Embed Size (px)
Citation preview
THE EFFECT OF P H AND OSMOLARITY ON THE ABILITY TO TOLERATE ARTIFICIAL TEARS
MICHAEL MOTOLKO, M.D., AND CALVIN W. BRESLIN, M.D. Toronto, Canada
Many patients with keratitis sicca complain that the commercially available artificial tears burn when they are instilled and fail to relieve their distressing symptoms. We examined the effects of altering both the pH and osmolarity of a hydroxypropyl methylcellulose tear substitute on the tolerance of 15 patients with varying degrees of keratitis sicca. Approximately equal numbers of patients selected the neutral hypotonie tear preparations and the isotonic or near-isotonic alkaline tear substitutes. The isotonic alkaline tear preparation was preferred by the majority of our patients with moderate or severe dry eyes. A commercially available alkaline tear substitute is needed.
Keratoconjunctivitis sicca is one of the more common distressing clinical problems facing the ophthalmologist. The symptoms range from mild ocular irritation to severe, disabling ocular pain and visual loss from corneal damage. Although artificial tears are the main therapy for the dry eye, many patients complain that the commercially available tear substitutes burn when instilled and fail to provide relief for their discomfort.
In an effort to provide our patients with a more comfortable artificial tear, we set out to determine empirically what features of an artificial tear were important for improved tolerance by the patient. Having confirmed that an alkaline tear substitute was preferred by the majority of our patients with keratitis sicca,1 we then examined the effects of varying both the pH and osmolarity of a hydroxypropyl methylcellulose tear substitute.
From the Department of Ophthalmology, University of Toronto, and the Toronto Western Hospital, Toronto, Canada.
Reprint requests to Calvin W. Breslin, M.D., 3101 Bloor St. West, Suite 311, Toronto, Ontario, M8X 2W2 Canada.
SUBJECTS AND METHODS
During an 18-month period, we studied 15 patients (three men and 12 women, ranging in age from 27 to 76 years) with keratitis sicca. All had moderate to severe symptoms of burning, foreign-body sensation, photophobia, or dryness associated with rose bengal staining of the cornea and conjunctiva, diminished height of the precorneal tear film meniscus (less than 0.5 mm), and less than 10 mm of wetting by Schirmer strip testing.
We asked each subject to grade the symptoms of burning, foreign-body sensation, dryness, itching, photophobia, tearing, blurred vision and tired eyes as absent, mild, moderate, or severe. Con-junctival injection, conjunctival chemo-sis, and rose bengal staining of the cornea, conjunctiva, or both were graded in a similar fashion. The height of the precorneal tear film meniscus was measured with the variable slit of a slit lamp.
All ocular therapy was discontinued 24 hours before the patient entered the study. The trial was divided into three parts and conducted in a randomized, double-masked, cross-over fashion.
AMERICAN JOURNAL OF OPHTHALMOLOGY 91:781-784, 1981 781
782 AMERICAN JOURNAL OF OPHTHALMOLOGY JUNE, 1981
The test solutions were a hydroxypro-pyl methylcellulose tear substitute with a borax-boric acid buffer system.
