Embed Size (px)
Citation preview
The Effects of Therapy on the Gait of Children with Down Syndrome: A
Systematic Review
By Lucia Botez, Steph Graetz, Colleen McDonald and Maria Notopoulos
Outline• Background
• Methods
• Results
• Article reviews
• Conclusions
• Limitationswww.foietlumiere.org/site/english/001.html
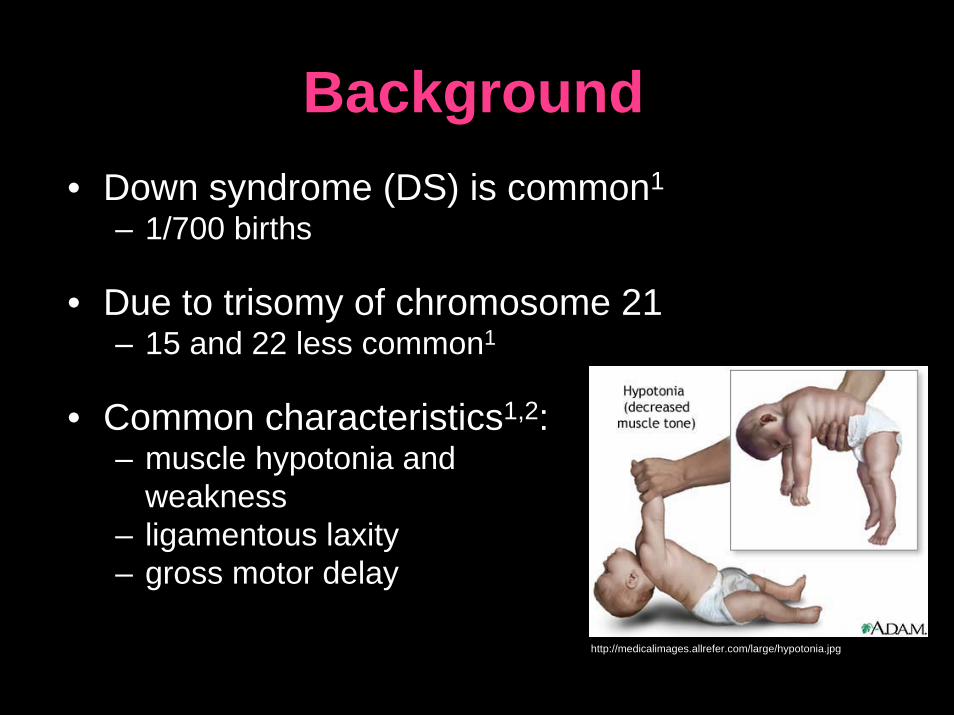
Background• Down syndrome (DS) is common1
– 1/700 births
• Due to trisomy of chromosome 21– 15 and 22 less common1
• Common characteristics1,2:– muscle hypotonia and
weakness– ligamentous laxity– gross motor delay
http://medicalimages.allrefer.com/large/hypotonia.jpg
Background• Walking achieved ~1year later than typically
developing children3,4,5
• Ambulation has psychosocial consequences6,7
• Parents of children with DS identify walking as most valued milestone8
www.cbdsa.com/images/Warrick_xmas06_008.jpg

Courtesy of Naznin-Virji Babul and the Down Syndrome Research Foundation
Background• Common therapy received9
– PT: strength, motor control, function
– OT: visual motor and manipulative skills, community participation
– SLP: oral motor skills, speech
• Therapy usually starts in infancy9
Can physical
therapy effect
the gait of
these children?
http://farm1.static.flickr.com/58/221312636_293942d007.jpg
What’s in the literature?
• Scarce overall
• Many reviews on early intervention and DS – Gibson and Harris 198810
– Nilholm 199611
• Review on motor development and DS– Lautteslager 2006 (Dutch)
www.childrensaustin.org/ama/icache/w300h400/orig/Lily.jpg
Why do this review?• No systematic review on gait and DS
• Literature in this area is unfocused
• Evidence-based practice
• Gait most important gross motor skill9
Objective
“To systematically review and rate the levels of
evidence and methodological quality of studies that
examined the effects of various therapeutic
interventions on the gait of children with DS” www.ndss.org/index.php?option=com_content&ta
sk=view&id=1812&Itemid=95
METHODOLOGY
Gabriel House of Mexico
Search Strategy1. General search in:
– CINAHL– EMBASE– ERIC– MEDLINE– PsychINFO
– PubMed– SPORTDiscus– Cochrane– CENTRAL
Autoalerts: OVID, EBSCO

1. Translocation 15.mp. 2. Translocation 21.mp. 3. Translocation 22.mp. 4. down$ syndrome.mp. 5. mongol$.mp. 6. trisomy.mp. 7. mental retard$.mp. 8. mental$ handicap$.mp. 9. activity.mp. 10. gait.mp. 11. walk$.mp. 12. train$.mp. 13. physical therapy.mp. 14. physiotherapy.mp. 15. exercis$.mp.
16. fitness.mp. 17. treatment.mp. 18. intervention.mp. 19. recreation.mp.20. stair walking.mp.21. physical medicine.mp. 22. exercise therapy.mp. 23. therapeutic exercise.mp. 24. movement.mp. 25. motor intervention.mp. 26. swim$.mp. 27. resistance.mp. heading word]28. climb$.mp. 29. active therapy.mp. 30. locomot$.mp.
31. ambulat$.mp. 32. run$.mp. 33. step$.mp. 34. hydrotherapy.mp. 35. hippotherapy.mp. 36. equinotherapy.mp. 37. pool exercise.mp. 38. aqua therapy.mp. 39. development.mp. 40. participation.mp. 41. impairment.mp. 42. function.mp. 43. functional outcome.mp. 44. motor performance.mp. 45. movement patterns.mp.

46. speed.mp. 47. distance.mp. 48. balance.mp. 49. coordination.mp. 50. gross motor.mp. 51. transfers.mp. 52. stand$.mp. 53. sit$.mp. 54. supine.mp. 55. prone.mp. 56. outcome.mp. 57. rate.mp. 58. physical activit$.mp. 59. rehabil$.mp. 60. strength$.mp.
61. flexib$.mp. 62. manual therapy.mp. 63. electrotherapy.mp. 64. recreation therapy.mp. 65. occupational therapy.mp. 66. active therap$.mp. 67.neurodevelopmentaltherapy.mp. 68. stair climbing.mp. 69. sport$.mp. 70. mobili$.mp. 71. play$.mp. 72. athelet$.mp. 73. taping.mp. 74. splint$.mp. 75. brac$.mp.
76. orthotic$.mp. 77. social$.mp. 78. measure$.mp. 79. velocity.mp. 80. assessment.mp. 81. roll$.mp. 82. posture.mp. 83. anti-gravity movement.mp. 84. independ$.mp. 85. grasp$.mp. 86. reach$.mp. 87. step$.mp. 88. jump$.mp. 89. agility.mp.
