Embed Size (px)
Citation preview
Eur J Clin Pharmacol (1988) 35:47-52 European Journa, of (~[]~[]:~(~Q~
@ Springer-Verlag 1988
The Effect of Cardiopulmonary Bypass on Plasma Protein Binding of Alfentanil
K. Kumar ~, D.P. Crankshaw 2, D.J. Morgan 1, and G. H. Beemer 2
1 Victorian College of Pharmacy, Melbourne 2 University Departments of Surgery and Anaesthetics, Amalgamated Melbourne and Essendon Hospitals, Victoria, Australia
Summary. The effect of cardiopulmonary bypass (CPB) on plasma concentration and protein binding of alfentanil was studied during continuous infu- sions in five cardiac surgical patients. Patients were given a loading infusion of 10 ~tg- min- 1. kg- 1 lean body mass (LBM) over 30 s followed by a fixed rate maintenance infusion of 1 ~tg.min -1.kg -1 LBM for the duration of surgery.
Prior to the commencement of CPB the total plasma alfentanil concentration was 177~g.1-1. This fell to 92 ~g. 1-1 2 min after commencement of CPB and rose to 155~g.1-1 at the end of CPB 2.01 h later. During the same period the unbound fraction of alfentanil rose from 0.16 to 0.35 two min after the start of CPB and fell gradually to 0.22 at the end of CPB. The unbound concentration prior to CPB was 29 ~tg.1-1 and was essentially un- changed by the onset of CPB, being 35 ~tg.1 - t at two min and then 31 p.g.1-1 at the end of CPB. There was a good correlation between alfentanil bound/unbound concentration ratio and plasma albumin concentration (r= 0.57) and plasma ~l-acid glycoprotein concentration (r= 0.80), indicating that the decrease in binding during CPB was due pri- marily to haemodilution.
In assessing the effects of CPB on plasma drug concentrations, it is therefore necessary to monitor unbound as well as total concentrations because the effects on these differ greatly.
Key words: alfentanil; plasma protein binding, car- diopulmonary bypass, intravenous infusion
The narcotic analgesics are currently the most com- monly used drugs for maintenance of anesthesia during cardiopulmonary bypass (CPB). While fen- tanyl has been in most common use, the recent
availability of alfentanil, with favourable pharma- cokinetic properties, has led to its increasing use [1]. Furthermore, the availability of a special infusion pump (BARD Harvard Mini-Infuser 950), which provides constant plasma concentration by means of programmed delivery based on elimination phar- macokinetics [2], has encouraged the use of alfen- tanil.
Cardiopulmonary bypass involves acute phy- siological changes including hemodilution, hy- potension, hypothermia and diminished renal and hepatic function [3]. Recently, we have shown that during programmed infusion of thiopentone [4] and methohexitone [5], dilution of plasma and hence of total drug concentration leaves the concentration of the unbound and therapeutically active fraction es- sentially unchanged. The onset of CPB has been shown to produce large changes in the plasma con- centration of other drugs. Increased total plasma concentrations during CPB have been reported for gallamine [6], alcuronium [7] and cephalothin [8] while increased total and unbound concentrations have been reported for d-tubocurarine [9]. On the other hand, a decrease in total plasma concentra- tions has been reported during CPB for pancuro- nium [10], propranolol [11], digitoxin [12], cefazolin [13] and fentanyl [14, 15] indicating that the effects vary from drug to drug.
Studies with alfentanil administered as a bolus during cardiac surgery have shown that the elimina- tion half-life of the drug is three times longer after CPB because of an increase in its distribution vol- ume [16]. During continuous infusion, commence- ment of CPB results in a decrease in the plasma al- fentanil concentration [1, 17] and a lower dose re- quirement based on somatic responses and systolic arterial pressure [17]. It was suggested that these changes might be due to changes in protein binding
48 K. Kumar et al.: Cardiopulmonary Bypass and Alfentanil Plasma Binding
as a result of the onset of CPB, but this has not been demonstrated.
Alfentanil, a basic drug, has been shown, in vitro, to be bound mainly to at-acid glycoprotein (AAG) and less to albumin, globulin and red blood cells in contrast to acidic drugs such as the barbitu- rates, which bind mainly to albumin [18]. In vitro studies of the effect of hemodilution have led to the suggestion that an increase in unbound fraction is likely during CPB [19].
