & Schwartz, G. E. (1976). Psychobiology of relaxation and related states: Amulti-process theory. In D. I. Mostofsky (Ed.), Behavioural control and the modificationof physiological activity (pp. 200–233). New York, NY: Free Press.
Ellermann, C. R., & Reed, P. G. (2001). Self-transcendence and depression in middle-ageadults. Western Journal of Nursing Research, 23, 698 –713. doi:10.1177/01939450122045492
Eppley, K. R., Abrams, A. I., & Shear, J. (1989). Differential effects of relaxation techniqueson trait anxiety: A meta-analysis. Journal of Clinical Psychology, 45, 957–974. doi:10.1002/1097-4679(198911)45:6�957::AID-JCLP2270450622�3.0.CO;2-Q
Esch, T., Fricchione, G. L., & Stefano, G. B. (2003). The therapeutic use of the relaxationresponse in stress-related diseases. Medical Science Monitor, 9, RA23–RA34.
Esch, T., Stefano, G. B., Fricchione, G. L., & Benson, H. (2002). The role of stress inneurodegenerative diseases and mental disorders. Neuroendocrinology Letters, 23, 199–208.
Felder, R. B., & Mifflin, S. W. (1994). Baroreceptor and chemoreceptor afferent processing inthe solitary tract nucleus. In I. R. A. Barraco (Ed.), Nucleus of the solitary tract (pp.169–186). Boca Raton, FL: CRC Press.
Forstmann, B. U., Dutilh, G., Brown, S., Neumann, J., von Cramon, D. Y., Ridderinkhof, K. R.,& Wagenmakers, E. (2008). Striatum and pre-SMA facilitate decision-making under timepressure. Proceedings of the National Academy of Sciences of the United States ofAmerica, 105, 17538–17542. doi:10.1073/pnas.0805903105
Fredrickson, B. L. (2000). Cultivating positive emotions to optimize health and well-being.Prevention & Treatment, 3, 1–25. doi:10.1037/1522-3736.3.1.31a
Fredrickson, B. L., & Joiner, T. (2002). Positive emotions trigger upward spirals towardemotional well-being. Psychological Science, 13, 172–175. doi:10.1111/1467-9280.00431
Ghoncheh, S., & Smith, J. C. (2004). Progressive muscle relaxation, yoga stretching, and ABCrelaxation theory. Journal of Clinical Psychology, 60, 131–136. doi:10.1002/jclp.10194
Giardino, N. D., Chan, L., & Borson, S. (2004). Combined heart rate variability and pulseoximetry biofeedback for chronic obstructive pulmonary disease: Preliminary findings.
407HRV Biofeedback Affects Anxiety and Relaxation
Applied Psychophysiology and Biofeedback, 29, 121–133. doi:10.1023/B:APBI.0000026638.64386.89
Gillani, N. B., & Smith, J. C. (2001). Zen meditation and ABC relaxation theory: Anexploration of relaxation states, beliefs, dispositions, and motivations. Journal of ClinicalPsychology, 57, 839–846. doi:10.1002/jclp.1053
Hardt, J., & Rutter, M. (2004). Validity of adult retrospective reports of adverse childhoodexperiences: Review of the evidence. Journal of Child Psychology and Psychiatry, 45,260–273. doi:10.1111/j.1469-7610.2004.00218.x
Hassett, A. L., Radvanski, D. C., Vaschillo, E. G., Vaschillo, B., Sigal, L. H., Karavidas, M. K.,. . . Lehrer, P. M. (2007). A pilot study of the efficacy of heart rate variability (HRV)biofeedback in patients with fibromyalgia. Applied Psychophysiology and Biofeedback,32, 1–10. doi:10.1007/s10484-006-9028-0
