Embed Size (px)
Citation preview

The Effectiveness of Financial Incentives for HealthBehaviour Change: Systematic Review and Meta-AnalysisEmma L. Giles1*, Shannon Robalino1, Elaine McColl2, Falko F. Sniehotta1, Jean Adams1
1 Institute of Health and Society, Newcastle University, Newcastle upon Tyne, Tyne and Wear, United Kingdom, 2 Newcastle Clinical Trials Unit, Institute of Health and
Society, Newcastle University, The Medical School, Framlington Place, Newcastle upon Tyne, Tyne and Wear, United Kingdom
Abstract
Background: Financial incentive interventions have been suggested as one method of promoting healthy behaviourchange.
Objectives: To conduct a systematic review of the effectiveness of financial incentive interventions for encouraging healthybehaviour change; to explore whether effects vary according to the type of behaviour incentivised, post-interventionfollow-up time, or incentive value.
Data Sources: Searches were of relevant electronic databases, research registers, www.google.com, and the reference listsof previous reviews; and requests for information sent to relevant mailing lists.
Eligibility Criteria: Controlled evaluations of the effectiveness of financial incentive interventions, compared to nointervention or usual care, to encourage healthy behaviour change, in non-clinical adult populations, living in high-incomecountries, were included.
Study Appraisal and Synthesis: The Cochrane Risk of Bias tool was used to assess all included studies. Meta-analysis wasused to explore the effect of financial incentive interventions within groups of similar behaviours and overall. Meta-regression was used to determine if effect varied according to post-intervention follow up time, or incentive value.
Results: Seventeen papers reporting on 16 studies on smoking cessation (n = 10), attendance for vaccination or screening(n = 5), and physical activity (n = 1) were included. In meta-analyses, the average effect of incentive interventions was greaterthan control for short-term (#six months) smoking cessation (relative risk (95% confidence intervals): 2.48 (1.77 to 3.46);long-term (.six months) smoking cessation (1.50 (1.05 to 2.14)); attendance for vaccination or screening (1.92 (1.46 to 2.53));and for all behaviours combined (1.62 (1.38 to 1.91)). There was not convincing evidence that effects were different betweendifferent groups of behaviours. Meta-regression found some, limited, evidence that effect sizes decreased as post-intervention follow-up period and incentive value increased. However, the latter effect may be confounded by the former.
Conclusions: The available evidence suggests that financial incentive interventions are more effective than usual care or nointervention for encouraging healthy behaviour change.
Trial Registration: PROSPERO CRD42012002393
Citation: Giles EL, Robalino S, McColl E, Sniehotta FF, Adams J (2014) The Effectiveness of Financial Incentives for Health Behaviour Change: Systematic Reviewand Meta-Analysis. PLoS ONE 9(3): e90347. doi:10.1371/journal.pone.0090347
Editor: Hamid Reza Baradaran, Iran University of Medical Sciences, Iran (Islamic Republic of)
Received December 5, 2013; Accepted January 28, 2014; Published March 11, 2014
Copyright: � 2014 Giles et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permitsunrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Funding: This work is produced under the terms of a Career Development Fellowship research training fellowship issued by the NIHR to JA. The views expressedare those of the authors and not necessarily those of the NHS, The National Institute for Health Research or the Department of Health. JA & ELG are funded in part,and FFS is funded in full by Fuse: the Centre for Translational Research in Public Health, a UKCRC Public Health Research Centre of Excellence. Funding for Fusefrom the British Heart Foundation, Cancer Research UK, Economic and Social Research Council, Medical Research Council, the National Institute for HealthResearch, under the auspices of the UK Clinical Research Collaboration, is gratefully acknowledged. The funders had no role in study design, data collection andanalysis, decision to publish, or preparation of the manuscript.
Competing Interests: Jean Adams is a PLOS ONE Editorial Board Member; this does not alter our adherence to PLOS ONE Editorial policies and criteria. No otherauthors have any conflicts of interest.
* E-mail: [email protected]
Introduction
Despite consistent efforts to encourage uptake of healthy
behaviours [1,2], unhealthy behaviours remain common in
developed countries [3]. Financial incentives have been suggested
as one method of promoting healthy behaviour change.
Individual decisions to engage in behavioural options are
influenced by beliefs about the likely consequences of performing
those behaviours [4]. Individuals commonly hold inconsistent
preferences for outcomes occurring at different points in the
future, and for outcomes that are more or less certain. In general,
outcomes that will occur in the near future or with more certainty,
are valued more than those in the distant future or with less
PLOS ONE | www.plosone.org 1 March 2014 | Volume 9 | Issue 3 | e90347