The aim of the present study was to examine the magnitude and time course of the effect of CPB on both total and unbound concentrations of alfen- tanil. We have used a bolus and constant rate infu- sion for drug administration to establish a stable concentration of alfentanil prior to CPB and there- fore enable the effects of CPB on drug concentra- tion and binding to be defined more clearly.
Methods
Five patients participated in the study after giving written, informed consent. None of the patients showed any clinical or biochemical evidence of hepatic dysfunction. The patients were undergoing coronary artery bypass graft surgery and the proto- col for the study was approved by the Board of Medical Research of the Royal Melbourne Hospi- tal.
All patients were premedicated at least 1 h be- fore surgery with papaverine 20rag, hyoscine 0.4 mg (Patients 1, 2, 3 and 5) or diazepam 5 mg PO, droperidol 2.5mg and morphine sulphate 5mg (Patient 4).
Alfentanil was administered as a rapid loading infusion of 10 Ixg.min -1-kg - t of lean body mass (LBM) over 30 s, followed by a maintenance infu- sion of lp~g.min-l.kg -1 LBM for the duration of surgery. The mean duration of the infusion was 3.35+0.28 h (Table 1). LBM (Table 1) was calcu- lated from height, total body weight and gender by
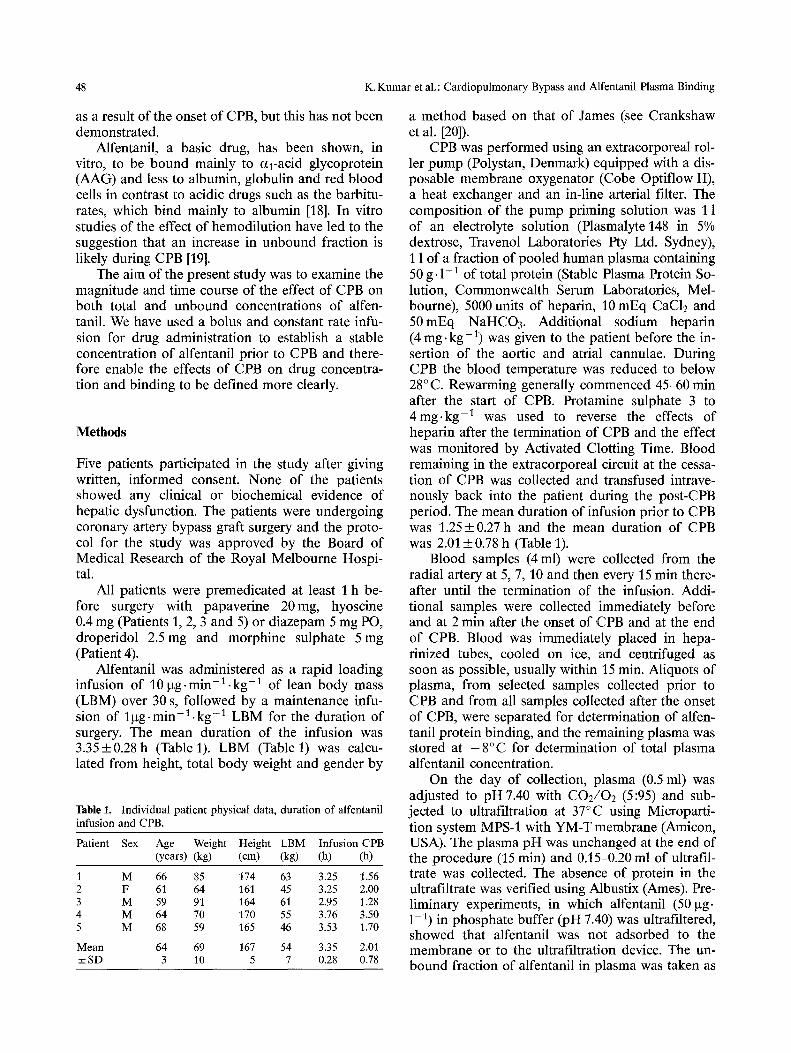
Table I. Individual patient physical data, duration of alfentanil infusion and CPB.
Patient Sex Age Weight Height LBM Infusion CPB (years) (kg) (cm) (kg) (h) (h)
1 M 66 85 174 63 3.25 1.56 2 F 61 64 161 45 3.25 2.00 3 M 59 91 164 61 2.95 1.28 4 M 64 70 170 55 3.76 3.50 5 M 68 59 165 46 3.53 1.70
Mean 64 69 167 54 3.35 2.01 ± S D 3 10 5 7 0.28 0.78
a method based on that of James (see Crankshaw et al. [20]).