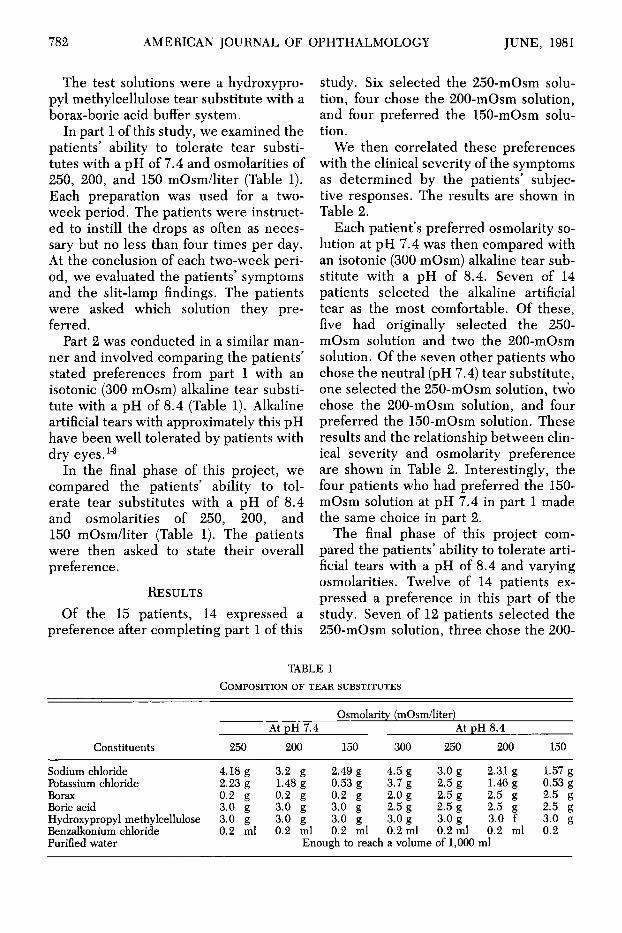
In part 1 of this study, we examined the patients' ability to tolerate tear substitutes with a pH of 7.4 and osmolarities of 250, 200, and 150 mOsm/liter (Table 1). Each preparation was used for a two-week period. The patients were instructed to instill the drops as often as necessary but no less than four times per day. At the conclusion of each two-week period, we evaluated the patients' symptoms and the slit-lamp findings. The patients were asked which solution they preferred.
Part 2 was conducted in a similar manner and involved comparing the patients' stated preferences from part 1 with an isotonic (300 mOsm) alkaline tear substitute with a pH of 8.4 (Table 1). Alkaline artificial tears with approximately this pH have been well tolerated by patients with dry eyes.1"3
In the final phase of this project, we compared the patients' ability to tolerate tear substitutes with a pH of 8.4 and osmolarities of 250, 200, and 150 mOsm/liter (Table 1). The patients were then asked to state their overall preference.
R E S U L T S
Of the 15 patients, 14 expressed a preference after completing part 1 of this
study. Six selected the 250-mOsm solution, four chose the 200-mOsm solution, and four preferred the 150-mOsm solution.
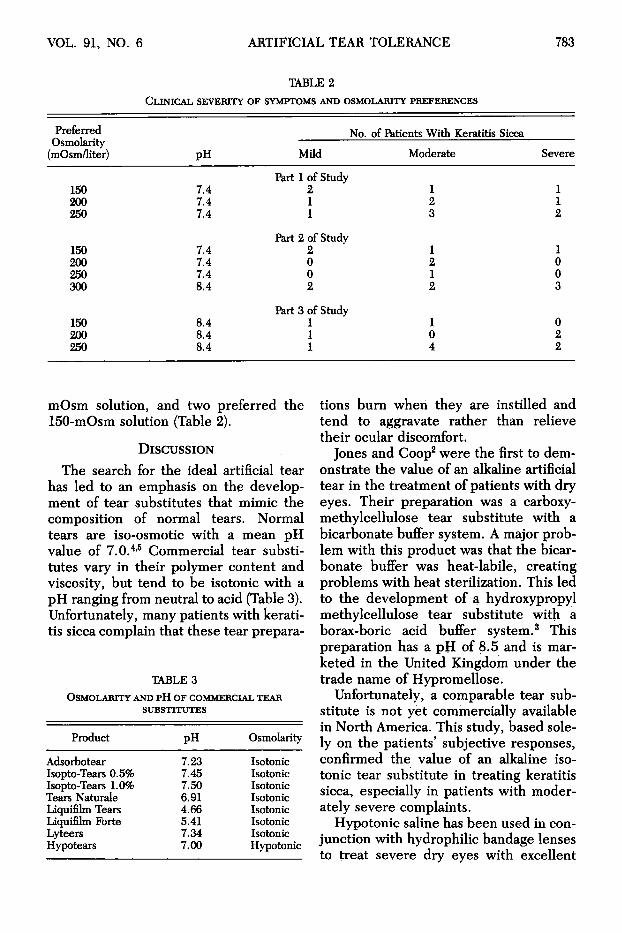
We then correlated these preferences with the clinical severity of the symptoms as determined by the patients' subjective responses. The results are shown in Table 2.