certainty [4]. Whilst anticipated health gains of healthy behaviours
are often delayed in time and are uncertain (e.g. reduced risk of
disease in the future), the financial and opportunity costs can be
immediate and certain (e.g. giving up leisure time to take part in
physical activity) [5]. As these immediate, certain costs are often
‘dis-valued’ more than the delayed, uncertain health benefits are
valued, individuals make a ‘rational’ choice to pursue unhealthy
behaviours. It is hypothesised that health promoting financial
incentive interventions (HPFI) provide near-immediate and
certain rewards for, or reduce the immediate costs of, health-
promoting behaviours, and so change the reward structure
associated with these behaviours making them more attractive to
individuals [5].
The complexities of HPFI and the challenges of defining them
have been previously acknowledged [6,7]. However, incentive
interventions share in common that they offer motivating rewards
contingent on behavioural performance [6,8]. Here we define
HPFI as cash or cash-like rewards (e.g. vouchers that can be
exchanged for goods or services) or penalties (e.g. reductions in
welfare benefits), provided contingent on performance of healthy
behaviours.
It is commonly suggested that HPFI are more useful for
encouraging simple one-off behaviours, such as attendance for
vaccinations, than more complex sustained behaviour change,
such as smoking cessation [9–11]. However, we are not aware of
any systematic evidence synthesis that has arrived at this
conclusion, but it may be related to a common concern that the
effects of HPFI diminish quickly after incentives are withdrawn
[12,13], meaning that any behaviour change achieved is unlikely
to be sustained. A previous review did conclude that external
rewards can reduce an individual’s internal motivation to pursue
behaviour change, such that they become dependent on the
reward, rather than any personal desire to pursue the healthy
behaviour [14]. However, this finding is based on laboratory-
based research and may not be generalisable to community
settings.
Some authors have suggested that HPFI may be more suitable
for, or attractive to, individuals living in more deprived
circumstances [15,16]. However, variations in effectiveness of
HPFI across population groups have not been systematically
explored. Overall, little is known about what makes an effective
HPFI, in terms of value, format or other characteristics of the
incentive, behaviour, or recipient.
A number of reviews, using both systematic and other methods,
have now been conducted on the effects of HPFI [11,17–23].
However, these focus on single, specific behaviours rather than
exploring the full range of healthy behaviours [17,21–23]; are
restricted to developing countries where absolute financial
hardship may be more common than in developed countries
[20]; or use non-systematic methods for searching and screening,
meaning that findings may be biased [11,18,19].
We aimed to fill the gaps identified by conducting a systematic
review of primary studies exploring the effectiveness of HPFI
compared to non-intervention or usual care, to encourage uptake
of any healthy behaviours, in non-clinical adult populations living
in high-income countries. We also explored whether the effects of
HPFI varied according to the type of behaviour incentivised,
follow-up time after incentive withdrawal, or the value or format of
the incentive itself.
Methods
The protocol (see File S1) for this review was published in full
[24] and registered with PROSPERO before searching com-
menced (Registration no. 2012:CRD42012002393). Although a
number of the original research questions could not be answered
due to limited data availability, there were no substantive
variations from the protocol. The review is reported according
to the Preferred Reporting Items for Systematic Reviews
(PRISMA) guidelines (see Checklist S1) [25].
Information sourcesRelevant electronic databases of peer-reviewed literature were
searched from the earliest date available to April 2012. These
were: Medline, Embase, Science Citation Index, Cumulated Index
to Nursing and Allied Health Literature (CINAHL), Social
Science Citation Index, PsycINFO, Applied Social Science Index
and Abstracts, International Bibliography for the Social Sciences
and The Cochrane Library (including DARE, CENTRAL, HTA,
and NHS EDD). The search strategy combined relevant terms for
‘incentives’, ‘behaviour’ and ‘behaviour change’. An example of
the full electronic search strategy used in MEDLINE is provided in
File S2 and this was adapted, as appropriate, for other databases.
Manual searches of online research registers (Current Con-
trolled Trials, clinicaltrials.gov) were conducted alongside searches
of www.google.com. Relevant National Academic Mailing List
groups (Jiscmail) were also sent requests for relevant information.
The reference lists of relevant previous reviews [11,17,18,21–
23,26–46] and all papers meeting the inclusion criteria [47–63]
were also reviewed. Citation searches of included papers were
conducted using Science Citation Index and Social Science
Citation Index.
Endnote 66 was used to manage search results.
Eligibility criteriaWe searched for published and unpublished controlled evalu-
ations of the effectiveness of HPFI, compared to no intervention or
usual care, to encourage uptake of healthy behaviours in non-
clinical adult populations, living in high-income countries. The
inclusion criteria are described in full in Table S1. The inclusion of
all controlled study designs was as suggested by the Cochrane
Effective Practice and Organisation of Care Group (http://epoc.
cochrane.org/epoc-resource). In order to focus on the effect of
financial incentives on health behaviour change, only studies that
had behavioural outcomes were included. Studies that used
process markers of change only (e.g. weight loss, but not physical
activity or diet) were excluded. We restricted the review to studies
measuring behaviour change using objective, or validated self-
reported, methods to ensure high levels of validity. By ‘validated
self-report’ we mean non-objective measures that have previously
been reported to be valid compared to an objective measure. We
restricted the review to non-clinical populations to ensure
applicability to behaviour change in free-living ‘healthy’ adults
and so ensure maximum public health applicability. Many
‘incentive’ schemes offer participants a non-guaranteed reward
for behaviour change – e.g. entry into a lottery. Individuals differ
in their conceptualisations of risk and uncertainty, and so we
restricted the review to HPFI interventions provided with 100%
certainty to ensure that such differences did not confound the
results.
Study selection and data collectionAfter exclusion of duplicates, the title and abstract of all
retrieved papers were screened by one researcher (ELG) to exclude
obviously irrelevant papers. The full texts of remaining papers
were independently screened by two researchers (ELG & JA) to
identify those meeting the inclusion criteria. Any disagreements
were resolved by discussions.
Systematic Review of Financial Incentives
PLOS ONE | www.plosone.org 2 March 2014 | Volume 9 | Issue 3 | e90347