CPB was performed using an extracorporeal rol- ler pump (Polystan, Denmark) equipped with a dis- posable membrane oxygenator (Cobe Optiflow II), a heat exchanger and an in-line arterial filter. The composition of the pump priming solution was 1 1 of an electrolyte solution (Plasmalyte 148 in 5% dextrose, Travenol Laboratories Pty Ltd. Sydney), 1 1 of a fraction of pooled human plasma containing 50 g. 1-1 of total protein (Stable Plasma Protein So- lution, Commonwealth Serum Laboratories, Mel- bourne), 5000 units of heparin, 10 mEq CaC12 and 50mEq NaHCO3. Additional sodium heparin (4 mg. kg-1) was given to the patient before the in- sertion of the aortic and atrial cannulae. During CPB the blood temperature was reduced to below 28°C. Rewarming generally commenced 45-60 min after the start of CPB. Protamine sulphate 3 to 4mg-kg - t was used to reverse the effects of heparin after the termination of CPB and the effect was monitored by Activated Clotting Time. Blood remaining in the extracorporeal circuit at the cessa- tion of CPB was collected and transfused intrave- nously back into the patient during the post-CPB period. The mean duration of infusion prior to CPB was 1.25 +0.27 h and the mean duration of CPB was 2.01 _+ 0.78 h (Table 1).
Blood samples (4 ml) were collected from the radial artery at 5, 7, 10 and then every 15 min there- after until the termination of the infusion. Addi- tional samples were collected immediately before and at 2 min after the onset of CPB and at the end of CPB. Blood was immediately placed in hepa- rinized tubes, cooled on ice, and centrifuged as soon as possible, usually within 15 min. Aliquots of plasma, from selected samples collected prior to CPB and from all samples collected after the onset of CPB, were separated for determination of alfen- tanil protein binding, and the remaining plasma was stored at - 8 ° C for determination of total plasma alfentanil concentration.
On the day of collection, plasma (0.5 ml) was adjusted to pH 7.40 with CO2/O2 (5:95) and sub- jected to ultrafiltration at 37°C using Microparti- tion system MPS-1 with YM-T membrane (Amicon, USA). The plasma pH was unchanged at the end of the procedure (15 min) and 0.15-0.20 ml of ultrafil- trate was collected. The absence of protein in the ultrafiltrate was verified using Albustix (Ames). Pre- liminary experiments, in which alfentanil (50 p~g. 1 - t ) in phosphate buffer (pH 7.40) was ultrafiltered, showed that alfentanil was not adsorbed to the membrane or to the ultrafiltration device. The un- bound fraction of alfentanil in plasma was taken as

K. Kumar et al.: Cardiopulmonary Bypass and Alfentanil Plasma Binding 49
the ratio of the ultrafiltrate concentration to the total in an unfiltered sample. Preliminary experi- ments also showed that binding determinations, carried out at 37°C and 25°C did not differ signifi- cantly.
Plasma and ultrafiltrate concentrations of alfen- tanil were determined by high pressure liquid chro- matography with ultraviolet detection, as described previously [21]. The detection limit of the assay was 1 lxg. 1-1. Plasma albumin and AAG concentrations were determined by radial immunodiffusion using Nor-Partigen plates (Behringwerke AG, Marburg, FRG). The influence of plasma concentration on al- fentanil plasma protein binding was determined by correlating the ratio of bound fraction (B) to un- bound fraction (F) with the concentration of pro- tein. Provided the dissociation constant for the drug-protein complex is much greater that molar concentration of unbound drug, there will be a lin- ear relationship between B /F and protein concen- tration [22].
Correlation between variables was investigated by linear regression and differences among means of two or more groups of dependent data by the Bonferroni t-test [23], assuming a normal distribu- tion. A probability less than 0.05 was considered statistically significant.