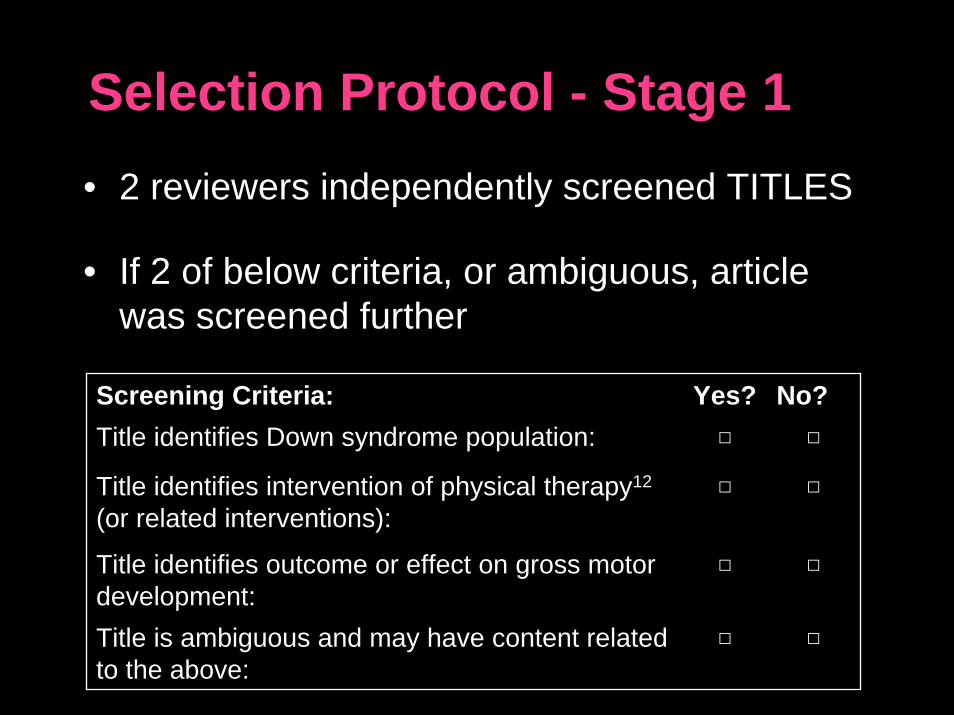
Selection Protocol - Stage 1
Screening Criteria: Yes? No?Title identifies Down syndrome population: □ □
Title identifies intervention of physical therapy12
(or related interventions):□ □
Title identifies outcome or effect on gross motor development:
□ □
Title is ambiguous and may have content related to the above:
□ □
• 2 reviewers independently screened TITLES
• If 2 of below criteria, or ambiguous, article was screened further
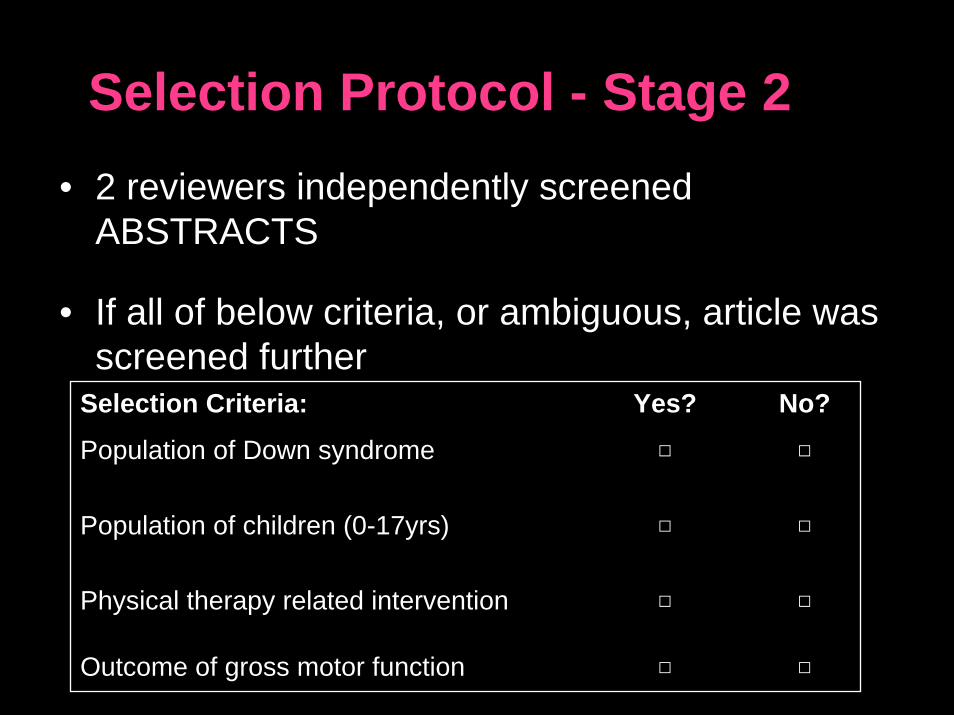
Selection Protocol - Stage 2• 2 reviewers independently screened
ABSTRACTS
• If all of below criteria, or ambiguous, article was screened further
Selection Criteria: Yes? No?
Population of Down syndrome □ □
Population of children (0-17yrs) □ □
Physical therapy related intervention □ □
Outcome of gross motor function □ □
Selection Protocol - Stage 3• FULL TEXT articles divided among
reviewers
• Each reviewer extracted population, intervention and outcome data
• A “PICO chart” was created
ww
w.d
sala
.org
/gra
phic
s/ph
otos
/bab
y_an
gels
-4.jp
g
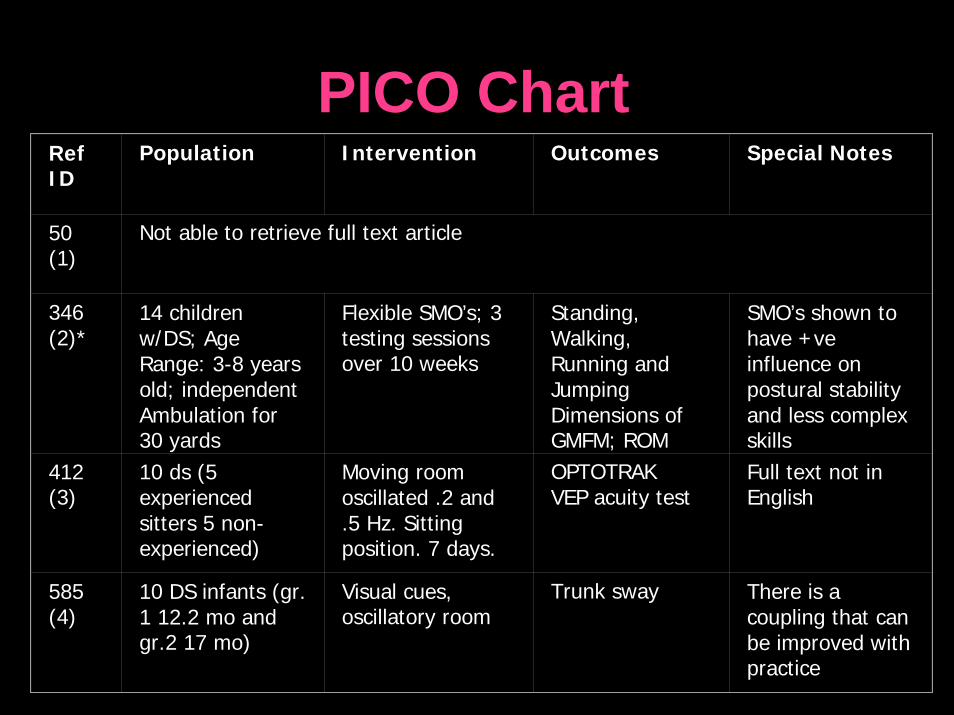
PICO ChartRef ID
Population Intervention Outcomes Special Notes
50 (1)
Not able to retrieve full text article
346(2)*
14 children w/DS; Age Range: 3-8 years old; independent Ambulation for 30 yards
Flexible SMO’s; 3 testing sessions over 10 weeks
Standing, Walking, Running and Jumping Dimensions of GMFM; ROM
SMO’s shown to have +veinfluence on postural stability and less complex skills
412 (3)
10 ds (5 experienced sitters 5 non-experienced)
Moving room oscillated .2 and .5 Hz. Sitting position. 7 days.