Data was extracted independently by two researchers (ELG &
JA) using a pro-forma developed for this purpose. Extracted
information included: bibliographic details, information on
participants, HPFI interventions, comparators, outcomes, study
design, and results. Incentive interventions were described using a
framework for this purpose [6]. Disagreements were resolved by
discussion.
The inclusion criteria restricted HPFI to those that would
definitely be provided if behaviour change occurred. The value of
these certain HPFI, over and above participant payments, were
identified and converted into 2011 US$ to allow comparisons
between studies (http://www.measuringworth.com/ppowerus/).
Uncertain, chance incentives (e.g. entry into lotteries), were offered
alongside certain incentives in some studies. As the probability of
winning, and the value of winnings, was often not clear, these were
not included in calculations of total incentive value.
Risk of biasRisk of bias in included studies was assessed independently by
two researchers (ELG & JA) using the Cochrane Risk of Bias
Review Guidelines [64]. Disagreements were resolved by discus-
sion.
Synthesis of resultsStudies examining the effects of HPFI for similar behaviours
were grouped together in a tabular summary for narrative
synthesis.
Incentives were described, using a framework for this purpose
[6], in terms of: direction (reward or penalty), form (cash, vouchers
or goods), magnitude, whether incentives were certain only or also
included chance components, target behaviour, frequency of
reward (all or some instances incentivised), immediacy of reward
in relation to behaviour, schedule (fixed or variable), and
recipient(s) of incentives (individuals or groups). Where studies
reported more than one relevant comparison (e. g. multi-arm trials
comparing a number of different incentive values to control), all
were identified and described.
For all groups of behaviours where more than one relevant
comparison was present and sufficient data were available, meta-
analysis was undertaken by group. Where more than one
intervention arm from a single study was included in a single
meta-analysis, the control group was divided in proportion to the
relative sizes in each intervention arm to avoid double counting
[65]. Many studies on smoking cessation included a number of
different follow-up points. Meta-analyses of smoking cessation
studies were performed for medium (#six months) and longer
term (.six months) follow-up points and included only the longest
follow-up point in each category from each study.
In addition to meta-analyses by behavioural group, an overall
meta-analysis including all comparisons from all included studies,
where data was available, was also performed. This was restricted
to only the longest follow-up point from studies including multiple
follow-ups.
Throughout, random-effects meta-analysis was conducted using
Cochrane Collaboration Review Manager 5.1. Risk ratios (RR)
and 95% confidence intervals (CI) were calculated for use in forest
plots. Where there was evidence of a high level of heterogeneity
(i.e. I2.75%) [66], further sub-group analyses by intervention
design were explored. Contour enhanced funnel plots were drawn
using Comprehensive Meta-Analysis 2.0 to assess potential
publication bias.
Meta-regression was conducted within the same groups as meta-
analyses, to explore whether log transformed study RR varied by
incentive value, or (where appropriate) follow-up period. No other
characteristics of interventions or participants were reported
consistently enough to allow exploration of the effects of these
on RR. Unrestricted maximum likelihood mixed-effects meta-
regression was conducted in Comprehensive Meta-Analysis 2.0
and meta-regression plots, with points proportional in size to
comparison weights drawn.
Results
The full text of three papers that were potentially relevant could
not be located and were excluded from the review [67–69]. The
full text of 350 papers were screened and a total of 17 papers met
the inclusion criteria and were included in the review (Figure 1).
Two papers reported data from different follow up points for the
same study, leaving 16 included studies [51,52].
The characteristics of included studies are summarised in Table
S2. Of the 16 studies, ten studies focused on smoking cessation
[48,50–54,59–63], five on attendance for vaccination or screening
[47,55–58], and one on physical activity [49]. All included studies
were randomised controlled trails (RCTs) or cluster RCTs. All 14
studies which provided information on location were conducted in
the USA [47–56,58,61–63]. Authors of the remaining studies were
based in the USA and it is likely that participants were too
[57,59,60].
Most HPFI offered were cash rewards [48,49,51,52,57,59–63]
and/or vouchers exchangeable for a specific range of goods or
services [47,55,56]. Two studies [53,54] used deposit contracts
where participants made cash deposits at the start of the study
which were only returned in the event of successful behaviour
change – resulting in potential financial penalties. Two studies also
included additional uncertain rewards contingent on behaviour
change (e.g. entry into lotteries) in addition to certain rewards
[50,58].
The total value of certain financial incentives that study
participants could receive for successful behaviour change, over
and above any payments for study participation, ranged from
$5.16 [57], to $786 (in 2011 $US) [62].
Intervention periods in the smoking cessation studies ranged
from two weeks [59,60], to 24 months [54], with post-intervention
follow-up periods ranging from four weeks [59,60] to 24 months
[50–52,54]. Most studies on attendance for vaccination or
screening involved a reward for one-off attendance with no
prolonged intervention or follow-up period [47,55–57]. One study
assessed repeated attendances for a series of injections over a 24
week period with incentives provided for each attendance [58].
The physical activity study had an intervention period of four
weeks with final follow-up immediately following the intervention
period [49].
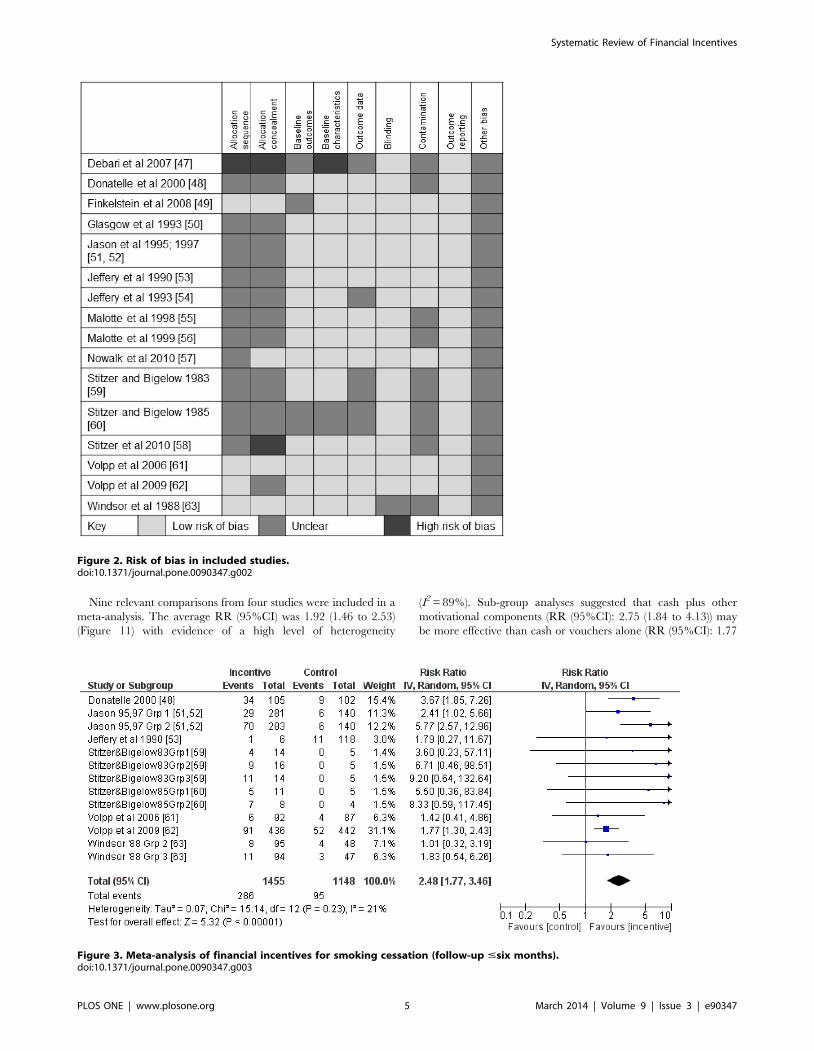
The risk of bias in included studies was low or unclear in most
areas in most studies (Figure 2). Allocation sequence and allocation
concealment, together with possible selection bias (the main source
of ‘other’ bias arising from using volunteer samples), were the main
potential sources of bias. The risk of bias was high in relation to
allocation sequence, allocation concealment, and baseline charac-
teristics in one study [47]. This study was not included in meta-
analyses or meta-regression due to insufficient data being
presented on numbers of participants in each group, and details
of outcomes in each group. Attempts to contact the authors were
unsuccessful.
Overall, 15 of the 16 studies met the criteria for inclusion in
meta-analyses and meta-regressions: all ten of the studies on
smoking cessation, four out of five of the studies on attendance for
vaccination and screening, and the single study on physical activity
– although this latter study was only included in the analysis of all
Systematic Review of Financial Incentives
PLOS ONE | www.plosone.org 3 March 2014 | Volume 9 | Issue 3 | e90347