Results
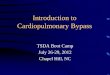
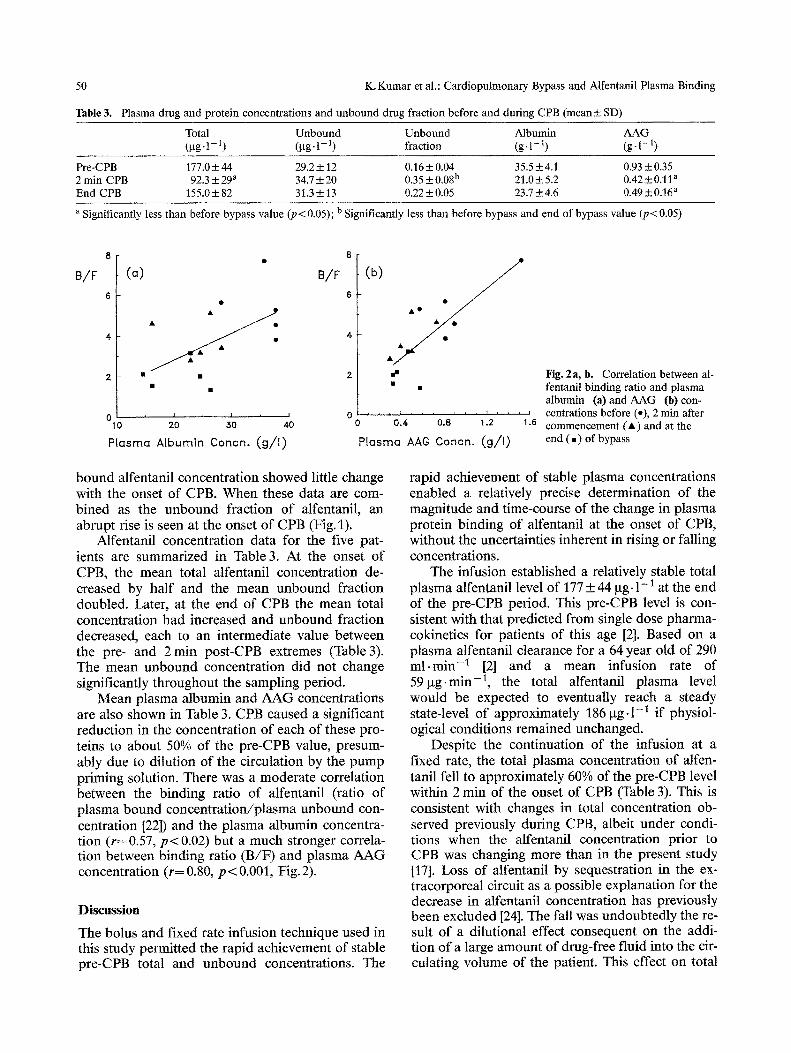
Individual patient physical data, duration of alfen- tanil infusion and of CPB are shown in Table 1. Re- cent preoperative and pre CPB drug therapy for each patient is summarized in Table 2. The plasma concentration of total and unbound alfentanil and the unbound fraction of alfentanil in plasma during intravenous administration of alfentanil are shown for a typical patient (Number 5) in Fig.1. In the time leading up to the onset of CPB, the total plas- ma concentration of alfentanil was relatively stable. On initiation of CPB, however, the total alfentanil concentration fell abruptly. In contrast, the un-
Table 2. Pre-operative and pre-CPB drug therapy in individual patients
Patient Drugs, previous 24 h Drugs, pre-CPB
1 Nifedipine 10 mg tds, GTN paste, atenolol 50 mg, dipyridamole 100 mg tds, temazepam 10 rag, aspirin 500 mg
GTN paste, dipyridamole 100 mg tds, temazepam 10 rag, aspirin 500 mg
Verapamil 80 mg tds, dipyridamole 100 mg tds, temazepam 10 mg, aspirin 500 mg
Dipyridamole 100 mg tds, diltiazem 120 mg bd, allopurinol 300 mg, ranitidine 150 mg bd, temazepam 10 mg nocte
Nifedipine 20 mg tds, GTN paste, frusemide 80 mg bd, dipyridamole 100 mg tds
diazepam 20 mg, gentamicin 160 mg, flucloxacillin 2 g, thiopental 50 mg, fentanyl 0.80 mg, pancuronium 9 rag, halothane
diazepam 10 mg, gentamicin 128 rag, fludoxacillin 2 g, thiopental 75 mg, fentanyl I mg, metaraminol 1 mg, pancuronium 9 rag, halothane
diazepam 10 mg, gentamicin 180 mg,, flucloxacillin 1.20 mg, fentanyl 1.20 mg, pancuronium 10 mg,metaraminol 0.5 mg, thiopental 75 mg, halothane
diazepam 5 mg, fentanyl 5.00 mg, pancuronium 2 mg, vecuronium 8 mg, flucloxacillin 2 g, gentamicin 160 mg, metaraminol 0.5 mg