Hayes, A. M., & Feldman, G. (2004). Clarifying the construct of mindfulness in the context ofemotion regulation and the process of change in therapy. Clinical Psychology: Scienceand Practice, 11, 255–262. doi:10.1093/clipsy.bph080
Heilman, K. J., Handelman, M., Lewis, G., & Porges, S. W. (2008). Accuracy of theStressEraser in the detection of cardiac rhythms. Applied Psychophysiology and Biofeed-back, 33, 83–89. doi:10.1007/s10484-008-9054-1
Kabat-Zinn, J. (2003). Mindfulness-based interventions in context: Past, present, and future.Clinical Psychology: Science and Practice, 10, 144–156. doi:10.1093/clipsy.bpg016
Karavidas, M. K., Lehrer, P. M., Vaschillo, E., Vaschillo, B., Marin, H., Buyske, S., . . . Hassett,A. (2007). Preliminary results of an open label study of heart rate variability biofeedbackfor the treatment of major depression. Applied Psychophysiology and Biofeedback, 32,19–30. doi:10.1007/s10484-006-9029-z
Kleen, M., & Reitsma, B. (2011). Appliance of Heart Rate Variability biofeedback in accep-tance and commitment therapy: A pilot study. Journal of Neurotherapy, 15, 170–181.doi:10.1080/10874208.2011.570695
Krisanaprakornkit, T., Krisanaprakornkit, W., Plyavhatkul, N., & Laopaiboon, M. (2006).Meditation therapy for anxiety disorders. Cochrane Database of Systematic Reviews, 1,CD004998.
Kudielka, B. M., & Kirschbaum, C. (2005). Sex differences in HPA axis responses to stress:A review. Biological Psychology, 69, 113–132. doi:10.1016/j.biopsycho.2004.11.009
Labbe, E., Schmidt, N., Babin, J., & Pharr, M. (2007). Coping with stress: The effectiveness ofdifferent types of music. Applied Psychophysiology and Biofeedback, 32, 163–168.doi:10.1007/s10484-007-9043-9
Lane, R. D., McRae, K., Reiman, E. M., Chen, K., Ahern, G. L., & Thayer, J. F. (2009). Neuralcorrelates of heart rate variability during emotion. NeuroImage, 44, 213–222. doi:10.1016/j.neuroimage.2008.07.056
Lehrer, P. M., Vaschillo, E., & Vaschillo, B. (2000). Resonant frequency biofeedback trainingto increase cardiac variability: Rationale and manual for training. Applied Psychophysi-ology and Biofeedback, 25, 177–191. doi:10.1023/A:1009554825745
Lehrer, P. M., Vaschillo, E., Vaschillo, B., Lu, S. E., Eckberg, D. L., Edelberg, R., . . .Hamer, R. (2003). Heart rate variability biofeedback increases baroreflex gain andpeak expiratory flow. Psychosomatic Medicine, 65, 796 – 805. doi:10.1097/01.PSY.0000089200.81962.19
Lehrer, P. M., Vaschillo, E., Vaschillo, B., Lu, S. E., Scardella, A., Siddique, M., & Habib,R. H. (2004). Biofeedback treatment for asthma. Chest, 126, 352–361. doi:10.1378/chest.126.2.352
Lehrer, P. M., Woolfolk, R. L., Rooney, A. J., McCann, B., & Carrington, P. (1983).Progressive relaxation and meditation. A study of psychophysiological and therapeuticdifferences between two techniques. Behavioral Research and Therapy, 21, 651–662.doi:10.1016/0005-7967(83)90083-9
Lehrer, P. M., Woolfolk, R. L., & Sime, W. E. (2007). Principles and practice of stressmanagement (3rd ed.) New York, NY: Guilford Press.