behaviours combined. The remaining study on attendance for
screening was excluded due to insufficient data [47].
Smoking cessationMeta-analyses of 13 comparisons from eight studies on smoking
cessation which reported outcomes #six months follow-up,
revealed an average RR (95% CI) of 2.48 (1.77 to 3.46)
(Figure 3) in favour of incentives. An I2 of 21%, indicating low
evidence of heterogeneity [66], was not explored further. Meta-
regression of this group of studies revealed no evidence that study
RR was associated with follow-up time (beta (95%CI): 20.003
(20.01 to 0.003); Figure 4) or total incentive value (beta (95%CI):
20.003 (20.001 to 0.0008); Figure 5).
Six studies, including eight comparisons, were included in meta-
analysis of the effect of financial incentives for smoking cessation
for follow-ups .six months. This revealed an average RR (95%
CI) of 1.50 (1.05 to 2.14) (Figure 6). An I2 of 76% indicated high
evidence of heterogeneity. Subgroup analyses suggested that the
average effect of cash-only financial incentives (RR (95%CI): 1.57
(1.06 to 2.32) was greater than that for other formats (RR
(95%CI): 1.16 (0.45 to 2.94) and that the latter was not statistically
significant. Although high heterogeneity remained in the cash-only
sub-group (I2 = 83%), all other sub-group analyses resulted in
inclusion of groups containing only one comparison.
Meta-regression showed no evidence that the log transformed
RR of financial incentives for smoking cessation with .six months
follow-up varied by follow-up period (coefficient (95%CI): 0.0005
(20.002 to 0.001); Figure 7). However there was some evidence
that log transformed RR increased as incentive value increased
(coefficient (95%CI): 0.001 (0.0002 to 0.003); Figure 8).
Contour enhanced funnel plots did not suggest any funnel plot
asymmetry for either group of smoking cessation comparisons
(Figure 9 and Figure 10) meaning that the risk of publication bias
was low.
Attendance for vaccination or screeningOf the five studies reporting on the use of financial incentives for
increasing attendance for vaccination and screening, one focused
on attendance at breast and cervical screening [47], two on
attendance for tuberculosis (TB) skin test reading [55,56] and one
each on attendance for influenza and hepatitis B vaccination
[57,58].
Figure 1. Flow diagram of study selection and exclusion.doi:10.1371/journal.pone.0090347.g001
Systematic Review of Financial Incentives
PLOS ONE | www.plosone.org 4 March 2014 | Volume 9 | Issue 3 | e90347
Nine relevant comparisons from four studies were included in a
meta-analysis. The average RR (95%CI) was 1.92 (1.46 to 2.53)
(Figure 11) with evidence of a high level of heterogeneity
(I2 = 89%). Sub-group analyses suggested that cash plus other
motivational components (RR (95%CI): 2.75 (1.84 to 4.13)) may
be more effective than cash or vouchers alone (RR (95%CI): 1.77
Figure 2. Risk of bias in included studies.doi:10.1371/journal.pone.0090347.g002
Figure 3. Meta-analysis of financial incentives for smoking cessation (follow-up #six months).doi:10.1371/journal.pone.0090347.g003
Systematic Review of Financial Incentives
PLOS ONE | www.plosone.org 5 March 2014 | Volume 9 | Issue 3 | e90347

(1.33 to 2.35)). Considerable heterogeneity remained in one subgroup
(I2 = 89%) but other approaches to subgroup analyses resulted in
subgroups containing only one comparison and were not pursued.
Meta-regression revealed no evidence that log transformed RR
varied by incentive value (coefficient (95%CI): 20.0004 (20.004
to 0.003); Figure 12). However, visual inspection of Figure 12
shows minimal variation in incentive values offered. A contour
enhanced funnel plot did not suggest any evidence of publication
bias (Figure 13).
Figure 4. Meta-regression of follow-up period on relative risk, smoking cessation (follow-up ,six months).doi:10.1371/journal.pone.0090347.g004
Figure 5. Meta-regression of incentive value on relative risk, smoking cessation (follow-up up ,six months).doi:10.1371/journal.pone.0090347.g005
Systematic Review of Financial Incentives
PLOS ONE | www.plosone.org 6 March 2014 | Volume 9 | Issue 3 | e90347

Physical activityOnly one relevant comparison was included on physical activity
and meta-analysis was not undertaken for this behavioural group
[49]. This study used pedometers to measure average daily
physical activity over one-week periods and rewarded increases in
physical activity with increasing cash incentives. Over the four
Figure 6. Meta-analysis of financial incentives for smoking cessation (follow-up .six months).doi:10.1371/journal.pone.0090347.g006
Figure 7. Meta-regression of follow-up period on relative risk, smoking cessation (follow-up .six months).doi:10.1371/journal.pone.0090347.g007
Systematic Review of Financial Incentives
PLOS ONE | www.plosone.org 7 March 2014 | Volume 9 | Issue 3 | e90347

Figure 8. Meta-regression of incentive value on relative risk, smoking cessation (follow-up of .six months).doi:10.1371/journal.pone.0090347.g008
Figure 9. Contour enhanced funnel plot, smoking cessation (follow-up #six months).doi:10.1371/journal.pone.0090347.g009
Systematic Review of Financial Incentives
PLOS ONE | www.plosone.org 8 March 2014 | Volume 9 | Issue 3 | e90347

Figure 10. Contour enhanced funnel plot, smoking cessation (follow-up .six months).doi:10.1371/journal.pone.0090347.g010
Figure 11. Meta-analysis of financial incentives for attendance at vaccination and screening.doi:10.1371/journal.pone.0090347.g011
Systematic Review of Financial Incentives
PLOS ONE | www.plosone.org 9 March 2014 | Volume 9 | Issue 3 | e90347

week intervention period, participants in the financial incentive
arm took part in an average of 16 more minutes of physical activity
per day than those in the control arm. This difference was
statistically significant.
All behavioursA total of 25 relevant comparisons were included in a meta-
analysis of all behaviours that included only the longest follow up
point from studies with multiple follow-ups. The average RR
Figure 12. Meta-regression of incentive value on relative risk, attendance at vaccination & screening.doi:10.1371/journal.pone.0090347.g012
Figure 13. Contour enhanced funnel plot, attendance at vaccination and screening.doi:10.1371/journal.pone.0090347.g013
Systematic Review of Financial Incentives
PLOS ONE | www.plosone.org 10 March 2014 | Volume 9 | Issue 3 | e90347