Each patient's preferred osmolarity solution at pH 7.4 was then compared with an isotonic (300 mOsm) alkaline tear substitute with a pH of 8.4. Seven of 14 patients selected the alkaline artificial tear as the most comfortable. Of these, five had originally selected the 250-mOsm solution and two the 200-mOsm solution. Of the seven other patients who chose the neutral (pH 7.4) tear substitute, one selected the 250-mOsm solution, two chose the 200-mOsm solution, and four preferred the 150-mOsm solution. These results and the relationship between clinical severity and osmolarity preference are shown in Table 2. Interestingly, the four patients who had preferred the 150-mOsm solution at pH 7.4 in part 1 made the same choice in part 2.
The final phase of this project compared the patients' ability to tolerate artificial tears with a pH of 8.4 and varying osmolarities. Twelve of 14 patients expressed a preference in this part of the study. Seven of 12 patients selected the 250-mOsm solution, three chose the 200-
Constituents
Sodium chloride Potassium chloride Borax Boric acid Hydroxypropyl methylcellulose Benzalkonium chloride Purified water
TABLE 1 COMPOSITION OF TEAR SUBSTITUTES
250
4.18 g 2.23 g 0.2 g 3.0 g 3.0 g 0.2 ml
At pH 7.4 200
3.2 g 1.48 g 0.2 g 3.0 g 3.0 g 0.2 ml
Eno
Osmolarity (mOsm/liter) At pH 8.4
150 300 250 200
2.49 g 4.5 g 3.0 g 2.31 g 0.53 g 3.7 g 2.5 g 1.46 g 0.2 g 2.0 g 2.5 g 2.5 g 3.0 g 2.5 g 2.5 g 2.5 g 3.0 g 3.0 g 3.0 g 3.0 f 0.2 ml 0.2 ml 0.2 ml 0.2 ml
ugh to reach a volume of 1,000 ml
150
1.57 g 0.53 g 2.5 g 2.5 g 3.0 g 0.2
VOL. 91, NO. 6 ARTIFICIAL TEAR TOLERANCE 783
TABLE 2 CLINICAL SEVERITY OF SYMPTOMS AND OSMOLARITY PREFERENCES
Preferred Osmolarity
(mOsm/liter)
150 200 250
150 200 250 300
150 200 250
PH
7.4 7.4 7.4
7.4 7.4 7.4 8.4
8.4 8.4 8.4
No.
Mild
Part 1 of Study 2 1 1
Part 2 of Study 2 0 0 2
Part 3 of Study 1 1 1
of Patients With Keratitis Sicca
Moderate
1 2 3
1 2 1 2
1 0 4
Severe
1 1 2
1 0 0 3
0 2 2
mOsm solution, and two preferred the 150-mOsm solution (Table 2).
DISCUSSION
The search for the ideal artificial tear has led to an emphasis on the development of tear substitutes that mimic the composition of normal tears. Normal tears are iso-osmotic with a mean pH value of 7.0.4,5 Commercial tear substitutes vary in their polymer content and viscosity, but tend to be isotonic with a pH ranging from neutral to acid (Table 3). Unfortunately, many patients with keratitis sicca complain that these tear prepara-
TABLE3 OSMOLARITY AND P H OF COMMERCIAL TEAR
SUBSTITUTES
Product
Adsorbotear Isopto-Tears 0.5% Isopto-Tears 1.0% Tears Naturale Liquifilm Tears Liquifilm Forte Lyteers Hypotears
PH
7.23 7.45 7.50 6.91 4.66 5.41 7.34 7.00
Osmolarity
Isotonic Isotonic Isotonic Isotonic Isotonic Isotonic Isotonic Hypotonie
tions burn when they are instilled and tend to aggravate rather than relieve their ocular discomfort.