diazepam 8 mg, fentanyl 1.00 rag, thiopental 100 mg, pancu- ronium 9 mg, gentamicin 120 mg, dopamine 0.20 mg/min, halothane
Tofal lug/))
Unbound lug/ l )
Unbound Fraction
200~
100~=i 0 t , I • ,
30
10
0 0.4
°2 f ~ - 0 0 6=0
i i
Z
i 120 180
Time (min)
Fig. 1. Total and unbound plasma concentrations and unbound fraction of alfentanil in Patient 5 during con- tinuous infusion of alfentanil. The horizontal arrows in- dicate the times of onset and cessation of bypass
50 IC Knmar et al.: Cardiopulmonary Bypass and Alfentanit Plasma Binding
Table 3. Plasma drug and protein concentrations and unbound drug fraction before and during CPB (mean_+ SD)
Total Unbound Unbound Albumin A A G (gg- 1- t) (gg- 1- ~) fi'action (g. 1-1) (g- 1-1)
Pre-CPB 177.0 + 44 29.2 _+ 12 0.16 + 0.04 35.5 _+ 4.1 0.93 + 0.35 2 rain CPB 92.3 + 29 a 34.7 + 20 0.35 + 0.08b 21.0 --+ 5.2 0.42_+ 0.11 a End CPB 155.0 + 82 31.3 + 13 0.22 + 0.05 23.7 +__ 4.6 0.49 _+ 0.16 a
a Significantly less than before bypass value (p< 0.05); b Significantly less than before bypass and end of bypass value (p < 0.05)
B/F (a) B/F
• m
°1o ' 2o 3o 4o
Plasma Albumin Concn. ( g / l )
8
(b)
6
4
2
o
P[asmo
• OQ • •0
dm
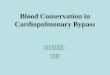
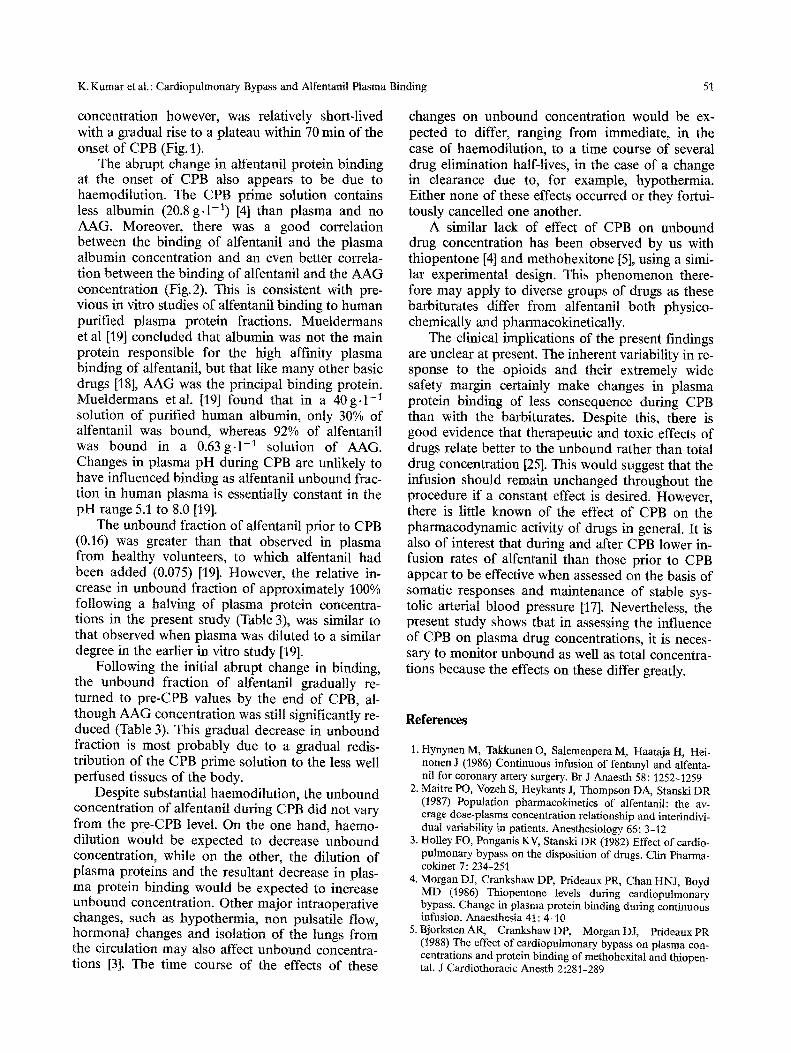
• • fentanil binding ratio and plasma albumin (a) and A A G (b) con-
, , , ~ , , , , , , , ~ . . . . c e n t r a t i o n s b e f o r e ( e ) , 2 m i n a f t e r 0,4 o,8 1.2 1.6 commencement (A) and at the
AAG C o n c n . ( g / I ) end ( , ) o f bypass
bound alfentanil concentration showed little change with the onset of CPB. When these data are com- bined as the unbound fraction of alfentanil, an abrupt rise is seen at the onset of CPB (Fig. 1).