(95%CI) was 1.62 (1.38 to 1.91) (Figure 14). Although an I2 of
84% suggested considerable heterogeneity, this was not explored
further.
Meta-regression showed some evidence that log transformed
RR decreased as post-intervention follow-up period increased
(coefficient (95%CI): 20.001 (20.002 to 20.0002); Figure 15) and
incentive value increased (coefficient (95%CI): 20.001 (20.002 to
20.0001); Figure 16). The funnel plot did not suggest clear
evidence of publication bias (Figure 17).
Discussion
Statement of principal findingsThis is the first systematic review which brings together
evidence on the effectiveness of financial incentive interventions
for encouraging uptake of the full range of health promoting
behaviours in non-clinical adult populations living in high-income
countries. A total of 17 papers reporting on 16 studies met the
inclusion criteria and were included in the review. These explored
the effect of HPFI on smoking cessation, attendance for
vaccinations or screening, and physical activity. Overall, this
Figure 14. Meta-analysis of financial incentives for all behaviours (latest follow-up point).doi:10.1371/journal.pone.0090347.g014
Systematic Review of Financial Incentives
PLOS ONE | www.plosone.org 11 March 2014 | Volume 9 | Issue 3 | e90347

review found evidence that HPFI were more effective than no
intervention, or usual care, in changing behaviours. This was seen
for groups of similar behaviours (i.e. smoking cessation, attendance
for vaccinations or screening) as well as when all behaviours were
combined. There was no clear evidence that HPFI were more
effective for ‘simple’ behaviours (e.g. attendance for vaccination or
screening) than ‘complex’ ones (e.g. smoking cessation). Financial
incentive interventions took a range of formats and it was difficult
to draw conclusions on the most effective of these, particularly
given the lack of detailed information on the exact nature of
interventions and study participants, as well as the absence of
trials which have sought to determine if effects of interventions
vary according to socio-demographic characteristics. When all
behaviours were grouped together, there was some evidence that
effect decreased as post-intervention period increased and as total
incentive value increased. However, it is possible that the latter
effect was confounded by the former.
Strength and weaknesses of studies in this reviewThis review found few controlled studies exploring the effect of
HPFI. The studies that were found were restricted to a small
number of behaviours. Further, primary, controlled studies
exploring the effect of financial incentives on change in a range
of other health-related behaviours are required.
The studies included did not appear to be at high risk of bias,
but there were some areas that were consistently at greater risk of
Figure 15. Meta-regression of follow-up point on relative risk, all behaviours (latest follow-up point).doi:10.1371/journal.pone.0090347.g015
Figure 16. Meta-regression of incentive value on relative risk, all behaviours (latest follow-up point).doi:10.1371/journal.pone.0090347.g016
Systematic Review of Financial Incentives
PLOS ONE | www.plosone.org 12 March 2014 | Volume 9 | Issue 3 | e90347

bias, particularly: allocation sequence generation and allocation
concealment. In most cases, information was not provided, rather
than it being clear that methods were weak. Future researchers
should consistently report trials according to existing reporting
guidance [70].
It appears that all 16 studies included in the review were US-
based, potentially limiting generalisability to other cultures and
contexts. Further studies based in other countries are required to
confirm that the effects reported here are generalisable to other
contexts.
The meta-regression plots revealed some gaps in the range of
incentive values and follow-up periods that have been explored. In
particular, few studies explored medium-size incentives (e.g. $40–
250) for encouraging attendance for vaccination and screening;
and few studies had post-intervention follow up periods beyond six
months.
Although we originally intended to explore if the effect of HPFI
varied according to recipient characteristics (e.g. age, gender,
socio-economic position), data was not reported in such a way to
allow this. Many other public health interventions are differentially
effective according to socio-demographic characteristics of partic-
ipants [71]. Further research is required to determine if HPFI are
particularly effective in some population groups.
Strengths and weaknesses of this reviewThis is the first systematic review and meta-analysis, that we are
aware of, that has explored the effect of financial incentives across
the full range of healthy behaviours in non-clinical settings in high-
income countries. Previous reviews have either focused on single
health behaviours [17,21–23], failed to use standard systematic
review methods [11,18,34], or have been limited to low and
middle-income countries [20].
Restriction to controlled study designs is recommended to
minimise risk of bias in conclusions and so increase confidence in
results (http://epoc.cochrane.org/epoc-resources). However, it
has been argued that other study designs can also contribute
useful information to reviews and an alternative approach to
evidence synthesis, for example a realist synthesis exploring the
context, mechanisms and outcomes of effective components of
financial incentive interventions for health behaviour change [72],
may help shed additional light on the financial incentive field. The
strict inclusion criteria, such as only including studies with
objective, or validated self-report behavioural outcome measures
and our focus on behaviour change (e.g. physical activity) rather
than proxies of this (e.g. body weight), further adds to the
confidence in the results; but similarly limits the number of studies
meeting the inclusion criteria.
Only studies comparing HPFI to usual care or no intervention
were included. Thus, the results indicate the effect of financial
incentives compared to minimal intervention. It is not, therefore,
clear how HPFI compare to other interventions. Given the
controversy associated with HPFI [73–76], society may prefer to
avoid the widespread use of HPFI if similarly effective alternative
interventions are available.
We used an extensive search strategy, including database
searches, expert recommendations of studies, and reference and
citation searches. As such, we are confident that we are unlikely to
have missed any relevant studies. However, it is difficult to
conclusively confirm this. In particular, three studies were not
fully screened for inclusion as the full papers could not be
retrieved [67–69].
We found considerable heterogeneity within some meta-
analyses. This likely reflects differences in methods, populations,
and interventions and is a reality of the type of intervention we
were studying [77]. We clearly presented the heterogeneity found,
whilst trying to choose appropriate sub-groups to limit it. We also
ensured that inclusion criteria were robust and checked that the
data was correct where in doubt (by contacting authors) before
undertaking meta-analyses [78].
Figure 17. Contour enhanced funnel plot, all behaviours (latest follow-up point).doi:10.1371/journal.pone.0090347.g017
Systematic Review of Financial Incentives
PLOS ONE | www.plosone.org 13 March 2014 | Volume 9 | Issue 3 | e90347