Jones and Coop2 were the first to demonstrate the value of an alkaline artificial tear in the treatment of patients with dry eyes. Their preparation was a carboxy-methylcellulose tear substitute with a bicarbonate buffer system. A major problem with this product was that the bicarbonate buffer was heat-labile, creating problems with heat sterilization. This led to the development of a hydroxypropyl methylcellulose tear substitute with a borax-boric acid buffer system.3 This preparation has a pH of 8.5 and is marketed in the United Kingdom under the trade name of Hypromellose.
Unfortunately, a comparable tear substitute is not yet commercially available in North America. This study, based solely on the patients' subjective responses, confirmed the value of an alkaline isotonic tear substitute in treating keratitis sicca, especially in patients with moderately severe complaints.
Hypotonie saline has been used in conjunction with hydrophilic bandage lenses to treat severe dry eyes with excellent
784 AMERICAN JOURNAL OF OPHTHALMOLOGY JUNE, 1981
results.6 We have also successfully used half-normal saline solutions to control the symptoms of dry eye in our patients who wear cosmetic hydrogel contact lenses.
One possible explanation of the success of hypotonie saline in these situations is that patients with keratitis sicca have hypertonic tears.7 Furthermore, Gilbard and Farris8 found that four of five patients with severe keratitis sicca preferred a half-normal saline tear substitute to an isotonic neutral tear substitute.8
Our results supported the view that a hypotonie tear substitute is a valuable therapeutic alternative in treating dry eyes. The majority of our patients with moderately severe dry eyes, however, preferred the isotonic or near-isotonic alkaline tear substitute to the half-normal saline, pH-neutral artificial tear. Part of this difference may be explained by the different methods used to determine clinical severity. In our series, clinical severity was determined by the patients' subjective responses rather than by rose bengal staining of the cornea and conjunctiva. We have found that objective slit-lamp findings correlate poorly with the severity of the patients' complaints.
It is clear that no one tear preparation is consistently better tolerated. The preferences of the patients may change, prob
ably reflecting the fluctuating nature of keratoconjunctivitis sicca. We have, however, demonstrated the value of a hypo-tonic neutral artificial tear and an isotonic alkaline tear substitute in treating patients with dry eyes. The isotonic alkaline tear substitute is especially valuable in those patients with moderately severe disease. A hypotonie tear substitute is now commercially available, and there is a need for an isotonic alkaline tear substitute as well.
REFERENCES 1. Raber, I., and Breslin, C. W.: Toleration of
artificial tears. The effect of pH. Can. J. Ophthalmol. 13:247, 1978.
2. Jones, B. R., and Coop, H. V.: The management of keratoconjunctivitis sicca. Trans. Ophthalmol. Soc. U.K. 85:379, 1965.
3. Wright, P.: Diagnosis and treatment of dry eyes. Trans. Ophthalmol. Soc. U.K. 91:119, 1971.
4. Carney, L. G., and Hill, R. M.: Human tear pH. Diurnal variations. Arch. Ophthalmol. 94:821, 1976.
5. Abelson, M. B., Udell, I. J., and Weston, J. H.: Normal human tear pH by direct measurement. Arch. Ophthalmol. 99:301, 1981.
6. Gasset, A. R., and Kaufman, H. E.: Hydro-philic lens therapy of severe keratoconjunctivitis sicca and'eonjunctival scarring. Am. J. Ophthalmol. 61:1185, 1971.
7. Gilbard, J. P., Earris, R. L., and Santamaria, J.: Osmolarity of tear microvolumes in keratoconjunctivitis sicca. Arch. Ophthalmol. 96:677, 1978.
8. Gilbard, J. P., and Farris, R. L.: Tear osmolarity and ocular surface disease in keratoconjunctivitis sicca. Arch. Ophthalmol. 97:1642, 1979.