OPTOTRAKVEP acuity test
Full text not in English
585 (4)
10 DS infants (gr. 1 12.2 mo and gr.2 17 mo)
Visual cues, oscillatory room
Trunk sway There is a coupling that can be improved with practice
Selection Protocol - Stage 3
• Common trends emerged– Early intervention– Vestibular training– Gait (reciprocal bipedal locomotion)
www.sharethedream.co.nz/images/paris.jpg
Final Inclusion Criteria• Studies
– Peer - reviewed journal, English
• Population– Clinical diagnosis of DS– 0 - 17 years of age
• Intervention– Any physical therapy related intervention
• Outcome– A variable of gait
Excluded: books,
abstracts from
conferences
Excluded: intervention for parents
Search Strategy2. Gait specific search:
a. Down syndromeb. gait OR locomotion OR walking OR walkc. a AND b
3. Hand-search:• Pediatric Physical Therapy• Gait and Posture • Ambulatory Pediatrics• Journal of Pediatric Healthcare • Pediatric Rehabilitation • Pediatric Gait: A New Millenium in Clinical Care
and Motion Analysis Technology
Search Strategy4. Forward citation searches on authors
5. Screened reference lists of included articles and background articles
6. Key authors and clinical experts contacted via e-mail
Search Strategy
• Articles saved in RefWorks– duplicates removed
• Ceased all search methods in June 2007
Gabriel House of Mexico
Methodological Quality• 2 reviewers
independently scored articles using PEDro
• Well known in PT community and valid
http://campos-davis.com/infoweek/infoweek/angelmaria.jpg
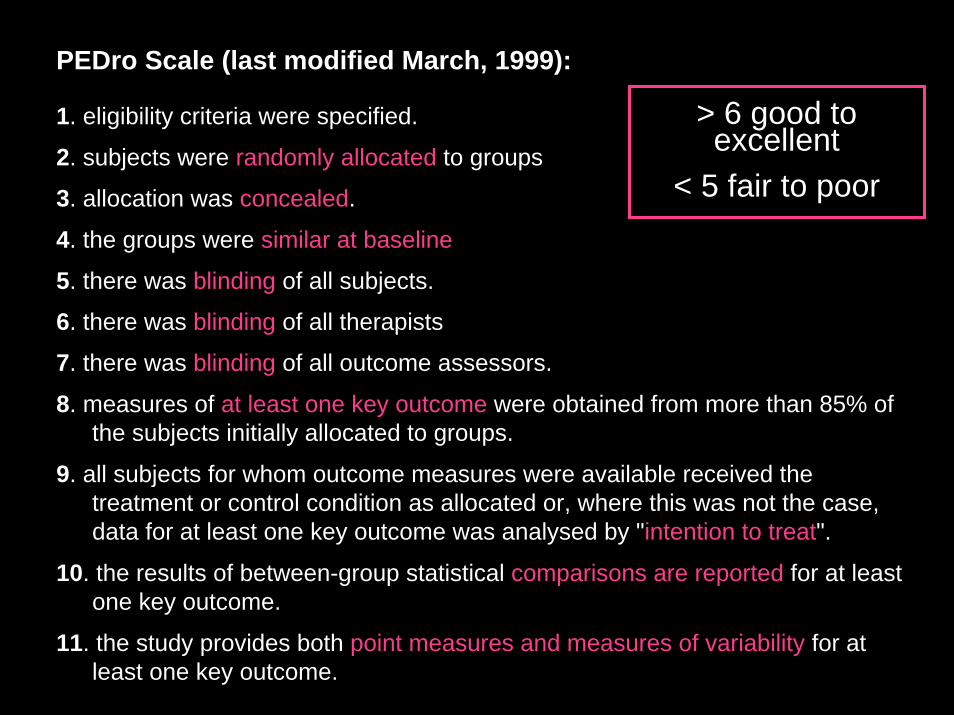
PEDro Scale (last modified March, 1999):
1. eligibility criteria were specified.
2. subjects were randomly allocated to groups
3. allocation was concealed.
4. the groups were similar at baseline
5. there was blinding of all subjects.
6. there was blinding of all therapists
7. there was blinding of all outcome assessors.
8. measures of at least one key outcome were obtained from more than 85% of the subjects initially allocated to groups.
9. all subjects for whom outcome measures were available received the treatment or control condition as allocated or, where this was not the case, data for at least one key outcome was analysed by "intention to treat".
10. the results of between-group statistical comparisons are reported for at least one key outcome.
11. the study provides both point measures and measures of variability for at least one key outcome.
> 6 good to excellent
< 5 fair to poor
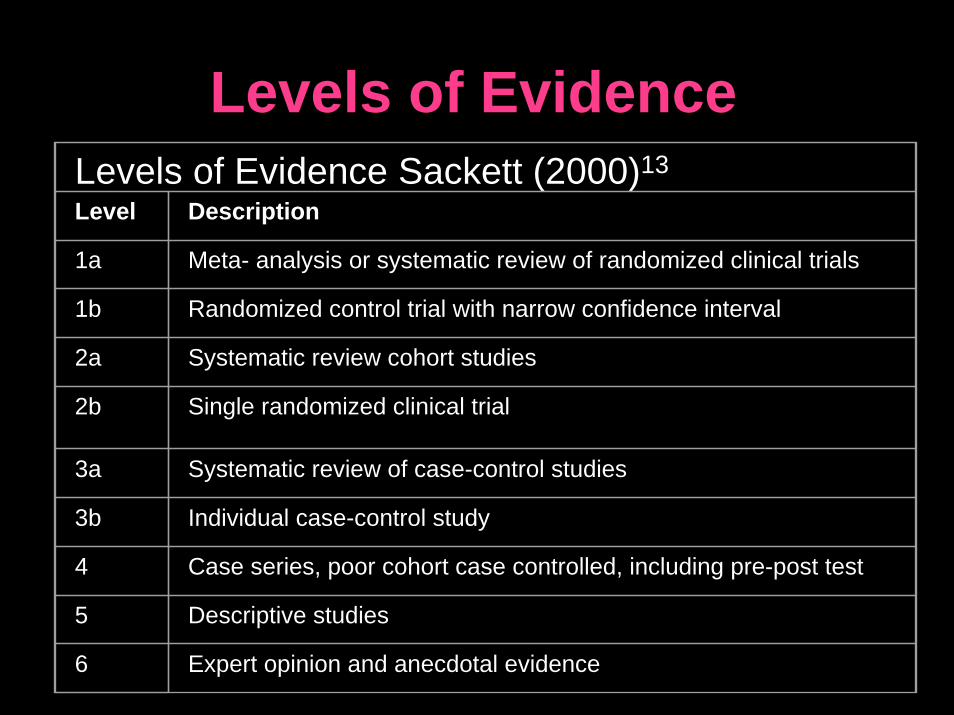
Levels of EvidenceLevels of Evidence Sackett (2000)13
Level Description
1a Meta- analysis or systematic review of randomized clinical trials
1b Randomized control trial with narrow confidence interval
2a Systematic review cohort studies
2b Single randomized clinical trial
3a Systematic review of case-control studies
3b Individual case-control study