Interpretation of findings and comparison to previousfindings
Unlike previous non-systematic reviews [11,18,34], we used
well-recognised systematic review methodology with clear inclu-
sion criteria, substantially reducing the risk of bias in our findings.
Unlike previous systematic reviews [17,21–23], our inclusion
criteria covered the full range of healthy behaviours in non-clinical
adult populations living in high-income countries. Together, these
represent significant improvements on previous reviews.
Similar to previous findings, we found evidence that financial
incentives are effective at encouraging health-promoting behav-
iours [21,23,34]. In the meta-regression including all behaviours,
there was some evidence that effectiveness may decrease over time
post intervention period. This has previously been reported
[17,21,23]. However, statistically significant effects persisted at
least until six months post-intervention follow-up in smoking
cessation studies, suggesting that effects do not suddenly drop off
once incentives are withdrawn. Many health promotion interven-
tions are associated with behaviour change in the short, but not
longer, term [79] and this problem is not unique to HPFI.
Previous authors have suggested that HPFI may be more
effective in changing one-off health behaviours (such as attendance
for vaccination and screening) than more complex behaviours
(such as smoking) [9,11,12,23]. This study did not find convincing
evidence of this with the average RR of incentives for attendance
at vaccinations and screening (RR 1.92 (1.46 to 2.53) being less
than that for medium term smoking cessation (RR 2.48 (1.77 to
3.46), but greater than that for longer term smoking cessation (RR
1.50 (1.05 to 2.14). It is possible that the distinction between ‘one-
off’ and ‘complex’ behaviours is a false dichotomy in the context of
HPFI – with incentives for smoking cessation rewarding a series of
one-off behaviours. However, McEachan et al (2010) provide
evidence that smoking and attending for screening are considered
conceptually different on a number of dimensions by both ‘experts’
and members of the public [80]. Further work could usefully
explore whether the effectiveness of HPFI varies according to the
behavioural dimensions identified by McEachan et al (2010) – but
not enough data was available for such analysis in the current
review.
Meta-regression of all behaviours combined showed some
evidence that effects decreased as incentive value increased. As
incentive value was positively correlated with longest post-
intervention follow-up point (r = 0.44, p = 0.03), the finding in
relation to incentive value may be confounded by that related to
follow-up period. Unfortunately we were not able to conduct
multi-variate meta-regression to take account of this. Furthermore,
we found a positive relationship between inventive value and effect
size in smoking cessation studies with follow up of .six months,
suggesting that this effect is not consistent. Very weak evidence in
favour of larger value HPFI being more effective has been
previously reported [21]. However, other authors have suggested
that larger incentive values may be interpreted by recipients as
reflecting that the behaviour incentivised is somehow ‘risky’ and
thus that a payment is needed to offset this [81]. There are likely to
be complex relationships between incentive value and character-
istics of both incentivised behaviours and recipients that require
more detailed exploration.
Similar to previous reviews, we also found that the majority of
studies were US-based [34], and that insufficient evidence is
currently available to determine optimal incentive value, or format
for changing health behaviours [18]. The average RR reported
here are larger than some previously reported. For example, in
their original review of incentives as well as competitions for
smoking cessation, Cahill & Perera (2008) reported a pooled odds
ratio (95%CI) at six months follow up of 1.44 (1.01 to 2.04) [17],
(pooled odds ratios are not reported in the updated version of this
review) [82]. The comparable figures for the results in this review
were 3.12 (1.95 to 4.97) (note this is an odds ratio for
comparability, but the figures shown elsewhere are risk ratios).
However, this previous review included both competitions, as well
as incentives, and these differences in inclusion criteria may
explain the differences in results found.
Implications for policy and practiceFinancial incentives may be a useful addition to the behavioural
change toolkit, particularly for encouraging smoking cessation and
attendance for vaccination and screening. We did not find
convincing evidence that HPFI work better for changing short-
term, one-off behaviours than longer term, more complex
behaviours and HPFI should be considered across the spectrum
of healthy behaviours. Although there has been some previous
concern that the effects of HPFI may be short-lived once
incentives are withdrawn, we did not find convincing evidence
of this. Nor did we find convincing evidence that larger incentive
values are associated with greater behaviour change. This suggests
that small incentives may be effective, although it is not clear from
our results if larger incentives produce larger effects. However,
these issues have not been systematically investigated and it is not
clear what the most effective value, or format, of HPFI is.
Conclusion
The available evidence from controlled studies suggests that
HPFI are more effective than usual care or no intervention at
encouraging healthy behaviour change amongst non-clinical adult
populations living in high income countries. There was not
convincing evidence that HPFI are more effective for ‘simple’
compared to ‘complex’ behaviours. There was some evidence that
effects decrease as post-intervention follow-up increases and as
incentive value increases. However, the available evidence is
substantially limited, particularly in relation to the range of
behaviours studied.
Supporting Information
File S1 Protocol.
(PDF)
File S2 Search strategy for identification of studies for financial
incentives.
(PDF)
Table S1 Inclusion criteria.
(PDF)
Table S2 Characteristics of included studies.
(PDF)
Checklist S1 PRISMA checklist.
(PDF)
Author Contributions
Conceived and designed the experiments: JA FFS EM. Performed the
experiments: ELG JA SR. Analyzed the data: JA ELG. Contributed
reagents/materials/analysis tools: ELG JA FFS SR EM. Wrote the paper:
ELG JA EM FFS SR.
Systematic Review of Financial Incentives
PLOS ONE | www.plosone.org 14 March 2014 | Volume 9 | Issue 3 | e90347