Levenson, M. R., & Crumpler, C. A. (1996). Three models of adult development. HumanDevelopment, 39, 135–149. doi:10.1159/000278429
408 Prinsloo, Derman, Lambert, and Rauch

Maier, S. F., & Watkins, L. R. (2010). Role of the medial prefrontal cortex in coping andresilience. Brain Research, 1355, 52–60. doi:10.1016/j.brainres.2010.08.039
Manzoni, G. M., Pagnini, F., Castelnuovo, G., & Molinari, E. (2008). Relaxation training foranxiety: A ten-years systematic review with meta-analysis. BMC Psychiatry, 8, 41.doi:10.1186/1471-244X-8-41
Matsumoto, M., & Smith, J. C. (2001). Progressive muscle relaxation, breathing exercises, andABC relaxation theory. Journal of Clinical Psychology, 57, 1551–1557. doi:10.1002/jclp.1117
Mikosch, P., Hadrawa, T., Laubreiter, K., Brandl, J., Pilz, J., Stettner, H., & Grimm, G. (2010).Effectiveness of respiratory-sinus-arrhythmia biofeedback on state-anxiety in patientsundergoing coronary angiography. Journal of Advanced Nursing, 66, 1101–1110. doi:10.1111/j.1365-2648.2010.05277.x
Miyake, A., Friedman, N. P., Emerson, M. J., Witzki, A. H., Howerter, A., & Wager, T. D.(2000). The unity and diversity of executive functions and their contributions to complex“Frontal Lobe” tasks: A latent variable analysis. Cognitive Psychology, 41, 49–100.doi:10.1006/cogp.1999.0734
Moore, A., & Malinowski, P. (2009). Meditation, mindfulness and cognitive flexibility.Consciousness and Cognition, 18, 176–186. doi:10.1016/j.concog.2008.12.008
Muench, F. (2008). The portable stresseraser heart rate variability biofeedback device: Back-ground and research. Biofeedback, 36, 35–39.
National Institute of Mental Health. (2012). Any anxiety disorder among adults. Retrieved fromhttp://www.nimh.nih.gov/statistics/1ANYANX_ADULT.shtml
Nemeroff, C. B., Mayberg, H. S., Krahl, C. E., McNamara, J., Frazer, A., Henry, T. R., . . .Brannan, S. K. (2006). VNS therapy in treatment-resistant depression: Clinical evidenceand putative neurobiological mechanisms. Neuropsychopharmacology, 31, 1345–1355.doi:10.1038/sj.npp.1301082
Nolan, R. P., Kamath, M. V., Floras, J. S., Stanley, J., Pang, C., Picton, P., & Young, Q. R.(2005). Heart rate variability biofeedback as a behavioral neurocardiac intervention toenhance vagal heart rate control. American Heart Journal, 149, 1137.
Orem, D. M., Petrac, D. C., & Bedwell, J. S. (2008). Chronic self-perceived stress andset-shifting performance in undergraduate students. Stress, 11, 73–78. doi:10.1080/10253890701535103
Prinsloo, G. E., Derman, W. E., Lambert, M. I., Muench, F., & Rauch, H. G. L. (2013). Theeffect of a single session of short duration biofeedback-induced deep breathing onmeasures of heart rate variability during laboratory-induced cognitive stress: A pilot study.Applied Psychophysiology and Biofeedback, 38, 81–90. doi:10.1007/s10484-013-9210-0
Prinsloo, G. E., Rauch, H. G. L., Karpul, D., & Derman, W. E. (2013). The effect of a singlesession of short duration heart rate variability biofeedback on EEG: A pilot study. AppliedPsychophysiology and Biofeedback, 38, 45–56. doi:10.1007/s10484-012-9207-0
Rauch, H., John, L., St. Clair Gibson, A., Noakes, T., & Vaughan, C. (2005, September).Validation study of EEG responses during a modified Stroop colour word test. Proceed-ings of the Physiology Society of Southern Africa 33rd Conference, Cape Town, SouthAfrica.