4 Case series, poor cohort case controlled, including pre-post test
5 Descriptive studies
6 Expert opinion and anecdotal evidence
Data Extraction
• Data extraction form made for review
• 2 reviewers independently extracted data onto form
Gabriel House of Mexico
Disagreement between reviewers at any of the above stages wasresolved by 3rd party arbitration
Data Analysis• Data extracted into
summary tables– Study characteristics– Outcomes and results
• Calculated Kappa– Stage 1, 2, 3– PEDro– Levels of Evidence
www.cdadc.com/jacobage6learningtoread.jpg
RESULTS
www.babble.com/CS/photos/may2007/images/19911/original.aspx
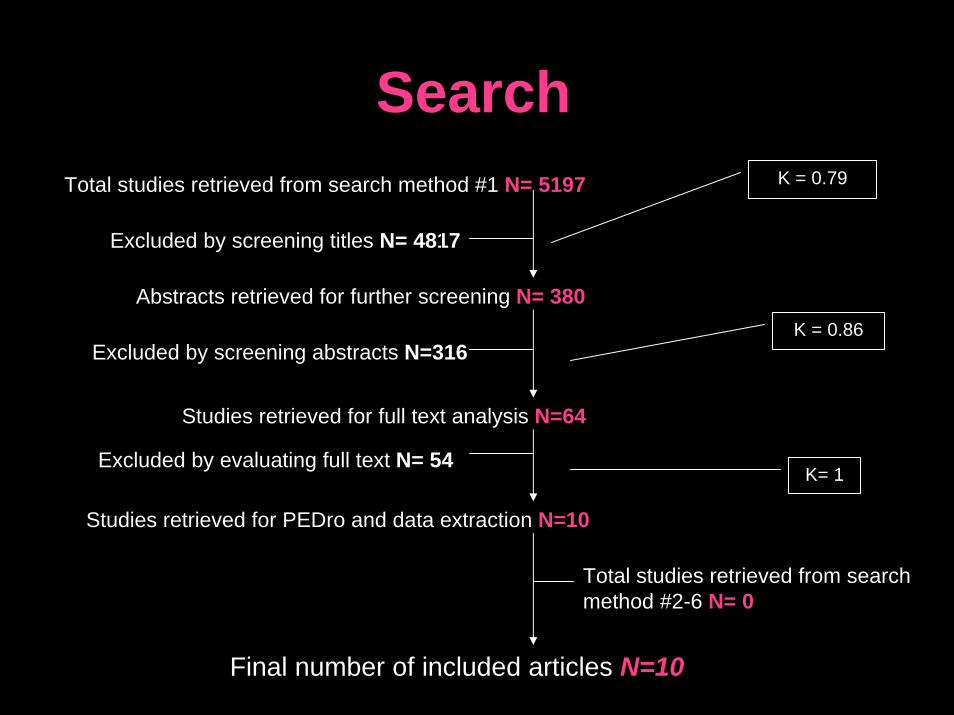
Search
Total studies retrieved from search method #2-6 N= 0
Total studies retrieved from search method #1 N= 5197
Excluded by screening titles N= 4817
Abstracts retrieved for further screening N= 380
Excluded by screening abstracts N=316
Studies retrieved for full text analysis N=64
Excluded by evaluating full text N= 54
Studies retrieved for PEDro and data extraction N=10
Final number of included articles N=10
K = 0.79
K = 0.86
K= 1
Articles• 3 articles on orthoses and 7 on other
interventions
• Total of 181 children with DS were studied
• 8 of 10 studies showed significant or positive results
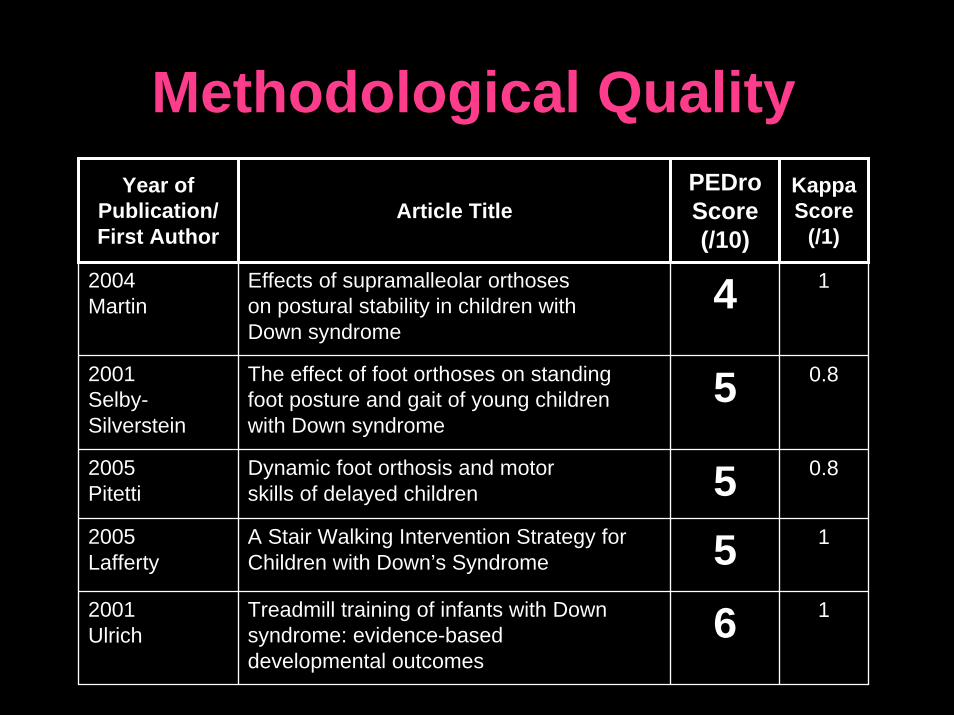
Methodological QualityYear of
Publication/First Author
Article TitlePEDroScore(/10)
KappaScore
(/1)
2004 Martin
Effects of supramalleolar orthoseson postural stability in children withDown syndrome
4 1
2001 Selby-Silverstein
The effect of foot orthoses on standing foot posture and gait of young children with Down syndrome
5 0.8
2005 Pitetti
Dynamic foot orthosis and motorskills of delayed children 5 0.8
2005Lafferty
A Stair Walking Intervention Strategy for Children with Down’s Syndrome 5 1
2001 Ulrich
Treadmill training of infants with Down syndrome: evidence-based developmental outcomes
6 1
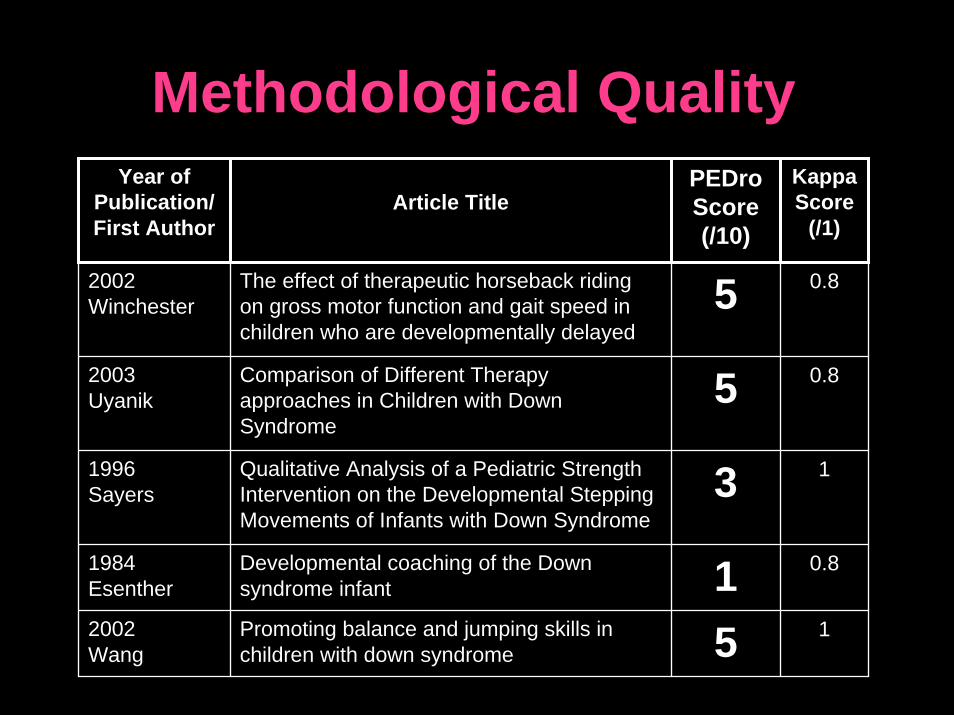
Methodological QualityYear of
Publication/First Author
Article TitlePEDroScore(/10)
KappaScore
(/1)
2002 Winchester
The effect of therapeutic horseback riding on gross motor function and gait speed in children who are developmentally delayed
5 0.8
2003 Uyanik
Comparison of Different Therapyapproaches in Children with DownSyndrome
5 0.8
1996 Sayers
Qualitative Analysis of a Pediatric Strength Intervention on the Developmental Stepping Movements of Infants with Down Syndrome
3 1
1984 Esenther
Developmental coaching of the Down syndrome infant 1 0.8
2002 Wang
Promoting balance and jumping skills in children with down syndrome 5 1
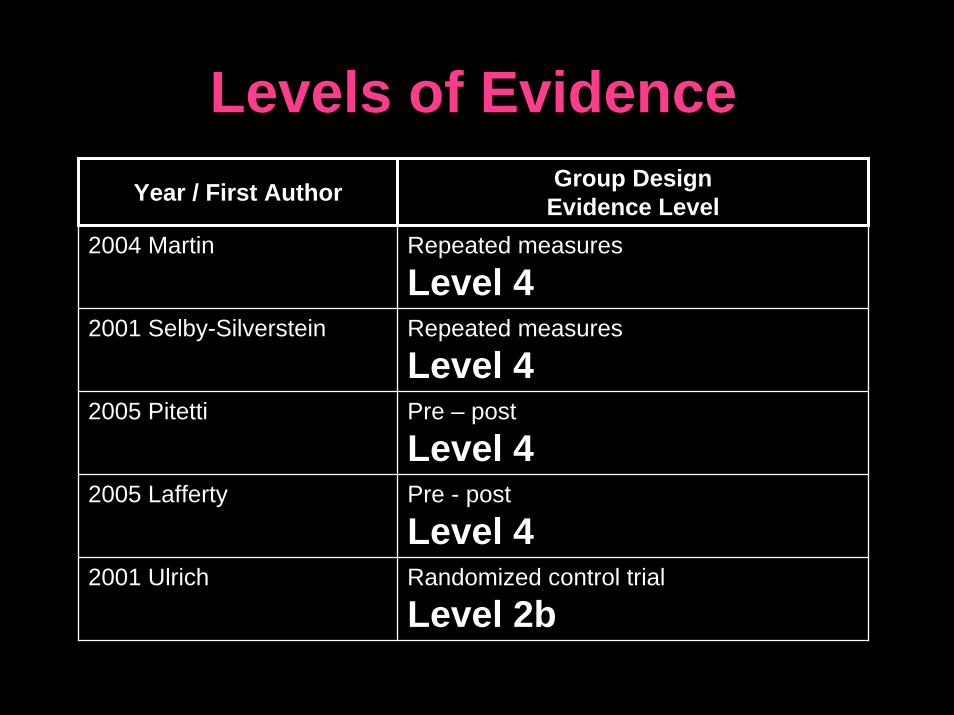
Levels of EvidenceYear / First Author Group Design
Evidence Level2004 Martin Repeated measures
Level 42001 Selby-Silverstein Repeated measures
Level 42005 Pitetti Pre – post