References
1. Department of Health (1998) Our healthier nation: a contract for health.
London: Her Majesty’s Stationery Office.
2. Department of Health (2004) Choosing health: making healthier choices easier.London: Her Majesty’s Stationery Office.
3. Eastwood P (2009) Health survey for England 2008: trend tables.
4. Mazur JE (1987) An adjusting procedure for studying delayed reinforcement. In:
Commons ML, Mazur JE, Nevin JA, Rachlin H, editors. Quantitative analysisof behaviour The effect of delay and intervening events on reinforcement value.
Hillsdale, New Jersey: Erlbaum.
5. Lowenstein G, Brennan T, Volpp K (2007) Asymmetric paternalism to improvehealth behaviors. Journal of the American Medical Association 298: 2415–2417.
6. Adams J, Giles EL, McColl E, Sniehotta F (2013) Carrots, sticks, and health
behaviours: a framework for documenting the complexity of financial incentiveinterventions to change health behaviours. Health Psychology Review.
7. Johnston M, Sniehotta F (2010) Financial incentives to change patient
behaviour. Journal of Health Services Research and Policy 15: 131–132.
8. Abraham C, Michie S (2008) A taxonomy of behaviour change techniques usedin interventions. Health Psychology 27: 379–387.
9. Jochelson K (2007) Paying the patient: improving health using financial
incentives. London: King’s Fund.
10. Crockett R, Weinman J, Hankins M, Marteau T (2009) Time orientation andhealth-related behaviour: measurement in general population samples. Psychol-
ogy & Health 24: 333–350.
11. Sutherland K, Christianson JB, Leatherman S (2008) Impact of targetedfinancial incentives on personal health behavior: a review of the literature.
Medical Care Research and Review 65: 36S–78.
12. Oliver A, Marteau T, Ashcroft RE (2009) Can financial carrots improve health?Journal of Health Services Research & Policy 14: 1–2.
13. Petry NM (2010) Contingency management treatments: controversies and
challenges. Addiction 105: 1507–1509.
14. Deci E, Koestner R, Ryan R (1999) A meta-analytic review of experimentsexamining the effects of extrinsic rewards on intrinsic motivation. Psychological
Bulletin 125: 627–668.
15. Aveyard P, Bauld L (2011) Incentives for promoting smoking cessation: what westill do not know. Cochrane Database Syst Rev Apr13: ED000027 Avaliable:
http://www.thecochranelibrary.com/details/editorial/1052523/Incentives-for-promoting-smoking-cessation-what-we-still-do-not-know.html.
16. Cookson R (2008) Should disadvantaged people be paid to take care of their
health? Yes. BMJ 337.
17. Cahill K, Perera R (2008a) Competitions and incentives for smoking cessation.Cochrane Database of Systematic Reviews doi: 10.1002/14651858.CD004307.
pub3
18. Kane R, Johnson P, Town R, Butler M (2004) A structured review of the effectof economic incentives on consumers’ preventive behavior. American Journal of
Preventive Medicine 27: 327–352.
19. Kavanagh J, Stansfield C, Thomas J (2009) Incentives to improve smoking,physical activity, dietary and weight management behaviours: a scoping review
of the research evidence. London: Institute of Education, University of London.
20. Lagarde M, Haines A, Palmer N (2007) Conditional cash transfers for improvinguptake of health interventions in low- and middle-income countries: a systematic
review. JAMA 298: 1900–1910.
21. Paul-Ebhohimhen V, Avenell A (2008) Systematic review of the use of financialincentives in treatments for obesity and overweight. Obesity Reviews 9: 355–
367.
22. Prendergast M, Podus D, Finney J, Greenwell L, Roll J (2006) Contingencymanagement for treatment of substance use disorders: a meta-analysis.
Addiction 101: 1546–1560.
23. Wall J, Mhurchu C, Blakely T, Rodgers A, Wilton J (2006) Effectiveness of
monetary incentives in modifying dietary behavior: a review of randomized,controlled trials. Nutrition Reviews 64: 518–531.
24. Adams J, Giles EL, McColl E, Sniehotta F (2012) A systematic review of the use
of financial incentives to encourage uptake of healthy behaviours: protocol.Systematic Reviews 1: doi:10.1186/2046-4053-1181-1151.
25. Moher D, Liberati A, Tetzlaff J, Altman DG, The Prisma Group (2009)
Preferred reporting items for systematic reviews and meta-analyses: thePRISMA statement. PLoS Med 6: e1000097.
26. Achat H, McIntyre P, Burgess M (1999) Health care incentives in immunisation.
Aust N Z J Public Health 23: 285–288.
27. Avenell A, Broom J, Brown T, Poobalan A, Aucott L, et al. (2004) Systematicreview of the long-term effects and economic consequences of treatments for
obesity and implications for health improvement. Health Technol Assessment 8:1–182.
28. Bryant J, Bonevski B, Paul C, McElduff P, Attia J (2011) A systematic review and
meta-analysis of the effectiveness of behavioural smoking cessation interventionsin selected disadvantaged groups. Addiction 106: 1568–1585.
29. Cahill K, Perera R (2008) Quit and win contests for smoking cessation.
Cochrane Database of Systematic Reviews 3: CD004986.
30. Flodgren G, Eccles M, Shepperd S, Scott A, Parmelli E, et al. (2011) Anoverview of reviews evaluating the effectiveness of financial incentives in
changing healthcare professional behaviours and patient outcomes. CochraneDatabase of Systematic Reviews 6: CD009255.
31. Guiffrida A, Torgerson D (1997) Should we pay the patient? Review of financial
incentives to enhance patient compliance. BMJ 315: 703–707.
32. Hey K, Perera R (2005) Competitions and incentives for smoking cessation.
Cochrane Database of Systematic Reviews 2: CD004307.
33. Hey K, Perera R (2005) Quit and win contests for smoking cessation. Cochrane
Database of Systematic Reviews 2: CD004986.
34. Kavanagh J, Stansfield C, Thomas J (2009) Incentives to improve smoking,
physical activity, dietary and weight management behaviours: a scoping review
of the research evidence. London: Institute of Education.
35. Kavanagh J, Oakley A, Harden A, Trouton A, Powell C (2011) Are incentive
schemes effective in changing uoung people’s behaviour? A systematic review.
Health Education Journal 70: 192–205.
36. Leeks KD, Hopkins D, Soler R, Aten A, Chattopadhyay S, et al. (2010)
Worksite-based incentives and competitions to reduce tobacco use. A systematic
review. Am J Prev Med 38: S263–274.
37. Lussier JP, Heil SH, Mongeon JA, Badger GJ, Higgins ST (2006) A meta-
analysis of voucher-based reinforcement therapy for substance use disorders.
Addiction 101: 192–203.
38. Matson D, Lee J, Hopp J (1993) The impact of incentives and competitions on
participation and quit rates in worksite smoking cessation programs. Am J Health
Promot 7: 270–280.
39. Morgan O (2005) Approaches to increase physical activity: reviewing the
evidence for exercise-referral schemes. Public Health 119: 361–370.
40. Ogilvie DEM, Hamilton V, Petticrew M (2005) Promoting walking and cycling
as an alternative to using cars: a systematic review. BMJ 329: 1–5.
41. O’Malley GC, Baker PRA, Francis DA, Perry I, Foster C (2012) Incentive-based
interventions for increasing physical activity and fitness (protocol). Cochrane
Database of Systematic Reviews 1.
42. Peersman G, Harden A, Oliver S (1998) Effectiveness of health promotion
interventions in the workplace: a review. London: Health Education Authority.
43. Roux L, Pratt M, Tengs T, Yore M, Yanagawa T, et al. (2008) Cost-effectiveness
of community-based physical activity interventions. American Journal of
Preventive Medicine 35: 578–588.
44. Sabatino SA, Habarta N, Baron RC, Coates RJ, Rimer BK, et al. (2008)
Interventions to increase recommendation and delivery of screening for breast,
cervical, and colorectal cancers by healthcare providers - systematic reviews of
provider assessment and feedback and provider incentives. Am J Prev Med 35:
S67–S74.
45. Stone E, Morton S, Hulscher M, Maglione M, Roth E, et al. (2002)
Interventions that increase use of adult immunization and cancer screening
services: a meta-analysis. Annals of Internal Medicine 136: 641–651.
46. Yabroff KR, Mandelblatt JS (1999) Interventions targeted towards patients to
increase mammography use. Cancer Epidemiology, Biomarkers and Prevention
8: 749–757.
47. Debari RR, Servodidio C, Palomares M, Rodruguez-Furlow M, Staff I (2007)
Patient compliance/incentive study. Oncol Nurs Forum 34: 488.
48. Donatelle R, Prows S, Champeau D, Hudson D (2000) Randomised controlled
trial using social support and financial incentives for high risk pregnant smokers:
significant older supporter (SOS) program. Tobacco Control 9: 67–69.
49. Finkelstein E, Brown D, Brown D, Buchner DA (2008) A randomized study of
financial incentives to increase physical activity among sedentary older adults.
Prev Med 47: 182–187.
50. Glasgow R, Hollis J, Ary D, Boles S (1993) Results of a year-long incentives-
based worksite smoking-cessation program. Addict Behav 18: 455–464.
51. Jason LA, McMahon SD, Salina D, D.. Hedeker, Stockton M, et al. (1995)
Assessing a smoking cessation intervention involving groups, incentives and self-
help manuals. Behav Ther 26: 393–408.
52. Jason LA, Salina D, McMahon SD, Hedeker D, Stockton M (1997) A worksite
smoking intervention: a 2-year assessment of groups, incentives and self-help.
Health Educ Res 12: 129–138.
53. Jeffery R, Hellerstedt W, Schmid T (1990) Correspondence programs for
smoking cessation and weight control: a comparison of two strategies in the
Minnesota heart health program. Health Psychol 9: 585–598.
54. Jeffery RW, Forster JL, French SA, Kelder SH, Lando HA, et al. (1993) The
healthy worker project: a worksite intervention for weight control and smoking
cessation. Am J Public Health 83: 395–401.
55. Malotte C, Rhodes F, Mais K (1998) Tuberculosis screening and compliance
with return for skin test reading among active drug users. Am J Public Health 88:
792–796.
56. Malotte C, Hollingshead J, Rhodes F (1999) Monetary versus nonmonetary
incentives for TB skin test reading among drug users. Am J Prev Med 16: 182–
188.
57. Nowalk MP, Lin CJ, Toback Sl, Rousculp MD, Eby C, et al. (2010) Improving
influenza vaccination rates in the workplace. Am J Prev Med 38: 237–246.
58. Stitzer M, Polk T, Bowles S, T.. Kosten (2010) Drug user’s adherence to a 6-
month vaccination protocol: effects of motivational incentives. Drug Alcohol
Depend 107: 76–79.
59. Stitzer M, Bigelow G (1983) Contingent payment for carbon monoxide
reduction: effects of pay amount. Behav Ther 14: 647–656.
Systematic Review of Financial Incentives
PLOS ONE | www.plosone.org 15 March 2014 | Volume 9 | Issue 3 | e90347