Alfentanil concentration data for the five pat- ients are summarized in Table 3. At the onset of CPB, the mean total alfentanil concentration de- creased by half and the mean unbound fraction doubled. Later, at the end of CPB the mean total concentration had increased and unbound fraction decreased, each to an intermediate value between the pre- and 2 min post-CPB extremes (Table 3). The mean unbound concentration did not change significantly throughout the sampling period.
Mean plasma albumin and AAG concentrations are also shown in Table 3. CPB caused a significant reduction in the concentration of each of these pro- teins to about 50% of the pre-CPB value, presum- ably due to dilution of the circulation by the pump priming solution. There was a moderate correlation between the binding ratio of alfentanil (ratio of plasma bound concentration/plasma unbound con- centration [22]) and the plasma albumin concentra- tion (r= 0.57, p< 0.02) but a much stronger correla- tion between binding ratio (B/F) and plasma AAG concentration (r= 0.80, p < 0.001, Fig. 2).
Discussion
The bolus and fixed rate infusion technique used in this study permitted the rapid achievement of stable pre-CPB total and unbound concentrations. The
Fig. 2a, b. Correlation between al-
rapid achievement of stable plasma concentrations enabled a relatively precise determination of the magnitude and time-course of the change in plasma protein binding of alfentanil at the onset of CPB, without the uncertainties inherent in rising or falling concentrations.
The infusion established a relatively stable total plasma alfentanil level of 177 + 44 gg. 1-1 at the end of the pre-CPB period. This pre-CPB level is con- sistent with that predicted from single dose pharma- cokinetics for patients of this age [2]. Based on a plasma alfentanil clearance for a 64 year old of 290 ml.min -1 [2] and a mean infusion rate of 59~tg.min -1, the total alfentanil plasma level would be expected to eventually reach a steady state-level of approximately 186 gg-1-1 if physiol- ogical conditions remained unchanged.
Despite the continuation of the infusion at a fixed rate, the total plasma concentration of alfen- tanil fell to approximately 60% of the pre-CPB level within 2 rain of the onset of CPB (Table 3). This is consistent with changes in total concentration ob- served previously during CPB, albeit under condi- tions when the alfentanil concentration prior to CPB was changing more than in the present study [17]. Loss of alfentanil by sequestration in the ex- tracorporeal circuit as a possible explanation for the decrease in alfentanil concentration has previously been excluded [24]. The fall was undoubtedly the re- sult of a dilutional effect consequent on the addi- tion of a large amount of drug-free fluid into the cir- culating volume of the patient. This effect on total
K. Kumar et al.: Cardiopulmonary Bypass and Atfentanil Plasma Binding 51
concentration however, was relatively short-lived with a gradual rise to a plateau within 70 rain of the onset of CPB (Fig. 1).
The abrupt change in alfentanil protein binding at the onset of CPB also appears to be due to haemodilution. The CPB prime solution contains less albumin (20.8 g.1-1) [4] than plasma and no AAG. Moreover, there was a good correlation between the binding of alfentanil and the plasma albumin concentration and an even better correla- tion between the binding of alfentanil and the AAG concentration (Fig.2). This is consistent with pre- vious in vitro studies of alfentanil binding to human purified plasma protein fractions. Mueldermans et al [19] concluded that albumin was not the main protein responsible for the high affinity plasma binding of alfentanil, but that like many other basic drugs [18], AAG was the principal binding protein. Mueldermans etal. [19] found that in a 40g.1 - t solution of purified human albumin, only 30% of alfentanil was bound, whereas 92% of alfentanil was bound in a 0.63g.1-1 solution of AAG. Changes in plasma pH during CPB are unlikely to have influenced binding as alfentanil unbound frac- tion in human plasma is essentially constant in the pH range 5.1 to 8.0 [19].