Level 42005 Lafferty Pre - post
Level 42001 Ulrich Randomized control trial
Level 2b
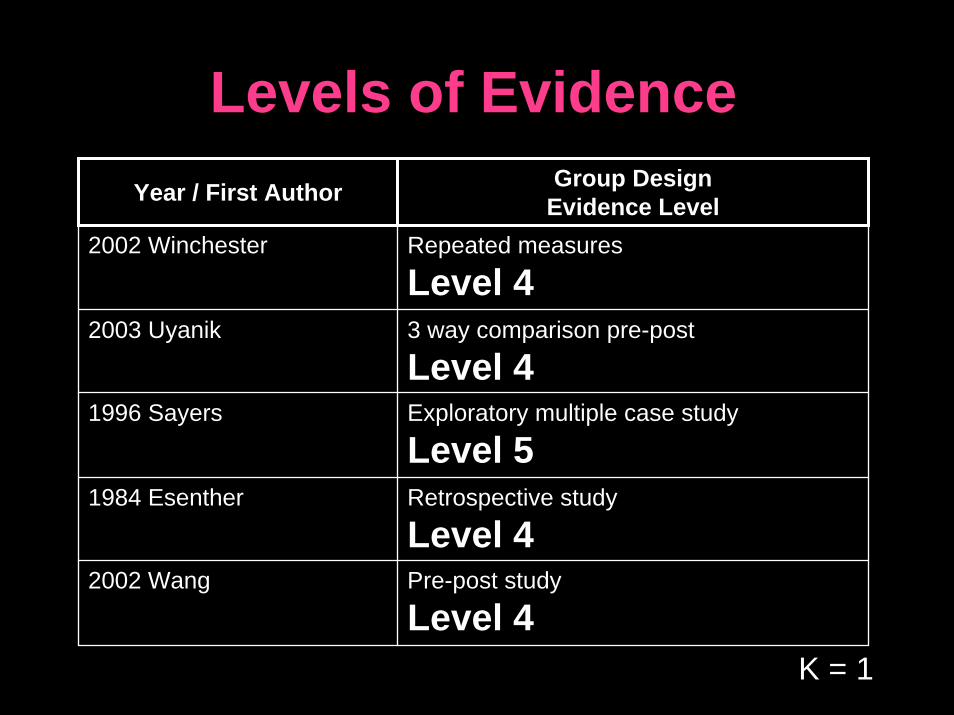
Levels of EvidenceYear / First Author Group Design
Evidence Level2002 Winchester Repeated measures
Level 42003 Uyanik 3 way comparison pre-post
Level 41996 Sayers Exploratory multiple case study
Level 51984 Esenther Retrospective study
Level 42002 Wang Pre-post study
Level 4K = 1

ARTICLE REVIEWS
www.beaumonthospitals.com/images/center/f3c_flowerdoll.jpg
Orthoses
www.footdoc.ca/www.FootDoc.ca/Orthotics.JPEG
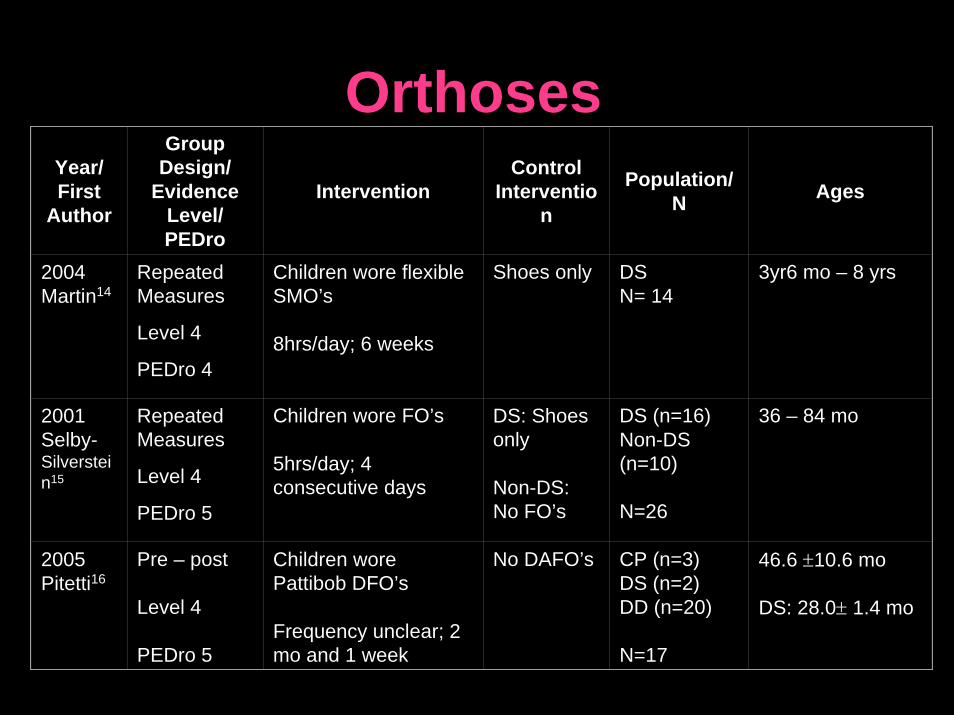
OrthosesYear/First
Author
Group Design/
Evidence Level/PEDro
InterventionControl
Intervention
Population/N Ages
2004 Martin14
Repeated Measures
Level 4
PEDro 4
Children wore flexibleSMO’s
8hrs/day; 6 weeks
Shoes only DSN= 14
3yr6 mo – 8 yrs
2001 Selby-Silverstein15
Repeated Measures
Level 4
PEDro 5
Children wore FO’s
5hrs/day; 4 consecutive days
DS: Shoes only
Non-DS: No FO’s
DS (n=16)Non-DS (n=10)
N=26
36 – 84 mo
2005 Pitetti16
Pre – post
Level 4
PEDro 5
Children wore Pattibob DFO’s
Frequency unclear; 2 mo and 1 week
No DAFO’s CP (n=3) DS (n=2)DD (n=20)
N=17
46.6 ±10.6 mo
DS: 28.0± 1.4 mo
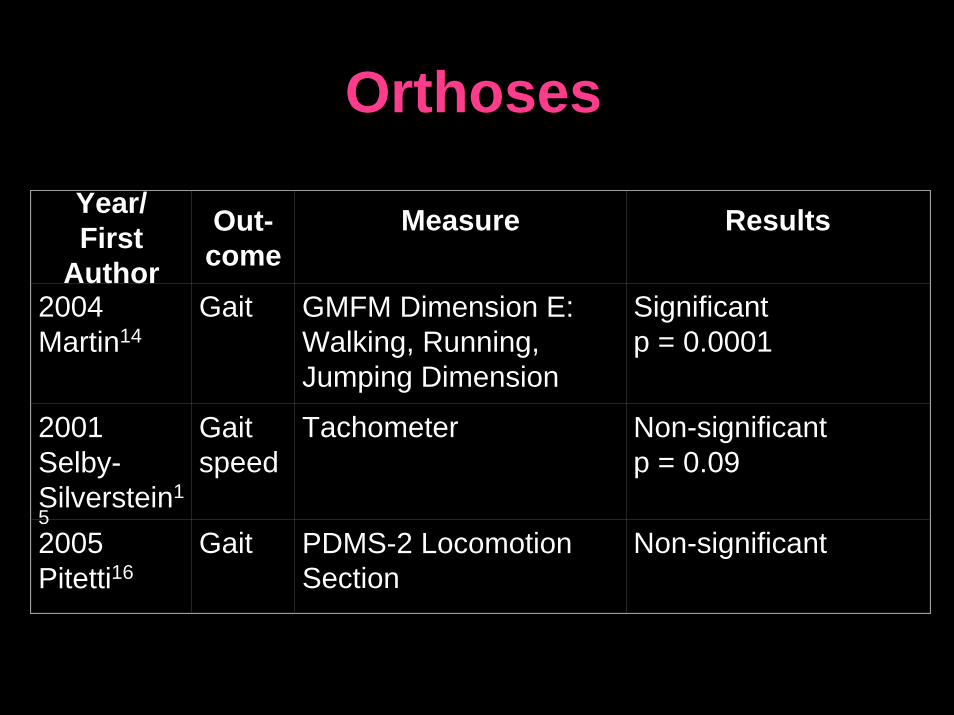
OrthosesYear/First
Author
Out-come
Measure Results
2004 Martin14
Gait GMFM Dimension E: Walking, Running, Jumping Dimension
Significant p = 0.0001
2001 Selby-Silverstein15
Gait speed
Tachometer Non-significantp = 0.09
2005 Pitetti16
Gait PDMS-2 Locomotion Section
Non-significant
Orthoses• Only intervention where multiple
studies were conducted
• Intervention and population varied
• Outcome measures varied
• Small sample sizes
• Only one control group
Orthoses
Clinical recommendation:
Clinicians should evaluate orthosessuitability and effectiveness on a case by case basis
Active Therapy / Stair Walking
www.faqs.org/health/images/uchr_04_img0399.jpg
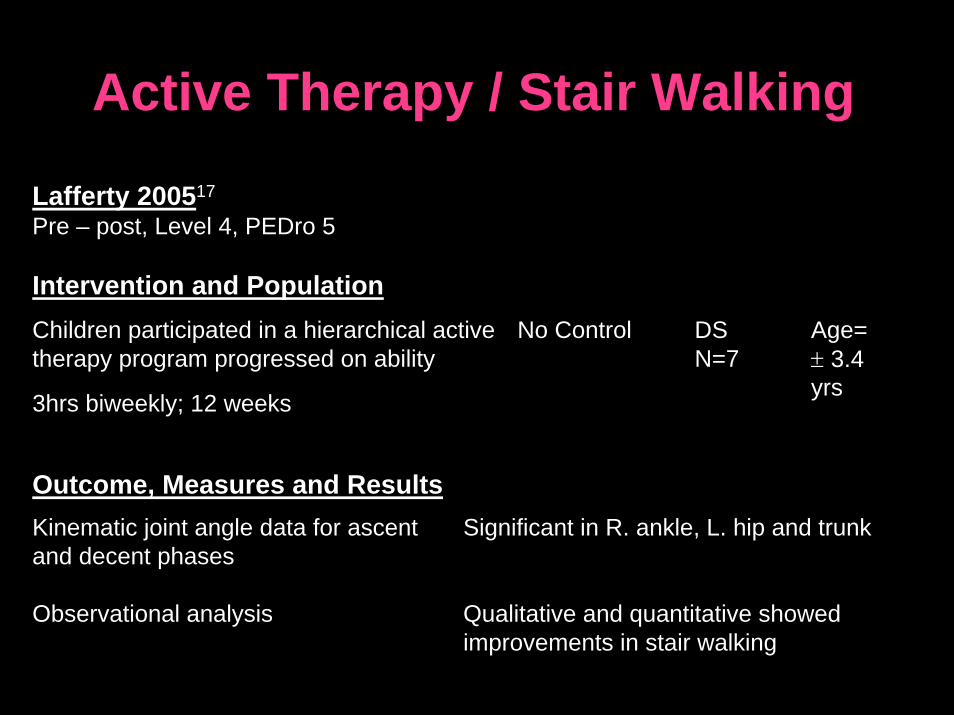
Active Therapy / Stair Walking
Children participated in a hierarchical active therapy program progressed on ability
3hrs biweekly; 12 weeks
No Control DSN=7
Age= ± 3.4 yrs
Kinematic joint angle data for ascent and decent phases
Observational analysis
Significant in R. ankle, L. hip and trunk
Qualitative and quantitative showed improvements in stair walking
Lafferty 200517
Pre – post, Level 4, PEDro 5
Intervention and Population
Outcome, Measures and Results
Active Therapy / Stair Walking• Whole and part task stair walking practice
improvements • Exercises could easily be used in therapy • Study design and methodology assessed as:
– Sackett Levels of Evidence: 4 – PEDro score: 5
• Most significant critique– Small sample size of only 7
Clinical recommendation: whole and part task stair walking may be useful to facilitate stair walking in children with DS
Treadmill Training
www.kines.umich.edu
Treadmill Training