60. Stitzer M, Bigelow G (1985) Contingent reinforcement for reduced breath
carbon monoxide levels: target-specific effects on cigarette smoking. Addict
Behav 10: 345–349.
61. Volpp K, Levy AG, Asch DA, Berlin JA, Murphy JJ, et al. (2006) A randomized
controlled trial of financial incentives for smoking cessation. Cancer Epidemi-
ology, Biomarkers and Prevention 15: 12–18.
62. Volpp KG, Troxel AB, Pauly MV, Glick HA, Puig A, et al. (2009) A randomized
controlled trial of financial incentives for smoking cessation. The New England
Journal of Medicine 360: 699–709.
63. Windsor R, Lowe J, Bartlett E (1988) The effectivness of a worksite self-help
smoking cessation program: a randomized trial. J Behav Med 11: 407–421.
64. Thomas B, Ciliska D, Dobbins M, Micucci S (2004) A process for systematically
reviewing the literature: providing the research evidence for public health
nursing interventions. Worldviews on Evidence-Based Nursing 1: 17–84.
65. Higgins J, Green S (2011) Cochrane handbook for systematic reviews of
interventions version 5.1. [updated March 2011]. Available: www.cochrane-
handbook.org: The Cochrane Collaboration.
66. Higgins J, Thompson S, Deeks J, Altman D (2003) Measuring inconsistency in
meta-analyses. BMJ 327: 557–560.
67. National Business Group on Health (2007) Financial incentives for healthy
lifestyles: who’s doing it, what’s legal and where’s the evidence? Avaliable: www.
businessgrouphealth.org/toolkits/et_financialincentives.cfm. Accessed 2013
June.
68. Robinow A (2007) Consumer incentives: strong examples in action: patient
choice health care. Philadelphia, PA: National Business Coalition on Health/
Leapfrog Group/Bridges to Excellence Meeting, Advancing Value-Driven
Health Care: The Third Annual Incentives and Rewards Symposium.
69. Resnick JH (1974) Smoking behavior - motives and incentives. Behavior
Therapy 5: 711–712.
70. Schulz K, Altman D, Moher D (2010) CONSORT 2010 Statement: updated
guidelines for reporting parallel group randomised trials. BMJ 340: c332.71. White M, Adams J, Heywood P (2009) How and why do interventions that
increase health overall widen inequalities within populations? In: Babones S,
editor. Social inequality and public health. Bristol: Policy Press. pp. 65–82.72. Pawson R (2006) Evidence based policy: a realist perspective. London: Sage.
73. Gardner B, Davies A, McAteer J, Michie S (2010) Beliefs underlying UKparents’ views towards MMR promotion interventions: a qualitative study.
Psychol Health Med 15: 220–230.
74. Oliver A, Marteau T, Ashcroft R (2009) Can financial carrots improve health?J Health Serv Res Policy 14: 1–2.
75. Parke J, Ashcroft R, Brown R, Marteau T, Seale C (2013) Financial incentives toencourage healthy behaviours: an analysis of UK media coverage. Health
Expect 16: 292–304.76. Promberger M, Brown R, Ashcroft R, Marteau T (2011) Acceptability of
financial incentives to improve health outcomes in the UK and US samples.
J Med Ethics 37: 682–687.77. Cochrane Collaboration (2002) Module 13: diversity and heterogeneity.
78. Higgins JPT, Thompson SG (2008) Commentary: heterogeneity in meta-analysis should be expected and appropriately quantified. International Journal
of Epidemiology 37: 1158–1160.
79. Rothman AJ (2000) Toward a theory-based analysis of behavioral maintenance.Health Psychology 19: 64–69.
80. McEachan RRC, Lawton RJ, Conner M (2010) Classifying health-relatedbehaviours: exploring similarities and differences amongst behaviours. British
Journal of Health Psychology 15: 347–366.81. Gneezy U, Meier S, Rey-Biel P (2011) When and why incentives (don’t) work to
modify behavior. Journal of Economic Perspectives 25: 191–210.
82. Cahill K, Perera R (2011) Competitions and incentives for smoking cessation.Cochrane Database of Systematic Reviews 4: CD004307.
Systematic Review of Financial Incentives
PLOS ONE | www.plosone.org 16 March 2014 | Volume 9 | Issue 3 | e90347





