The unbound fraction of alfentanil prior to CPB (0.16) was greater than that observed in plasma from healthy volunteers, to which alfentanil had been added (0.075) [19]. However, the relative in- crease in unbound fraction of approximately 100% following a halving of plasma protein concentra- tions in the present study (Table 3), was similar to that observed when plasma was diluted to a similar degree in the earlier in vitro study [19].
Following the initial abrupt change in binding, the unbound fraction of alfentanil gradually re- turned to pre-CPB values by the end of CPB, al- though AAG concentration was still significantly re- duced (Table 3). This gradual decrease in unbound fraction is most probably due to a gradual redis- tribution of the CPB prime solution to the less well perfused tissues of the body.
Despite substantial haemodilution, the unbound concentration of alfentanil during CPB did not vary from the pre-CPB level. On the one hand, haemo- dilution would be expected to decrease unbound concentration, while on the other, the dilution of plasma proteins and the resultant decrease in plas- ma protein binding would be expected to increase unbound concentration. Other major intraoperative changes, such as hypotherrnia, non pulsatile flow, hormonal changes and isolation of the lungs from the circulation may also affect unbound concentra- tions [3]. The time course of the effects of these
changes on unbound concentration would be ex- pected to differ, ranging from immediate, in the case of haemodilution, to a time course of several drug elimination half-lives, in the case of a change in clearance due to, for example, hypothermia. Either none of these effects occurred or they fortui- tously cancelled one another.
A similar lack of effect of CPB on unbound drug concentration has been observed by us with thiopentone [4] and methohexitone [5], using a simi- lar experimental design. This phenomenon there- fore may apply to diverse groups of drugs as these barbiturates differ from alfentanil both physico- chemically and pharmacokinetically.
The clinical implications of the present findings are unclear at present. The inherent variability in re- sponse to the opioids and their extremely wide safety margin certainly make changes in plasma protein binding of less consequence during CPB than with the barbiturates. Despite this, there is good evidence that therapeutic and toxic effects of drugs relate better to the unbound rather than total drug concentration [25]. This would suggest that the infusion should remain unchanged throughout the procedure if a constant effect is desired. However, there is little known of the effect of CPB on the pharmacodynamic activity of drugs in general. It is also of interest that during and after CPB lower in- fusion rates of alfentanil than those prior to CPB appear to be effective when assessed on the basis of somatic responses and maintenance of stable sys- tolic arterial blood pressure [17]. Nevertheless, the present study shows that in assessing the influence of CPB on plasma drug concentrations, it is neces- sary to monitor unbound as well as total concentra- tions because the effects on these differ greatly.