Stepping on a treadmill + traditional PT
From 1 – 8 mins, 5 days/week, until independently walking
Control: traditional PT, 2x/week, until independently walking
DS, N=30
Control (N=15) Experiment (N=15)
Ages:
Control (312.1 days±)Experiment (302.6 days±)
Independent walking: # of days from onset of study until independent
Significant p=0.02 Experiment: 300 days ±Control: 401 days ±
Ulrich et al. 20018
Randomized control trial, Level 2b, PEDro 6
Intervention and Population
Outcome, Measures and Results
Clinical recommendation: treadmill training should be considered as a treatment option for infants with DS
• Treadmill training is unique and innovative
• Of the reviewed studies it is the highest quality– Sackett Levels of Evidence: 2b– PEDro score: 6
• Outcomes showed statistically significant improvements
• ? practicality of implementation for clinicians
Treadmill Training
Horseback Riding
www.downsyndromefoundation.org/images/PICT0035.JPG
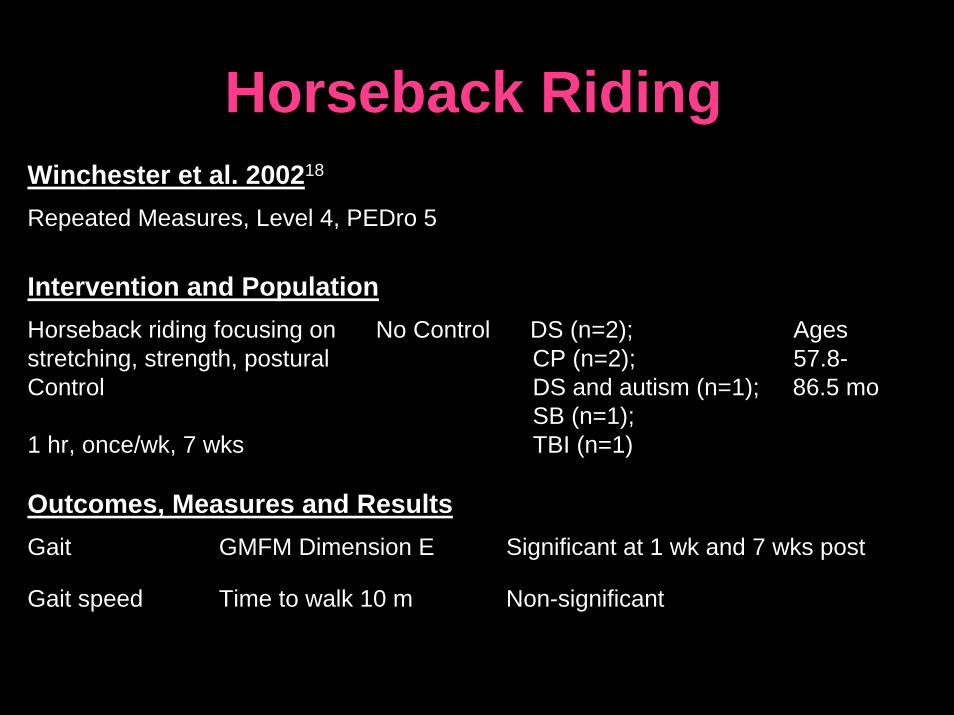
Horseback RidingWinchester et al. 200218
Repeated Measures, Level 4, PEDro 5
Intervention and PopulationHorseback riding focusing on No Control DS (n=2); Ages stretching, strength, postural CP (n=2); 57.8-Control DS and autism (n=1); 86.5 mo
SB (n=1);1 hr, once/wk, 7 wks TBI (n=1)
Outcomes, Measures and ResultsGait GMFM Dimension E Significant at 1 wk and 7 wks post
Gait speed Time to walk 10 m Non-significant
Horseback Riding• Previously shown to improve strength and balance in
developmentally delayed children19,20
• Sustained improvements at 7 week follow- up
• Study design quality and methodology assessed as: – Sackett Levels of Evidence: 4 – PEDro score: 5
• Most significant critique– Small sample size of 7, only 3 had DS
Clinical recommendation: therapeutic horseback riding may be considered for use when treating the gait of children with DS in combination with other therapies

Sensory Integration Therapy, Vestibular Therapy, or
Neurodevelopmental Therapy
www.whiterose4jon.net/sitebuilder/images/Jon-in-Swing-597x451.jpg
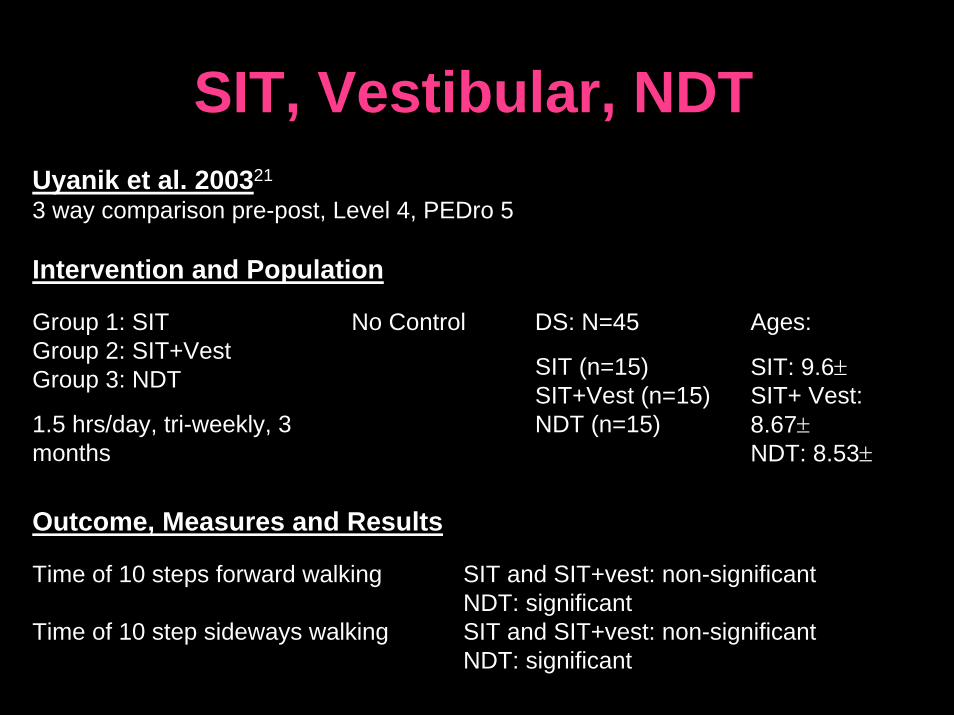
SIT, Vestibular, NDT
Group 1: SIT Group 2: SIT+VestGroup 3: NDT
1.5 hrs/day, tri-weekly, 3 months
No Control DS: N=45
SIT (n=15)SIT+Vest (n=15)NDT (n=15)
Ages:
SIT: 9.6±SIT+ Vest: 8.67±NDT: 8.53±
Time of 10 steps forward walking
Time of 10 step sideways walking
SIT and SIT+vest: non-significant NDT: significantSIT and SIT+vest: non-significant NDT: significant
Uyanik et al. 200321
3 way comparison pre-post, Level 4, PEDro 5
Intervention and Population
Outcome, Measures and Results
SIT, Vestibular, NDT• Study design quality and methodology assessed
as: – Sackett Levels of Evidence: 4 – PEDro score: 5
• One of the largest sample sizes of articles analyzed
• Most significant critique– No control group