Reiner, R. (2008). Integrating a portable biofeedback device into clinical practice for patientswith anxiety disorders: Results of a pilot study. Applied Psychophysiology and Biofeed-back, 33, 55–61. doi:10.1007/s10484-007-9046-6
Renaud, P., & Blondin, J. P. (1997). The stress of Stroop performance: Physiological andemotional responses to color-word interference, task pacing, and pacing speed. Interna-tional Journal of Psychophysiology, 27, 87–97. doi:10.1016/S0167-8760(97)00049-4
Ressler, K., & Mayberg, H. S. (2007). Targeting abnormal neural circuits in mood and anxietydisorders: From the laboratory to the clinic. Nature Neuroscience, 10, 1116–1124.doi:10.1038/nn1944
Resstel, L. B. M., & Correa, F. M. A. (2006). Medial prefrontal cortex NMDA receptors andnitric oxide modulate the parasympathetic component of the baroreflex. European Journalof Neuroscience, 23, 481–488. doi:10.1111/j.1460-9568.2005.04566.x
409HRV Biofeedback Affects Anxiety and Relaxation
Richardson, K. M., & Rothstein, H. R. (2008). Effects of occupational stress managementintervention programs: A meta-analysis. Journal of Occupational Health Psychology, 13,69–93. doi:10.1037/1076-8998.13.1.69
Roemer, L., Lee, J. K., Salters-Pedneault, K., Erisman, S. M., Orsillo, S. M., & Menning, D. S.(2009). Mindfulness and emotion regulation difficulties in generalised anxiety disorder:Preliminary evidence for independent and overlapping contributions. Behavior Therapy,40, 142–154. doi:10.1016/j.beth.2008.04.001
Sauro, M. D., Jorgensen, R. S., & Pedlow, C. T. (2003). Stress, glucocorticoids, and memory:A meta-analytic review. Stress, 6, 235–245. doi:10.1080/10253890310001616482
Sherlin, L., Gevirtz, R., Wyckoff, S., & Muench, F. (2009). Effects of Respiratory SinusArrythmia Biofeedback versus Passive Biofeedback Control. International Journal ofStress Management, 16, 233–248. doi:10.1037/a0016047
Smith, J. C. (2004). Alterations in brain and immune function produced by mindfulnessmeditation: Three caveats. Psychosomatic Medicine, 66, 148–152.
Smith, J. C. (2005a). Relaxation, meditation, and mindfulness: A mental health practitioner’sguide to new and traditional approaches. New York, NY: Springer.
Smith, J. C. (2005b). Smith Relaxation States Inventory 3 (SRSI3). Raleigh, NC: LuluPress.Smith, J. C. (2007). The psychology of relaxation. In P. M. Lehrer, R. L. Woolfolk, & W. E.
Sime (Eds.), Principles and practice of stress management (3rd ed., pp. 38–52). NewYork, NY: Guilford Press.
Smith, J. C. (2010). Smith Relaxation States Inventory 3 (SRSI3). Raleigh, NC: LuluPress.Smith, J. C., Wedell, A. B., Kolotylo, C. J., Lewis, J. E., Byers, K. Y., & Segin, C. M. (2000).
ABC Relaxation Theory and factor structure of relaxation states, recalled relaxationactivities, dispositions, and motivations. Psychological Reports, 86, 1201–1208.
Spielberger, C. (1983). Manual for the State-Trait Anxiety Inventory. Palo Alto, CA: ConsultingPsychologists Press.
Stroop, J. R. (1935). Studies of interference in serial verbal reactions. Journal of ExperimentalPsychology, 18, 643–662.
Thayer, J. F., Ahs, F., Fredrikson, M., Sollers, J. J., & Wager, T. D. (2012). A meta-analysisof heart rate variability and neuroimaging studies: Implications for heart rate variability asa marker of stress and health. Neuroscience and Biobehavioral Reviews, 36, 747–756.doi:10.1016/j.neubiorev.2011.11.009
Thayer, J. F., & Brosschot, J. F. (2005). Psychosomatics and psychopathology: Looking up anddown from the brain. Psychoneuroendocrinology, 30, 1050–1058. doi:10.1016/j.psyneuen.2005.04.014
Thayer, J. F., & Lane, R. D. (2000). A model of neurovisceral integration in emotion regulationand dysregulation. Journal of Affective Disorders, 61, 201–216. doi:10.1016/S0165-0327(00)00338-4
van de Vooren, H., Gademan, M. G. J., Swenne, C. A., Ten Voorde, B. J., Schalij, M. J.,& Van Der Wall, E. E. (2006). Baroreflex sensitivity, blood pressure buffering andresonance: What are the links? Computer simulation of healthy subjects and heartfailure patients. Journal of Applied Physiology, 102, 1348 –1356. doi:10.1152/japplphysiol.00158.2006
Vaschillo, E. G., Vaschillo, B., & Lehrer, P. (2006). Characteristics of Resonance in Heart RateVariability Stimulated by Biofeedback. Applied Psychophysiology and Biofeedback, 31,129–142. doi:10.1007/s10484-006-9009-3
Walker, L. G. (1990). The measurement of anxiety. Postgraduate Medical Journal, 66 Suppl,2, S11–S17.