References
1. Hynynen M, Takkunen O, Salemenpera M, Haataja H, Hei- nonen J (1986) Continuous infusion of fentanyl and alfenta- nil for coronary artery surgery. Br J Anaesth 58:1252-1259
2. Maitre PO, Vozeh S, Heykants J, Thompson DA, Stanski DR (1987) Population pharmacokinetics of alfentanil: the av- erage dose-plasma concentration relationship and interindivi- dual variability in patients. Anesthesiology 66:3-12
3. Holley FO, Ponganis KV, Stanski DR (1982) Effect of cardio- pulmonary bypass on the disposition of drugs. Clin Pharma- cokinet 7:234-251
4. Morgan D J, Crankshaw DP, Prideaux PR, Chan HNJ, Boyd MD (1986) Thiopentone levels during cardiopulmonary bypass. Change in plasma protein binding during continuous infusion. Anaesthesia 41:4-I0
5. Bjorksten AR, Crankshaw DP, Morgan D J, lMdeaux PR (t988) The effect of cardiopulmonary bypass on plasma con- centrations and protein binding of methohexital and thiopen- tal. J Cardiothoracic Anesth 2:281-289

52 K. Kumar et al.: Cardiopulmonary Bypass and Alfentanil Plasma Binding
6. Shanks CA, Ramzan IM, WalkerJS, Brown KF (1983) Gal- lamine disposition in open-heart surgery involving cardiopul- monary bypass. Clin Pharmacol Ther 33:792-799
7. Walker JS, Brown KF, Shanks CA (1983) Alcuronium kinet- ics in patients undergoing cardiopulmonary bypass surgery. Br J Clin Pharmacol 15:237-244
8. Miller KW, Chan KKH, McCoy HG, Fischer RP, Lind- say WD, ZaskeDE (1979) Cephalothin kinetics: Before, during and after cardiopulmonary bypass surgery. Clin Phar- macol Ther 26:54-62
9. Walker JS, Shanks CA, Brown KF (1984) Altered d-tubocura- rine disposition during cardiopulmonary bypass surgery. Clin Pharmacol Ther 35:686-694
10. d'Hollander AA, Dnvaldestin P, Henzel D, Nevelsteen M, BombletJP (1983) Variations in pancuronium requirement, plasma concentration, and urinary excretion induced by car- diopulmonary bypass with "hypothermia. Anesthesiology 58: 505-509
l l . PlachetkaJR, SalomonNW, CopelandJG (1981) Plasma propranolol before, during and after cardiopulmonary bypass. Clin Pharmacot Ther 30:745-751
12. Storstein L, Nitter-Hauge S, Field N (1979) Effect of cardio- pulmonary bypass with heparin administration on digitoxin pharmacokinetics, serum electrolytes, free fatty acids, and renal function. J Cardiovasc Pharmacol 1 : 191-204
13. Miller KW, McCoy HG, Chan KKH, Fischer RP, Lind- say WG, Seifert RD, Zaske DE (1980) Effect of cardiopulmo- nary bypass on cefazolin disposition. Clin Pharmacol Ther 27:550-556
t4. Koren G, Goresky G, Crean P, Klein J, MacLeod SM (1984) Pediatric fentanyl dosing based on pharmacokinetics during cardiac surgery. Anesth Analg 63:577-582
15. Sprigge JS, Wynands JE, Whalley DG, Bevan DR, Town- send GE, Nathan H, PatelYC, SrikantCB (1982) Fentanyl infusion anesthesia for aortocoronary bypass surgery: Plasma levels and haemodynamic response. Anesth Analg 61: 972-978
16. Hug CC, deLange S, Burro AGL (1983) Alfentanil pharmaco- kinetics in patients before and after cardiopulmonary bypass. Anesth Anatg 62:266
17. deLange S, deBruijn NP (1983) Alfentanil-oxygen anaesthe- sia: Plasma concentrations and clinical effects during vari- able rate-continuous infusion for coronary' artery surgery. Br J Anaesth 55:183 S-189 S
18. Wood M (1986) Plasma drug binding: Implications for anes- thesiologists. Anesth Analg 65:786-804
19. Mueldermans WEG, Hurkmans RMA, Heykants JJP (1982) Plasma protein binding and_distribution of fentanyl, sufenta- nil, alfentanil and lofentanil in blood. Arch Int Pharmacodyn 257:4-19
20. Crankshaw DP, Boyd MD, Bjorksten AR (1987) Plasma drug efflux: A new approach to optimization of drug infusion for constant blood concentration of thiopental and methohexital. Anesthesiology 67:32-41
21. Kumar K, Morgan D J, Crankshaw DP (1987) Determination of fentanyl and alfentanil in plasma by high-performance liquid chromatography with ultraviolet detection. J Chroma- tography 419:464-468
22. Nilsen OG, Leren P, Aakesson I, Jacobsen S (1978) Binding of quindine in sera with different levels of triglycerides, cho- lesterol and orosomucoid protein. Biochem Pharmacol 27: 871-876
23. Miller RG (1981) Simultaneous statistical inference. Springer, New York
24. Skacel M, Knott C, Reynolds F, Aps C (1986) Extracorporeal circuit sequestration of fentanyl and alfentanil. Br J Anaesth 58:947-949
25. SvenssonCK, WoodruffMN, BaxterJG, LalkaD (1986) Free drug concentration monitoring in clinical practice. Rationale and current status. Clin Pharmacokinet: 450-469
Received: March 3, 1988 accepted: March 31, 1988
Dr. D.J. Morgan Victorian College of Pharmacy 38l Royal Parade, Parkville, Victoria 3052 Australia