Clinical recommendation: Since NDT was found to be effective at improving walking skills of children with DS it may be considered a treatment option
Strength Intervention
www.uoregon.edu/~vaintrob/katya/climb_up.jpg
Strength Intervention
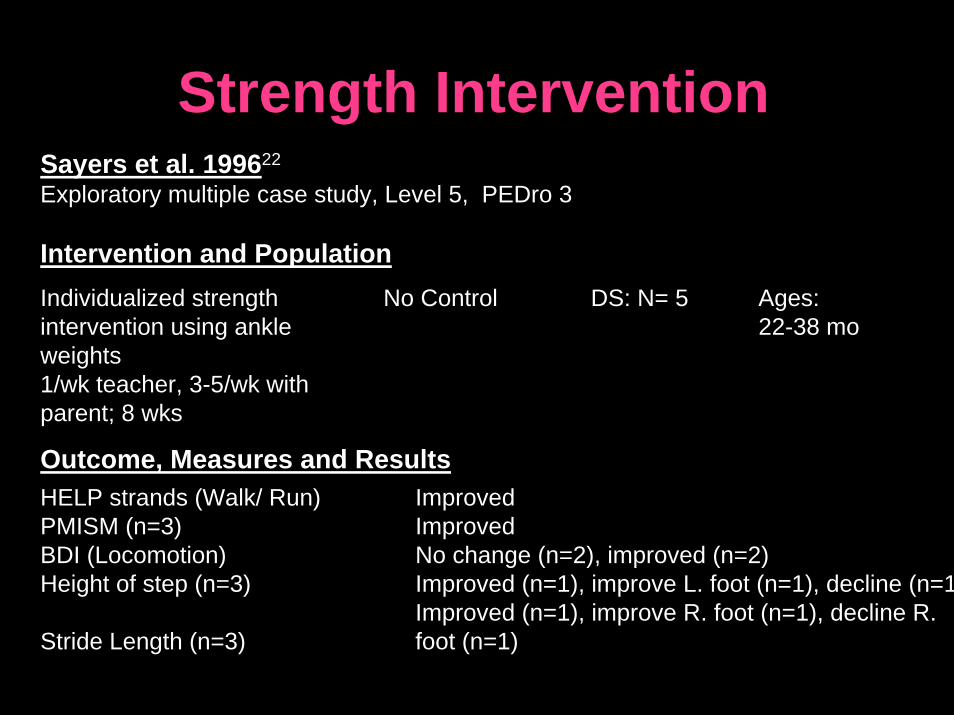
Individualized strength intervention using ankle weights 1/wk teacher, 3-5/wk with parent; 8 wks
No Control DS: N= 5 Ages: 22-38 mo
HELP strands (Walk/ Run) PMISM (n=3)BDI (Locomotion) Height of step (n=3)
Stride Length (n=3)
Improved ImprovedNo change (n=2), improved (n=2) Improved (n=1), improve L. foot (n=1), decline (n=1Improved (n=1), improve R. foot (n=1), decline R. foot (n=1)
Sayers et al. 199622
Exploratory multiple case study, Level 5, PEDro 3
Intervention and Population
Outcome, Measures and Results
Strength Intervention• Study design quality and methodology assessed as:
– Sackett Levels of Evidence: 5 – PEDro score: 3
• Results are difficult to interpret– Qualitative study design– Lack statistical analyses – Small sample size: 1 withdrawal, 1 child incomplete data
• Acknowledging each child’s health needs and individualization of therapy is commended
Clinical recommendations: we are unable to draw any clinical conclusions from this research
Developmental Coaching
http://community.nursingspectrum.com/MagazineArticles/article.cfm?AID=12259
Developmental CoachingEsenther 198423
Retrospective Study, Level 3, PEDro 1
Intervention and PopulationDevelopmental coaching with Control: Normative DS Ages not3 hand skills, 3 mobility skills values from literature N=40 reportedtargeted of typical children
Duration and frequency of intervention not specified
Outcomes, Measures and Results
Independent walking : Bonaparte 40% achieved free walking by 18 Infant Parent Service (BIPS) months of agefree walking category
Clinical recommendations: we are unable to draw any clinical conclusions from this research
Developmental Coaching• Of the reviewed studies it is the lowest quality
– Sackett Levels of Evidence: 4– PEDro score: 1
• Most significant critique– Retrospective study design without true experimental
manipulation– No integrated control group
• Uncertainty of intervention
Jump Training
www.theulloms.com/hopscotch2.jpg
Jump TrainingWang et al. 200224
Pre-Post, Level 4, PEDro 5
Intervention and Population
Horizontal and vertical Control: Typically DS Ages:jump practice developing children N=20 3-6 years
30 min practice sessions3 x/week, 6 weeks
Outcomes, Measures and Results
Gait: # of steps walking on a Significantly greater pre-post forward line and balance beam scores compared to typically
developing children
Jump Training• Study design quality and methodology assessed
as: – Sackett Levels of Evidence: 4– PEDro score: 5
• Improvements of only 1-2 additional steps is statistically significant but is it functionally significant ?