Wang, J., Korczykowski, M., Rao, H., Fan, Y., Pluta, J., Gur, R. C., . . . Detre, J. A. (2007).Gender difference in neural response to psychological stress. Social Cognitive andAffective Neuroscience, 2, 227–239. doi:10.1093/scan/nsm018
Williams, K. A., Kolar, M. M., Reger, B. E., & Pearson, J. C. (2001). Evaluation of aWellness-Based Mindfulness Stress Reduction intervention: A controlled trial. AmericanJournal of Health Promotion, 15, 422–432. doi:10.4278/0890-1171-15.6.422
Zeidan, F., Johnson, S. K., Diamond, B. J., David, Z., & Goolkasian, P. (2010). Mindfulnessmeditation improves cognition: Evidence of brief mental training. Consciousness andCognition, 19, 597–605. doi:10.1016/j.concog.2010.03.014
410 Prinsloo, Derman, Lambert, and Rauch
Zucker, T. L., Samuelson, K. W., Muench, F., Greenberg, M. A., & Gevirtz, R. N. (2009). Theeffects of respiratory sinus arrhythmia biofeedback on heart rate variability and posttrau-matic stress disorder symptoms: A pilot study. Applied Psychophysiology and Biofeed-back, 34, 135–143. doi:10.1007/s10484-009-9085-2
Received March 13, 2011Revision received August 21, 2013
Accepted September 17, 2013 �
Members of Underrepresented Groups:Reviewers for Journal Manuscripts Wanted
If you are interested in reviewing manuscripts for APA journals, the APAPublications and Communications Board would like to invite your participation.Manuscript reviewers are vital to the publications process. As a reviewer, youwould gain valuable experience in publishing. The P&C Board is particularlyinterested in encouraging members of underrepresented groups to participatemore in this process.
If you are interested in reviewing manuscripts, please write APA Journals [email protected]. Please note the following important points:
• To be selected as a reviewer, you must have published articles in peer-reviewed journals. The experience of publishing provides a reviewer with thebasis for preparing a thorough, objective review.
• To be selected, it is critical to be a regular reader of the five to six empiricaljournals that are most central to the area or journal for which you would liketo review. Current knowledge of recently published research provides areviewer with the knowledge base to evaluate a new submission within thecontext of existing research.
• To select the appropriate reviewers for each manuscript, the editor needsdetailed information. Please include with your letter your vita. In the letter,please identify which APA journal(s) you are interested in, and describe yourarea of expertise. Be as specific as possible. For example, “social psychol-ogy” is not sufficient—you would need to specify “social cognition” or“attitude change” as well.
• Reviewing a manuscript takes time (1–4 hours per manuscript reviewed). Ifyou are selected to review a manuscript, be prepared to invest the necessarytime to evaluate the manuscript thoroughly.
APA now has an online video course that provides guidance in reviewingmanuscripts. To learn more about the course and to access the video, visithttp://www.apa.org/pubs/authors/review-manuscript-ce-video.aspx.
411HRV Biofeedback Affects Anxiety and Relaxation



























![Love Getting to the Heart of It With Tom Stone [Episode 43] Wired for Success TV](https://img.pdfslide.net/doc/110x75/552d52c94a7959065d8b4691/love-getting-to-the-heart-of-it-with-tom-stone-episode-43-wired-for-success-tv.jpg)