Clinical recommendations: balance and jumping hadpositive (although small) effects, thus, it could be considered as part of a program to improve the gait of children with DS
Conclusions• Current research is a heterogeneous mix of
interventions and outcomes
• Low quality designs overall
• We recommend combinations of different therapies that accommodate child’s specific needs and preferences
• We strongly encourage all pediatrictherapists to continuously re-evaluate each child’s progress in order to ensure best evidence practice

Future Research• More research must be
done
• Higher quality research
• Optimal treatment parameters
• Emerging research25-30 www.goldcoastdownsyndrome.org
Limitations• Some studies could not be evaluated
because full text not in English
• Authors lack of expertise in the field of publishing literature
• Limited experience in working with children with DS

AcknowledgementsThank you to clinicians and researchers Anne Chin, Bonnie Forrester, Julia Looper, Kenneth Pitetti, Charmayne Ross and Dale Ulrich
www.goldcoastdownsyndrome.org
Special thank you to:
Susan HarrisNaznin Virji-Babul Charlotte Beck Angela Busch For their support and contributions ☺

References1. Goodman CC, Fuller KS, Boissonnault WG. Pathology: Implications for the Physical Therapist. 2nd
ed. Philadelphia: Elsevier; 2003. 2. Shields N, Dodd K. A systematic review on the effects of exercise programmes designed to improve
strength for people with Down syndrome. Phys Ther Rev. 2004;9:109-115. 3. Carr J. Mental and motor development in young mongol children. J Ment Defic Res. 1970;14:205-220. 4. Hall B. Somatic deviations in newborn and older mongoloid children: Follow up investications. Acta
Paediatr Scand. 1970;59:199-204. 5. Share J, Veale AMO. Developmental Landmarks for Children with Down's Syndrome (Mongolism).
Dunedin, New Zealand: University of Otago Press; 1974. 6. Harris SR. Physical therapy and infants with down's syndrome: The effects of early intervention.
Rehabil Lit. 1981;42:339-343. 7. Bax M. Walking. Dev Med and Child Neur. 1991;33:471-472.8. Ulrich DA, Ulrich BD, Angulo-Kinzler RM, Yun J. Treadmill training of infants with down syndrome:
Evidence-based developmental outcomes. Pediatrics. 2001;108:E84-E84. 9. Jobling A, Virji-Babul N, Nichols D. Children with down syndrome: Discovering the joy of movement.
Joperd. 2006;77:34-54. 10. Gibson D, Harris A. Aggregated early intervention effects for Down’ssyndrome persons: patterning
and longevity of benefits. J Mental Def Research. 1988;32:1–17.11. Nilholm C. Early intervention with children with Down syndrome—past and future issues. Down
Syndrome: Res Pract. 1996;4:51–5812. 14th General Meeting World Confederation of Physical Therapy. Description of Physical Therapy-
What is Physical Therapy? Available at: http://www.wcpt.org/policies/description/whatis.php. Accessed July/22, 2007.
References13. Sackett DL, Strauss SE, Richardson WS. Evidence-Based Medicine: How to Practice and Teach
EBM. London: Churchill-Livingstone; 2000. 14. Martin K. Effects of supramalleolar orthoses on postural stability in children with Down syndrome.
Developmental Medicine & Child Neurology. 2004;46:406-411. 15. Selby-Silverstein L, Hillstrom HJ, Palisano RJ. The effect of foot orthoses on standing foot posture
and gait of young children with down syndrome. Neurorehabilitation. 2001;16:183-193. 16. Pitetti K, Wondra V. Dynamic foot orthosis and motor skills of delayed children. Journal of Prosthetics
& Orthotics (JPO). 2005;17:21-26. 17. Lafferty ME. A stair-walking intervention strategy for children with down's syndrome. Journal of
Bodywork & Movement Therapies. 2005;9:65-74. 18. Winchester P, Kendall K, Peters H, Sears N, Winkley T. The effect of therapeutic horseback riding on
gross motor function and gait speed in children who are developmentally delayed. Phys Occup TherPediatr. 2002;22:37-50.
19. Campbell S. Efficacy of therapeutic horseback riding on posture in children with cerebral palsy. Phys Ther. 1990;90:135-140.
20. Bertoti D. Clinical suggestions: Effect of therapeutic horseback riding on posture in children with cerebral palsy. Phys Ther. 1991;10:1505-1512.
21. Uyanik M, Bumin G, Kayihan H. Comparison of different therapy approaches in children with down syndrome. Pediatr Int. 2003;45:68-73.
22. Sayers LK, Cowden JE, Newton M, Warren B, Eason B. Qualitative analysis of a pediatric strength intervention on the developmental stepping movements of infants with down syndrome. Adapted Physical Activity Quarterly. 1996;13:247-268.
23. Esenther SE. Developmental coaching of the down syndrome infant. Am J Occup Ther. 1984;38:440-445.
24. Wang W, Ju Y. Promoting balance and jumping skills in children with down syndrome. Percept Mot Skills. 2002;94:443-448.
ReferencesFuture Research
25. Looper, Julia E. Ulrich, Dale A. The Effects of Foot Orthoses on Gait in New Walkers with Down syndrome. Pediatric Physical Therapy. 2006;18(1):96-97. Not yet published.
26. Wu, Jianhu. The effect of early treadmill training on gait. Gait and Posture. Not yet published.
27. Ulrich D and Angulo Barroso R. Optimizing treadmill training to improve onset and quality of gait in infants with Down syndrome . Current Research.
28. Ulrich D and Angulo Barroso R. Long term outcomes of preambulatory treadmill training in children with Down syndrome. Current Research.
29. Llpyd M, Ulrich D. Relationship between kicking and motor milestones in infants with Down syndrome:An early intervention study. Current Research.
30. Ulrich D. The effects of learning to ride a two wheel bicycle in 8-15 year old children with Down syndrome: A randomized trial. Current Research.
ReferencesPhotographs1. Gabriel House of Mexico2. http://medicalimages.allrefer.com/large/hypotonia.jpg3. www.cbdsa.com/images/Warrick_xmas06_008.jpg4. http://farm1.static.flickr.com/58/221312636_293942d007.jpg5. www.childrensaustin.org/ama/icache/w300h400/orig/Lily.jpg6. www.ndss.org/index.php?option=com_content&task=view&id=1812&Itemid=957. www.dsala.org/graphics/photos/baby_angels-4.jpg8. http://www.sharethedream.co.nz/images/paris.jpg9. http://campos-davis.com/infoweek/infoweek/angelmaria.jpg10. http://www.plan.ca/belong/uploaded_images/beautiful_baby_cdss-756468.bmp11. http://www.cdadc.com/jacobage6learningtoread.jpg12. www.babble.com/CS/photos/may2007/images/19911/original.aspx13. www.beaumonthospitals.com/images/center/f3c_flowerdoll.jpg14. \www.footdoc.ca/www.FootDoc.ca/Orthotics.JPEG15. www.faqs.org/health/images/uchr_04_img0399.jpg16. www.kines.umich.edu/17. www.downsyndromefoundation.org/images/PICT0035.JPG18. www.whiterose4jon.net/sitebuilder/images/Jon-in-Swing-597x451.jpg19. www.uoregon.edu/~vaintrob/katya/climb_up.jpg20. http://community.nursingspectrum.com/MagazineArticles/article.cfm?AID=1225921. http://www.theulloms.com/hopscotch2.jpg22. www.goldcoastdownsyndrome.org23. www.foietlumiere.org/site/english/001.html
Video1. Naznin-Virji Babul. Down Syndrome Research Foundation.

Questions???w
ww
.pla
n.ca
/bel
ong/
uplo
aded
_im
ages
/bea
utifu
l_ba
by_c
dss-
7564
68.b
mp